Introduction
The Achilles tendon is one of the thickest and
strongest tendons in the human body, but is also one of the most
frequently ruptured (1). Ganestam
et al (2) recently
demonstrated that the probability of acute Achilles tendon rupture
has increased from 26.95 to 31.17 out of 105 individuals
between 1994 and 2013 in Denmark. However, there is currently no
definitive consensus on whether surgery should be chosen to repair
the ruptured acute Achilles tendon. Surgical treatment is often
preferred in healthy and active patients (3). Khan et al (3) published a meta-analysis of randomized
controlled blind prospective trials suggesting that conservative
treatment with surgical treatment can reduce the incidence of
Achilles tendon rupture. However, as surgical incision
complications are more likely, incision complications can be
reduced by percutaneous suturing.
The systematic analysis based on randomized
controlled trials published by Wilkins and Bisson (4) came to the same conclusion. A
meta-analysis based on a randomized controlled trial published by
Deng et al (5) suggested that
surgical treatment effectively reduced the re-rupture rate and may
be a better choice for the treatment of acute Achilles tendon
rupture. However, a meta-analysis based on randomized controlled
trials published by Sororeanu et al (6) suggested that conservative treatment did
not increase the rate of Achilles tendon rupture and, at the same
time, avoided incision complications. Surgical treatment is often
preferred in healthy and active patients (7). It is recommended that conservative
treatment should be considered if patient require functional
rehabilitation (6). Additionally,
surgical repair should be preferred at centers that do not employ
early range-of-motion protocols as it has been revealed to decrease
the re-rupture risk in such patients (6).
For surgical treatment, open surgery, small incision
or percutaneous suturing are also controversial (7). Del Buono et al (8) indicated that percutaneous techniques
exhibit the following advantages: Low complication rate, reduced
operating time, accelerated rehabilitation, reduced cost and
improved aesthetic results. However, they may lead to a higher rate
of recurrence than open surgical restoration techniques. However,
Li et al (9) demonstrated
that there was no statistically significant difference in
recurrence rate between percutaneous treatment and open surgery.
Sural nerve involvement was also a major difficulty in percutaneous
minimally invasive techniques, leading to damage and inflexibility
(10). Due to the small incision and
limited exposure range during percutaneous minimally invasive
surgery, the sural nerve cannot be directly viewed (8). The sural nerve at the proximal side of
the lateral malleolus is associated with the lateral side of the
Achilles tendon (11). Suture
needles can easily damage the sural nerves when they are blindly
suturing Achilles tendons (11).
Certain techniques have been used to avoid the risk
of nerve injury for doctors, including endoscopy-assisted
percutaneous restoration (8),
internal splinting technique (11)
and the modified Mayo needle technique (12–14).
However, there was no method that reduced the risk of nerve injury
and achieved a satisfactory clinical result for patients. A study
demonstrated that the duration of surgery was increased with the
use of endoscopic techniques (12).
When using the modified Mayo needle technique, a lateral incision
tends to allow visualization of the nerve (13). In the process of percutaneous
minimally invasive suture, because the sural nerve travels between
the Achilles tendon and the external malleolus, the nerve is not
exposed and protected during the surgery, and the nerve may be
damaged through the nerve during the blind suture (14). The surgical incision is relatively
increased and the operation time is expended accordingly.
Therefore, the surgery is cumbersome and the problem of sural nerve
injury cannot be solved simply and quickly. A channel-assisted
minimally invasive repair (CAMIR) (15) that was recently devised by the
present authors, has achieved satisfactory clinical effects. The
present study aimed to biomechanically compare two commercially
available, minimally invasive percutaneous techniques and a gold
standard open Achilles repair (10,16) with
the techniques of CAMIR and CAMIR augmentation during a simulated,
progressive rehabilitation program. Therefore, the present study
aimed to investigate the biomechanical comparison of
channel-assisted minimally invasive restoration and three common
Achilles tendon restoration techniques in an in vitro model
via a progressive rehabilitation program.
Materials and methods
Animals
A total of 21 12-month-old skeletally mature male
pigs (weight, 50±10 kg; Animal Laboratory, General Hospital of
People's Liberation Army, Beijing, China) were housed in cages and
exposed to a 12-h light/dark cycle. Pigs were fed regularly with
commercially available pig food. The right and left hind legs were
used for the present study. Pigs were housed between 23 and 25°C,
65–75% humidity. The Ethics Committee for Experiments on Animals of
General Hospital of People's Liberation Army approved all
procedures performed in the present study.
Experimental design
A total of 42 fresh porcine Achilles tendons were
obtained from 21 pigs following their sacrifice, stored at −20°C
and thawed for 12 h by infiltrating 0.9% NaCl prior to testing at
room temperature. The proximal tenotomy, simulated midsubstance
rupture, was made at 4 cm over the end of the plantar flexor
tendon. The distal tenotomy was made ~2 cm below the end of the
plantar flexor tendon. Moisture of the tendon was maintained with
saline sprays during the preparation and testing. The width and
thickness of all specimens were measured at the proximal end and
the suture end using vernier calipers (Guilin Guanglu Digital
Measurement & Control Co., Ltd., Guilin, China). The 42 tendons
were randomly assigned into six groups (n=7 each) and were
subjected to different Achilles restoration techniques: Krackow
(16), Achillon (17,18),
percutaneous Achilles repair system (PARS), channel-assisted
minimally invasive repair (CAMIR) (15), CAMIR augmentation (CAMIR+)
and CAMIR-5 (repair with No. 5 Ethibond suture).
