Introduction
Sepsis refers to an unregulated host response caused
by an infection, resulting in life-threatening organ dysfunction.
Conditions of sepsis usually progress rapidly and the prognosis is
poor. Sepsis is the main cause of death in ICU (1). Abnormal coagulation system is
considered as one of the important mechanisms of the occurrence and
development of sepsis and multiple organ dysfunction syndrome
(2). With the progression of sepsis,
the presence of coagulopathy and coagulation dysfunction is an
independent factor affecting the outcome of the disease (3). Abnormality of various coagulation
function indicators such as D-dimer, platelet count (PLT),
prothrombin time (PT), activated partial thromboplastin time
(APTT), and fibrinogen (FIB) was closely correlated with the
severity of sepsis (4).
Thromboelastography (TEG) is a simple,
cytological-based coagulation test that has the advantages of short
measurement time, low blood use, and unaffected heparin. TEG can
trace the coagulation process of the body as a form of a graph,
which can more intuitively reflect the interaction of various
substances in the blood coagulation process (5). TEG reflects the whole process from the
beginning of coagulation to the dissolution of blood clots through
R values, K value, Angle, MA, comprehensive coagulation index (CI)
and LY30. Those factors reflect changes in clotting factors,
platelets, fibrin, and fibrinolysis at various stages of
coagulation. As a result of the effect, the overall functional
status of all substances participating in the clotting process is
monitored (6). Studies have
confirmed that the MA value in TEG testing is a comprehensive
assessment of the quantity and function of FIB and platelets
involved in blood clot formation and can effectively reflect the
functional status of platelets (7,8). Both
the α-angle and K-time are indicators of FIB function, so the
changes in FIB function can be analyzed based on α-angle and
K-time. Previous findings have shown that monitoring patients'
coagulation parameters and TEG parameters can help determine the
prognosis and severity of the disease (9). TEG is easy to operate and the graphic
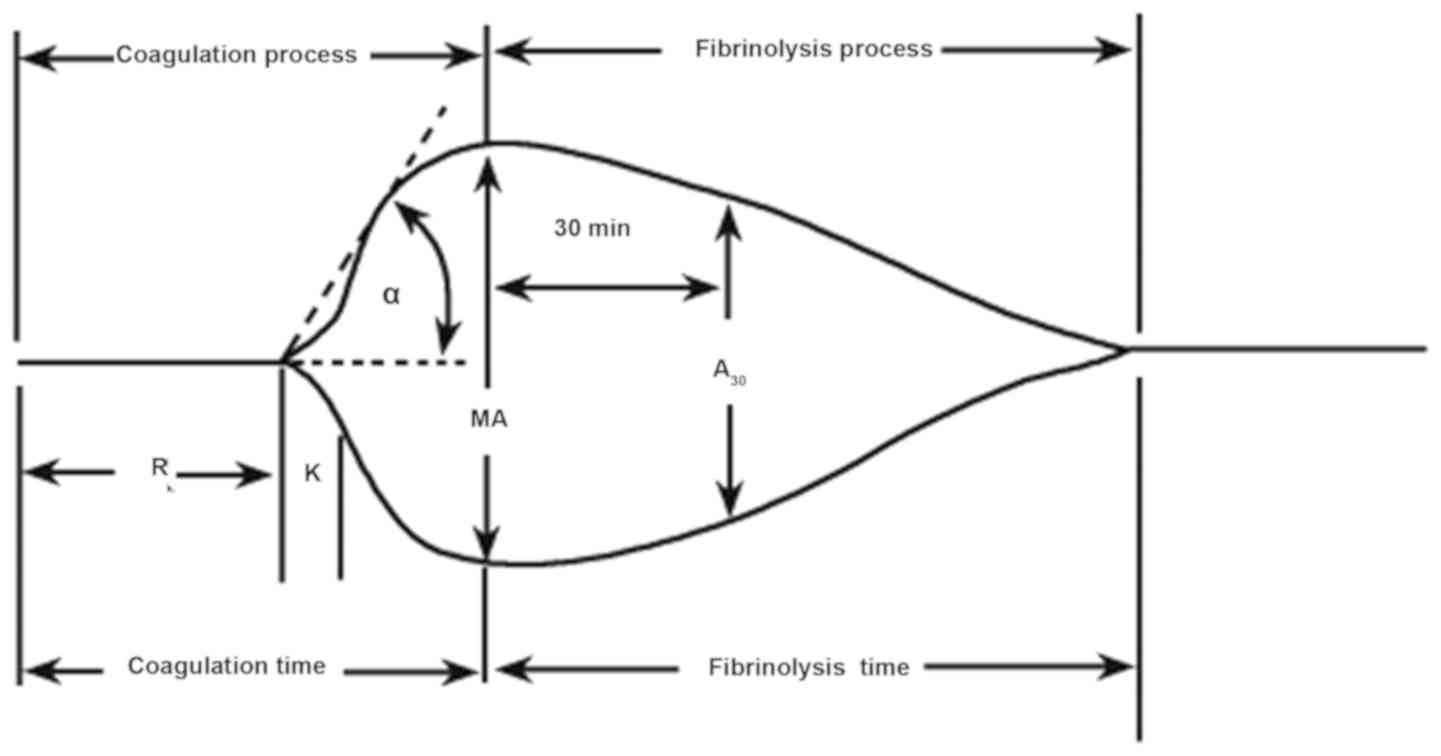
is easy to understand. The schematic diagram and diagnostic tree of
the TEG are shown in Figs. 1 and
2.
