Introduction
As one of the leading causes of nasal respiratory
obstruction in childhood, adenoid hypertrophy affects ~3% of
children (1). The upper airway
obstruction caused by adenoid hypertrophy may seriously affect
maxillofacial and dental development (2). Besides that, nasal airway obstruction
caused by this disease may lead to a series of problems including
behavioral issues, night discomfort, daytime sleepiness and poor
school performance (1). Moreover,
adenoid hypertrophy is often combined with allergic rhinitis, which
in turn increases the difficulties in the treatment and prolongs
the duration of disease (3).
Allergic diseases are closely correlated with the incidence of
adenoid hypertrophy (4). Therefore,
the inhibition of allergic reaction may benefit the prevention and
treatment of adenoid hypertrophy.
As a receptor for cysteinyl leukotrienes, cysteinyl
leukotriene receptor 1 (CYSLTR1) has been reported to play
essential roles in mediating a variety of hypersensitivity and
allergic reactions (5). It has been
confirmed that the expression level of CYSLTR1 is abnormally
upregulated in adenoid tissue of patients with adenoid hypertrophy,
indicating the involvement of CYSLTR1 in the progression of this
disease (6). However, the mechanism
of the role of CYSLTR1 in adenoid hypertrophy remains unknown
yet.
In the present study, expression of CYSLTR1 in
adenoid tissue of patients with different degree of adenoid
hypertrophy was detected. The correlation between the expression
level of CYSLTR1 and clinical characteristics of patients were
analyzed. In addition, the interaction between CYSLTR1 and
extracellular signal-regulated kinase (ERK)1/2 was studied as
well.
Patients and methods
Patients
A total of 40 patients with adenoid hypertrophy were
selected during the period from January 2014 to January 2016 in
Children's Hospital of Hebei Province (Shijiazhuang, China). All
patients were diagnosed by symptoms including snoring, apnoea,
nasal, congestion, and so on. Nasopharyngeal obstruction was
detected using pharyngorhinoscopy or CT imagining. Patients with a
history of allergy or allergy-related diseases, such as allergic
rhinitis, were excluded from this study. There are 18 females and
22 males, and the age ranged from 4 to 8 years with an average age
of 5.9±0.9 years. The patients were divided into mild-moderate
group (<80% of the nasopharyngeal space had been occupied by the
hypertrophied adenoid) and severe group (>80% of the
nasopharyngeal space had been occupied by the hypertrophied
adenoid). The mild-moderate group included 10 females and 14 males,
and the age ranged from 4 to 8 years with an average age of 5.6±0.8
years. The severe group included 8 females and 8 males, and the age
ranged from 4 to 8 years with an average age of 6.1±0.8 years. At
the same time, a total of 20 children without adenoid hypertrophy
but needed surgical operations on adenoid due to other reasons were
also included as control group. The control group included 10
females and 10 males, and the age ranged from 4 to 8 years with an
average age of 6.9±1.1 years. Tissue was collected from adenoid
during surgical operations, and was immediately stored in liquid
nitrogen before use. All participants' parents signed informed
consent. The Ethics Committee of the Children's Hospital of Hebei
Province approved this study.
Cell culture and transfection
Primary human adenoid epithelial cells (HAECs) were
from the stock of our lab. This cell line was derived from a 6
years old child (male) who received adenoidectomy in our hospital.
Cells were cultured with NHS medium supplemented with 10% heat
inactivated horse serum (Biological Industries, Beit-Haemek,
Israel) in an incubator (37°C). Cells were cultured overnight to
reach 80–90% confluent before transfection. CysLTR1 siRNA (h)
(sc-43712) and control siRNA-A (sc-37007) were purchased from Santa
Cruz Biotechnology (Dallas, TX, USA). The vector overexpressing
CysLTR1 was constructed by inserting a EcoRI-EcoRI fragment
containing the full length DNA sequence of CysLTR1 into pIRSE2-EGFP
provided by Clontech (Palo Alto, CA, USA). Transfection was
performed using Lipofectamine 2000 transfection reagent (11668–019)
provided by Invitrogen (Thermo Fisher Scientific, Inc., Waltham,
MA, USA). All operations were performed in strict accordance with
the instructions provided by Invitrogen (Thermo Fisher Scientific,
Inc.).
