Introduction
Fracture is a very common bone injury. The incidence
of fractures in the hands, forearm and feet of children is high,
especially in the ankles, and the global accident rate is 187 out
of every 100,000 people. However, there are differences in the
incidence of fractures in different countries with different
genders and ages (1–3). Childhood is the most vigorous and
active stage of growth and development in a person's life. The
growth and development of the skeletal system is significantly
different from adults in terms of tissue anatomy, mechanical
properties, injury and healing characteristics. At the same time,
due to children's imperfect development of the nervous system, low
tolerance, a strong reaction after fracture, manifested as anxiety,
crying, kicking, etc., can lead to an extension of the range of
fracture damage. Therefore, high-quality care for fractures is
especially important. Nursing staff should be familiar with the
above characteristics, combined with nursing professional skills
and clinical experience, in order to take corresponding measures in
the nursing work to prevent various complications and promote
fracture healing. Owing to the special nature of children's bones,
delay and/or improper treatment of ankle fractures in children may
result in skeletal deformities and disability (4). The balance between the activity of
osteoblasts and osteoclasts promotes bone formation, and the
healing of fracture requires large amounts of osteoblasts (5). There is increasing evidence indicated
that inflammation reaction plays an important role in the
pathogenesis of ankle fracture. It has been reported that there is
a link between osteoclasts and inflammatory cytokines, including a
large number of TNF-α and IL-1β produced after fracture (6).
Resolvins (RVs) are a class of anti-inflammatory
bioactive small molecules derived from ω-PUFA docosahexaenoic acid
(DHA) under natural condition (7).
Resolvin D1 (RvD1) is one of the most widely and intensively
studied RVs with potent anti-inflammatory and erythropoietic
activity (7,8). It has significant efficacy in the
treatment of inflammation-related diseases. Pattern Recognition
Receptors (PRRs) belong to the innate immune system and are
responsible for identifying the pathogen-associated molecular
pattern (PAMP) of pathogenic microorganisms, and then activating
innate and adaptive immune responses (9). NLRP3 inflammasome is involved in the
development of chronic inflammatory responses, which consists of
NLRP3, ASC, and caspase-1 (10).
Nuclear factor-κB (NF-κB), a significant therapeutic target for the
control of inflammatory processes. RvD1 has been reported to
inhibit NF-κB signaling pathway and cytokines to protect against
ischemia-reperfusion kidney injury (11). Furthermore, RvD1 has been reported to
inhibit NLRP3 inflammasome and NF-κB signaling pathway in
STZ-induced diabetic retinopathy rats (12). However, the anti-inflammatory role of
RvD1 in ankle fracture has not been clarified.
Therefore, the present study investigated the
effects of RvD1on inflammatory response using MG-63 cells
stimulated with LPS as an inflammatory process model. The findings
of current study demonstrated that RvD1 reduced the expression of
inflammatory cytokines (IL-1β, IL-6 and TNF-α) in
lipopolysaccharide (LPS)-induced MG-63 cells. Moreover, RvD1
down-regulated the expression of p-p38, NF-κB (p50) and NLRP3
inflammasome in MG-63 cells treated with LPS. Therefore, the
function of RvD1 may be a new direction for the treatment of ankle
fractures.
Materials and methods
Reagents
LPS (Escherichia coli, 0111:B4) was obtained from
Sigma-Aldrich; Merck KGaA, (Darmstadt, Germany). RvD1 was purchased
from Cayman Chemical Company, (Ann Arbor, MI, USA). Dulbecco's
modified Eagle's medium (DMEM) and fetal bovine serum (FBS) were
purchased from Gibco; Thermo Fisher Scientific, Inc., (Waltham, MA,
USA). Primary antibodies: TNF-α (1:1,000; cat. no. 3707), IL-1β
(1:1,000; cat. no. 12703), IL-6 (1:1,000; cat. no. 12153), p-p38
(1:1,000; cat. no. 1170), NF-κB (p50) (1:1,000; cat. no. 13586),
NLRP3 (1:1,000; cat. no. 15101), ASC (1:1,000; cat. no. 67824),
cleaved caspase-1 (1:1,000; cat. no. 4199), caspase-1 (1:1,000;
cat. no. 3866), and COX-2 (1:1,000; cat. no. 12282), β-actin
(1:5,000; cat. no. 4970), and the anti-rabbit and anti-mouse
horseradish peroxidase-linked secondary antibody were purchased
from Cell Signaling Technology, Inc., (Danvers, MA, USA). IL-1β
(cat. no. E-EL-H0149c), IL-6 (cat. no. E-EL-H0102c) and TNF-α (cat.
no. E-EL-H0109c) ELISA kits were purchased from Elabscience
Biotechnology Co., Ltd, (Hubei, China).
Patients
A total of 35 peripheral blood samples (2 ml per
individual) from 35 children with ankle fracture, as well as 35
peripheral blood samples from 35 healthy children were collected at
our hospital from 2016 to 2017. The average age of children with
ankle fracture and the healthy controls were 5.5±1.3 and 5.6±1.2
years old, respectively. Equal proportion of boys and girls in both
groups. Informed consent was obtained from the parents or guardians
of all children enrolled and the present study, and the present
study was approved by the Ethics Committee of Children's Hospital
Affiliated to Nanjing Medical University.
Cell culture
The human osteoblastic osteosarcoma cell line MG-63
was purchased from the American Type Culture Collection (cat. no.
