Introduction
Sepsis is a generalized systemic inflammatory
disease with a high prevalence. There are approximately 18 million
people on average suffering from sepsis per year around the world,
and this number is still rising each year (1–3). Sepsis
is one of the leading causes of death in the intensive care unit,
and there are nearly 14,000 people worldwide die of secondary
diseases on average every day (4,5). In
recent years, although great strides have been made in the
anti-infective treatment, the mortality rate of sepsis patients
still ranges from 25 to 60% (6,7). Sepsis
treatment is expensive, and the use of medical resources is also
very serious (7,8). Therefore, strengthening the early
diagnosis, treatment and prognosis of patients with sepsis plays a
very significant role.
Recently, studies have shown that changes in
C-reactive protein (CRP) and procalcitonin (PCT) levels can prompt
the severity of sepsis, and CRP and PCT tests have advantages of
short time and high sensitivity, which are of great significance
for the diagnosis and differential diagnosis of early infection
(9,10). CRP is a non-specific and
inflammation-related protein that is produced in the liver and
regulated by plasma interleukin-6 (IL-6). When infection or body
damage occurs, the concentration of CRP will be greatly altered
(11). PCT is a glycoprotein with no
hormonal activity, whose sensitivity to viral and bacterial
infections is high; for example, sepsis can lead to a large change
in its level (12). Therefore,
changes in CRP and PCT levels in patients in the intensive care
unit were detected in this study, so as to explore their predictive
and prognostic effects on sepsis.
Patients and methods
Study objects
A total of 203 patients aged 21–76 years admitted to
the Intensive Care Unit of Qilu Hospital of Shandong University in
Dongying (Dongying, China) from May 2014 to May 2016 were selected
and divided into the sepsis (n=60) and the non-sepsis group
(n=143). In the sepsis group, there were 21 mild-to-moderate cases,
including 12 males and 9 females with an average age of 43.2±21.3
years, 19 severe cases, including 11 males and 8 females with an
average age of 58.5±19.6 years, and 20 cases with septic shock,
including 12 males and 8 females with an average age of 68.1±23.5
years. In the non-sepsis group, there were 143 cases with
colorectal cancer, including 82 males and 61 females with an
average age of 35.1±1.6 years. The diagnostic criteria were in line
with the International Guidelines for Management of Severe Sepsis
and Septic Shock (Version 2016). The study was approved by the
Ethics Committee of Qilu Hospital of Shandong University in
Dongying and informed consents were signed by the patients and/or
guardians.
Detection methods
Venous blood (3 ml × 2) was drawn from all the
subjects the morning after admission, placed into a vacuum tube
containing anticoagulant and then sent to the Laboratory Medicine
of Qilu Hospital of Shandong University in Dongying for the
detection of CRP and PCT expression levels. Fasting venous blood
samples of patients in the control group were extracted for
detection during the physical examination. CRP level was measured
by immunoturbidimetry, and kits were provided by Beijing Strong
Biotechnologies, Inc. (Beijing, China). The detection was performed
by using the Beckman Coulter AU5800 automatic biochemical analyzer
(Beckman Coulter, Inc., Brea, CA, USA). The standard and accusative
reagents were provided by the manufacturer, and experiments were
conducted in strict accordance with the kit instructions. PCT level
was tested with the QMT8000 Immunoquantitative Analyzer (Getein
Biotech, Inc., Nanjing, Cina), and kits were also supplied by the
company.
Observation indexes
Differences in CRP and PCT levels in patients at
admission between the two groups were compared; differences in CRP
and PCT levels in patients who died of sepsis and those surviving
from the disease at 1 and 2 weeks after admission and those at
admission were analyzed; predictive effects of CRP and PCT levels
on sepsis in the intensive care unit patients and their influence
on the prognosis of patients with sepsis were analyzed. The latest
CRP and PCT levels detected before death were taken as the standard
for the dead patients with the survival time less than 1 or 2
weeks, and the data of patients at 1 or 2 weeks after admission
were included, respectively.
Statistical analysis
Statistical analysis was conducted using SPSS 19.0
software [AsiaAnalytics (formerly SPSS China), Shanghai, China].
