Introduction
Middle cerebral artery (MCA) aneurysms are among the
most common intracranial angioma in the anterior cerebral
circulation (1). The MCA bifurcation
is a preferred site for aneurysm formation, and is involved in
18–20% in all aneurysms encountered (2). A clinical study has indicated that MCA
aneurysms are typically complex, multi-lobed and incorporate
eloquent vascular branches (3).
Critical surgical management at strategic points has been applied
for the treatment of MCA aneurysms (4). Surgical treatments of poor-grade MCA
aneurysms are associated with large sylvian hematomas following
prophylactic hinged craniectomy (5).
Of note, clinical and radiologic outcomes have suggested that
endovascular treatment for MCA aneurysms has an acceptable safety
profile with low rates of technical failure and re-treatment
(6).
Endovascular treatment has been widely used for the
treatment of MCA aneurysms (7). A
previous study demonstrated that the low-profile visualized
intraluminal support (LVIS) device is a novel tool for the
treatment of wide-necked intracranial aneurysms (8). Endovascular and surgical options for
ruptured MCA aneurysms indicate the superiority of endovascular vs.
open microneurosurgical clipping for the treatment of ruptured MCA
bifurcation aneurysms (9). A study
also reported that the feasibility of the endovascular treatment of
MCA aneurysms may be assessed by using a procedural 3D imaging and
remodeling technique (10).
Endovascular treatment of MCA aneurysms with coils may be
successfully performed without inducing any neurologic deficits in
most patients (11). In addition,
endovascular treatment may be safely and effectively performed in
selected cases of MCA aneurysm (12). Initial subtotal aneurysm occlusion
may progress to total occlusion (13). Furthermore, endovascular treatment
for MCA aneurysms decreased the morbidity and mortality rates
compared with those achieved by conventional clipping, which
suggested that combined treatment by endovascular and bypass
surgery is capable of efficiently treating giant complex fusiform
MCA aneurysms (14). Of note, a
previous study has indicated that stent assistance contributed to
the beneficial effect of endovascular treatment of MCA aneurysms,
and identified that stent assistance achieves total or subtotal
occlusion of large and giant aneurysms in 90% of cases (15).
In the present study, the efficacy of endovascular
treatment with stent was evaluated in a total of 92 patients with
MCA aneurysm. The clinical presentation, aneurysmal
characteristics, technical feasibility and procedural
complications, as well as the angiographic and clinical follow-up
results were compared between patients who were treated with LVIS
stent or non-LVIS stent.
Materials and methods
Patient population
The present study included 92 patients with MCA
aneurysm who presented at Ningbo Second Hospital (Ningbo, China)
between June 2014 and May 2016. Patients who underwent surgical
with LVIS device or non-LVIS stent were recruited. Patients were
offered the choice between LVIS device or a non-LVIS stent. A total
of 50 patients were male (54.3%) and 42 patients were female
(45.7%). Their age ranged from 42.3 to 65.4 years (mean age,
53.85±11.55 years). A total of 53 patients (57.6%) received
endovascular treatment with LVIS stent and 39 (42.4%) received
endovascular treatment with non-LVIS stent (Table I). The major exclusion criteria were
as follows: A World Federation of Neurosurgical Societies grade 5
(16), massive cerebral infarction
(>50% of the MCA aneurysms) demonstrable on computed tomography
(CT) examination, and patients with a history of tumor, migraine,
cerebral hemorrhage or brain surgery injury. The major inclusion
criteria were as follows: Digital subtraction angiography imaging
studies demonstrating occlusion of a unilateral internal carotid
artery or MCA and a modified Rankin Scale (mRS) score of 0–2
(17). NRS scores of patients were
determined as described previously (18).
 | Table I.Clinical data of middle cerebral
artery aneurysm patients. |
Table I.