Real-time quantitative PCR
Total RNA was extracted from adenoid tissue using
TRIzol reagent (Invitrogen; Thermo Fisher Scientific, Inc.).
NanoDrop™ 2000 Spectrophotometers (Thermo Fisher Scientific, Inc.,
Wilmington, DE, USA) was used to check the quality of all those RNA
samples, and only the samples with A260/A280 ratio between 1.8 and
2.0 were used. SuperScript III Reverse Transcriptase (Thermo Fisher
Scientific, Inc.) was used to carry out reverse transcription to
synthesize cDNA. PCR reaction system was prepared using
SYBR®-Green Real-Time PCR Master Mixes provided by
Thermo Fisher Scientific, Inc. The following primers were used:
CysLTR1 forward, 5′-TGACCGCTGCCTTTTTAGTC-3′ and reverse,
5′-AGGAGAGGGTCAAAGCAACA-3′; β-actin forward, GACCTCTATGCCAACACAGT
and reverse, AGTACTTGCGCTCAGGAGGA. PCR reaction conditions were:
95°C for 2 min, followed by 40 cycles of 95°C for 20 sec and 65°C
for 40 sec. Expression level of CysLTR1 was normalized to
endogenous control β-actin using 2−ΔΔCT method. PCR
reactions were performed in triplicates, and each RNA sample was
tested three times.
Western blot analysis
Peripheral blood (5 ml) was extracted from each
participant on the day of admission. Routine method was used to
extract total protein from adenoid tissue, whole blood and HAECs.
BCA method was used to test protein quality, followed by 10%
SDS-PAGE gel electrophoresis to separate different proteins.
Transmembrane was performed (20 V) to transfer protein to PVDF
membrane. Membranes were blocked with 5% skimmed milk, followed by
incubation with corresponding primary antibodies including rabbit
anti-p-ERK1/2 (Thr202/Tyr204) antibody (1:2,000; ab214362),
anti-ERK2 antibody (1:2,000; ab32081) and anti-GAPDH (1:1,000;
ab9845; all Abcam) overnight at 4°C. Then membranes were washed
with PBS, followed by incubating with IgG-HRP secondary antibody
(1:1,000; MBS435036; MyBioSource, San Diego, CA, USA) at room
temperature for 2 h. After washing with PBS, ECL method
(Sigma-Aldrich; Merck KGaA, Darmstadt, Germany) was used to detect
signals. Relative expression levels of ERK2 and p-ERK 1/2 were
normalized to endogenous control GAPDH using Image J software.
Statistical analysis
All statistical analyses were performed using SPSS
19.0 (SPSS Inc., USA). Comparison of normal distribution data (x ±
s) between two group were performed by t test, and comparisons
among multiple groups were performed by one-way analysis of
variance and LSD test. Comparisons of non-normal distribution data
were performed by non-parametric Mann-Whitney U test. P<0.05 was
considered to indicate a statistically significant difference.