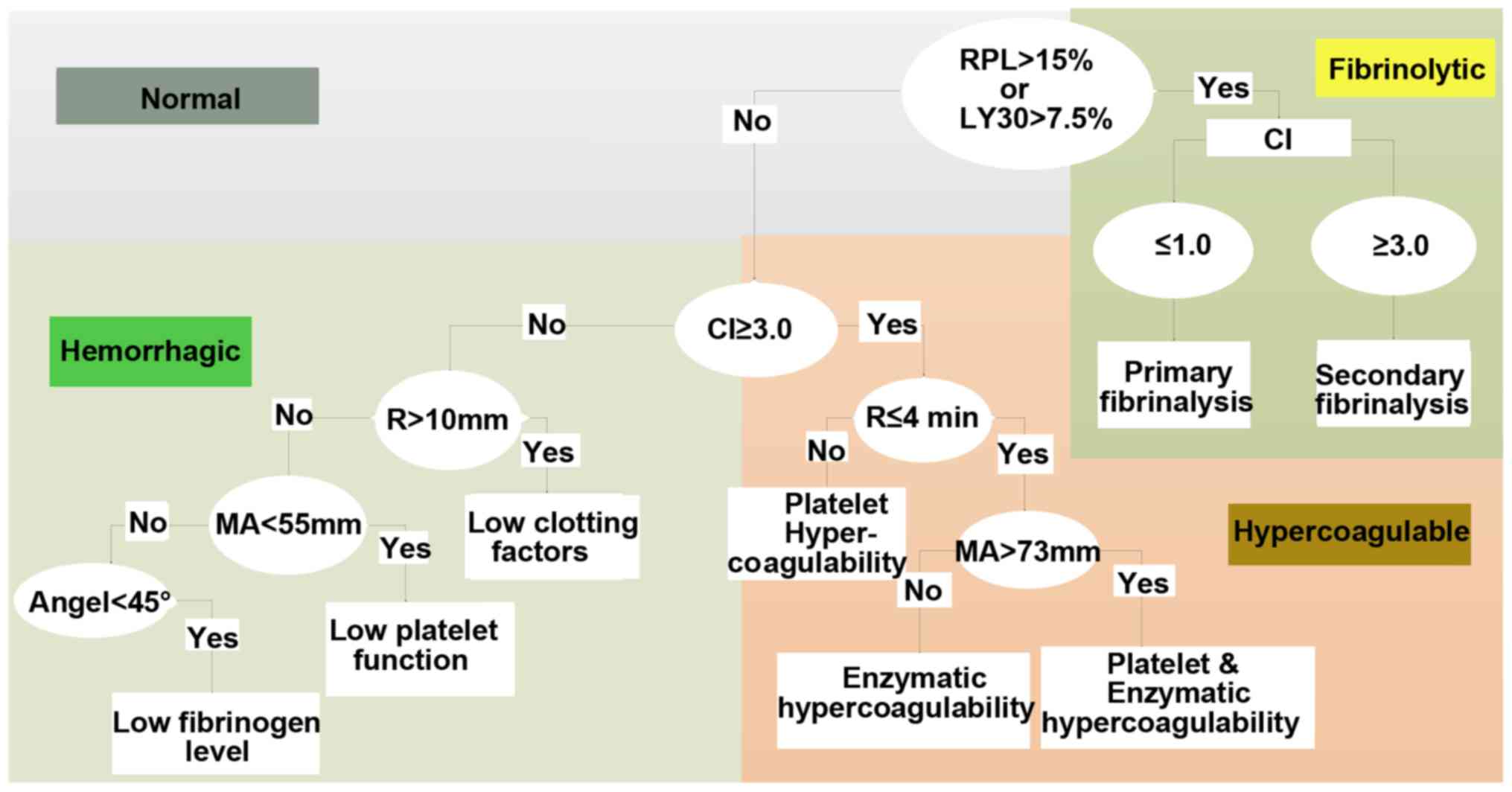 | Figure 2.Diagnostic tree of the TEG. R time,
refers to the time from the start to the amplitude of 2 mm in TEG
image. The R time reflects the process of coagulation initiation.
The prolonged R value represents the lack of clotting factor in the
body, indicating a hypocoagulable state, and conversely indicating
a hypercoagulable state in the body. K time, refers to the time
between the amplitude of 2 and 20 mm in the TEG image. K time
reflects the rate of blood clot formation and is an indicator of
FIB function. The prolongation of K time suggested that the
function of FIB was reduced, and on the contrary, it meant that FIB
was hyperfunctioning. α angle is the slope from R to K in the TEG
image. K time and α angle reflect the common effect of fibrin and
platelets on the beginning of clot formation. The MA value reflects
the maximum hardness or strength of the clot formation. The main
manifestation is the platelet aggregation function, which can also
reflect the stability of the thrombus. The increase of MA value
indicates that the platelet function is hyperactive, and vice versa
is the reduced platelet function. CI is a comprehensive coagulation
that reflects the overall state of coagulation. Normal value of CI
is between −3 and 3; CI <-3 indicates hypocoagulable state, and
conversely suggests a hypercoagulable state. LY30 refers to the
percentage of fibrinolysis 30 min after the clot reached maximum
intensity and indicates the rate of fibrinolysis. TEG,
thromboelastography; FIB, fibrinogen; MA, maximum amplitude; CI,
coagulation index. |
Findings have shown that TEG can provide a more
comprehensive assessment of coagulation status in patients with
sepsis and can more sensitively detect abnormal coagulation
(10). Coagulation disorders in
patients with sepsis are complex and variable, disseminated
intravascular coagulation (DIC) may occur and the prognosis is
poor. However, DIC is an intermediate link not an independent
disease in the complex pathological process of many diseases.
