Introduction
Crossed fused renal ectopia (CFRE) is a rare
congenital anomaly in which both kidneys are located and fused on
the same side of the body, with a high incidence of stone formation
and urinary tract infection (1).
CFRE is the second most frequently observed congenital malformation
of the kidney after horseshoe anomaly, and occurs in 1 in
1,000–2,000 autopsies and ~0.01% of live births (1,2). There
are six primary categories of CFRE; however, there is no specific
clinical manifestation or standardized guideline for the management
of upper urinary tract calculi in CFRE (3). Due to the abnormal anatomical structure
of the kidney and ureter, as well as the abnormal relationship with
the surrounding structures (including the small bowel, vertebral
column and blood vessels), the treatment of upper urinary tract
calculi is technically challenging for urologists (4). Few studies have reported the treatment
of kidney stones in patients with CFRE and several treatment
methods are available, including extracorporeal shock wave
lithotripsy (ESWL) (5,6), percutaneous nephrolithotomy (PCNL)
(4,7–11),
laparoscopic nephrolithotomy (12)
and retrograde intrarenal surgery (RIRS) (13,14).
Open stone surgery is no longer performed in many hospitals and
there is not an optimal approach that is applicable in all cases
due to different stones sizes and different types of CFRE as
reported in the literature (11,12,15). In
the present study, all patients with CFRE and upper urinary tract
stones reported in the literature between 1996 and 2016 were
reviewed. Two patients treated at Xiangya Hospital (Changsha,
China) were retrospectively reviewed to provide suggestions for the
effective management of such patients in clinical practice.
Materials and methods
Ethics statement
The 2 patients involved in the present study
provided written informed consent to publish their case details.
The present study was reviewed and approved by the Ethics Committee
of Xiangya Hospital, Central South University (Changsha,
China).
Case study
Patient 1
Patient 1 was a 51-year-old woman admitted in
September 2013, who presented with a 10-day history of right flank
and right lower-abdominal pain with repeated urinary infections
over the past 2 years. The patient reported no gross hematuria and
no history of surgery or chronic renal disease. Physical
examination revealed mild knocking pain over the right flank