CRL-1427; Manassas, VA, USA). MG-63 cells were cultured in DMEM
containing 10% FBS, 0.1 mM nonessential amino acids, 1%
penicillin/streptomycin, and 1.0 mM sodium pyruvate (Gibco; Thermo
Fisher Scientific, Inc.), and incubated in a humidified environment
at 37°C with 5% CO2. For the experiments, MG-63 cells
(1×105 cells per well) were seeded into 6-well plates
and randomly divided into following six groups: 1) control group
(medium only), 2) LPS group (LPS 1 µg/ml), 3) vehicle control+ LPS
(0.1% ethanol +LPS 1 µg/ml) 4) RvD1 50+ LPS group (RvD1 50 nM + LPS
1 µg/ml), and 5) RvD1 100+ LPS group (RvD1 100 nM + LPS 1 µg/ml),
RvD1 200+ LPS group (RvD1 200 nM + LPS 1 µg/ml). In RvD1 group,
cells were pretreated with RvD1 (50, 100, 200 nM) (13) 2 h prior to LPS administration.
Cell viability assay
Cell viability was tested using MTT according to the
manufacturer's protocol. Briefly, MG-63 cells (5×104
cells/well) were seeded in 24-well plates, pretreated with
different concentrations of RvD1 (50, 100, 200 nM) for 2 h, then
these cells were treated with or without 1 µg/ml LPS for 48 h, then
removed the medium and incubated with 0.5 mg/ml MTT (Sigma-Aldrich;
Merck KGaA, Darmstadt, Germany) at 37°C for 4 h. Then, removed the
supernatant and added the DMSO (Sigma-Aldrich; Merck KGaA) for a
further 30 min at 37°C in the dark. The absorbance at 540 nm was
measured using Bio-Rad absorbance reader (Bio-Rad Laboratories,
Inc., Hercules, CA, USA).
ELISA assay
The supernatants were collected from the peripheral
blood of healthy controls and children with ankle fracture by
centrifugation at 3,000 × g for 15 min at 4°C. The levels of IL-1β
(cat. no. E-EL-H0149c), IL-6 (cat. no. E-EL-H0102c) and TNF-α (cat.
no. E-EL-H0109c) in the peripheral blood of healthy controls and
children with ankle fracture was detected by ELISA kits according
to the manufacturer's protocol.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Total RNA from MG-63 cells was extracted using
TRIzol (Invitrogen; Thermo Fisher Scientific, Inc.) after 24 h of
incubation, according to the manufacturer's protocol. 1 µg of total
RNA was reverse-transcribed into cDNA using TaqMan microRNA Reverse
Transcription kit (Invitrogen; Thermo Fisher Scientific, Inc),
following the manufacturer's protocol. TaqMan® Universal
PCR Master Mix kit (Thermo Fisher Scientific, Inc.) was used to
analyze the mRNA levels. The amplification conditions were as
following: 95°C for 10 min, followed by 40 cycles of 95°C for 10
sec and 60°C for 60 sec. The primer sequences used were as
following: IL-1β, forward, 5′-TGTGAAATGCCACCTTTTGA-3′ and reverse,
5′-TGAGTGATACTGCCTGCCTG-3′; IL-6, forward,
5′-CCGGAGAGGAGACTTCACAG-3′ and reverse, 5′-CAGAATTGCCATTGCACA-3′;
TNF-α, forward, 5′-GAACTGGCAGAAGAGGCACT-3′ and reverse,
5′-GGTCTGGGCCATAGAACTGA-3′; cyclooxygenase (COX)-2, forward,
5′-TCCATTGACCAGAGCAGAGA-3′ and reverse, 5′-TCTGGACGAGGTTTTTCCAC-3′;
GAPDH was used as internal controls, forward,
5′-GGCATTGCTCTCAATGACAA-3′ and reverse, 5′-TGTGAGGGAGATGCTCAGTG-3′.
The 2−ΔΔCq method was used to quantify relative gene
expression (14).
Western blot analysis
Total protein from MG-63 cells and the corresponding
cell culture medium was extracted using lysis buffer (Beijing
Solarbio Science & Technology Co., Ltd., Beijing, China). BCA
assay (Thermo Fisher Scientific, Inc.) was used to measure the
protein concentrations. Equal amount of proteins (25 µg/lane) were
subjected to 10% SDS-PAGE and than electro-transferred onto PVDF
membranes (EMD Millipore, Billerica, MA, USA). Then, the membranes
were blocked with 5% skim milk for 1 h at room temperature, and
subsequently incubated with primary antibodies: TNF-α, IL-1β, IL-6,
p-p38, NF-κB (p50), NLRP3, ASC, cleaved caspase-1, caspase-1,
COX-2, and β-actin overnight at 4°C. Then the membranes were
incubated with an appropriate horseradish peroxidase-linked
secondary antibody at room temperature for 1 h. Protein bands were
visualized using an enhanced chemiluminescence system (Pierce)
according to the manufacturer's instructions and quantified using
Quantity One Version 4.6 Image software (Bio-Rad Laboratories,
Inc.).
Statistical analysis
Statistical analyses were performed using SPSS
v.19.0 (SPSS, Inc., Chicago, IL, USA). Student's t-tests and
one-way ANOVA followed by NSK tests were performed to analyze the
differences between groups. Data were expressed as the mean ±
standard deviation. P<0.05 was considered to indicate a
statistically significant difference.
