Introduction
Pulmonary cryptococcosis is a pulmonary fungal
disease caused by Cryptococcus neoformans, an opportunistic
pathogen, which may cause infection regardless of whether the
body's immunity is low or not (1–3).
Pulmonary neoformans with multiple nodules or mass is a type of
primary pulmonary cryptococcosis; it is defined as a pulmonary
disease caused by Cryptococcus neoformans, in which the
number of intrapulmonary lesions is ≥2, the maximum nodule diameter
is <3 cm and the maximum mass diameter is ≥3 cm (4–6). Due to
the lack of typical signs on computed tomography (CT), the disease
is prone to be misdiagnosed as lung cancer accompanied by
intrapulmonary metastasis or tuberculosis. The present study was
aimed at improving the understanding of this disease by comparing
the CT signs with the pathological resultsin 20 patients and then
using the pathological results to explain the CT signs.
Intrapulmonary metastasis of lung cancer manifests
as multiple intrapulmonary nodules or masses with signs on CT
including lobulation, irregular margins, spiculation, vascular
convergence sign and pleural indentation (7–9).
Pulmonary tuberculosis on CT manifests as multiple intrapulmonary
nodules or masses presenting signs including irregular margins,
satellite lesions and tree-in-bud sign (10,11). It
is difficult to differentiate pulmonary cryptococcosis with
multiple nodules or masses from lung cancer accompanied by
intrapulmonary metastasis or pulmonary tuberculosis, which may lead
to incorrect treatment. Since CT is non-invasive and reproducible,
it is commonly used for evaluating lung diseases. Therefore, CT
should be used to improve the accuracy of the diagnosis of this
disease.
Patients and methods
The present study retrospectively enrolled 20
patients presenting with multiple nodules or masses on CT. They
were selected from 68 patients with primary pulmonary
cryptococcosis, who presented at three tertiary grade-A hospitals
[The Second Affiliated Hospital of Qiqihar Medical College
(Qiqihar), the Chinese PLA General Hospital (Beijing) and Beijing
Shijitan Hospital (Beijing)] between January 2012 and December
2016. All of the 20 patients were pathologically confirmed to have
primary pulmonary cryptococcosis. Of these, six underwent segmental
or wedge resection of the lung and 14 underwent CT-guided
percutaneous biopsy. The clinical data of the 20 patients,
including the clinical manifestations, imaging signs, pathological
results and treatment, were retrospectively analyzed.
Histopathological images were utilized for diagnostic purposes.
Since the present study was retrospective, the ethics committees of
the three hospitals determined thatno informed consent was required
from the patients.
Results
General patient information
The 20 patients included 14 males and 6 females with
a mean age of 49.69 years (range, 27–78 years). The individual data
for each patient are presented in Table
I. Within the cohort, 6 patients had underlying diseases
including diabetes, cancer, cirrhosis of the liver and pulmonary
tuberculosis; furthermore, 1 patient had a history of exposure to
birds. A total of 12 patients presented with symptoms, including an
elevated temperature, cough, chest pain and abdominal pain, while
the remaining 8 patients had no symptoms.
 | Table I.Clinical characteristics of the