Sex and treatment effects were compared by the χ2 test;
measurement data were expressed as mean ± SD; the non-parametric
Kolmogorov-Smirnov (K-S) test was selected to compare the data
between the two groups, and comparisons among various groups were
conducted by using the analysis of variance. The receiver operating
characteristic (ROC) curves of CRP and PCT of subjects were drawn;
logistic regression analysis was used to analyze the correlation of
CRP and PCT with the poor prognosis of patients. Univariate Cox
regression analysis was used to analyze the related factors
affecting the prognosis of patients with sepsis. A P<0.05 was
considered to indicate a statistically significant difference.
Results
Clinical data
There were a total of 203 patients in the intensive
care unit. In the sepsis group, there were 60 patients with
colorectal cancer, including 35 males and 25 females with an
average age of 56.6±21.5 years; in the non-sepsis group, there were
143 patients with colorectal cancer, including 82 males and 61
females with an average age of 35.1±11.6 years. There was a
difference in age between the two groups (P<0.05), but no
differences in other basic data such as sex were found (P>0.05)
(Tables I–III).
 | Table I.Comparisons of basic data between the
two groups of patients. |
Table I.
Comparisons of basic data between the
two groups of patients.
| Basic data | Sepsis group | Non-sepsis group | P-value |
|---|
| No. of cases (n) | 60 | 143 |
|
| Sex
(male/female) | 35/25 | 82/61 | 0.579 |
| Age (years) | 56.6±21.5 | 40.1±11.6 | 0.036 |
| Smoking history, n
(%) |
|
| 0.556 |
| Yes | 17 (28.33) | 33 (23.08) |
|
| No | 43 (71.67) | 110 (76.92) |
|
| Place of residence, n
(%) |
|
| 0.372 |
| City | 41 (68.33) | 82 (57.34) |
|
|
Countryside | 19 (31.67) | 61 (42.66) |
|
| Table III.Prognosis of patients with sepsis. |
Table III.
Prognosis of patients with sepsis.
