Introduction
The human intestine is also known as the second
brain, on the surface of which numerous intestinal flora play an
important role, impacting on the body's immune system, endocrine
system and spiritual emotion; most importantly, it is closely
related to digestive diseases (1).
However, it has been found in previous studies that intestinal
flora disturbance may lead to the occurrence or aggravation of
coronary heart disease (CHD) to a certain extent (2). In patients with CHD, the total amount
of bacteria in the intestine is increased, but the content of
probiotics is reduced and the content of harmful strains is
increased; in particular, intestinal flora disturbance in obese
patients is more likely to become a risk factor for CHD (3). In healthy people, intestinal flora is
relatively stable, because the mucus produced by the intestinal
mucosa contains a certain amount of antimicrobial peptides, which
are a kind of protein that prevents the overgrowth of intestinal
flora. At the same time, the secretion and expression of
antimicrobial peptides are inhibited when the number of intestinal
flora is too low (4). When the
body's homeostasis is damaged, the intestinal flora species and the
level of antibacterial peptides will change, leading to the
occurrence of intestinal flora disturbance and a variety of related
diseases (5). Compared with healthy
people, obese patients are more prone to intestinal flora
disturbance (6), of which the most
representative is the decreased proportion of Bacteroidetes,
the increased proportion of phylum Firmicutes and
over-metabolism of intestinal Clostridium, causing energy
metabolism disorder and obesity (OB)-related metabolic diseases
(7). On the other hand, when
intestinal flora disturbance occurs, the immune system will be
destroyed, the harmful strains in the intestine can secrete
endotoxins and so on, and the intestinal mucosa will be damaged,
causing excessive intravascular inflammatory response, elevated
levels of inflammatory factors in serum, along with increased
expression of adhesion molecules, disorders of vascular regulatory
factor secretion and endothelial damage, eventually leading to
atherosclerosis (8). Therefore, to
explore the relationship of the intestinal flora changes and
inflammatory factors in obese patients with CHD can effectively
reduce the incidence rate of CHD in obese patients and provide more
treatment methods for patients with CHD.
Patients and methods
General data
A total of 75 obese patients in Child Health Care of
Zaozhuang Hospital from March 2015 to September 2016 were selected,
and all selected patients with body mass index (BMI) of ≥28
kg/m2, and the degree of arterial stenosis above 70–75%
according to the patient's clinical manifestations,
electrocardiogram or coronary arteriongraphy were diagnosed with
CHD. They were divided into OB alone (n=40) and OB with CHD group,
including 53 males and 22 females aged 32–75 years with an average
age of (46.73±5.32) years. The present study was approved by the
Ethics Committee of Maternity and Child Health Care of Zaozhuang
(Zaozhuang, China). Signed informed consents were obtained from all
participants before the study. Exclusion criteria; patients with
previous history of chronic diseases, such as hypertension or
diabetes; with severe infectious diseases; with diseases related to
immune dysfunction; with cardiac status and myocardial diseases;
with severe valvular heart disease; and patients who did not use
probiotics, antibiotics or other related drugs that affected the
intestinal flora prior to inclusion into the experiment.
Methods
Detection of total intestinal flora
load and main strains
The feces of the included patients were collected,
and 350 g of the middle part of the feces was selected as the final
specimen. The SYBR-Green I fluorescence quantitative polymerase
chain reaction (PCR) was used to determine the total load of all
bacteria and the main strain load in the feces, including two
probiotic strains, Bifidobacteria and Lactobacilli,
and six kinds of harmful bacteria, Escherichia coli,
Helicobacter pylori, Streptococcus, Staphylococcus, Pseudomonas
aeruginosa and Veillonella. The strain deoxyribonucleic
acid was extracted using the kit provided by Shandong Science and
Technology Co., Ltd., (Shandong, China) and the PCR was carried
out. Finally, the results were measured by the Light Cycler PCR
analyzer (Roche Molecular Diagnostics, Pleasanton, CA, USA). The
logarithm of the fecal bacterial copy number / gram represented the
intestinal bacterial load.
Detection of fecal uric acid
content
The middle part of the feces was centrifuged several
times, and the supernatant was taken in the colorimetric cup to
detect the fecal uric acid (FUA) content by enzyme colorimetric
assay. The results were expressed by the uric acid content
decomposed by the intestinal flora (IFUA) in one gram of feces and
the original FUA content.
