Introduction
Infantile hemangioma is one of the most common
benign tumors affecting children, occurring in 4–10% of all infants
and ~10–15% require medical treatment (1,2). The
tumors consist of endothelial cells and stromal components,
including fibroblasts, pericytes and mast cells (3,4).
Following the proliferation phase, endothelial cells are replaced
with adipocytes, which subsequently determine the involution of the
tumor (5).
Before 2008, various therapies have been established
to treat infantile hemangioma, including cortisone, vincristine,
interferon-α and lasertherapy; however, these therapeutic
treatments have been demonstrated to be associated with potentially
severe adverse side effects (5).
Following reports on antiproliferative effects of propranolol by
Léauté-Labrèze et al (6) in
2008, various studies have been performed investigating the
mechanisms by which propranolol induces the involution of
hemangiomas (1,2). Propranolol is a non-selective β-blocker
used worldwide as the first-line therapy for hemangiomas (5). Several mechanisms, including
vasoconstriction, blocking of proangiogenic signals and induction
of apoptosis, have been suggested as underlying mechanisms
(2).
Vincristine is a chemotherapeutical agent that
inhibits endothelial cell growth by blocking mitosis and the
formation of microtubules by direct cytotoxicity (7). Furthermore, vincristine is used as a
second or third-line therapeutical agent in life-threatening
situations, including severe bleeding, blocked airway or Kassabach
Meritt syndrome, or in steroid-resistant and steroid-dependent
hemangiomas (8).
It has been established that the vascular
endothelial growth factor (VEGF) and basic fibroblastic growth
factor (bFGF) stimulate cell proliferation, which subsequently
results in the growth of hemangiomas (5). A well-studied antiangiogenic treatment
is bevacizumab, a humanized monoclonal antibody that binds to VEGF
and inhibits angiogenesis (9).
Bevacizumab is used in treating certain types of cancer, including
colon or lung cancer, affecting adults (9). Treatment of patients with hemangiomas
has not been studied extensively (10).
The aim of the present study was to assess effects
of propranolol on human umbilical vein endothelial cells (HUVECs)
and BJ human normal fibroblasts (BJs). Furthermore, the efficacy of
vincristine and bevacizumab in combination with propranolol was
assessed. To investigate the activity of the drugs and various drug
combinations, the present study established an in vitro
model consisting of normal fibroblasts and HUVECs to mimic the
primary source of hemangiomas. Effects of propranolol, a clinically
approved hemangioma treatment, on cell growth were compared with
bevacizumab, aVEGF inhibitor, and vincristine, a mitosis inhibitor.
Effects of various treatment combinations were evaluated to
determine potential synergic effects.
Materials and methods
Cell cultures
BJs (CRL-2522) were purchased from the American Type
Culture Collection (Manassas, VA, USA) and HUVECs were provided by
Dr. Olga Soritau, from the Oncology Institute ‘I. Chiricuță’
(Cluj-Napoca, Romania) established from a primary source at the
European Collection of Authenticated Cell Cultures (Salisbury,
UK).
BJs were cultured at 37°C in a 5% CO2
incubator in Eagle's Minimum Essential medium (MEM, Sigma-Aldrich;
Merck KGaA, Darmstadt, Germany) and HUVECs were cultured in
Endothelial Cell Growth medium (ECG, Cell Applications, Inc., San
Diego, CA, USA); media were supplemented with 10% fetal calf serum
(Sigma-Aldrich; Merck KGaA).
Cells were trypsin-digested at 75–85% subconfluency
and seeded at 12×103 cells/well in 96-well plates with
190 µl media (as described above). BJs were passaged 9–12 times and
HUVECs were passaged 18–20 times. Passages were performed twice a
week and no replacement of media was performed in between.
Drug preparations
Vincristine sulfate was purchased from Sindan Pharma
SRL (Sindovin; Bucharest, Romania). A total of 1 mg vincristine
(excipient, anhydrous lactose monohydrate) was dissolved in 500 µl
ultrapure water (Lonza Group, Ltd., Basel, Switzerland) to obtain a
2,000 µg/ml stock and serial dilutions (1,000, 750, 500, 250, 125,
62.5, 32 and 16 µl/ml) were prepared with PBS. Concentrations in
the culture medium were 100, 50, 25, 12.5, 6.25, 3.12, 1.6 and 0.8
µg/ml.
Propranolol chloral hydrate was purchased from
Sintofarm SA (Propranolol; Bucharest, Romania). A total of 40 mg
propranolol (excipients, lactose monohydrate, microcrystalline
cellulose and cornstarch) was dissolved in 1,000 µl of ultrapure
water to obtain a 40 mg/ml stock. Serial dilutions between
2,000-15.6 µl/ml (2,000, 1,000, 500, 250, 125, 62.5, 31.25 and 15.6
µl/ml) were prepared in PBS. In vitro drug concentrations
were extrapolated from in vivo doses based on previous
studies (11–13).
Bevacizumab was purchased from Roche Applied Science
(Avastin; Penzberg, Germany) and provided as a 25 mg/ml solution in
water, containing excipients including trehalose dihydrate, sodium
phosphate and polysorbate 20. Serial dilutions were prepared using
the 25 mg/ml stock solution to obtain final concentrations between
19.5–2,500 µg/ml in cell culture medium.
Various propranolol concentrations were combined
with a subcytotoxic concentration of vincristine and bevacizumab.
All aforementioned propranolol concentrations were combined with
subcytotoxic 10 µg/ml vincristine or 100 µg/ml bevacizumab.
Cytotoxicity measurements
For single drug treatments, medium was removed from
the wells and replaced with 10 µl drug stock in PBS plus 190 µl of
ECG for HUVECs and MEM for BJs, respectively. For combination
treatments, medium was replaced with 10 µl of each drug stock
solution in PBS plus 180 or 170 µl medium for dual or triple drug
combinations, respectively. When cells were adherent to 96-well
plates, drug treatments were administered for 24 h at 37°C as
follows: in pairs; propranolol with vincristine, propranolol with
bevacizumab and vincristine with bevacizumab; or with all three
administered together. Cytotoxicity was then measured. Assays were
performed in triplicate with untreated, viable cells used as
negative controls. Blanks were based on cell culture media and were
recorded in parallel.
Following incubation with the treatment, plates were
subjected to MTT analyses (Sigma-Aldrich; Merck KGaA) according to
a previously described protocol (14). Formazan crystals were dissolved in
150 µl dimethyl sulfoxide (Titolchimica, Pontecchio Polesine,
Italy) and the intensity of coloration was measured
spectrophotometrically, at 570 nm. Coloration is directly
proportional to the number of living cells and resulting absorbance
values were used to determine half inhibitory concentration
(IC50) values from dose-response curves usingGraph Pad
Prism 5 (GraphPad Software, Inc., La Jolla, CA, USA).
