Introduction
An accessory middle cerebral artery (AMCA) is a
relatively uncommon anomaly of the middle cerebral artery (MCA) in
which the AMCA arises from the anterior cerebral artery (ACA) that
coexists with the main trunk of the MCA (1,2). The
angiographic incidence of AMCA is 0.32% (3). Anatomically, an AMCA mainly acts as
collateral circulation for the MCA. Similar to other intracranial
vessels, the AMCA is involved in many diseases, such as aneurysms
and cerebral infarction (4–6). Although arteriovenous malformations
(AVMs) can theoretically occur in an AMCA, this finding is
extremely rare (7). Most AVMs drain
through the veins of the brain, and the drainage vein has, in some
patients, been found to be enlarged or stenosed or to exhibit
tortuousness (8). However, AVMs
accompanied by developmental venous anomalies (DVAs) are rare, and
only approximately 20 relevant articles have been published in the
literature to date (7). A DVA is a
benign and mostly silent condition without clinical symptoms
(9). However, when a DVA merges with
an AVM, due to the high blood flow in the AVM, drainage of blood
from the DVA is difficult, resulting in drainage resistance. This
feature creates complications within the AVM and makes DVAs prone
to bleeding (10). Cases in which an
AMCA was accompanied by an AVM and a DVA are rarely reported.
However, the treatment of one such case is reported in this paper,
and the relevant literature is reviewed.
Case report
A 47-year-old woman was admitted due to a headache
accompanied by nausea and vomiting for 1 h. The patient had always
been healthy without any history of hypertension or diabetes. This
disease was not induced by any other condition. The patient
developed a sudden and severe headache at rest and subsequently
developed nausea and vomiting accompanied by the inability to use
her right limb and dysphasia. The patient was admitted to our
hospital after symptom onset. At the time of presentation, the
patient was alert with no seizure. An admission examination showed
the following. The patient was alert but exhibited incomplete motor
aphasia. The left limbs moved freely, while the right limbs were
reflexive (muscle strength grade III). The Babinski sign was
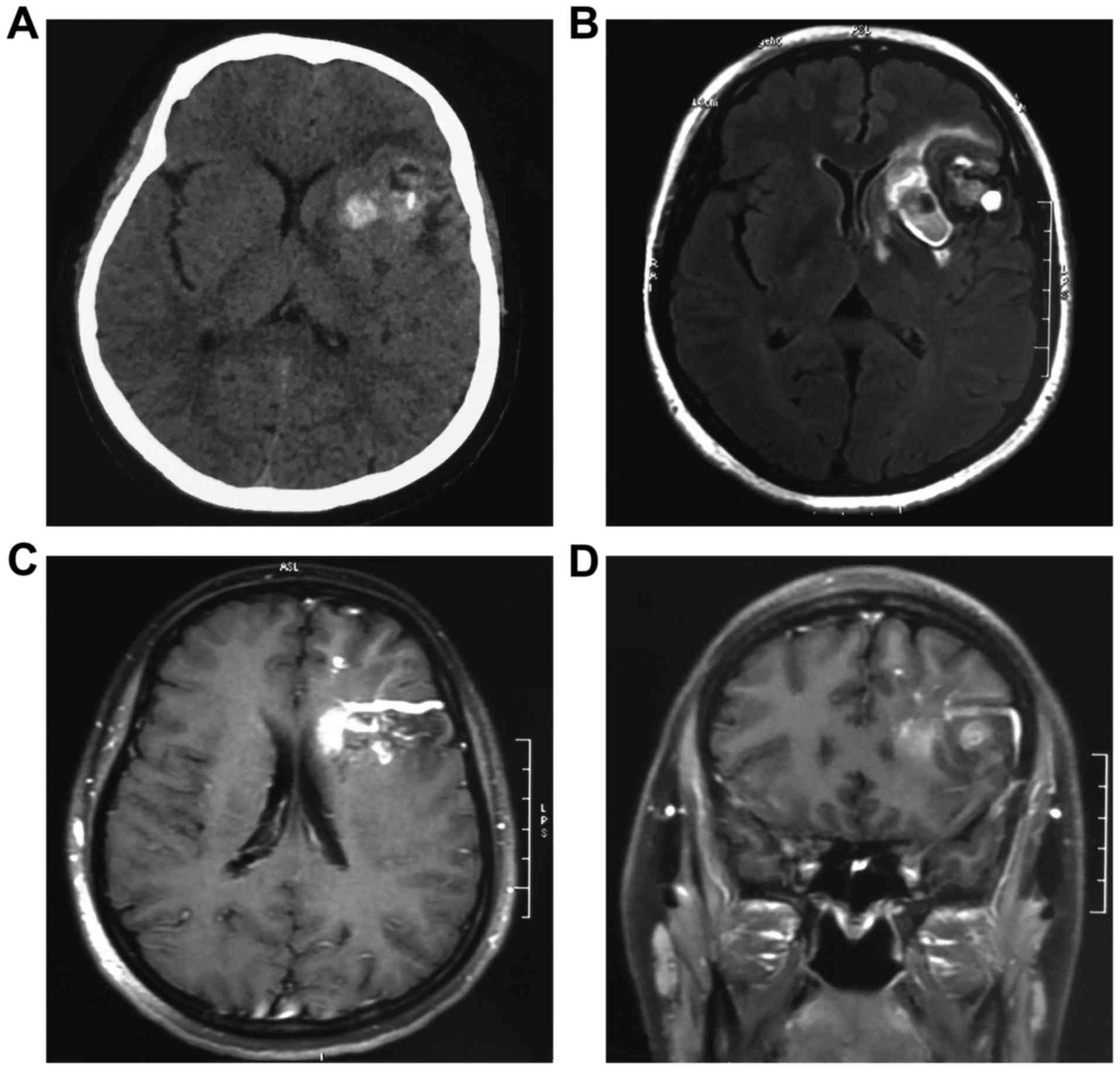
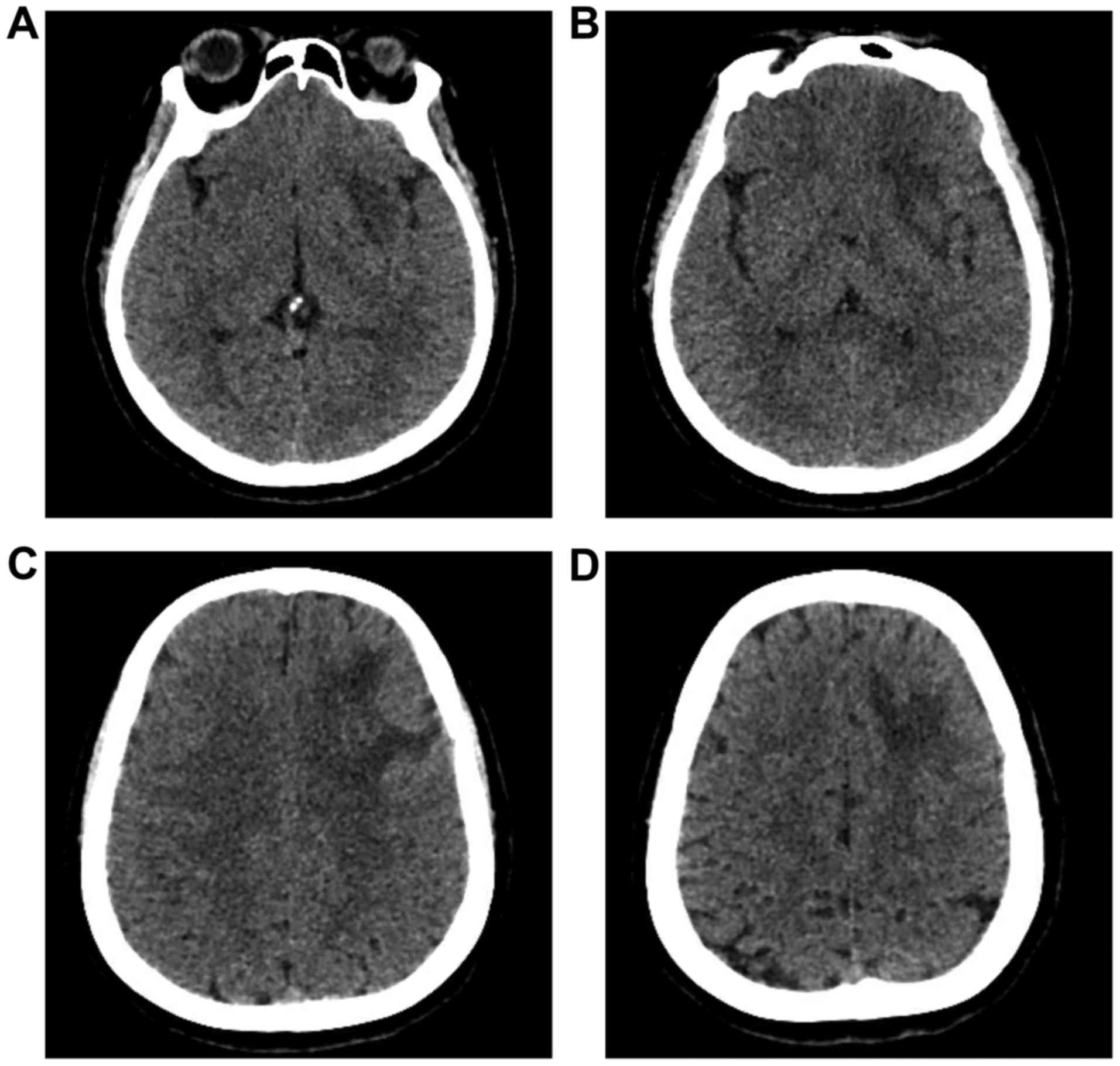
positive in the right lower limb. A head CT and MRI after admission
showed lesions in the left Sylvian fissure and insular lobe. CT
showed high and slightly high mixed densities. The signals were
confounding on MRI. An abnormally thickened vein extended from the
brain surface to the deep lesions (Fig.
