Introduction
Cholangiocarcinoma is a common malignant tumor of
the digestive system, occurring in the hepatic duct and
extrahepatic bile duct. The main clinical manifestations include
serious progressive obstructive jaundice, impaired liver function,
slim body and underweight (1,2).
Patients with cholangiocarcinoma usually present a long history of
bile duct stones, which has a certain impact on patients'
psychological state and quality of life. These patients usually
have poor prognoses (3,4). As a malignant tumor originating from
the bile duct epithelial cells, cholangiocarcinoma is difficult to
detect in the early stage and has strong invasiveness. Therefore,
most patients reach the advanced stage at the time of diagnosis
(5). As far as the treatment of
cholangiocarcinoma is concerned, relief of progressive obstruction
is the first and necessary step, which is achieved by surgery in
order to restore the normal excretion of bile and eliminate
jaundice. The surgery is then followed by chemotherapy and other
treatments (6). Surgical treatment
is traumatic and can incur a profound stress response, influencing
patients' postoperative recovery and quality of life (7). Most patients with cholangiocarcinoma
are middle-aged or elderly people, who may experience difficulties
in their postoperative recovery due to age (8). In addition, patients' adverse reactions
to chemotherapy impose further burden to postoperative recovery.
Therefore, implementation of comprehensive rehabilitation therapy
is necessary to promote patients' recovery and improve quality of
life after surgical treatment of cholangiocarcinoma.
Comprehensive rehabilitation therapy for cancer
refers to a combination of medical treatment, psychological
counseling, nutritional support and physical exercise, aiming at
improving the quality of life, promoting patients' recovery and
prolonging survival (9). According
to studies, comprehensive rehabilitation therapy has already been
implemented in breast cancer (10)
and cervical cancer (11) with high
response rates. However, to the best of our knowledge, there is no
relevant report on comprehensive rehabilitation therapy implemented
in postoperative care of patients with cholangiocarcinoma. Studies
need to be conducted to determine if comprehensive rehabilitation
therapy is effective in a specific cancer in spite of successful
implementations in other cancers. This study aims to provide an
optimal solution to postoperative treatment of cholangiocarcinoma
by implementing comprehensive rehabilitation therapy in
postoperative patients with cholangiocarcinoma and exploring its
impact on patients' quality of life.
Patients and methods
Subjects
Retrospective analysis was performed on 219 patients
with cholangiocarcinoma who underwent surgery in Yidu Central
Hospital of Weifang (Weifang, China) from April 2014 to June 2017.
There were 138 males and 81 females with an average age of 63.5±6.4
years. Of these patients, 116 received comprehensive rehabilitation
therapy in addition to routine treatment after surgery and were
assigned to the experimental group. The remaining 103 patients
received only routine treatment after surgery and were assigned to
the control group. As shown in Table
I, there were no significant differences in sex, age, and
pathological staging between the two groups (P>0.05).
 | Table I.Patients' general medical records [n
(%)]. |
Table I.
Patients' general medical records [n
(%)].
| Variables | Experimental group
(n=116) | Control group
(n=103) | χ2
value | P-value |
|---|
| Sex |
|
| 0.064 | 0.800 |
| Male | 74 (63.79) | 64 (62.14) |
|
|
|
Female | 42 (36.21) | 39 (37.86) |
|
|
| Age (years) |
|
| 0.225 | 0.635 |
| ≤63 | 69 (59.48) | 58 (56.31) |
|
|
|
>63 | 47 (40.52) | 45 (43.69) |
|
|
| BMI
(kg/m2) |
|
| 0.061 | 0.805 |
| ≤21 | 65 (56.03) | 56 (54.37) |
|
|
|
>21 | 51 (43.97) | 47 (45.63) |
|
|
| Alcohol
consumption |
|
| 0.019 | 0.891 |
| Yes | 72 (62.07) | 63 (61.17) |
|
|
| No | 44 (37.93) | 40 (38.83) |
|
|
| Tumor location |
|
| 0.029 | 0.986 |
|
Intrahepatic
cholangiocarcinoma | 35 (30.17) | 30 (29.13) |
|
|
| Hilar
cholangiocarcinoma | 42 (36.21) | 38 (36.89) |
|
|
| Distal
cholangiocarcinoma | 39 (33.62) | 35 (33.98) |
|
|
| Pathological
type |
|
| 0.197 | 0.978 |
| Papillary
carcinoma | 41 (35.34) | 36 (34.95) |
|
|
|
Sclerosing cancer | 22 (18.97) | 19 (18.45) |
|
|
| Nodular
carcinoma | 32 (27.59) | 27 (26.21) |
|
|
| Diffuse
invasive carcinoma | 21 (18.10) | 21 (20.39) |
|
|
The study was approved by the Ethics Committee of
Yidu Central Hospital of Weifang. Patients who participated in this
research had complete clinical data. Signed informed consents were
obtained from the patients and/or guardians.