area.
The results of routine laboratory monitoring,
including hemogram, renal function and urine analysis, were normal.
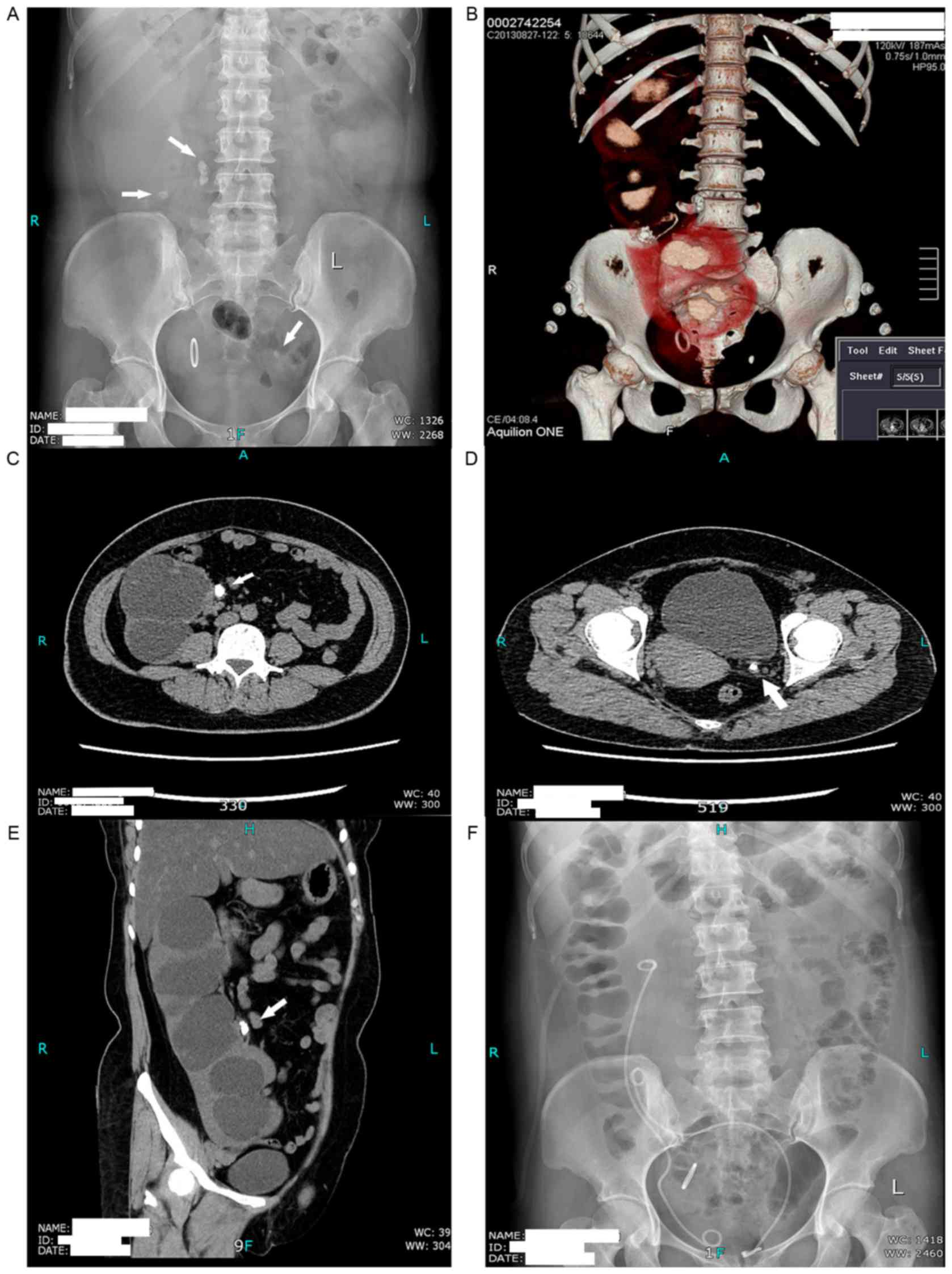
Radiography of the kidneys, ureters and bladder revealed several
right renal lower calices calculi and two possible ureteral
calculi, one located on the right side at the level of the third
lumbar vertebra and the other at the left ureteral orifice.
Abdominal computed tomography (CT) scan revealed a left-to-right
crossed fused kidney. The CT simultaneously confirmed bilateral
ureteral calculi (right, 2×1 cm; left, 0.5×0.8 cm) and right renal
calculi. The bilateral pelvicalyceal systems were moderately
dilated as a result (Fig. 1).
The patient was placed in a lithotomy position under
general anesthesia. Ureteroscopy revealed that the left calculus
was located in the left lower segment ureter ~0.5 cm from the left
ureteral orifice. The calculus was subsequently fragmented with a
holmium laser as previously described (16). The left ureter was completely twisted
to the right side and so the ureteroscope was unable to move
forward any further following intracorporeal lithotripsy. A 6 F
ureteral stent was placed in the left ureter and a 4 F ureteral
catheter was placed in the right ureter for the right PCNL. The
patient was subsequently turned to a prone position and a posterior
upper calyx puncture was performed as previously described
(4). Tract dilation was serially
performed using a fascial dilator from 8 F to 16 F and a matched
peel-away sheath was placed in the tract as previously described
(4). The stones were fragmented with
a holmium laser or pneumatic lithotripter through an 8 F rigid
ureteroscope. The stone-free status was confirmed, a 6 F double-J
stent (Bard, Murray Hill, NJ, USA) was inserted via the
percutaneous tract with the assistance of a guide wire and a
matched size nephrostomy tube was inserted in the collecting
system. The total surgical duration was 95 min. No obvious bleeding
occurred.
The patient's postoperative course was uneventful.
The duration of postoperative analgesia was 12 h and a
postoperative abdominal X-ray did not reveal any stone shadows
(Fig. 1F). The Foley catheter and
nephrostomy tube were removed at days 1 and 2 postoperatively,
respectively. The patient was discharged on day 3 post-surgery. The
two double-J stents were removed via cystoscopy at 1 month
post-surgery.