Clinical manifestations of DIC are complex and very diverse. Basic
diseases and clinical manifestations are the basis for the
diagnosis of DIC. Any single laboratory index used for DIC
diagnosis has significant limitations. It has been shown that TEG
can identify hypocoagulable states in patients with severe sepsis
and hypercoagulative states in non-DIC patients with severe sepsis
(11). In addition, the maximum
amplitude (MA) of thromboelastometry in patients with severe sepsis
in ICU stayed constant for several days, and the MA of
hypocoagulable states independently predicted 28-day mortality
(12). In patients with severe
sepsis, changes in TEG variables suggest that progressively
worsening hypocoagulation is associated with the risk of death and
bleeding (13).
At present, the Acute Physiology, Age and Chronic
Health Evaluation (APACHE II) system II is the most widely used
method for assessing the condition and prognosis of critically ill
patients. APACHE II scores can be used to assess the severity of
the disease and has a certain value for prediction of prognosis and
mortality risk (14,15). Higher APACHE II scores indicate
heavier disease, worse prognosis and higher mortality rate
(16).
Previous findings have shown that (17,18),
APACHE II score and Sequential Organ Failure Assessment (SOFA) can
be used to effectively evaluate the prognosis of critically ill
patients, and those factors are closely correlated. With the update
of the definition of sepsis (Sepsis-3), the concept of quick
Sequential Organ Failure Assessment (qSOFA) and systemic
inflammatory response syndrome (SIRS) have been proposed. However,
SOFA remains the most reliable method for the diagnosis of sepsis
(19). Furthermore, the accuracy of
predicting in-hospital mortality of SOFA is higher than that of
SIRS or qSOFA scores when adult patients with suspected infections
in ICU showed a SOFA score ≥2 (20).
For this study, clinical data of 81 patients with
sepsis were collected. The patients were grouped and TEG data were
compared to observe changes in coagulation function. The purpose of
this study was to investigate the correlation between TEG
indicators and the severity of sepsis and provide a theoretical
basis for the early detection and treatment of coagulopathy.
Patients and methods
Patients
The present study used a prospective research method
to collect clinical data of coagulation in 81 patients with sepsis
who were admitted to the Department of Intensive Care, General
Hospital of Ningxia Medical University (Yinchuan, China) from April
1, 2015 to December 31, 2015. Inclusion criteria were: i) ICU
sepsis patients admitted to General Hospital of Ningxia Medical
University from April, 2015 to December, 2015; ii) conformity to
the diagnostic criteria for sepsis and septic shock (refer to 2016
International Guidelines for Treatment of Sepsis and Septic Shock)
(21); iii) age ≥18 years. Exclusion
criteria: i) patients with incomplete records of medical records;
ii) patients with acute cardiovascular and cerebrovascular
diseases, liver cirrhosis, congenital coagulation disorder, organ
transplantation, blood system diseases, hypersplenism or chronic
renal insufficiency or patients needing kidney replacement therapy,
long-term radiotherapy and chemotherapy.
The study was approved by the Ethics Committee of
General Hospital of Ningxia Medical University. Signed informed
consent was obtained from the patients or the guardians.