Clinical data of middle cerebral
artery aneurysm patients.
| Characteristic | Males | Females | P-value |
|---|
| Patients | 50 (54.3%) | 42 (45.7%) | 0.68 |
| Age (years) | 42.3–62.6 | 45.2–65.4 | 0.24 |
| Headache and
dizziness (pre-treatment) | 12 (13.0%) | 10 (10.9%) | 0.86 |
| Ischemic
infarction | 7 (7.6%) | 4 (4.3%) | 0.034 |
| Neck pain | 18 (19.6%) | 15 (16.3%) | 0.62 |
| Mass effect | 23 (25.0%) | 10 (10.9%) | 0.028 |
| Asymptomatic | 12 (13.0%) | 7 (7.6%) | 0.025 |
| Initial Raymond
grade |
|
|
|
| 1 | 19 (20.7%) | 17 (18.5%) | 0.83 |
| 2 | 17 (18.5%) | 14 (15.2%) | 0.62 |
| 3 | 14 (15.2%) | 11 (12.0%) | 0.78 |
| Procedural
complications | 10 (10.9%) | 8 (8.7%) | 0.86 |
| Aneurysm length
(mm) | 4.5–13.8 | 5.2–14.6 | 0.75 |
| Stent treatment |
|
|
|
| LVIS | 28 (30.4%) | 25 (27.2%) | 0.75 |
|
Non-LVIS | 22 (23.9%) | 17 (18.5%) | 0.36 |
Surgical procedure and LVIS
stenting
All surgical procedures were performed under general
anesthesia using biplane angiographic equipment. The 6F guiding
catheter was placed in the distal V2 segment of the vertebral
artery. Reconstructive treatment included the LVIS stent-assisted
or non-LVIS stent treatment. Stent sizes were selected according to
the largest diameter of the parent artery and the length of the
aneurysm. Other details of the surgical procedure were identical to
those described previously (19).
Angiographic and clinical assessment
and follow-up
Clinical outcomes were evaluated at the 6-month
follow up. The efficacy of endovascular treatment with LVIS stent
or non-LVIS stent was analyzed according to the Raymond
classification (20). The pre- and
post-operative angiographic analysis was generally performed at 0
and 6 months by using magnetic resonance angiography followed by
digital subtraction angiography (21).
CT scans
The MCA aneurysm patients were subjected to pre- and
post-operative CT scanning, and the volume of aneurysms (V) was
calculated using the following formula: V=a × b × c/2, with a,
height; b, length; and c, width. CT was performed to identify the
lesions as described previously (22). The clinical outcome at 6 months was
evaluated using the Glasgow outcome scale (23).
Headache score
The improvement of headache was determined by
assessing the headache at the 6-month follow-up compared with the
pre-operative one. In the present study, ‘markedly improved
headaches’ were defined as an increase in pain scores by 3–5 points
determined by a numeric rating scale (NRS) (24).
Statistical analysis
Statistical analyses were performed using SPSS 19.0
(IBM Corp., Armonk, NY, USA). Headache improvement of patients
after endovascular treatment with LVIS stent or non-LVIS stent was
compared using the unpaired 2-tailed t-test, Mann-Whitney
U-test or Pearson's χ2 test.
P<0.05 was considered to indicate a statistically
significant difference.
Results
Characteristics of MCA aneurysm
patients
A total of 92 patients with MCA aneurysm were
recruited in the present study. The mean age of the MCA aneurysm
patients was 53.85±11.55 years. The cohort included 50 male and 42
female patients. The clinical, demographic and angiographic
characteristics of the MCA aneurysm patients are summarized in
Table I. No significant difference
between the two groups was observed for ischemic infarction and
mass effect. A flow chart indicating the stages of the present
study is provided in Fig. 1.
