Introduction
Intracerebral hemorrhage is a common and
frequently-occurring disease with high mortality and disability
rates, accounting for 10–15% of cerebrovascular diseases, and the
mortality rate is greater than 50% (1). The curative effect is directly affected
by the therapeutic method after intracerebral hemorrhage. The
minimally invasive hematoma evacuation early used for patients with
hypertensive intracerebral hemorrhage can reduce the compression to
surrounding brain tissue by hematoma, and ischemia and edema caused
by local hematoma compression can be relieved; after hematoma is
removed, the damage of brain tissue around hematoma caused by
hematoma decomposition product can also be reduced, thus
ameliorating brain function. Additionally, great attention has been
paid to the neuroprotective effect of mild hypothermia therapy; it
can protect brain tissue via inhibiting inflammatory response,
reducing brain edema, decreasing metabolism of brain tissue
(2,3). In recent years, the study on
intracerebral hemorrhage has gradually focused on brain function
protection of brain tissues around the hematoma, generally
considering that inflammatory response is involved in the
pathological process of the damage of brain tissue around hematoma
after intracerebral hemorrhage. In the early stage of intracerebral
hemorrhage, inflammatory response already exist in the local brain
tissue around the hematoma; therein, nuclear factor-κB (NF-κB) and
inflammatory cytokine, tumor necrosis factor-α (TNF-α), play
important roles, which can aggravate the damage of brain tissue
around the hematoma after intracerebral hemorrhage. By comparing
postoperative expression of NF-κB and TNF-α after treatment with
mild hypothermia combined with minimally invasive hematoma
evacuation or minimally invasive hematoma evacuation only, the
present study aimed to investigate the protective effect of mild
hypothermia therapy in reducing inflammatory damage after minimally
invasive hematoma evacuation in the treatment of intracerebral
hemorrhage.
Patients and methods
Clinical data
A total of 206 patients with acute spontaneous
hypertensive intracerebral hemorrhage in Shanghai Renji Hospital
(Shanghai, China) between May 2014 and September 2016 were
collected. The patients, 111 males and 95 females, were treated
within 48 h of onset, and they suffered the first onset at the
average age of 55.67±21.53 years. This study was approved by the
Ethics Committee of Shanghai Renji Hospital. Signed written
informed consents were obtained from all participants before the
study. All patients conformed to the Fourth Cerebrovascular
Diseases Academic Meeting of the Chinese Medical Association:
Diagnostic Points of Various Cerebrovascular Diseases and diagnosed
as intracerebral hemorrhage by head computed tomography (CT) and
magnetic resonance imaging (MRI). Calculation of hematoma volume
after intracerebral hemorrhage: According to the CT film
measurement and Coniglobus formula (volume = π/6 × length × width ×
layer) calculation, the amount of bleeding was >30 ml (4). The National Institutes of Health Stroke
Scale (NIHSS) score was used before and after treatment and
examined by the same neurology physician. Patients were treated by
minimally invasive hematoma evacuation on the day of onset or on
the following day (<48 h). The mild hypothermia treatment group
received local mild hypothermia therapy immediately after the
operation, and the conventional therapies including dehydrant and
brain protectants were taken by the two groups. Exclusion criteria:
All of the following cases were excluded to avoid confusion of
inflammatory markers: i) Patients with inflammatory disease within
half a month; ii) patients who were accompanied by severe
complications; iii) patients with cardiovascular diseases, trauma,
surgery, age less than 18 years or pregnancy within 6 months; iv)
patients using drugs, such as anticoagulants, corticosteroids and
β-receptor blockers; v) patients with abnormal blood pressure,
systolic pressure >210 mmHg or <100 mmHg; diastolic pressure
>110 mmHg or <50 mmHg; and vi) patients or their families who
refused surgery.
Minimally invasive hematoma evacuation
and mild hypothermia therapy
YL-1 type disposable intracranial hematoma grinding
puncture needle (produced by Beijing Wantefu Medical Apparatus,
Co., Ltd., Beijing, China) was utilized to perform minimally
invasive hematoma evacuation. Before the surgery, blood pressure
was controlled below 160/100 mmHg. The surgery was conducted under
local anesthesia. The whole body water circulation type cooling
blanket plus local cerebral mild hypothermia therapy with ice cap
was adopted. Sedatives were used for patients with shivers. The
whole body water circulation type cooling blanket (P&C-A type
cooling blanket; Hengbang, Beijing, China) and −4 to −2°C ice cap
(HGT-200 II type; Beijing D&W Medical Equipment Co., Ltd.,
Beijing, China) were utilized as superficial hypothermia treatment.