Apoptosis induction
Apoptotic and necrotic cell counts in treated BJs
and HUVECs were determined by flow cytometry using the Alexa Fluor
488 Annexin V/propidium iodide (PI) Apoptosis kit (Invitrogen;
Thermo Fisher Scientific, Inc.) following a previously described
method (15). BJs and HUVECs were
incubated in six-well plates at 2×105 cells/ml in 3 ml
media for 24 h and treated with the following drugs for 24 h: 50
µg/ml propranolol, 10 µg/ml vincristine, 50 µg/ml bevacizumab,
propranolol (50 µg/ml) plus vincristine (10 µg/ml), propranolol (50
µg/ml) plus bevacizumab (50 µg/ml), vincristine (10 µg/ml) plus
bevacizumab (50 µg/ml) and propranolol (50 µg/ml) plus vincristine
(10 µg/ml) plus bevacizumab (50 µg/ml). Untreated cells were used
as a negative control. Following treatment, cells were harvested,
washed with Binding Buffer provided by the kit, incubated for 15
min at room temperature with Alexa Fluor 488-labeled Annexin V and
PI. Samples were subjected to analysis using the FACS Canto II
flow-cytometer (Becton Dickinson; BD Biosciences; Franklin Lakes,
NJ, USA). Two experiments were performed per treatment and mean
values were determined using FACS Canto software (BD FACS Diva
version 6.1; Becton Dickinson; BD Biosciences). AlexaFluor
488-labeled apoptotic cells were identified and analyzed using a
530/30 nm filter and PI-labeled necrotic cells were detected using
a 575/26 nm filter.
Statistical analysis
Statistical analyses were performed using GraphPad
Prism5 (GraphPad Software, Inc.). IC50 values were
determined as the mean ± standard deviation, by performing a
non-linear regression analysis on the logarithm of the
concentration vs. the normalized absorbance. Each value was
determined in triplicate and three independent measurements were
performed. Cell growth rates were compared using one-way analysis
of variance and Dunnett's multiple comparison test, with untreated
cells as reference and using a 95% confidence interval (CI). For
apoptosis evaluation, 10,000 individual single-cell measurements
were evaluated and comparisons are based on one-way analysis of
variances followed by Bonferroni post-hoc tests using a 95% CI.
Correlation between the number of early apoptotic cells, late
apoptotic cells and dead cells was assessed using a nonparametric
Spearman correlation with a 95% CI. P<0.05 was considered to
indicate a statistically significant result.
Results
Cell growth inhibition
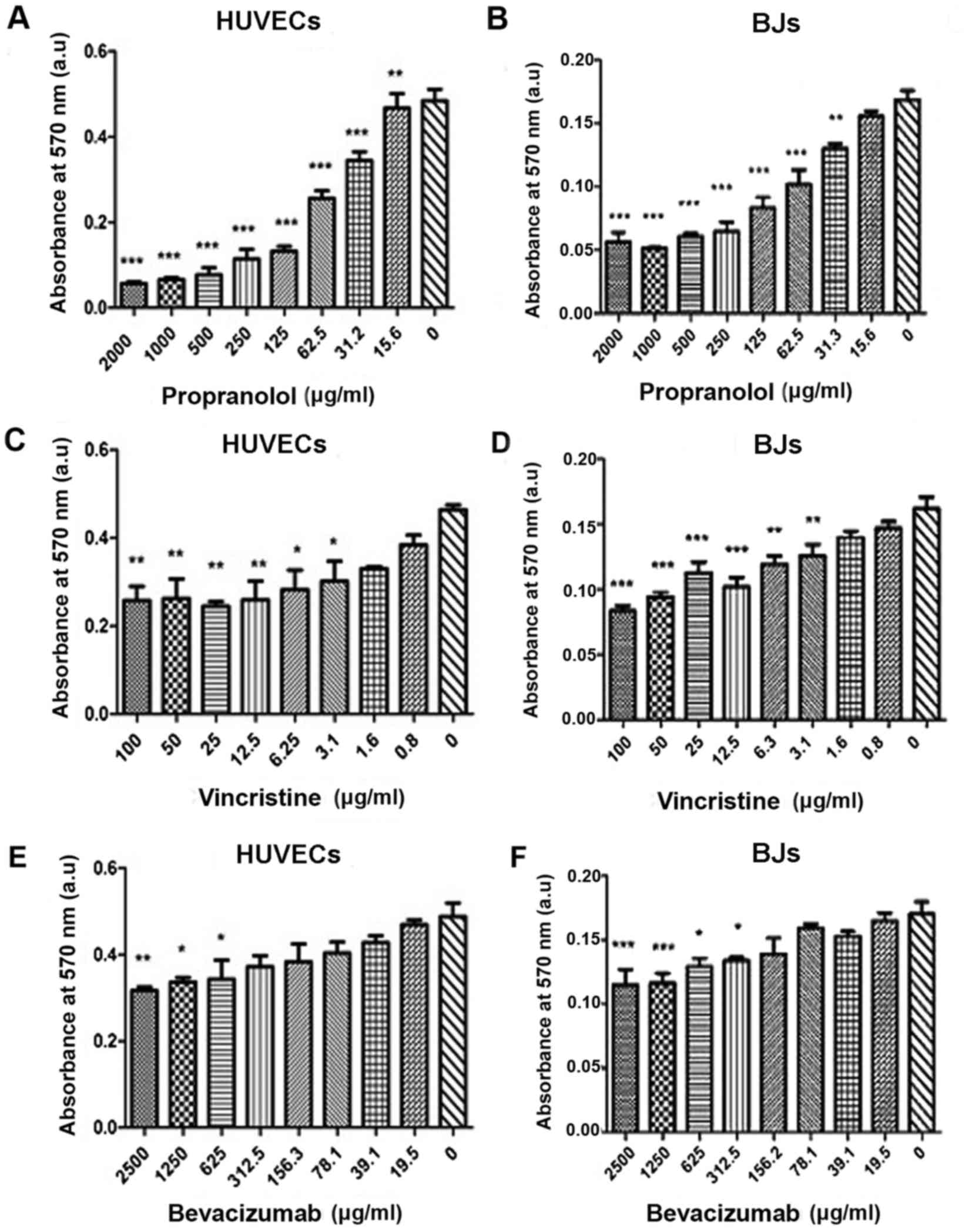
In vitro cytotoxicity was determined for
propranolol, vincristine and bevacizumab using HUVECs and BJs to
determine novel therapeutic strategies. Following treatment with
various propranolol concentrations (15.6–2,000 µg/ml), as
aforementioned, results revealed that the β-blocker inhibited
growth of BJs and HUVECs in a dose-dependent manner (Fig. 1A and B, respectively). A more marked
effect was observed in BJs compared with HUVECs. Vincristine
inhibited growth in >50% of cell populations for BJs and HUVECS
at 100 µg/ml (Fig. 1C and D).