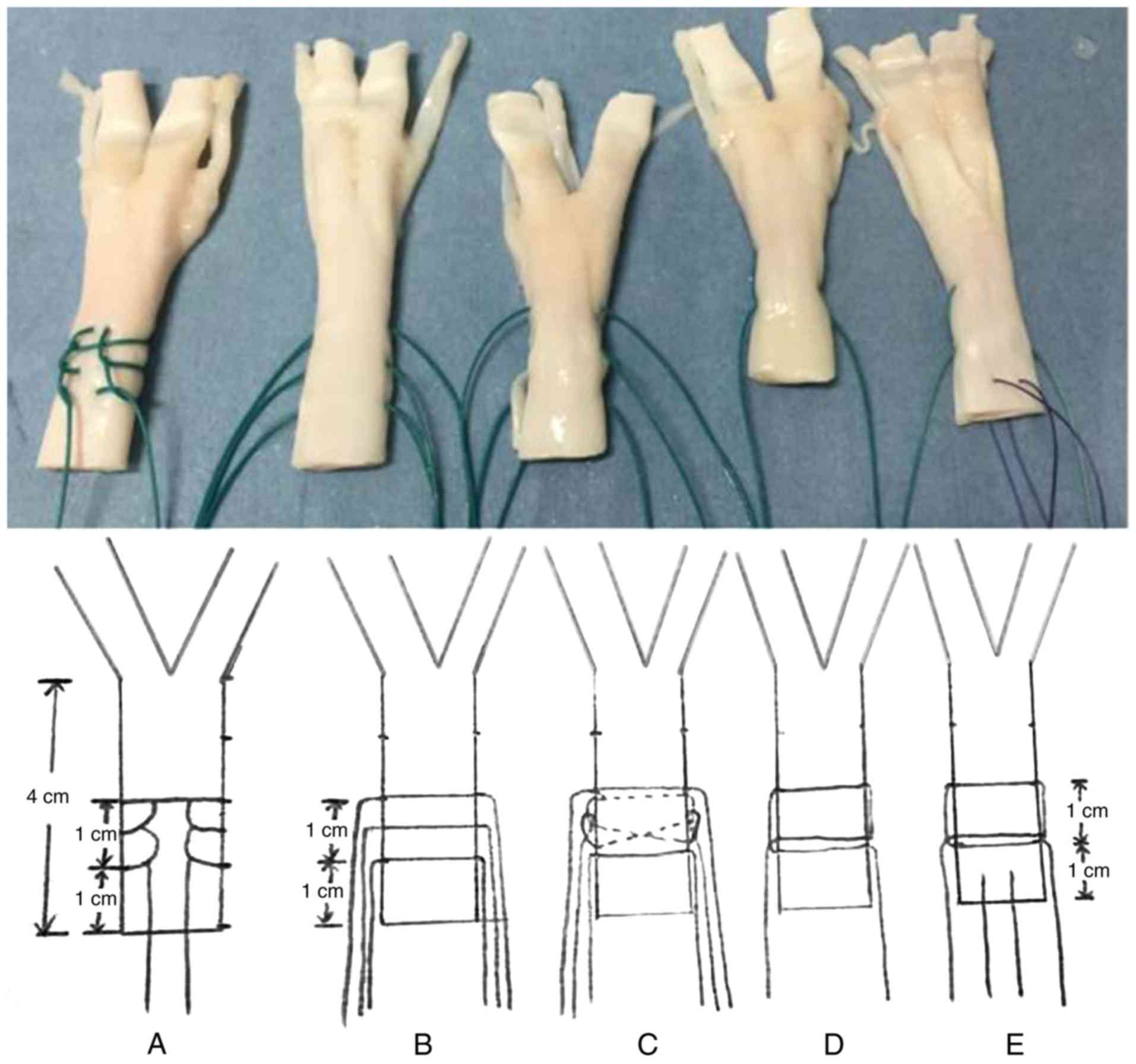
Simulated tears were subsequently repaired using the
randomly assigned restoration technique (Fig. 1). This figure presents all Achilles
restoration techniques, however as the only difference between
CAMIR and CAMIR-5 is the size of the suture, one image is used to
represent the two techniques. All surgical restorations were
performed by a single foot and ankle fellowship-trained orthopedic
surgeon. Suturing commenced 1 cm from the proximal edge of tendon
specimens, and a constant 1 cm was maintained from the proximal to
distal strand. The Achillon, PARS, Krackow and CAMIR methods were
applied using No. 2 Ethibond (Ethicon, Inc., Cincinnati, OH, USA).
CAMIR+ was applied using No. 2 Ethibond (Ethicon, Inc.)
sutures augmented with intermittent sutures of absorbable Vicryl
2-0. CAMIR-5 was applied using No. 5 Ethibond (Ethicon, Inc.).
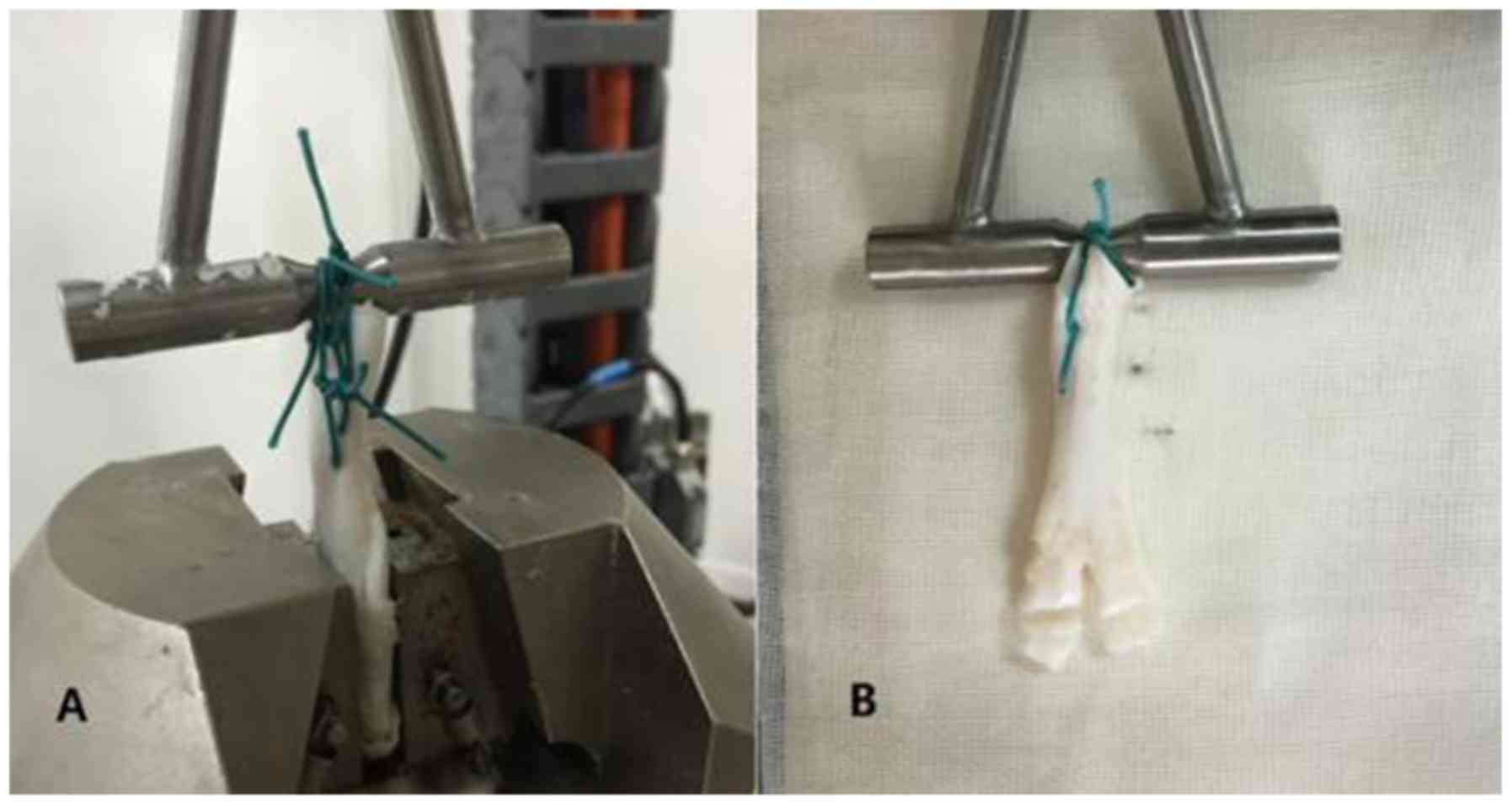
Biomechanics testing
A universal material testing dynamometer (Electro
Puls E10000; Instron, Norwood, MA, USA) was used to cyclically load
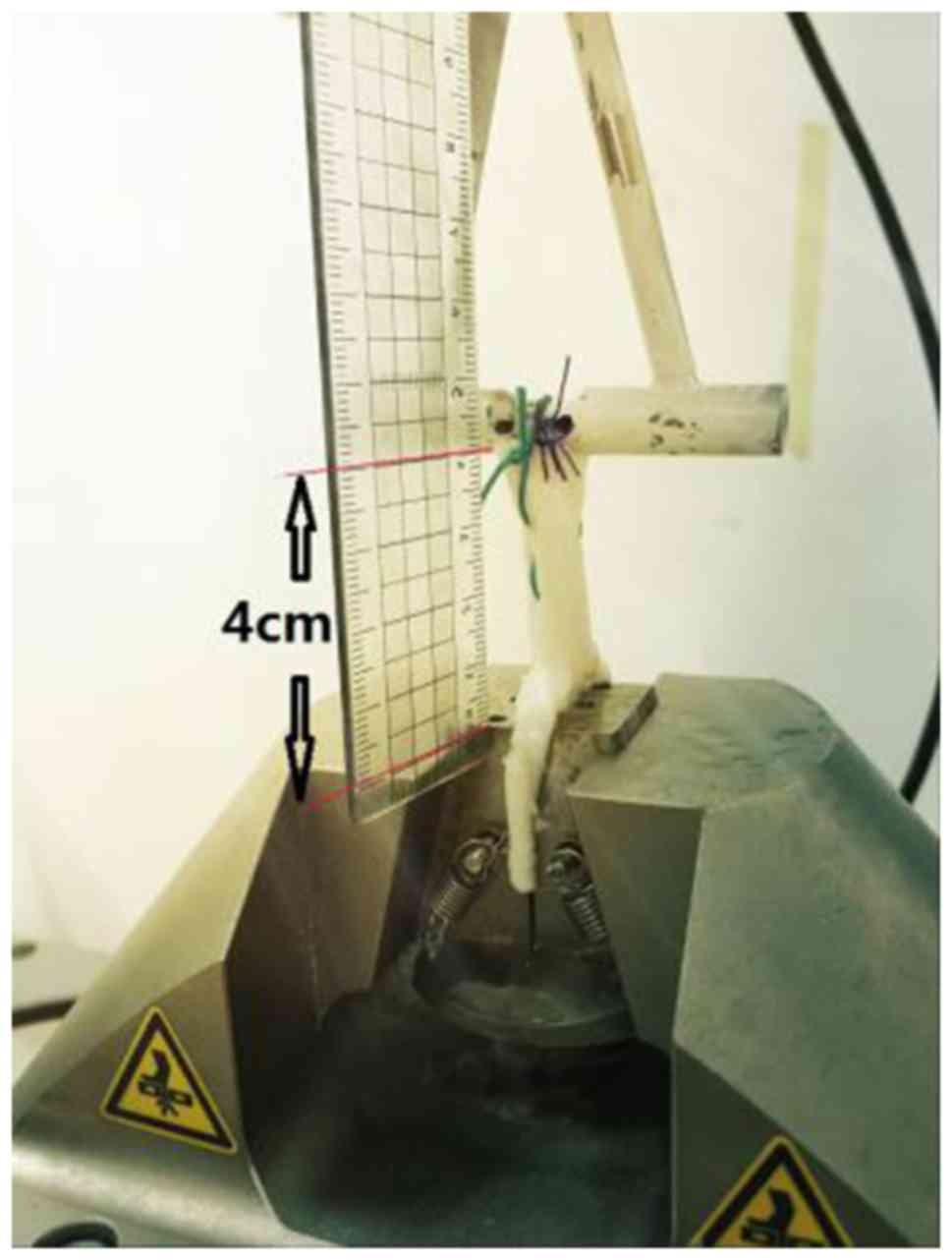
the tendons. Following the completion of suture-graft constructs,
each specimen was mounted below the dynamometer with the
non-sutured end of the tendon wrapped with gauze to eliminate
slippage while secured in a custom clamp. The free strands of the
suture were tied with ‘8’ square knots over a custom bar of the