The brain temperature was decreased to 32.5–34.5°C, which was
displayed by tympanic temperature. The brain temperature was
replaced by tympanic temperature on the affected side. Brain
temperature = tympanic temperature ±0.5°C was regarded as standard,
and it was measured by OMRON infrared ear thermometer after
operation, 2 times per day, followed by taking the highest value.
The duration of mild hypothermia was 3–7 days. Rewarming method:
After mild hypothermia was stopped, the rewarming by 0.5°C should
be maintained for patients approximately every 12 h, followed by
natural rewarming of body temperature to ~37°C.
NIHSS score
The NIHSS score was used before and after treatment
(5,6). The full marks are 42 points. The degree
of nerve function defect was divided into: Mild, NIHSS score <7
points; moderate, NIHSS score 7–15 points; and severe, NIHSS >15
points.
Detection of NF-κB and TNF-α
The hypertensive patients with cerebral hemisphere
bleeding volume over 30 ml treated by minimally invasive hematoma
evacuation on the day or second days of intracelebral hemorrhage
were selected. The brain tissue fragments around hematoma taken out
with rinsing during operation and at postoperative 1, 3 and 7 days
were collected and immediately fixed using formaldehyde, followed
by keeping at normal temperature. Meanwhile, 2 ml morning fasting
venous blood was extracted, centrifuged and placed at −40°C.
Statistical analysis
The experimental results were treated by SPSS 17.0
software (version X; SPSS, Inc., Chicago, IL, USA). The numerical
value was expressed as mean ± standard deviation (SD). The
independent sample t-test was used for the comparison between two
groups. A P<0.05 was considered to indicate a statistically
significant difference.
Results
NIHSS scores in the two groups of
patients
The basic data at admission in the two groups of
patients are shown in Table I. There
were no statistically significant differences in sex, age, average
initial NIHSS score, blood pressure, bleeding amount and other
indexes in patients between the two groups. NIHSS score was the
highest at admission and on the 1st day after treatment, which was
gradually decreased with the treatment; it was significantly lower
in group B than that in group A at 3 and 7 days, and the
differences were statistically significant (P<0.05) (Table II).
 | Table I.Basic data of patients at admission
(mean ± SD). |
Table I.
Basic data of patients at admission
(mean ± SD).
| Items | Group A (n=103) | Group B (n=103) | P-value |
|---|
| Age (years) | 51.53±15.39 | 52.87±14.40 | 0.19 |
| Admission delay
(h) | 4.39±1.98 | 4.75±2.06 | 0.83 |
| NIHSS score | 17.04±3.06 | 16.79±2.56 | 0.56 |
| Bleeding amount
(ml) | 38.19±9.32 | 39.02±10.74 | 0.92 |
| Systolic pressure
(mHg) | 148.73±17.59 | 145.94±15.64 | 0.37 |
| Diastolic pressure
(mmHg) | 96.29±11.59 | 88.65±14.60 | 0.18 |
| Temperature (°C) | 37.26±0.39 | 37.02±0.40 | 0.84 |
| White blood cell
(×109) | 12.18±2.86 | 11.93±1.95 | 0.31 |
| Monocyte
(×109) | 0.79±0.36 | 0.78±0.41 | 0.27 |
| Lymphocyte
(×109) | 4.38±0.39 | 4.28±0.63 | 0.42 |
| Neutrophile
granulocyte (×109) | 8.04±1.89 | 7.93±1.59 | 0.48 |
| Blood glucose
(mmol/l) | 8.05±2.34 | 8.21±3.62 | 0.26 |
| Table II.NIHSS scores in the two groups of
patients (points, mean ± SD). |
Table II.
NIHSS scores in the two groups of
patients (points, mean ± SD).
| Groups | No. | At admission | 1 day | 3 days | 7 days |
|---|
| A | 103 | 16.96±3.06 | 16.39±3.56 | 15.99±2.75 | 14.37±2.07 |
| B | 103 | 17.05±2.97 | 16.28±2.78 |
15.01±2.04a |
12.38±1.45a |
Dynamic changes of serum TNF-α in the
two groups of patients
Radioimmunoassay kit for serum TNF-α in two groups
of patients was purchased from Wuhan Boster Biological Technology,
Co., Ltd. (Wuhan, China). The concentration in group A was the
highest at 3 days after treatment, and rapidly decreased at 7 days
with the treatment; the serum TNF-α concentration in group B was
gradually decreased, which had no difference at day 1 between the
two groups; the concentration was significantly lower in group B
than that in group A at days 3 and 7, and the differences were
statistically significant (P<0.05) (Table III).
| Table III.Comparison of serum TNF-α
concentrations in patients between the two groups (ng/ml, mean ±
SD). |
Table III.