patients with primary pulmonary cryptococcosis with multiple
nodules or masses (n=20). |
Table I.
Clinical characteristics of the
patients with primary pulmonary cryptococcosis with multiple
nodules or masses (n=20).
| No./age/gender | History | Symptoms | Location | Size (cm) | No. of nodules | CT presentation | CT primary
diagnosis | Biopsy style | Pathology | Treatment | Prognosis |
|---|
| 1/M/30 | Contact with
birds | Cough,
expectoration | RIL | Max: 1.9×1.7; around
nodule: 1.6–2.0 | 3 | A near-pleural mass
with clusters of round satellite lesions along bronchus, irregular
margin, air bronchogram, halo sign around nodule, cavity | Infected lesions | Paracentesis | Granulomatous
lesions, Cryptococcus in macrophages, PAS (+) | Fluconazole for 20
months | Significant reduction
and disappearance, no re-examination |
| 2/F/55 | Breast cancer
surgery | Cough | RIL | Max: 5.2×3.6; around
nodule: 1.1–1.5 | 4 | A near-pleural mass
with clusters of round satellite lesions along bronchus, air
bronchogram, lymphonodus (+) | Lung cancer with
intrapulmonary metastasis | Paracentesis | Granulomatous
lesions, Cryptococcus in macrophages, lymph nodes exhibited
reactive hyperplasia, PAS (+) | Fluconazole for 12
months | No
re-examination |
| 3/M/54 | Hypertension | Stomachache | RIL+LUL | Max: 2.3×1.7; around
nodule: 0.6–1.0 | 3 | A mass with clusters
of round satellite lesions along bronchus, irregular margin, halo
sign and air bronchogram | Granuloma | Paracentesis | Granulomatouslesions,
Cryptococcus in macrophages, PAS (+), acid fast stain
(−) | Fluconazole for 9
months | Significant reduction
and disappearance, no re-examination |
| 4/M/68 | Pulmonary
tuberculosis | Chest pain | RUL | Max: 3.1×2.0; around
nodule: 1.6–2.0 | 4 | A near-pleural mass
with clusters of round satellite lesions along bronchus, irregular
margin, long spicule, irregular calcification | Tuberculosis or lung
cancer with intrapulmonary metastasis | Operation | Granulomatous lesions
with necrosis, Cryptococcus and Candidain necrotic
tissue, pulmonary interstitial lymphocytic infiltration PAS (+),
acid fast stain (−) | Fluconazole for 3
months | No
re-examination |
| 5/M/39 | Hypertension | Chest pain | LIL | Max: 3.2×1.8; around
nodule: 0.6–1.0 | 5 | Three masses,
clusters of distribution, with round satellite lesions along
bronchus, some with lobulation, irregular margin, pleural
indentation and cavity | Tuberculosis | Operation | Granulomatous
lesions, Cryptococcus in macrophages, PAS (+) | None | No
recurrence |
| 6/M/78 | Hypertension | Elevated temperature,
cough, chill | RIL | Max: 2.1×1.3; around
nodule: 0.1–0.5 | 4 | A near-pleural mass
with clusters of satellite lesions along bronchus, spicule | Infected lesions | Paracentesis | Granulomatous lesions
without necrosis, Cryptococcus inmacrophages, PAS (+) | Fluconazole for 13
months | No recurrence |
| 7/M/45 | Reflux
esophagitis | Chest pain | RIL | Max: 1.9×1.3; around
nodule: 0.1–0.5 | 4 | A near-pleural mass
with satellite lesions along bronchus, irregularmargin, air
bronchogram, long spicule, pleural indentation, SUV 5.43 on
PET-CT | Lung cancer with
intrapulmonary metastasis | Operation | Granulomatous
lesions, Cryptococcus in macrophages, PAS (+), acid fast
stain (−) | Fluconazole for 3
months | Unknown |
| 8/M/37 | None | Cough,
