Introduction
Rectal cancer is the most common type of malignant
tumor in digestive tract and one of the leading causes of death in
humans. It mainly occurs in people over 45 years, and the incidence
is higher in men than in women (1,2). With
the changes in people's diet structure and the lack of physical
exercise, incidence of rectal cancer has increased year by year,
and 1,000,000 new cases were reported each year (3,4). With
the growth of aging population, proportion of elderly patients with
rectal cancer is gradually increased, but treatment of elderly
patients with rectal cancer has not been well studied (5). Approximately 81% of rectal cancer
occurs near the anal sphincter. Surgical resection is the only
radical treatment for malignant tumors, while surgical treatment of
rectal cancer is challenged by the retention of anus and anus
function. Surgical treatment is also a very dangerous treatment for
elderly rectal cancer patients (6,7).
Radiotherapy is one of the basic treatment methods
for patients with malignant tumors. However, toxic effects of
long-term radiotherapy are unbearable. Efficacy of radiotherapy
will also decrease over time, so finding a mild and effective drug
is critical (8,9). Oxaliplatin and fluorouracil are two
widely used drugs in tumor treatment. There are also studies on the
use of oxaliplatin and fluorouracil for the treatment of rectal
cancer, but the efficacy and adverse reactions of the two drugs
used for the treatment of rectal cancer are unclear. In addition,
study of oxaliplatin combined with fluorouracil on treatment
outcomes of conventional radiotherapy in the treatment of rectal
cancer is rare (10,11).
Therefore, this study investigated the therapeutic
efficacy and safety of oxaliplatin and fluorouracil combined with
radiotherapy in treatment of rectal cancer. In addition,
sensitization effects of oxaliplatin and fluorouracil on
radiotherapy were also explored to investigate the application
values of oxaliplatin and fluorouracil in treatment of patients
with rectal cancer.
Materials and methods
Research subjects
From March 2014 to March 2015, 73 patients with
rectal cancer confirmed by histopathological examinations were
selected in Laigang Hospital Affiliated to Taishan Medical
University (Laiwu, China). All 73 patients were older than 60 years
and had a mean age of 68.43±7.75 years. Among them, 40 were males
and 33 were females. All patients were diagnosed as rectal cancer
by histopathological examination. All patients received
radiotherapy and chemotherapy for the first time. None had been
treated with oxaliplatin and fluorouracil in the past or was
allergic to these drugs. Patients had no liver, kidney and other
organ dysfunction. Patients had no abnormal bleeding or coagulation
abnormalities. Patients who had been treated, patients with large
tumors, patients with other diseases of lung or chest wall, and
patients with lymph node metastasis were excluded. This study was
approved by the medical Ethics Committee of Laigang Hospital
Affiliated to Taishan Medical University. Patients or their
families signed an informed consent.
Human rectal cancer cell line SW837 (cat. no. C1258)
was purchased from Shanghai Guandao Bioengineering Co., Ltd.
(Shanghai, China) and cultured in RPMI-1640 medium (Shanghai
Gaochuang Chemical Technology Co., Ltd., Shanghai, China) in an
incubator (37°C, pH 6.8–7.4, 5% CO2).
Methods
Patients were randomly divided into 3 groups:
oxaliplatin group (25 cases): intravenous infusion of oxaliplatin
(100 mg/m2; Hubei Yuancheng Saichuang Science and
Technology Co., Ltd., Wuhan, China; state approval no. H20020648)
on the first day; fluorouracil group (24 cases): intravenous
infusion of fluorouracil (375 mg/m2, state approval no.
H20030345) from day 1 to day 5; combination group (24 cases),
intravenous infusion of oxaliplatin (100 mg/m2) on the
first day and intravenous infusion of fluorouracil (375
mg/m2) from day 1 to day 5. All patients were treated
with radiotherapy at the same time, radiation dose was 45.0–50.4 Gy
and 21 days was 1 course of treatment, and efficacy and safety were
evaluated after 2 courses of treatment. Treatment was performed
until disease progression or until toxicity could not be tolerated
by patients (no more than 6 courses of treatment).