Inclusion and exclusion criteria
Patients who were diagnosed with cholangiocarcinoma
by pathological test were eligible for this study. Patients who met
the following criteria were excluded from this study: i) patients
who had already received chemotherapy and/or radiotherapy; ii)
patients who had other serious organ disorders; iii) patients who
were unable to undergo surgery; iv) patients who had
cognitive-communication disorders; and v) patients who were not
cooperative with the examination.
Methods
After surgery, patients in the control group
received only chemotherapy, while patients in the experimental
group received comprehensive rehabilitation therapy under expert
guidance in addition to chemotherapy. The detailed protocols are
given below. i) Nutritional support: patients were weak after
surgery, and the body was in a state of high metabolism. Their
diets were designed and prepared by professional nutritionists to
provide effective enteral and parenteral nutrition support. The
goal was to promote patients' physical recovery by improving their
nutritional status. After referring to The American Society for
Parenteral and Enteral Nutrition (12), a jejunal nutrition tube was indwelled
in each patient during operation, and at 12 h after surgery the
patient was fed with 5% glucose sodium chloride solution. When the
patient stayed in bed after surgery, the daily calorie intake of
the patient was 104.3 kJ, which could be increased to 125.7 kJ
after the patient got out of bed. If the patient had no discomfort,
enteral nutrition combined with parenteral nutrition was gradually
replaced by parenteral nutrition according to their condition and
gastrointestinal function. ii) Physical exercise: when the patient
woke up after surgery, stayed in bed to rest for 1 week. During
that time, the patient rested in a semi-reclining position to
better control drainage and breathing. The patient was later
instructed to carry out appropriate exercises by correctly changing
his body position in the bed. Early ambulation was always
encouraged. During ambulation, the patient was instructed to take
aerobic exercises, such as walking or Tai Chi, to promote recovery.
iii) Psychological counseling: after surgery patients may
experience postoperative irritability and anxiety associated with
pain. Therefore, in comprehensive rehabilitation therapy patients
received psychological counseling. Briefly, medical professionals
made more conversations with each individual patient on a daily
basis, and a group psychological counseling was run twice a week.
The goal was to relieve the patient's psychological stress, in
order to participate more actively in the overall rehabilitation.
iv) Health knowledge expansion: cancer knowledge was imparted to
patients and their families once or twice every week, especially
knowledge about cholangiocarcinoma. v) Miscellaneous: during
chemotherapy, patients could choose to listen to some soft and
light music. Music therapy could reduce distress associated with
chemotherapy by shifting patients' attention from chemotherapy to
something pleasant.
The clinical outcome, physical function,
psychological health status, and the nutritional status of
spatients in the two groups were assessed after the rehabilitation
treatment.