expectoration | RUL+LIL | LIL: 3.0×2.2 RUL:
2.0×1.6 | 2 | LIL: Mass, irregular
margin, lobulation, cavity, air bronchogram, long spicule; RUL: A
mass with a nodule, irregular margin, air bronchogram, spicule | Infected lesions | Paracentesis | Granulomatous
lesions, Cryptococcus in macrophages, PAS (+) | Caspofungin,
itraconazole for 15 days, fluconazole for 6 months | Significant reduction
and disappearance, no re-examination |
| 9/M/65 | Hypertension | None | RML | Max: 2.0×1.6; around
nodule: 0.6–1.0 | 4 | A nodule with
clusters of satellite lesions along bronchus, lobulation, short
spicule, air bronchogram, pleural indentation, lymphonodus (+) | Lung cancer with
intrapulmonary metastasis | Operation | Granulomatous
lesions, organized lesions, Cryptococcus in macrophages,
lymph nodes with reactive hyperplasia, PAS (+), acid fast stain
(−) | None | No
re-examination |
| 10/M/47 | Hypertension,
diabetes | None | RUL+LIL | LIL-Max: 3.4×2.8;
around nodule: 1.1–1.5 | 6 | LIL: A near-pleural
mass with clusters of satellite lesions alongbronchus, irregular
margin, lobulation, SUV9.3 in PET-CT; RUL: A nodule with
lobulation, blood vessel convergence, SUV5.56 on PET-CT | Lung cancer with
intrapulmonary metastasis | Paracentesis | Granulomatous
lesions, organized lesions, Cryptococcus in macrophages,
PAS(+), acid fast stain (−) | Fluconazole for 10
months | No
re-examination |
| 11/M/67 | Cirrhosis, spleen
resection | None | LIL | Max: 1.0×0.7;
around nodules: 0.1–0.5 | 4 | A near-pleural mass
with clusters of satellite lesions along bronchus, air bronchogram,
lobulation | Lung cancer with
intrapulmonary metastasis | Paracentesis | Granulomatous
lesions, Cryptococcus in macrophages, PAS (+) | Fluconazole for 5
months | No
re-examination |
| 12/F/38 | None | None | Whole lung | Max: 1.5×1.4;
around nodule: 0.1–0.5 | 9 | Multiple nodules in
the whole lung, particularly one nodule with clusters of satellite
lesions along bronchus | Uncertain | Paracentesis | Granulomatous
lesions, Cryptococcus in macrophages, PAS (+) | Fluconazole for 6
months | No
re-examination |
| 13/M/54 | None | None | RUL | Max: 1.1×0.8;
around nodule: 0.1–0.5 | 3 | A nodule with
clusters of satellite lesions along bronchus, irregular margin,
long spicule, air bronchogram | Lung cancer with
intrapulmonary metastasis | Operation | A solid region
composed of hyperplastic fibrous tissue, granulomatouslesions,
organized lesions, Cryptococcus in macrophages, PAS (+),
acid fast stain (−) | None | No
re-examination |
| 14/F/30 | None | Cough | RML+RIL | Max: 2.1×2.0;
around nodule: 0.6–1.0 | 4 | Two masses with
clusters of satellite lesions along bronchus, one mass with halo
sign, another with lobulation | Infected
lesion | Paracentesis | Granulomatous
lesions, organized lesions, Cryptococcus in macrophages, PAS
(+) | Fluconazole for 10
months | No
re-examination |
| 15/M/51 | None | None | LIL | Max: 1.6×1.3;
around nodules: 0.1–0.5 | 5 | A nodule with
clusters of satellite lesions along bronchus, lobulation, spicule,
pleural indentation, blood vessel convergence, calcification | Lung cancer with
intrapulmonic metastasis | Operation | Granulomatous
lesions with necrosis, Cryptococcus in necrotic tissue PAS
(+), acid fast stain (−) | None | No
re-examination |
| 16/F/44 | Non-Hodgkin
lymphoma | Elevated
temperature | LIL | Max:1.3×1.2; around