Results
Expression of CYSLTR1 in adenoid
tissue and whole blood of patients with adenoid hypertrophy
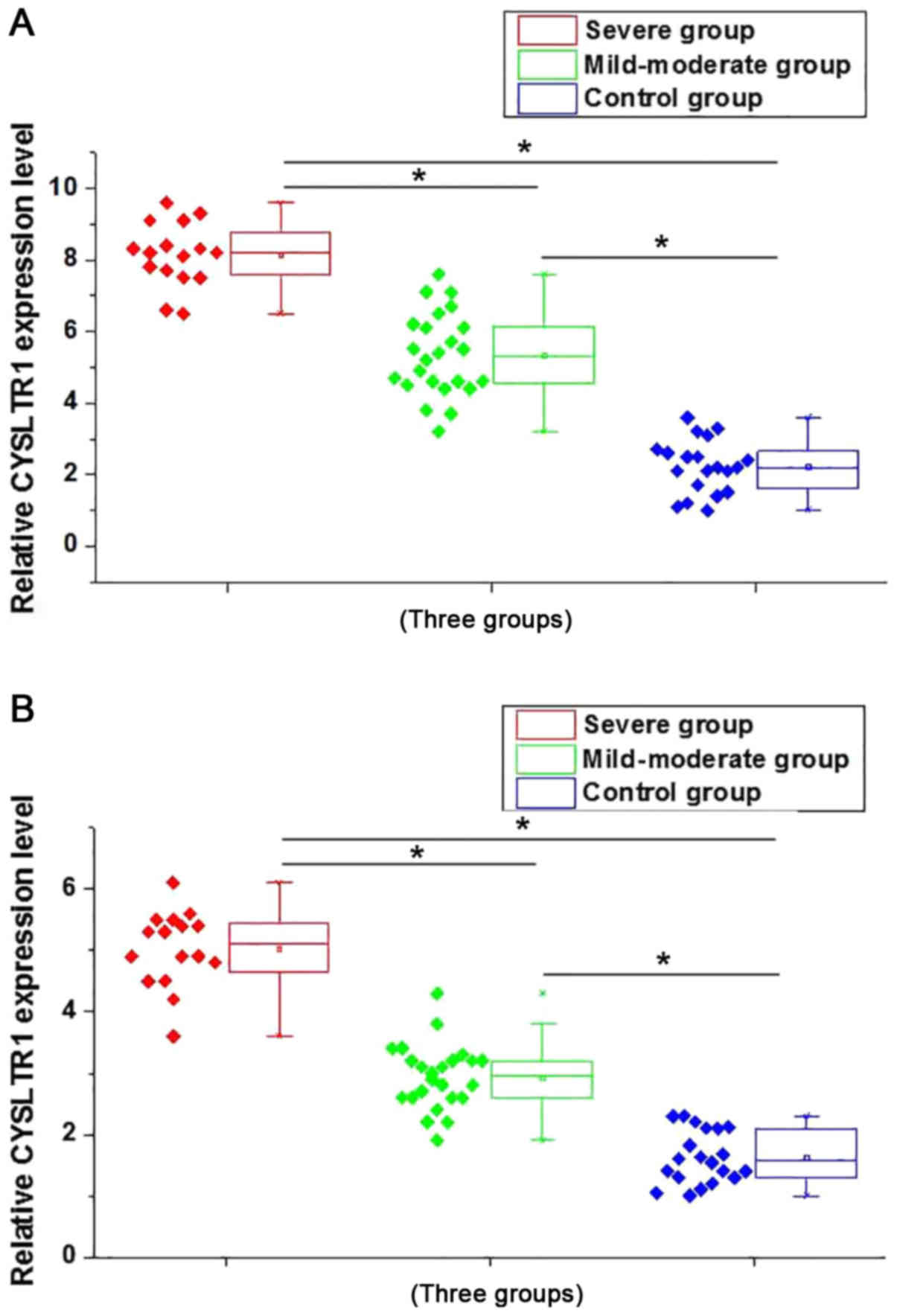
Expression of CYSLTR1 in adenoid tissue and whole
blood of patients with adenoid hypertrophy were detected by
qRT-PCR. As shown in Fig. 1A,
compared with control group, expression level of CYSLTR1 in adenoid
tissue of patients in mild-moderate group and severe group were
significant increased (P<0.05). Besides that, compared with
mild-moderate group, expression level of CYSLTR1 in adenoid tissue
was also significantly increased in patients of severe group
(P<0.05). Similar results were found in the expression of
CYSLTR1 in whole blood of patients in different groups. As shown in
Fig. 1B, highest expression level of
CYSLTR1 was found in severe group, followed by mild-moderate group
and control group (P<0.05). Those results suggest that CYSLTR1
is involved in the development of adenoid hypertrophy, and the
expression level of CYSLTR1 is positively correlated with the
severity of this disease.