Detection of levels of blood uric acid
and inflammatory factors
Peripheral blood (20 ml) was extracted from the
included patients after 10 h of fasting and water deprivation
overnight, and the upper serum was taken. Serum (8 ml) was used to
determine C-reactive protein (CRP), interleukin-6 (IL-6) and tumor
necrosis factor-α (TNF-α) by immunoturbidimetry, with the reagents
and instruments provided by Shandong Biological Instrument Company
(Jinan, China), and the remaining 12 ml was used to detect blood
uric acid (BUA) level by phosphotungstic acid method with 8,100
automatic biochemical analyzer.
The diagnostic criteria for coronary
artery stenosis
Any one lesion in circumflex branch of left coronary
artery, left anterior descending and right coronary artery
indicated the single- any two lesions indicated the double-, and
all lesions indicated the triple-vessel lesion; moreover, when the
left main coronary artery lesion occurred, it was also the
double-vessel lesion whether or not complicated with other branch
lesions; when the left main coronary artery lesion was combined
with the right coronary artery lesion, it was also the
triple-vessel lesion; Gensini score was calculated (Table I).
 | Table I.Gensini score calculation. |
Table I.
Gensini score calculation.
| Angiostegnosis | Score | Diseased artery | Score |
|---|
| <25% | 1 | Left main | 5 |
| 25–50% | 2 | Left descending
branch or proximal circumflex artery | 2.5 |
| 51–75% | 4 | Middle left anterior
descending branch | 1.5 |
| 76–90% | 8 | Distal left anterior
descending branch anterior | 1 |
| 91–99% | 16 | Middle and distal
left circumflex artery | 1 |
| 100% | 32 | Right coronary
artery, small branch | 1, 0.5 |
Statistical analysis
The data were processed by SPSS 19.0 (IBM Corp.,
Armonk, NY, USA), collection data are expressed as mean ± SD,
enumeration data were compared by χ2 test, and
correlation analysis was used for two factors. P<0.05 was
considered to indicate a statistically significant difference.
Results
Comparison of general data between the
CHD and OB group
There were no statistically significant differences
in age, sex, previous history of basic diabetes and hypertension,
and BMI between the CHD and the OB group (P>0.05), and the data
were comparable (Table II).
| Table II.Comparisons of general data between
the CHD and the OB group. |
Table II.
Comparisons of general data between
the CHD and the OB group.
|
| Groups |
|
|---|
|
|
|
|
|---|
| General data | CHD (n=35) | OB (n=40) | P-value |
|---|
| Age (years) | 47.61±4.99 | 45.82±5.28 | 0.873 |
| Sex
(male/female) | 25/10 | 28/12 | 0.798 |
| Diabetes | 0 | 0 | 0.916 |
| Hypertension | 0 | 0 | 0.916 |
| BMI
(kg/m2) | 29.42±3.96 | 28.96±4.70 | 0.577 |
Comparisons of total bacterial and
main strain load between the CHD and the OB group
The total bacterial load in the CHD was
significantly higher than that in the OB group. The levels of two
probiotic strains, Bifidobacterium and Lactobacillus,
were significantly lower than those in the OB group, but the levels
of harmful strains, including Escherichia coli, Helicobacter
pylori, Streptococcus and Staphylococcus, were
significantly higher than those in the OB group, and the
differences were statistically significant (P<0.05); but there
were no differences in Pseudomonas aeruginosa and
Veillonella (P>0.05) (Table
III).
| Table III.Comparisons of total bacterial load
and main strain load between the CHD and the OB group. |
Table III.
Comparisons of total bacterial load
and main strain load between the CHD and the OB group.
|
| Groups |
|
|---|
|
|
|
|
|---|
| Bacterial load | CHD (n=35) | OB (n=40) | P-value |
|---|
| Total bacterial
load | 12.03 | 7.79 | 0.001 |
|
Bifidobacteria | 2.98 | 6.82 | >0.05 |
|
Lactobacillus | 1.29 | 5.41 | 0.005 |
| Escherichia
coli | 8.96 | 5.42 | 0.019 |
| Helicobacter
pylori | 9.41 | 6.89 | 0.017 |
|
Streptococcus | 8.05 | 3.92 | 0.001 |
|
Staphylococcus | 6.43 | 3.06 | 0.047 |
| Pseudomonas
aeruginosa | 5.71 | 6.38 | 0.072 |
|
Veillonella | 5.23 | 5.17 | 0.083 |
Comparison of the levels of FUA and
BUA between the CHD and the OB group
The levels of IFUA and BUA in the CHD were higher
than those in the OB group, but the FUA content was lower than that
in the OB group (P<0.05) (Table
IV). Comparison of levels of inflammatory factors between the
CHD and the OB group. The levels of peripheral blood inflammatory
factors in the CHD group, including CRP, IL-6 and TNF-α, were
significantly higher than those in the OB group (P<0.05)
(Table V).
| Table IV.Comparisons of the levels of FUA and
BUA between the CHD and the OB group. |
Table IV.