Patient 2
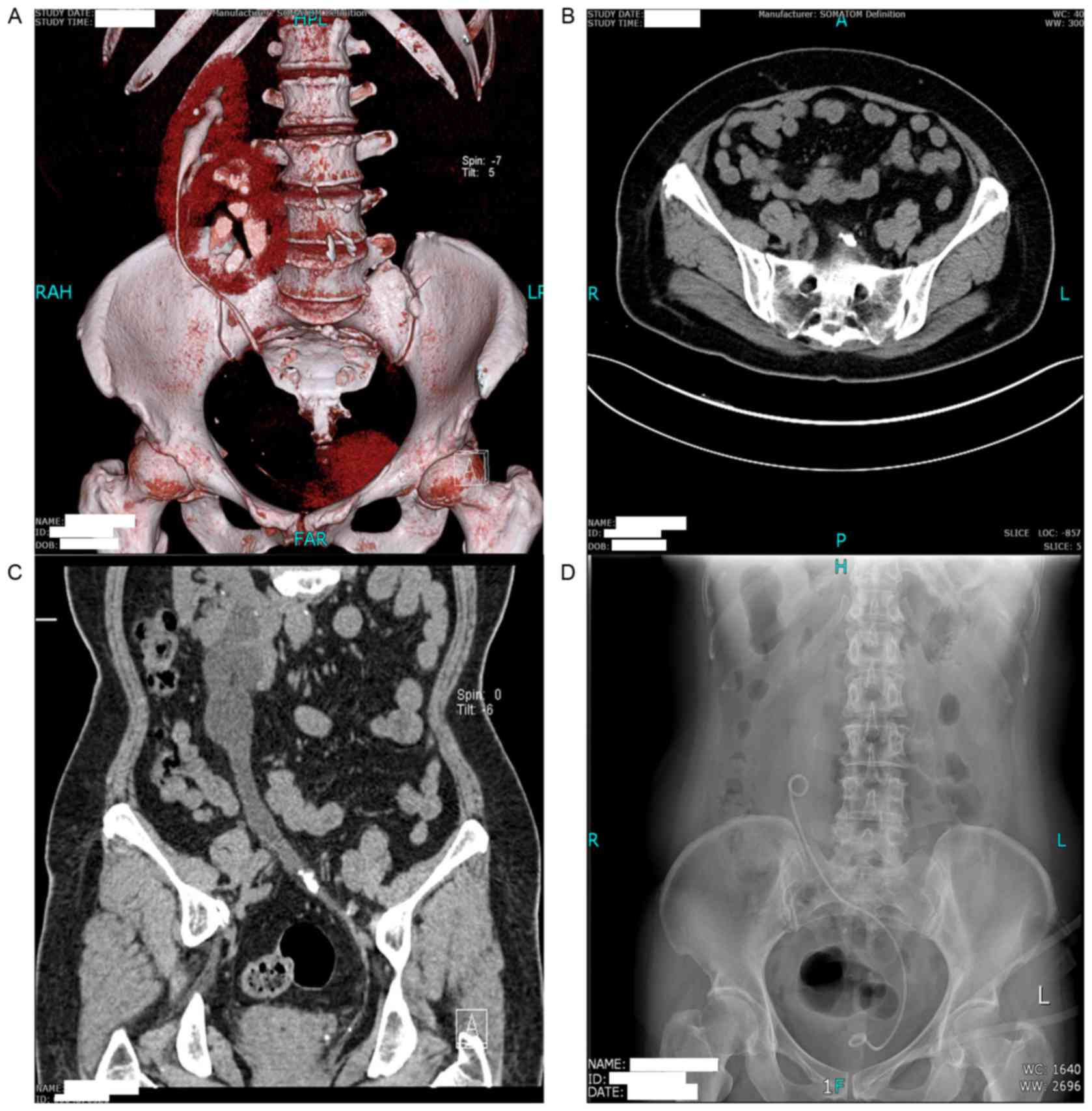
Patient 2 was a 62-year-old woman admitted in March
2016, who presented with a 3-month history of intermittent right
flank pain and repeated urinary infections over the preceding 8
years. No abnormalities were identified in standard laboratory
tests, with the exception of microhematuria. A CT scan revealed a
left-to-right crossed fused kidney in her abdomen and a left
ureteral stone (1.5×1 cm) was detected, causing the ectopic kidney
pelvicalyceal system and the upper ureters to be moderately dilated
(Fig. 2). An intracorporeal
lithotripsy by ureteroscope under intravertebral anesthesia was
planned. However, the left ureter was seriously twisted to the
right side, and so it was not possible to move forward to the right
location of the ureteral stone with a rigid ureteroscope. As such,
a flexible ureteroscope was used. The calculus was identified ~10
cm from the left ureteral orifice and subsequently completely
fragmented using a holmium laser. No stent or urinary drain was
inserted postoperatively, and the patient was discharged
uneventfully on day 2 post-surgery.