Procedural complications and clinical
outcome
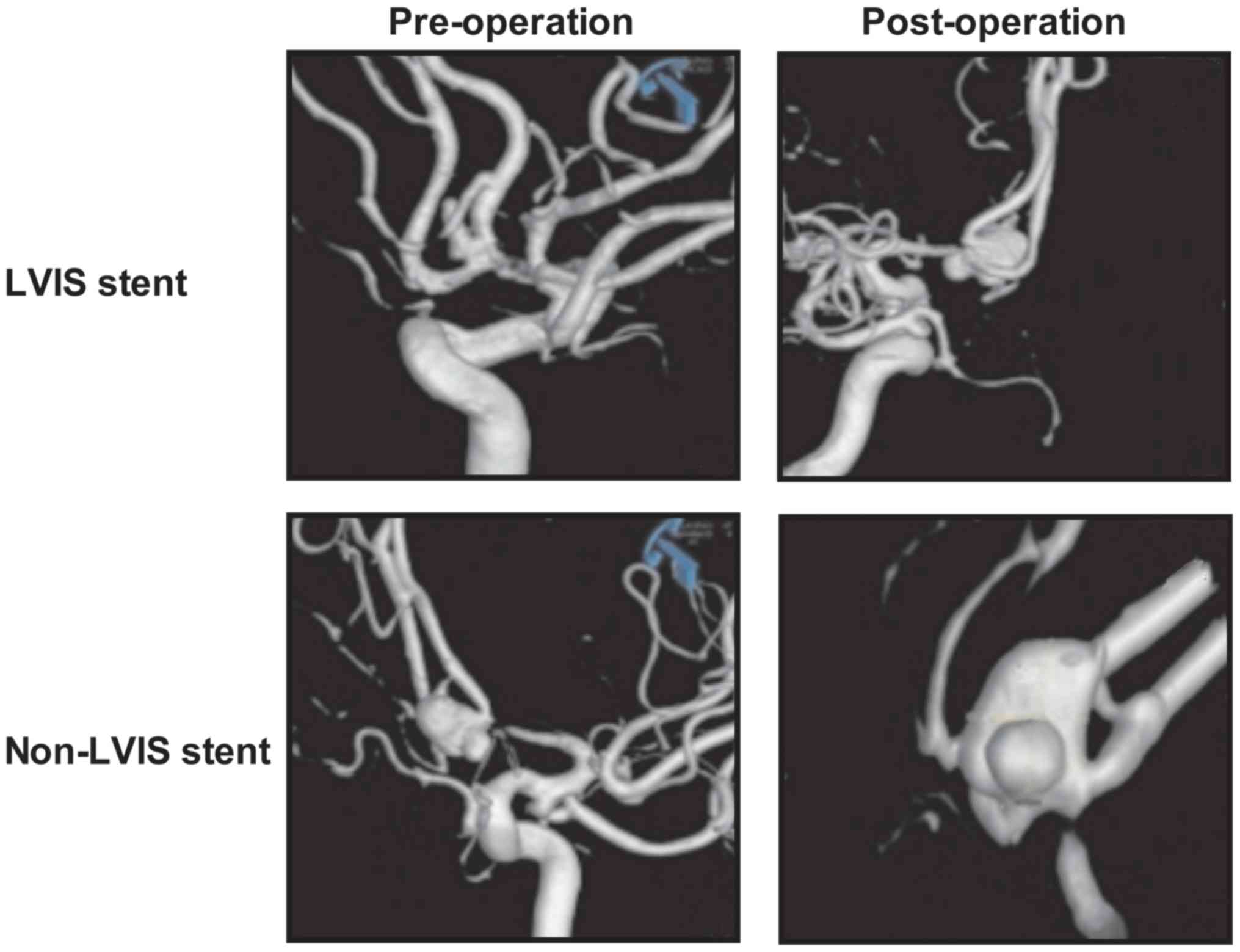
All patients with MCA aneurysm received successful
endovascular treatment with LVIS stent or non-LVIS stent. The
outcomes indicated that endovascular treatment with LVIS stent
removed a larger amount of hematoma compared with the non-LVIS
stent. Head angiography demonstrated that the aneurysms in the MCA
were removed in all patients after endovascular treatment with LVIS
stent or non-LVIS stent (Fig. 2). It
was observed that those patients who received endovascular
treatment with LVIS stent exhibited a better recovery according to
the GOS score compared with those subjected to endovascular
treatment with non-LVIS stent (Table
II).
| Table II.Clinical outcomes and mean ratio of
hematoma removal. |
Table II.
Clinical outcomes and mean ratio of
hematoma removal.