Grouping method
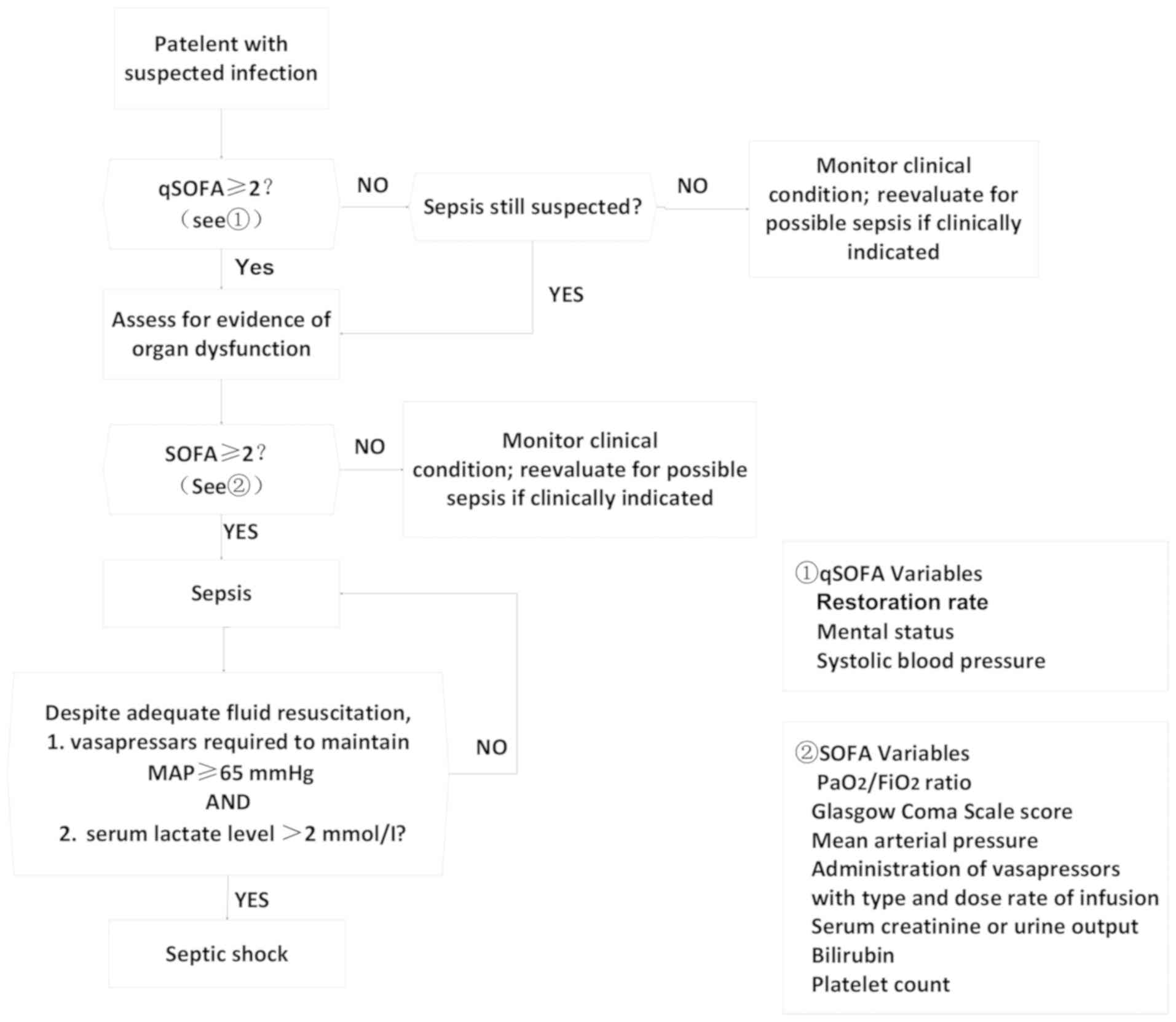
According to the 2016 International Guidelines for
Treatment of Sepsis and Septic Shock, patients were divided into
sepsis and septic shock groups (diagnostic criteria are shown in
Fig. 3). TEG indicators of the two
groups at the time of ICU entry and 6 h after ICU entry were
compared. According to the median APACHE II score within 24 h after
ICU admission, the patients were divided into two groups: group A
(APACHE II score ≤13, n=51); group B (APACHE II score >13,
n=30), TEG indicators were compared between the two groups.
According to the Disseminated Intravascular Coagulation Diagnosis
Integral System (CDSS), the patients were divided into non-DIC
group (CDSS <7 points) and DIC group (CDSS ≥7 points), and TEG
indexes were compared between the two groups. Correlations between
TEG indexes and SOFA scores of 81 patients at the time of ICU entry
were analyzed. Patients were divided into survival group and
non-survival group and correlations between TEG indicators and
prognosis were analyzed.
Survey contents (using self-made
questionnaires to collect case data for statistical analysis)
General conditions: patient's age, sex, presence of
underlying disease, number of ICU stays, total days of
hospitalization, diagnosis, and prognosis. Monitoring indicators:
coagulation function (PT, APTT, FIB, TT, FDP, DD, 3P test) and
thrombo-elastogram parameters (R, K, MA, α, CI), LY30 value and PLT
at the time of admission to the ICU and 6 h after admission.
According to the diagnostic criteria of sepsis and septic shock
group APACHE II scoring was performed within 24 h. Grouping was
performed according to median APACHE II score. DIC scores were
calculated according to CDSS and grouped according to DIC scores.
SOFA score and TEG index grouping and prognostic grouping were also
performed.
Normal reference values
Routine coagulation monitoring: APTT, 27.6–34.3 sec;
TT, 10.3–16.6 sec; PT, 9.9–12.8 sec; PTA, 70–130%; FIB, 2.0–4.6
g/l; DD, <1.5 mg/l, FDP, 0–5 µg/ml. Blood routine: PLT,
100–300×109/l; PCT, 0.114–0.282%; PLCR, 13–43%; MPV,
7.6–13.2 fl; PDW, 9.0–17.0 fl. Thromboplasty index: R value, 5–10
min; MA value, 50–70 mm; α angle, 53–72 deg; K time, 1–3 min; CI,
−3 to 3; LY30, −3-4.0%.
Statistical analysis
SPSS 17.0 statistical software (SPSS, Inc., Chicago,
IL, USA) was used to process all the data. Normal distribution data
were expressed as mean ± standard deviation. Mann-Whitney test was
used for comparison between groups. Pearson rank was used for
correlation analysis between two variables. P<0.05 was
considered to indicate a statistically significant difference.
Results
Patients
Age range of the 81 sepsis patients was 19–84 years
and the average age was 59.14±13.42 years. The patients included 52
males (64.2%) and 29 females (35.8%). There were no significant
differences in the patient's sex, age and other basic data among
sepsis group, APACHE II score group, DIC group, TEG index and SOFA
score correlation group and prognosis group (Tables I–III).
 | Table I.Sepsis groups (mean ± standard
deviation). |
Table I.
Sepsis groups (mean ± standard
deviation).
| Basic data | Sepsis group
(n=45) | Septic shock group
(n=36) |
|---|
| Age | 58.71±12.36 | 59.67±14.78 |
| Sex | 31 males | 21 males |
|
| 14 females | 15 females |
| APACHE II
score | 10.7±0.5 | 17.2±5.9 |
| Table III.DIC and non-DIC groups (mean ±
standard deviation). |
Table III.