universal material testing machine, mimicking a suture post in
vivo (19–21). The non-sutured end of the tendon was
in close proximity to the bar to minimize elongation of the suture.
The whole suture constructs, from below the bar to above the clamp,
were maintained at a standard length of 4 cm for testing (Fig. 2). Each tendon was pre-tensioned to 50
N for 2 min to remove slack from the construct. Each specimen was
subjected to a loading protocol representative of a progressive,
postoperative rehabilitation program (3,000 total cycles)
consisting of three cyclic loading stages of 1,000 cycles at 1 Hz
as follows: i) 20–100 N, ii) 20–191 N and iii) 20–369 N. Sutures
that were maintained following all 1,000 cycles of loading were
subsequently pulled to failure at a rate of 25 mm/sec for each
cyclic loading stage. Loads were selected to mimic a progressive,
postoperative rehabilitation protocol and were based on previous
literature describing load ranges experienced by the Achilles
tendon during passive ankle flexion (20–100 N) and walking in a CAM
walker with (191 N) and without (369 N) a 1-inch heel lift
(22,23). Failure was defined as tendon
breakage, suture breakage or suture pullout. Cyclics and elongation
were monitored and recorded continuously throughout testing by
dynamometer. The mode of failure for each construct and the number
of stitch knots of different techniques were also recorded.