Comparison of serum TNF-α
concentrations in patients between the two groups (ng/ml, mean ±
SD).
| Groups | No. | 1 day | 3 days | 7 days |
|---|
| A | 103 | 3.1385±0.3759 | 3.4984±0.5730 | 2.8046±0.7028 |
| B | 103 | 3.0037±0.4291 |
2.8304±0.4826a |
1.1840±0.7820a |
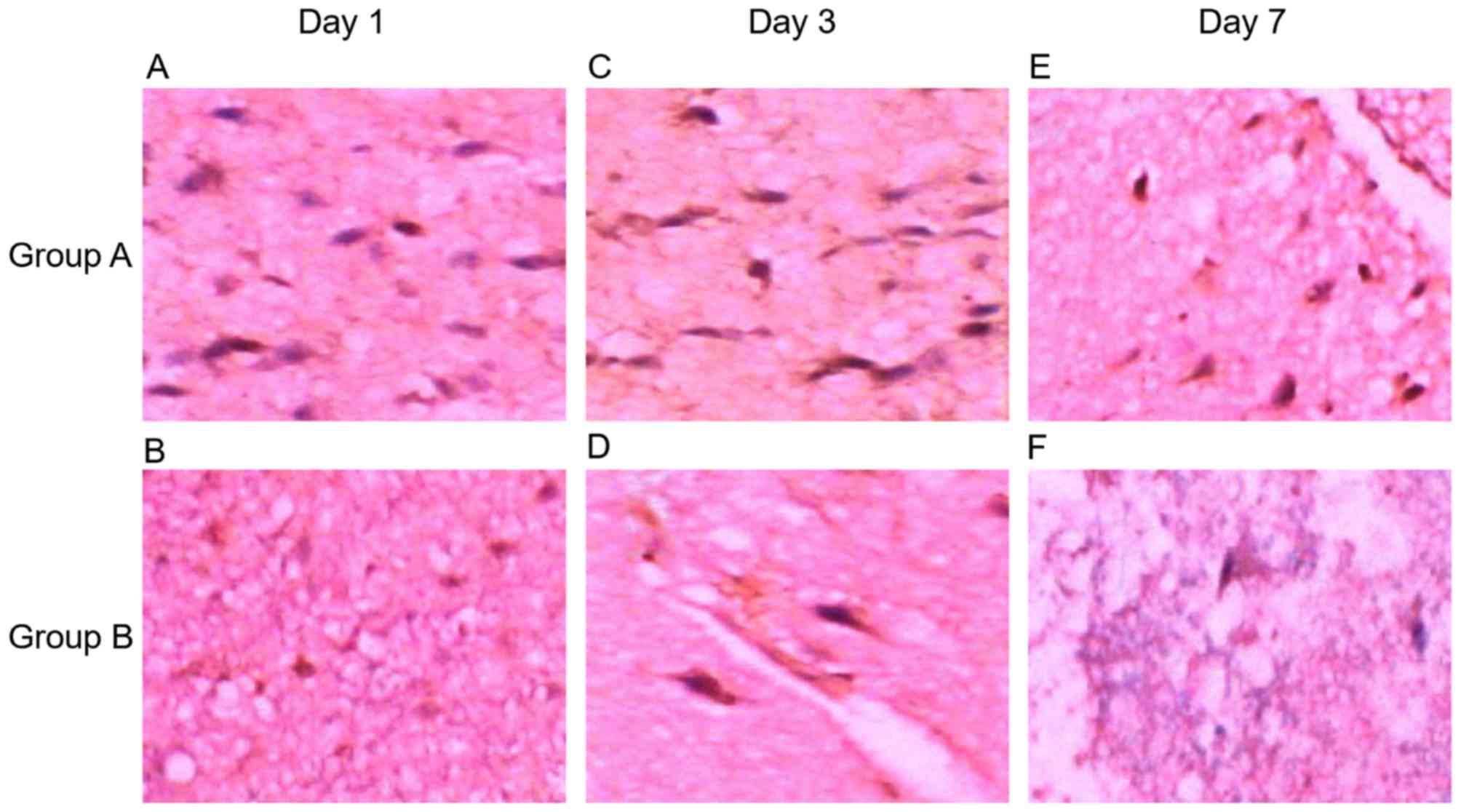
Immunohistochemical staining and NF-κB
determination
Hematoxylin and eosin (H&E) staining displayed
loose tissue around the hematoma, extensive extravascular space,
and a gap around the nerve cells and glial cells (Fig. 1A; H&E, magnification, ×200);
nerve cell body atrophy, karyopyknosis, Nissls body disappearance
and eosinophilic change in cytoplasm; a large number of neutrophils
and lymphocytes existed around the hematoma (Fig. 1B; H&E, magnification, ×100).