DIC and non-DIC groups (mean ±
standard deviation).
| Basic data | Non-DIC group
(n=64) | DIC group
(n=17) |
|---|
| Age | 59.70±13.17 | 57.00±14.55 |
| Sex | 37 males | 15 females |
|
| 27 females | 2 females |
Comparison of TEG parameters between
patients with sepsis and septic shock
At the time of ICU entry, compared with sepsis
group, K time in septic shock group was significantly longer than
that of sepsis group (Fig. 4B), and
the angle α, MA value and CI decreased significantly (Fig. 4C,D,F), while LY30 increased
significantly (Fig. 4E). After 6 h,
ICU entry, compared with sepsis group, R value and K time of the
septic shock group were significantly prolonged (Fig. 4A and B), while the MA value, CI, and
α angle were significantly decreased (Fig. 4C,D,F), and LY30 was significantly
increased (Fig. 4E).
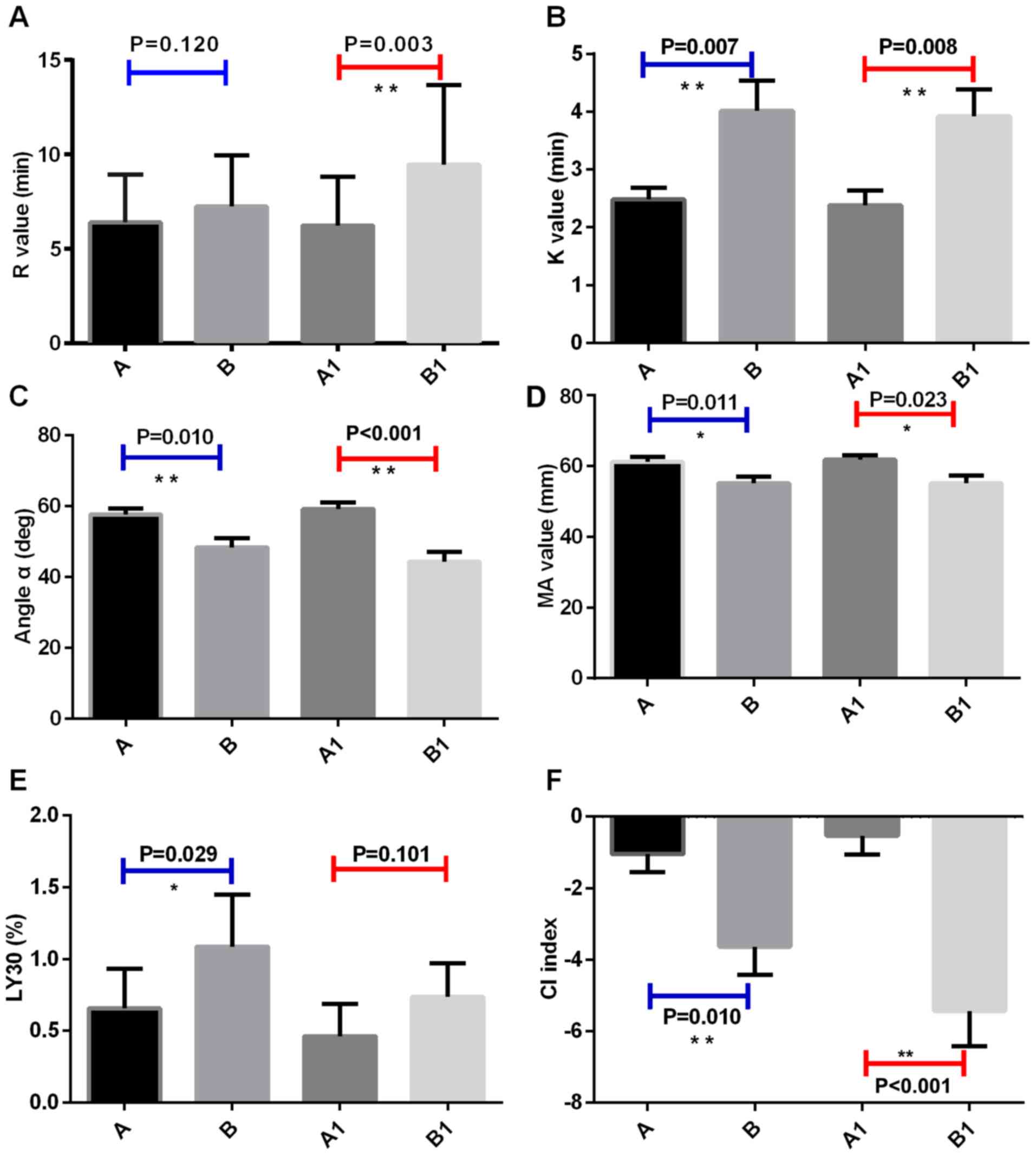 | Figure 4.Comparison of TEG detection parameters
between sepsis and septic shock groups. TEG test indicators for
patients with sepsis in ICU; TEG test indicators for the patients
with septic shock in ICU. A1, TEG indicators of sepsis patients in
ICU at 6 h after admission. B1, TEG indicators of septic shock
patients in ICU at 6 h after admission. (A) R value, (B) K time,
(C) α angle, (D) MA value, (E) LY30, and (F) CI (*P≤0.05;
**P≤0.01). TEG, thromboelastography; MA, maximum amplitude; CI,
coagulation index. |
APACHE II score grouping and TEG index
comparison
TEG test indicators at ICU entry
Compared with group A, group B had longer K value,
lower MA value, lower CI index and lower LY30 (P<0.05). TEG test
indicators at ICU entry are shown in Table IV.
| Table IV.APACHE II score grouping and TEG
index (± standard deviation) at admission (mean ± standard
deviation). |
Table IV.