Results
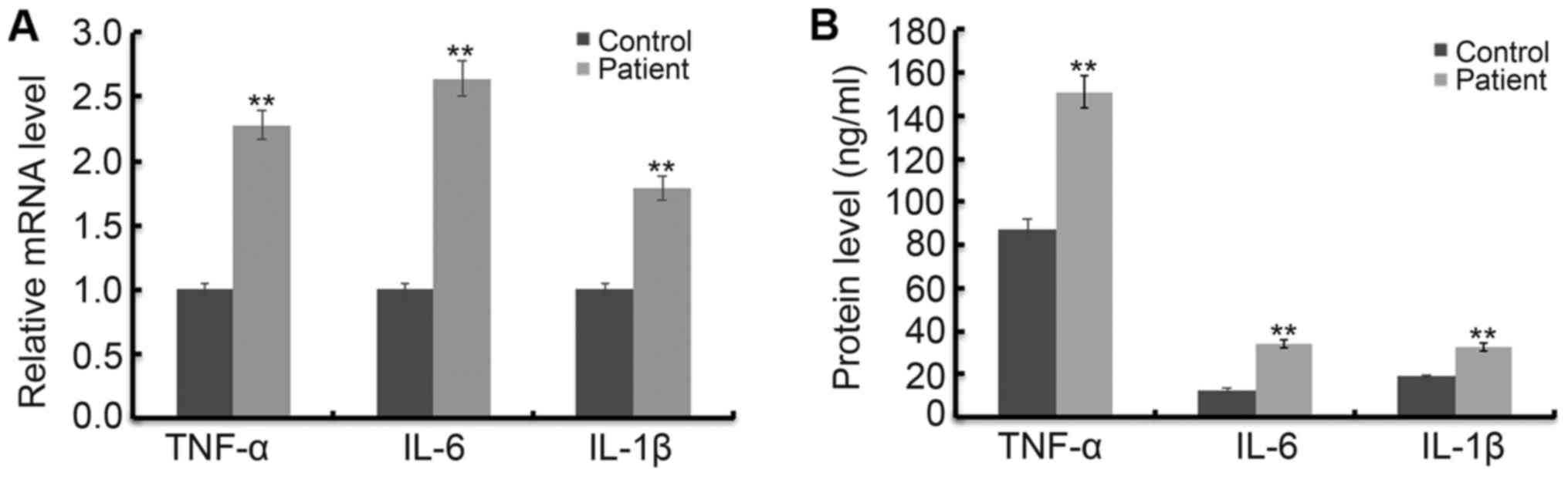
Levels of TNF-α, IL-1β and IL-6 in
children with ankle fracture are higher than those in healthy
children
In order to determine the increase in inflammatory
response in fractured children, the level of TNF-α, IL-1β and IL-6
was detected using RT-qPCR and western blot assay respectively. As
shown in Fig. 1A, the mRNA levels of
TNF-α, IL-1β and IL-6 were significantly increased in children with
ankle fractures compared with the healthy children. In addition,
the results of ELISA assay indicated that protein levels of TNF-α,
IL-1β and IL-6 were significantly increased in children with ankle
fractures compared with the healthy children (Fig. 1B).
RvD1 represses LPS induced
proliferation inhibition in MG-63 cells
To study whether RvD1 has toxic effects on the human
osteoblastic osteosarcoma cell line MG-63, MG-63 cells were
pretreated with different concentrations of RvD1 (50, 100, 200 nM)
for 2 h, then these cells were treated with or without 1 µg/ml LPS
for 48 h. Then, cell viability was detected using MTT. The results
showed that there was no significant changes in absorbance between
RvD1 treatment groups and the control group, indicating that RvD1
did not induce cytotoxicity in MG-63 cells (Fig. 2A). However, compared with the control
group, cell viability was significantly reduced by LPS treatment,
and these reductions were markedly reversed by RvD1 treatment,
indicating RvD1 inhibited LPS mediated cell proliferation
inhibition (Fig. 2B).
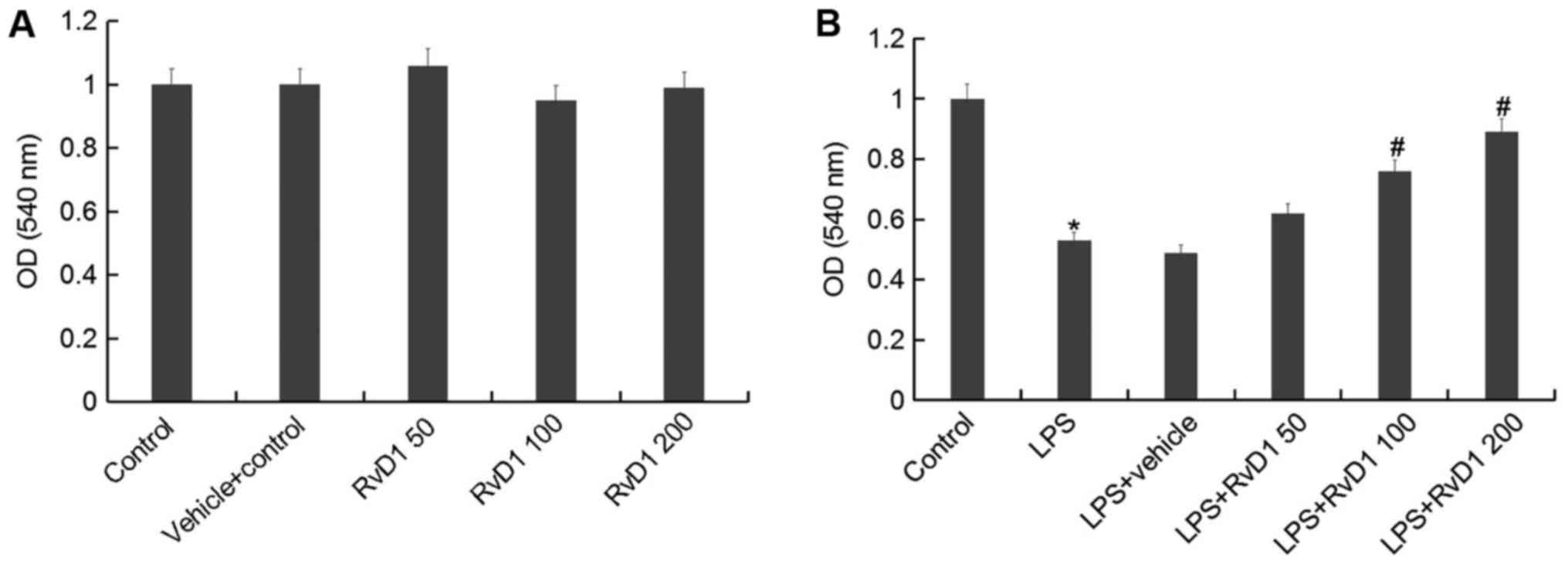 | Figure 2.RvD1 shows no cytotoxicity on MG-63
cells. To study whether RvD1 has toxic effects on the human
osteoblastic osteosarcoma cell line MG-63, MG-63 cells were
pretreated with different concentrations of RvD1 (50, 100, 200 nM)
for 2 h, then these cells were treated without (A) or with (B) 1
µg/ml LPS for 48 h. Then, cell viability of MG-63 cells was