Efficacy evaluation criteria (12): Efficacy was evaluated the first time
after 2 courses of diseases. Patients were divided into complete
remission (CR), partial remission (PR), stable disease (SD), and
progression disease (PD) groups according to conditions of solid
tumors. Remission rate (RR) = (CR+PR)/number of patients; disease
control rate (DCR) = (CR+PR+SD)/number of patients.
SW837 cells were cultured in RPMI-1640 medium
containing oxaliplatin (5 mg/l), fluorouracil (18 mg/l), or
oxaliplatin (5 mg/l) and fluorouracil (18 mg/l) for 6 h. Then
radiotherapy was performed with a dose of 6 Gy. MTT assay was used
to observe the inhibitory effects of oxaliplatin, fluorouracil, and
oxaliplatin combined with fluorouracil on proliferation of SW837
cells at 12, 24, 48 and 72 h after radiotherapy. Cell proliferation
and sensitization ratio were compared. Each experiment was
performed 3 times.
MTT assay to detect in vitro
proliferation of SW837
SW837 was used to prepare single cell suspension.
Cells were routinely cultured in a 96-well cell culture plate. Part
of the cultured cells was taken at 6 h and 20 µl of MTT (5 mg/ml)
was added, followed by incubation at 37°C for 4 h. Supernatant
containing the impurities was exhausted, and dimethyl sulfoxide
formulation was added and shaken on a horizontal shaker for 15 min.
Finally, the absorbance at 570 nm was measured by using an
enzyme-linked immunosorbent assay. The above steps were repeated at
12, 24, 48 and 72 h, respectively. MTT test kit was purchased from
Shanghai LM Bioengineering Co., Ltd. (Shanghai, China).
Statistical analysis
SPSS 19.0 (Asia Analytics Formerly SPSS, Beijing,
China) was used. Enumeration data were expressed as a rate and
compared by χ2 test. Measurement data was expressed as
mean ± standard deviation, and ANOVA was used for comparison among
groups, and repeated measures ANOVA was used for intra-group
comparisons, and LSD tests were used for comparison between two
groups, as post hoc tests. P<0.05 was considered to indicate a
statistically significant difference.
Results
General information
Seventy-three patients with rectal cancer had a mean
age of 68.43±7.75 years. Oxaliplatin group included 16 male and 9
female patients, with a mean age of 67.59±7.88 years. Fluorouracil
group included 15 male and 9 female patients, with a mean age of
69.13±7.24 years. Combination group included 16 males and 8
females, with a mean age of 68.57±8.13 years. There was no
difference in the basic data such as the average age, sex, and
clinical stages among the three groups (P>0.05) (Table I).
 | Table I.General information. |
Table I.
General information.
| Variables | Oxaliplatin
group | Fluorouracil
group | Combination
group | χ2/F | P-value |
|---|
| No. of cases | 25 | 24 | 24 |
|
|
| Sex (n, %) |
|
|
| 0.013 | 0.987 |
| Male | 16 (64.0) | 15 (62.5) | 16 (66.67) |
|
|
|
Female | 9
(36.0) | 9
(37.5) | 8 (33.3) |
|
|
| Age (years) | 67.59±7.88 | 69.13±7.24 | 68.57±8.13 | 0.248 | 0.781 |
| Ethnicity (n, %) |
|
|
| 0.073 | 0.931 |
|
Chinese | 21 (84.0) | 20 (83.3) | 21 (87.5) |
|
|
|
Minority | 4
(16.0) | 4
(16.7) | 3
(12.5) |
|
|
| Clinical stage (n,
%) |
|
|
| 0.027 | 0.974 |
|
T1+T2 | 16 (64.0) | 14 (58.3) | 15 (62.5) |
|
|
|
T3+T4 | 9
(36.0) | 10 (41.7) | 9
(37.5) |
|
|
| Place of residence
(n, %) |
|
|
| 0.006 | 0.994 |
|
Urban | 12 (48.0) | 12 (50.0) | 11 (45.8) |
|
|
| Rural
region | 13 (52.0) | 12 (50.0) | 13 (54.2) |
|
|
| Degree of
differentiation (n, %) |
|
|
| 0.058 | 0.945 |
| Highly
differentiated | 19 (76.0) | 17 (70.8) | 18 (75.0) |
|
|
|
Medium-low
differentiation | 6
(24.0) | 7
(29.2) | 6
(25.0) |
|
|
Analysis of treatment effects after
two courses of treatment
After two courses of treatment, ANOVA analysis
showed no significant differences in DCR, CR, PR, SD and PD among
the three groups (P>0.05), and there was statistical difference
in RR (P<0.05). LSD test results showed that RR was higher in
the combination group than in the oxaliplatin and the fluorouracil
groups (P<0.05), and there was no difference between the
oxaliplatin and the fluororacil groups (P>0.05) (Table II).