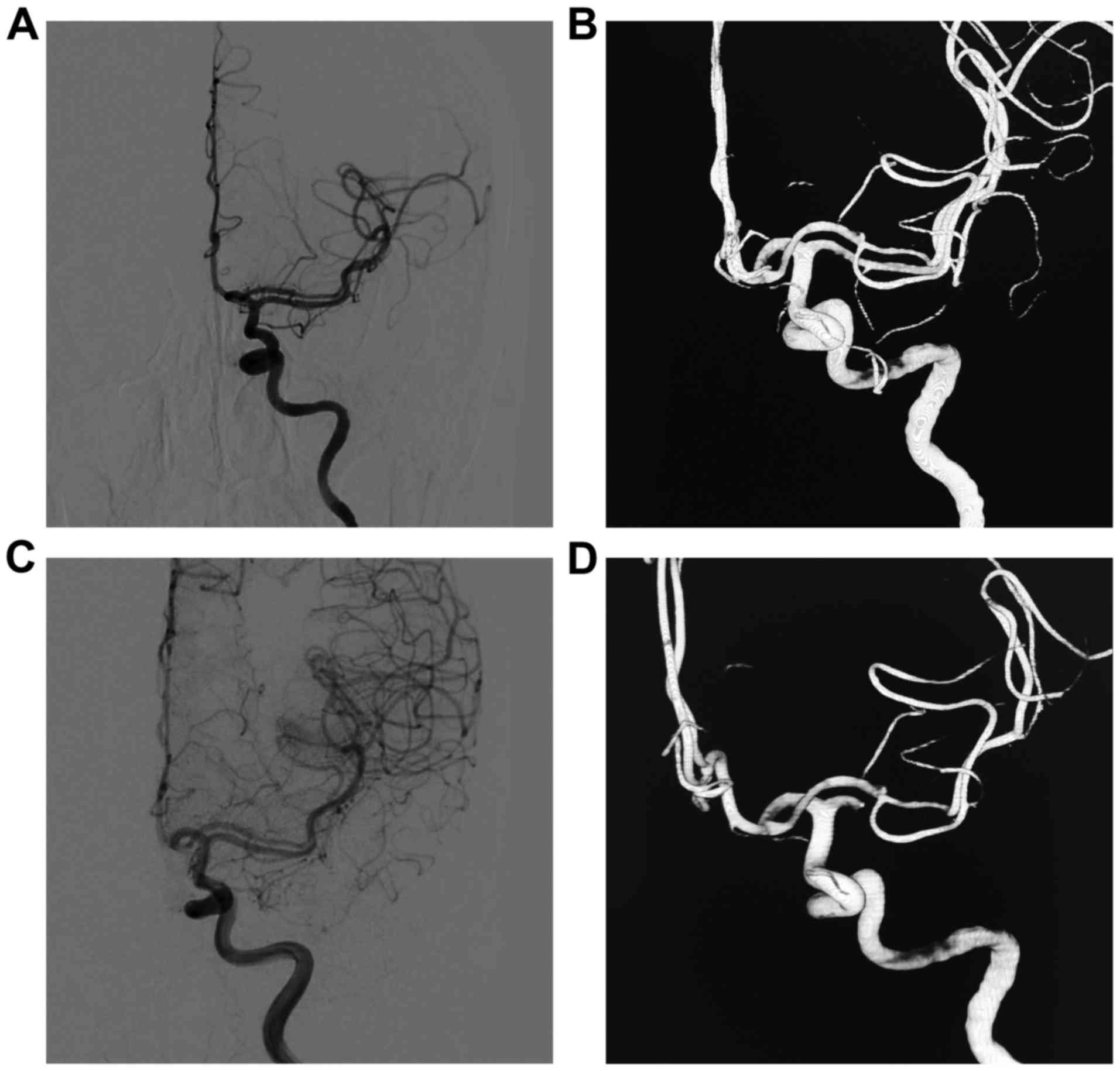
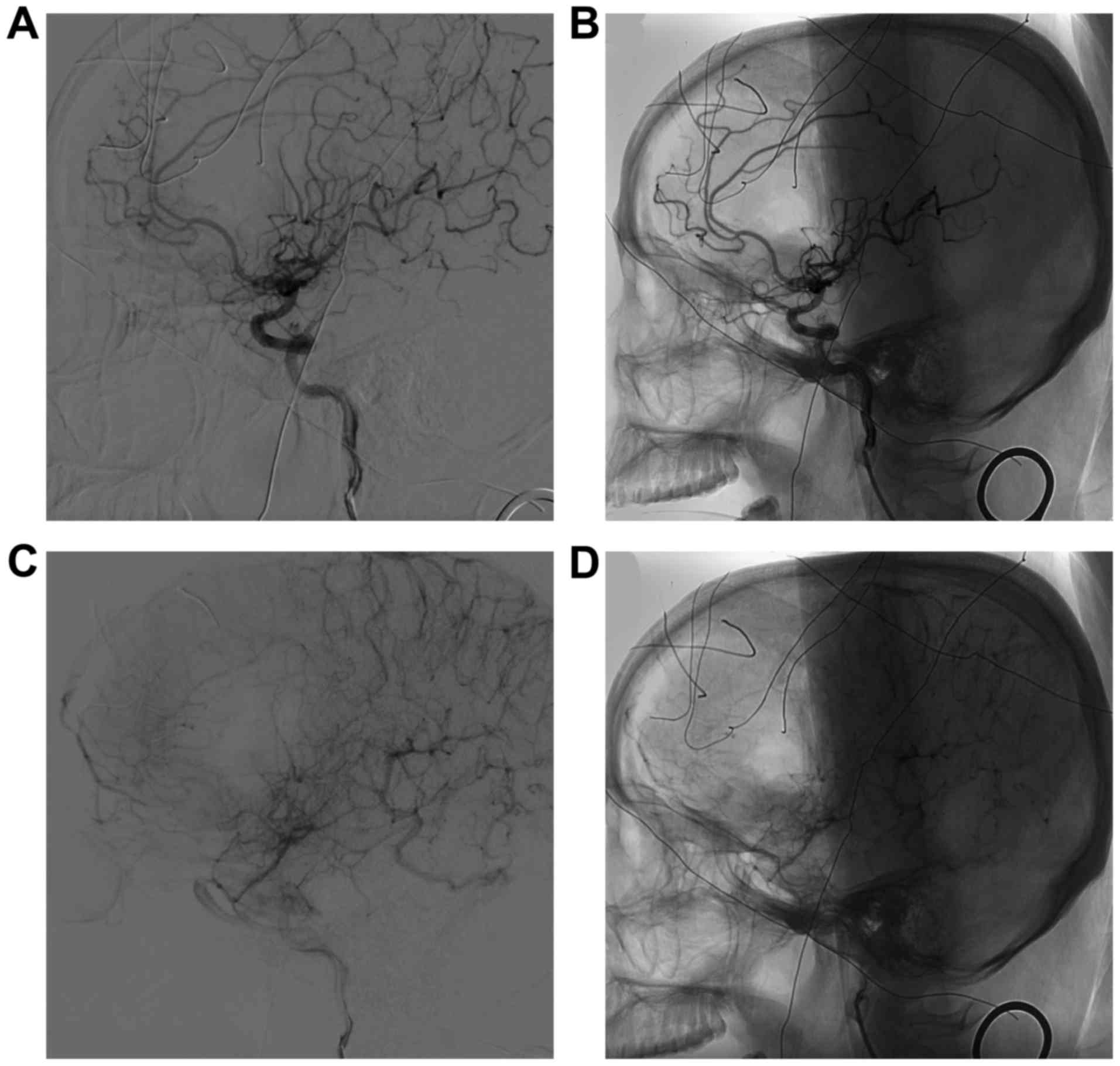
1). Further DSA revealed a vascular malformation in the left
MCA and an AMCA that originated from the anterior communicating
artery (Fig. 2A and B). The vascular
malformation in the AMCA was seen in the deep Sylvian fissure
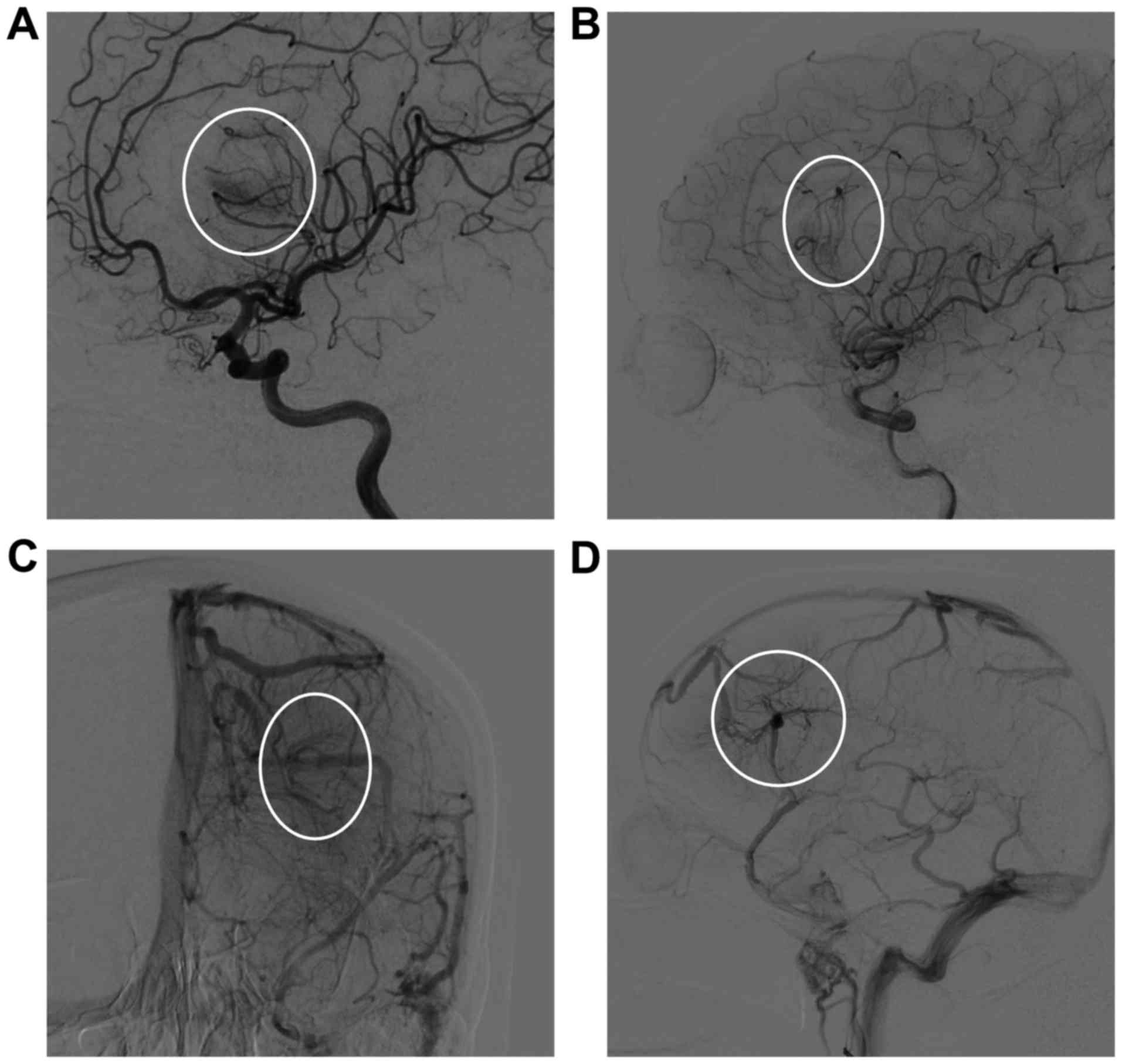
(Fig. 2C and D). The vascular
malformation was diffuse, and a small number of fine branching
arteries served as its blood supply. It drained into the DVA
(Fig. 3). The patient was diagnosed
with a left frontal hemorrhage with an AMCA that merged with an AVM
and a DVA. AVM resection was scheduled to be performed in a hybrid
operating room.
Surgical treatment was performed in a hybrid
operating room. Femoral artery puncture was performed, and an
arterial sheath was inserted. A left expanded pterional approach
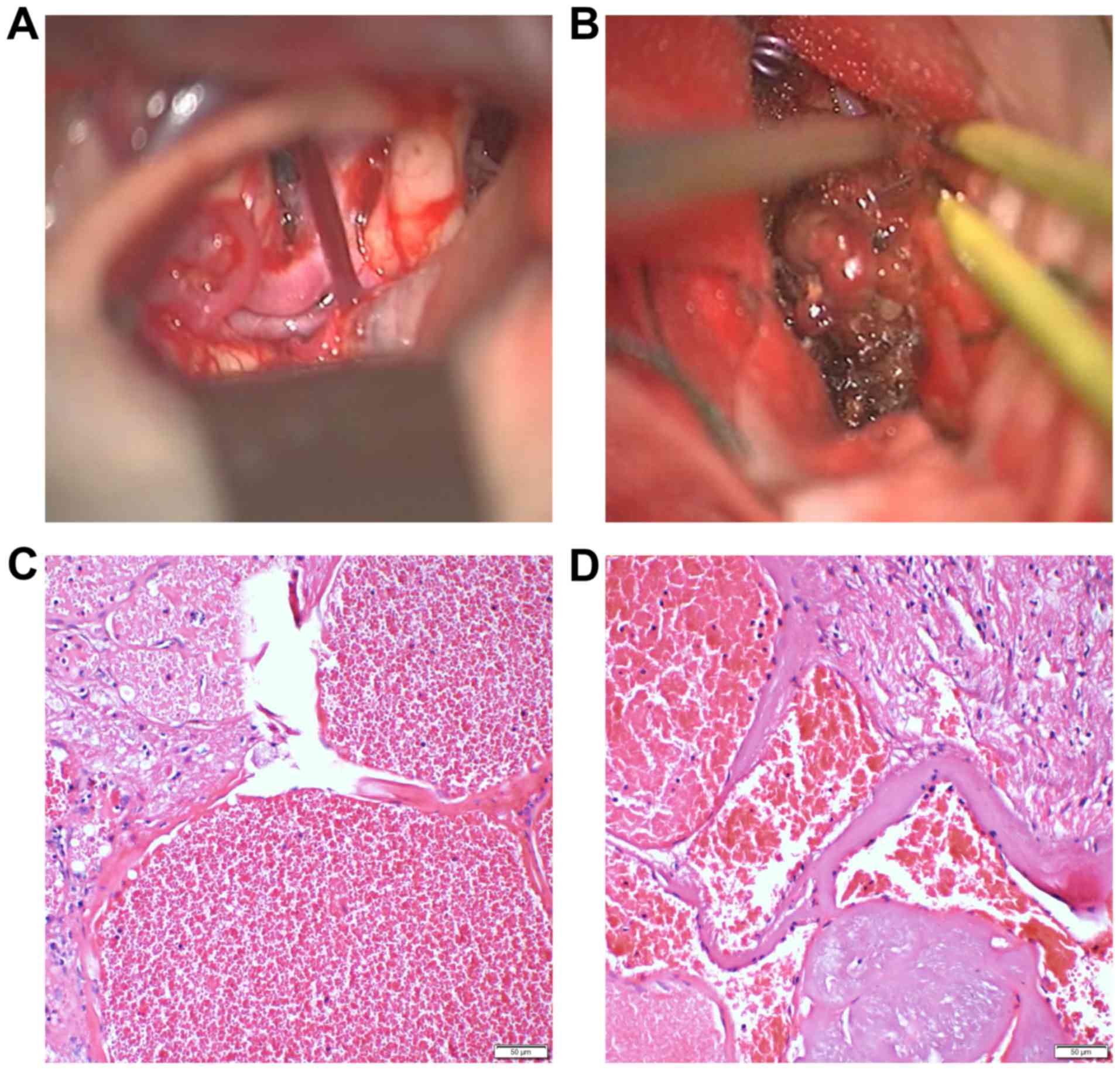
was adopted during surgery. The AMCA originating from the anterior
communicating artery could be seen at the chiasmatic cistern after
the Sylvian fissure on the left side was opened (Fig. 4A). The AVM was located on the surface
of the insular lobe of the deep Sylvian fissure. The major feeding
artery of the AVM, which originated from the AMCA, was clipped. The
AVM and the DVA were subsequently removed from the AVM, which
resulted in obsolete hemorrhage in the AVM. The AVM was diffuse,
and the venous end drained into the DVA (Fig. 4B). The final pathological examination