measured by MTT assay. Control, Cells Without any treatment;
Vehicle control, Cells treated with 0.1% ethanol; RvD1 50, RvD1
100, RvD1 200: 50, 100 and 200 nM RvD1 treatment group. LPS, 1
µg/ml LPS treatment group; LPS + vehicle, 1 µg/ml LPS + 0.1%
ethanol treatment group; LPS + RvD1 50, 1 µg/ml LPS + 50 nM RvD1
treatment group; LPS + RvD1 100, 1 µg/ml LPS + 100 nM RvD1
treatment group; LPS + RvD1 200, 1 µg/ml LPS + 200 nM RvD1
treatment group. *P<0.05 vs. Control; #P<0.05 vs.
LPS. RvD1, resolvin D1. |
RvD1 significantly inhibits the LPS
induced increase of TNF-α, IL-1β and IL-6
We then investigated the effect of RvD1 on
inflammatory response of MG-63 cells. MG-63 cells were pretreated
with different concentrations of RvD1 (50, 100, 200 nM) for 2 h,
then these cells were treated with or without 1 µg/ml LPS for 48 h.
The mRNA and protein levels of TNF-α, IL-1β and IL-6 were
determined using RT-qPCR and western blot respectively. As shown in
Fig. 3, the mRNA and protein levels
of TNF-α, IL-1β and IL-6 were significantly increased in the LPS
treatment alone group compare with the control group, and these
increases were dose-dependently reversed following treatment with
RvD1.
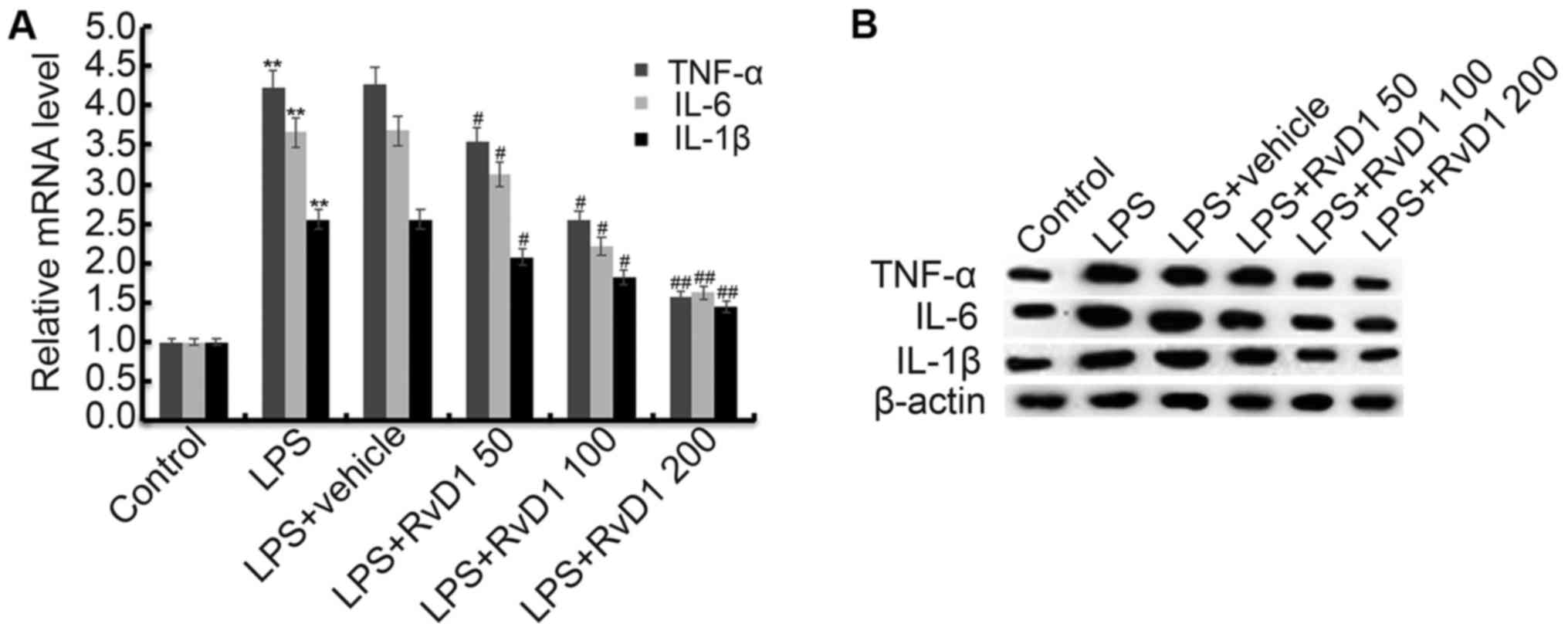 | Figure 3.Effect of RvD1 on TNF-α, IL-1β and
IL-6 expression. MG-63 cells were pretreated with different
concentrations of RvD1 (50, 100, 200 nM) for 2 h, then these cells
were treated with or without 1 µg/ml LPS for 48 h. The mRNA (A) and
protein (B) levels of TNF-α, IL-1β and IL-6 were determined using
RT-qPCR and western blot respectively. Control, Cells without any
treatment; LPS, 1 µg/ml LPS treatment group; LPS + vehicle, 1 µg/ml
LPS + 0.1% ethanol treatment group; LPS + RvD1 50, 1 µg/ml LPS + 50
nM RvD1 treatment group; LPS + RvD1 100, 1 µg/ml LPS + 100 nM RvD1
treatment group; LPS + RvD1 200, 1 µg/ml LPS + 200 nM RvD1
treatment group. **P<0.01 vs. Control; #P<0.05 vs.