| Table II.Analysis of treatment effects after
two courses of treatment (n, %). |
Table II.
Analysis of treatment effects after
two courses of treatment (n, %).
| Variables | Oxaliplatin
group | Fluorouracil
group | Combination
group | χ2 | P-value |
|---|
| No. of cases | 25 | 24 | 24 |
|
|
| RR | 7 (28.0) | 6 (25.0) | 15
(62.5)a | 6.437 | 0.013 |
| DCR | 16 (64.0) | 16 (66.7) | 21 (87.5) | 3.431 | 0.068 |
| CR | 0 (0.0) | 1 (4.2) | 2 (8.3) | 2.163 | 0.146 |
| PR | 7 (28.0) | 5 (20.8) | 13 (54.2) | 3.733 | 0.057 |
| SD | 9 (36.0) | 10 (41.7) | 6 (25.0) | 0.814 | 0.370 |
| PD | 9 (36.0) | 8 (33.3) | 4 (16.7) | 2.219 | 0.141 |
Incidence of adverse reactions after 2
courses of treatment
ANOVA analysis showed that there were statistically
significant differences in incidence of neutropenia among three
groups (P<0.05), while there were no differences in incidence of
other adverse reactions (P>0.05). LSD test showed that incidence
of neutropenia was higher in the combination group than that in the
oxaliplatin and the fluorouracil groups (P<0.05). Incidence of
other adverse reactions in the combination group was not
significantly different from those in the oxaliplatin and the
fluorouracil groups (P>0.05) (Table
III).
| Table III.Incidence of adverse reactions after 2
courses of treatment (n, %). |
Table III.
Incidence of adverse reactions after 2
courses of treatment (n, %).
| Variables | Oxaliplatin
group | Fluorouracil
group | Combination
group | χ2 | P-value |
|---|
| No. of cases | 25 | 24 | 24 |
|
|
| Vomiting | 3 (12.0) | 15 (62.5) | 4 (16.67) | 0.160 | 0.690 |
| Diarrhea | 4 (16.0) | 11 (45.8) | 6 (25.0) | 0.511 | 0.477 |
| Neutropenia | 7 (28.0) | 6 (25.0) | 15
(62.5)a | 6.437 | 0.013 |
| Anemia | 6 (24.0) | 7 (29.2) | 12 (50.0) | 3.733 | 0.057 |
|
Thrombocytopenia | 8 (32.0) | 8 (33.3) | 9 (37.5) | 0.159 | 0.691 |