| Item | Mild sepsis | Severe sepsis | Septic shock | P-value |
|---|
| No. of cases (n) | 21 | 19 | 20 |
|
| Survival, n (%) | 19 (90.48) | 10 (52.63) | 5 (25.00) | 0.029 |
| Death, n (%) | 2 (9.52) | 9 (47.37) | 15 (75.00) |
|
Prognosis of patients with sepsis
As of May 2016, there were 26 death cases in the
sepsis group, with a mortality rate of 43.33%. Septic shock
occurred in most of them, with a mortality rate as high as 75%,
which was significantly higher than those of patients with mild and
severe sepsis (P<0.05). There was no case of death in the
non-sepsis group, and systemic inflammatory responses in patients
were controlled and did not develop into sepsis (Table III).
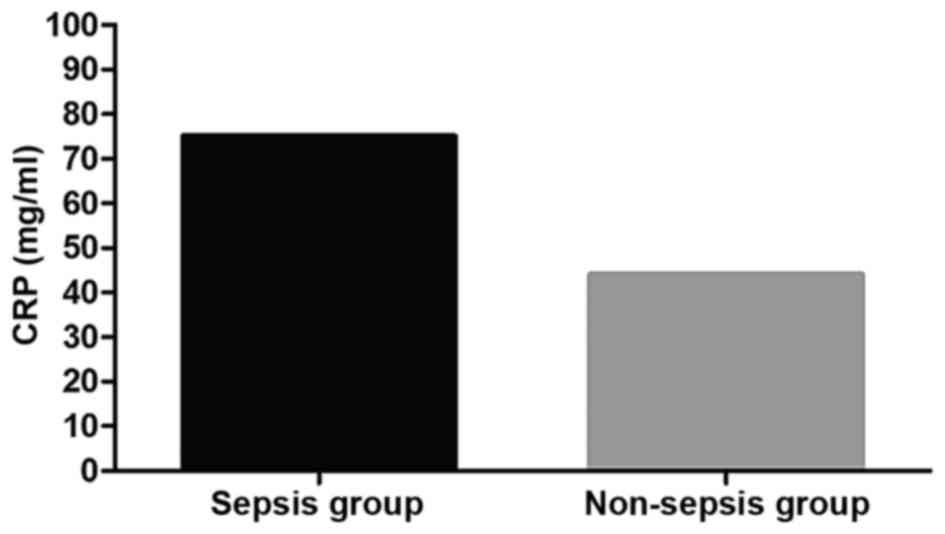
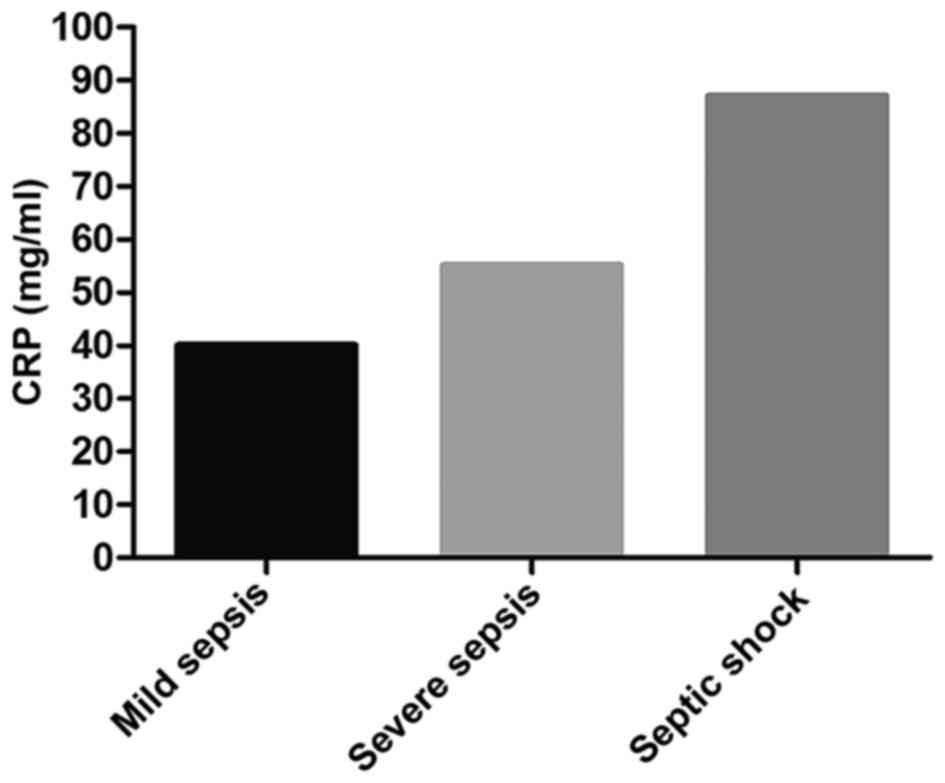
Detection results of CRP
At admission, the average level of CRP in the sepsis
was obviously higher than that in the non-sepsis group (P<0.05).
In the sepsis group, the average CRP level in patients with septic
shock was higher than that in patients with severe sepsis and mild
sepsis (P<0.05); the average CRP level in patients with severe
sepsis was higher than that in patients with mild sepsis
(P<0.05). Comparisons of CRP levels in patients who died of
sepsis at 1 and 2 weeks after admission and those at admission
showed that there were no changes (P>0.05); CRP level in
patients surviving sepsis at 1 week after admission was clearly
decreased compared with that at admission (P<0.05); CRP level in
those at 2 weeks after admission was significantly reduced compared
with that at admission (P<0.05). The average level of CRP of
patients who died of sepsis was higher than that of those who
survived (P<0.05) (Figs. 1 and
2 and Table IV).
| Table IV.Comparisons of the detection results
of CRP between patients surviving sepsis and those who died
(mg/ml). |
Table IV.
Comparisons of the detection results
of CRP between patients surviving sepsis and those who died
(mg/ml).