Observation indicators
Clinical outcome after 1 month of treatment was
evaluated and defined as complete remission, partial remission,
stable disease and progressive disease, according to the RECIST 1.1
guidelines (13). The response rate
was defined as the proportion of patients achieving complete
remission and partial remission. Nutritional status of patients
before surgery, at 1 day and at 1 month after surgery was measured
according to the Nutritional Risk Screening endorsed by the
European Society for Clinical Nutrition and Metabolism (ESPEN)
(14). The quality of life at 1
month after surgery was assessed based on the QLQ-C30 quality of
life questionnaire (15). The
questionnaire included 30 items in 5 categories: role function,
physical function, emotional function, cognitive function and
social function. Higher score indicated higher quality of life. The
negative emotions that patients experienced at 1 month after
surgery were assessed using the self-rating anxiety scale (SAS) and
the self-rating depression scale (SDS) (16).
Statistical analysis
The data acquired in this study were analyzed using
SPSS 19.0 statistics software from Asia Analytics (formerly SPSS
China, Beijing, China). χ2 test was used for the
comparison of enumeration data. t-test was used for the comparison
of measurement data. P<0.05 was considered to indicate a
statistically significant difference.
Results
Clinical outcomes in the two
groups
As shown in Table
II, after surgery and chemotherapy, the clinical outcome in the
experimental group was: 10 cases with complete remission, 79 cases
with partial remission, 17 cases with stable disease, and 10 cases
with progressive disease. The response rate was 76.72%. The
clinical outcome in the control group was: 3 cases with complete
remission, 45 cases with partial remission, 40 cases with stable
disease, and 15 cases with progressive disease. The response rate
was 46.60%. Thus, the response rate in the experimental group was
significantly higher than that in the control group
(P<0.05).
| Table II.Clinical outcomes in the two groups [n
(%)]. |
Table II.
Clinical outcomes in the two groups [n
(%)].
| Outcome | Experimental group
(n=116) | Control group
(n=103) | χ2
value | P-value |
|---|
| Complete
remission | 10 (8.62) | 3 (2.91) | − | − |
| Partial
remission | 79
(68.10) | 45 (43.69) | − | − |
| Stable disease | 17
(14.66) | 40 (38.83) | − | − |
| Progressive
disease | 10 (8.62) | 15 (14.56) | − | − |
| Response rate | 89
(76.72) | 48 (46.60) | 21.13 | <0.001 |
Nutritional status scores in the two
groups
As shown in Table
III, the nutritional status scores before surgery, at 1 day and
at 1 month after surgery were 22.31±3.26, 20.17±2.12 and 28.52±2.73
points, respectively, in the experimental group, and 23.01±3.18,
20.56±2.23 and 24.16±2.09 points, respectively, in the control
group. There were no significant differences in nutritional status
scores between the two groups before surgery and at 1 day after
surgery. However, at 1 month after surgery, the nutritional status
score in the experimental group was significantly higher than that
in the control group (P<0.05).
| Table III.Nutritional status scores in the two
groups. |
Table III.
Nutritional status scores in the two
groups.
| Time point | Experimental group
(n=116) | Control group
(n=103) | t value | P-value |
|---|
| Before surgery | 22.31±3.26 | 23.01±3.18 | 1.604 | 0.110 |
| 1 day after
surgery | 20.17±2.12 | 20.56±2.23 | 1.326 | 0.186 |
| 1 month after
surgery | 28.52±2.73 | 24.16±2.09 | 13.14 | <0.001 |
Quality of life scores at 1 month
after surgery in the two groups
As shown in Table
IV, the scores for the role function, physical function,
emotional function, cognitive function and social function in the
experimental group were all higher than those in the control group,
and the differences were statistically significant (P<0.05).
| Table IV.Quality of life scores at 1 month
after surgery in the two groups. |
Table IV.
Quality of life scores at 1 month
after surgery in the two groups.
