Introduction
With the changes in dietary structure and population
aging in China, atherosclerosis has become the most common cause of
renal artery stenosis. It is estimated that atherosclerosis
accounts for about 70% in all causes of renal artery stenosis in
China, and 90% in Europe and America (1,2). Studies
have shown that the advanced age, hypertension, hyperlipidemia,
diabetes mellitus, renal insufficiency and peripheral vascular
disease are high-risk factors of atherosclerotic renal artery
stenosis (ARAS), and ARAS has a relatively high prevalence rate in
cardiovascular diseases (3–8). ARAS causes a decrease in renal blood
flow, which activates the renin-angiotensin system, leading to
elevated blood pressure, whereas progressive lumen stenosis may
lead to renal ischemia, causing progressive renal parenchymal
damage, decreased renal function and ultimately leading to renal
failure (9,10).
Percutaneous renal artery stent implantation (PTRAS)
can relieve the renal artery stenosis, restore the renal blood
flow, block the activation of renin-angiotensin-aldosterone system
(RAAS), treat the renal artery stenosis hypertension (RASH), and
retard the progression of nephropathy and renal insufficiency.
Numerous studies have shown that PTRAS can be used in the treatment
of ARAS-induced hypertension, improving the renal function of
patients with ARAS. Therefore, PTRAS has been used by many
clinicians in clinical practice (11–13).
However, in many clinical randomized controlled trials evaluating
the curative effects of simple drug therapy and intervention
combined with drug therapy on ARAS in recent years, there are no
significant benefits for ARAS patients in the improvement of renal
function, adverse cardiovascular events and long-term survival rate
after revascularization, and patients also need to bear the
relevant surgical risk, so whether PTRAS can benefit ARAS patients
clinically is still controversial (14–17).
In this study, the curative effect of PTRAS on 230
patients with ARAS and the factors influencing the prognosis of
PTRAS were retrospectively analyzed, so as to provide a reference
for selecting the therapeutic scheme of patients with renal artery
stenosis.
Patients and methods
Research subjects
Patients receiving renal arteriography in the
Cardiovascular Intervention Center of the Catheterization Room,
Department of Cardiology of Taizhou Hospital of Traditional Chinese
Medicine (Taizhou, China) from January 2010 to September 2014 were
enrolled. They were diagnosed with ARAS via renal arteriography
combined with clinical data according to the International
Classification of Disease, Ninth Revision, Clinical Modification
(ICD-9-CM), and received renal arterial stent implantation.
Patients were followed up to detect the general conditions, blood
pressure, types of antihypertensive drugs used, serum creatinine
(SCr), renogram, and adverse cardiogenic and nephrogenic events;
230 patients with complete data were followed up for 36 months.
This study was approved by the Ethics Committee of Taizhou Hospital
of Traditional Chinese Medicine (Taizhou, China). Signed written
informed consents were obtained from the patients and/or
guardians.
Inclusion and exclusion criteria. Noninvasive and
invasive examinations were initially performed to confirm that
renal artery stenosis had hemodynamic significance. Renal artery
stenosis diameter ≥70% usually indicates the hemodynamic
significance, and the physiological significance of mild stenosis
depends on the resistance of peripheral renal vessels or renal
autoregulation system conditions. In order to accurately determine
the degree of stenosis in patients with critical stenosis (renal
artery stenosis, 50–70%), the trans-lesion pressure gradient can be
measured; the peak systolic pressure difference >10% or the mean
pressure difference >5% indicates the hemodynamic significance,
which can be used as an indication of interventional therapy.
Inclusion criteria (18,19):
Renal artery stenosis patients with hemodynamic significance who
had the following clinical manifestations and definite indications
for percutaneous renal angioplasty may benefit from the
intervention treatment: hypertension in patients aged <30 years
old or late-onset hypertension in patients aged >60 years old;
hypertension remains uncontrollable after combined application of
at least three different types of antihypertensive drugs (one of
which is diuretics); abnormal changes in blood pressure, including
malignant, refractory or resistant hypertension (malignant
hypertension refers to hypertension complicated by acute target
organ damage, such as acute renal failure, acute decompensated
heart failure, hypopsia, and progression into grades III and IV
retinopathy); inability to tolerate antihypertensive drugs; recent
azotemia or further deterioration of renal function after taking
angiotensin-converting enzyme inhibitors (ACEI) or adrenergic
receptor-binding (ARB) antihypertensive drugs; renal atrophy or
different sizes in both kidneys (with a difference of >1.5 cm);
patients with unexplained deterioration of renal function; cardiac
disorder syndrome: recurrent transient pulmonary edema and unstable
angina secondary to left ventricular dysfunction.