| Time | Patient surviving
sepsis | Patient died of
sepsis | t-value | P-value |
|---|
| No. of cases (n) | 34 | 26 |
|
|
| At admission | 52.2±11.3 | 64.5±10.9 | 2.365 | 0.047 |
| 1 week after
admission | 42.1±8.4a |
68.2±10.4c | 2.933 | 0.036 |
| 2 weeks after
admission | 35.2±7.7b | 69.5±9.4d | 3.114 | 0.027 |
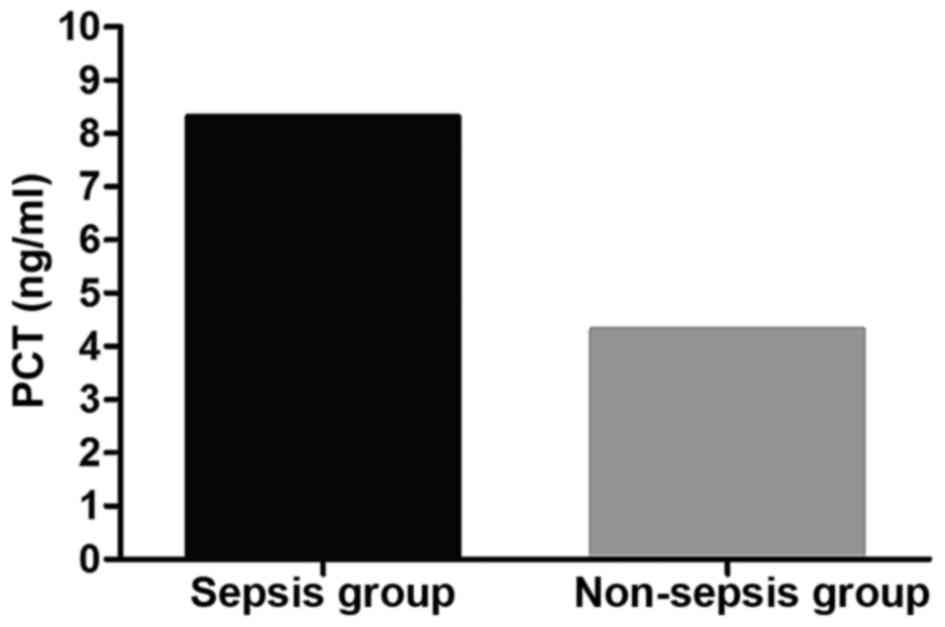
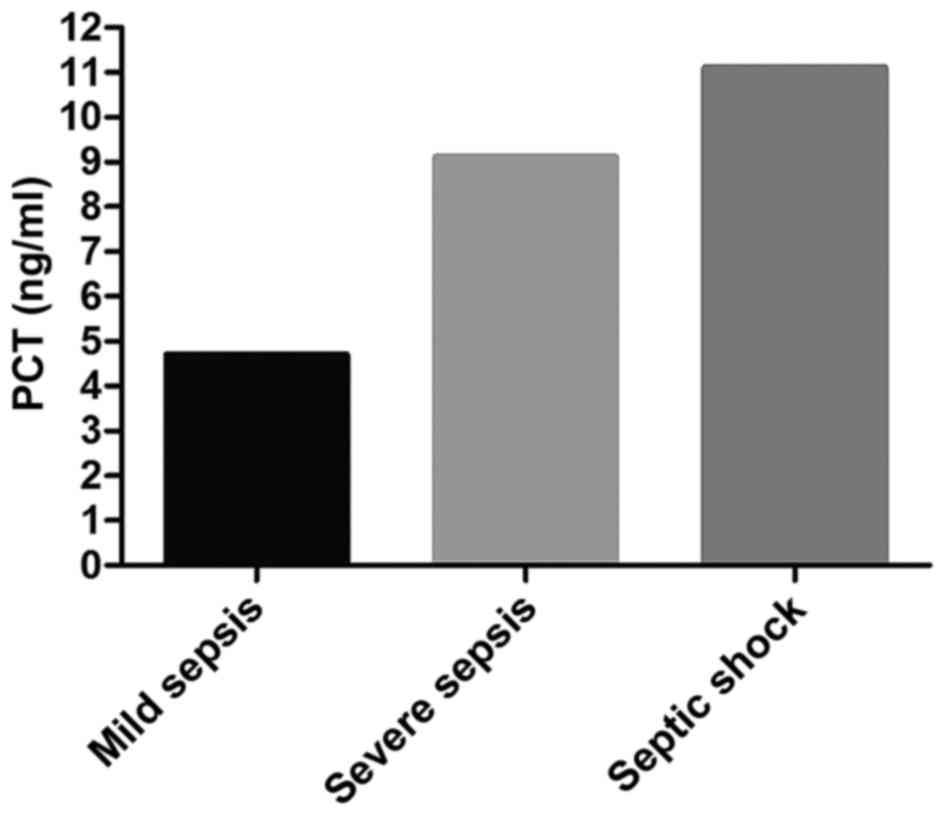
Detection results of PCT
The average PCT level in the sepsis group was
significantly higher than that in the non-sepsis group (P<0.05).