| Transaminase
elevating | 11 (44.0) | 10 (41.7) | 12 (50.0) | 0.169 | 0.682 |
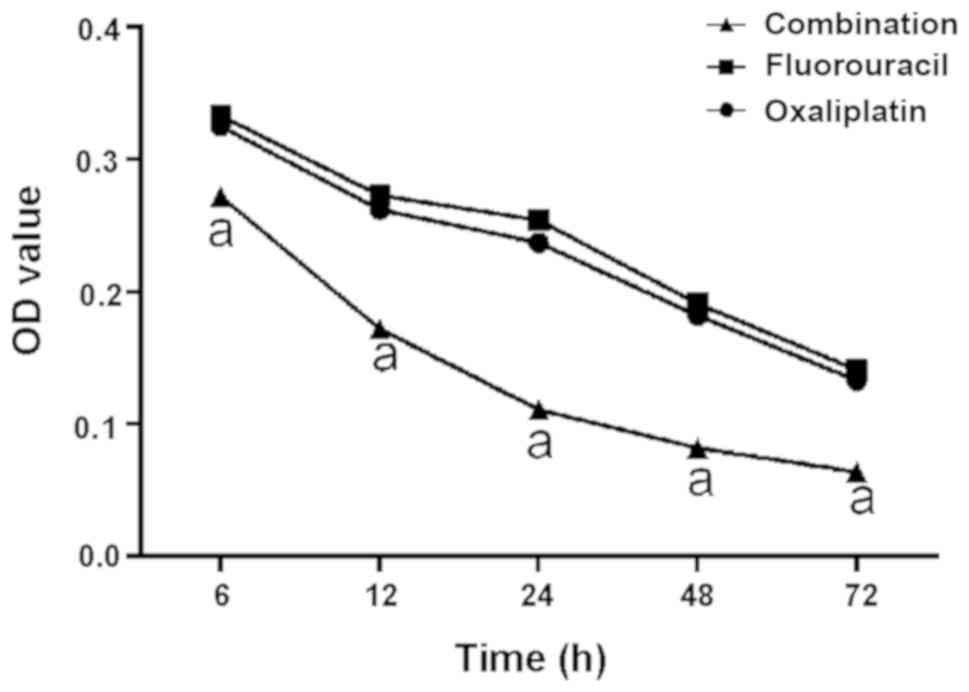
Radiosensitization of SW837 cells by
oxaliplatin and fluorouracil
In vitro proliferation assay of SW837 by MTT
assay showed that OD values of three groups of cells decreased with
time. No significant difference was found in OD values between
oxaliplatin and fluorouracil groups at 6, 12, 24, 48 and 72 h
(P>0.05). However, OD values at 6, 12, 24, 48 and 72 h points in
the combination group were lower than those in the oxaliplatin and
the fluorouracil groups (P<0.05). Proliferation ability of SW837
cells in the combination group was significantly lower than that in
the oxaliplatin and fluorouracil groups (P<0.05). ANOVA analysis
showed that sensitization was not significantly different among the
three groups of cells at 12 h (P>0.05), while significant
differences were found at 24, 48 and 72 h (P<0.05). LSD test
analysis showed that sensitization ratio of the combination group
was higher than that of the oxaliplatin and the fluorouracil groups
at 24, 48 and 72 h (P<0.05), while there was no significant
difference in sensitization ratio between the oxaliplatin and the
fluorouracil groups. Intragroup sensitization ratio comparison
results showed that sensitization ratios of the three groups of
cells at 24, 48 and 72 h were higher than those at 12 h
(P<0.05). There was no significant difference in sensitization
ratios among three groups of cells at 24 and 48 h (P>0.05), and
sensitization ratio at 72 h in the combination group was higher
than that at 24 and 48 h (P<0.05). Sensitization ratios of the
oxaliplatin and the fluorouracil groups at 72 h were not
significantly different from those at 24 and 48 h (P>0.05;
Fig. 1; Table IV).
| Table IV.Radiosensitization of SW837 cells by
oxaliplatin and fluorouracil. |
Table IV.