| Parameter | LVIS stent
(n=53) | Non-LVIS stent
(n=39) | P-value |
|---|
| Removal ratio of
hematoma in the first operation | 0.26±0.046 | 0.35±0.050 | 0.024 |
| GOS |
|
|
|
| 1 | 5 (9.4%) | 8
(20.5%) | 0.042 |
| 2 | 4 (7.5%) | 10 (25.6%) | 0.015 |
| 3 | 8
(19.0%) | 4
(10.3%) | 0.030 |
| 4 | 8
(19.0%) | 5
(12.8%) | 0.042 |
| 5 | 28 (52.8%) | 12 (30.8%) | 0.0048 |
Clinical outcome at follow-up
At follow-up, the mean headache NRS score in the
majority of patients who had received endovascular treatment with
LVIS stent was lower compared with that in the patients subjected
to endovascular treatment with non-LVIS stent. The post-operative
headaches of the 92 MCA aneurysm patients, including duration,
frequency, quality and intensity, based on the NRS score, are
listed in Table III. Outcomes
demonstrated that 4 (7.5%) patients experienced headache daily, 3
(5.7%) had a headache on 5–15 days per month and 46 (86.8%)
patients had a headache less frequently than that after
endovascular treatment with LVIS stent. However, 8 (20.5%) patients
suffered from headache daily, 10 (25.6%) patients had a headache on
5–15 days per month and 21 (53.8%) patients had a headache less
frequently than that after endovascular treatment with non-LVIS
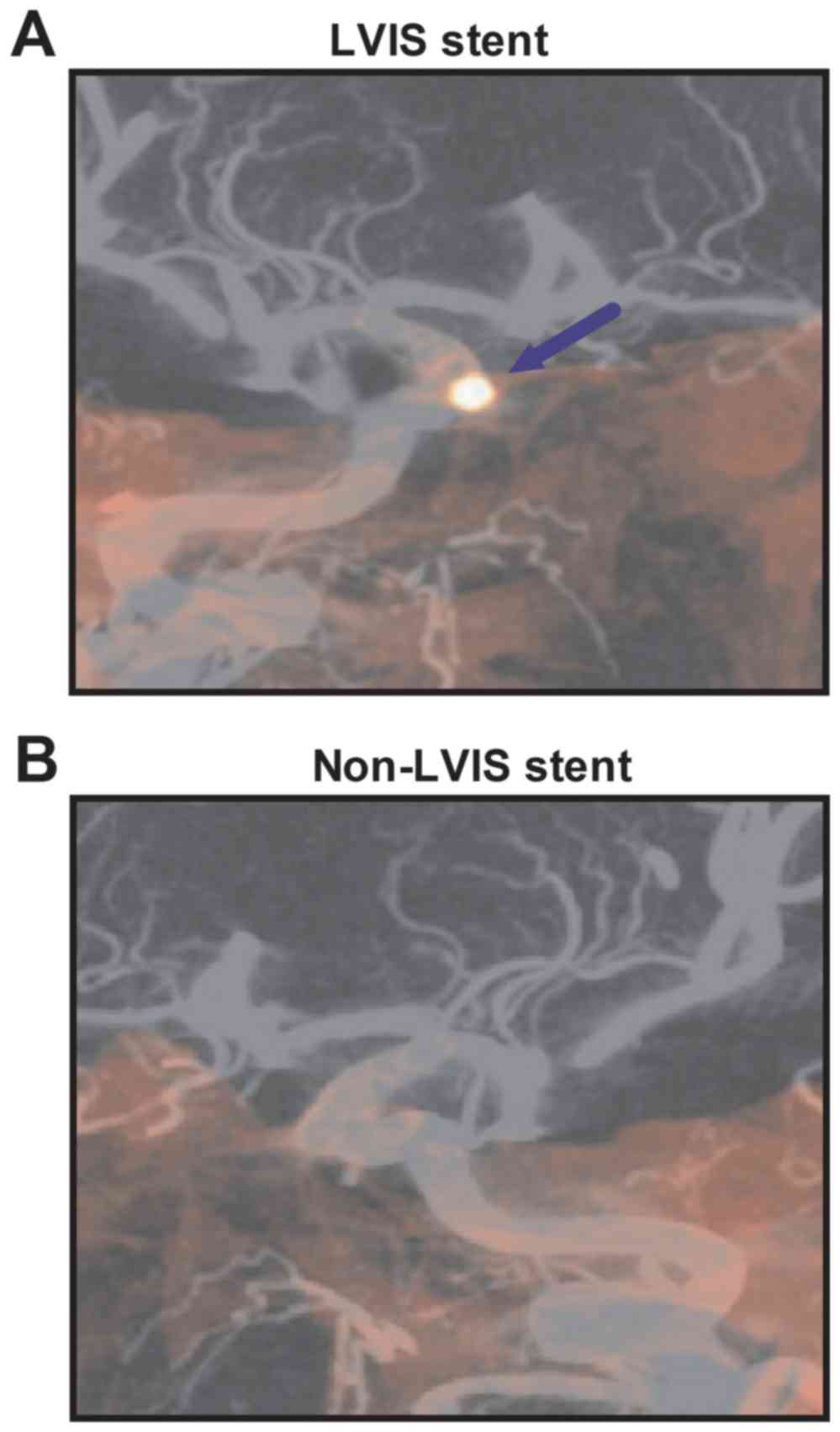
stent within the 6-months follow-up. Representative angiography
images of LVIS stent and non-LVIS stent cases were shown in
Fig. 3. The results of the LVIS
stent use exhibited an improved vascular morphology within the
aneurysm compared with the non-LVIS stent treatment.
| Table III.Characteristics of post-operative
headache. |
Table III.