In the sepsis group, the average level of PCT in patients with
septic shock was higher than that in patients with severe sepsis
and mild sepsis (P<0.05); the average PCT level in patients with
severe sepsis was higher than that in patients with mild sepsis
(P<0.05). Comparison of the average PCT level in patients who
died of sepsis at 1 week and 2 weeks after admission and that at
admission showed there were no changes (P>0.05). PCT level in
patients surviving from sepsis at 1 week after admission was
overtly lowered compared with that at admission (P<0.05); PCT
level in those at 2 weeks after admission significantly declined
compared with that at admission (P<0.05). The average level of
PCT in patients who died of sepsis was higher than that in patients
surviving from it (P<0.05) (Figs.
3 and 4 and Table V).
| Table V.Comparisons of the detection results
of PCT between patients surviving sepsis and those who died
(ng/ml). |
Table V.
Comparisons of the detection results
of PCT between patients surviving sepsis and those who died
(ng/ml).
| Time | Patient surviving
sepsis | Patient died of
sepsis | t-value | P-value |
|---|
| No. of cases (n) | 34 | 26 |
|
|
| At admission | 5.8±1.2 | 7.8±1.6 | 2.269 | 0.038 |
| 1 week after
admission |
3.4±0.9a |
8.9±2.1c | 3.012 | 0.024 |
| 2 weeks after
admission |
2.1±0.4b |
8.1±1.4d | 3.985 | 0.015 |
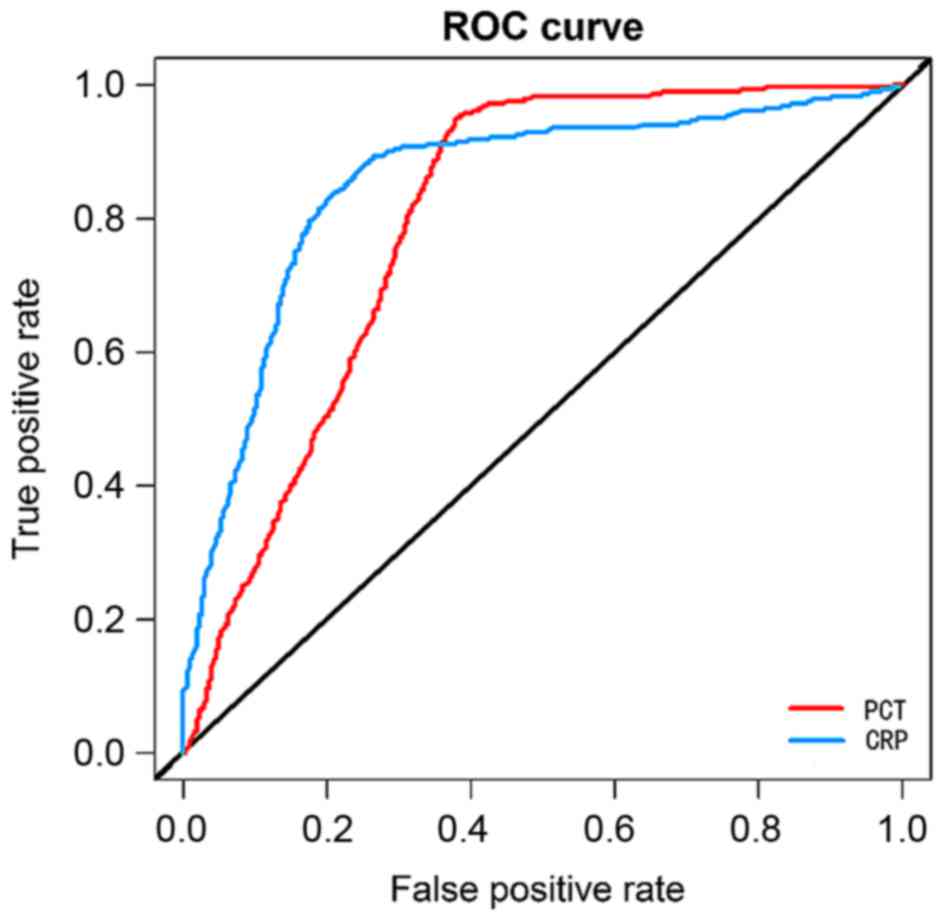
Logistic regression analysis and ROC
analysis
Logistics regression analysis showed that PCT and
CRP levels in patients in the intensive care unit were closely
related to the severity of sepsis and the prognosis of patients.