LPS; ##P<0.01 vs. LPS. RvD1, resolvin D1. |
RvD1 significantly inhibits the LPS
induced activation of p38, NF-κB (p50) and increase of COX-2
To investigate the molecular mechanism of
anti-inflammatory effect of RD1 on LPS treated MG-63 cells, p38,
NF-κB (p50) and COX-2 were analyzed in our present study. As shown
in Fig. 4, the protein levels of
p-p38, and NF-κB (p50) were significantly up-regulated compare with
the control group. And the mRNA and protein levels of COX-2
markedly up-regulated compare with the control group. RvD1
treatment markedly inhibited the LPS induced up-regulation of
p-p38, NF-κB (p50) and COX-2 expression.
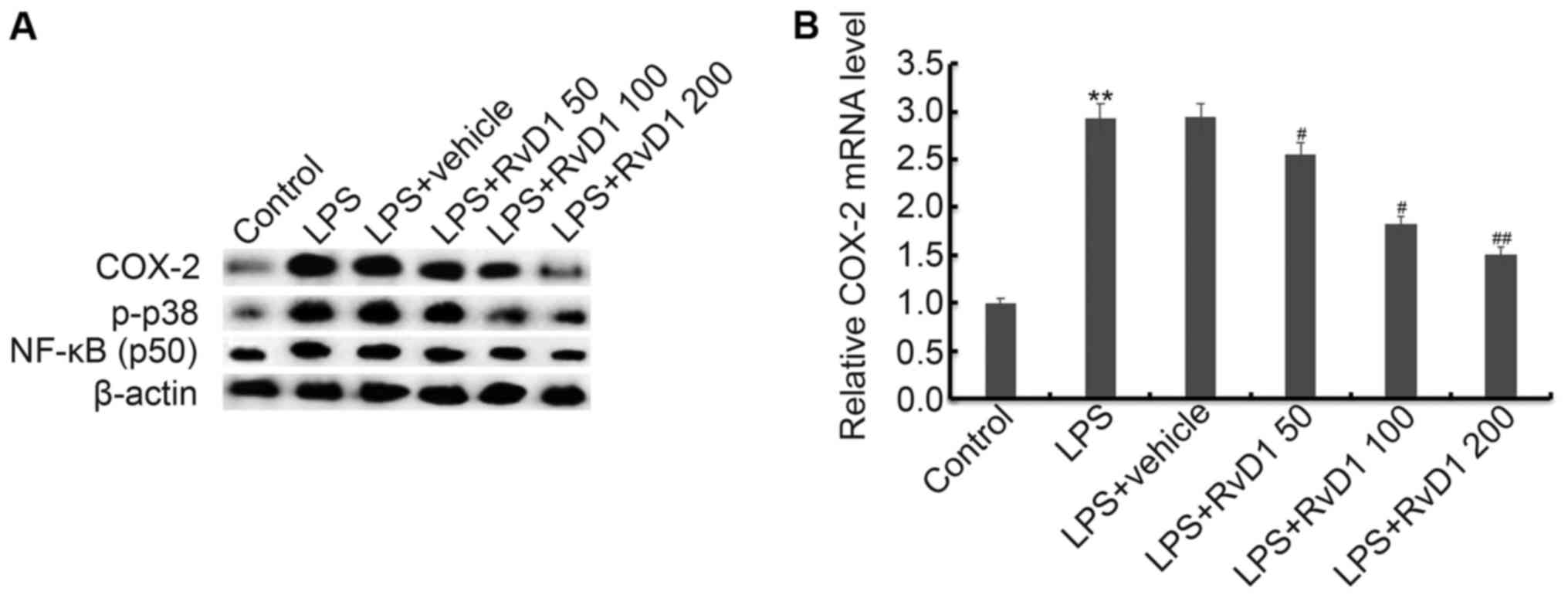 | Figure 4.Effect of RvD1 on activation of
p38MAPK-NF-κB pathway and COX-2 expression. MG-63 cells were
pretreated with different concentrations of RvD1 (50, 100, 200 nM)
for 2 h, then these cells were treated with or without 1 µg/ml LPS
for 48 h. Then, protein (A) levels of COX-2, p-p38, NF-κB (p50) and
p-p65 were detected by western blot analysis. The mRNA level of
COX-2 was detected using RT-qPCR (B). Control, Cells without any
treatment; LPS, 1 µg/ml LPS treatment group; LPS + vehicle, 1 µg/ml
LPS + 0.1% ethanol treatment group; LPS + RvD1 50, 1 µg/ml LPS + 50
nM RvD1 treatment group; LPS + RvD1 100, 1 µg/ml LPS + 100 nM RvD1
treatment group; LPS + RvD1 200, 1 µg/ml LPS + 200 nM RvD1
treatment group. **P<0.01 vs. Control; #P<0.05 vs.