nodule: 0.6–1.0 | 3 | Three masses with
clusters of round satellite lesions along bronchus, lobulation in
certain instances, irregular margin, cavity, halo sign, blood
vessel convergence | Infected
lesion | Paracentesis | Granulomatous
lesions, organized lesions, Cryptococcus in macrophages, PAS
(+) | Fluconazole for 13
months | Significant
reduction and disappearance |
| 17/M/50 | None | None | RUL | Max: 2.5×1.6;
around nodule: 1.1–1.5 | 8 | A near-pleural mass
with clusters of satellite lesions along bronchus, lobulation in
certain instances | Infected
lesion | Paracentesis | Granulomatous
lesions, Cryptococcus in macrophages, foam cells in alveolar
space, PAS (+), acid fast stain (−) | Fluconazole for 5
months | No
re-examination |
| 18/M/60 | Non-Hodgkin
lymphoma | None | RML | Max: 1.7×1.5;
around nodule: 0.1–0.5 | 6 | A mass with
clusters of round satellite lesions along bronchus, some with
lobulation, halo sign, blood vessel convergence | Infected
lesion | Operation | Granulomatous
lesions with necrosis, Cryptococcus and Candidain
necrotic tissue, PAS (+), acid fast stain (−) | None | No
re-examination |
| 19/F/27 | None | Chest pain | LIL | Max: 4.6×4.1;
around nodule: 2.1–2.5 | 3 | Three near-pleural
masses, cavity, lobulation in certain instances | Tuberculosis | Paracentesis | Granulomatous
lesions with necrosis, Cryptococcus and Candidain
necrotic tissue, PAS (+), acid fast stain (−) | Fluconazole for 9
months | No
re-examination |
| 20/F/53 | Thyroid cancer
surgery; radioiodine therapy | Cough | RIL+LIL | Max: 2.7×2.5;
around nodule: 1.5–2.0 | 7 | Multiple round
nodules of unequal size, air bronchogram | Pulmonary
metastasis | Paracentesis | Granulomatous
lesions, Cryptococcus and Candidain necrotic tissue,
PAS (+), acid fast stain (−) | Fluconazole for 12
months | No
re-examination |
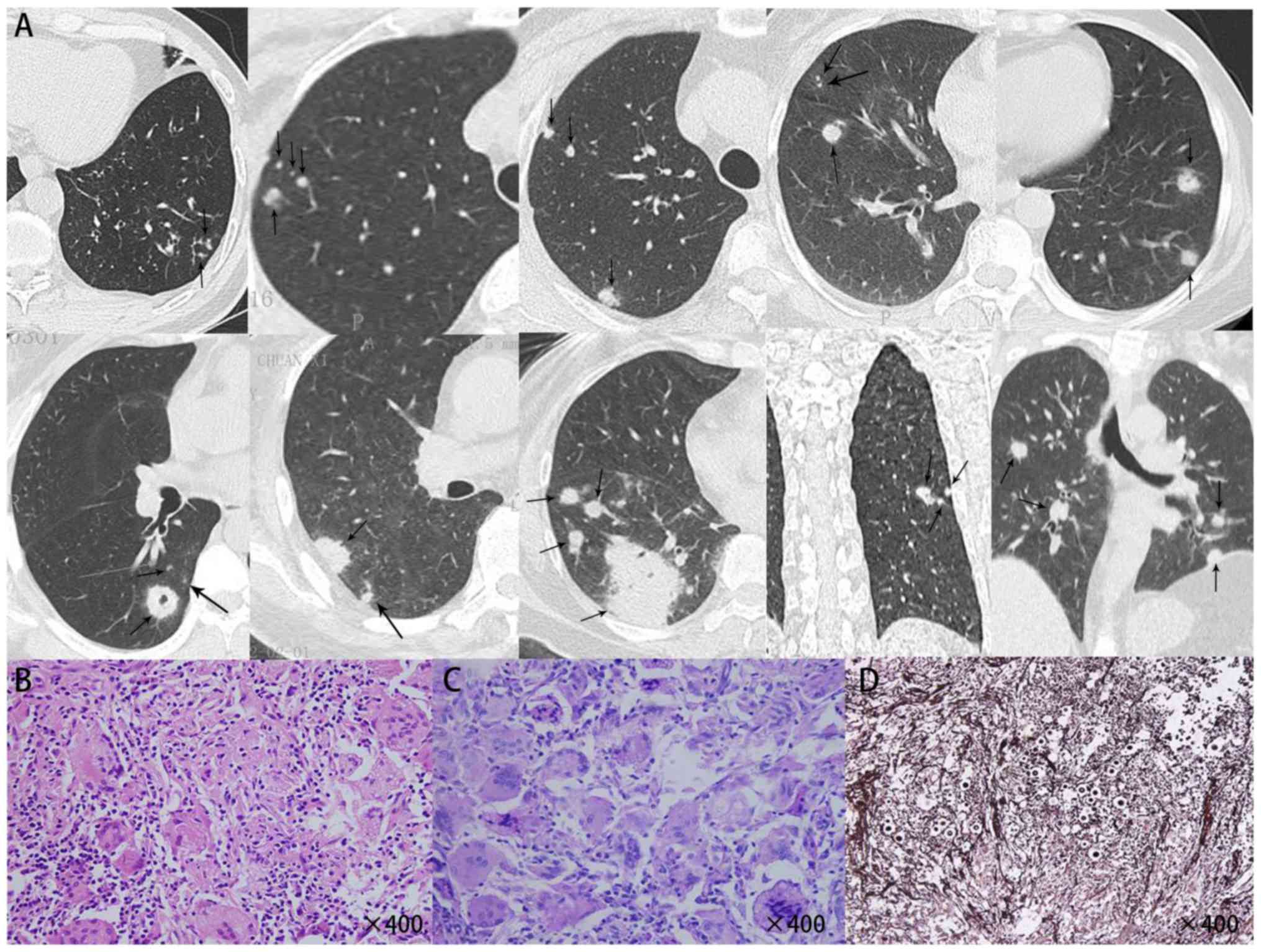
CT examination
The site of the lesion on chest CT was the right
upper lobe in 3 patients, the right middle lobe in 2 patients, the
right lower lobe in 4 patients, the left lower lobe in 5 patients,
the right upper lobe and left lower lobe in 2 patients, the right
middle lobe and right lower lobe in 1 patient, the right lower lobe
and left upper lobe in 1 patient, the right lower lobe and left
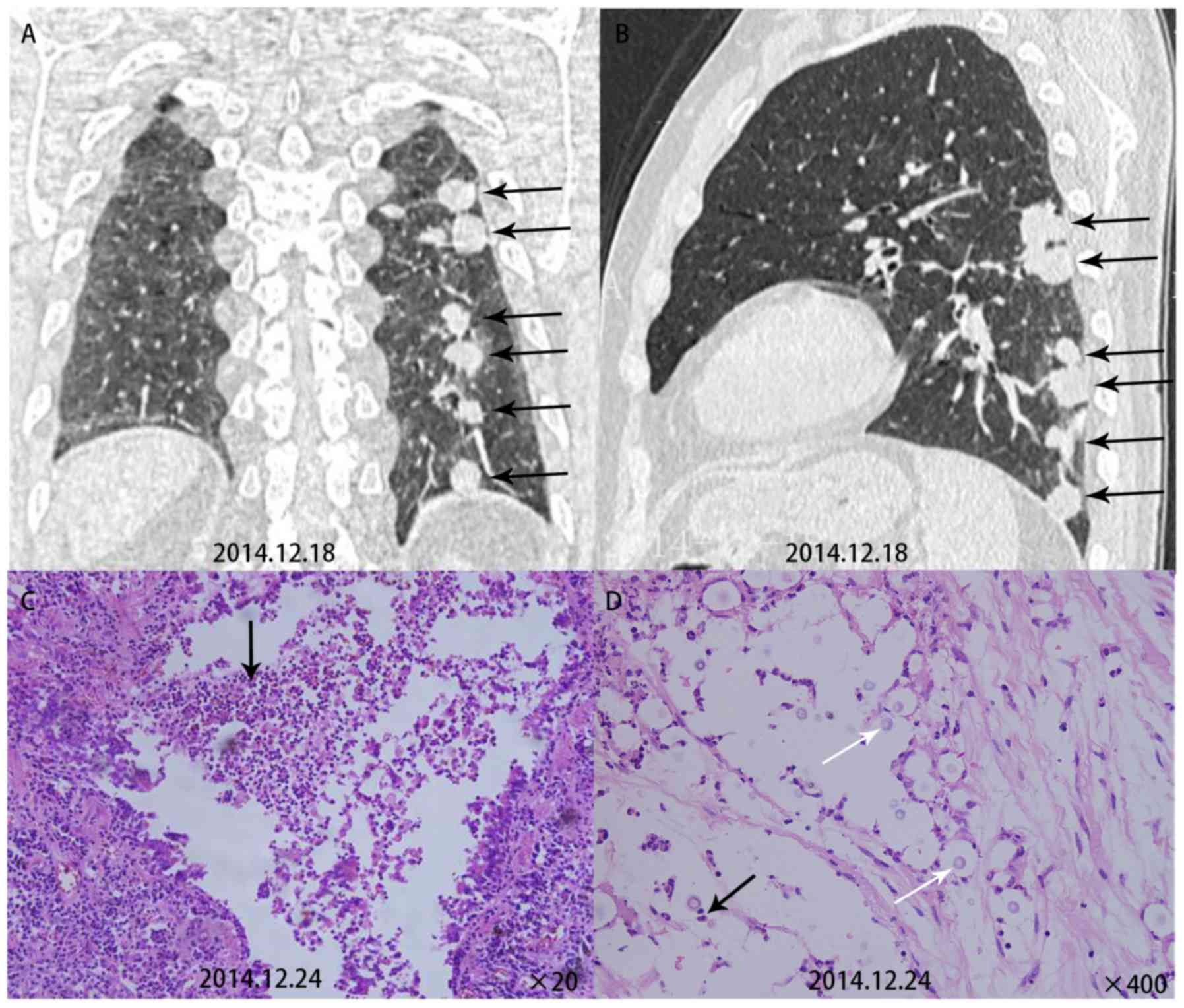
lower lobe in 1 patient, as well as all lobes in 1 patient. The
number of nodules or masses was 2–4 in 13 patients, 5–7 in 5
patients and 8–10 in 2 patients (Fig.
1). All primary lesions were located within 2 cm below the
pleura. The diameter range of the lesions was 0.1–1.0 cm in 7
patients, 1.1–2.0 cm in 9 patients, 2.1–3.0 cm in 6 patients and
>3.1 cm in 3 patients. The diameter range of the satellite
lesions was 0.1–0.5 cm in 7 patients, 0.6–1.0 cm in 5 patients,
1.1–1.5 cm in 3 patients, 1.6–2.0 cm in 4 patients and >2.1 cm
in 1 patient. Nodules were commonly round and distributed along the
bronchi. They presented with lobulation (11/20), irregular margins
(9/20), speculation (7/20), vascular convergence sign (4/20) and
pleural indentation (4/20). A total of 8 patients were misdiagnosed
with lung cancer accompanied by intrapulmonary metastasis;
accompanying calcificationin 2 patients and cavities in 4 patients
were also noted. A total of 3 patients were misdiagnosed with
pulmonary tuberculosis.