Exclusion criteria: elderly patients with weak
constitution; patients whose disease was difficult to be
controlled; patients who could not tolerate the interventional
surgery; patients who were in the active stage of arterial
inflammation; patients with the long diameter of renal atrophy
<7 cm or intrarenal arterial resistance index >0.8; patients
with a serious allergic history of contrast agent or cholesterol
embolism; patients receiving renal artery anatomy thus not suitable
for interventional therapy or interventional therapy affected by
subsequent treatments.
Preoperative preparation. After admission, patients
were asked about their medical history and received physical
examinations, blood routine examination, biochemistry, coagulation,
echocardiography, renal color ultrasound and renal imaging before
operation to clear the condition of disease. Patients and their
families were informed of the purpose, methods and risks of
operation, and signed the informed consent. The meridian approach
was established, antihypertensive and anti-platelet drugs were used
routinely, and water and electrolyte balance was maintained. At 1
day before operation and on the day of operation, patients took
orally 300 mg aspirin and 300 mg clopidogrel hydrogen sulfate, and
1 ml/min normal saline was given for hydration at 24 h before
operation.
Renal artery stent implantation method. The femoral
or radial artery was punctured to send the catheter to the renal
artery lesions for arteriography, and then the degree of lesion
(lumen diameter and lesion length) was assessed. The guide wire was
pushed through the lesion vessel, and the balloon was sent to the
lesion along the guide wire and expanded. The stent was sent along
the guide wire to the renal vascular stenosis, followed by
positioning, dilation of the balloon and release of the stent, so
that the stent was fully adherent to the vessel. Arteriography was
performed again to observe the effect of stent implantation. If
there was no residual stenosis, thrombosis, vascular tear, vascular
dissection and other complications, the guide catheter could be
withdrawn under the guidance of guide wire. After the hemostasis of
arterial puncture site by compression, the operation was finished.
Postoperative residual stenosis <30% indicated the successful
operation, and stent diameter ≥50% indicated the in-stent
restenosis.
Postoperative management. Electrocardiogram and
blood pressure continued to be monitored, and 1 ml/min normal
saline was given for hydration. Vasopressor was withdrawn after
operation for 24 h, and the changes in the blood pressure of
patients were observed. Patients took 75 mg/day clopidogrel
hydrogen sulfate orally for at least 3 months, and 100 mg/day
aspirin orally for at least 36 months. The blood lipid and blood
pressure management was also provided every month.
Observation indexes. Patients enrolled were followed
up for 36 months after operation, and the following indexes were
collected. The peripheral arterial pressure in left upper limb of
patients was measured under a quiet state before and after renal
artery stent implantation 3 times, and the averages were taken. The
changes in the types of antihypertensive drugs used by the patients
were recorded. SCr and renogram results of patients were monitored
and recorded before and after renal artery stent implantation.
Estimated glomerular filtration rate (eGFR) was calculated: in
males eGFR (ml/min/1.73 m2) = [175 × SCr (mg/dl) - 1.234
× age (years old) - 0.179]; in females eGFR (ml/min/1.73
m2) = [175 × SCr (mg/dl) - 1.234 × age (years old) -
0.179] × 0.79. Hypertension, diabetes mellitus, hyperlipemia,
stroke and other complications in patients were recorded, and
Charlson comorbidity index (CCI) (20) was scored for patients, and the
comorbidities considered included diabetes mellitus, hyperlipemia,
stroke, smoking history, and congestive heart failure (CHF).
Whether adverse cardiogenic and nephrogenic events occurred within
36 months after renal artery stent implantation was detected
(17), including death, myocardial
infarction, stroke, hospitalization due to CHF, deterioration of
renal function (excluding other reasons, decrease of eGFR by ≥30%
over the initial value for ≥60 days), and permanent replacement
therapy of renal function required.