LPS; ##P<0.01 vs. LPS. RvD1, resolvin D1 |
RvD1 markedly inhibits the LPS induced
activation of NLRP3 inflammasome
Previous studies indicated that NLRP3 inflammasome
activation can be inhibited by RvD1. Therefore, in our study we
finally investigated the effect of RvD1 on NLRP3 inflammasome
activation in MG-63 cells. Our results indicated that compared with
the control group, the expression of NLRP3, ASC, cleaved caspase-1
and caspase-1 were all markedly up-regulated in the LPS treatment
alone group. RvD1 treatment markedly inhibited LPS induced
up-regulation of NLRP3, ASC, cleaved caspase-1 and caspase-1
(Fig. 5).
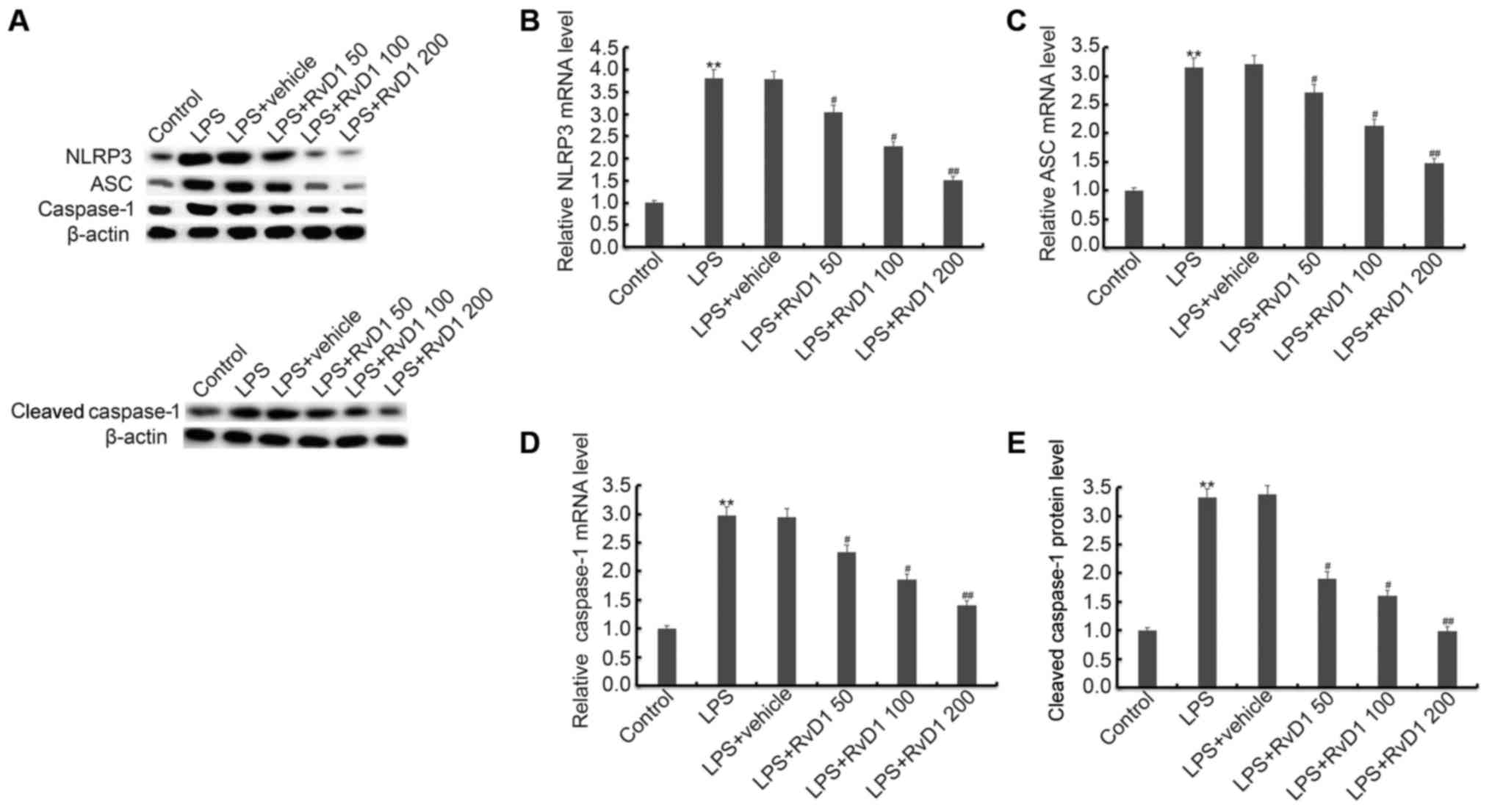 | Figure 5.(A-E) Effect of RvD1 on NLRP3
inflammasome. MG-63 cells were pretreated with different
concentrations of RvD1 (50, 100, 200 nM) for 2 h, then these cells
were treated with or without 1 µg/ml LPS for 48 h. Then, protein
(A, E) level of NLRP3, ASC and cleaved caspase-1/caspase-1, and
mRNA (B-D) levels of NLRP3, ASC and caspase-1 were detected by
western blot analysis and RT-qPCR. Control, cells without any
treatment; LPS, 1 µg/ml LPS treatment group; LPS + vehicle, 1 µg/ml
LPS + 0.1% ethanol treatment group; LPS + RvD1 50, 1 µg/ml LPS + 50
nM RvD1 treatment group; LPS + RvD1 100, 1 µg/ml LPS + 100 nM RvD1
treatment group; LPS + RvD1 200, 1 µg/ml LPS + 200 nM RvD1
treatment group. **P<0.01 vs. Control; #P<0.05 vs.