Bevacizumab was revealed to be the weakest cytotoxic agent in the
tested cell lines compared with propranolol and vincristine
(Fig. 1E and F).
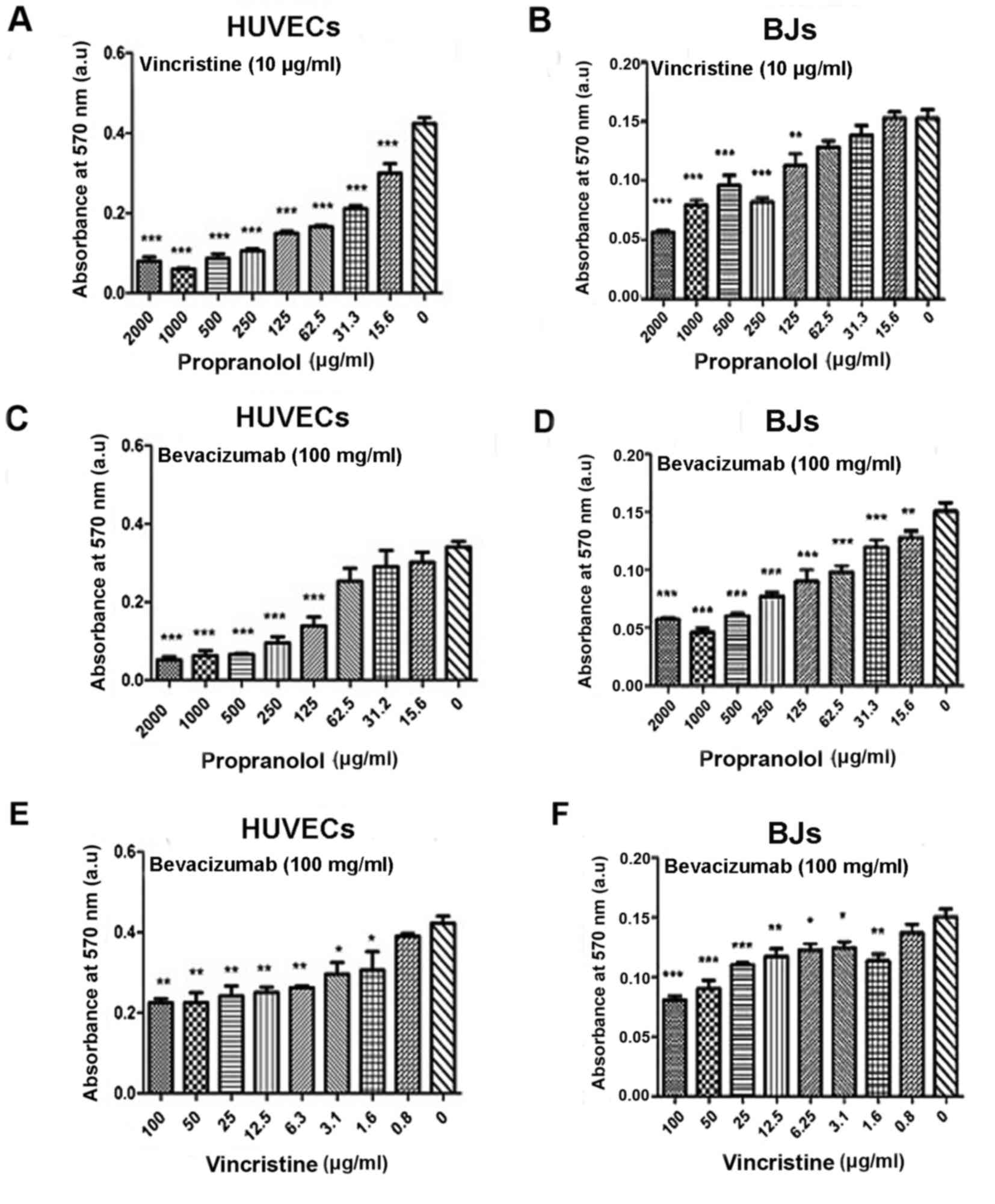
In order to investigate effects of combined
treatments, various concentrations of propranolol, as
aforementioned, were administered in combination with sublethal
concentrations of vincristine (10 µg/ml) or bevacizumab (100 µg/ml)
to BJs und HUVECs (Fig. 2).
Nonlinear dose-response curves were generated to
determine IC50 values for the various drug treatments
using BJs and HUVECs (Table I).
Decreased IC50values indicate higher levels of
cytotoxicity. In every IC50 value evaluation, the absorbance
measurement of the untreated cells served as the reference value
for 100% viability. Therefore on every sigmoidal curve, which
generates the IC50 value, measurements correspond to the untreated
cells. The results confirmed a significantly increased treatment
effect of propranolol when combined with vincristine (10 µg/ml) or
bevacizumab (100 µg/ml) compared with the propranolol alone
(Table I). IC50 values
were lower in HUVECs compared with BJs, following treatment with
propranolol. Following combination treatment with bevacizumab or
vincristine, IC50 values in BJs decreased, increasing
the cytotoxic treatment effect by 72.35 and 63.74%, respectively.
In comparison, the percentages in HUVECs were lower in combination
treatment, the cytotoxic effect was increased only by 19.52% with
bevacizumab and 33.49% with vincristine. In HUVECs and BJs, triple
treatment with propranolol, bevacizumab and vincristine resulted in
a decreased IC50 compared with the single propranolol
treatment and cytotoxicity increased by 94.78 and 89.55%,
respectively (data not shown).
 | Table I.IC50 values determined in
HUVECs and BJs treated with propranolol, vincristine and
bevacizumab and combinations of the drugs. |
Table I.