Analyses of risk factors of adverse cardiogenic and
nephrogenic events. Patients were divided into adverse event group
and control group according to whether adverse cardiogenic and
nephrogenic events occurred in patients. Multivariate regression
analyses were performed with relevant factors of adverse events
(including age, sex, smoking history, stroke, diabetes mellitus,
hyperlipemia, congestive heart failure and CCI score) as
variables.
Statistical analysis. Statistical Product and
Service Solutions (SPSS) 19.0 software (IBM Corp., Armonk, NY, USA)
was used for the analysis. Chi-square test was used for the
comparison of OR values and t-test for the comparison of SCr and
eGFR. Data are presented as mean ± standard deviation to evaluate
the curative effect of PTRAS. Logistic regression analyses were
used to analyze the risk factors related to adverse cardiogenic and
nephrogenic events after PTRAS. P<0.05 suggested that the
difference was statistically significant.
Results
Baseline data of patients
Among a total of 230 cases enrolled, there were 128
males and 102 females aged 63.5±14.1 years old with a course of
hypertension of 15.3±11.8 years. Preprocedure, 2.8±1.2 types of
antihypertensive drugs were used, and there were 123 cases with a
smoking history, 143 cases of hyperlipemia, 183 cases of coronary
heart disease, 78 cases of diabetes mellitus, and 36 cases of
stroke. A total of 286 stenotic renal arteries were treated, among
which 56 cases received bilateral renal artery stent implantation,
and 174 cases received unilateral renal artery stent implantation.
The success rate of renal artery stent implantation was 100%, and
no serious complications related to operation occurred (Table I).
 | Table I.Baseline characteristics of ARAS
patients. |
Table I.
Baseline characteristics of ARAS
patients.
| Parameters | Patients |
|---|
| Sex |
| Male, n
(%) | 128 (55.7) |
| Female, n
(%) | 102 (44.3) |
| Age (years) | 63.5±14.1 |
| Systolic pressure
(mmHg) | 158.7±20.5 |
| Diastolic pressure
(mmHg) | 92.6±10.1 |
| Number of
antihypertensive medications | 2.8±1.2 |
| SCr (µmol/l) | 130.3±51.4 |
| Smoking history, n
(%) | 123 (53.5) |
| Hyperlipidemia, n
(%) | 143 (62.2) |
| Coronary heart
disease, n (%) | 183 (79.6) |
| Diabetes mellitus, n
(%) | 78 (33.9) |
| Stroke, n (%) | 36 (15.7) |
Changes in blood pressure before and
after PTRAS
Before operation, the mean systolic blood pressure
of patients was 158.7±20.5 mmHg, and the mean diastolic blood
pressure was 92.6±10.1 mmHg. At 24 h after operation, the mean
systolic blood pressure of patients was decreased to 131.4±13.8
mmHg, and the mean diastolic blood pressure was decreased to
71.7±8.5 mmHg. At 36 months after operation, the mean systolic
blood pressure was 135.2±10.4 mmHg, and the mean diastolic blood
pressure was 72.7±7.9 mmHg (P<0.01). The blood pressure of
patients at each time-point after operation was significantly
decreased compared with that before operation (P<0.05). The
number of types of antihypertensive drugs used was decreased from
2.8±1.2 before operation to 2.0±0.9 36 months after operation
(P<0.01) (Table II).
| Table II.Comparison of blood pressure before
and after PTRAS. |
Table II.
Comparison of blood pressure before
and after PTRAS.