Characteristics of post-operative
headache.
| Characteristic | LVIS stent (n=53)
(%) | Non-LVIS stent
(n=39) (%) | P-value |
|---|
| Frequency |
|
Daily | 4 (7.5) | 8 (20.5) | 0.036 |
| 5–15
days/month | 3 (5.7) | 10 (25.6) | 0.022 |
| 15–30
days/year | 46 (86.7) | 21 (53.8) | 0.0048 |
| Duration |
| <1
h | 14 (26.4) | 6 (15.4) | 0.0065 |
| 1–12
h | 2 (3.8) | 6 (15.4) | 0.036 |
| 1–2
days | 3 (5.7) | 8 (20.5) | 0.022 |
| 2–7
days | 1 (1.9) | 5 (12.8) | 0.0088 |
| Features |
|
Swelling | 1 (1.9) | 3 (7.7) | 0.0092 |
|
Pressure-like | 1 (1.9) | 2 (5.1) | 0.088 |
|
Throbbing | 2 (3.8) | 3 (7.7) | 0.078 |
|
Stabbing | 1 (1.9) | 4 (10.3) | 0.0083 |
|
Other | 2 (3.8) | 1 (2.6) | 0.688 |
| Intensity |
|
<1 | 46 (86.8) | 30 (76.9) | 0.0046 |
|
1–3 | 5 (9.4) | 3 (7.7) | 0.56 |
|
4–7 | 1 (1.9) | 4 (7.5) | 0.0083 |
|
8–10 | 1 (1.9) | 2 (5.1) | 0.688 |
Clinical efficacy and safety of
endovascular treatment with LVIS stent
The CT scan demonstrated that endovascular treatment
with LVIS stent significantly improved pre-operative and
intra-operative ruptures (data not shown). Outcomes revealed that
endovascular treatment with LVIS stent had less post-operative
symptoms and less disability than endovascular treatment with
non-LVIS stent (Table IV).
Exploratory outcomes were assessed to identify potential predictors
for headache improvement, intra-operative ruptures and disability
following endovascular treatment with LVIS stent and endovascular
treatment with non-LVIS stent, which may be used for evaluating
improvements of certain symptoms. Outcomes demonstrated that
patients in the LVIS stent group exhibited lower levels of chronic
migraine, tension-type intension and headache severity compared
with the non-LVIS stent group (Table
V).
| Table IV.Clinical complications of
endovascular treatment with LVIS stent. |
Table IV.
Clinical complications of
endovascular treatment with LVIS stent.
| Feature | LVIS stent (n=53)
(%) | Non-LVIS stent
(n=39) (%) | P-value |
|---|
| Pre-operative
ruptures | 0 (0) | 2 (5.1) | <0.01 |
| Intra-operative
ruptures | 2
(3.8) | 4
(10.3) |
0.038 |
| Post-operative
symptoms | 1
(1.9) | 3 (7.7) |
0.042 |
| Disability | 2
(3.8) | 7
(17.9) | <0.01 |
| Table V.Factors associated with headache
outcomes. |
Table V.
Factors associated with headache
outcomes.
| Characteristic | LVIS stent (n=53)
(%) | Non-LVIS stent
(n=39) (%) | P-value |
|---|
| Chronic
migraine | 2 (3.8) | 4 (10.3) |
0.84 |
| Tension-type
intension | 3 (5.7) | 6 (15.4) |
0.50 |
| Headache
severity | 2 (3.8) | 4 (7.7) |
0.84 |
| Posterior
circulation | 3 (5.7) | 5 (12.8) |
0.64 |
| Headache
improved | 43 (81.1) | 20 (51.3) | <0.01 |
| Headache not
improved | 10 (18.9) | 19 (48.7) | <0.01 |
Discussion
MCA aneurysms are the most common types of lesion in
the intracranial artery wall, and frequently lead to headache,
dizziness, ischemic infarction, neck pain and mass effect, while
certain cases may also be asymptomatic (25). Evidence has indicated that LVIS stent
assists in the mechanical removal of thromboembolisms after
embolization of MCA aneurysms (26,27). In
the present study, it was reported that endovascular treatment with
LVIS stent efficiently removed MCA aneurysms, significantly
improved the clinical symptoms and resulted in favorable outcomes.
