Introduction
Autoimmune thyroid disease (AITD), which includes
Graves' disease and Hashimoto's thyroiditis (HT), is characterized
by a variable degree of lymphocytic infiltration of the thyroid
gland and reactivity to self-thyroid antigens, due to a combination
of genetic and environmental factors (1,2). Cluster
of differentiation (CD)4+ T helper lymphocytes have a
key role in the pathogenesis of autoimmune diseases (3). CD4+ helper T cells are
subdivided into functionally distinct subsets, including T helper
(Th)1, Th2, Th17 and Treg cells, which predominantly produce
interferon (IFN)-γ as it has a critical role in the regulation of
the cellular-mediated immune response, and interleukin (IL)-4, IL-5
and IL-10, which are involved in the modulation of antibody
production and antigen-specific immunosuppression (4–6). A
relatively newly discovered subset of T helper cells, Th17, that
primarily produce IL-17 may be involved not only in the defense
against certain pathogens but also in driving inflammation and
autoimmunity (7). Another subset of
CD4+ T cells, Th3 lymphocytes, predominantly synthesize
tumor growth factor-β and are considered as regulatory cells
(8). In animal models of autoimmune
diseases, Th1 cells mediate tissue damage and disease progression;
whereas Th2 cells are associated with disease remission and
suppression of the immune response (9). While Th17 cells promote autoimmunity,
Treg cells can control autoimmunity and have a critical role in
autoimmune pathogenesis by maintaining self-tolerance and
controlling the activation of autoreactive CD4+ T
effector cells (10).
Hashimoto's disease is likely to exist at a higher
frequency than is diagnosed clinically, and its frequency appears
to be increasing (11). Positive
thyroglobulin antibodies (TgAb) and thyroid peroxidase antibodies
(TPOAb) are present in patients with HT, positive TPOAb are
identified in 12–26% of the general population and TgAb in ~14%
(12). High titers of thyroglobulin
antibodies (TgAb) and thyroid peroxidase antibodies (TPOAb) are
present in many patients with HT. Most patients with HT maintain a
euthyroid state throughout their lifetime without any medical
treatment, whereas others become hypothyroid. Approximately 20% of
patients exhibit signs and symptoms of mild hypothyroidism when
initially seen (13). Progression
from subclinical hypothyroidism to overt hypothyroidism typically
develops over a period of several years and occurs at a rate of ~5%
a year; the presence of either subclinical hypothyroidism or raised
thyroid antibodies indicates an increased risk of overt
hypothyroidism and the risk is greater when these factors occur
together (14). In Hashimoto's
disease, both Th1 and Th2 responses are found (15), although with different reciprocal
intensity in relationship with the clinical expression of the
disease process (16–18). However, recent studies have
demonstrated the existence of new subpopulations of T helper cells
that are also important in immunoregulation and host defense, like
Treg cells and Th17 cells (19–21). In
recent years, discoveries pertaining to this newly identified T
helper subset in humans and mice have accumulated with tremendous
speed (22–24). There is a negative reciprocal
regulatory relationship between Treg and Th17 lymphocytes; patients
with AITD exhibit an expansion of Th17 cells and these cells are
involved in the pathogenesis of AITD (25). Enhanced levels of Th17 cells and Th17
cytokines are found in patients with AITD, predominantly those with
HT (26). Another previous study
suggested that the proportion of activated cytotoxic T cells and
the titer of TgAb are independently involved in the disease
severity of HT (16). However, to
our knowledge, the frequency of T helper cells has not been
investigated in a large, community-based sample with different
stages of HT, and the possible impact on the health of the patient
remains unclear.
In this respect, the present study aimed to
characterize the alteration of T helper cells, particularly Th17
and Treg cells, in patients with different stages of HT and healthy
euthyroid controls in a large sample study. The aim being to
further to clarify the role of the imbalance between T helper cells
with the pathology or disease outcomes in HT and to analyze the
association between the imbalance with thyroid-specific
autoantibodies.
Subjects and methods
Subjects
This study was approved by the Ethics Committee of
People's Hospital of Xinjiang Uygur Autonomous Region and informed
consent was obtained from all participants prior to blood
collection. A total of 596 individuals, aged 18–80 years, were
recruited from two communities in Urumqi (Xinjiang, China) between
May and June 2013. We excluded participants who had missing lab
results (n=139) and those with hyperthyroidism (n=17). Finally, 389
patients with HT, who positive for anti-thyroid antibody including
TPOAb and/or TgAb (318 females and 71 males, aged 20–80 years), and
51 healthy euthyroid controls without thyroid antibodies (31
females and 20 males, aged 19–79 years) were enrolled. The overt
hypothyroidism HT group (34 patients) contained participants with
thyrotropin >4.2 mIU/l (normal, 0.27–4.2 mIU/l), and free
thyroxine (FT4) <11.5 pmol/l (normal, 11.5–22.7 pmol/l). The
subclinical hypothyroidism HT group (148 patients) contained
participants with thyrotropin >4.2 mIU/l, and FT4 within the
normal range. The euthyroid HT group (207 patients) contained
participants that had HT, as determined via TPOAb and/or TgAb
positivity, but were euthyroid.
Thyroid function and
autoantibodies
Venous blood samples were drawn after an overnight
fast of at least 8 h and were centrifuged for 5 min at 4°C at 2,136
× g after collection. Blood samples were collected and stored at
−80°C Thyroid parameters, serum TSH, levels of TgAb and TPOAb, and
serum concentrations of FT4 and free triiodothyronine (FT3) were
measured using an electro-chemiluminometric analyzer (E601; Roche
Diagnostics GmbH, Mannheim, Germany), with an interassay variance
of <10%. Serum levels of >35 IU/ml TPOAb and/or >116 IU/ml
TgAb were considered autoantibody positivity. The normal range of
TSH is 0.27–4.2 mIU/l, and the normal range of serum FT4 is
11.5–22.7 pmol/l.