Radiosensitization of SW837 cells by
oxaliplatin and fluorouracil.
| Time period | Oxaliplatin
group | Fluorouracil
group | Combination
group | F | P-value |
|---|
| 12 h | 0.84±0.12 | 0.73±0.11 | 0.89±0.13 | 1.389 | 0.319 |
| 24 h | 1.58±0.24 | 1.42±0.23 |
2.01±0.41a | 6.440 | 0.032 |
| 48 h | 1.65±0.23 | 1.46±0.25 |
2.31±0.45a | 3.698 | 0.042 |
| 72 h | 1.83±0.35 | 1.80±0.33 |
3.44±0.56a | 14.54 | 0.005 |
Discussion
Progression of rectal cancer in elderly is
complicated and course of disease is long. Most patients are
diagnosed in middle and advanced stages. Health conditions in
elderly are poor and complications may easily happen. Old patients
have low tolerance to chemoradiation. Many elderly patients with
rectal cancer are also worried about the adverse reactions caused
by chemoradiation (13,14). Therefore, it is critical for elderly
patients to choose safe and effective drugs.
In this study, no significant differences in DCR,
CR, PR, SD and PD were found between the oxaliplatin and
fluorouracil groups. RR was higher in the combination group than
those in the oxaliplatin and fluorouracil groups. Rödel et
al (15) showed that oxaliplatin
combined with fluorouracil for adjuvant treatment of regional
rectal cancer can effectively improve the patient's clinical
staging. André et al (16)
also stated that combination of oxaliplatin and 5-fluorouracil for
treatment of colon cancer patients can effectively improve the
survival rate of patients. Similar findings were found in this
study, indicating that efficacy of oxaliplatin in combination with
fluorouracil for the treatment of rectal cancer is promising.
However, due to time constraints, we failed to obtain information
on the survival rate of patients. We will further analyze and
report on survival in future studies. Although the use of
oxaliplatin in combination with fluorouracil increased the efficacy
of rectal cancer treatment, it also increased the incidence of some
adverse reactions. For example, incidence of neutropenia in
patients receiving oxaliplatin and fluorouracil was higher than
that of patients received oxaliplatin and fluorouracil alone, and
incidence of anemia in patients treated with combination therapy
also increased. Hong et al (17) also found that the incidence of
neutropenia in patients with rectal cancer treated with oxaliplatin
combined with fluorouracil increased. Similar findings were found
in our study. However, incidence of vomiting and diarrhea showed
decline trend in patients treated with combination therapy,
compared with the fluorouracil group. Therefore, we speculate that
oxaliplatin may improve the digestive system of patients and
balance the adverse effects of fluorouracil on the digestive
system. However, both oxaliplatin and fluorouracil have
myelosuppressive effects (18,19),
which may increase the incidence of neutropenia and anemia.
Therefore, the safety still needs to be explored. This may be
related to the small sample size, and we will conduct a further
analysis with a large sample size to further confirm our
findings.
In this study, human rectal cancer cell line SW837
was used to investigate the radiosensitization of oxaliplatin and
fluorouracil. Results of this study found that oxaliplatin and
fluorouracil have a certain radiosensitization effects on SW837
cells during radiotherapy, and combination of the two drugs showed
stronger radiosensitization effects. After treatment with
radiotherapy for 72 h, sensitization effect of combination group
was twice higher than that of oxaliplatin and fluorouracil groups.
Study of oxaliplatin combined with fluorouracil for
radiosensitization is rare. Lee et al (20) reported that oxaliplatin can enhance
the sensitivity of rectal cancer to radiotherapy. Tang et al
(21) also reported that
fluorouracil can increase the radiosensitivity of human colorectal
cancer. Oxaliplatin (22) is a
platinum-based drug that antagonizes DNA replication and
transcription. Fluorouracil (23)
exerts an antitumor effect by blocking the conversion of
deoxyribose uric acid and interfering with the synthesis of DNA.
Mechanism of action of the two drugs is different, so theoretically
they can be used in combination to exert synergistic effects to
increase the radiosensitivity of tumor cells. However, clinical
studies are needed to verify the findings.