| Category | Experimental group
(n=116) | Control group
(n=103) | t value | P-value |
|---|
| Role function | 76.76±3.18 | 58.55±2.79 | 44.79 | <0.001 |
| Physical
function | 73.16±2.93 | 59.12±2.78 | 36.25 | <0.001 |
| Emotional
function | 74.12±2.89 | 60.11±3.09 | 34.66 | <0.001 |
| Cognitive
function | 72.69±3.11 | 59.54±2.91 | 32.19 | <0.001 |
| Social
function | 73.87±2.77 | 58.69±2.90 | 39.59 | <0.001 |
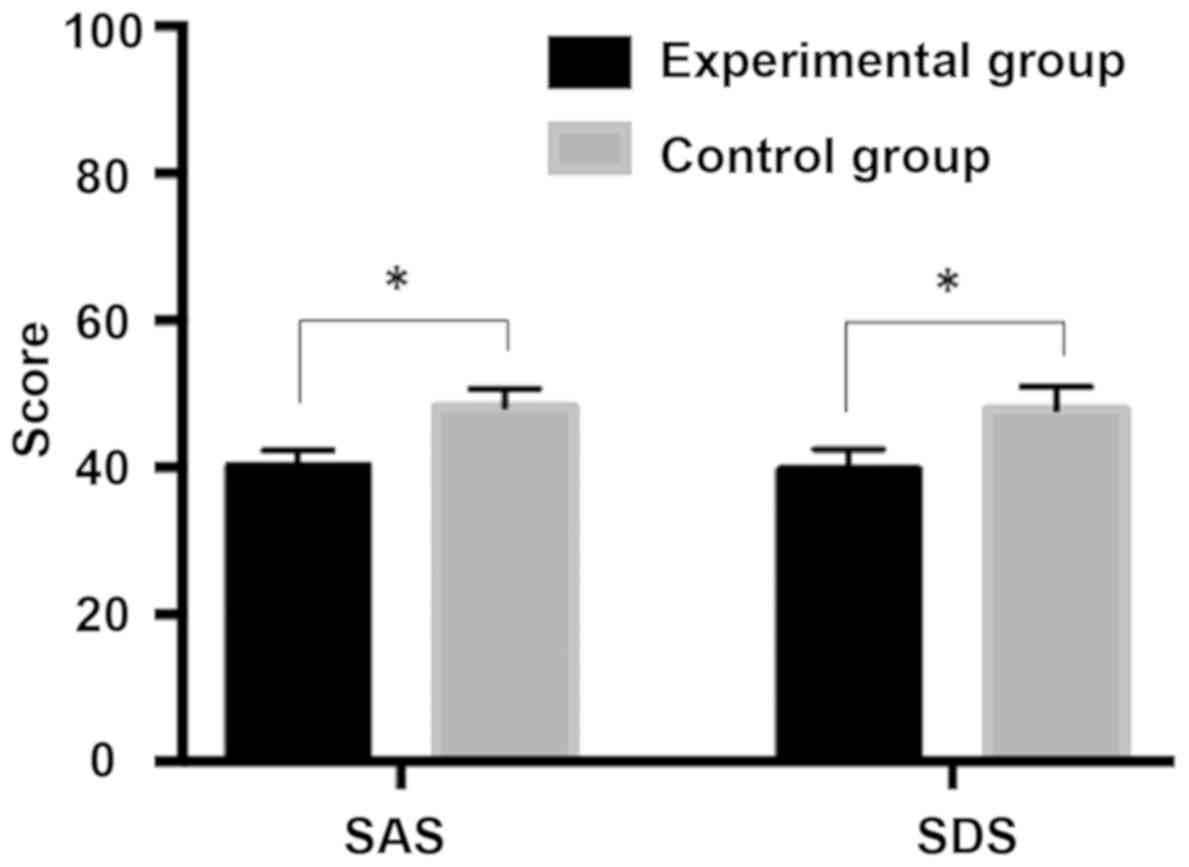
SAS and SDS scores at 1 month after
surgery in the two groups
As shown in Table V
and Fig. 1, the SAS and SDS scores
were 40.12±2.13 and 39.66±2.79 points, respectively, in the
experimental group, and 48.17±2.56 and 47.91±3.03 points;
respectively; in the control group. Apparently, both scores in the
experimental group were significantly lower than those in the
control group, and the differences were statistically significant
(P<0.05).
| Table V.SAS and SDS scores at 1 month after
surgery in the two groups. |
Table V.