| Time | Systolic pressure
(mmHg) | Diastolic pressure
(mmHg) | No. of
antihypertensive medications |
|---|
| Preprocedure | 158.7±20.5 | 92.6±10.1 | 2.8±1.2 |
| Postprocedure |
| 24 h | 131.4±13.8 | 71.7±8.5 | 2.1±1.1 |
| 12
months | 132.3±14.4 | 72.9±8.7 | 2.2±1.0 |
| 24
months | 133.9±12.6 | 74.5±8.8 | 2.1±1.2 |
| 36
months | 135.2±10.4 | 72.7±7.9 | 2.0±0.9 |
Changes in renal functions before and
after PTRAS
SCr was increased in 123 cases (53.5%) and decreased
in 107 cases (46.5%). The levels of SCr at 24 h (140.5±60.1 µmol/l)
and at 36 months (133.2±55.6 µmol/l) after PTRAS were slightly
increased compared with that before operation (130.3±51.4 µmol/l),
and there were no statistically significant differences
(P>0.05). eGFR at each time-point after operation was slightly
decreased compared with that before operation, but the difference
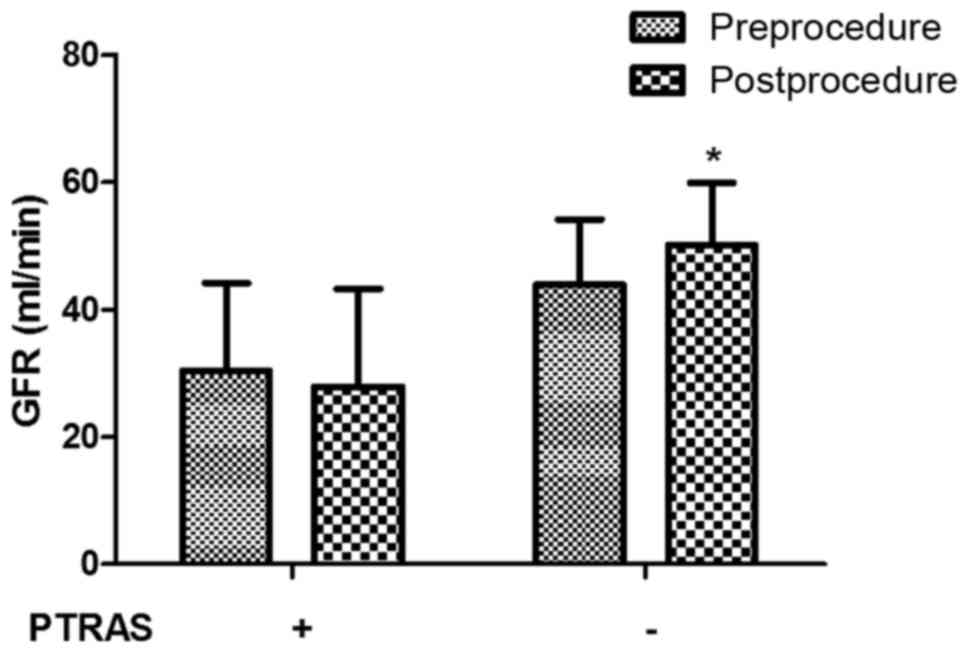
was not statistically significant (P>0.05) (Table III). A total of 90 patients
underwent renography at 1 year before and after operation to
evaluate the renal functions. A total of 90 cases of renal artery
stenosis (>70%) were treated with stent implantation, including
54 cases of unilateral renal artery stenosis and 36 cases of
bilateral renal artery stenosis. GFR on the side of receiving PTRAS
had no significant change compared with that before operation
(P>0.05), but GFR on the unaffected side without receiving PTRAS
was significantly increased compared with that before operation
(P=0.0014) (Fig. 1).
| Table III.Comparison of renal function before
and after PTRAS. |
Table III.
Comparison of renal function before
and after PTRAS.
| Time | SCr (µmol/l) | eGFR (ml/min/1.73
m2) |
|---|
| Preprocedure | 130.3±51.4 | 70.1±17.7 |
| Postprocedure |
| 24 h | 140.5±60.1 | 67.3±15.2 |
| 12
months | 139.8±55.7 | 68.4±17.5 |
| 24
months | 136.1±52.4 | 69.3±18.9 |
| 36 months | 133.2±55.6 | 68.8±19.1 |
Analyses of risk factors of adverse
cardiogenic or nephrogenic events after PTRAS
During the follow-up period, there were a total of
56 cases of adverse cardiogenic or nephrogenic events (24.3%),
including 5 cases of all-cause death, 10 cases of myocardial
infarction, 5 cases of stroke, 10 cases of hospitalization due to
heart failure, 23 cases of deterioration of renal function, and 3
cases of permanent dialysis treatment (Table IV). Patients were divided into
adverse event group and control group according to whether adverse
cardiogenic and nephrogenic events occurred during the follow-up.
Multivariate regression analyses of adverse cardiogenic or
nephrogenic events after PTRAS showed that the occurrence of
adverse events was obviously associated with advanced age (≥65
years old), higher CCI score (≥2 points), diabetes mellitus, stroke
and CHF (P<0.05) (Table V).
| Table IV.The occurrence of cardiovascular or
renal adverse events after PTRAS. |
Table IV.