Correlation between the expression
levels of CYSLTR1 and the pathological stages
Expression levels of CYSLTR1 in both adenoid tissue
and whole blood were divided into high expression group and low
expression group according to the median value of relative
expression level. Correlations between the expression levels of
CYSLTR1 in both adenoid tissue and whole blood and the clinical
data of patients including age, sex, and pathological stages were
analyzed. As shown in Tables I and
II, expression levels of CYSLTR1 in
adenoid tissue and whole blood showed no significant correlations
with age and sex, but showed significant correlations with the
severity of disease, and higher degree of severity was followed by
the higher expression level of CYSLTR1.
 | Table I.Correlation between the expression
level of CYSLTR1 in adenoid tissue and the clinical characteristics
of patients. |
Table I.
Correlation between the expression
level of CYSLTR1 in adenoid tissue and the clinical characteristics
of patients.
|
|
|
| CYSLT1
expression |
|
|---|
|
|
|
|
|
|
|---|
| Clinicopathological
features | Groups | Total | High | Low | P-value |
|---|
| Sex | Female | 18 | 9 | 9 | 0.77 |
|
| Male | 22 | 10 | 12 |
|
| Age (years) | >6 | 22 | 11 | 11 | 0.48 |
|
| ≤6 | 18 | 7 | 11 |
|
| Stage | Severe | 16 | 13 | 3 | <0.00001 |
|
| Mild-moderate | 24 | 2 | 22 |
|
| Table II.Correlation between the expression
level of CYSLTR1 in whole blood and the clinical characteristics of
patients. |
Table II.
Correlation between the expression
level of CYSLTR1 in whole blood and the clinical characteristics of
patients.
|
|
|
| CYSLT1
expression |
|
|---|
|
|
|
|
|
|
|---|
| Clinicopathological