LVIS stent is a novel device designed as an auxiliary for the
endovascular treatment of MCA aneurysms (28). The present study indicated that
endovascular treatment with LVIS stent significantly improved
headaches compared with endovascular treatment with non-LVIS
stent.
Endovascular treatment of MCA aneurysms with the
LVIS junior stent provided excellent trackability and
deliverability, and is safe and effective in the treatment of
wide-necked MCA aneurysms with tortuous and smaller parent vessels
(29). The present study reported
that endovascular treatment with LVIS stent is a safe method for
the treatment of MCA aneurysms in a total of 92 patients, which
also significantly improved the symptoms of MCA aneurysms,
including the duration, frequency, quality, location and intensity
of headaches. Wang et al (28) suggested that the LVIS stent has
certain hemodynamic effects on cerebral aneurysms. Ge et al
(30) have indicated that
endovascular treatment with LVIS stent may achieve a greater
complete or near-complete occlusion rate compared with the non-LVIS
stent treatment; however, there was no significant difference in
procedure-associated complications and clinical outcomes between
cases treated with LVIS and enterprise stents. The present study
indicated that endovascular treatment with LVIS stent resulted in
less post-operative symptoms and less cases with disability than
endovascular treatment with non-LVIS stent. However, the present
study only investigated endovascular treatment with the LVIS device
in a small population of patients with MCA aneurysms. Further
investigation of cerebral hemodynamics using positron emission
tomography after endovascular treatment with the LVIS stent or
non-LVIS stent should be performed in the future using a larger
number of MCA aneurysm patients.
A previous study has indicated that the LVIS stent
is a safe and effective device for endovascular treatment (31). The present study reported that
endovascular treatment using the LVIS stent significantly reduced
pre-operative and intra-operative ruptures, and resulted in less
post-operative symptoms and cases of disability than endovascular
treatment with non-LVIS stent according to the mRS.
Zhu et al (32) have indicated that the LVIS stent
decreased the risk of blood blister-like aneurysm recurrence
compared with the non-LVIS stent and did not increase the risk of
procedure-associated complications in 37 patients with intracranial
carotid artery. Although the present study did not the evaluate
risk of blood blister-like aneurysm recurrence, it indicated that
MCA aneurysm patients who received endovascular treatment with LVIS
stent had a better outcome compared with non-LVIS stent group. Of
note, exploratory outcomes suggested that endovascular treatment
with LVIS stent significantly improved factors associated with
headache outcomes, including chronic migraine, tension-type
intension, headache severity, posterior circulation.
In conclusion, the present study analyzed the
efficacy of endovascular treatment with LVIS stent in patients with
MCA aneurysm. It has been previously reported that endovascular
treatment with LVIS stent has certain hemodynamic effects on MCA
aneurysms. Given the complex technique and the efficacy of
endovascular treatment with LVIS stent, this method may be used to
decrease headache and post-operative syndrome, which should be
taken into consideration for patients with MCA aneurysm. However,
long-term and cohort studies are required to validate these results
in larger populations.
Acknowledgements
Not applicable.
Funding
No was funding received.
Availability of data and materials
The analyzed data sets generated during the study
are available from the corresponding author on reasonable
request.
Authors' contributions
XF performed the experiments, prepared and analyzed
experimental data. FC designed the experiments. The final version
of the manuscript has been read and approved by all authors.
Ethical approval and consent to
participate
This retrospective study was approved by the Ethics
Committee of Ningbo Second Hospital (Ningbo, China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Diaz OM, Rangel-Castilla L, Barber S, Mayo
RC, Klucznik R and Zhang YJ: Middle cerebral artery aneurysms: A
single-center series comparing endovascular and surgical treatment.
World Neurosurg. 81:322–329. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Baharoglu MI, Lauric A, Safain MG,
Hippelheuser J, Wu C and Malek AM: Widening and high inclination of
the middle cerebral artery bifurcation are associated with presence
of aneurysms. Stroke. 45:2649–2655. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Esposito G and Regli L: Reply to the
comment on the article ‘selective-targeted extra-intracranial
bypass surgery in complex middle cerebral artery aneurysms:
Correctly identifying the recipient artery using indocyanine green
videoangiography’: Recipient artery identification. Neurosurgery.