Flow cytometry analyses
Peripheral blood mononuclear cells (PBMCs) were
prepared from heparinized venous blood by density-gradient
centrifugation within 8 h of blood collection. Stained cells were
analyzed using a flow cytometer (BD LSRII; BD Biosciences, Franklin
Lakes, NJ, USA). All reagents and fluorescent antibodies used in
the present study were produced by BD Biosciences. PBMC were
cultured in PMA + ionomysin + Brefeldin A (BFA) for 4 h at 37°C in
a humidified atmosphere containing 5% CO2. Following
incubation, the suspended cells were washed twice in cold PBS and
were resuspended in cold PBS. According to the supplier's protocol,
aliquots (200 µl) of PBMC were incubated with mouse anti-human CD3
(cat. no. 563798), CD4 (cat. no. 555346) and CD8 (cat. no. 557834)
FITC antibodies (all BD Biosciences) for 20 min at 48°C. The
working concentration of the antibodies was 1:100 dilution. Cells
were then fixed with Human FoxP3 Buffer A fixation reagent.
Following incubation for 10 min at room temperature in the dark,
cells were rinsed twice in 2 ml of appropriate concentration
reagent to cross membranes (Human FoxP3 Buffer C). Aliquots of
suspended cells in permeabilization buffer were incubated for 30
min at room temperature in the dark with IFN-y, IL-4, IL-17A and
Foxp3 antibodies, respectively. After rinsing in 2 ml of
permeabilization buffer, PBMCs were resuspended in 500 µl PBS and
analyzed using FCS express software, version 4 for the BD LSRII
flow cytometer.
Statistical analysis
Continuous variables are presented as means ±
standard deviation and median (interquartile range) for the
non-normally distributed variables. Student's t-test or
non-parametric Mann Whitney U test were used to determine whether
differences between means were significant. Mann-Whitney U test was
used to analyze the difference in the proportion of T helper cell
subsets between the examined groups. Spearman rank correlation
coefficient was also used to analyze the correlation between
anti-thyroid antibody and the proportion of peripheral Th cell
subsets. P<0.05 was considered to indicate a statistically
significant difference. Statistical analyses were performed using
SPSS v.16.0 (SPSS, Inc., Chicago, IL, USA).
Results
Clinical characteristics of
subjects
A total of 440 subjects were recruited into this
study, including 51 normal controls (47.59±12.38 years; 20 males
and 31 females) and 389 patients with HD (46.70±13.34 years; 71
males and 318 females). There was no significant difference among
the four groups regarding age (P=0.654) and FT3 levels (P=0.424).
Relevant clinical and biochemical data for all HT patients and
healthy controls are presented in Table
I. Subgroups of HT patients included 207 euthyroid HT patients
(46.05±13.51 years; 46 males and 161 females), 148 subclinical
hypothyroid HT patients (47.44±13.14 years; 23 males and 125
females), and 34 overt hypothyroid HT patients (47.50±13.30 years;
2 males and 32 females). Titers of TPOAb and TgAb were
significantly higher in HT patients with overt hypothyroidism than
in HT patients with subclinical hypothyroidism (P=0.035 and
P=0.001, respectively). Clinical and biochemical data of the
subgroups of HT patients are presented in Table II.
 | Table I.Clinical characteristics of HT
patients and healthy controls enrolled in the present study. |
Table I.
Clinical characteristics of HT
patients and healthy controls enrolled in the present study.
|
Characteristics | Control | Hashimoto's
thyroiditis |
|---|
| N
(male/female) | 51 (20/31) | 389 (71/318) |
| Mean age |
47.59±12.38 |
46.70±13.34 |
| TPOAb, IU/ml
(IQR) | 29.85
(27.35–31.73) | 89.13
(38.53–355.30)a |
| TgAb, IU/ml
(IQR) | 27.01
(19.9–30.55) | 214.9
(48.62–540.00)a |
| TSH, mIU/l
(IQR) | 2.06
(1.61–3.19) | 4.02
(2.40–5.98)a |
| FT4, pmol/l | 14.92±1.81 | 13.88±2.86 |
| FT3, pmol/l |
5.39±0.44 |
5.20±0.69 |
| Table II.Clinical characteristics of the
subgroups of Hashimoto's thyroiditis patients enrolled in the
present study. |
Table II.
Clinical characteristics of the
subgroups of Hashimoto's thyroiditis patients enrolled in the
present study.