Comparisons of the levels of FUA and
BUA between the CHD and the OB group.
|
| Groups |
|
|---|
|
|
|
|
|---|
| Uric acid level | CHD (n=35) | OB (n=40) | P-value |
|---|
| IFUA (mg/g) | 0.42±0.15 | 0.15±0.09 | 0.001 |
| FUA (µmol/l) | 13.93±7.97 | 19.08±4.93 | 0.001 |
| BUA (µmol/l) | 492.92±75.41 | 301.53±49.83 | 0.001 |
| Table V.Comparison of the levels of
inflammatory factors between the CHD and the OB group. |
Table V.
Comparison of the levels of
inflammatory factors between the CHD and the OB group.
|
| Groups |
|
|---|
|
|
|
|
|---|
| Inflammatory
factors | CHD (n=35) | OB (n=40) | P-value |
|---|
| TNF-α (pg/ml) | 14.29±4.18 | 8.64±2.29 | 0.001 |
| IL-6 (ng/l) | 17.43±2.23 | 8.41±1.16 | 0.001 |
| CRP (mg/l) | 8.42±1.44 | 2.81±1.68 | 0.001 |
Comparison of the coronary artery
lesions and Gensini score between the CHD and the OB group
By comparison of two groups of patients, it was
found that the incidence rate of single coronary artery lesion
(14.93%) in the CHD group was lower than that in patients without
CHD (51.19%), but the incidence rate of double- and triple-vessel