74:E457–E458. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mrak G, Paladino J, Stambolija V, Nemir J
and Sekhar LN: Treatment of giant and large fusiform middle
cerebral artery aneurysms with excision and interposition radial
artery graft in a 4-year-old child: Case report. Neurosurgery. 10
Suppl 1:E172–E177. 2014.PubMed/NCBI
|
|
5
|
Wang HJ, Ye YF, Shen Y, Zhu R, Yao DX and
Zhao HY: Surgical treatment of poor grade middle cerebral artery
aneurysms associated with large sylvian hematomas following
prophylactic hinged craniectomy. J Huazhong Univ Sci Technolog Med
Sci. 34:716–721. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mortimer AM, Bradley MD, Mews P, Molyneux
AJ and Renowden SA: Endovascular treatment of 300 consecutive
middle cerebral artery aneurysms: Clinical and radiologic outcomes.
AJNR Am J Neuroradiol. 35:706–714. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Eboli P, Ryan RW, Alexander JE and
Alexander MJ: Evolving role of endovascular treatment for MCA
bifurcation aneurysms: Case series of 184 aneurysms and review of
the literature. Neurol Res. 36:332–338. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Behme D, Weber A, Kowoll A, Berlis A,
Burke TH and Weber W: Low-profile visualized intraluminal support
device (LVIS Jr) as a novel tool in the treatment of wide-necked
intracranial aneurysms: Initial experience in 32 cases. J
Neurointerv Surg. 7:281–285. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Santiago-Dieppa DR, Pannell JS and
Khalessi AA: Endovascular and surgical options for ruptured middle
cerebral artery aneurysms: Review of the literature. Stroke Res
Treat. 2014:3159062014.PubMed/NCBI
|
|
10
|
Vanzin JR, Mounayer C, Piotin M, Spelle L,
Boissonnet H and Moret J: Endovascular treatment of unruptured
middle cerebral artery aneurysms. J Neuroradiol. 32:97–108. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Iijima A, Piotin M, Mounayer C, Spelle L,
Weill A and Moret J: Endovascular treatment with coils of 149
middle cerebral artery berry aneurysms. Radiology. 237:611–619.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lee CY, Kim CH, Sohn SI and Hong JH:
Urgent bypass surgery following failed endovascular treatment in
acute symptomatic stroke patient with MCA occlusion. Neurologist.
22:14–17. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Doerfler A, Wanke I, Goericke SL,
Wiedemayer H, Engelhorn T, Gizewski ER, Stolke D and Forsting M:
Endovascular treatment of middle cerebral artery aneurysms with
electrolytically detachable coils. AJNR Am J Neuroradiol.
27:513–520. 2006.PubMed/NCBI
|
|
14
|
Suzuki S, Tateshima S, Jahan R, Duckwiler
GR, Murayama Y, Gonzalez NR and Viñuela F: Endovascular treatment
of middle cerebral artery aneurysms with detachable coils:
Angiographic and clinical outcomes in 115 consecutive patients.
Neurosurgery. 64:876–889. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Arustamyan SR, Yakovlev SB, Bocharov AV,
Bukharin EY, Dorokhov PS, Mikeladze KG and Belousova OB:
Endovascular treatment of large and giant intracranial aneurysms
using stent assistance. Zh Vopr Neirokhir Im N N Burdenko.
79:28–37. 2015.(In English; Russian). View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Inamasu J, Nakae S, Ohmi T, Kogame H,
Kawazoe Y, Kumai T, Tanaka R, Wakako A, Kuwahara K, Ganaha T and
Hirose Y: The outcomes of early aneurysm repair in World federation
of neurosurgical societies grade V subarachnoid haemorrhage
patients with emphasis on those presenting with a Glasgow Coma
Scale score of 3. J Clin Neurosci. 33:142–147. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Patel N, Rao VA, Heilman-Espinoza ER, Lai
R, Quesada RA and Flint AC: Simple and reliable determination of
the modified rankin scale score in neurosurgical and neurological
patients: The mRS-9Q. Neurosurgery. 71:971–975. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Can A, Castro VM, Ozdemir YH, Dagen S, Yu
S, Dligach D, Finan S, Gainer V, Shadick NA, Murphy S, et al:
Association of intracranial aneurysm rupture with smoking duration,
intensity, and cessation. Neurology. 89:1408–1415. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang CC, Fang YB, Zhang P, Zhu X, Hong B,
Xu Y, Liu JM and Huang QH: Reconstructive endovascular treatment of
vertebral artery dissecting aneurysms with the Low-profile
visualized intraluminal support (LVIS) device. PLoS One.