Statistical analysis
The maximum number of cycles is expressed as the
median (minimum, maximum). The analysis of variance was used for
the amount of stretch, and the expression was mean ± standard
deviation. To detect the effect size of one sample for differences
in repaired elongation at the end of the first loading cycle, 7
specimens per group were required to achieve an 80% positive rate.
The data of this calculation was based on the result of a pilot
investigation and statistical analysis performed prior to
completion of testing. Statistical analysis was performed using
SPSS version 13.0 (SPSS, Inc., Chicago, IL, USA). One-way analysis
of variance was applied to evaluate differences in the mean width
and thickness of the tendon in each group, and the elongation
following 10, 1,000, 2,000 and 3,000 cycles. The Kruskal-Wallis
test was used to assess if there was an association between the
restoration technique and the number of cycles to total
restorations failure. If a significant effect was noted, a post hoc
Mann-Whitney U test (with Bonferroni corrections for multiple
comparisons) was performed to assess differences between the
different techniques. P<0.05 was considered to indicate a
statistically significant difference.
Results
Biomechanics test of Achilles
tendon
There were no significant differences in Achilles
tendon consistency among groups (Table
I). All restorations survived during the first stage of cyclic
loading (20–100 N, 1,000 cycles), however 21 samples failed the
second phase and 21 samples failed the third phase (3,000 cycles in
all three stages; data not shown).
 | Table I.The consistency of Achilles
tendon. |
Table I.
The consistency of Achilles
tendon.
| Group | Thickness (mm) | Width (mm) |
|---|
| Achillon | 13.66±0.72 | 4.63±0.58 |
| PARS | 13.42±0.66 | 4.37±0.54 |
| Krackow | 13.56±0.68 | 4.48±0.62 |
| CAMIR | 13.46±0.70 | 4.51±0.56 |
|
CAMIR+ | 13.61±0.72 | 4.59±0.69 |
| CAMIR-5 | 13.46±0.68 | 4.52±0.49 |
Failure time of cycle test
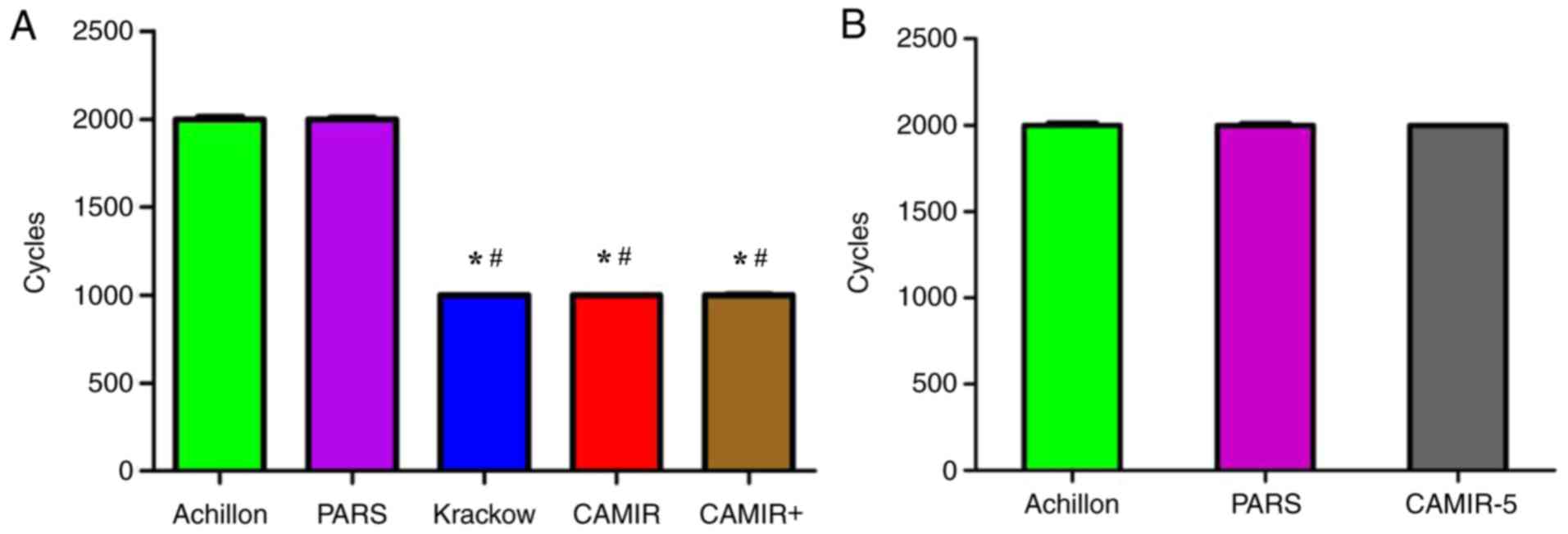
There was no significant difference in the number of
cycles before restoration failure among the following restoration
methods: Krackow, median 1,000 (range, 1,000–1,000); CAMIR, median
1,000 (range, 1,000–1,000); and CAMIR+ median 1,000
(range, 1,000–1,004). However, they were significantly less than
that observed in the 2 percutaneous repair methods: Achillon,
median 2,000 (range, 2,000–2,013); and PARS median 2,000 (range,
2,000–2,010; P<0.05; Fig. 3A). In
addition, there was no significant differences in cycles between
CAMIR-5 (median, 2,000; range, 2,000–2,003), and Achillon and PARS
(Fig. 3B).
Tendons in the CAMIR group are
repaired with the No. 2 Ethibond suture test
Following the 10th cycle of cyclic loading, CAMIR
and CAMIR+ restoration exhibited a mean elongation of
2.16±1.12 and 2.03±0.93 mm respectively, which were not
significantly different than Krackow (1.97±0.56 mm), Achillon
(1.67±0.74 mm) or PARS (2.02±1.03 mm). Following the 1,000th cycle,
the mean elongation of CAMIR (7.51±1.77 mm) and CAMIR+
(7.11±1.50 mm) exhibited no significant difference compared with
Krackow (7.32±1.09 mm), but were significantly longer than Achillon
(3.19±0.57 mm) and PARS (3.73±0.66 mm; P<0.05; Table II).
| Table II.Elongation following 10 and 1,000
cycles for the different repair techniques using No. 2 Ethibond
suture. |
Table II.