IC50 values determined in
HUVECs and BJs treated with propranolol, vincristine and
bevacizumab and combinations of the drugs.
|
| IC50
(µg/ml) |
|---|
|
|
|
|---|
| Treatment | BJs | HUVECs |
|---|
| Propranolol |
148.32±0.07aaa |
81.94±0.06aaa |
| Vincristine |
24.81±0.08aaa |
17.89±0.07aa |
| Bevacizumab |
182.70±0.09b |
96.91±0.06b |
| Propranolol plus
vincristine (10 µg/ml) |
53.78±0.06b |
54.50±0.06aaa |
| Propranolol plus
bevacizumab (100 µg/ml) |
41.01±0.05aaa |
65.95±0.03b |
| Vincristine plus
bevacizumab (100 µg/ml) |
17.73±0.10aaa |
9.77±0.07aa |
| Propranolol plus
vincristine (10 µg/ml) plus bevacizumab (100 µg/ml) |
7.73±0.11aaa |
8.56±0.04aaa |
Apoptosis induction
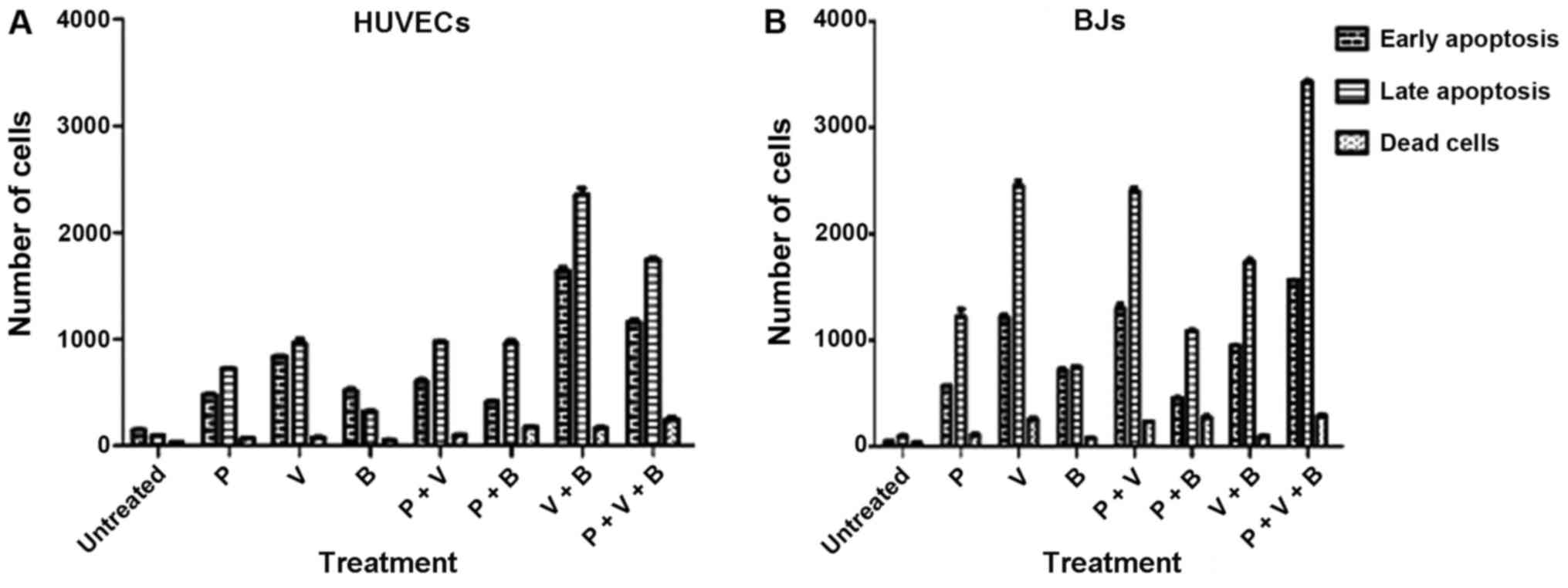
Following 24 h treatment, apoptosis levels were
determined in HUVECs and BJs, treated with one therapeutic agent or
a combination of them. In the present study, the number of cells in
early apoptotic stages following treatment was markedly increased
compared with the untreated control samples (Figs. 3 and 4). Vincristine was the most potent inducer
of programmed cell death in HUVECs and BJs in vitro compared
with the propranolol and bevacizumab treated group (P<0.001;
Table II). When using combination
treatment, vincristine plus bevacizumab induced the highest levels
of apoptosis in HUVECs (Figs. 3G,
4G and 5), in comparison with the BJs where triple
therapy was most effective. In addition, the results revealed that
among all single drug treatments, with either propranolol,
vincristine or bevacizumab, the greatest number of HUVECs found in
the late apoptotic stage was when using vincristine (P<0.001;
Table II). This observation was
similar to the number of HUVECs found in the late apoptotic stage
following combination treatment with propranolol plus vincristine.
Treatment with vincristine plus bevacizumab was revealed to
significantly increase cell numbers in late stage apoptosis
compared with mono-treatments, combination treatment of propranolol