LPS; ##P<0.01 vs. LPS. RvD1, resolvin D1. |
Discussion
In the present study, we demonstrated that the
levels of IL-1β, IL-6 and TNF-α were up-regulated in children with
ankle fracture compared with the healthy children. Pretreatment of
RvD1 dose-dependently reversed the LPS induced up-regulation of
IL-1β, IL-6, TNF-α, and COX-2 mRNA and protein levels, and also
decreased expression of the p-p38, NF-κB (50), and NLRP3
inflammasome, including NLRP3, ASC, cleaved caspase-1/caspase-1
induced by LPS treatment in MG-63 cells. These findings suggested
that RvD1 may relieve ankle fracture by inhibiting inflammatory
response via repressing NLRP3 inflammasome and NF-κB signaling
pathway. The anti-inflammatory function of RvD1 may reduce
osteoclast and increase osteoblast thus promoting bone formation.
Therefore, the present study identified a potential new method for
the treatment of ankle fractures.
Inflammation plays a critical role in ankle
fracture. Persistent elevation of inflammatory cytokines such as
IL-1β, IL-6 and TNF-α is associated with poor prognosis in children
with ankle fracture (15). LPS
administration significantly increased the level of IL-1β, IL-6 and
TNF-α, which was used to establish the cellar inflammation model of
ankle fractures. RvD1 has been shown to down-regulated the level of
TNF-α and IL-6 in BALF of mice with LPS induced ALI (16). In the present study, we found that
RvD1 dose-dependently down-regulated level of IL-1β, IL-6 and TNF-α
in LPS induced MG-63 cells.
In order to better understand the immediate cellular
response to an ankle fracture and further study the
anti-inflammatory function by the application of RvD1, we
hypothesized that it may be possible to counteract the inflammatory
signaling pathway involved in the injury-mediated response by RvD1.
NLRP plays a critical role in the development of chronic
inflammatory response through the up-regulation of the
pro-inflammatory cytokines IL-18 and IL-1β (17). Activation of the NLRP3 inflammasome
has been demonstrated in a wide variety of diseases, including
liver injury (18). Previous study
has reported that RvD1 abrogates hHcys-induced podocyte injury by
inhibition of the NLRP3 inflammasome activation (19). RvD1 plays a protective role in STZ
induced diabetic retinopathy by inhibiting the level of activation
of the NLRP3 inflammasome (12). Our
results demonstrated that RvD1 inhibited the expression of NLRP3,
ASC, cleaved caspase-1 and caspase-1 induced by LPS in MG-63 cells.
There results indicated that RvD1 alleviated ankle fracture may be
by inhibiting the NLRP3 inflammasome.
NF-κB, a ubiquitously expressed transcription factor
that regulates many inflammatory cytokines. It has been reported
that activation of NF-κB participates in NLRP3 inflammasome
activation (20). Previous study has
reported that RvD1 markedly reduced acute lung injury associated
mortality through inhibiting the activation of NF-κB pathway
(21). In addtion, RvD1 has been
shown to regulate NF-κB activation to reduce mucosal inflammation
(22). Furthermore, RvD1 markedly
inhibited IMQ induced activation of ERK1/2, p38, JNK (c-Jun
N-terminal protein kinase, a subfamily of MAPKs), and NF-κB
(23). Our present study found that
RvD1 could repress LPS induced NF-κB and p38 activation.
Ankle injury commonly result in persistent pain,
muscle wasting, functional impairments and stiffness (24). Till now, there is insufficient
evidence to favor any particular rehabilitation approach after
ankle fracture. The key to reducing pain and fracture healing is
timely diagnosis, treatment and high-quality care. The Ottawa Ankle
Rule (OAR) (25,26) has been reported to help to determine
whether radiography suitable for the diagnosis of ankle fracture in
children with ankle pain. However, when pediatric emergency
department (ED) nurses accurately apply and interpret OAR, children
in the hospital ED receive treatment from the nurse Cooperative
Practice Program (CPP) to minimize ankle radiography, waiting
times, and costs without an increased rate of missed fractures
(27).
In summary, the present study demonstrated that RvD1
decreased the level of IL-1β, IL-6 and TNF-α in LPS treated MG-63
cells, which may be mediated by inhibiting the activation of
p38/NF-κB/NLRP3 inflammation signaling pathway, may therefore
relieve ankle fracture. RvD1 may be a potential therapeutic agent
for ankle fracture treatment.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
DC, JP and YS designed the study, and performed data
collection and analysis. YT and PZ were responsible for
interpreting results. All authors collaborated to develop the
manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
parents or guardians of all children enrolled and the present
study, and the present study was approved by the Ethics Committee
of Children's Hospital Affiliated to Nanjing Medical
University.
Patient consent for publication
All patients provided consent for publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
MacIntyre NJ and Dewan N: Epidemiology of
distal radius fractures and factors predicting risk and prognosis.
J Hand Ther. 29:136–145. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Moon RJ, Harvey NC, Curtis EM, de Vries F,
van Staa T and Cooper C: Ethnic and geographic variations in the
epidemiology of childhood fractures in the United Kingdom. Bone.
85:9–14. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hedstrom EM, Svensson O, Bergström U and
Michno P: Epidemiology of fractures in children and adolescents.
Acta Orthop. 81:148–153. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chevalley T, Bonjour JP, van Rietbergen B,
Rizzoli R and Ferrari S: Fractures in healthy females followed from
childhood to early adulthood are associated with later menarcheal
age and with impaired bone microstructure at peak bone mass. J Clin
Endocrinol Metab. 97:4174–4181. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
He Z, Selvamurugan N, Warshaw J and
Partridge NC: Pulsed electromagnetic fields inhibit human
osteoclast formation and gene expression via osteoblasts. Bone.