Elongation following 10 and 1,000
cycles for the different repair techniques using No. 2 Ethibond
suture.
| Group | Elongation
following 10 cycles (mm) | Elongation
following 1,000 cycles (mm) |
|---|
| Achillon | 1.67±0.74 | 3.19±0.57 |
| PARS | 2.02±1.03 | 3.73±0.66 |
| Krackow | 1.97±0.56 |
7.32±1.09a |
| CAMIR | 2.16±1.12 |
7.51±1.77a |
|
CAMIR+ | 2.03±0.93 |
7.11±1.50a |
Tendons in the CAMIR-5 group are
repaired with the No
5 Ethibond suture test
Following the 10th and 2,000th cycle of cyclic
loading, the elongation of CAMIR-5 exhibited no significant
difference vs. Achillon or PARS. However, at the 1,000th cycle, the
elongation of CAMIR-5 remained greater than that of Achillon and
PARS restorations (P<0.05; Table
III).
| Table III.Elongation following 10, 1,000 and
2,000 cycles for the CAMIR group repaired with No. 5 Ethibond
suture, and the Achillon and PARS groups repaired with No. 2
Ethibond. |
Table III.
Elongation following 10, 1,000 and
2,000 cycles for the CAMIR group repaired with No. 5 Ethibond
suture, and the Achillon and PARS groups repaired with No. 2
Ethibond.
| Group | Elongation
following 10 cycles (mm) | Elongation
following 1,000 cycles (mm) | Elongation
following 2,000 cycles (mm) |
|---|
| Achillon | 1.67±0.74 | 3.19±0.57 | 7.96±1.25 |
| PARS | 2.02±1.03 | 3.73±0.66 | 8.15±1.32 |
| CAMIR-5 | 1.59±0.56 |
4.97±1.47a | 7.99±1.68 |
| P-value | 0.561 | 0.01 | 0.971 |
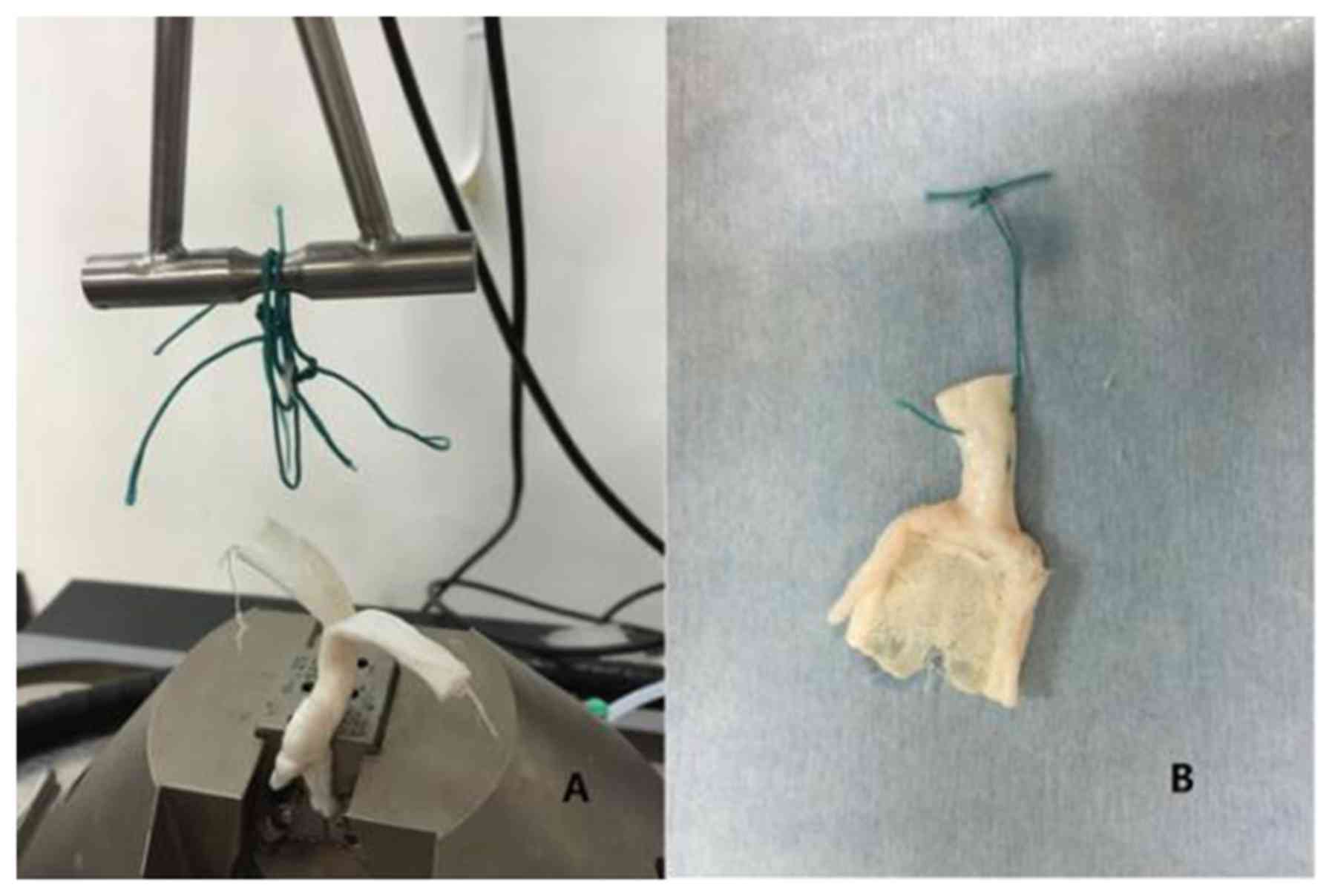
The number of sutures and knots
The primary mechanism of failure was suture break at
the suture-tendon interface (Achillon, 3/7; PARS, 0/7; Krackow,
0/7; CAMIR, 1/7; CAMIR+, 0/7; CAMIR-5, 0/7) and breakage
of knots (Achillon, 4/7; PARS, 7/7; Krackow, 7/7; CAMIR, 6/7;
CAMIR+, 7/7; CAMIR-5, 7/7; Fig. 4). The number of stitch knots in each
group was 3 (Achillon), 3 (PARS), 1 (Krackow), 1 (CAMIR) and 3
(CAMIR+; Fig. 5).
Discussion
Compared with open restoration, percutaneous
techniques have many advantages, including minimized incisions,
reduced surgery duration, improved cosmetic appearance and reduced
rate of complication (24,25). Compared with conservative treatment,
it may also decrease the risk of rupture reoccurrence (26,27). In
the present study, CAMIR techniques were used easily through a
minimal incision, on the tendon ends. The channel of CAMIR, which
was designed by the authors of the present study, may reduce the
risk of nerve injury, and achieved a satisfactory clinical effect
(15). Early rehabilitation therapy
is helpful to reduce postoperative complications of Achilles
tendons, and yield a better effect of treatment for patients
(28–30). However, following minimally invasive
surgical treatment, surgeons often recommend cast immobilization to
decrease the elongation of suture construct and the risk of failure
(31). In order to provide reliable
evidence for postoperative rehabilitation via the CAMIR technique,
the present study simulated a progressive rehabilitation program
with three stages of cyclic loading to compare the strength with
the commonly used Krackow technique (32,33) and
the minimally invasive Achillon and PARS techniques, and evaluated
the subsequent biomechanics (25,29).