In conclusion, combination of oxaliplatin and
fluorouracil is safe and effective for the treatment of rectal
cancer in elderly. Combination of oxaliplatin and fluorouracil can
increase sensitivity of cancer cells to radiotherapy. So it should
be popularized in clinical practices.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
JX conceived the study and was responsible for the
treatment of patients. XLi was responsible for MTT assay. XLv
contributed to cell culture. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Laigang Hospital Affiliated to Taishan Medical University (Laiwu,
China). Signed informed consents were obtained from the patients or
the guardians.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Péron J, Bylicki O, Laude C, Martel-Lafay
I, Carrie C and Racadot S: Nonoperative management of squamous-cell
carcinoma of the rectum. Dis Colon Rectum. 58:60–64. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jeong BG, Kim DY and Kim SY: Concurrent
chemoradiotherapy for squamous cell carcinoma of the rectum.
Hepatogastroenterology. 60:512–516. 2013.PubMed/NCBI
|
|
3
|
Cancer Genome Atlas Network: Comprehensive
molecular characterization of human colon and rectal cancer.
Nature. 487:330–337. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Musio D, De Felice F, Manfrida S, Balducci
M, Meldolesi E, Gravina GL, Tombolini V and Valentini V: Squamous
cell carcinoma of the rectum: The treatment paradigm. Eur J Surg
Oncol. 41:1054–1058. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nagpal K and Bennett N: Colorectal surgery
and its impact on male sexual function. Curr Urol Rep. 14:279–284.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rouanet P, Mourregot A, Azar CC, Carrere
S, Gutowski M, Quenet F, Saint-Aubert B and Colombo PE: Transanal
endoscopic proctectomy: An innovative procedure for difficult
resection of rectal tumors in men with narrow pelvis. Dis Colon
Rectum. 56:408–415. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hendren S and Fiscella K: Patient
navigation improves the care experience for patients with newly
diagnosed cancer. J Clin Oncol. 32:3–4. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Moran MS, Schnitt SJ, Giuliano AE, Harris
JR, Khan SA, Horton J, Klimberg S, Chavez-MacGregor M, Freedman G,
Houssami N, et al: Society of Surgical Oncology-American Society
for Radiation Oncology consensus guideline on margins for
breast-conserving surgery with whole-breast irradiation in stages I
and II invasive breast cancer. Int J Radiat Oncol Biol Phys.
88:553–564. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Specht L, Yahalom J, Illidge T, Berthelsen
AK, Constine LS, Eich HT, Girinsky T, Hoppe RT, Mauch P, Mikhaeel
NG, et al: ILROG: Modern radiation therapy for Hodgkin lymphoma:
Field and dose guidelines from the international lymphoma radiation
oncology group (ILROG). Int J Radiat Oncol Biol Phys. 89:854–862.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Thuss-Patience PC, Hofheinz RD, Arnold D,
Florschütz A, Daum S, Kretzschmar A, Mantovani-Löffler L, Bichev D,
Breithaupt K, Kneba M, et al: Perioperative chemotherapy with
docetaxel, cisplatin and capecitabine (DCX) in gastro-oesophageal
adenocarcinoma: A phase II study of the Arbeitsgemeinschaft
Internistische Onkologie (AIO){dagger}. Ann Oncol. 23:2827–2834.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Schwartzberg LS, Rivera F, Karthaus M,
Fasola G, Canon JL, Hecht JR, Yu H, Oliner KS and Go WY: PEAK: A
randomized, multicenter phase II study of panitumumab plus modified
fluorouracil, leucovorin, and oxaliplatin (mFOLFOX6) or bevacizumab
plus mFOLFOX6 in patients with previously untreated, unresectable,
wild-type KRAS exon 2 metastatic colorectal cancer. J Clin Oncol.
32:2240–2247. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lai Q, Avolio AW, Graziadei I, Otto G,
Rossi M, Tisone G, Goffette P, Vogel W, Pitton MB and Lerut J:
European Hepatocellular Cancer Liver Transplant Study Group:
Alpha-fetoprotein and modified response evaluation criteria in
solid tumors progression after locoregional therapy as predictors
of hepatocellular cancer recurrence and death after
transplantation. Liver Transpl. 19:1108–1118. 2013.PubMed/NCBI
|
|
13
|
Marks J, Nassif G, Schoonyoung H, DeNittis
A, Zeger E, Mohiuddin M and Marks G: Sphincter-sparing surgery for
adenocarcinoma of the distal 3 cm of the true rectum: Results after
neoadjuvant therapy and minimally invasive radical surgery or local
excision. Surg Endosc. 27:4469–4477. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Muro K: Systemic chemotherapy for
metastatic colorectal cancer - Japanese Society for Cancer of the
Colon and Rectum (JSCCR) Guidelines 2016 for treatment of
colorectal cancer. Nihon Shokakibyo Gakkai Zasshi. 114:1217–1223.