The occurrence of cardiovascular or
renal adverse events after PTRAS.
| Cardiovascular or
renal adverse events | Patients, n (%) |
|---|
| All-cause deaths | 5 (8.9) |
| Myocardial
infarction | 10 (17.9) |
| Stroke | 5 (8.9) |
| Heart failure | 10 (17.9) |
| Deterioration of
renal function | 23 (41.1) |
| Permanent dialysis
treatment | 3 (5.4) |
| Table V.OR value and 95% CI of adverse events
after PTRAS with different comorbidities. |
Table V.
OR value and 95% CI of adverse events
after PTRAS with different comorbidities.
| Comorbidity | Adverse event, n
(%) | OR (95% CI) | P-value |
|---|
| Sex |
|
Male | 33 (58.9) | 1.193
(0.648–2.197) | 0.644 |
|
Female | 23 (41.1) |
|
|
| Age (years) |
|
≥65 | 41 (73.2) | 2.610
(1.347–5.060) | 0.005 |
|
<65 | 15 (26.8) |
|
|
| CCI score |
| 1 | 3 (5.4) | 1.0 |
|
| 2 | 10 (17.9) | 4.136
(1.084–15.780) | 0.039 |
| 3 | 29 (51.8) | 15.421
(4.419–53.807) | <0.001 |
| ≥4 | 14 (25) | 28.424
(7.001–115.325) | <0.001 |
| Smoking
history | 32 (57.1) | 1.641
(0.894–3.013) | 0.125 |
| Diabetes
mellitus | 21 (37.5) | 2.147
(1.121–4.112) | 0.023 |
| Stroke | 26 (46.4) | 3.209
(1.695–6.077) | <0.001 |
| Hyperlipidemia | 29 (51.8) | 0.758
(0.414–1.388) | 0.438 |
| CHF | 25 (44.6) | 3.446
(1.801–6.594) | <0.001 |
Discussion
With the development of interventional therapy,
renal artery stent implantation has become one of the main methods
for the treatment of ARAS. PTRAS can restore the renal blood
supply, block the damage of ischemia to the kidney and improve the
renal function (21). Improvement in
blood pressure control, promotion of cardiac function and renal
blood supply are favorable factors for the prognosis of patients.
The results of this study showed that PTRAS could effectively
control the blood pressure, and block the progressive deterioration
of renal function of patients, but it did not significantly improve
the renal function of patients. Large-scale multi-center randomized
controlled clinical trials have shown that the effect of renal
artery intervention on the body is mainly manifested in blood
pressure, and it has no significant effects on the protection of
renal function and mortality rate (15,17),
which are similar to the results in this study. There may be
several following reasons for this outcome brought by
interventional therapy: i) in the absence of distal protection,
interventional procedure may cause micro-thrombosis, cholesterol
crystal embolism and contrast agent-induced renal damage, lead to
impaired renal function and offset the benefit from interventional
therapy; ii) renal artery stenosis is a long-term slow-onset lesion
accompanied by long-term renal ischemia during the course, which
can lead to irreversible changes, such as renal fibrosis and
glomerular sclerosis; and iii) after interventional therapy,
stenotic arterial blood flow is improved, and the renal perfusion
pressure is increased; the high pressure and high perfusion can
further accelerate the renal parenchymal damage. In this study,
patients were followed up for 36 months, and the incidence rate of
adverse cardiogenic or nephrogenic events was 24.3%, which was
lower than that in CORAL stent treatment group (35.1%) (17). In addition, ARAS patients received
renography in this study and results showed that GFR on the
unaffected side, namely the kidney without receiving PTRAS, of
patients with unilateral ARAS after PTRAS has no significant
change, but GFR on the side receiving stent implantation was
increased compared with that before PTRAS, which can be explained
by the disappearance of a compensatory mechanism, but such reasons
as progression of atherosclerosis or other accompanying diseases
are not excluded.