Treatment and histopathological
examination
Based on the characteristics of their imaging data,
8 of the 20 patients underwent segmental or wedge resection of the
lung and 12 underwent CT-guided percutaneous biopsy. All of them
underwent histopathological examination. HE staining indicated that
Cryptococcus neoformans-infested lesions were engulfed by
macrophages (Fig. 1), and around
them, a larger number of infiltrating lymphocytes were present,
which formed multinucleated macrophages or granulomas, which were
at times accompanied by coagulative necrosis. Specific staining
indicatedthat the lesions wereperiodic acid-Schiff (+), Giemsa (+)
andacid fast stain (−). A total of 5 patients underwent surgical
monotherapy, 12 patients underwent antifungal monotherapy and three
patients underwent surgery in combination with antifungal therapy.
Voriconazole 200–400 mg/day was administered for treatment. The
treatment period was 3–6 months in 6 patients, 6–12 months in 6
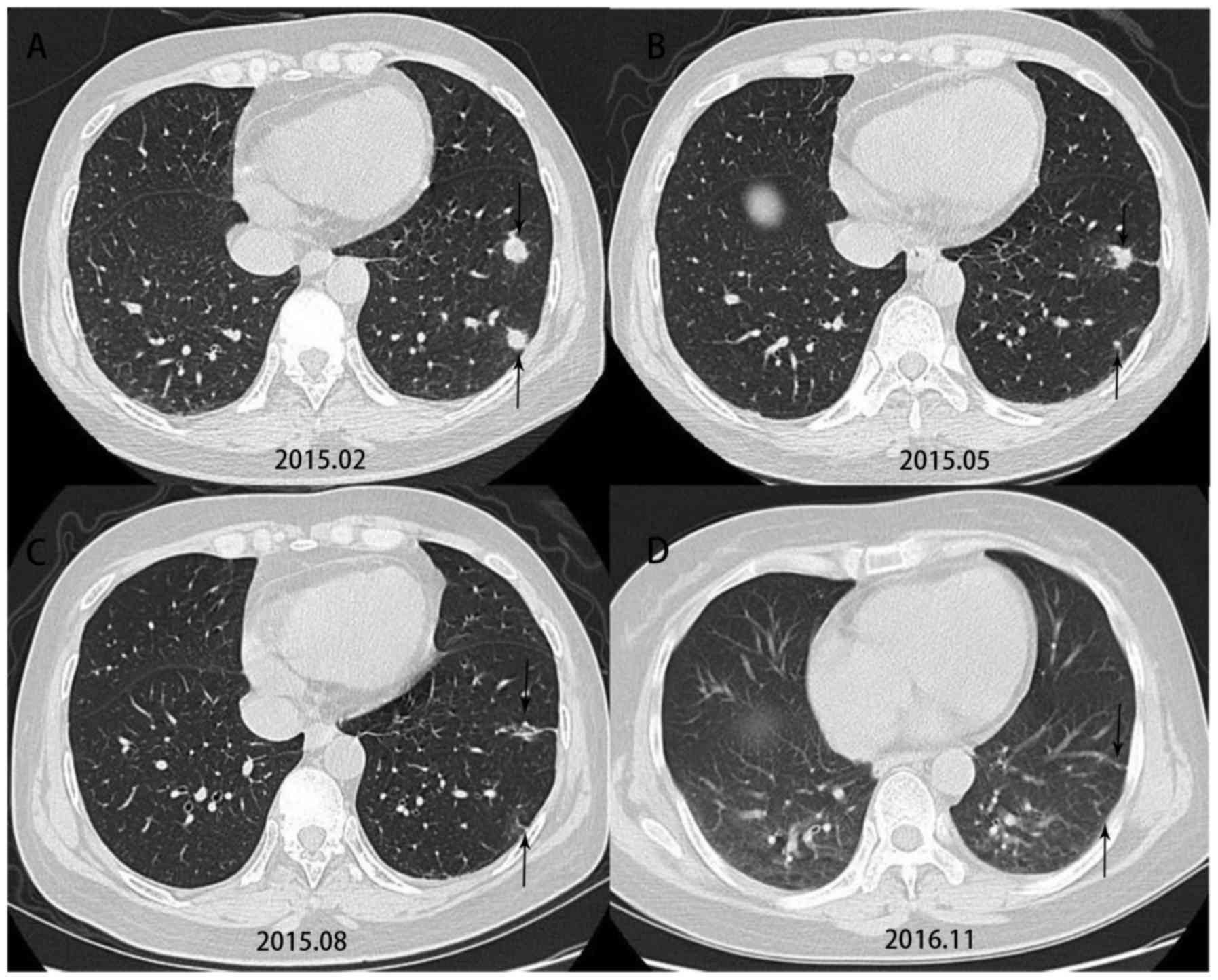
patients and >12 months in 3 patients. In Patient 16, the lesion
shrank significantly after antifungal therapy (Fig. 2). Except for one patient whose
follow-up result was unknown, noneof the other 19 patients had any
recurrence at follow-up.