Literature review
PubMed (ncbi.nlm.nih.gov/PubMed) was searched for articles
published in English between May 1996 and May 2016. The search
terms used were as follows: ‘Stone,’ ‘stones,’ ‘calculus,’
‘calculi,’ ‘urolithiasis,’ ‘crossed fused,’ ‘CFRE,’ ‘kidney’ and
‘renal.’ ‘Bladder’ and ‘urethral’ were excluded from the search.
Articles that did not describe the treatment of patients were also
excluded.
Results
Case study
The 2 patients were discharged uneventfully without
major or minor complications. At the time of writing (follow-up
duration was 31 months in case 1 and 2 months in case 2), the
patients were asymptomatic and stone free with no notable
complications.
Literature review
Details of the case study patients and the patients
reported in the literature publications are summarized in Table I. Two studies (17,18)
included cases of crossed fused kidneys in their study groups with
more detailed description. It was therefore not possible to extract
enough information for analysis and so these articles were excluded
from the results. In the reviewed studies, patients were aged 12–81
years, with a mean age of 42.3±18.5 years. Of the 19 patients
reported, 10 were males and 8 were females. The ratio of renal
ectopic side was left:right, 9:8.
 | Table I.Previous reports of management of
upper urinary tract calculi in crossed fused renal ectopia. |
Table I.
Previous reports of management of
upper urinary tract calculi in crossed fused renal ectopia.
| Author, year | Patients | Mean age, years | Sex | Manifestation | Therapy history | Side | Stone location | Mean stone
burden | Surgical
technique | Number of
surgeriesa | Outcome | (Refs.) |
|---|
| Aminsharifi et
al, 2009 | 1 | 32 | M | Right flank pain | ESWL | Right | Pelvis | 25 mm | LNL | 1 | Total clearance | (12) |
| Kato et al,
2000 | 1 | 63 | F | Right flank pain,
microhematuria | None | Right | Proximal ureter | 12 mm | ESWL | 2 | Total clearance | (6) |
| Srivastava et
al, 2010 | 2 | 55 | 1 F, 1 M | – | None | – | Renal | 25 mm | 1 PCNL, 1
lap-assisted PCNL | 1 | Total
clearance | (10) |
| Maldonado-Alcaraz
et al, 2012 | 1 | 55 | M | Left renal colic,
microhematuria | None | Left | Pelvis | 20 mm | PCNL | 1 | Total
clearance | (8) |
| Ugurlu et
al, 2015 | 1 | 22 | F | – | ESWL | Left | Calyx | 85
mm2 | RIRS | 2 | Residual stone | (13) |
| Amin et al,
2009 | 1 | 25 | M | Right flank pain,
microhematuria | None | Right | Pelvicalyceal | Staghorn | Conservative | 0 | Residual stone | (20) |
| Taslim et
al, 2012 | 1 | 34 | M | Right flank
pain | None | Right | Pelvis | 14 mm | Conservative | 0 | Residual stone | (15) |
| Larre et al,
2007 | 1 | 40 | M | Left ureteral
colic | None | Left | Calyx | 18 mm | ESWL | 1 | Residual stone | (5) |
| Abdeldaeim et
al, 2011 | 1 | 12 | – | – | ESWL | Left | Pelvis | 169.7
mm2 | PCNL | 1 | Total
clearance | (9) |
| Gupta et al,
2009 | 4 | 30 | F:M, 1:1 | – | None | 3 Left 1 Right | 2 calyx 2
pelvis | 22 mm | PCNL | 1 | Total
clearance | (4) |
| Ghosh et al,
2008 | 1 | 81 | M | Left flank
pain | None | Left | Pelvis | – | PCN | 1 | Residual stone | (11) |
| Mishra et
al, 2013 | 1 | 68 | F | Abdominal pain | None | Right | Pelvicalyceal | Staghorn | PCNL, F-PCNL | 3 | Total
clearance | (7) |
| Resorlu et
al, 2015 | 1 | 28 | M | Left flank