APACHE II score grouping and TEG
index (± standard deviation) at admission (mean ± standard
deviation).
| TEG indexes | Group A | Group B | P-value |
|---|
| R value (min) | 6.39±2.57 | 9.54±4.90 | 0.087 |
| K value (min) | 2.60±1.48 | 3.79±2.94 | 0.013a |
| α angle (deg) | 56.18±13.36 | 44.01±16.75 | 0.055 |
| MA value (mm) | 60.59±9.69 | 54.14±13.07 | 0.022a |
| CI | −1.29±3.66 | −5.61±6.45 | 0.019a |
| LY30 (%) | 0.79±2.24 | 0.37±0.57 | 0.030a |
TEG test indicators at 6 h after ICU
entry (Table V)
Compared with group A, R value was prolonged, CI
decreased, MA value decreased, K time was prolonged and α angle
decreased in group B (P≤0.05; P≤0.01).
Comparison of DIC grouping and TEG
indicators
The comparison of DIC grouping and TEG indicators is
shown in Table VI. The results
showed that compared with non-DIC group, the median R value of TEG
was prolonged, and CI index was decreased in DIC group, indicating
that the body was in a state of hypocoagulation. MA value was
decreased, indicating that platelet function was decreased. K time
was prolonged, and α angle was decreased, suggesting that
fibrinogen function was decreased.
| Table VI.DIC grouping and TEG indicators (mean
± standard deviation). |
Table VI.
DIC grouping and TEG indicators (mean
± standard deviation).
| Coagulation
indicators | Non-DIC group