lesions were significantly higher than those in patients without
CHD (30.66 and 56.15%), and the differences were statistically
significant (P<0.05) (Table
VI).
| Table VI.Comparison of the coronary artery
lesions and Gensini score between the CHD and the OB group. |
Table VI.
Comparison of the coronary artery
lesions and Gensini score between the CHD and the OB group.
|
| Groups |
|
|---|
|
|
|
|
|---|
| Lesion | CHD (n=35) | OB (n=40) | P-value |
|---|
| Single-vessel
lesion | 14.93% | 51.19% | 0.001 |
| Double-vessel
lesion | 30.66% | 18.25% | 0.029 |
| Triple-vessel
lesion | 54.41% | 30.56% | 0.021 |
| Gensini score
(points) | 36.26±19.38 | 9.69±15.87 | >0.05 |
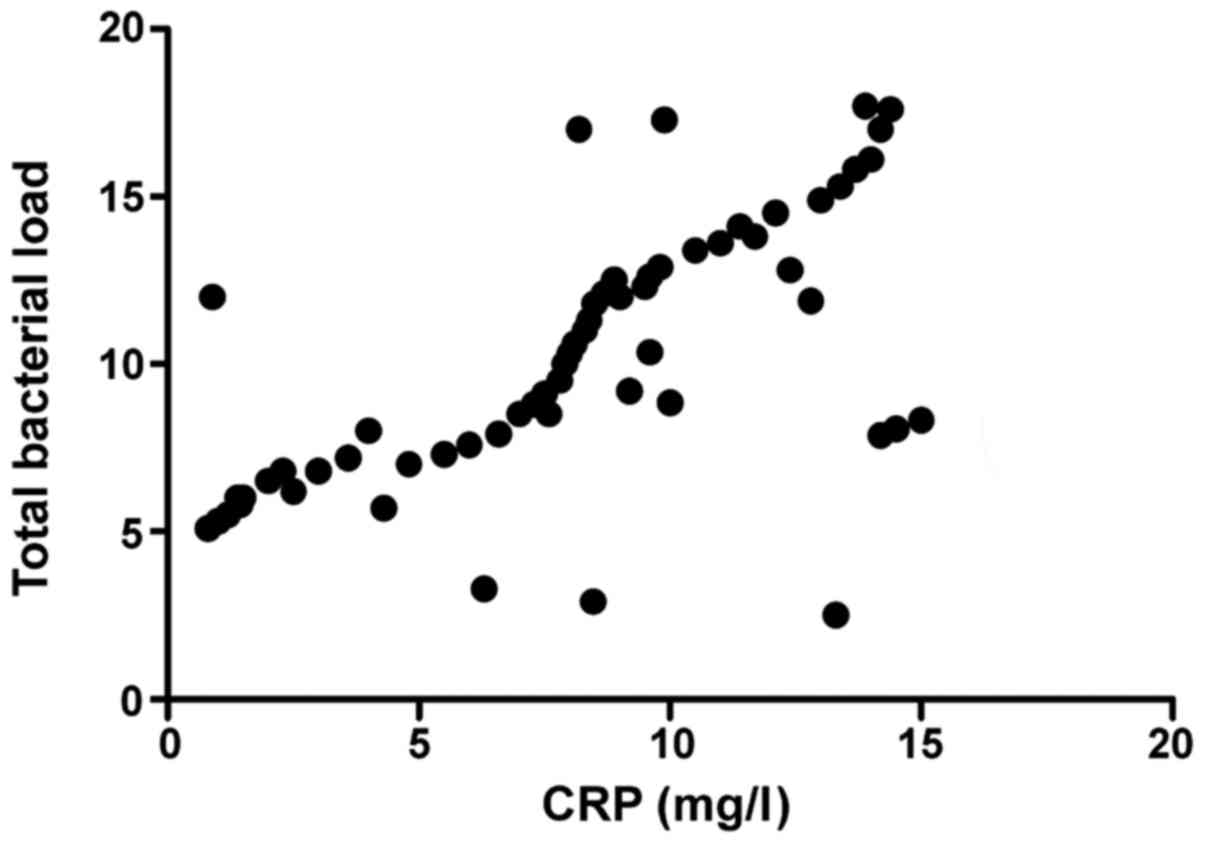
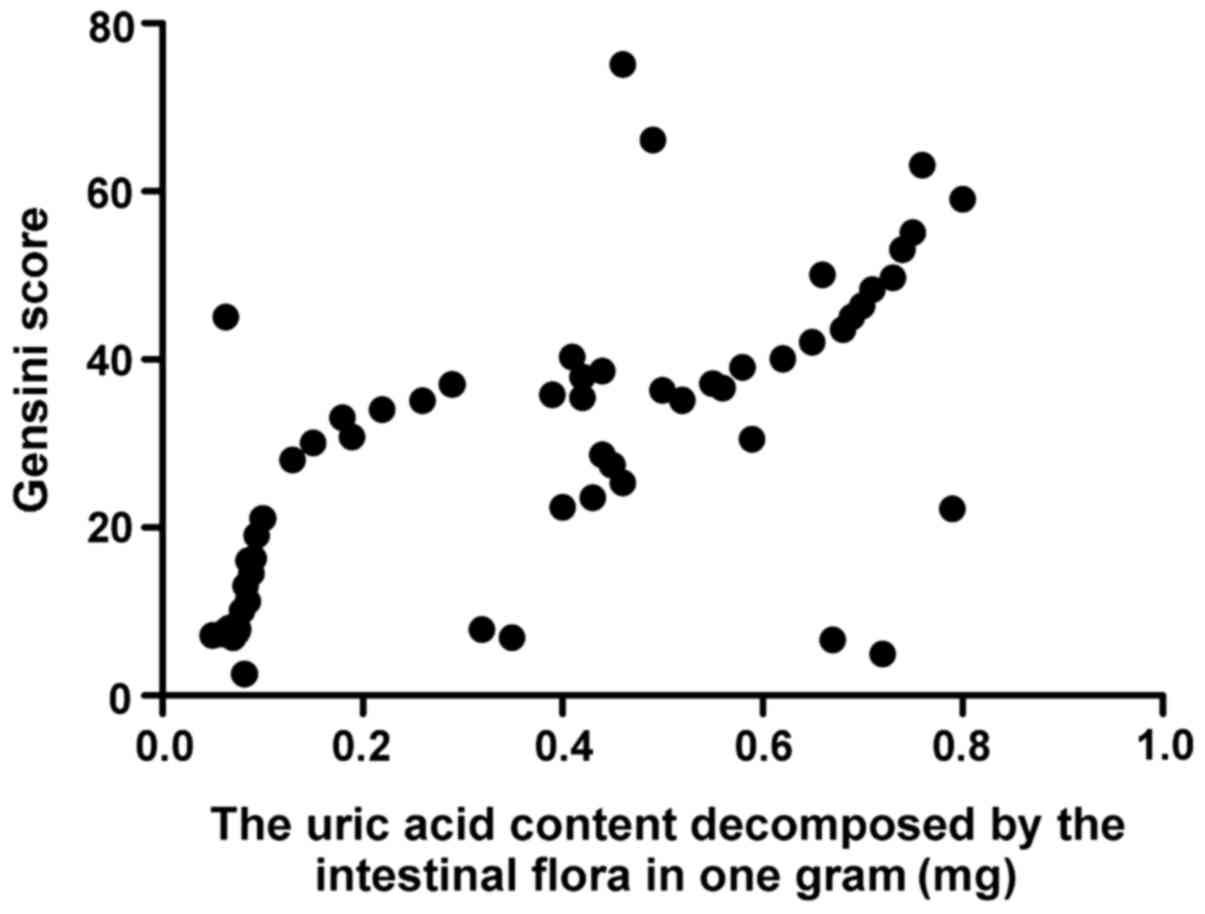
Correlation analysis
The total intestinal flora load was positively
correlated with CRP (r=0.793, P>0.05) and Gensini score
(r=0.893, P>0.05), CRP was positively correlated with Gensini
score (r=0.796, P<0.001), and the activity of FUA decomposed by
intestinal flora was positively correlated with Gensini score
(r=0.647, P<0.001) (Figs.