pain | None | Left | Calyx | 15 mm | RIRS | 1 | Total
clearance | (14) |
| Present study | 2 | 51 | F | Right flank
pain | None | Right | Calyx, ureter | 20 mm | PCNL, URS | 1 | Total
clearance | – |
|
|
| 62 | F | Right flank pain,
urinary tract infection | None | Right | Ureter | 15 mm | RIRS | 1 | Total
clearance |
|
As demonstrated in Table
I, all patients suffered from different degrees of pain on the
affected side, with or without hematuria. Up to 89% of patients
presented with renal stones, whereas a small number of patients
presented with ureteral calculi. A total of 3 patients had a
history of failed ESWL. Patients received a variety of different
treatments including conservative management in (n=2), ESWL (n=2),
PCNL (n=11), laparoscope nephrolithotomy (n=1) and RIRS (n=3).
Final complete stone clearance was achieved in 14 patients (73.7%)
following single or multiple treatment sessions. No intraoperative
or postoperative complications, including blood transfusion,
uncontrolled hemorrhage and injury of surrounding viscera, were
reported.
Discussion
CFRE is an uncommon congenital anomaly in which an
ectopic kidney crosses the midline and merges with the orthotopic
kidney on the other side, with two ureters inserted into their
normal positions within the bladder trigone (1). CFRE has been reported to occur in 1 in
1,000–2,000 autopsies (2) and is
slightly more common in males (3:2) (3). Left-to-right crossover occurs more
frequently than right-to-left fusion (19). Depending on the extent of fusion,
location or rotation of the fused renal mass, the anomalous entity
may be categorized as a unilateral fused kidney with inferior or
superior ectopia, a sigmoid or S-shaped kidney, a lump kidney, an
L-shaped kidney or a disc kidney (3). The mechanism that causes the ectopic
renal anomaly remains to be elucidated; however, it has been
hypothesized that inappropriate development of the ureteral bud and
metanephric blastema in embryo may be one of the causes (19).
The majority of patients with CFRE present no
symptoms during their lifetime and the congenital anomaly is often
typically identified by chance during a routine physical
examination (1). Due to the abnormal
anatomic location, patients with CFRE are more susceptible to
urinary tract infections and calculus formation; as such, the
common manifestations include vague abdominal pain, hematuria,
pyuria and lower urinary tract symptoms (12). The majority of patients, as well as
the patients reviewed in the present study, present with varying
degrees of flank pain and microscopic hematuria (6–8,20) Various imaging studies, including
ultrasonography, intravenous urography, CT or magnetic resonance
imaging, may be used to estimate the crossed fused kidney (12). CT is widely utilized in preoperative
assessment as it may be utilized to precisely identify the
anatomical characteristics of the anomaly and the anatomical
relationship between the kidney and surrounding structures
(21).
The majority of asymptomatic individuals do not
require invasive treatment for a long time, until hydronephrosis or
renal function decrease is detected or ureter calculi impedes
urinary drainage (1). Techniques
used for management of upper urinary tract calculi in CRFE include
ESWL, PCNL, laparoscope, flexible nephroscopy or ureteroscopy
(6,8,10,12,13).