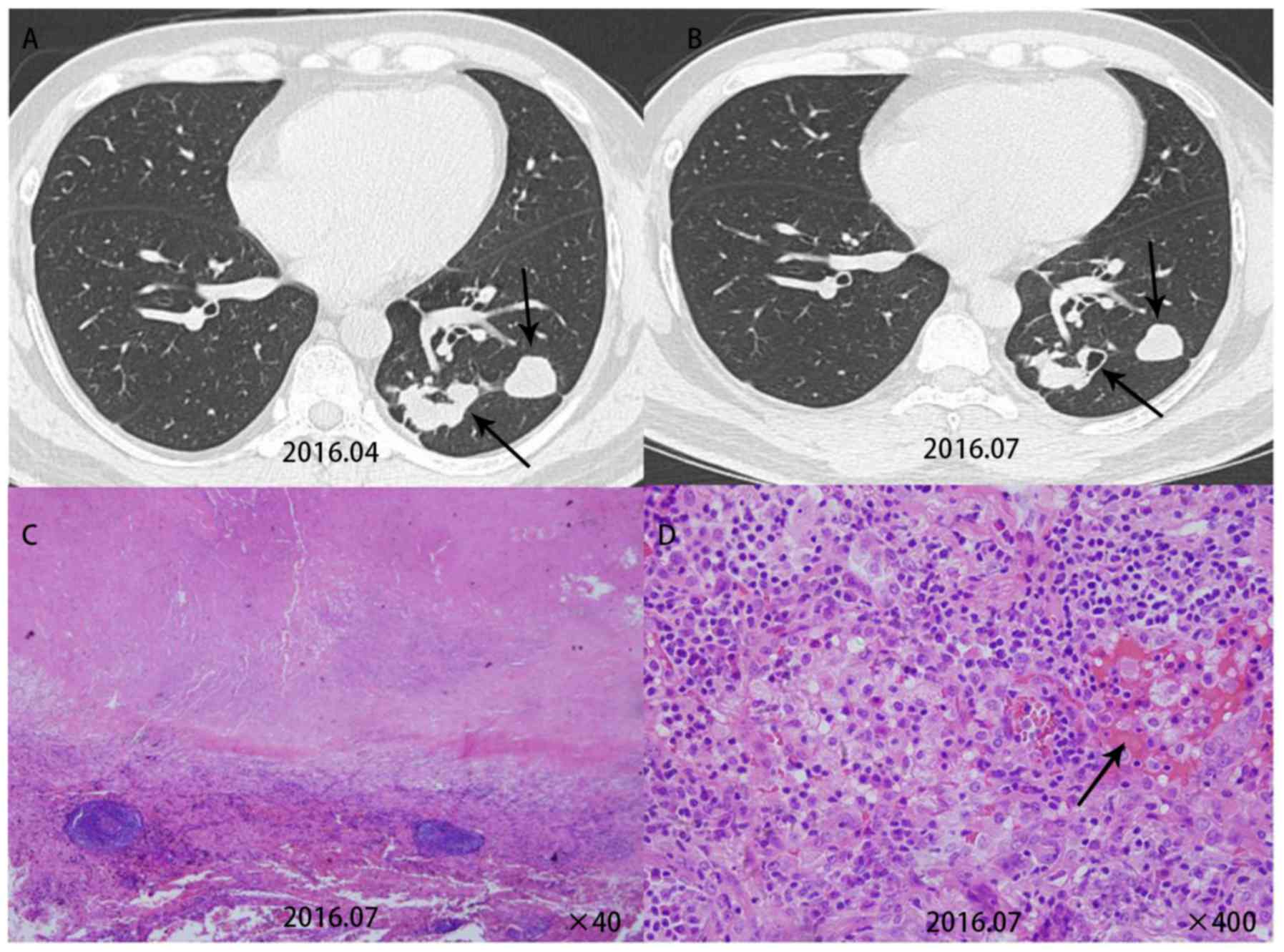
Comparison of CT with
histopathological results
Comparison of CT signs with the pathological
resultsindicated that it was possible to explain certain CT signs
by the pathological results. Patient 5 had multiple nodules in the
lower left lobe. A re-examination after three months revealed
cavities in this patient. This patient was then given surgical
treatment. Pathological examination for this patient revealed
cryptococcal granuloma accompanied by coagulative necrosis and
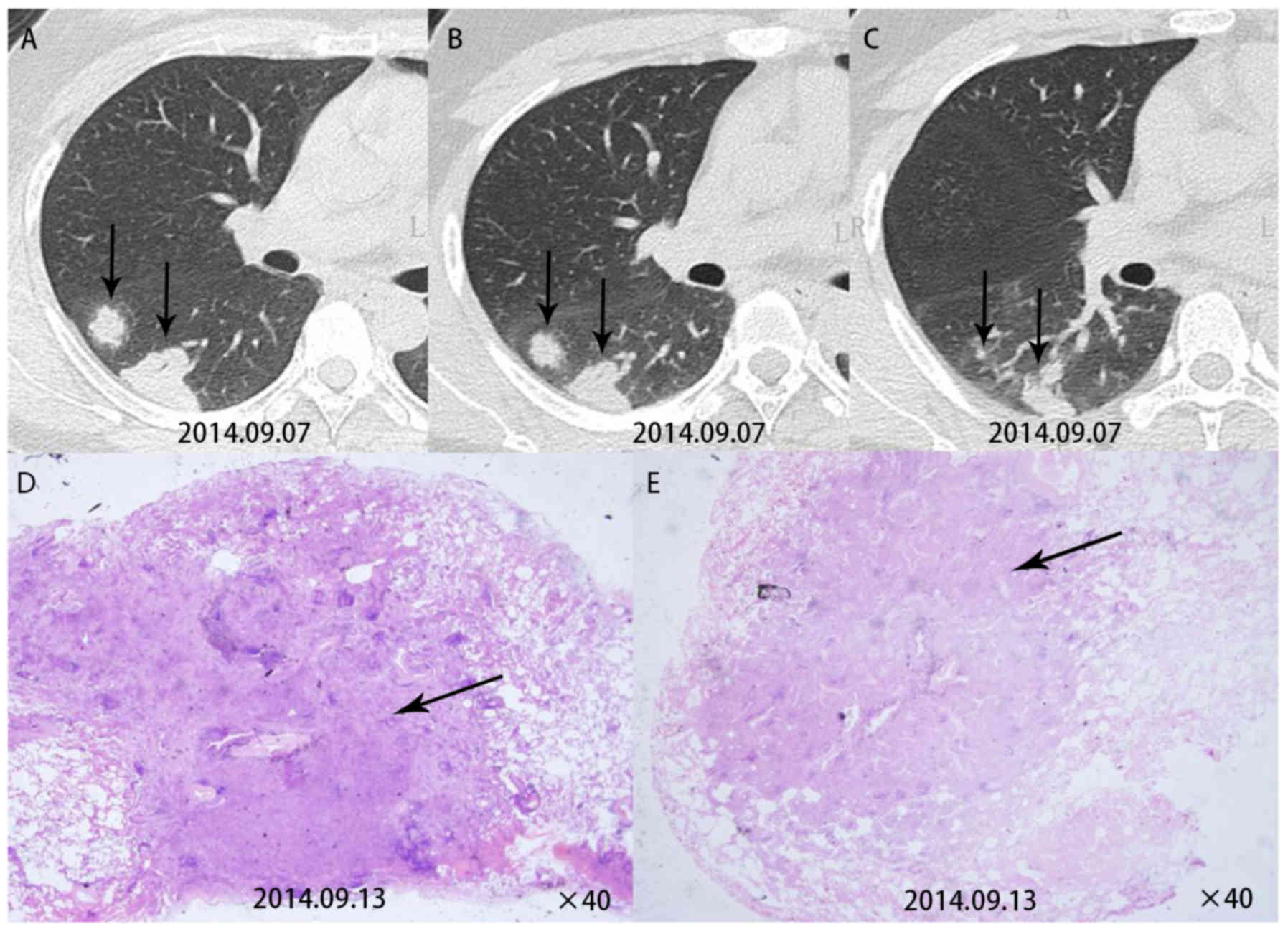
vasculitis formation (Fig. 3).
Patient 7 had multiple subpleural nodules in the dorsal segments of
the right lower lobe. A pathological examination for this patient
revealed inflammatory granulomas near the pleura (Fig. 4). Patient 9 had multiple round
nodules distributed along the bronchial tract. A pathological
examination for this patient revealed free Cryptococcus
neoformans in the bronchioles and lung alveoli (Fig. 5).
Discussion
As multislice CT is widely used, the detection rate
of pulmonary cryptococcosis is increasing year by year, and
mostinfected individuals are a population with abnormal immune
function (12). In line with this,
the present study also indicated that pulmonary cryptococcosis with
multiple nodules frequently occurred in a population with normal
immune function; 70% of the patients were males; 35% had underlying
diseases or susceptibility factors and 60% had clinical
symptoms.
Pulmonary cryptococcosis with multiple nodules has
diverse CT signs (13) and it is
prone to be misdiagnosed as lung cancer accompanied by
intrapulmonary metastasis or tuberculosis. However, pulmonary
cryptococcosis has certain unique characteristics: i) The lesion
commonly occurs in the right lung; ii) a cluster of lesions is
located within 2 cm below the pleura; iii) the primary lesion
commonly has a diameter of 1.1–2.0 cm. Satellite lesions are
usually smaller in diameter (commonly 0.1–1.0 cm). Round satellite
nodules are distributed along the bronchial tract, and no
tree-in-bud pattern is present; iv) cavities and calcification may
be caused.
Comparison between CT signs and pathological results
may enhance the understanding of how CT signs of the disease occur
and gain a deeper understanding of the disease. Due to the small
diameter of the spores of Cryptococcus neoformans (1–2 µm),
they are prone to be inhaled to reach the bronchioles and terminal
bronchioles (14), where they are