Studies have shown that ARAS is often complicated
with other atherosclerotic diseases, such as coronary heart
disease, CHF and stroke, and these diseases jointly promote the
progression of atherosclerosis (22,23). In
this study, multivariate regression analyses of adverse cardiogenic
and nephrogenic events after PTRAS showed that the CCI score (≥2
points), advanced age (≥65 years old), diabetes mellitus, stroke
and CHF are risk factors related to adverse cardiogenic and
nephrogenic events in ARAS patients after PTRAS. Elderly patients
with ARAS suffer from systemic function degradation, so its
predictive value in adverse events after PTRAS is not unique. Among
the various risk factors, CCI score ≥4 points has the highest
predictive value. In addition to correcting the renal artery
stenosis, the optimal treatment of hypertension, diabetes mellitus,
cerebrovascular diseases and other accompanying diseases can really
improve the prognosis of patients; before the therapeutic regimen
is developed for ARAS patients, the comorbidity of patients must be
taken into full account, and the individualized therapeutic regimen
should be developed (24–26).
A limitation for the current study is that this was
a single-center retrospective analysis with limited number of
patients enrolled, thus leading to a certain bias in the results.
In the future, the experimental design can be improved, the sample
size can be expanded, and randomized controlled clinical trials can
be performed, increasing the reliability of results.
In conclusion, PTRAS can effectively control the
blood pressure, reduce the types of antihypertensive drugs used and
prevent the deterioration of renal function of patients with ARAS,
but it cannot improve the renal function of patients obviously. Age
(≥65 years old), CCI score (≥2 points), diabetes mellitus, stroke
and CHF are risk factors leading to adverse cardiogenic or
nephrogenic events after PTRAS.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YH contributed to the design of the study. YZ was
responsible for the acquisition of the data, HW and YW for the data
analysis, YY for the data interpretation, and YH for the
preparation of the manuscript. CC and JL performed the patients'
follow up. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Taizhou Hospital of Traditional Chinese Medicine (Taizhou, China).
Signed written informed consents were obtained from the patients
and/or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Safian RD: Atherosclerotic renal artery
stenosis. Curr Treat Options Cardiovasc Med. 5:91–101. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Safian RD and Textor SC: Renal-artery
stenosis. N Engl J Med. 344:431–442. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tanemoto M, Saitoh H, Satoh F, Satoh H,
Abe T and Ito S: Predictors of undiagnosed renal artery stenosis
among Japanese patients with risk factors of atherosclerosis.
Hypertens Res. 28:237–242. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang Y, Ge JB, Qian JY and Ye ZB:
Prevalence and risk factors of atherosclerotic renal artery
stenosis in 1,200 Chinese patients undergoing coronary angiography.
Nephron Clin Pract. 104:c185–c192. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Marcantoni C, Rastelli S, Zanoli L,
Tripepi G, Di Salvo M, Monaco S, Sgroi C, Capodanno D, Tamburino C
and Castellino P: Prevalence of renal artery stenosis in patients
undergoing cardiac catheterization. Intern Emerg Med. 8:401–408.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang Y, Ho DS, Chen WH, Wang YQ, Lam WF,
Shen ZJ, Lu CZ and Chui M: Prevalence and predictors of renal
artery stenosis in Chinese patients with coronary artery disease.
Intern Med J. 33:280–285. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Salehi N, Firouzi A, Gholoobi A, Shakerian
F, Sanati HR, Ahmadabadi MN and Moradi M: Relationship between
distribution of coronary artery lesions and renal artery stenosis
in patients undergoing simultaneous coronary and renal angiography.
Clin Med Insights Cardiol. 5:35–40. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Goldfarb DA: Prevalence of renovascular
disease in the elderly: A population-based study. J Urol.
170:1053–1054. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Neves PD, Oliveira AA, Oliveira MC,
Machado JR, Reis MA, Mendonça HM, Resende LA and Marques VP:
Research of multiarterial atherosclerotic disease in hypertensive
patients with renal artery stenosis. J Bras Nefrol. 34:243–250.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Textor SC: Atherosclerotic renovascular
disease as a cause of end-stage renal disease: Cost considerations.
Blood Purif. 14:305–314. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Henry M, Benjelloun A, Henry I, Polydorou
A and Hugel M: Renal angioplasty and stenting: Is it still
indicated after ASTRAL and STAR studies? J Cardiovasc Surg
(Torino). 51:701–720. 2010.PubMed/NCBI
|
|
12
|
Sarac TP: Influence and critique of the
ASTRAL and CORAL trials. Semin Vasc Surg. 24:162–166. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kanjwal K and Figueredo VM: Controversies
in the management of the renal artery stenosis. Cardiol J.