Unreliable stitching or incorrect rehabilitation
treatment may make the suture constructs elongate easily, result in
suture failure or making the Achilles tendon itself, elongate,
which will lead to heel raise difficultly and claudication
(28). These cause great physical
and psychological harm to patients. Therefore, the elongation of
the suture constructs under strain is a valuable test of
biomechanics. The restoration of elongation was evaluated in the
present study, instead of any direct measurement of repair site
gapping as described in previous literature (10,34). The
elongation of Achilles tendons were recorded directly using an
Instron biomechanical testing machine, including elongation of the
entire tested construct, which may be in accordance with real-life
observations in clinical practice. These measurements included the
elongation of Achilles tendon tissue itself, the knot tightening or
slipping, the suture being pulled through tendon and stretching of
the suture material, which is similar to elongation in clinical
practice. In the current study, eight square knots were used for
each sample, and the knot size was the same, so that the baseline
of the knot tightening or slipping was the same to offset the
interference of this factor.
In addition, by suturing 1 cm from the proximal edge
of tendon specimens, maintaining a 1 cm distance from the proximal
to distal strand, and ensuring the non-sutured end of the tendon
was in close proximity to the bar to minimize the elongation of
suture, the baseline length of the sutures in each group was
demonstrated to be basically the same, thus minimizing the
influence of the stretching material factor. At the same time, to
ensure that no significant differences in thicknesses and widths
were identified between samples from all groups, each sample was 6
cm and the distance between the clamp and the bar was 4 cm, thereby
ensuring that the baseline of each sample was consistent.
Therefore, the elongation measured during the biomechanical testing
reflected the elongation of Achilles tendon tissue itself, as well
as the sutures being pulled through tendon and stretching of the
suture material (27). The total
cycles following repair failure were another valuable index that
reflected the strength of stitching technique. These reported
values were recorded automatically by an Instron machine when the
restoration failure occurred.
The comparisons of the biomechanical parameters in
open and percutaneous restoration, and between the different
percutaneous techniques were also conflicting. Few studies have
assessed the simulated, progressive rehabilitation protocol. The
majority of the studies consist of static experiments, which assess
the maximum tensile strength or are failure experiments. Cyclic
loading is less clinically assessed compared with the physiological
state of the sputum. Mark-Christensen et al (28) compared the strength of tendons
repaired with percutaneous techniques Achillon and PARS. Results
demonstrated that the number of cycles prior to restoration failure
in the Achillon group was significantly less than in the PARS
groups, as the width and length of the Achilles tendons were
detected by a differential variable reluctance transducer; the
tendons were 2 mm in width and 9.5 mm in length. Otherwise,
biomechanics testing demonstrated that the PARS group restorations
resisted maximum load failure better than the Achillon group
restorations (data not shown). Therefore, it was indicated that
percutaneous repair techniques applying locking sutures offered a
better strength of construction under cyclic and ultimate loads,
compared with a restoration technique that used non-locking
sutures. PARS was stronger than Achillon.
A previous study compared three commercially
available, minimally invasive percutaneous techniques, Achillon,
PARS and Speed Bridge, with an open Achilles restoration, modified
Kessler, during a simulated and progressive rehabilitation program
(31). Results demonstrated that the
open restoration technique significantly reduced when compared with
all minimally invasive percutaneous restoration methods following
250 cycles. There were no significant differences in mean
displacements observed following 250 cycles between the Achillon,
PARS, and Speed Bridge restorations, and there were no significant
differences in the total number of cycles to failure between
minimally invasive percutaneous restorations and open restorations.
Clanton et al (31) revealed
that minimally invasive percutaneous restoration techniques were
susceptible to significant early restoration elongation when
compared with open restorations, but the ultimate strengths of
restorations (as indicated by failure cycles) were comparable among
the open and percutaneous restoration techniques.
Lee et al (10) previously compared percutaneous
Achillon, 4-strand Krackow, and an epitendinous augmented 4-strand
Krackow restoration techniques during a simulated and progressive
rehabilitation program, and it was reported that gap resistance was
significantly better in augmented Krackow restorations (2,213
cycles to total failure gapping) vs. non-augmented restorations
(1,268 cycles) and percutaneous restorations (102 cycles). Lee
et al (10) also indicated
that open restoration techniques (Krackow) making use of locking
sutures offered a better construct of strength under cyclic loads
compared with percutaneous restoration techniques (Achillon) that
used only non-locking sutures. Otherwise, the cross-stitch weave
augmentation significantly increased restoration strength and gap
resistance. The current biomechanical experimental literature
reported large differences in results and the conclusions were not
consistent.
The present study indicated that there was no
significant difference in the elongation at the end of the tenth
cycle in all samples of Achilles tendons. And the majority of
elongations did not occur in the initial 10 cycles, which
contradicts the results of a previous study (27). The authors of the present study
considered that the preloading of 50 N, 2 min prior to the cyclic
program Therefore, preloading may partially reduce the restoration
elongation and deformation of tendons that occur during initial
loading (first 10 cycles). All tendons were survived in the first
stage of cyclic loading (20–100 N).
The Krackow, CAMIR and CAMIR+ groups
stitched by No. 2 sutures all failed during the second stage of
cyclic loading (20–191 N), whereas Achillon and PARS groups
stitched by No. 2 sutures all failed during the third stage of
cyclic loading (20–369 N). Following 1,000 cycles, the mean
elongation of CAMIR and CAMIR+ restoration groups
exhibited no significant differences with the Krackow restoration
group, but were lower than those of the Achillon and PARS repair
groups. This indicated that stitching with the CAMIR with No. 2
suture was as strong as the Krackow technique, but was still weaker
than the Achillon and PARS techniques. Otherwise, augmentation with
lower resisted intensity sutures did not increase the strength and
elongation resistance. All restorations provided reliable strength
for postoperative isokinetic training.
The 90% failure rate of sutures in the current
experiment was due to a rupture at the suture junction, indicating
that stress was predominantly located at the suture junction. The
current study revealed that Achillon and PARS are stronger compared
with CAMR and Krackow as they hold one end of the Achilles tendon
by three lines. The three lines divided the stress and reduced the
stress concentration at the knot. The study by McKeon et al
(19) also demonstrated that
increasing the number of sutures increased suture strength.
However, the more sutures and knots in the tendon, the greater the
risk of postoperative complications (35–39).