after removal showed an irregular vascular shape that consisted of
various types of expanded and transparent veins and abnormal
muscularized arteries. An abnormal arteriovenous anastomosis was
also observed along with brain tissues between vessels and was
diagnosed as an AVM (Fig. 4C and D).
DSA was performed after AVM resection, which showed that the AVM
and DVA were completely removed (Fig.
5). The patient recovered well within one week of the surgery.
A one-month follow-up CT scan showed good recovery in the brain
tissue (Fig. 6). The patient was in
good condition, had grade IV muscle strength in the right limb, and
could take care of herself.
Discussion
In 1973, Teal et al (11) proposed using the term ‘AMCA’ to
describe an anomalous artery arising from the ACA. The origin of an
AMCA can be the proximal or distal ACA, and the vessel that arises
from the ACA then runs in the Sylvian fissure along with the main
trunk of the MCA to supply part of the MCA territory (11,12). The
angiographic incidence of AMCA is 0.32% (3). Manelfe et al (13) classified AMCA into three types: Type
1 is an anomalous vessel that arises from the internal carotid
artery at a point proximal to its bifurcation (the duplicated MCA
in Teal's classification), type 2 originates from the proximal
portion of the ACA, and type 3 originates from the distal portion
of the first segment of the ACA (A1) near the anterior