features | Groups | Total | High | Low | P-value |
|---|
| Sex | Female | 18 | 11 | 7 | 0.90 |
|
| Male | 22 | 13 | 9 |
|
| Age (years) | >6 | 22 | 12 | 10 | 0.53 |
|
| ≤6 | 18 | 8 | 10 |
|
| Stage | Severe | 16 | 15 | 1 | <0.00001 |
|
| Mild-moderate | 24 | 2 | 22 |
|
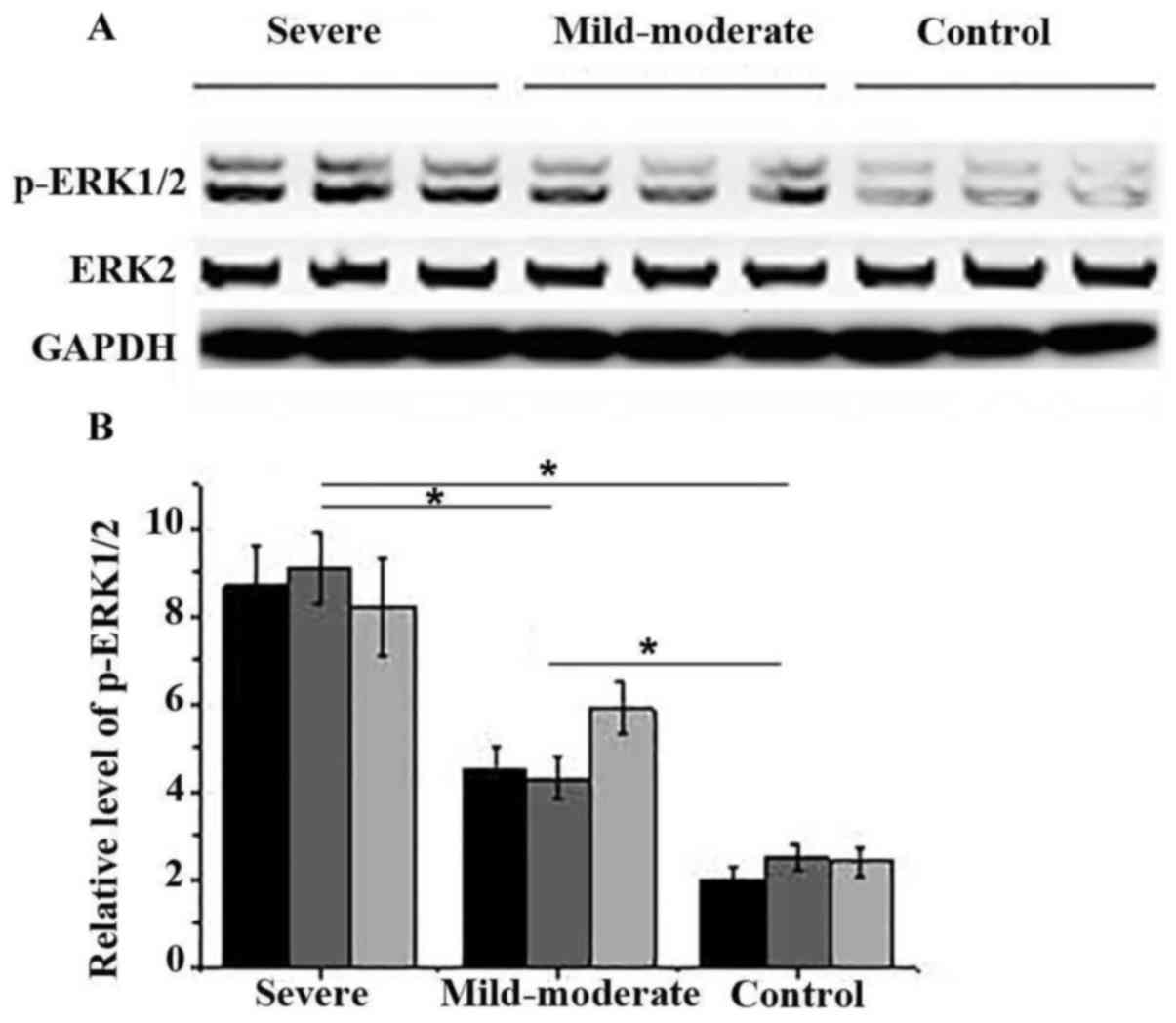
Effects of adenoid hypertrophy on the
activation of ERK1/2
The activation of ERK1/2 is involved in various
allergic reactions, which are the main causes of adenoid
hypertrophy. Therefore, the phosphorylation of in ERK1/2 in adenoid
tissue of three randomly selected participants was detected by
western blot. As shown in Fig. 2, no
significant differences in expression levels of ERK2 were found
between different groups of patients. However, levels of p-ERK1/2
were significantly higher in patients of severe group and
mild-moderate group than in control group (P<0.05). In addition,
compared with mild-moderate group, levels of p-ERK1/2 were also
significantly increased in patients of severe group (P<0.05).
Those data suggest that the activation of ERK1/2 is involved in the
development of adenoid hypertrophy and higher activation levels
indicate higher degree of severity.
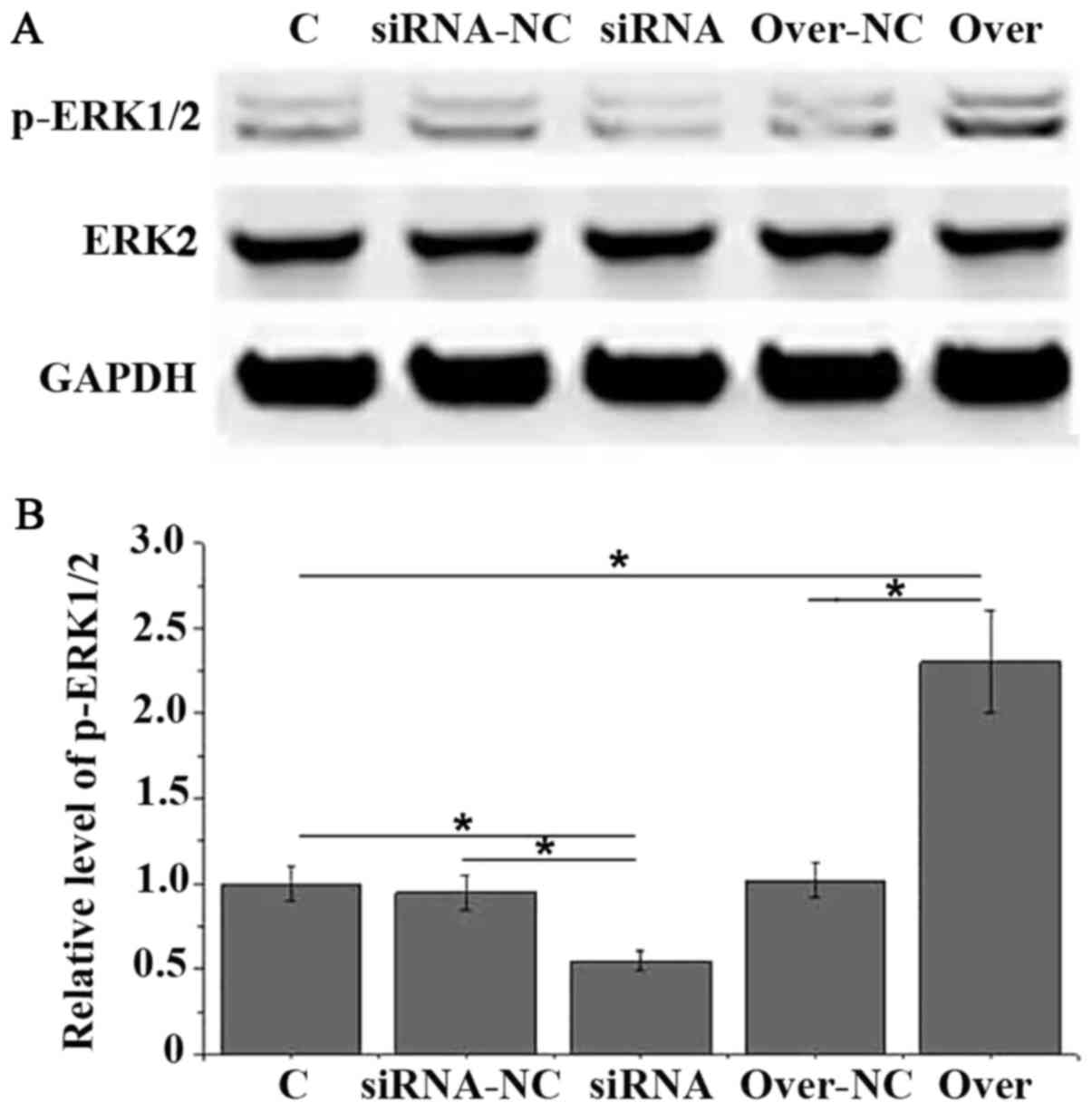
Effects of CYSLTR1 silencing and
overexpression on phosphorylation of ERK1/2 in HAECs
It is known that CYSLTR1 can interact with ERK1/2 to
perform its biological functions. In this study, CYSLTR1 was
silenced and overexpressed in HAECs. CYSLTR1 silencing was
confirmed by measuring the expression level of CYSLTR1by qRT-PCR
(data not show) to investigate the interactions between CYSLTR1 and
ERK1/2. As shown in Fig. 3, no
significant differences in expression levels of ERK2 were found