SAS and SDS scores at 1 month after
surgery in the two groups.
| Score | Experimental group
(n=116) | Control group
(n=103) | t value | P-value |
|---|
| SAS | 40.12±2.13 | 48.17±2.56 | 25.39 | <0.001 |
| SDS | 39.66±2.79 | 47.91±3.03 | 20.97 | <0.001 |
Discussion
Currently, the main treatment methods for
cholangiocarcinoma are surgery, radiotherapy and chemotherapy. In
terms of surgical treatment, both operation and intraoperative
anesthesia can cause tissue trauma and mental distress to patients
(17). In addition, postoperative
pain can lead to stress reactions as well as negative emotions,
while radiotherapy and chemotherapy may cause adverse reactions,
thereby extending hospital stay (18). Seifter has reported that multiple
problems, such as functional disorders, psychological disorders,
physical disability, and social disorders exist at different levels
in most cancer patients (19).
Therefore, the implementation of comprehensive rehabilitation
therapy for cancer patients is becoming increasingly urgent.
Although it has been proposed to implement psychological
counseling, nutritional support and physical exercise in
postoperative care of cancer patients to improve their quality of
life (20), there is still little
research on comprehensive rehabilitation therapy for cancer
patients. In this study, comprehensive rehabilitation therapy was
implemented in postoperative care of patients with
cholangiocarcinoma, and its impact on patients' quality of life was
explored, aiming at finding a better solution for postoperative
recovery of patients with cholangiocarcinoma.
Comparing the clinical outcomes at 1 month after
surgery between the two groups, it was found that the response rate
in the experimental group (76.72%) was significantly higher than
that in the control group (46.60%), and the difference was
statistically significant (P<0.05). This finding suggests that
implementing comprehensive rehabilitation therapy enhances the
therapeutic efficacy of surgery and chemotherapy in patients. The
underlying reason of this effect is that the improvement of
patients' mood and quality of life due to comprehensive
rehabilitation therapy made patients more cooperative in the
treatment. As a result, more favorable clinical outcome was
observed. Comparing the nutritional status scores, quality of life
scores, and SAS and SDS scores at 1 month after surgery between the
two groups, it was found that all the scores in the experimental
group were significantly better than those in the control group
(P<0.05). These findings indicate that implementing
comprehensive rehabilitation therapy improves patients' quality of
life and promotes their acceptance of and integration into the
normal social life; plus, the dietary guidance for patients can
effectively improve the nutritional status of patients. Good health
and psychological counseling reduced the negative emotions of
patients. Patients were more cooperative in postoperative
chemotherapy and their overall recovery when they were in a healthy
psychological and physiological state. Our results are consistent
with a literature report, in which Saggini et al concluded
that comprehensive rehabilitation therapy in cancer patients
significantly improves patients' quality of life (21). In the present study, we did not
however develop different comprehensive rehabilitation treatment
plans for patients at different stages of cholangiocarcinoma, which
is the limitation of the current research, and still needs to be
addressed.
In summary, in clinical anticancer treatment,
synergistic implementation of comprehensive rehabilitation therapy
can improve cholangiocarcinoma patients' psychological health
status, nutritional status and overall quality of life, and reduce
the impact of negative emotions on patients' physical state.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
SL and LZ were responsible for the surgery and
chemotherapy treatment; LA assisted with observation indicators.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Yidu Central Hospital of Weifang (Weifang, China). Patients who
participated in this research had complete clinical data. Signed
informed consents were obtained from the patients and/or
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jonas S, Benckert C, Thelen A,
Lopez-Hänninen E, Rösch T and Neuhaus P: Radical surgery for hilar
cholangiocarcinoma. Eur J Surg Oncol. 34:263–271. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Khan SA, Thomas HC, Davidson BR and
Taylor-Robinson SD: Cholangiocarcinoma. Lancet. 366:1303–1314.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Koh KC, Lee H, Choi MS, Lee JH, Paik SW,
Yoo BC, Rhee JC, Cho JW, Park CK and Kim HJ: Clinicopathologic
features and prognosis of combined hepatocellular
cholangiocarcinoma. Am J Surg. 189:120–125. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Choi SB, Kim KS, Choi JY, Park SW, Choi
JS, Lee WJ and Chung JB: The prognosis and survival outcome of
intrahepatic cholangiocarcinoma following surgical resection:
Association of lymph node metastasis and lymph node dissection with
survival. Ann Surg Oncol. 16:3048–3056. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wang M, Fang M, Zhu J, Feng H, Warner E,
Yi C, Ji J, Gu X and Gao C: Serum N-glycans outperform CA19-9 in
diagnosis of extrahepatic cholangiocarcinoma. Electrophoresis.