Therefore, it was deemed that best practice included selecting the
surgical procedure that required fewer sutures and provided
reliable strength for early passive motion of the ankle joint.
CAMIR, which used only one suture, did not fail during the 20–100 N
cycle, indicating that the use of CAMIR can provide reliable
strength for early passive ankle joint activity.
The CAMIR suture method, which used No. 5 Ethibond
sutures, failed in 86% of the samples as the suture was broken at
the knot, rather than the suture that pulled the Achilles tendon.
In order to test the reliability of the CAMIR suture method and
increase the strength of the suture, No. 5 Ethibond sutures were
selected, and it was revealed that the strength of the suturing in
the fifth thread of the CAMIR-5 group was indistinguishable from
the Achillon and PARS methods, which sutured with the second
thread. The results suggested that the CAMIR suture strength can be
increased by increasing the thickness and tensile strength of the
suture, therefore this method is very reliable. The difference
between the CAMIR, PARS and Achillon methods is that CAMIR has 1
line at the proximal and 1 line at the distal, with a total of 2
knots, and PARS and Achillon have 3 lines at the proximal and 3
lines at the distal, with a total of 6 knots located among the
stumps. More knots in the soft tissue under the skin may lead to
incision complications. In the present study, pull-out from the
tendon accounted for 43% of failure of Achillon restoration, which
was more prevalent than in other groups. In this experiment, 43% of
Achillon's failure was due to suture breakage, which was more
prevalent than in other groups. PARS, CAMIR, and Krackow techniques
all have locking sutures, which allow the structure of the locking
mechanism to grip the Achilles tendon tighter when the pulling
force applied to the suture increases (28). The stitching structure of Achillon
uses 3 parallel lines, and there is no locking structure, which
cannot convert the pulling force into grasping force (28). As the pulling force increases, the
sutures cut the Achilles tendon and cause the suture to fail
(28).
In the present study, Achillon and PARS restoration
techniques were comprised of three sutures, whereas Krackow and
CAMIR require only one suture. Although three sutures enhanced the
strength of stitching, there were three large knots on the sides of
the end of tendons. The present study only simulated one side of
the Achilles tendon rupture as only three knots were used. In
clinical practice, six knots are used as there are two broken ends
when the Achilles tendon breaks. Achilles tendon rupture typically
occurred 2–6 cm proximal to the tendon for inserting (36), where coverage of tissue and skin is
not thick. Too many sutures and knots with a larger caliber of
suture may increase the risk of suture reactivity, which may cause
postoperative complications, such as abscess, granuloma or fistula
at the incision site, and infection (37–39).
There were a number of limitations in the present
investigation. Firstly, the use of porcine Achilles tendon
specimens may not perfectly represent the dimensions and
architecture observed in human tendons. However, porcine tendon has
been used in a number of studies evaluating different fixation
techniques for tendon restoration (19,20).
Secondly, percutaneous restorations in the present study were made
using an open approach simulating the restoration technique without
specialized stitching devices, which may have led to inaccurate
repairing. In clinical practice, percutaneous sutures often do not
expose the threading site and cannot be viewed directly. In
particular, it is difficult for the three sutures in the Achillon
method to pass through the maximum diameter of the Achilles tendon
as in the current study, thereby weakening the suture strength.
Finally, one side of the lacerated tendon ends were sutured, which
has also been the case in multiple studies evaluating different
fixation techniques for tendon restoration (23,24).
However, the limited number of samples is the main disadvantage of
the present study. In future studies, a large number of samples are
required.
In conclusion, the suture structure of CAMIR can
achieve reliable suture strength with fewer stitches and knots,
reaching the strength of the open Krackow restoration technique,
but weaker than Achillon and PARS techniques. To a certain extent,
the greater the tensile strength of the suture used, the stronger
the tensile strength of the CAMIR suture structure. The
intermittent reinforcement of the broken ends does not improve the
suturing strength.
Acknowledgements
Not applicable.
Funding
The present study was supported by Beijing Municipal
Science & Technology Commission (grant no.
Z161100000516192).
Availability of data and materials
All data generated or analyzed during the current
study are included in this published article.
Authors' contributions
HQ, YC and XJ performed the surgeries. HQ wrote the
manuscript. HQ, HC, PT and LW proposed experimental theories and
designed the experiment. LW trained HQ, YC, and XJ to use the
experimental instruments. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The Ethics Committee for Experiments on Animals of
General Hospital of People's Liberation Army (Beijing, China)
approved all procedures in the present study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jozsa L, Kvist M, Balint BJ, Reffy A,
Järvinen M, Lehto M and Barzo M: The role of recreational sport
activity in Achilles tendon rupture. A clinical, pathoanatomical,
and sociological study of 292 cases. Am J Sports Med. 17:338–343.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ganestam A, Kallemose T, Troelsen A and
Barfod KW: Increasing incidence of acute Achilles tendon rupture
and a noticeable decline in surgical treatment from 1994 to 2013. A
nationwide registry study of 33,160 patients. Knee Surg Sports
Traumatol Arthrosc. 24:3730–3737. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Khan RJ, Fick D, Keogh A, Crawford J,
Brammar T and Parker M: Treatment of acute achilles tendon
ruptures. A meta-analysis of randomized, controlled trials. J Bone
Joint Surg Am. 87:2202–2210. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wilkins R and Bisson LJ: Operative versus
nonoperative management of acute Achilles tendon ruptures: A
quantitative systematic review of randomized controlled trials. Am
J Sports Med. 40:2154–2160. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Deng S, Sun Z, Zhang C, Chen G and Li J:
Surgical treatment versus conservative management for acute
Achilles tendon rupture: A systematic review and meta-analysis of
randomized controlled trials. J Foot Ankle Surg. 56:1236–1243.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Soroceanu A, Sidhwa F, Aarabi S, Kaufman A
and Glazebrook M: Surgical versus nonsurgical treatment of acute
Achilles tendon rupture: A meta-analysis of randomized trials. J
Bone Joint Surg Am. 94:2136–2143. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hattrup SJ and Johnson KA: A review of
ruptures of the Achilles tendon. Foot Ankle. 6:34–38. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Del Buono A, Volpin A and Maffulli N:
Minimally invasive versus open surgery for acute Achilles tendon
rupture: A systematic review. Br Med Bull. 109:45–54. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li Q, Wang C, Huo Y, Jia Z and Wang X:
Minimally invasive versus open surgery for acute Achilles tendon
rupture: A systematic review of overlapping meta-analyses. J Orthop
Surg Res. 11:652016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lee SJ, Sileo MJ, Kremenic IJ, Orishimo K,
Ben-Avi S, Nicholas SJ and McHugh M: Cyclic loading of 3 Achilles
tendon repairs simulating early postoperative forces. Am J Sports
Med. 37:786–790. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Aibinder WR, Patel A, Arnouk J, El-Gendi
H, Korshunov Y, Mitgang J and Uribe J: The rate of sural nerve
violation using the Achillon device: A cadaveric study. Foot Ankle
Int. 34:870–875. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Carmont MR and Maffulli N: Modified
percutaneous repair of ruptured Achilles tendon. Knee Surg Sports
Traumatol Arthrosc. 16:199–203. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Maffulli N, Longo UG, Maffulli GD, Khanna
A and Denaro V: Achilles tendon ruptures in elite athletes. Foot
Ankle Int. 32:9–15. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Maffulli N, Longo UG, Ronga M, Khanna A
and Denaro V: Favorable outcome of percutaneous repair of Achilles
tendon ruptures in the elderly. Clin Orthop Relat Res.