engulfed by a large number of macrophages around the tracts below
the bronchioles and within alveolar septa (15), to then form inflammatory granulomas
below the pleura. Thus, a typical CT manifestation is characterized
in that the lesion is mostly located within 2 cm below the pleura.
After Cryptococcus neoformans enters the body, its capsule
rapidly enlarges with its diameter reaching 4–10 µm order to
withstand phagocytosis by macrophages. It travels freely in the
bronchioles and lung alveoli and may be carried in streaming air to
reach other parts of the lung during breathing, thereby causing
bronchial dissemination. Furthermore, at the time that
Cryptococcus neoformans is initially inhaled into the lungs,
it may inhabit multiple sites of the lungs and then cause multiple
lesions distributed along the bronchi. Pathology images have
indicated that Cryptococcus neoformans may travel freely in
lung alveoli and terminal bronchioles, which may be the cause of
bronchial dissemination. Furthermore, inflammatory granulomas and
fibrous tissue are formed after Cryptococcus neoformans is
engulfed by macrophages. Fibrous tissues have contractile forces
(16), so that the lesion appears
rounded on CT, and the nodules are lobulated due to the unequal
contractile forces. Cryptococcus neoformans may form a
polysaccharide capsule as a protection against macrophage
phagocytosis and may not produce any substances, including mucus,
to block the bronchioles during the infection process (17). Thus, there was no tree-in-bud pattern
on CT. The pathology images contained a large number of
inflammatory cells around the blood vessels, whose infiltration
resulted in vasculitis to ultimately cause coagulative necrosis.
Therefore, cavities were observed on CT.
It is recommended that pulmonary cryptococcosis is
treated with oral fluconazole for antifungal therapy (18,19). The
regimen for fluconazole treatment is 200–400 mg/days for 3–6 months
for asymptomatic patients, 6–12 months forpatients with mild to
moderate symptoms and >12 months for patients with severe
pulmonary infection. Antifungal therapy with fluconazole is not
required for asymptomatic patients who have undergone surgery. For
those with symptoms who have undergone surgery, fluconazole is
administered at 200–400 mg/day for three months. According to our
experience, fluconazole is the best choice for the treatment of
this disease and there is no requirement for surgery.