The higher the PCT and CRP levels were, the more severe the sepsis
and the worse the prognosis would be (r=0.826, P=0.007; r=0.732,
P=0.012). With death as the end of the prognosis of patients, the
values of PCT and CRP in predicting the death of patients were
relatively great, and their areas under the curve (AUC) were 0.734
and 0.699, respectively, and 95% confidence intervals (95% CIs)
were 0.665–0.874 and 0.601–0.792, respectively (Fig. 5).
Univariate Cox regression
analysis
PCT level at 6.9 ng/ml represented that the
specificity and sensitivity of the poor prognosis of patients with
sepsis were 73.6 and 77.5%, respectively, so PCT=6.9 ng/ml was
taken as the critical point between high concentration and low
concentration. CRP concentration at 55.7 mg/l indicated that the
specificity and sensitivity of the poor prognosis of patients were
64.6 and 77.4%, respectively, so CRP=55.7 mg/l was taken as the
critical point between high concentration and low concentration.
Univariate Cox regression analysis revealed that CRP, PCT and age
might be risk factors for the poor prognosis of patients with
sepsis (Table VI).
| Table VI.Univariate Cox regression
analysis. |
Table VI.
Univariate Cox regression
analysis.
|
| Univariate
analysis |
|---|
|
|
|
|---|
| Factors | HR (95% CI) | P-value |
|---|
| Sex (male vs.
female) | 0.734
(0.247–2.356) | 0.792 |
| Age (<50 vs. ≥50
years) | 2.145
(1.549–4.566) | 0.012 |
| CRP (low vs.
high) | 2.141
(1.269–2.724 | 0.013 |
| PCT (low vs.
high) | 3.044
(1.258–7.336) | 0.011 |
Discussion
Sepsis is one of the major causes of patient's death
in the intensive care unit. It leads to the body's use of a large
amount of sugar, lipids and proteins, thus changing the energy
metabolism mode and the rate of energy utilization of patients,
which will cause an additional burden and may also cause
concurrence with hypoproteinemia in patients (13,14).
Moreover, the body's resistance to sepsis-induced tissue damage and
inflammatory responses can further undermine the body's metabolic
balance, and even cause organ failure (15,16).
Therefore, it is very important to predict the occurrence of sepsis
in patients in the intensive care unit, control and treat sepsis in
patients in the intensive care unit, and improve patients' quality
of life and survival time. In this study, the predictive values of
PCT and CRP for sepsis in patients in the intensive care unit and
the prognostic values for patients with sepsis were explored by
examining changes in PCT and CRP levels in patients in the
intensive care unit.
In this study, changes in PCT and CRP levels in 203
intensive care unit patients were measured, and the results
revealed that patients with sepsis had higher levels of PCT and CRP
than non-sepsis patients, suggesting that PCT and CRP may be
related to the occurrence of sepsis. However, no patients without
sepsis was found to develop into patients with sepsis in this
study. Therefore, whether changes in PCT and CRP levels have values
in predicting sepsis needs to be further investigated. The study of
Su et al (17) found that PCT
cannot be completely used to predict the risk of sepsis after
transplantation. The most sensitive indicator for neonatal sepsis
diagnosis is CRP (18). However,
there are few studies on whether CRP can be used as a predictor for
sepsis, so more studies are needed to analyze whether these two
markers can be predictors for sepsis.