1–4).
Discussion
The process of maintaining human life and health,
the stability of intestinal flora plays a significant role, and
intestinal flora disturbance not only leads to the occurrence of
digestive diseases (9), but also
affects the occurrence and development of other diseases of the
body, such as metabolic, immune and cardiovascular system diseases,
and also affects the changes in brain emotion (10). In healthy people, intestinal flora is
in a state of balance, which can protect the body, promote the
digestion and absorption of food, and maintain the homeostasis of
the internal environment. When the intestinal flora disturbance
occurs, it will cause various diseases of the body (11). Increasing experimental data show that
intestinal flora disturbance in obese patients is related to the
occurrence of CHD (12). It has been
found that the increase of intestinal pathogens is related to
cardiac risk events and the severity and prognosis of disease, and
a variety of harmful strains in the intestine may play a
superimposed effect (13). When the
total load of bacteria and harmful bacteria in the intestine is
increased, and the number of probiotics is reduced, it will
aggravate the overreaction of inflammatory stress and increase the
possibility of coronary atherosclerotic heart disease (14). It was also found in the present study
that the total bacterial load and harmful bacteria load in the CHD
were significantly higher than those in the OB group, the
differences were statistically significant (P<0.05), and the
total bacterial load was positively correlated with the Gensini
score. In addition, most of the clinical views believe that the
occurrence of cardiovascular disease is related to the elevated BUA
level (15). When intestinal flora
disturbance occurs, the increased harmful bacteria will lead to the
increased level of FUA decomposed by bacteria, decreased level of
original FUA (16), and the increase
of BUA level, which is consistent with the conclusion of the
present study.
It was found in an in vitro study that a
variety of Lactobacilli and Bifidobacteria were
extracted from feces of normal people and concluded that these two
strains had very strong effects, and the most obvious one was
against Pseudomonas aeruginosa preventing the formation of
pseudomembrane (17). When
intestinal flora disturbance occurs in obese patients, the
intestinal mucosa will be damaged, the body's inflammatory response
is excessive, and the serum levels of CRP, IL-6 and TNF-α are
elevated; atherosclerosis itself is an inflammatory disease
(18). The increased levels of
inflammatory factors lead to vascular endothelial damage, along
with increased expression of adhesion molecules, disorders of
vascular regulatory factor secretion, and vascular endothelial
damage, eventually leading to atherosclerosis. It was also found in
the present study that the levels of inflammatory factors in obese
patients complicated with CHD were significantly higher than those
in only obese patients, and the inflammatory factor levels were
positively correlated with total intestinal bacterial load and
Gensini score, indicating that when flora disturbance occurs in
obese patients, the higher the inflammatory factor levels are, the
greater the possibility of CHD will be (19,20).
In conclusion, the occurrence of flora disturbance
in obese patients may lead to CHD, and the levels of inflammatory
factors and the level of uric acid decomposed by intestinal
bacteria are also closely related to the occurrence and development
process of the disease. The treatment of intestinal flora
disturbance and reduction of inflammatory response can prevent or
treat CHD to some extent.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
XL designed the study, CL collected and analysed the
data, XL prepared the manuscript. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Maternity and Child Health Care of Zaozhuang (Zaozhuang, China).