between different groups of cells. Compared with control group,
level of p-ERK1/2 was significant reduced in HAECs with CYSLTR1
silencing and significant increased in HAECs with CYSLTR1
overexpression (P<0.05). Those data suggest that CYSLTR1 can
regulate the activation of ERK1/2 to participate in the development
of adenoid hypertrophy.
Discussion
Allergic reactions were found to be highly
associated with the development of adenoid hypertrophy in both
children and adults, and ~60% of the patients show different
degrees of allergic manifestations (7). In another study, Huang and Giannoni
reported that sensitivity to mold allergens was a major risk factor
for adenoid hypertrophy in children with allergic rhinitis, which
prevents children from the exposure to molds bringing beneficial
effects to the prevention of adenoid hypertrophy (8). Cysteinyl leukotriene receptors
including CYSLTR1 play pivotal roles in mediating airway remodeling
caused by allergic reactions by binding to those cysteinyl
leukotrienes (9). The polymorphism
of CYSLTR1 was also found to be correlated with the
hypersensitivity to foods and drugs, such as aspirin (10). The involvement of CYSLTR1 in adenoid
hypertrophy still has not been well studied except one recent study
reporting that expression level of CYSLTR1 was significantly
increased in adenoid tissues of children with adenoid hypertrophy
compared with the healthy children (6). Concordant results were found in this
study. In this study, expression level of CYSLTR1 was found to be
significantly higher in the adenoid tissue and whole blood of
children with adenoid hypertrophy than in healthy control children.