In our study, patients with sepsis were further
subdivided in detail according to different components, which
showed that with the aggravation of sepsis in patients, PCT and CRP
levels were also increased. Therefore, logistics regression
analysis was used to analyze the relationships of PCT and CRP
levels with the severity of sepsis, which revealed that the higher
the PCT and CRP levels were, the more severe the sepsis in patients
would be. Univariate Cox regression analysis also manifested that
PCT and CRP might be risk factors for the poor prognosis of
patients with sepsis. Studies of Savva et al (19), and Ashour et al (20) proved that soluble triggering receptor
expressed on myeloid cells 1 (sTREM-1) and PCT have very good
effects in assessing the severity of sepsis. Currently, there is
little research on the value of CRP in assessing the severity of
sepsis. However, Huo et al (21) found that autophagy-related 16-like 1
(ATG16L1) gene polymorphism is closely related to the severity of
sepsis. Whether ATG16L1 affects PCT and CRP levels is worth further
investigation.
During this study, there were 26 cases of death
(43.33%). The prognosis of patients with sepsis was also analyzed.
Logistic regression analysis showed that the higher the PCT and CRP
levels were, the higher the risk of poor prognosis would be.
Further ROC curve analysis revealed that PCT and CRP have good
values in the prognosis of patients with sepsis. PCT is a good
indicator for the diagnosis and prognosis of sepsis, and PCT and
CRP levels are closely related to the severity of infection and
organ dysfunction (22). A study of
Franekova et al (23) also
revealed that serum PCT and CRP can predict the prognosis of
children with sepsis, which is consistent with our results. A study
of Sonawane et al (24)
indicated that CRP can also be used as an early predictor of sepsis
in patients with thermal burns. Therefore, PCT and CRP are good
indicators for the diagnosis and prognosis of sepsis, but their
joint diagnostic values remain to be further explored.
In conclusion, the detection of changes in CRP and
PCT levels has great clinical value in assessing the prognosis of
patients with sepsis. High-level CRP and PCT indicate a poor
prognosis in patients with sepsis.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
QL contributed to design of the study and was
responsible for detection of CRP and PCT levels. He also drafted
and revised the manuscript. XG analyzed and interpreted statistical
analysis. Both authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Qilu Hospital of Shandong University in Dongying (Dongying, China)
and informed consents were signed by the patients and/or
guardians.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Thimmulappa RK, Lee H, Rangasamy T, Reddy
SP, Yamamoto M, Kensler TW and Biswal S: Nrf2 is a critical
regulator of the innate immune response and survival during
experimental sepsis. J Clin Invest. 116:984–995. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Agyeman PKA, Schlapbach LJ, Giannoni E,
Stocker M, Posfay-Barbe KM, Heininger U, Schindler M, Korten I,
Konetzny G, Niederer-Loher A, et al: Epidemiology of blood
culture-proven bacterial sepsis in children in Switzerland: a
population-based cohort study. Lancet Child Adolesc Health.
1:123–133. 2017. View Article : Google Scholar
|
|
3
|
Thimmulappa RK, Lee H, Rangasamy T, Reddy
SP, Yamamoto M, Kensler TW and Biswal S: Nrf2 is a critical
regulator of the innate immune response and survival during
experimental sepsis. J Clin Invest. 116:984–995. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kaukonen KM, Bailey M, Suzuki S, Pilcher D
and Bellomo R: Mortality related to severe sepsis and septic shock
among critically ill patients in Australia and New Zealand,
2000–2012. JAMA. 311:1308–1316. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ferrer R, Martin-Loeches I, Phillips G,
Osborn TM, Townsend S, Dellinger RP, Artigas A, Schorr C and Levy
MM: Empiric antibiotic treatment reduces mortality in severe sepsis
and septic shock from the first hour: Results from a
guideline-based performance improvement program. Crit Care Med.
42:1749–1755. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vincent JL, Opal SM, Marshall JC and
Tracey KJ: Sepsis definitions: Time for change. Lancet.
381:774–775. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liu V, Escobar GJ, Greene JD, Soule J,
Whippy A, Angus DC and Iwashyna TJ: Hospital deaths in patients
with sepsis from 2 independent cohorts. JAMA. 312:90–92. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Caironi P, Tognoni G, Masson S, Fumagalli
R, Pesenti A, Romero M, Fanizza C, Caspani L, Faenza S, Grasselli
G, et al: ALBIOS Study Investigators: Albumin replacement in
patients with severe sepsis or septic shock. N Engl J Med.