38:2749–2756. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Morise Z, Sugioka A, Tokoro T, Tanahashi
Y, Okabe Y, Kagawa T and Takeura C: Surgery and chemotherapy for
intrahepatic cholangiocarcinoma. World J Hepatol. 2:58–64. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee SG, Song GW, Hwang S, Ha TY, Moon DB,
Jung DH, Kim KH, Ahn CS, Kim MH, Lee SK, et al: Surgical treatment
of hilar cholangiocarcinoma in the new era: The Asan experience. J
Hepatobiliary Pancreat Sci. 17:476–489. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lazaridis KN and Gores GJ:
Cholangiocarcinoma. Gastroenterology. 128:1655–1667. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Huether A, Höpfner M, Baradari V, Schuppan
D and Scherübl H: Sorafenib alone or as combination therapy for
growth control of cholangiocarcinoma. Biochem Pharmacol.
73:1308–1317. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cho OH, Yoo YS and Kim NC: Efficacy of
comprehensive group rehabilitation for women with early breast
cancer in South Korea. Nurs Health Sci. 8:140–146. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tilley DM, Hristov S, Templeton DJ, Sharp
NC and O'Connor CC: Cervical cancer screening and abnormalities
among women in a residential drug-rehabilitation program. Aust J
Prim Health. 18:266–267. 2012. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Compher C, Jain AK, Nichol PF, Blackmer A,
Earthman C, Evans DC, McCarthy MS, Taylor B and Mehta N: Research
Agenda 2018: The American Society for Parenteral and Enteral
Nutrition. JPEN J Parenter Enteral Nutr. 42:838–844. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tsuchida Y and Therasse P: Response
evaluation criteria in solid tumors (RECIST): New guidelines. Med
Pediatr Oncol. 37:1–3. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Donini LM, Poggiogalle E, Molfino A,
Rosano A, Lenzi A, Rossi Fanelli F and Muscaritoli M:
Mini-nutritional assessment, malnutrition universal screening tool,
and nutrition risk screening tool for the nutritional evaluation of
older nursing home residents. J Am Med Dir Assoc.
17:959.e11–959.e18. 2016. View Article : Google Scholar
|
|
15
|
Derogar M, van der Schaaf M and Lagergren
P: Reference values for the EORTC QLQ-C30 quality of life
questionnaire in a random sample of the Swedish population. Acta
Oncol. 51:10–16. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dunstan DA, Scott N and Todd AK: Screening
for anxiety and depression: Reassessing the utility of the Zung
scales. BMC Psychiatry. 17:3292017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Doherty B, Nambudiri VE and Palmer WC:
Update on the diagnosis and treatment of cholangiocarcinoma. Curr
Gastroenterol Rep. 19:22017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Xue F and Huang F: The effect of
psychological intervention on nutrient status of perioperative
patients with lung cancer. Iran J Public Health. 47:531–537.
2018.PubMed/NCBI
|
|
19
|
Seifter EJ: Clinical Oncology, Second
Edition. J Natl Cancer Inst. 93:632001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Saotome T, Klein L and Faux S: Cancer
rehabilitation: A barometer for survival? Support Care Cancer.
23:3033–3041. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Saggini R, Bellomo RG, Carmignano SM and
Saggini A: Cancer pain - the role of an integrated, comprehensive
rehabilitation program in its management. In: Updates on Cancer
Treatment. Rangel LBA and Silva IV: InTech. 2015
|