2017.PubMed/NCBI
|
|
15
|
Rödel C, Graeven U, Fietkau R, Hohenberger
W, Hothorn T, Arnold D, Hofheinz RD, Ghadimi M, Wolff HA,
Lang-Welzenbach M, et al: German Rectal Cancer Study Group:
Oxaliplatin added to fluorouracil-based preoperative
chemoradiotherapy and postoperative chemotherapy of locally
advanced rectal cancer (the German CAO/ARO/AIO-04 study): Final
results of the multicentre, open-label, randomised, phase 3 trial.
Lancet Oncol. 16:979–989. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
André T, de Gramont A, Vernerey D,
Chibaudel B, Bonnetain F, Tijeras-Raballand A, Scriva A, Hickish T,
Tabernero J, Van Laethem JL, et al: Adjuvant fluorouracil,
leucovorin, and oxaliplatin in stage II to III colon cancer:
Updated 10-year survival and outcomes according to BRAF mutation
and mismatch repair status of the MOSAIC study. J Clin Oncol.
33:4176–4187. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hong YS, Nam BH, Kim KP, Kim JE, Park SJ,
Park YS, Park JO, Kim SY, Kim TY, Kim JH, et al: Oxaliplatin,
fluorouracil, and leucovorin versus fluorouracil and leucovorin as
adjuvant chemotherapy for locally advanced rectal cancer after
preoperative chemoradiotherapy (ADORE): An open-label, multicentre,
phase 2, randomised controlled trial. Lancet Oncol. 15:1245–1253.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Dai X, Zhang X, Wang C, Jiang J and Wu C:
Paclitaxel/oxaliplatin/fluorouracil (TOF) regimen versus
S-1/oxaliplatin (SOX) regimen for metastatic gastric cancer
patients. Oncotarget. 8:30495–30501. 2017.PubMed/NCBI
|
|
19
|
Xiao H, Xiong L, Song X, Jin P, Chen L,
Chen X, Yao H, Wang Y and Wang L: Angelica sinensis polysaccharides
ameliorate stress-induced premature senescence of hematopoietic
cell via protecting bone marrow stromal cells from oxidative
injuries caused by 5-fluorouracil. Int J Mol Sci. 18:182017.
View Article : Google Scholar
|
|
20
|
Lee EM, Hong YS, Kim KP, Lee JL, Kim SY,
Park YS, Choi DH, Kim JH, Lim SB, Yu CS, et al: Phase II study of
preoperative chemoradiation with S-1 plus oxaliplatin in patients
with locally advanced rectal cancer. Cancer Sci. 104:111–115. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tang M, Lu X, Zhang C, Du C, Cao L, Hou T,
Li Z, Tu B, Cao Z, Li Y, et al: Downregulation of SIRT7 by
5-fluorouracil induces radiosensitivity in human colorectal cancer.
Theranostics. 7:1346–1359. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gheidari F, Bakhshandeh B,
Teimoori-Toolabi L, Mehrtash A, Ghadir M and Zeinali S: TCF4
silencing sensitizes the colon cancer cell line to oxaliplatin as a
common chemotherapeutic drug. Anticancer Drugs. 25:908–916. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Amorim R, Pinheiro C, Miranda-Gonçalves V,
Pereira H, Moyer MP, Preto A and Baltazar F: Monocarboxylate
transport inhibition potentiates the cytotoxic effect of
5-fluorouracil in colorectal cancer cells. Cancer Lett. 365:68–78.
2015. View Article : Google Scholar : PubMed/NCBI
|