Signed informed consents were obtained from all patients or their
guardians before the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Yang T, Santisteban MM, Rodriguez V, Li E,
Ahmari N, Carvajal JM, Zadeh M, Gong M, Qi Y, Zubcevic J, et al:
Gut dysbiosis is linked to hypertension. Hypertension.
65:1331–1340. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lau E, Carvalho D and Freitas P: Gut
microbiota: Association with NAFLD and metabolic disturbances.
BioMed Res Int. 2015:1–10. 2015. View Article : Google Scholar
|
|
3
|
Qin J, Li Y, Cai Z, Li S, Zhu J, Zhang F,
Liang S, Zhang W, Guan Y, Shen D, et al: A metagenome-wide
association study of gut microbiota in type 2 diabetes. Nature.
490:55–60. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ley RE, Turnbaugh PJ, Klein S and Gordon
JI: Microbial ecology: Human gut microbes associated with obesity.
Nature. 444:1022–1023. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wahlström A, Sayin SI, Marschall HU and
Bäckhed F: Intestinal crosstalk between bile acids and microbiota
and its impact on host metabolism. Cell Metab. 24:41–50. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Canfora EE, Jocken JW and Blaak EE:
Short-chain fatty acids in control of body weight and insulin
sensitivity. Nat Rev Endocrinol. 11:577–591. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Biedermann L and Rogler G: The intestinal
microbiota: Its role in health and disease. Eur J Pediatr.
174:151–167. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Eckburg PB, Bik EM, Bernstein CN, Purdom
E, Dethlefsen L, Sargent M, Gill SR, Nelson KE and Relman DA:
Diversity of the human intestinal microbial flora. Science.
308:1635–1638. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhang J, Chen SL and Li LB: Correlation
between intestinal flora and serum inflammatory factors in patients
with Crohn's disease. Eur Rev Med Pharmacol Sci. 21:4913–4917.
2017.PubMed/NCBI
|
|
10
|
Sargent J: Obesity: Rethinking
inflammation and adipocyte homeostasis. Nat Rev Endocrinol.
10:4462014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
van Greevenbroek MM, Schalkwijk CG and
Stehouwer CD: Obesity-associated low-grade inflammation in type 2
diabetes mellitus: Causes and consequences. Neth J Med. 71:174–187.
2013.PubMed/NCBI
|
|
12
|
El Kaoutari A, Armougom F, Gordon JI,
Raoult D and Henrissat B: The abundance and variety of
carbohydrate-active enzymes in the human gut microbiota. Nat Rev
Microbiol. 11:497–504. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tang C, Ahmed K, Gille A, Lu S, Gröne HJ,
Tunaru S and Offermanns S: Loss of FFA2 and FFA3 increases insulin
secretion and improves glucose tolerance in type 2 diabetes. Nat
Med. 21:173–177. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kimura I, Ozawa K, Inoue D, Imamura T,
Kimura K, Maeda T, Terasawa K, Kashihara D, Hirano K, Tani T, et
al: The gut microbiota suppresses insulin-mediated fat accumulation
via the short-chain fatty acid receptor GPR43. Nat Commun.
4:18292013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kasai C, Sugimoto K, Moritani I, Tanaka J,
Oya Y, Inoue H, Tameda M, Shiraki K, Ito M, Takei Y, et al:
Comparison of the gut microbiota composition between obese and
non-obese individuals in a Japanese population, as analyzed by
terminal restriction fragment length polymorphism and
next-generation sequencing. BMC Gastroenterol. 15:1002015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bishara J, Farah R, Mograbi J, Khalaila W,
Abu-Elheja O, Mahamid M and Nseir W: Obesity as a risk factor for
clostridium difficile infection. Clin Infect Dis. 57:489–493. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wang H and Eckel RH: Lipoprotein lipase:
From gene to obesity. Am J Physiol Endocrinol Metab. 297:271–288.
2009. View Article : Google Scholar
|
|
18
|
Kotzbeck P and Zechner R:
Angiopoietin-like 4: An endogenous break of intestinal lipid
digestion. Mol Metab. 3:88–89. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bäckhed F, Manchester JK, Semenkovich CF
and Gordon JI: Mechanisms underlying the resistance to diet-induced
obesity in germ-free mice. Proc Natl Acad Sci USA. 104:979–984.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mahalle N, Garg M, Kulkarni M and Naik S:
Association of inflammatory cytokines with traditional and
nontraditional cardiovascular risk factors in indians with known
coronary artery disease. Ann Med Health Sci Res. 4:706–712. 2014.
View Article : Google Scholar : PubMed/NCBI
|