370:1412–1421. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yang AP, Liu J, Yue LH, Wang HQ, Yang WJ
and Yang GH: Neutrophil CD64 combined with PCT, CRP and WBC
improves the sensitivity for the early diagnosis of neonatal
sepsis. Clin Chem Lab Med. 54:345–351. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Henriquez-Camacho C and Losa J: Biomarkers
for sepsis. BioMed Res Int. 2014:5478182014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gao L, Liu X, Zhang D, Xu F, Chen Q, Hong
Y, Feng G, Shi Q, Yang B and Xu L: Early diagnosis of bacterial
infection in patients with septicopyemia by laboratory analysis of
PCT, CRP and IL-6. Exp Ther Med. 13:3479–3483. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhang Y and Zhou L: Diagnostic value of
C-reactive protein and procalcitonin for bacterial infection in
acute exacerbations of chronic obstructive pulmonary disease. Zhong
Nan Da Xue Xue Bao Yi Xue Ban. 39:939–943. 2014.(In Chinese).
PubMed/NCBI
|
|
13
|
Seymour CW, Liu VX, Iwashyna TJ,
Brunkhorst FM, Rea TD, Scherag A, Rubenfeld G, Kahn JM,
Shankar-Hari M, Singer M, et al: Assessment of clinical criteria
for sepsis: For the third international consensus definitions for
sepsis and septic shock (Sepsis-3). JAMA. 315:762–774. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kaukonen KM, Bailey M, Pilcher D, Cooper
DJ and Bellomo R: Systemic inflammatory response syndrome criteria
in defining severe sepsis. N Engl J Med. 372:1629–1638. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mayr FB, Yende S and Angus DC:
Epidemiology of severe sepsis. Virulence. 5:4–11. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hotchkiss RS, Monneret G and Payen D:
Immunosuppression in sepsis: A novel understanding of the disorder
and a new therapeutic approach. Lancet Infect Dis. 13:260–268.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Su L, Feng L, Song Q, Kang H, Zhang X,
Liang Z, Jia Y, Feng D, Liu C and Xie L: Diagnostic value of
dynamics serum sCD163, sTREM-1, PCT, and CRP in differentiating
sepsis, severity assessment, and prognostic prediction. Mediators
Inflamm. 2013:9698752013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Li Z, Wang H, Liu J, Chen B and Li G:
Serum soluble triggering receptor expressed on myeloid cells-1 and
procalcitonin can reflect sepsis severity and predict prognosis: A
prospective cohort study. Mediators Inflamm. 2014:6410392014.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Savva A, Plantinga TS, Kotanidou A, Farcas
M, Baziaka F, Raftogiannis M, Orfanos SE, Dimopoulos G, Netea MG
and Giamarellos-Bourboulis EJ: Association of autophagy-related
16-like 1 (ATG16L1) gene polymorphism with sepsis severity in
patients with sepsis and ventilator-associated pneumonia. Eur J
Clin Microbiol Infect Dis. 33:1609–1614. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ashour FH, Maghraby HM and Hassan AS:
Procalcitonin as a diagnostic and prognostic marker of sepsis in
critically Ill patients in intensive care unit. Egypt J Hosp Med.
68:2017.
|
|
21
|
Huo JM, Huo R, Hu L, Lu SW and Zu J: Value
of procalcitonin, high sensitivity C-reactive protein and
pancreatic stone protein in predicting prognosis of children with
sepsis. Sichuan Da Xue Xue Bao Yi Xue Ban. 48:422–426. 2017.(In
Chinese). PubMed/NCBI
|
|
22
|
John J, Chisthi MM and Kuttanchettiyar KG:
C-reactive protein: An early predictor of sepsis in patients with
thermal burns. Int Surg J. 4:628–632. 2017. View Article : Google Scholar
|
|
23
|
Franekova J, Kieslichova E, Brezina A,
Brodska H, Secnik P and Jabor A: Presepsin can replace
procalcitonin in the prediction of sepsis in transplant patients
after antithymocyte globulin administration. Clin Chem Lab Med.
53:S5332015.
|
|
24
|
Sonawane VB, Gaikwad SU, Kadam NN and
Gavhane J: Comparative study of diagnostic markers in neonatal
sepsis. J Nepal Paediatr Soc. 34:111–114. 2014. View Article : Google Scholar
|