In summary, pulmonary cryptococcosis with multiple
nodules or masses frequently occurs below the pleura. The circular
nodules distributed along the bronchi are mostly lobulated, and
cavities and calcifications may be present. As pulmonary
cryptococcosis is prone to being misdiagnosed as lung cancer or
tuberculosis, the pathological results may be used to explain the
CT signs so as to improve the understanding of this disease.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Qiqihar
Medical University Scientific Research Funding Program (grant no.
QY2016M-15), the Beijing Outstanding Young Talent Fund (grant no.
2014000021469G253), the National Natural Science Fund Youth Project
(grant no. 81700007), the Railway Head Corporation (grant no.
J2015C001-B) and the National Science and Technology Major Project
of China (grant no. 2015ZX09J15105-004). The funders had no role in
study design, datacollection and analysis, decision to publish or
preparation of the manuscript.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contribution
DW and XX conceived and designed the current study.
CW, SZ, XM and JG were responsible for the collection and analysis
of patient data. LF and YW collected the samples and performed
parts of the experiments. Lei Pan performed the experiments and
analyzed the results.
Ethical approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interest.
References
|
1
|
Kwon-Chung KJ, Fraser JA, Doering TL, Wang
Z, Janbon G, Idnurm A and Bahn YS: Cryptococcus neoformans and
Cryptococcus gattii, the etiologic agents of Cryptococcosis. Cold
Spring Harb Perspect Med. 4:a0197602014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gates-Hollingsworth MA and Kozel TR:
Serotype sensitivity of a lateral flow immunoassay for cryptococcal
antigen. Clin Vaccine Immunol. 20:634–635. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pappas PG: Cryptococcal infections in
non-HIV-infected patients. Trans Am Clin Climatol Assoc. 124:61–79.
2013.PubMed/NCBI
|
|
4
|
Lackner M, de Hoog GS, Yang L, Moreno
Ferreira L, Ahmed SA, Andreas F, Kaltseis M, Nagl M, Lass-Flörl C,
Risslegger B, Rambach G, et al: Proposed nomenclature for
Pseudallescheria, Scedosporium and related genera. Fungal
Diversity. 67:1–10. 2014. View Article : Google Scholar
|
|
5
|
Coelho C, Bocca AL and Casadevall A: The
intracellular life of cryptococcus neoformans. Annu Rev Pathol.
9:219–238. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kebede T and Reda N: Pulmonary
cryptococ-coma mimicking pulmonary malignancy in an immunocompetent
adult: A case report. Ethiop Med J. 50:275–278. 2012.PubMed/NCBI
|
|
7
|
McQuiston TJ and Williamson PR:
Paradoxical roles of alveolar macrophages in the host response to
Cryptococcus neoformans. J Infect Chemother. 18:1–9. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Perfect JR and Bicanic T: Cryptococcosis
diagnosis and a treatment: What do we know now. Fungal Genet Biol.
78:49–54. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yamakawa H, Yoshida M, Yabe M, Baba E,
Okuda K, Fujimoto S, Katagi H, Ishikawa T, Takagi M and Kuwano K:
Correlation between clinical characteristics and chest computed
to-mography findings of pulmonary cryptococcosis. Pulm Med.
2015:7034072015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Schweigert M, Dubecz A, Beron M, Ofner D
and Stein HJ: Pulmonary infections imitating lung cancer: Clinical
presentation and therapeutical approach. Ir J Med Sci. 182:73–80.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hector A, Kirn T, Ralhan A,
Graepler-Mainka U, Berenbrinker S, Riethmueller J, Hogardt M,
Wagner M, Pfleger A, Autenrieth I, et al: Microbial colonization
and lung function in adolescents with cystic fibrosis. J Cyst
Fibros. 15:340–349. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
La Hoz RM and Pappas PG: Cryptococcal
infections: Changing epidemiology and implications for therapy.
Drugs. 73:495–504. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tseng HK, Liu CP, Ho MW, Lu PL, Lo HJ, Lin
YH, Cho WL and Chen YC; Taiwan Infectious Diseases Study Network
for Cryptococcosis, : Microbiological, epidemiological, and
clinical characteristics and outcomes of patients with
cryptococcosis in Taiwan, 1997–2010. PLoS One. 8:e619212013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zaragoza O, Rodrigues ML, De Jesus M,
Frases S, Dadachova E and Casadevall A: The capsule of the fungal
pathogen Cryptocoecus neoformans. Adv Appl Miembiol. 68:133–216.
2009. View Article : Google Scholar
|
|
15
|
Ma H and May RC: Virulence in cryptococcus
species. Adv Appl Micmbiol. 67:131–190. 2009. View Article : Google Scholar
|
|
16
|
Xie X, Xu B, Yu C, Chen M, Yao D, Xu X,
Cai X, Ding C, Wang L and Huang X: Clinical analysis of pulmonary
cryptococcosis in non-hiv patients in south china. Int J Clin Exp
Med. 8:3114–3119. 2015.PubMed/NCBI
|
|
17
|
Chang CC, Sorrell TC and Chen SC:
Pulmonary cryptococcosis. Semin Respir Crit Care Med. 36:681–691.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brizendine KD, Baddley JW and Pappas PG:
Predictors of mortality and differences in clinical features among
patients with Cryptococcosis according to immune status. PLoS One.
8:e604312013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Perfect JR: Fungal diagnosis: How do we do
it and can we do better? Curr Med Res Opin. 4 Suppl 29:1–11.
2013.
|