|
Characteristics | HT-EU | HT-SH | HT-OH |
|---|
| N
(male/female) | 207 (46/161) | 148 (23/125) | 34 (2/32) |
| Mean age |
46.05±13.51 |
47.44±13.14 |
47.50±13.30 |
| TPOAb, IU/ml
(IQR) | 76.89
(38.84–257.70) | 95.43
(37.77–395.90) | 248.6
(66.10–537.90)a |
| TgAb, IU/ml
(IQR) | 192.3
(45.47–538.50) | 196.8
(40.02–515.40) | 440.7
(260.8–690.40)a |
| TSH, mIU/l
(IQR) | 2.51
(1.63–3.57) | 5.84
(4.85–7.74) | 15.94
(7.80–37.07)a |
| FT4, pmol/l | 15.29±1.90 |
14.42±2.06a |
9.10±2.38a |
| FT3, pmol/l |
5.39±0.58 |
5.26±0.60 | 4.57±0.88 |
Proportion of peripheral Th1 and Th2
cells
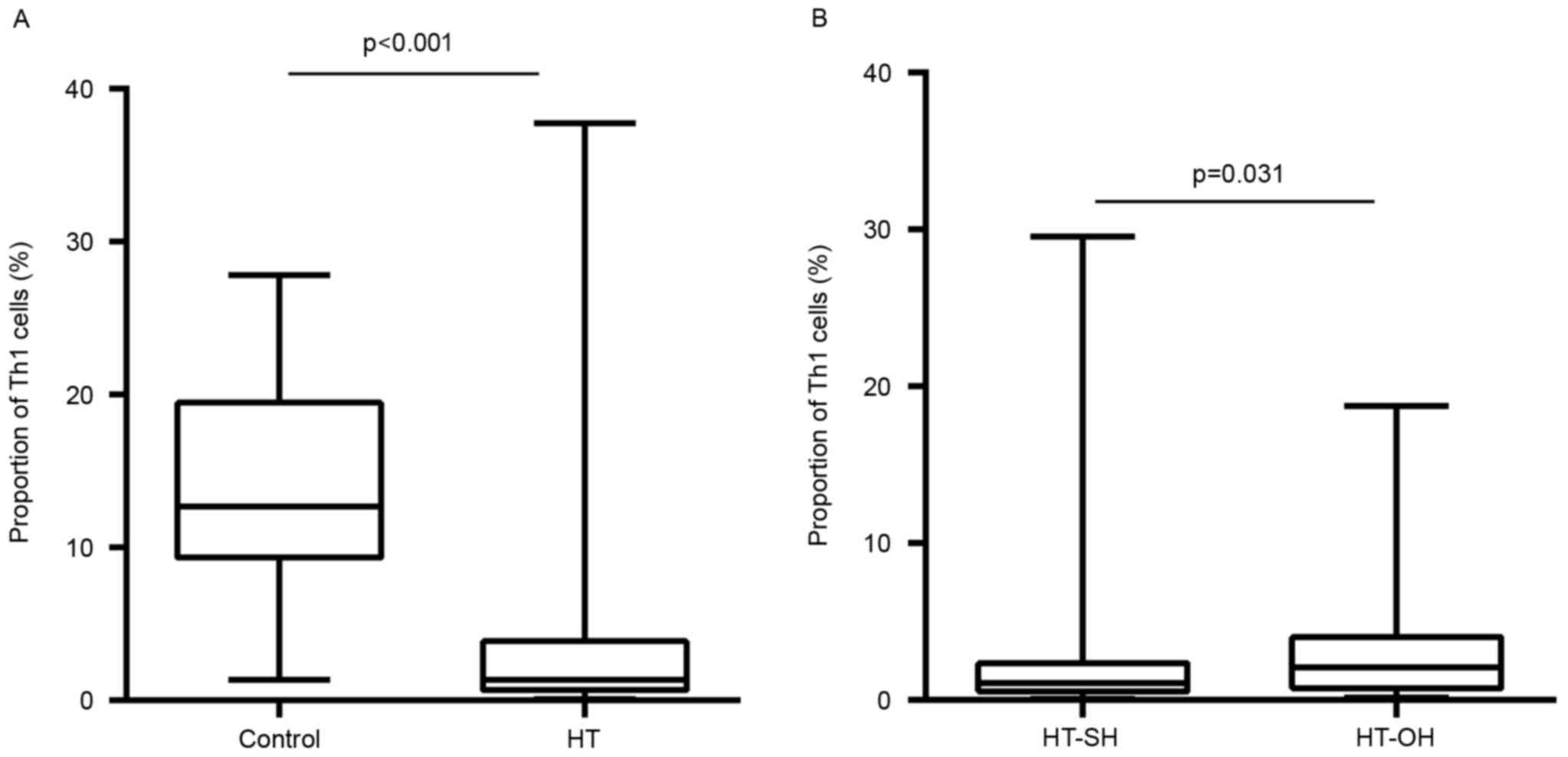
The proportions of peripheral Th1 cells in Th cells
in the HT patients were significantly lower than those healthy
euthyroid controls (3.9±6.0 vs. 14.2±6.3%; P<0.001; Fig. 1A). The Th1 proportions in patients