12:e01800792017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Stapleton CJ, Torok CM, Rabinov JD,
Walcott BP, Mascitelli JR, Leslie-Mazwi TM, Hirsch JA, Yoo AJ,
Ogilvy CS and Patel AB: Validation of the modified raymond-roy
classification for intracranial aneurysms treated with coil
embolization. J Neurointerv Surg. 8:927–933. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Davis BJ, Oberstar E, Royalty K, Schafer S
and Mistretta C: Volumetric limiting spatial resolution analysis of
four-dimensional digital subtraction angiography. J Med Imaging
(Bellingham). 3:0135032016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Matsumoto M, Kodama N, Sakuma J, Sato S,
Oinuma M, Konno Y, Suzuki K, Sasaki T, Suzuki K, Katakura T and
Shishido F: 3D-CT arteriography and 3D-CT venography: The separate
demonstration of arterial-phase and venous-phase on 3D-CT
angiography in a single procedure. AJNR Am J Neuroradiol.
26:635–641. 2005.PubMed/NCBI
|
|
23
|
Hong I, Li CY and Velozo CA: Item-Level
Psychometrics of the Glasgow Outcome Scale: Extended Structured
Interviews. OTJR (Thorofare N J). 36:65–73. 2016.PubMed/NCBI
|
|
24
|
Alghadir AH, Anwer S and Iqbal ZA: The
psychometric properties of an Arabic numeric pain rating scale for
measuring osteoarthritis knee pain. Disabil Rehabil. 38:2392–2397.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Aoki T, Yoshitomi M, Yamamoto M, Hirohata
M and Morioka M: Ruptured de novo aneurysm arising at a site remote
from the anastomosis 14 years after superficial temporal
Artery-middle cerebral artery bypass: A case report. Neurosurgery.
71:E905–E909. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Alghamdi F, Mine B, Morais R, Scillia P
and Lubicz B: Stent-assisted coiling of intracranial aneurysms
located on small vessels: Midterm results with the LVIS Junior
stent in 40 patients with 43 aneurysms. Neuroradiology. 58:665–671.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Darflinger RJ and Chao K: Using the barrel
technique with the LVIS Jr (Low-profile Visualized Intraluminal
Support) stent to treat a wide neck MCA bifurcation aneurysm. J
Vasc Interv Neurol. 8:25–27. 2015.PubMed/NCBI
|
|
28
|
Wang C, Tian Z, Liu J, Jing L, Paliwal N,
Wang S, Zhang Y, Xiang J, Siddiqui AH, Meng H and Yang X: Flow
diverter effect of LVIS stent on cerebral aneurysm hemodynamics: A
comparison with Enterprise stents and the Pipeline device. J Transl
Med. 14:1992016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Feng Z, Li Q, Zhao R, Zhang P, Chen L, Xu
Y, Hong B, Zhao W, Liu J and Huang Q: Endovascular treatment of
middle cerebral artery aneurysm with the LVIS junior stent. J
Stroke Cerebrovasc Dis. 24:1357–1362. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ge H, Lv X, Yang X, He H, Jin H and Li Y:
LVIS stent versus enterprise stent for the treatment of unruptured
intracranial aneurysms. World Neurosurg. 91:365–370. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Luo JJ, Zhang ZH, Liu QX, Zhang W, Wang JH
and Yan ZP: Endovascular brachytherapy combined with stent
placement and TACE for treatment of HCC with main portal vein tumor
thrombus. Hepatol Int. 10:185–195. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhu D, Fang Y, Yang P, Zhang P, Chen L, Xu
Y, Hong B, Huang Q and Liu JM: Overlapped stenting combined with
coiling for blood Blister-like aneurysms: Comparison of low-profile
visualized intraluminal support (LVIS) stent and Non-LVIS stent.
World Neurosurg. 104:729–735. 2017. View Article : Google Scholar : PubMed/NCBI
|