plus vincristine and triple treatment (P<0.05; Table II and Fig. 5).
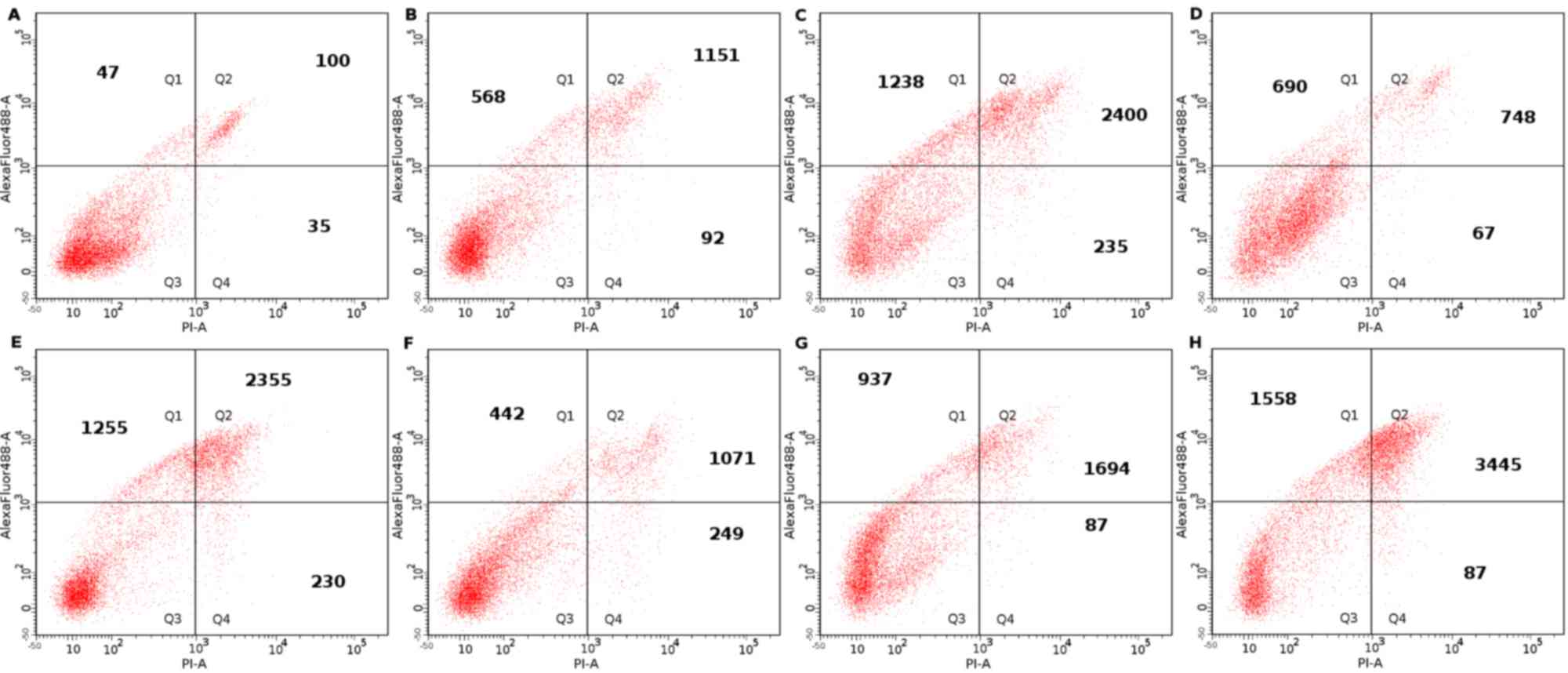
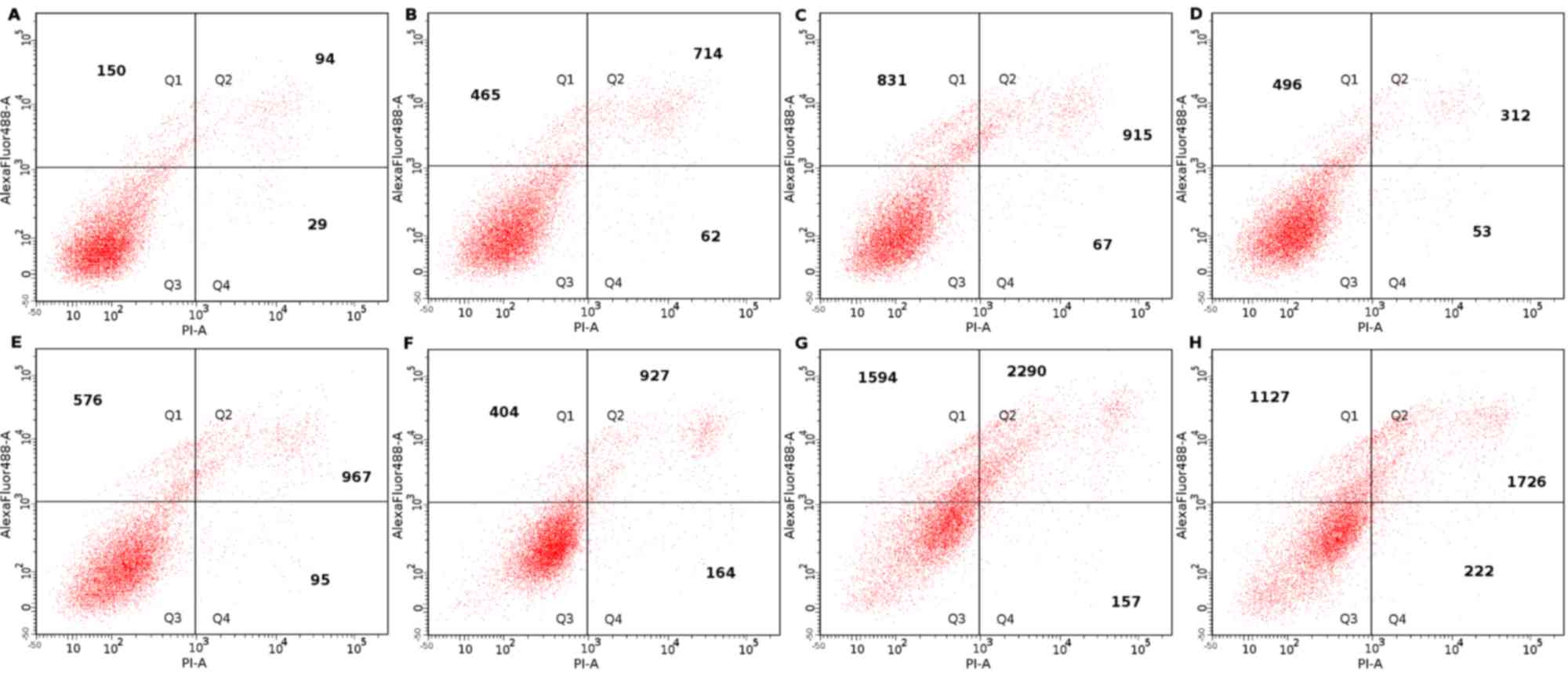 | Figure 3.Apoptosis evaluation of HUVECs
treated with propranolol, vincristine and bevacizumab and
combinations of the drugs. Representative images of flow
cytometry-based apoptosis evaluation of HUVECs (A) untreated or
treated with (B) propranolol (50 µg/ml), (C) vincristine (10
µg/ml), (D) bevacizumab (50 µg/ml), (E) propranolol (50 µg/ml) plus
vincristine (10 µg/ml), (F) propranolol (50 µg/ml) plus bevacizumab
(50 µg/ml), (G) vincristine (10 µg/ml) plus bevacizumab (50 µg/ml),
and (H) propranolol (50 µg/ml) plus vincristine (10 µg/ml) plus
bevacizumab (50 µg/ml). HUVECs, human umbilical vein endothelial
cell; Q1, quadrant representative of early apoptosis; Q2, quadrant
representative of late apoptosis; Q3, quadrant representative of
viable cells; Q4, quadrant representative of dead cells. |
 | Figure 4.Apoptosis evaluation of BJs treated
with propranolol, vincristine and bevacizumab and combinations of
the drugs. Representative images of flow cytometry-based apoptosis
evaluation of BJs (A) untreated or treated with (B) propranolol (50
µg/ml), (C) vincristine (10 µg/ml), (D) bevacizumab (50 µg/ml), (E)
propranolol (50 µg/ml) plus vincristine (10 µg/ml), (F) propranolol
(50 µg/ml) plus bevacizumab (50 µg/ml), (G) vincristine (10 µg/ml)
plus bevacizumab (50 µg/ml), and (H) propranolol (50 µg/ml) plus
vincristine (10 µg/ml) plus bevacizumab (50 µg/ml). BJ, CRL-2522
human normal fibroblast; Q1, quadrant representative of early
apoptosis; Q2, quadrant representative of late apoptosis; Q3,
quadrant representative of viable cells; Q4, quadrant
representative of dead cells. |
| Table II.Number of apoptotic and dead HUVECs
and BJs treated with propranolol, vincristine and bevacizumab and
combinations of the drugs, determined by flow cytometry. |
Table II.