(n=65) | DIC group
(n=16) | P-value |
|---|
| MA value (mm) | 60.69±8.92 | 49.24±12.1 | 0.001b |
| K value (min) | 2.78±1.63 | 4.73±4.08 | 0.017b |
| R value (min) | 6.51±2.65 | 7.83±2.36 | 0.036a |
| α angle (deg) | 55.46±13.84 | 45.77±14.58 | 0.025a |
| CI | −1.46±3.70 | −5.17±5.08 | 0.006b |
| LY30 (%) | 0.64±1.73 | 1.70±2.78 | 0.056 |
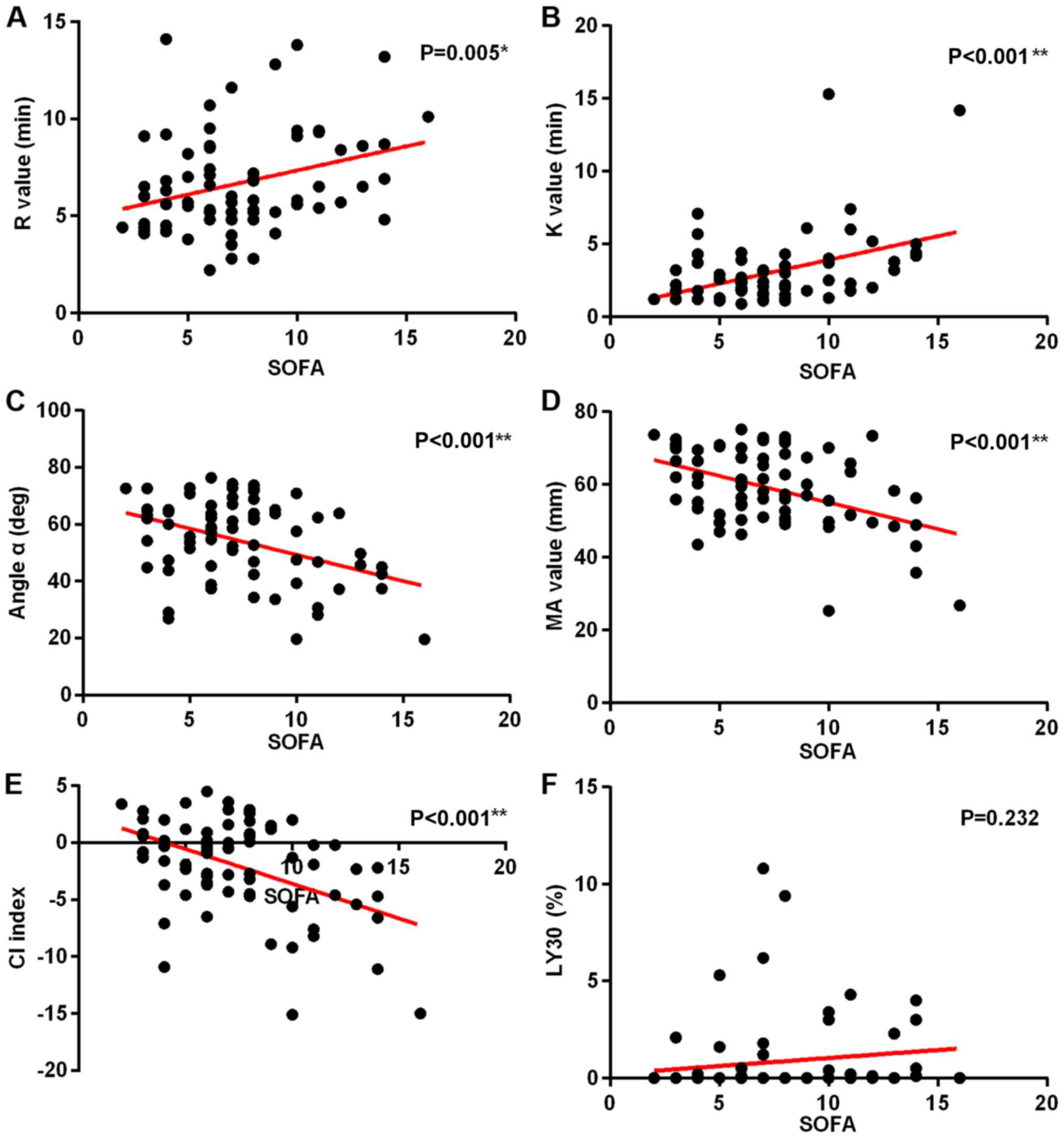
Correlation analysis between SOFA
scores and TEG indicators
With the increase of SOFA scores, R value and K time
increased significantly (Fig. 5A and
B), while α angle, MA value, and CI decreased significantly
(Fig. 5C-E). Fig. 5F shows that there is no significant
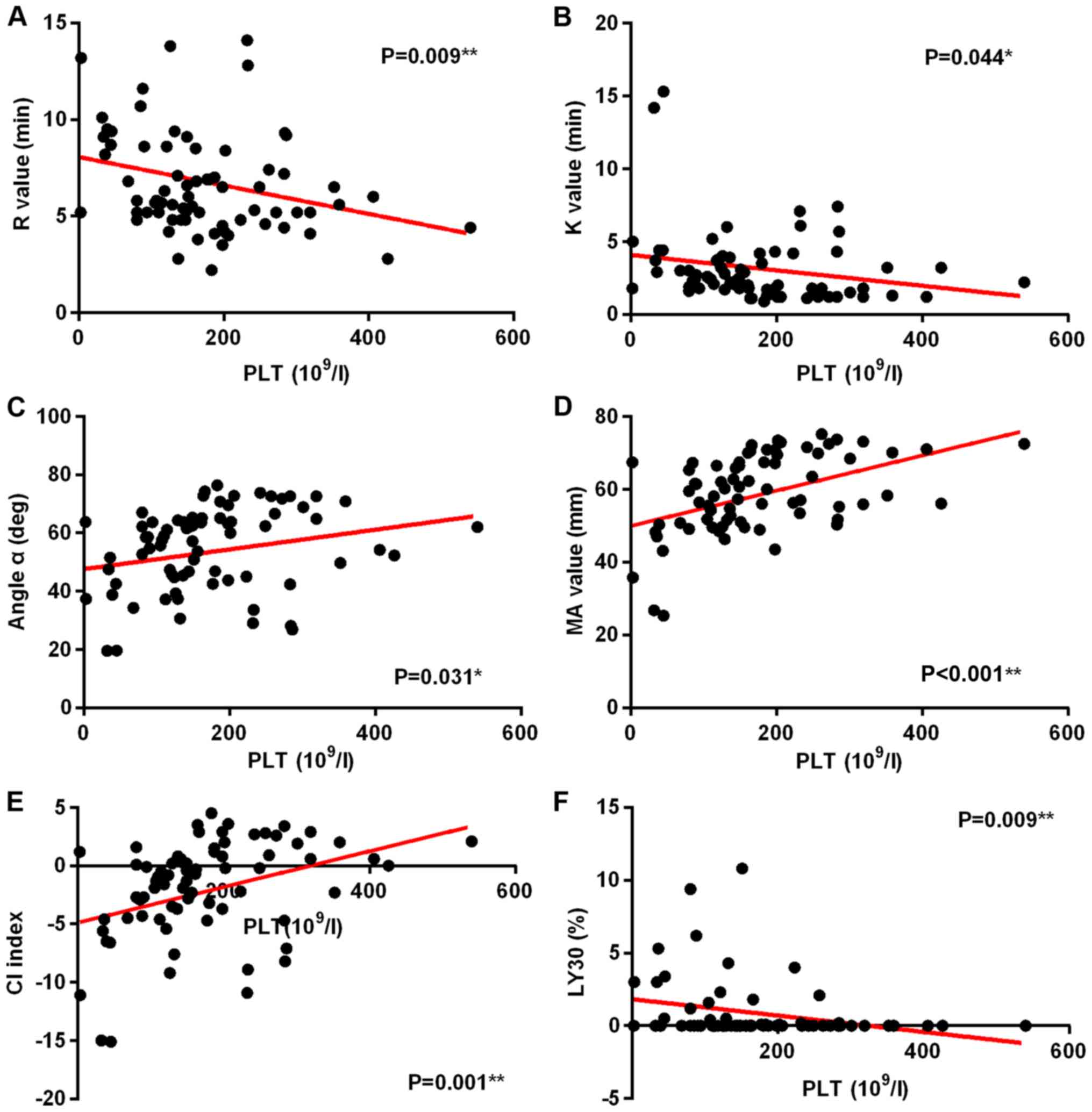
correlation between SOFA score and LY30. In this group, a
correlation study of PLTs and TEG indicators was also performed. It
was found that with the decrease of PLT, R value, K value, and LY30
decreased significantly (Fig.
6A,B,F), while α angle, and MA value and CI increased
significantly (Fig. 6C-E)
(P<0.05).
Prognostic groups and TEG
indicators
Prognostic groups and TEG indicators are shown in
Table VII. No statistical
significance was found between prognostic groups in TEG indicators
at the time of ICU entry and 6 h after ICU entry.
| Table VII.Prognosis and TEG index (mean ±
standard deviation). |
Table VII.