communicating artery (14). The AMCA
in this patient originated from the anterior communicating artery
and was classified as Manelfe type 3. Typically, an AMCA serves as
the collateral blood supply to the MCA territory. However, the
clinical significance of AMCAs remains obscure (15).
Similar to normal MCAs, AMCAs can also be associated
with many diseases, such as intracranial aneurysms (4), cerebral infarction (5), and moyamoya disease (6). However, an AMCA combined with an AVM is
very rare, especially with the vein of the AVM draining into the
DVA, as in this case. Due to differences in the development of the
AMCA, such arteries can vary in diameter (16), and there are large differences in the
feeding area distribution of its arteries (17). For example, when the blood supply to
the AMCA is extensive, the consequences are more severe if the AMCA
undergoes an acute infarction (5,18).
Moreover, when the ACMA is large with abundant blood flow, the
artery is also prone to aneurysms (19,20).
Therefore, the development of an AMCA may be associated with
diseases. Although an AVM combined with an AMCA is relatively rare,
we report such a case in this article.
AVMs are a type of congenital cerebrovascular
condition which, along with capillary telangiectasia, cavernous
malformation, and DVA, represent the 4 most commonly recognized
subgroups of cerebrovascular malformations (21). An AVM is a collection of arteries and
veins that form without an intervening capillary bed (22). However, a DVA is usually a collection
of radiating veins that converge on a large and centrally located
draining vein (23). This is
classically described as having a fan-shaped ‘caput medusae’
appearance, according to a large prospective autopsy series, DVA is
the most common type of vascular malformation in the brain. It is
now accepted that DVA generally follow a benign clinical course
(24).
Therefore, during embryonic development, an AVM and
a DVA may occur on an AMCA, as is the case in the patient described
in this paper. It is possible that the AVM formed first, and then
venous hypertension around the draining vein occurred, and the
disturbed normal venous drainage due to venous hypertension caused
by preexisting arteriovenous shunting may have promoted the
development of a DVA (25). The
first patient with a coexisting AVM and DVA was reported by Huang
et al (26) in 1984, and a
literature review of 22 cases was published by Zhang et al
(7) in 2017. However, no reports
have described an AVM accompanied by both a DVA and an AMCA.
When an AVM is accompanied by a DVA, the risk of
hemorrhage is as high as 68%, and these patients are more prone to
bleeding than are those with a single AVM (38%) (7). This finding may be related to the
tenuous and slow-adapting terminal angioarchitecture that could
lead to suboptimal venous drainage in the DVA (27,28).