Urologists in many countries have abandoned open surgery due to the
rapid development of minimally invasive technology (12). Conservative management has been
reported in two previous articles (15,20);
however, this only relieves pain and the obstruction remains. It
was reported that 1 patient with a proximal ureter stone achieved
final stone-free status following two sessions of ESWL (6); however, ESWL was unsuccessful for
steinstrasse formation in another patient with a renal stone
(5). An additional 3 patients with
renal stones and a history of failed ESWL were identified in the
present study (9,12,13).
These results suggest that ESWL may not a suitable choice for CFRE
with upper urinary tract calculi.
PCNL as a minimally invasive method is considered
the gold standard for treating stones located in the kidney and
upper ureter, particularly large or complex stones, and has also
been used to manage renal anomalies of ectopia, fusion or
malrotated kidneys (4,18,22). A
study by Blackburne et al (23) reported their experience of PCNL in 37
patients with horseshoe kidneys. In their series, the final
stone-free rate was 81.1%. A total of 10 out of 11 patients (90.9%)
who were identified to have undergone PCNL in the present study
achieved stone clearance except one patient, whose therapeutic
outcome was unclear from the literature (11); unfortunately, the author did not
describe the subsequent treatment of the patient. The anatomical
deformity in patients with CFRE increases the risk of damaging the
surrounding visceral and renal aberrant vessel injuries during
surgery; therefore, special auxiliary methods, such as
laparoscopic-assisted approaches, may be necessary (12). A study by Srivastava et al
(10) reported a complex case with
musculoskeletal deformities resulting in a lack of access to the
collecting system by PCNL under image guidance as the bowel was
posterior to the crossed kidney. Therefore, a laparoscopic-assisted
PCNL was performed, which achieved complete clearance of stones in
a single session without any complications (10).
For large calculus or staghorn renal stones, PCNL
may not be as effective as previously believed. A recent study
reported that the more invasive the chosen procedure, the higher
the one-stage stone-free rate, the lower the need for ancillary
procedures and the lower the cost of hospitalization (24). A study by Mishra et al
(7) reported a 68-year-old female
with a staghorn stone in her right ectopic kidney, for whom a
residual stone remained following two PCNL treatments. A flexible
nephroscope was used to access the site and achieve final total
stone clearance in the third stage procedure. A study by
Aminsharifi et al (12)
reported another alternative treatment, laparoscopic
nephrolithotomy, which consists of two procedures: Laparoscopic
pyeloplasty and concomitant pyelolithotomy. However, this demanding
surgery requires considerable professional surgical techniques and
a long learning curve, as the existence of complex anatomical
malformations and fragile renal vasculature increases the risk of
injury to the aberrant renal vessels and makes it difficult to
define the anatomical structures of the ectopic kidney (12).
In recent years, flexible ureterorenoscopy has been
widely used to treat renal stones due to higher stone-free rates,
minimal invasion and fewer complications (25). RIRS is to be an alternative to PCNL
for the management of large renal calculi (≤3.5 cm) (26) and has been demonstrated as a safe and
effective measure for treating stone disease in patients with
horseshoe kidneys (27). A study by
Resorlu et al (14) reported
a 28-year-old male with calyceal stones in his ectopic kidney who
underwent RIRS with a good outcome. Another study reported a case
in which the location of the renal calyceal stone was not reached
following two RIRS procedures; however, the author did not discuss
the reasons for this failure (13).
In the present study, the left ureteral calculus near the ureteral
orifice in patient 1 was removed using ureteroscopy. However, due
to the seriously twisted ureter crossing the midline, RIRS was used
to remove calculi successfully in patient 2.
In conclusion, the results of the present study
suggest that, for the treatment of CFRE with upper urinary tract
calculi, conservative treatment and ESWL are unsatisfactory.