with overt hypothyroidism HT were significantly higher than those
in subclinical hypothyroidism HT patients (3.6±4.3 vs. 2.7±4.4%;
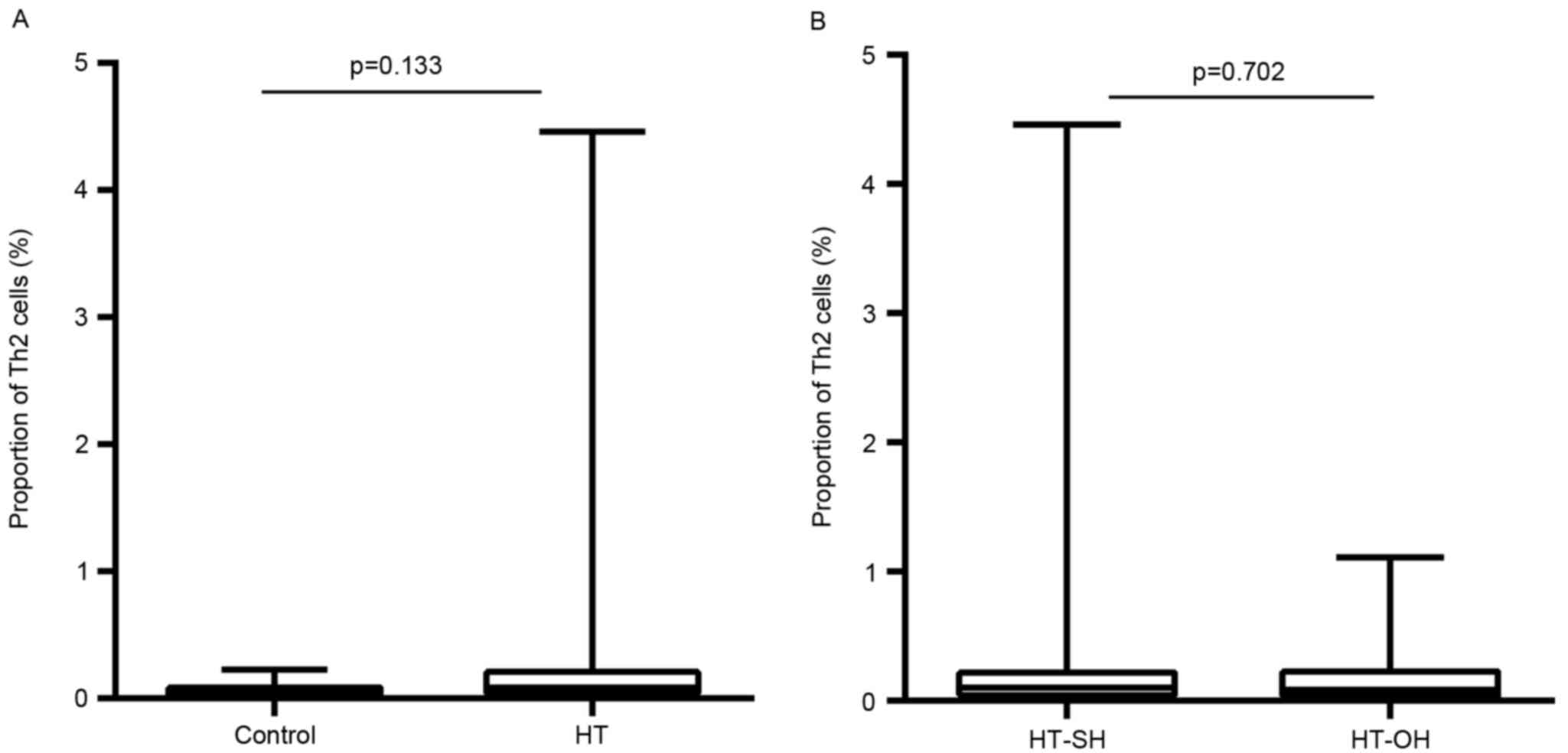
P=0.031; Fig. 1B). In contrast, the
proportions of Th2 cells in Th cells were significantly higher in
patients with HT than those with euthyroid controls (0.2±0.3 vs.
0.06±0.05%; P<0.001; Fig. 2A).
This proportion did not differ significantly between patients with
overt hypothyroidism HT and subclinical hypothyroidism HT (0.2±0.4
vs. 0.2±0.3%; P=0.702; Fig. 2B). The
Th1/Th2 ratio in HT patients was lower than that control subjects
(P<0.001). However, no apparent differences were found between
overt hypothyroid HT and subclinical hypothyroid HT patients
(P=0.146).
Proportion of peripheral Th17 and Treg
cells