Therefore, patients with both an AVM and a DVA must be treated when
rupture and bleeding occur. Microsurgical resection is an effective
method for treating a ruptured AVM, especially when the AVM is
shallow and is located in a non-relocating area (29). Whether the DVA needs to be removed
during AVM resection must be determined. Despite the risk imposed
by the aberrant drainage, successful neurosurgical management of
these transitional lesions should target the AVM and retain a
tissue-dependent DVA with low hemorrhagic risk. This prevents the
DVA from draining normal brain tissue after removal and prevents
catastrophic venous infarction (7).
The patient described in our paper had a diffusely
developed AVM with unclear boundaries. We found bulky veins in the
DVA, and the AVM around the DVA was gradually removed.
Intraoperative DSA showed that the AVM was completely removed, and
the DVA was not visible. We adopted a hybrid operation procedure
for this patient because it ensured the complete clearance of the
AVM. Intraoperative DSA can also be performed to accurately
determine the position of the AVM (30,31). No
serious complications occurred after the operation, and the
patient's physical activity gradually recovered. However, a
one-month postoperative follow-up CT scan showed that cerebral
edema persisted, and this may have be related to the removal of the
DVA during the operation.
In addition to microsurgical resection of AVMs and
DVAs, radiosurgery, embolization and combination therapy are
effective treatments (7). In 2017,
Zhang et al (7) reviewed 22
cases of coexisting AVMs and DVAs. Of these, stereotactic
radiosurgery was performed in 7 cases, embolization was performed
in 6 cases, surgical resection was performed in 4 cases, and
multimodal therapy was performed in 5 cases. AVMs were treated by
targeted embolization, and the DVAs were carefully preserved
(32). When an AVM is accompanied by
a DVA and no evidence of bleeding is present, radiotherapy is also
an effective treatment. Aksoy et al (10) performed radiosurgery in a patient
with both an AVM and a DVA and reported a good patient outcome at
the 6-month follow-up evaluation. However, as the effect of
radiation is generally delayed until 2–4 years, whether the patient
remained well at a longer-term follow-up is unclear (10). Nevertheless, it is important to note
that only the AVM should be obliterated by radiosurgery, whereas
the DVA should be completely preserved (9).
Therefore, as reported in this rare case, AVMs can
be found in an AMCA and can also be simultaneously observed with a
DVA. Hybrid surgical treatment can be used to remove AVMs, and this
approach can improve the patient's prognosis.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
KL analysed the patient data and wrote the initial
draft. YG, LQ and BX collected the images of the patients and
analyzed the literature. JY and KX were the surgeons who treated
the patient. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the First Hospital of Jilin University and written
informed consent form was obtained from the patients. All
procedures performed were in accordance with the ethical standards
of the institutional and/or national research committee and with
the 1964 Helsinki declaration and its later amendments or
comparable ethical standards.
Patient consent for publication
Not applicable.
Competing interests
The authors have declared that they have no
competing interests.
References
|
1
|
Fujiwara K, Saito K and Ebina T: Saccular
aneurysm of the accessory middle cerebral artery-case report.
Neurol Med Chir (Tokyo). 43:31–34. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Uchiyama N: Anomalies of the middle
cerebral artery. Neurol Med Chir (Tokyo). 57:261–266. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Watanabe T and Togo M: Accessory middle
cerebral artery. Report of four cases. J Neurosurg. 41:248–251.
1974. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lee CC, Liu ZH, Jung SM and Yang TC:
Ruptured aneurysm of the accessory middle cerebral artery
associated with moyamoya disease: A case report. Chang Gung Med J.
34:541–547. 2011.PubMed/NCBI
|
|
5
|
Hiramatsu Y, Wakita M, Matsuoka H, Kasuya
J, Hamada R and Takashima H: Cerebral infarction associated with
accessory middle cerebral arteries: Two case reports. Intern Med.
53:1381–1384. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Komiyama M and Yasui T: Accessory middle
cerebral artery and moyamoya disease. J Neurol Neurosurg
Psychiatry. 71:129–130. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang M, Connolly ID, Teo MK, Yang G, Dodd
R, Marks M, Zuccarello M and Steinberg GK: Management of
arteriovenous malformations associated with developmental venous
anomalies: A literature review and report of 2 cases. World
Neurosurg. 106:563–569. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kurita H, Shin M, Ueki K, Kawamoto S and
Kirino T: Congestive brain oedema associated with a pial
arteriovenous malformation with impaired venous drainage. Acta
Neurochir (Wien). 143:339–342. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kurita H, Sasaki T, Tago M, Kaneko Y and
Kirino T: Successful radiosurgical treatment of arteriovenous
malformation accompanied by venous malformation. AJNR Am J
Neuroradiol. 20:482–485. 1999.PubMed/NCBI
|
|
10
|
Aksoy FG, Gomori JM and Tuchner Z:
Association of intracerebral venous angioma and true arteriovenous
malformation: A rare, distinct entity. Neuroradiology. 42:455–457.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Teal JS, Rumbaugh CL, Bergeron RT and
Segall HD: Anomalies of the middle cerebral artery: Accessory
artery, duplication and early bifurcation. Am J Roentgenol Radium
Ther Nucl Med. 118:567–575. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Komiyama M, Nakajima H, Nishikawa M and
Yasui T: Middle cerebral artery variations: Duplicated and
accessory arteries. AJNR Am J Neuroradiol. 19:45–49.