Number of apoptotic and dead HUVECs
and BJs treated with propranolol, vincristine and bevacizumab and
combinations of the drugs, determined by flow cytometry.
| A, Early apoptotic
cells within a population of 10,000 cells |
|---|
|
|---|
| Treatment | HUVECs | BJs | R | P-value |
|---|
| Untreated | 150±3 | 47±4 |
|
|
| Propranolol | 465±14c | 568±2c |
|
|
| Vincristine | 831±6c |
1238±34c |
|
|
| Bevacizumab | 496±27c | 690±31c |
|
|
| Propranolol plus
vincristine (10 µg/ml) | 576±31c |
1255±58c |
|
|
| Propranolol plus
bevacizumab (50 µg/ml) | 404±12c | 442±13c |
|
|
| Vincristine plus
bevacizumab (50 µg/ml) |
1,594±53c | 937±8c |
|
|
| Propranolol plus
vincristine (10 µg/ml) plus bevacizumab (50 µg/ml) |
1,127±41c | 1558±4c | 0.833 | 0.077 |
|
| B, Late
apoptotic cells within a population of 10,000 cells |
|
|
Treatment | HUVECs | BJs | R | P-value |
|
| Untreated | 94±2 | 100±11 |
|
|
| Propranolol | 714±8c |
1151±98c |
|
|
| Vincristine | 915±58c |
2400±69c |
|
|
| Bevacizumab | 312±10b | 748±4c |
|
|
| Propranolol plus
vincristine (10 µg/ml) | 967±7c |
2355±57c |
|
|
| Propranolol plus
bevacizumab (50 µg/ml) | 927±44c |
1071±14c |
|
|
| Vincristine plus
bevacizumab (50 µg/ml) |
2290±86c |
1694±50c |
|
|
| Propranolol plus
vincristine (10 µg/ml) plus bevacizumab (50 µg/ml) |
1726±22c |
3445±27c | 0.743 | 0.0288 |
|
| C, Dead cells
within a population of 10,000 cells |
|
|
Treatment | HUVECs | BJs | R | P-value |
|
| Untreated | 29±3 | 35±2 |
|
|
| Propranolol | 62±6d | 92±16a |
|
|
| Vincristine | 67±9d | 235±23c |
|
|
| Bevacizumab | 53±1d | 67±9d |
|
|
| Propranolol plus
vincristine (10 µg/ml) | 95±4b | 230±1c |
|
|
| Propranolol plus
bevacizumab (50 µg/ml) | 164±10c | 249±27c |
|
|
| Vincristine plus
bevacizumab (50 µg/ml) | 157±12c | 87±7a |
|
|
| Propranolol plus
vincristine (10 µg/ml) plus bevacizumab (50 µg/ml) | 222±32c | 267±22c | 0.895 | 0.0109 |
In BJs, treatment with vincristine, vincristine plus
propranolol and triple treatment increased the number of cells in
late stage apoptosis to the greatest extent, when compared with the
other cycle cell stages (P<0.05; Table II; Fig.
5).
Propranolol in combination treatments resulted in
increased cell death, compared with combination treatments without
Propranolol; however, as subcytotoxic concentrations of propranolol
were used, the number of dead cells were lower, indicating
increased apoptosis (Figs.
3–5).
Furthermore, the results revealed that there was a
correlation between HUVECs and BJs regarding the number of cells in
early stage apoptosis at varying treatment options (Spearman
r-factor, 0.833; P=0.077; Table
II). Correlation was further observed between HUVECs and BJs at
late stage apoptosis (r-factor, 0.743; P=0.0288) and with respect
to the number of dead cells (r-factor, 0.895; P=0.0109; Table II).
Discussion
Infantile hemangiomas are benign vascular tumors
that are characterized by a proliferative, involution and involuted
phase (3). They appear during the
first few months of life and proliferate following stimulation by
several growth factors, including VEGF and bFGF (5). Following the proliferative phase,
hemangiomas rapidly enter the involution phase, where levels of
secreted VEGF and bFGF fall and cells undergo apoptosis (16). To date, several studies performed on
hemangioma-derived cells (16) and
HUVECs (17) have demonstrated an
arrest in cell proliferation and subsequent involution of the
tumor.
HUVECs represent a primary endothelial cell model
(18). Furthermore, HUVECs are
similar to hemangioma cells, as they react similarly to endothelial
cells present in infantile hemangiomas (19). Several studies were performed using
HUVECs to analyze the effects exhibited by Propranolol that result
in the involution of hemangiomas (16,17).
Further studies used HUVECs as control cell cultures to compare
hemangioma-derived stem cells (4) or
hemangioma-derived endothelial cells (20). In addition, BJs were used in the
present study, to mimic the connective tissue of infantile
hemangiomas, composed of fibroblasts, pericytes and mast cells
(3,4,21). The
present study investigated therapeutic effects of vincristine,
propranolol and bevacizumab on HUVEC and BJ cells.
Ji et al (16)
demonstrated that propranolol induced apoptosis in
hemangioma-derived cells via activation of caspase-3 and −9,
following the intrinsic pathway. Pan et al (22) revealed that propranolol in
vitro induces the inhibition of cell cycle progression,
concomitantly with decreased nitric oxide and VEGF levels through
the downregulation of the phosphoinositide 3-kinase/protein kinase
B/endothelial nitric oxide synthase/VEGF signaling pathway. In
addition, Tu et al (23)
revealed that apoptosis is induced both via the intrinsic and the
extrinsic pathway. Ou et al (20) performed a study on hemangioma-model
cells (hemEC) that demonstrated that the inhibition of
proliferation and induction of apoptosis is associated with
downregulation of VEGF receptor 2. Lamy et al (17) investigated effects of propranolol on
HUVECs and demonstrated inhibition of cell growth in a
dose-dependent manner, which was in line with the results of the
present study. This effect was further observed in BJs in the
present study, which suggested that the therapeutic effect of
propranolol on hemangiomas may be due to the inhibition of growth
in the sustaining tissue. However, this observation requires
further experimental evidence based specific hemangioma cells for
validation. Cell growth inhibition exerted by propranolol was
significantly increased in BJs and HUVECs, when treatment was
combined with subcytotoxic concentrations of vincristine and
bevacizumab, as presented in Figs. 1
and 2. In addition, IC50
values decreased when propranolol was administered together with
either the mitosis or the VEGF inhibitors. The cytotoxicity of each
drug was stronger in HUVECs compared with BJs; however, the
synergistic effect following treatment with propranolol plus the
two inhibitors was enhanced in BJs compared with HUVECs.