Ultrasonographic-guided, CT-guided or laparoscopic-assisted PCNL
are safe and effective methods for treating renal calculi in such
patients and laparoscopic nephrolithotomy is an alternative choice
for large or staghorn renal stones. Ureteroscopy is the first
choice for patients with ureter calculi, whereas RIRS should be
used when the stone is unreachable in the seriously twisted ectopic
ureter. RIRS may become the first line of treatment for renal
stones (≤3.5 cm) in crossed renal deformity due to its multiple
merits.
Acknowledgements
The present study was supported by the National
Nature Science Foundation of China (grant no. 81570627) and the Key
Program of the Science and Technology Department of Hunan Province
(project no. 2015JC3132).
Glossary
Abbreviations
Abbreviations:
|
CFRE
|
crossed fused renal ectopic
|
|
ESWL
|
extracorporeal shock wave
lithotripsy
|
|
F
|
female
|
|
Lap
|
laparoscopic
|
|
F-PCNL
|
flexible percutaneous
nephrolithotomy
|
|
LNL
|
laparoscopic nephrolithotomy
|
|
M
|
male
|
|
PCN
|
percutaneous nephrostomy
|
|
RIRS
|
retrograde intrarenal surgery
|
|
URS
|
ureteroscopy
|
References
|
1
|
Shapiro E, Bauer SB and Chow JS: Anomalies
of upper urinary tractWein AJ, Kavoussi LR, Novick AC, Partin AW
and Peters CA: Campbell Walsh Urology. 10th. Philadelphia: Elsevier
Saunders; pp. 3140–3145. 2012
|
|
2
|
Ajayi S, Mamven M, Tabari A, Ojji D and
Ibrahim A: Crossed fused renal ectopia presenting as recurrent
lower abdominal pain and urinary tract infection. Afr J Med Med
Sci. 42:193–196. 2013.PubMed/NCBI
|
|
3
|
Solanki S, Bhatnagar V, Gupta AK and Kumar
R: Crossed fused renal ectopia: Challenges in diagnosis and
management. J Indian Assoc Pediatr Surg. 18:7–10. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gupta NP, Mishra S, Seth A and Anand A:
Percutaneous nephrolithotomy in abnormal kidneys: single-center
experience. Urology. 73:7107142009. View Article : Google Scholar
|
|
5
|
Larré S, Carpentier X, Sèbe P, Tassart M,
Cussenot O and Traxer O: A report of unusual crossed fused renal
ectopia and minimal invasive management of calculi. Surg Radiol
Anat. 29:393–395. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kato M, Ioritani N, Aizawa M, Inaba Y,
Watanabe R and Orikasa S: Extracorporeal shock wave lithotripsy for
a ureteral stone in crossed fused renal ectopia. Int J Urol.
7:270–273. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mishra S, Ganesamoni R, Ganpule AP, Sabnis
RB and Desai MR: Supine percutaneous nephrolithotomy for bilateral
complete staghorn calculi in an L-shaped cross-fused renal ectopic
anomaly. Urology. 81:e3–e4. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Maldonado-Alcaraz E, Martinez-Vargas JA,
Moreno-Palacios J, Serrano-Brambila EA and Velázquez-Quintero S:
Percutaneous nephrolithotomy in crossed fused renal ectopia:
Superior calyceal access under fluoroscopic control. Arch Esp Urol.
65:582–585. 2012.(In English, Spanish). PubMed/NCBI
|
|
9
|
Abdeldaeim HM, Hamdy SA and Mokhless IA:
Percutaneous nephrolithotomy for the management of stones in
anomalous kidneys in children. J Pediatr Urol. 7:239–243. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Srivastava A, Gupta P, Chaturvedi S, Singh
P, Kapoor R, Dubey D and Kumar A: Percutaneous nephrolithotomy in
ectopically located kidneys and in patients with musculoskeletal
deformities. Urol Int. 85:37–41. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ghosh BC, DeSantis M, Kleyner Y and Zak Y:
Crossed fused renal ectopia with calculi. J Am Coll Surg.