468:1039–1046. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen H, Ji X and Tang P, Liang X and Tang
P: Channel-assisted minimally invasive repair of acute Achilles
tendon rupture. J Orthop Surg Res. 10:1672015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Krackow KA, Thomas SC and Jones LC: A new
stitch for ligament-tendon fixation. Brief note. J Bone Joint Surg
Am. 68:764–766. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Calder JD and Saxby TS: Early, active
rehabilitation following mini-open repair of Achilles tendon
rupture: A prospective study. Br J Sports Med. 39:857–859. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Assal M, Jung M, Stern R, Rippstein P,
Rippstein P, Delmi M and Hoffmeyer P: Limited open repair of
Achilles tendon ruptures: A technique with a new instrument and
findings of a prospective multicenter study. J Bone Joint Surg Am.
84-A:161–170. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
McKeon BP, Heming JF, Fulkerson J and
Langeland R: The Krackow stitch: A biomechanical evaluation of
changing the number of loops versus the number of sutures.
Arthroscopy. 22:33–37. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ostrander RV, Saper MG and Juelson TJ: A
biomechanical comparison of modified krackow and locking loop
suture patterns for soft-tissue graft fixation. Arthroscopy.
32:1384–1388. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hapa O, Erduran M, Havitçioğlu H, Çeçen B,
Akşahin E, Güler S and Atalay K: Strength of different Krackow
stitch configurations using high-strength Suture. J Foot Ankle
Surg. 52:448–450. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Orishimo KF, Burstein G, Mullaney MJ,
Kremenic IJ, Nesse M, McHugh MP and Lee SJ: Effect of knee flexion
angle on Achilles tendon force during passive dorsiflexion. J Foot
Ankle Surg. 47:34–39. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Akizuki KH, Gartman EJ, Nisonson B,
Ben-Avi S and McHugh MP: The relative stress on the Achilles tendon
during ambulation in an ankle immobilizer: Implications for
rehabilitation after Achilles tendon repair. Br J Sports Med.
35:329–334. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
McMahon SE, Smith TO and Hing CB: A
meta-analysis of randomised controlled trials comparing
conventional to minimally invasive approaches for repair of an
Achilles tendon rupture. Foot Ankle Surg. 17:211–217. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cretnik A, Kosanovic M and Smrkolj V:
Percutaneous versus open repair of the ruptured Achilles tendon: A
comparative study. Am J Sports Med. 33:1369–1379. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ebinesan AD, Sarai BS, Walley GD and
Maffulli N: Conservative, open or percutaneous repair for acute
rupture of the Achilles tendon. Disabil Rehabil. 30:1721–1725.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cetti R, Christensen SE, Ejsted R, Jensen
NM and Jorgensen U: Operative versus nonoperative treatment of
Achilles tendon rupture. A prospective randomized study and review
of the literature. Am J Sports Med. 21:791–799. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Mark-Christensen T, Troelsen A, Kallemose
T and Barfod KW: Functional rehabilitation of patients with acute
Achilles tendon rupture: A meta-analysis of current evidence. Knee
Surg Sports Traumatol Arthrosc. 24:1852–1859. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Nilsson-Helander K, Silbernagel KG, Thomeé
R, Faxén E, Olsson N, Eriksson BI and Karlsson J: Acute Achilles
tendon rupture: A randomized, controlled study comparing surgical
and nonsurgical treatments using validated outcome measures. Am J
Sports Med. 38:2186–2193. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Brumann M, Baumbach SF, Mutschler W and
Polzer H: Accelerated rehabilitation following Achilles tendon
repair after acute rupture-Development of an evidence-based
treatment protocol. Injury. 45:1782–1790. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Clanton TO, Haytmanek CT, Williams BT,
Civitarese DM, Turnbull TL, Massey MB, Wijdicks CA and LaPrade RF:
A biomechanical comparison of an open repair and 3 minimally
invasive percutaneous Achilles tendon repair techniques during a
simulated, progressive rehabilitation protocol. Am J Sports Med.
43:1957–1964. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Demetracopoulos CA, Gilbert SL, Young E,
Baxter JR and Deland JT: Limited-open Achilles tendon repair using
locking sutures versus nonlocking sutures: An in vitro model. Foot
Ankle Int. 35:612–618. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Heitman DE, Ng K, Crivello KM and Gallina
J: Biomechanical comparison of the Achillon tendon repair system
and the Krackow locking loop technique. Foot Ankle Int. 32:879–887.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Benthien RA, Aronow MS, Doran-Diaz V,
Sullivan RJ, Naujoks R and Adams DJ: Cyclic loading of Achilles
tendon repairs: A comparison of polyester and polyblend suture.
Foot Ankle Int. 27:512–518. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Nichol SA and Silk WK: Empirical evidence
of a convection-diffusion model for pH patterns in the rhizospheres
of root tips. Plant Cell Environment. 24:967–974. 2001. View Article : Google Scholar
|
|
36
|
Cevik M: Acquired Umbilico-inguinal
fistula with persistent discharge due to suture reaction: A case
report and review of the literature. Case Rep Med. 2012:2163452012.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Aktas S and Kocaoglu B: Open versus
minimal invasive repair with Achillon device. Foot Ankle Int.
30:391–397. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Casha JN and Hadden WA: Suture reaction
following skin closure with subcuticular polydioxanone in total
knee arthroplasty. J Arthroplasty. 11:859–861. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Kara A, Celik H, Seker A, Uysal MA, Uzun M
and Malkoc M: Granuloma formation secondary to Achilles tendon
repair with nonabsorbable suture. Int J Surg Case Rep. 5:720–722.
2014. View Article : Google Scholar : PubMed/NCBI
|