1998.PubMed/NCBI
|
|
13
|
Manelfe C, David J and Rascol A: L'artère
cérébrale moyenne accessoire. A propos de 17 casSociété Française
de Neuroradiologie. Paris: 1975, (In French).
|
|
14
|
Abanou A, Lasjaunias P, Manelfe C and
Lopez-Ibor L: The accessory middle cerebral artery (AMCA).
Diagnostic and therapeutic consequences. Anatom Clin. 6:305–309.
1984. View Article : Google Scholar
|
|
15
|
Komiyama M, Nishikawa M and Yasui T: The
accessory middle cerebral artery as a collateral blood supply. AJNR
Am J Neuroradiol. 18:587–590. 1997.PubMed/NCBI
|
|
16
|
Reis CV, Zabramski JM, Safavi-Abbasi S,
Hanel RA, Deshmukh P and Preul MC: The accessory middle cerebral
artery: Anatomic report. Neurosurgery. 63 1 Suppl 1:ONS10–ONS14.
2008.PubMed/NCBI
|
|
17
|
Takahashi M, Uchino A and Suzuki C:
Anastomosis between accessory middle cerebral artery and middle
cerebral artery diagnosed by magnetic resonance angiography. Surg
Radiol Anat. 39:685–687. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liu ZS, Zhou LJ, Sun Y, Kuang XW, Wang W
and Li C: Sufficient collateral blood supply from accessory middle
cerebral artery in a patient with acute ischemic stroke. Interv
Neuroradiol. 21:215–217. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Teramoto S, Tokugawa J, Nakao Y and
Yamamoto T: Caudate haemorrhage caused by pseudoaneurysm of
accessory middle cerebral artery. BMJ Case Rep. 2015:pii:
bcr2015213335. 2015.PubMed/NCBI
|
|
20
|
Parthasarathy R, Goel G, Gupta V, Narang
KS, Anand S and Jha AN: Endovascular glue embolization of
dissecting aneurysm of type-3 accessory middle cerebral artery: A
contralateral approach. Interv Neuroradiol. 21:664–668. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
McCormick WF: The pathology of vascular
‘arteriovenous’ malformations. J Neurosurg. 24:807–816. 1966.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chen W, Choi EJ, McDougall CM and Su H:
Brain arteriovenous malformation modeling, pathogenesis, and novel
therapeutic targets. Transl Stroke Res. 5:316–329. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Brinjikji W, El-Masri AE, Wald JT,
Flemming KD and Lanzino G: Prevalence of cerebral cavernous
malformations associated with developmental venous anomalies
increases with age. Childs Nerv Syst. 33:1539–1543. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sarwar M and McCormick WF: Intracerebral
venous angioma. Case report and review. Arch Neurol. 35:323–325.
1978. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Yanaka K, Hyodo A and Nose T: Venous
malformation serving as the draining vein of an adjoining
arteriovenous malformation. Case report and review of the
literature. Surg Neurol. 56:170–174. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Huang Y, Robbins A, Patel S and Chaudhary
M: Cerebral venous malformations and a new classification of
cerebral malformations. The cerebdral venous system and its
disorders. 373–474. 1984.
|
|
27
|
da Costa L, Wallace MC, Ter Brugge KG,
O'Kelly C, Willinsky RA and Tymianski M: The natural history and
predictive features of hemorrhage from brain arteriovenous
malformations. Stroke. 40:100–105. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Shakur SF, Liesse K, Amin-Hanjani S,
Carlson AP, Aletich VA, Charbel FT and Alaraj A: Relationship of
cerebral arteriovenous malformation hemodynamics to clinical
presentation, angioarchitectural features and hemorrhage.
Neurosurgery. 63 Suppl 1:S136–S140. 2016. View Article : Google Scholar
|
|
29
|
Magro E, Gentric JC, Batista AL, Kotowski
M, Chaalala C, Roberge D, Weill A, Stapf C, Roy D, Bojanowski MW,
et al: The treatment of brain AVMs Study (TOBAS): An all-inclusive
framework to integrate clinical care and research. J Neurosurg.
128:1823–1829. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Shi L, Li W, Xu K, Guo Y and Yu J: Current
status of combined surgical and endovascular methods for
intracranial neurovascular diseases in a hybrid operating room. Int
J Clin Exp Med. 9:20741–20753. 2016.
|
|
31
|
Yu J, Guo Y, Xu B, Chen X and Xu K: Onyx
embolization and surgical removal as a treatment for hemorrhagic
AVM in a hybrid operating room. Int J Clin Exp Med. 9:22494–22501.
2016.
|
|
32
|
Fok KF, Holmin S, Alvarez H, Ozanne A,
Krings T and Lasjaunias PL: Spontaneous intracerebral hemorrhage
caused by an unusual association of developmental venous anomaly
and arteriovenous malformation. Interv Neuroradiol. 12:113–121.
2006. View Article : Google Scholar : PubMed/NCBI
|