In addition, expression level of CYSLTR1 was also higher in
patients with severe adenoid hypertrophy than in patients with
mild-moderate adenoid hypertrophy. There are possibly two different
resources of CYSLTR1 in blood. It is known that blood leukocytes
can express CYSLTR1 (11).
Circulating CYSLTR1 may also exist in blood. However, this
uncertainty may not affect our conclusions. Besides that,
expression level of CYSLTR1 in adenoid tissue and whole blood of
children with adenoid hypertrophy showed no significant
correlations with age and sex, but it was significantly correlated
with the severity of disease. Those results suggest that CYSLTR1 is
involved in the development of adenoid hypertrophy and expression
level of CYSLTR1 is positively correlated with the severity of the
disease.
As two related protein-serine/threonine kinases,
ERK1 and ERK2, or ERK1/2 are two key players in Ras-Raf-MEK-ERK
signal transduction cascade, which has been confirmed to be with
pivotal roles in the regulation of various biological processes
including cell survival, migration, adhesion, proliferation,
differentiation and metabolism, and cell cycle progression
(12). Recent studies have also
shown that the activation of ERK1/2 also has important functions in
allergic responses and the inhibition of ERK1/2 activation can help
reduce allergic inflammation (13).
In the study of allergen-induced lung inflammation, Chen et
al reported that downregulation of ERK1/2 could inhibit the
development of bronchial asthma by reducing inflammatory responses
(14). In another study, ERK1/2
kinase inhibition was found to be able to attenuate Th2 immune
response induced by allergens in mouse model (15). Based on our knowledge, the
involvement of ERK1/2 kinase in the development of adenoid
hypertrophy still has not yet been reported. In our study, no
significant differences in expression of ERK2 were found between
different groups. However, the level of p-ERK1/2 was significantly
higher in patients with adenoid hypertrophy than in healthy
children. In addition, the level of p-ERK1/2 was also significantly
higher in severe group than in mild-moderate group. Those data
suggest that the activation of p-ERK1/2 is involved in the
progression of adenoid hypertrophy.
It has been reported that the biological functions
of CYSLTR1 in allergic responses is closely related to the
activation of ERK1/2 signaling pathway (16). In the present study, HAECs with
CYSLTR1 overexpression and knockdown were constructed to
investigate the interactions between CYSLTR1 and ERK1/2. No
significant differences in the expression level of ERK2 were found
among different groups of cells, but the level of p-ERK1/2 was
found to be significantly higher in HAECs with CYSLTR1
overexpression compared with control cells. In contrast, level of
p-ERK1/2 was significantly decreased in HAECs with CYSLTR1
knockdown. Those results suggest that CYSLTR1 has no effects on the
expression level of ERK2, but CYSLTR1 expression can induce the
activation of ERK1/2 through phosphorylation, so as to increase
allergic reaction and promote the development of adenoid
hypertrophy.
In conclusion, expression level of CYSLTR1 is
positively correlated with the progression of adenoid hypertrophy.
CYSLTR1 expression can induce the activation of ERK1/2 to
contribute to the development of adenoid hypertrophy. This study
provided the basis for future studies, which aim to investigate the
clinical value of CYSLTR1 in the treatment of adenoid hypertrophy.
Although this study has the unavoidable limitation of small sample
size, the results are representative and convincing. Future studies
with bigger sample size will further confirm the conclusions that
are made in the present study.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
WG and SA designed experiments; WG and JL performed
experiments, WG, JL and QL analyzed data; SA wrote the manuscript;
all authors read the manuscript.
Ethics approval and consent to
participate
The Ethics Committee of the Children's Hospital of
Hebei Province approved this study. All participants' parents
signed informed consent for their inclusion within the study.