It has been established that VEGF is one of the most
potent growth factors inducing proliferation in hemangiomas
(14). However, single treatment
with bevacizumab, aVEGF inhibitor, exhibited the weakest effect on
viability in the tested cell lines of the current study. This may
be associated with the mechanism of action of VEGF inhibitors,
which do not directly affect apoptosis levels, but indirectly
affect apoptosis by decreasing levels of growth factor, resulting
in decreased levels of proliferation and subsequent cell cycle
arrest (24,25). However, combination treatment of
bevacizumab plus vincristine resulted in a significant increase in
apoptosis levels compared with bevacizumab and vincristine single
treatments and the determined IC50significantly
decreased in HUVECs for vincristine plus bevacizumab compared with
vincristine single treatment, as shown in Table II. This synergy between a direct
cytotoxic and a VEGF inhibitor bevacizumab has been established in
malignant solid tumors, including lung or colon cancer and has been
revealed to reduce VEGF levels and enhance cytotoxic effects of the
chemotherapeutical agents, which subsequently results in improved
therapeutic outcomes (26,27). As a result, cell growth may not only
be dependent on growth factors, but may be associated with numerous
other mechanisms, including mitosis inhibition. A similar effect
was observed in BJs. Liu et al (28) demonstrated that combination treatment
using bevacizumab and TRC105, two angiogenesis inhibitors with
varying mechanisms of action, suppresses HUVEC growth to a greater
extent when compared with single treatments. The results of the
present study demonstrated that using a therapeutic approach based
on different mechanism of action increased the efficacy in tumor
arrest and involution, when compared with treatment with two agents
that have a similar mechanism. Effects of bevacizumab may be
increased in in vivo studies, particularly when combined
with other treatments, compared with the in vitro model due
to the increased secretion of growth factor observed in viable
cells; however, further experimental proof is required. Hayot et
al (29) investigated several
agents, including vincristine, vinblastine, vindesine and
vinorelbine, to determine their effects on HUVECs and demonstrated
that vincristine has an antiangiogenic effect, even when
administered at non-cytotoxic concentrations (10 µg/ml). The
present study demonstrated marked cytotoxic effects of vincristine
administered at 100 µg/ml in single or at 10 µg/ml in combination
treatment with bevacizumab and/or propranolol. The results
suggested that the cytotoxic effects of vincristine, via
antiangiogenesis or direct cytotoxicity, were dependent on the
concentration. Consequently the question remains, whether the
concentration of vincristine administered in vivo has
antiangiogenic or directly cytotoxic effects, suggesting that the
range of vincristine administrable to patients is large and
adaptable to patient needs. However, further investigations in this
direction are required.
Following treatment, early apoptosis can occur
within 30 min or thereafter, depending on cell and exposure type
(30). In the current study, cells
in early and late apoptosis were differentiated. In HUVECs,
combination of vincristine and bevacizumab increased cells numbers
in early and late stage apoptosis compared with triple treatment
with propranolol, vincristine and bevacizumab. In BJs, triple
treatment with propranolol, vincristine and bevacizumab exhibited
the most pronounced apoptosis induction compared with all other
treatment options. This difference between the cell lines may be
due to varying proliferation rates and longer doubling times of
BJs.
Regarding monotherapy, vincristine was revealed to
be the most potent therapeutic agent in BJs and HUVECs inducing
early and late stage apoptosis compared with the other single
treatment regiments. The next best results were obtained with
propranolol, which induced higher levels on late apoptosis compared
with cells in early apoptosis. Treatment with bevacizumab plus
vincristine exhibited a greater combinatory therapeutic effect
compared with propranolol plus vincristine. This may be due to the
similar mechanism of action exhibited by propranolol and
vincristine, while bevacizumab and vincristine exhibit varying
mechanisms of action. Future studies are required to elucidate the
antiangiogenic mechanism of the combination of these drugs.
Patients with infantile hemangioma require prolonged
treatment with propranolol to achieve tumor regression, which may
be due to the fact that propranolol predominantly induces late
apoptosis, as was shown in our study. In hemangiomas that are
difficult to treat or life threatening and where rapid therapeutic
effects are required, vincristine is used (5). The various combinations of the drugs
used in the current study require further investigation on specific
hemangioma cell cultures or tissues, to evaluate novel therapeutic
strategies for patients with infantile hemangiomas.
In conclusion, a marked synergistic effect on HUVECs
and BJs was observed following administration of propranolol with
bevacizumab and vincristine. Apoptosis was induced by the various
treatments trialed in the present study; however, triple treatment
exhibited the most marked increase in apoptosis in BJs and
vincristine plus bevacizumab exhibited the strongest effect in
HUVECs. The results of the present study may constitute a basis for
novel drug testing and drug repurposing regarding the treatment of
infantile hemangiomas.
Acknowledgements
The authors would like to thank Dr Olga Soritau
(Oncology Institute ‘I. Chiricuță’, Cluj-Napoca, Romania) for
supplying the HUVECs.
Funding
The current study was supported by the framework of
PCD 2016 of the University of Medicine and Pharmacy ‘Iuliu
Hatieganu’ (Cluj-Napoca, Romania; grant no.
7690/12/15.04.2016).
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
MB generated and analyzed data and contributed to
the writing of the article. EFF designed the cytotoxicity studies,
performed the experiments and revised the manuscript. OVB
documented research and conceived and designed the current study.
MC designed and performed the flow cytometry analysis, and
elaborated and revised the manuscript. GP and CLB were involved in
the drafting of the manuscript and its critical revision for
important intellectual content. AT coordinated the study,
supervised its progress and approved the final version of the
article for publication. All authors read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rotter A and de Oliveira ZNP: Infantile
hemangioma: Pathogenesis and mechanisms of action of propranolol. J
Dtsch Dermatol Ges. 15:1185–1190. 2017. View Article : Google Scholar
|
|
2
|
Storch CH and Hoeger PH: Propranolol for
infantile haemangiomas: Insights into the molecular mechanisms of
action. Br J Dermatol. 163:269–274. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schwartz RA, Sidor MI, Musumeci ML, Lin RL
and Micali G: Infantile haemangiomas: A challenge in paediatric
dermatology. J Eur Acad Dermatol Venereol. 24:631–638. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Harbi S, Wang R, Gregory M, Hanson N,
Kobylarz K, Ryan K, Deng Y, Lopez P, Chiriboga L and Mignatti P:
Infantile hemangioma originates from a dysregulated but not fully
transformed multipotent stem cell. Sci Rep. 6:358112016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Léauté-Labrèze C: Infantile hemangioma:
Update and treatment. Arch Pediatr. 20:517–522. 2013.(In French).