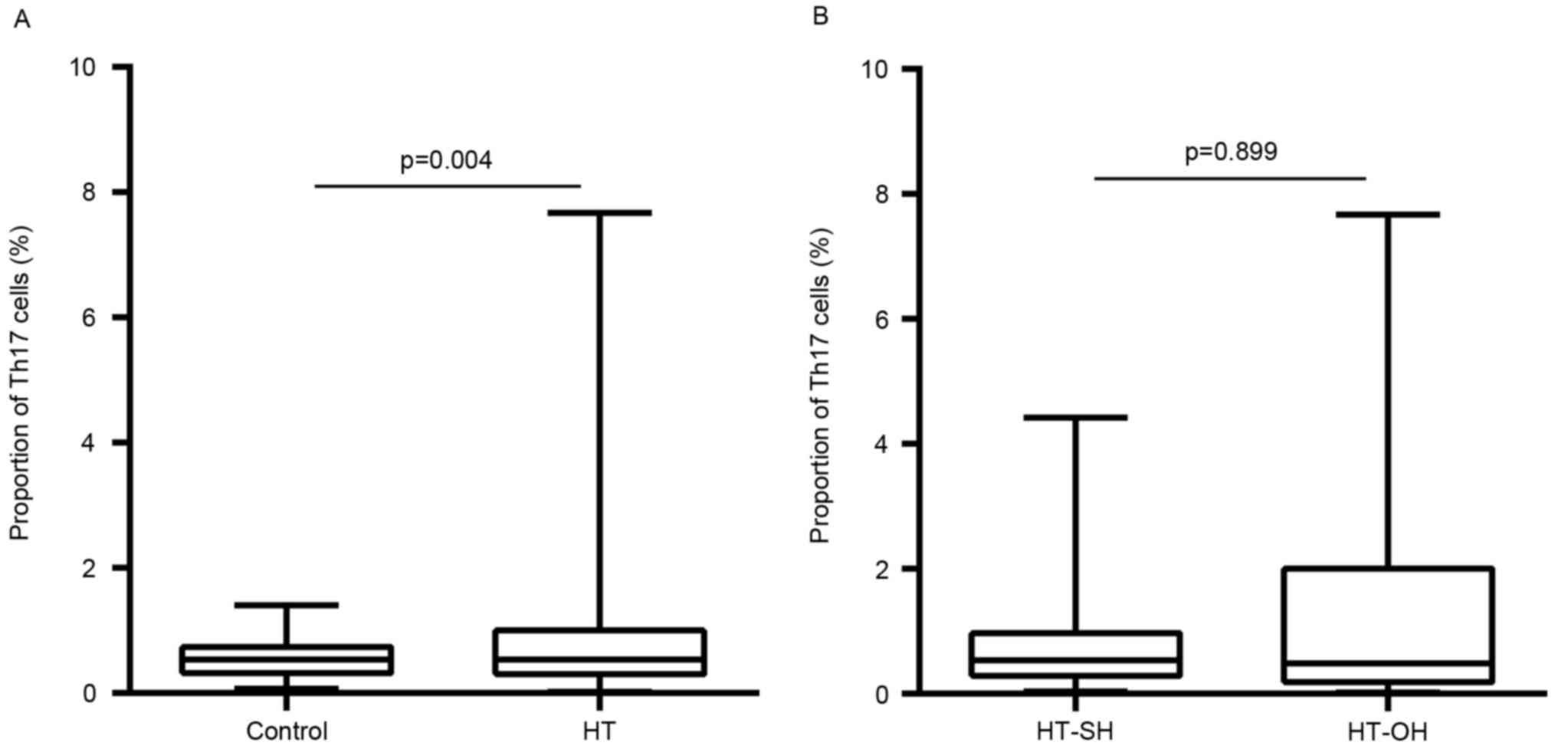
Peripheral proportions of Th17 and Treg cells are
presented in Figs. 3 and 4, respectively. The proportions of
peripheral Th17 cells were not significantly different between the
patients with HT and control subjects (0.9±0.9 vs. 0.6±0.3%;
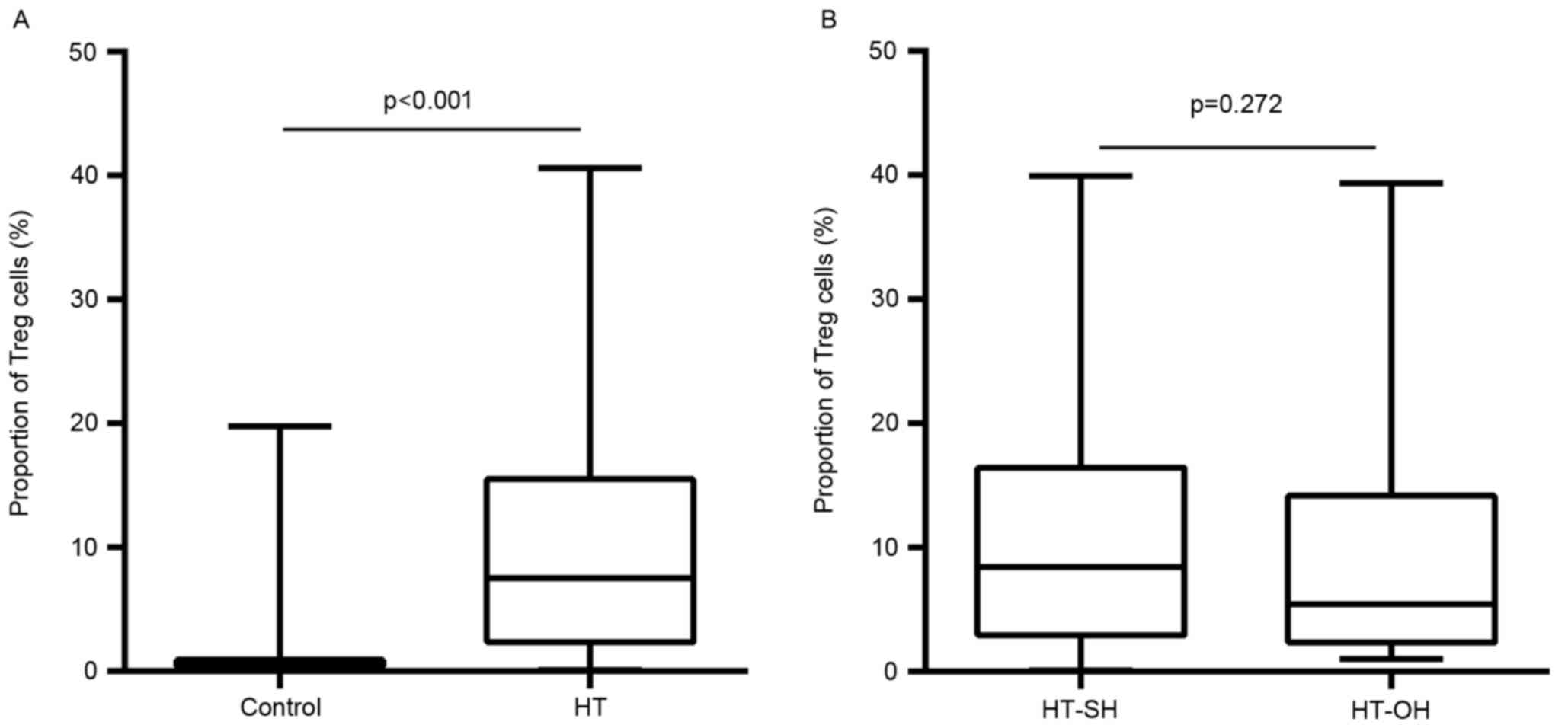
P=0.566; Fig. 3A). The proportions
of peripheral Treg cells in Th cells in HT patients were
significantly higher than those in control subjects (10.2±9.4 vs.
1.2±2.7%; P<0.001; Fig. 4A).
These proportions did not differ significantly between patients
with overt hypothyroidism HT (Th17, 0.8±0.9%; Treg, 11.0±9.4%) and
subclinical hypothyroidism HT (Th17, 1.2±1.6% P=0.899; Treg,
9.5±10.1% P=0.272; Figs. 3B and
4B). The Th17/Treg ratio in HT
patients was lower than that control subjects (P<0.001).