20:11–16. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bax L, Mali WP, Buskens E, Koomans HA,
Beutler JJ, Braam B, Beek FJ, Rabelink TJ, Postma CT, Huysmans FT,
et al: STAR Study Group: The benefit of STent placement and blood
pressure and lipid-lowering for the prevention of progression of
renal dysfunction caused by atherosclerotic ostial stenosis of the
renal artery. The STAR-study: Rationale and study design. J
Nephrol. 16:807–812. 2003.PubMed/NCBI
|
|
15
|
Wheatley K, Ives N, Gray R, Kalra PA, Moss
JG, Baigent C, Carr S, Chalmers N, Eadington D, Hamilton G, et al:
ASTRAL Investigators: Revascularization versus medical therapy for
renal-artery stenosis. N Engl J Med. 361:1953–1962. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jaff MR, Bates M, Sullivan T, Popma J, Gao
X, Zaugg M and Verta P: HERCULES Investigators: Significant
reduction in systolic blood pressure following renal artery
stenting in patients with uncontrolled hypertension: Results from
the HERCULES trial. Catheter Cardiovasc Interv. 80:343–350. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cooper CJ, Murphy TP, Cutlip DE, Jamerson
K, Henrich W, Reid DM, Cohen DJ, Matsumoto AH, Steffes M, Jaff MR,
et al: CORAL Investigators: Stenting and medical therapy for
atherosclerotic renal-artery stenosis. N Engl J Med. 370:13–22.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rundback JH, Sacks D, Kent KC, Cooper C,
Jones D, Murphy T, Rosenfield K, White C, Bettmann M, Cortell S, et
al: AHA Councils on Cardiovascular Radiology, High Blood Pressure
Research, Kidney in Cardiovascular Disease, Cardio-Thoracic and
Vascular Surgery, and Clinical Cardiology, and the Society of
Interventional Radiology FDA Device Forum Committee: Guidelines for
the reporting of renal artery revascularization in clinical trials.
American Heart Association. Circulation. 106:1572–1585. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Campbell NR, Kaczorowski J, Lewanczuk RZ,
Feldman R, Poirier L, Kwong MM, Lebel M, McAlister FA and Tobe SW:
Canadian Hypertension Education Program: 2010 Canadian Hypertension
Education Program (CHEP) recommendations: The scientific summary -
an update of the 2010 theme and the science behind new CHEP
recommendations. Can J Cardiol. 26:236–240. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yu TM, Sun CS, Lin CL, Wang CY, Chang PY,
Chou CY, Chuang YW, Lee BJ and Kao CH: Risk factors associated with
end-stage renal disease (ESRD) in patients with atherosclerotic
renal artery stenosis: A nationwide population-based analysis.
Medicine (Baltimore). 94:e9122015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Uder M and Humke U: Endovascular therapy
of renal artery stenosis: Where do we stand today? Cardiovasc
Intervent Radiol. 28:139–147. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chábová V, Schirger A, Stanson AW,
McKusick MA and Textor SC: Outcomes of atherosclerotic renal artery
stenosis managed without revascularization. Mayo Clin Proc.
75:437–444. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wright JR, Shurrab AE, Cheung C, Waldek S,
O'Donoghue DJ, Foley RN, Mamtora H and Kalra PA: A prospective
study of the determinants of renal functional outcome and mortality
in atherosclerotic renovascular disease. Am J Kidney Dis.
39:1153–1161. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Liu J, Huang Z, Gilbertson DT, Foley RN
and Collins AJ: An improved comorbidity index for outcome analyses
among dialysis patients. Kidney Int. 77:141–151. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Karanikas G, Becherer A, Wiesner K,
Dudczak R and Kletter K: ACE inhibition is superior to angiotensin
receptor blockade for renography in renal artery stenosis. Eur J
Nucl Med Mol Imaging. 29:312–318. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Onuigbo MA: Evidence of the syndrome of
rapid onset end-stage renal disease (SORO-ESRD) in the acute kidney
injury (AKI) literature - preventable causes of AKI and SORO-ESRD -
a call for re-engineering of nephrology practice paradigms. Ren
Fail. 35:796–800. 2013. View Article : Google Scholar : PubMed/NCBI
|