Additionally, NF-κB was expressed in brain tissue around the
hematoma in 206 patients, showing dynamic changes, which reached
the peak at day 3, and increased at days 1 and 7. NF-κB expression
was reduced in patients in the mild hypothermia combined with
minimally invasive hematoma evacuation group compared to that in
the minimally invasive hematoma evacuation group. NF-κB was mainly
expressed in the inflammatory cells, microglia and neural cells
(Fig. 2).
Discussion
It has been demonstrated that mild hypothermia has a
neuroprotective effect on patients with cerebral vascular disease,
cerebral trauma and cerebral injury after cardiopulmonary
resuscitation (7–9). The recent experiment and clinical study
have indicated that mild hypothermia can also protect brain
function after intracerebral hemorrhage via inhibiting immune
inflammatory response, decreasing vascular permeability and
reducing brain edema, stabilizing ion pump and inhibiting nerve
excitability cascade reactions, reducing brain metabolism and other
mechanisms. The cerebral protective effect of mild hypothermia was
first applied in the study by Busto in 1987, and it has become the
focus of brain protection again in recent years (10). The study revealed that the duration
of mild hypothermia over 48 h can effectively reduce brain injury,
and the longest duration is better when not more than 196 h,
temperature 32–35°C. Currently, the studies of cardiopulmonary
resuscitation showed that brain hypothermia induced by local
cooling or combined with whole body cooling methods at the
beginning of resuscitation that make patients reach target
temperature (34°C) 2 h earlier has a high safety and feasibility,
and prognosis of the nervous system is significantly ameliorated
(11,12). Furthermore, no increase of
complications such as heart disease, inflammatory lesion, and
disturbance of blood coagulation, electrolyte abnormality, blood
glucose abnormality or blood pressure abnormality has been found.
Hence, we adopted whole body cooling plus local brain mild
hypothermia therapy, decreasing brain temperature to 32.5–34.5°C,
lasting 3–7 days for mild hypothermia therapy, to treat patients
with intracerebral hemorrhage after surgery of minimally invasive
hematoma evacuation.
Clinical studies have revealed that during the acute
cerebral hemorrhage period, body's inflammatory response is
activated by central nervous system due to brain cell injury, thus
producing a large number of inflammatory cytokines, such as TNF-α
and IL-6; a great quantity of secretion and expression of
inflammatory cytokines with proinflammatory effects is positively
correlated with brain injury (13,14). In
a variety of inflammatory factors, TNF-α shows the earliest
expression and the most release, while NF-κB is an important
pathway in the expression and progression of TNF-α, IL-6 and other
inflammatory mediators, which is a crucial regulator of immune
inflammatory reaction. Minimally invasive hematoma evacuation can
decrease the hematoma volume, reduce the compression to surrounding
brain tissue by hematoma, relieve cerebral edema, decrease
intracranial pressure, reduce production of inflammatory factors
and alleviate inflammatory injury, thus protecting brain cell
function. Our experimental results displayed that after hemorrhage,
TNF-α concentration in blood and NF-κB expression in brain tissue
around hematoma changed in line with the illness; TNF-α content in
serum was increased on the 1st day, reaching the peak on the 3rd
day, and was the lowest on the 7th day; the same manner of change
could be seen in NF-κB expression in brain tissue around the
hematoma. TNF-α content and NF-κB expression were lower in the mild
hypothermia combined with minimally invasive hematoma evacuation
group than those in the single minimally invasive surgery group at
each time-point. NIHSS was the highest at admission and on the 1st
day after treatment in the two groups of patients, and it was
decreased with the treatment; the score was distinctly higher at 3
days than that at 7 days, which was consistent with the changes of
TNF-α and NF-κB. NIHSS score was obviously lower in the mild
hypothermia combined with minimally invasive hematoma evacuation
group than that in the single minimally invasive hematoma
evacuation group at 3 and 7 days.