However, no apparent differences were found between overt and
subclinical hypothyroid HT patients (P=0.053).
Titers of thyroid-specific
autoantibodies
Given the findings that patients with HT had higher
serum TPOAb and TgAb levels and a lower proportion of Th1 cells, we
evaluated the correlation using Spearman rank correlation analysis.
A negative correlation (r=−0.134, P=0.008 and r=−0.114, P=0.024,
respectively) was detected between TPOAb levels and Th1 cells, and
TgAb levels and Th1 cells in patients with HT. Further analysis
also revealed a negative correlation between Th1/Th2 ratio and
Th17/Treg ratio with the two TPOAb and TgAb autoantibodies
(r=−0.192, P<0.001; r=−0.126, P=0.008; r=−0.165, P=0.001;
r=−0.211, P<0.001, respectively) (data not shown).
Discussion
The present study demonstrated that the proportions
of peripheral Th1 cells were lower in patients with HT than in
euthyroid control subjects, and a higher proportion of Th2 and Treg
cells were found in the peripheral blood of patients with HT.
Furthermore, the proportions of peripheral Th1 cells, but not Th17,
Th2 and Treg, were elevated in HT patients with overt
hypothyroidism when compared with HT patients with subclinical
hypothyroidism. These data suggest that HT patients with a higher
proportion of Th1 cells are more inclined to experience rapid
destruction of thyroid follicular cells, resulting in
hypothyroidism.
HT is an autoimmune disorder, characterized by the
formation of tertiary lymphoid follicles within the thyroid
(containing T cells, predominantly Th1, and B cells), in which the
T-lymphocytes have an important role, with the diffuse process of
thyroid follicules destruction generating hypofunction, and the
presence of high titers of antiTPO and/or antiTg antibodies in the
serum. The incidence of HT is 15–20 times more likely in women than
in men (27). It is essentially the
same process that the thyroid lymphocytic infiltrates when either
of the thyroid autoantibodies are detected in serum, and this
phenomenon presents in the ranges from focal thyroiditis to the
lymphadenoid goitre of HT (1).
A prevalent Th1 cytokine profile is typically found
in patients with organ-specific autoimmune disease, while a
prevalent Th2 profile is usually associated with systemic
autoimmunity (28). Our results
showed a normal to low percentage of Th1 cells and an increased
percentage of Th2 cells in all peripheral blood samples from
patients with HT. This result confirmed the prevalent Th1
polarization in circulation. As reported previously, Th1 and Th2
cells are the extreme polarized forms of CD4+ Th cells,
when it becomes dangerous, Th1 can be shifted to a less polarized
profile Th0, or even Th2, via a process called immune deviation
(29). Predominance of the immune
response of Th1 accelerates the apoptosis of thyrocytes (30), which mediated by Fas and TRAIL,
leading to HT (2,31). Whereas the predominance of a Th2
immune response induces antigen-specific B cells to produce
antithyroid antibodies, just as stimulatory antiTSH receptor
antibodies are responsible for Graves' disease and the blocking
antiTSH receptor antibodies are responsible for atrophic
thyroiditis; thus, the balance of Th1-Th2 directly affects the
clinical expression of thyroid autoimmunity (32). However, in the HT patients with overt
hypothyroidism investigated in the present study, a significant
increase in the proportion of Th1 cells was noted when compared
with that of subclinical hypothyroid HT patients. Hypothyroidism is
not only the result of thyrocyte destruction, but also of thyroid
function impairment in HT, which has been proposed to be induced by
Th1 cytokines (29). Hence, we
propose that Th1 cells may be present in different stages in
patients with HT and depend on the severity of disease.
Increasing evidence supports the hypothesis that
Th17 and Treg cells participate in the process of HT (26,33).
Th17 lymphocytes are critical for the pathogenesis of different
inflammatory and autoimmune conditions (7). Tregs are a subset of CD4+ T
cells that suppress the excessive immune response, protect against
tissue injury and prevent autoimmune diseases (10). The opposite role of these two kinds
of CD4+ T cells can be seen in the development of
autoimmune diseases, while Th17 cells promote autoimmunity, Treg
cells control it (10,34). A recent study reported the decreased
frequency and/or function of Treg cells in human autoimmune
diseases (35). However, another
study reported that, in autoimmune thyroiditis, Treg cell frequency
and/or function is enhanced when compared with normal donors
(36), and indicated that patients
with HT exhibit enhanced levels of Th17 cells in their peripheral
blood. In the present study, we observed an enhanced frequency of
peripheral Th17 cells in patients with HT than in control subjects;
however, the proportions of peripheral Treg cells in patients with
HT were significantly higher than in control subjects. This
suggests a compensatory attempt to overcome or reduce the
autoimmunity by accelerating Treg cell activity (37). This is a notable finding as it has
previously been hypothesized that the opposite roles of Th17, Treg
cells and alteration of Th17/Treg may participate in the
pathogenesis of HT (10,34). Although the Th17/Treg ratio in
patients with HT was lower than in control subjects, no significant
differences in the Th17/Treg ratio were found between our subgroups
of overt hypothyroid HT patients and subclinical hypothyroid HT
patients. These data suggest that the suppressive nature of Treg
function is most likely a defect in autoimmune disease and patients
are not able to reverse the clinical course of inflammation.