206:7532008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Aminsharifi A, Niroomand R, Kroup M and
Hosseini MM: Laparoscopic nephrolithotomy in a patient with crossed
fused renal ectopia. Nat Rev Urol. 6:675–679. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ugurlu IM, Akman T, Binbay M, Tekinarslan
E, Yazici ö, Akbulut MF, Özgör F and Müslümanoğlu AY: Outcomes of
retrograde flexible ureteroscopy and laser lithotripsy for stone
disease in patients with anomalous kidneys. Urolithiasis. 43:77–82.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Resorlu M, Kabar M, Resorlu B, Doluoglu
OG, Kilinc MF and Karakan T: Retrograde intrarenal surgery in
cross-fused ectopic kidney. Urology. 85:e5–e6. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Taslim BB, Abdulwasiu BA, Olusegun S,
Oluwatoyin AC and Omolara MM: Crossed renal ectopia coexisting with
nephrolithiasis in a young Nigerian man. Arab J Nephrol Transplant.
5:107–110. 2012.PubMed/NCBI
|
|
16
|
Yan Z, Xie G, Yuan H and Cheng Y: Modular
flexible ureteroscopy and holmium laser lithotripsy for the
treatment of renal and proximal ureteral calculi: A single-surgeon
experience of 382 cases. Exp Ther Med. 10:1467–1471. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nadu A, Schatloff O, Morag R, Ramon J and
Winkler H: Laparoscopic surgery for renal stones: Is it indicated
in the modern endourology era? Int Braz J Urol. 35:9–18. 2009.17–8.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rana AM and Bhojwani JP: Percutaneous
nephrolithotomy in renal anomalies of fusion, ectopia, rotation,
hypoplasia, and pelvicalyceal aberration: Uniformity in
heterogeneity. J Endourol. 23:609–614. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bhojwani N, Hartman JB, Ahmed M, Morgan R
and Davidson JC: Management of ureteral obstruction in crossed
fused renal ectopia: A case report. Can Urol Assoc J. 8:E752–E744.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Amin MU, Khan S and Nafees M: Crossed
fused renal ectopia with staghorn calculus and gross
hydronephrosis. J Coll Physicians Surg Pak. 19:69–70.
2009.PubMed/NCBI
|
|
21
|
Singer A, Simmons MZ and Maldjian PD:
Spectrum of congenital renal anomalies presenting in adulthood.
Clin Imaging. 32:183–191. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Moosanejad N, Firouzian A, Hashemi SA,
Bahari M and Fazli M: Comparison of totally tubeless percutaneous
nephrolithotomy and standard percutaneous nephrolithotomy for
kidney stones: a randomized, clinical trial. Braz J Med Biol Res.
49:e48782016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Blackburne AT, Rivera ME, Gettman MT,
Patterson DE and Krambeck AE: Endoscopic Management of Urolithiasis
in the Horseshoe Kidney. Urology. 90:45–49. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Aminsharifi A, Irani D, Masoumi M,
Goshtasbi B, Aminsharifi A and Mohamadian R: The management of
large staghorn renal stones by percutaneous versus laparoscopic
versus open nephrolithotomy: A comparative analysis of clinical
efficacy and functional outcome. Urolithiasis. 44:551–557. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Elbir F, Başıbüyük İ, Topaktaş R, Kardaş
S, Tosun M, Tepeler A and Armağan A: Flexible ureterorenoscopy
results: Analysis of 279 cases. Turk J Urol. 41:113–118. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Palmero JL, Durán-Rivera AJ, Miralles J,
Pastor JC and Benedicto A: Comparative study for the efficacy and
safety of percutaneous nefhrolithotomy (PCNL) and retrograde
intrarenal surgery (RIRS) for the treatment of 2–3,5 cm kidney
stones. Arch Esp Urol. 69:67–72. 2016.(In English, Spanish).
PubMed/NCBI
|
|
27
|
Gokce MI, Tokatli Z, Suer E, Hajiyev P,
Akinci A and Esen B: Comparison of shock wave lithotripsy (SWL) and
retrograde intrarenal surgery (RIRS) for treatment of stone disease
in horseshoe kidney patients. Int Braz J Urol. 42:96–100. 2016.
View Article : Google Scholar : PubMed/NCBI
|