In conclusion, mild hypothermia combined with
minimally invasive hematoma evacuation can alleviate inflammatory
response of brain tissue around hematoma in hypertensive
intracerebral hemorrhage, thus effectively ameliorating and
improving brain function. Our experimental results also confirmed
the safety, effectiveness and feasibility of mild hypothermia
combined with minimally invasive hematoma evacuation.
Acknowledgements
Not applicable.
Funding
The present study was financially supported by The
Science and Technology Developing Fundation of Shanghai Pudong New
Area (Shanghai, China)
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
JiZ and QM designed the study, ZQi and JuZ collected
the data, ZQu and JuZ analysed the data, JiZ and ZQu prepared the
manuscript, JiZ and CW performed the experiments. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Shanghai Renji Hospital (Shanghai, China). Signed written informed
consents were obtained from all participants before the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Xu Y, Guo J, Liu X, Li J, Wang J and Hou
L: Can herbal medicine cause hematoma enlargement of hypertensive
intracerebral hemorrhage within 24 hrs time window? A retrospective
study of 256 cases from a single center in china. Evid Based
Complement Alternat Med. 2015:8687312015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Liu L and Yenari MA: Clinical application
of therapeutic hypothermia in stroke. Neurol Res. 31:331–335. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kollmar R, Staykov D, Dörfler A,
Schellinger PD, Schwab S and Bardutzky J: Hypothermia reduces
perihemorrhagic edema after intracerebral hemorrhage. Stroke.
41:1684–1689. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Broderick JP, Brott TG, Duldner JE,
Tomsick T and Huster G: Volume of intracerebral hemorrhage. A
powerful and easy-to-use predictor of 30-day mortality. Stroke.
24:987–993. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Schlegel D, Kolb SJ, Luciano JM, Tovar JM,
Cucchiara BL, Liebeskind DS and Kasner SE: Utility of the NIH
Stroke Scale as a predictor of hospital disposition. Stroke.
34:134–137. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Young FB, Weir CJ and Lees KR: GAIN
International Trial Steering Committee and Investigators:
Comparison of the National Institutes of Health Stroke Scale with
disability outcome measures in acute stroke trials. Stroke.
36:2187–2192. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Abou-Chebl A, Sung G, Barbut D and Torbey
M: Local brain temperature reduction through intranasal cooling
with the RhinoChill device: Preliminary safety data in
brain-injured patients. Stroke. 42:2164–2169. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ma LL, Song L, Yu XD, Yu TX, Liang H and
Qiu JX: The clinical study on the treatment for acute cerebral
infarction by intra-arterial thrombolysis combined with mild
hypothermia. Eur Rev Med Pharmacol Sci. 21:1999–2006.
2017.PubMed/NCBI
|
|
9
|
Martin-Schild S, Hallevi H, Shaltoni H,
Barreto AD, Gonzales NR, Aronowski J, Savitz SI and Grotta JC:
Combined neuroprotective modalities coupled with thrombolysis in
acute ischemic stroke: A pilot study of caffeinol and mild
hypothermia. J Stroke Cerebrovasc Dis. 18:86–96. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Busto R, Dietrich WD, Globus MY, Valdes I,
Scheinberg P and Ginsberg MD: Small differences in intraischemic
brain temperature critically determine the extent of ischemic
neuronal injury. J Cereb Blood Flow Metab. 7:729–738. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tsai MS, Barbut D, Wang H, Guan J, Sun S,
Inderbitzen B, Weil MH and Tang W: Intra-arrest rapid head cooling
improves post resuscitation myocardial function in comparison with
delayed post resuscitation surface cooling. Crit Care Med.
36:434–439. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Guan J, Barbut D, Wang H, Li Y, Tsai MS,
Sun S, Inderbitzen B, Weil MH and Tang W: A comparison between head
cooling begun during cardiopulmonary resuscitation and surface
cooling after resuscitation in a pig model of cardiac arrest. Crit
Care Med. 36:428–433. 2008. View Article : Google Scholar
|
|
13
|
Nimmo AJ and Vink R: Recent patents in CNS
drug discovery: The management of inflammation in the central
nervous system. Recent Patents CNS Drug Discov. 4:86–95. 2009.
View Article : Google Scholar
|
|
14
|
Werner C and Engelhard K: Pathophysiology
of traumatic brain injury. Br J Anaesth. 99:4–9. 2007. View Article : Google Scholar : PubMed/NCBI
|