Predominance of the Th1 phenotype can induce
cell-mediated apoptosis in thyrocytes with subsequent HT (29). Eventually, thyroid atrophy and
myxedema may occur (38). Patients
with AITD due to lymphocytic infiltration of the thyroid have a
high incidence of TgAb and TPOAb in their serum (1). Bona et al (39) observed a direct correlation between
anti-TPO antibody levels and the resistance of T cells to apoptosis
in untreated patients with HT. A significant correlation between
serum TPOAb/TgAb and Th1 cells supports the contention that
antibodies are involved in the promotion of thyroid
antibody-elicited immune responses. Antibody-mediated cytotoxicity
leads to more damage to thyroid tissue in comparison to T cells and
cytokine-mediated apoptosis (40).
There have been various studies addressing the issue
of Th cells in HT patients; however, to our knowledge, the majority
have been restricted by the amount of samples and animal
experiments. As a results, the pathogenesis and progression of HT
remains to be fully elucidated. The present study demonstrated
that, in a large community-based sample, that an enhanced Th1, but
not Th2 or Th17, immune response by Treg depletion is sufficient
for the development of hypothyroidism in patients with HT. This
finding appears to reflect a higher sustainability of the Th1
immune response. Although we do not have a commendable explanation
for our partially contradictory results, it is feasible that the
apparent discrepancies between previous studies (32,35) and
our work may be due, at least in part, to the larger sample size of
this study, different genetic background of the individuals
studied, the presence or absence of HT, and the stage of the
hypothyroidism in patients. Furthermore, only the peripheral T-cell
subsets, not the intrathyroidal T cells, were studied and we did
not exclude participants with other autoimmune conditions. In any
case, we propose that performing a longitudinal study of Th cells
in HT patients with or without hypothyroidism would be beneficial,
predominantly because it has been suggested that a Th1-Th2 shift
and Th17/Treg imbalance may occur during the evolution of HT.
In conclusion, our data suggest that patients with
HT exhibit enhanced differentiation of Th1 lymphocytes, and that
these cells may participate in the development of hypofunction in
HT patients. Another important finding of the study was the reduced
numerical proportion of Treg cells in patients with HT, indicating
a compensatory attempt to overcome or reduce the autoimmunity, but
this was not related to the severity of hypothyroidism in HT
patients. This observation of thyroid autoimmunity from our study
reflects the complexity of immune-thyroid interactions, clarifying
the pathogenic roles of immune interaction. These data may support
improved clinical management and earlier intervention in the
progression of HT.
Acknowledgements
This study was supported by the Natural Science
Foundation of Xinjiang Uygur Autonomous Region (grant no.
2013211A105) and the Fund for Less Developed Regions from the
National Natural Science Foundation of China (grant no.
81260127).
References
|
1
|
Weetman AP: Autoimmune thyroid disease.
Autoimmunity. 37:337–340. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Stassi G and De Maria R: Autoimmune
thyroid disease: New models of cell death in autoimmunity. Nat Rev
Immunol. 2:198–204. 2002. View
Article : Google Scholar
|
|
3
|
Druet P, Sheela R and Pelletier L: Th1 and
Th2 cells in autoimmunity. Chem Immunol. 63:138–170. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Salgame P, Abrams JS, Clayberger C,
Goldstein H, Convit J, Modlin RL and Bloom BR: Differing lymphokine
profiles of functional subset of human CD4 and CD8 T cell clones.
Science. 254:279–282. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Carter LL and Dutton RW: Type 1 and Type
2: A fundamental dichotomy for a T-cell subsets. Curr Opin Immunol.
8:336–342. 1991. View Article : Google Scholar
|
|
6
|
Mosmann TR and Sad S: The expanding
universe of T-cell subsets: Th1, Th2 and more. Immunol Today.
17:138–146. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Torchinsky MB and Blander JM: T helper 17
cells: Discovery, function, and physiological trigger. Cell Mol
Life Sci. 67:1407–1421. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shevach EM: Suppressor T cells: Rebirth,
function and homeostasis. Curr Biol. 10:R572–R575. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Liblau RL, Singer SM and McDevitt HO: Th1
and Th2 CD4+ T cells in the pathogenesis of organ-specific
autoimmune disease. Immunol Today. 16:34–38. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang S, Xu H, Wang Y, Ma J, Mao C, Shao Q,
Ma B, Xu W and Yang S: Regulatory T cells induced by rAAV carrying
the forkhead box P3 gene prevent autoimmune thyroiditis in mice.
Int J Mol Med. 18:1193–1199. 2006.PubMed/NCBI
|
|
11
|
Staii A, Mirocha S, Todorova-Koteva K,
Glinberg S and Jaume JC: Hashimoto thyroiditis is more frequent
than expected when diagnosed by cytology which uncovers a
pre-clinical state. Thyroid Res. 3:112010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
McLeod DS and Cooper DS: The incidence and
prevalence of thyroid autoimmunity. Endocrine. 42:252–265. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gordin A, Saarinen P, Pelkonen A and
Lamberg BA: Serum thyroglobulin and the response to thyrotropin
releasing hormone in symptomless autoimmune thyroiditis and in
borderline and overt hypothyroidism. Acta Endocrinol (Copenh).
75:274–285. 1974.PubMed/NCBI
|
|
14
|
Weetman AP: Hypothyroidism: Screening and
subclinical disease. BMJ. 314:1175–1178. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nanba T, Watanabe M, Inoue N and Iwatani
Y: Increases of the Th1/Th2 cell ratio in severe hashimoto's
disease and in the proportion of Th17 cells in intractable graves'
disease. Thyroid. 19:495–501. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Watanabe M, Yamamoto N, Maruoka H, Tamai
H, Matsuzuka F, Miyauchi A and Iwatani Y: Independent involvement
of CD8+CD25+ cells and thyroid autoantibodies in disease severity
of Hashimoto's disease. Thyroid. 12:801–808. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ito C, Watanabe M, Okuda N, Watanabe C and
Iwatani Y: Association between the severity of Hashimoto's disease
and the functional +874A/T polymorphism in the interferon-gamma
gene. Endocr J. 53:473–478. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Nanba T, Watanabe M, Akamizu T and Iwatani
Y: The 590CC genotype in the IL4 gene as a strong predictive factor
for the development of hypothyroidism in Hashimoto disease. Clin
Chem. 54:621–623. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Alunno A, Manetti M, Caterbi S,
Ibba-Manneschi L, Bistoni O, Bartoloni E, Valentini V, Terenzi R
and Gerli R: Altered immunoregulation in rheumatoid arthritis: The
role of regulatory T cells and proinflammatory Th17 Cells and
therapeutic implications. Mediators Inflamm. 2015:7517932015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Figueiredo AS and Schumacher A: The T
helper type 17/regulatory T cell paradigm in pregnancy. Immunology.