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Léauté-Labrèze C, Dumas de la Roque E,
Hubiche T, Boralevi F, Thambo JB and Taïeb A: Propranolol for
severe hemangiomas of infancy. N Engl J Med. 358:2649–2651. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Raphael MF, Breur JM, Vlasveld FA, Elbert
NJ, Liem YT, Kon M, Breugem CC and Pasmans SG: Treatment of
infantile hemangiomas: Therapeutic options in regard to side
effects and adverse events-a review of the literature. Expert Opin
Drug Saf. 15:199–214. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wasserman JD, Mahant S, Carcao M, Perlman
K and Pope E: Vincristine for successful treatment of
steroid-dependent infantile hemangiomas. Pediatrics.
135:e1501–e1505. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yamashita-Kashima Y, Fujimoto-Ouchi K,
Yorozu K, Kurasawa M, Yanagisawa M, Yasuno H and Mori K: Biomarkers
for antitumor activity of bevacizumab in gastric cancer models. BMC
Cancer. 12:372012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pourazizi M, Kabiri S and Abtahi-Naeini B:
Intralesional bevacizumab (Avastin®) as a novel addition
to infantile hemangioma management: A medical hypothesis. J Res
Pharm Pract. 6:190–191. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Stiles J, Amaya C, Pham R, Rowntree RK,
Lacaze M, Mulne A, Bischoff J, Kokta V, Boucheron LE, Mitchell DC
and Bryan BA: Propranolol treatment of infantile hemangioma
endothelial cells: A molecular analysis. Exp Ther Med. 4:594–604.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hein M and Graver S: Tumor cell response
to bevacizumab single agent therapy in vitro. Cancer Cell Int.
13:942013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chao MW, Lai MJ, Liou JP, Chang YL, Wang
JC, Pan SL and Teng CM: The synergic effect of vincristine and
vorinostat in leukemia in vitro and in vivo. J Hematol Oncol.
8:822015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fischer-Fodor E, Mot A, Deac F, Arkosi M
and Silaghi-Dumitrescu R: Towards hemerythrin-based blood
substitutes: Comparative performance to hemoglobin on human
leukocytes and umbilical vein endothelial cells. J Biosci.
36:215–221. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ceballos-Torres J, Virag P, Cenariu M,
Prashar S, Fajardo M, Fischer-Fodor E and Gómez-Ruiz S: Anti-cancer
applications of titanocene-functionalised nanostructured systems:
An insight into cell death mechanisms. Chemistry. 20:10811–10828.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ji Y, Li K, Xiao X, Zheng S, Xu T and Chen
S: Effects of propranolol on the proliferation and apoptosis of
hemangioma-derived endothelial cells. J Pediatr Surg. 47:2216–2223.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lamy S, Lachambre MP, Lord-Dufour S and
Béliveau R: Propranolol suppresses angiogenesis in vitro:
Inhibition of proliferation, migration, and differentiation of
endothelial cells. Vascul Pharmacol. 53:200–208. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bouis D, Hospers GA, Meijer C, Molema G
and Mulder NH: Endothelium in vitro: A review of human vascular
endothelial cell lines for blood vessel-related research.
Angiogenesis. 4:91–102. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zou HX, Jia J, Zhang WF, Sun ZJ and Zhao
YF: Propranolol inhibits endothelial progenitor cell homing: A
possible treatment mechanism of infantile hemangioma. Cardiovasc
Pathol. 22:203–210. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ou JM, Yu ZY, Qiu MK, Dai YX, Dong Q, Shen
J, Wang XF, Liu YB, Quan ZW and Fei ZW: Knockdown of VEGFR2
inhibits proliferation and induces apoptosis in hemangioma-derived
endothelial cells. Eur J Histochem. 58:22632014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ritter MR, Butschek RA, Friedlander M and
Friedlander SF: Pathogenesis of infantile haemangioma: New
molecular and cellular insights. Expert Rev Mol Med. 9:1–19. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Pan WK, Li P, Guo ZT, Huang Q and Gao Y:
Propranolol induces regression of hemangioma cells via the
down-regulation of the PI3K/Akt/eNOS/VEGF pathway. Pediatr Blood
Cancer. 62:1414–1420. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tu JB, Ma RZ, Dong Q, Jiang F, Hu XY, Li
QY, Pattar P and Zhang H: Induction of apoptosis in infantile
hemangioma endothelial cells by propranolol. Exp Ther Med.
6:574–578. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Margolin K, Gordon MS, Holmgren E,
Gaudreault J, Novotny W, Fyfe G, Adelman D, Stalter S and Breed J:
Phase Ib trial of intravenous recombinant humanized monoclonal
antibody to vascular endothelial growth factor in combination with
chemotherapy in patients with advanced cancer: Pharmacologic and
long-term safety data. J Clin Oncol. 19:851–856. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Jain RK: Tumor angiogenesis and
accessibility: Role of vascular endothelial growth factor. Semin
Oncol. 29 (6 Suppl 16):S3–S9. 2002. View Article : Google Scholar
|
|
26
|
Sandler A, Gray R, Perry MC, Brahmer J,
Schiller JH, Dowlati A, Lilenbaum R and Johnson DH:
Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell
lung cancer. N Engl J Med. 355:2542–2550. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kabbinavar F, Irl C, Zurlo A and Hurwitz
H: Bevacizumab improves the overall and progression-free survival
of patients with metastatic colorectal cancer treated with
5-fluorouracil-based regimens irrespective of baseline risk.
Oncology. 75:215–223. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Liu Y, Tian H, Blobe GC, Theuer CP,
Hurwitz HI and Nixon AB: Effects of the combination of TRC105 and
bevacizumab on endothelial cell biology. Invest New Drugs.
32:851–859. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hayot C, Farinelle S, De Decker R,
Decaestecker C, Darro F, Kiss R and Van Damme M: In vitro
pharmacological characterizations of the anti-angiogenic and
anti-tumor cell migration properties mediated by
microtubule-affecting drugs, with special emphasis on the
organization of the actin cytoskeleton. Int J Oncol. 21:417–425.
2002.PubMed/NCBI
|
|
30
|
Anguissola S, Garry D, Salvati A, O'Brien
PJ and Dawson KA: High content analysis provides mechanistic
insights on the pathways of toxicity induced by amine-modified
polystyrene nanoparticles. PLoS One. 9:e1080252014. View Article : Google Scholar : PubMed/NCBI
|