Consent for publication
All participants' parents signed informed consent
for the publication of their child's data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Koca CF, Erdem T and Bayındır T: The
effect of adenoid hypertrophy on maxillofacial development: An
objective photographic analysis. J Otolaryngol Head Neck Surg.
45:482016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Raffat A and ul Hamid W: Cephalometric
assessment of patients with adenoidal faces. J Pak Med Assoc.
59:747–752. 2009.PubMed/NCBI
|
|
3
|
Liu W, Zhou L, Zeng Q and Luo R:
Combination of mometasone furoate and oxymetazoline for the
treatment of adenoid hypertrophy concomitant with allergic
rhinitis: A randomized controlled trial. Sci Rep. 7:404252017.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Evcimik MF, Dogru M, Cirik AA and Nepesov
MI: Adenoid hypertrophy in children with allergic disease and
influential factors. Int J Pediatr Otorhinolaryngol. 79:694–697.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Honda T and Kabashima K: Leukotrienes as
key mediators and amplifiers in allergic inflammation: Insights
from the bench and clinic. Exp Dermatol. 23:95–96. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhu MH, Liang M, Wang ZJ, Shen Y, Wen HY,
Zhai JM and Yang XB: Expression of CysLTR-1 and CysLTR-2 in adenoid
tissues from children with adenoid hypertrophy. Zhongguo Dang Dai
Er Ke Za Zhi. 17:159–163. 2015.(In Chinese). PubMed/NCBI
|
|
7
|
Al-juboori AN, Fadhil A and Sahib N:
Adenoid hypertrophy in adult patients and its relation with
allergy. Eur Sci J. 10:481–487. 2014.
|
|
8
|
Huang SW and Giannoni C: The risk of
adenoid hypertrophy in children with allergic rhinitis. Ann Allergy
Asthma Immunol. 87:350–355. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Henderson WR Jr, Chiang GK, Tien YT and
Chi EY: Reversal of allergen-induced airway remodeling by CysLT1
receptor blockade. Am J Respir Crit Care Med. 173:718–728. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kim SH, Ye YM, Hur GY, Lee SK, Sampson AP,
Lee HY and Park HS: CysLTR1 promoter polymorphism and requirement
for leukotriene receptor antagonist in aspirin-intolerant asthma
patients. Pharmacogenomics. 8:1143–1150. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Roskoski R Jr: ERK1/2 MAP kinases:
Structure, function, and regulation. Pharmacol Res. 66:105–143.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Figueroa DJ, Breyer RM, Defoe SK, Kargman
S, Daugherty BL, Waldburger K, Liu Q, Clements M, Zeng Z, O'Neill
GP, et al: Expression of the cysteinyl leukotriene 1 receptor in
normal human lung and peripheral blood leukocytes. Am J Respir Crit
Care Med. 163:226–233. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
El-Hashim AZ, Renno WM, Raghupathy R,
Abduo HT, Akhtar S and Benter IF: Angiotensin-(1–7) inhibits
allergic inflammation, via the MAS1 receptor, through suppression
of ERK1/2- and NF-κB-dependent pathways. Br J Pharmacol.
166:1964–1976. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chen H, Xu X, Teng J, Cheng S, Bunjhoo H,
Cao Y, Liu J, Xie J, Wang C, Xu Y and Xiong W: CXCR4 inhibitor
attenuates allergen-induced lung inflammation by down-regulating
MMP-9 and ERK1/2. Int J Clin Exp Pathol. 8:6700–6707.
2015.PubMed/NCBI
|
|
15
|
Saw S and Arora N: PI3K and ERK1/2 kinase
inhibition potentiate protease inhibitor to attenuate allergen
induced Th2 immune response in mouse. Eur J Pharmacol. 776:176–184.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Paulucci BP, Pereira J, Picciarelli P,
Levy D and Di Francesco RC: Expression of cysteinyl leukotriene
receptor 1 and 2 (CysLTR1 and CysLTR2) in the lymphocytes of
hyperplastic tonsils: Comparison between allergic and nonallergic
snoring children. Int Forum Allergy Rhinol. 6:1151–1158. 2016.
View Article : Google Scholar : PubMed/NCBI
|