148:13–21. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pyzik A, Grywalska E, Matyjaszek-Matuszek
B and Roliński J: Immune disorders in hashimoto's thyroiditis: What
do we know so far? J Immunol Res 2015. 9791672015.
|
|
22
|
Safdari V, Alijani E, Nemati M and
Jafarzadeh A: Imbalances in T cell-related transcription factors
among patients with hashimoto's thyroiditis. Sultan Qaboos Univ Med
J. 17:e174–e180. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hirahara K and Nakayama T: CD4+ T-cell
subsets in inflammatory diseases: Beyond the Th1/Th2 paradigm. Int
Immunol. 28:163–171. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sehrawat S and Rouse BT: Interplay of
regulatory T cell and Th17 cells during Infectious diseases in
humans and animals. Front Immunol. 8:3412017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Marazuela M, García-López MA,
Figueroa-Vega N, de la Fuente H, Alvarado-Sánchez B,
Monsiváis-Urenda A, Sánchez-Madrid F and González-Amaro R:
Regulatory T cells in human autoimmune thyroid disease. J Clin
Endocrinol Metab. 91:3639–3646. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Figueroa-Vega N, Alfonso-Pérez M,
Benedicto I, Sánchez-Madrid F, González-Amaro R and Marazuela M:
Increased circulating pro-inflammatory cytokines and Th17
lymphocytes in hashimoto's thyroiditis. J Clin Endocrinol Metab.
95:953–962. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cipolla C, Sandonato L, Graceffa G,
Fricano S, Torcivia A, Vieni S, Latteri S and Latteri MA: Hashimoto
thyroiditis coexistent with papillary thyroid carcinoma. Am Surg.
71:874–878. 2005.PubMed/NCBI
|
|
28
|
Romagnani S: Regulation of T cell
response. Clin Exp Allergy. 36:1357–1366. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lichiardopol C and Moţa M: The thyroid and
autoimmunity. Rom J Intern Med. 47:207–215. 2009.PubMed/NCBI
|
|
30
|
Corona G, Biagini C, Rotondi M, Bonamano
A, Cremonini N, Petrone L, Conforti B, Forti G and Serio M:
Correlation between, clinical, biochemical, color Doppler
ultrasound thyroid parameters, and CXCL-10 in autoimmune thyroid
diseases. Endocr J. 55:345–350. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Fountoulakis S, Vartholomatos G, Kolaitis
N, Frillingos S, Philippou G and Tsatsoulis A: Differential
expression of Fas system apoptotic molecules in peripheral
lymphocytes from patients with Graves' disease and Hashimoto's
thyroiditis. Eur J Endocrinol. 158:853–859. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Tsatsoulis A: The role of stress in the
clinical expression of thyroid autoimmunity. Ann N Y Acad Sci.
1088:382–395. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Glick AB, Wodzinski A, Fu P, Levine AD and
Wald DN: Impairment of regulatory T-cell function in autoimmune
thyroid disease. Thyroid. 23:871–878. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bettelli E, Carrire Y, Gao W, Korn T,
Strom TB, Oukka M, Weiner HL and Kuchroo VK: Reciprocal
developmental pathways for the generation of pathogenic effector
Th17 and regulatory T cells. Nature. 441:235–238. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Liu Y, Tang X, Tian J, Zhu C, Peng H, Rui
K, Wang Y, Mao C, Ma J, Lu L, et al: Th17/Treg cells imbalance and
GITRL profile in patients with Hashimoto's thyroiditis. Int J Mol
Sci. 15:21674–21686. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Brusko TM, Putnam AL and Bluestone JA:
Human regulatory T cells: Role in autoimmune disease and
therapeutic opportunities. Immunol Rev. 223:371–390. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kahaly GJ, Shimony O, Gellman YN, Lytton
SD, Eshkar-Sebban L, Rosenblum N, Refaeli E, Kassem S, Ilany J and
Naor D: Regulatory T-cells in Graves' orbitopathy: Baseline
findings and immunomodulation by anti-T lymphocyte globulin. J Clin
Endocrinol Metab. 96:422–429. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Buchanan WW and Harden RM: Primary
hypothyroidism and Hashimoto's thyroiditis A continuous spectrum.
Arch Intern Med. 115:411–417. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Bona G, Defranco S, Chiocchetti A,
Indelicato M, Biava A, Difranco D, Dianzani I, Ramenghi U, Corrias
A, Weber G, et al: Defective function of Fas in T cells from
paediatric patients with autoimmune thyroid diseases. Clin Exp
Immunol. 133:430–437. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chiovato L, Bassi P, Santini F, Mammoli C,
Lapi P, Carayon P and Pinchera A: Antibodies producing
complement-mediated thyroid cytotoxicity in patients with atrophic
or goitrous autoimmune thyroiditis. J Clil Endocrinol Metab.
77:1700–1705. 1993. View Article : Google Scholar
|