106:194–203. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Huang H, Zhao N, Xu X, Xu Y, Li S, Zhang J
and Yang P: Dose-specific effects of tumor necrosis factor alpha on
osteogenic differentiation of mesenchymal stem cells. Cell Prolif.
44:420–427. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Serhan CN, Hong S, Gronert K, Colgan SP,
Devchand PR, Mirick G and Moussignac RL: Resolvins: A family of
bioactive products of omega-3 fatty acid transformation circuits
initiated by aspirin treatment that counter proinflammation
signals. J Exp Med. 196:1025–1037. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sun YP, Oh SF, Uddin J, Yang R, Gotlinger
K, Campbell E, Colgan SP, Petasis NA and Serhan CN: Resolvin D1 and
its aspirin-triggered 17R epimer. Stereochemical assignments,
anti-inflammatory properties and enzymatic inactivation. J Biol
Chem. 282:9323–9334. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Werners AH and Bryant CE: Pattern
recognition receptors in equine endotoxaemia and sepsis. Equine Vet
J. 44:490–498. 2009. View Article : Google Scholar
|
|
10
|
Mori MA, Bezy O and Kahn CR: Metabolic
syndrome: Is Nlrp3 inflammasome a trigger or a target of insulin
resistance? Circ Res. 108:1160–1162. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Duffield JS, Hong S, Vaidya VS, Lu Y,
Fredman G, Serhan CN and Bonventre JV: Resolvin D series and
protectin D1 mitigate acute kidney injury. J Immunol.
177:5902–5911. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yin Y, Chen F, Wang W, Wang H and Zhang X:
Resolvin D1 inhibits inflammatory response in STZ-induced diabetic
retinopathy rats: Possible involvement of NLRP3 inflammasome and
NF-κB signaling pathway. Mol Vis. 23:242–250. 2017.PubMed/NCBI
|
|
13
|
Xu J, Gao X, Yang C, Chen L and Chen Z:
Resolvin D1 attenuates Mpp+-induced parkinson disease via
inhibiting inflammation in PC12 Cells. Med Sci Monit. 23:2684–2691.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Adams SB, Leimer EM, Setton LA, Bell RD,
Easley ME, Huebner JL, Stabler TV, Kraus VB, Olson SA and Nettles
DL: Inflammatory microenvironment persists after bone healing in
intra-articular ankle fractures. Foot Ankle Int. 38:479–484. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Liao Z, Dong J, Wu W, Yang T, Wang T, Guo
L, Chen L, Xu D and Wen F: Resolvin D1 attenuates inflammation in
lipopolysaccharide-induced acute lung injury through a process
involving the PPARγ/NF-κB pathway. Respir Res. 13:1102012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Strowig T, Henao-Mejia J, Elinav E and
Flavell R: Inflammasomes in health and disease. Nature.
481:278–286. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Menzel CL, Sun Q, Loughran PA, Pape HC,
Billiar TR and Scott MJ: Caspase-1 is hepatoprotective during
trauma and hemorrhagic shock by reducing liver injury and
inflammation. Mol Med. 17:1031–1038. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Li G, Chen Z, Bhat OM, Zhang Q,
Abais-Battad JM, Conley SM, Ritter JK and Li PL: NLRP3 inflammasome
as a novel target for docosahexaenoic acid metabolites to abrogate
glomerular injury. J Lipid Res. 58:1080–1090. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Shao A, Wu H, Hong Y, Tu S, Sun X, Wu Q,
Zhao Q, Zhang J and Sheng J: Hydrogen-rich saline attenuated
subarachnoid hemorrhage-induced early brain injury in rats by
suppressing inflammatory response: possible involvement of NF-κB
pathway and NLRP3 inflammasome. Mol Neurobiol. 53:3462–3476. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wang B, Gong X, Wan JY, Zhang L, Zhang Z,
Li HZ and Min S: Resolvin D1 protects mice from LPS-induced acute
lung injury. Pulm Pharmacol Ther. 24:434–441. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Colby JK, Abdulnour RE, Sham HP, Dalli J,
Colas RA, Winkler JW, Hellmann J, Wong B, Cui Y, El-Chemaly S, et
al: Resolvin D3 and aspirin-triggered resolvin D3 are protective
for injured epithelia. Am J Pathol. 186:1801–1813. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Xu J, Duan X, Hu F, Poorun D, Liu X, Wang
X, Zhang S, Gan L, He M, Zhu K, et al: Resolvin D1 attenuates
imiquimod-induced mice psoriasiform dermatitis through MAPKs and
NF-κB pathways. J Dermatol Sci. 89:127–135. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zwipp H, Hoffmann R, Thermann H and
Wippermann BW: Rupture of the ankle ligaments. Int Orthop.
15:245–249. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Stiell IG, Greenberg GH, McKnight RD, Nair
RC, McDowell I, Reardon M, Stewart JP and Maloney J: Decision rules
for the use of radiography in acute ankle injuries. Refinement and
prospective validation. JAMA. 269:1127–1132. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Stiell IG, McKnight RD, Greenberg GH,
McDowell I, Nair RC, Wells GA, Johns C and Worthington JR:
Implementation of the Ottawa ankle rules. JAMA. 271:827–832. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Karpas A, Hennes H and Walsh-Kelly CM:
Utilization of the Ottawa ankle rules by nurses in a pediatric
emergency department. Acad Emerg Med. 9:130–133. 2002. View Article : Google Scholar : PubMed/NCBI
|