Prognosis and TEG index (mean ±
standard deviation).
| Coagulation
index | Survival | Death | P-value |
|---|
| MA value (mm) | 58.48±10.40 | 58.20±11.78 | 0.841 |
| K value (min) | 3.12±2.24 | 3.33±3.20 | 0.937 |
| R value (min) | 6.59±2.42 | 7.57±3.38 | 0.301 |
| α angle (deg) | 53.26±14.29 | 57.77±15.45 | 0.640 |
| CI | −2.08±4.06 | −2.69±5.13 | 0.733 |
| LY30 (%) | 0.91±2.15 | 0.57±1.22 | 0.851 |
| MA 1 (mm) | 15.63±4.03 | 58.49±13.36 | 0.715 |
| K 1 (min) | 3.10±2.41 | 2.87±2.47 | 0.480 |
| R 1 (min) | 7.46±3.80 | 8.57±3.56 | 0.118 |
| α angle (deg) | 52.84±16.54 | 51.35±16.58 | 0.711 |
| CI | −2.50±5.31 | −3.64±5.31 | 0.359 |
| LY30 1 (%) | 0.46±1.14 | 1.15±2.41 | 0.118 |
Discussion
Sepsis is the leading cause of death in critically
ill patients worldwide. Pathogenesis of this disease remains
unclear and efforts are being made on the diagnosis and treatment
of this disease. An increasing number of studies have shown that
the activation of the coagulation system and microcirculatory
dysfunction play a very important role in the occurrence and
development of sepsis. It has been shown that coagulation disorder
is persistent throughout sepsis and is an important factor for
prognosis (22). Findings of the
present study suggest that the coagulation disorders in patients
with sepsis main have the following mechanisms: i) tissue factor
induces the production of thrombin through an exogenous coagulation
pathway, thus FIB is activated and converted into fibrin, and
platelet activation aggregates (23); ii) impaired systemic physiological
anticoagulant system, such as the lack of activated protein C,
antithrombin III, and tissue factor pathway inhibitors, causes
downregulation of anticoagulation (24); iii) disturbance of the fibrinolytic
system occurs, and the concentration of plasminogen activator
inhibitor-I in plasma increases, resulting in the closure of the
fibrinolytic system (10), which
leads to decreased fibrinolysis. Activation of the coagulation
system and the subsequent downregulation contribute to the disorder
of coagulation in patients with sepsis. Inflammatory response
interacts with disturbance of coagulation to cause organ
dysfunction. Therefore, timely monitoring of coagulation changes
and early treatment of coagulopathy can block the deterioration of
sepsis. At present, the coagulation function monitoring methods
commonly used in clinical practice include traditional coagulation
function testing and TEG tests. Traditional coagulation test can
only evaluate part of the clotting system and cannot truly reflect
the blood coagulation balance in the body. TEG has obvious
advantages in reflecting the effects of plasma components and
cellular components on blood clotting at different stages of
coagulation, assessing the overall blood coagulation, and
determining coagulation factor function.
The TEG test can convert the kinetic process of
coagulation to a tracing curve, which can more intuitively reflect
the interaction of various substances in the coagulation process
(25). Changes in clotting factors,
platelets, fibrin, and fibrinolysis at various stages of
coagulation, as well as the state of the substances involved in the
coagulation process, can all be well reflected by the TEG test
(7). The main parameters of the TEG
test include coagulation reaction time (R value), CI, MA,
coagulation rate (α angle), and kinetics of clot development (K
values). TEG has been widely used clinically, especially in
cardiovascular surgery, organ transplant surgery, blood
transfusion, anticoagulation and antiplatelet therapy.
The current study shows that an increase of severity
of disease is accompanied by an increase of APACHE II score. The
extent of coagulation disorders is positively correlated with the
severity of the disease. In this study, 81 patients were divided
into different groups according to five grouping method.
Based on the 2016 International Guidelines for the
Treatment of Sepsis and Septic Shock, patients were divided into
sepsis group and septic shock group, and TEG indicator at the time
of ICU entry and 6 h after ICU entry were compared. At the time of
ICU entry, compared with sepsis group, K time in septic shock group
was significantly longer than that of sepsis group, and the angle
α, MA value and CI decreased significantly, while LY30 increased
significantly, indicating that patients in septic shock group
exhibited hypocoagulable states, platelet and FIB functions were
reduced, and fibrinolysis progressed. At 6 h after ICU entry,
compared with sepsis group, R value and K time of the septic shock
group were significantly prolonged, while the MA value, CI, and α
angle were significantly decreased, and LY30 was significantly
increased, indicating that patients in the shock group showed
hypocoagulation, and platelet function and FIB function were
significantly reduced. This set of results shows that the degree of
disorder in coagulation function of patients is positively
correlated with the severity of sepsis. When sepsis occurs,
bacteria and endotoxins stimulate vascular endothelial cells,
activate the release of various cytokines, coagulation factors, and
vasoactive substances, activate platelet aggregation, and condense
TXB2 and cytokines, leading to tissue ischemia, hypoxia, the
formation of micro-thrombosis, damage to the vascular endothelium,
inhibited anticoagulation system and fibrinolytic system,
microcirculation disorders, and ultimately the development of
septic shock (26). Results obtained
in this study are in accordance with the law of occurrence and
development of coagulation in sepsis. The specific coagulation
status reflected in TEG is prolongation of K and the decrease of α
angle suggested a decrease in FIB function, a decrease in MA value
suggested a decrease in platelet function, and a decrease in CI
suggested a tendency toward hypocoagulability. This reflects the
complete picture of coagulation, which is also an advantage of TEG.
Traditional coagulation function test does not reflect the status
of platelet and FIB function, but only reflects the quantitative
changes. Results of this group study showed that the more severe
the condition of patients with sepsis, the greater the degree of
coagulation disorders. Clinical monitoring of coagulation function,
and timely and effective treatment may block or delay the
occurrence and development of sepsis.
APACHE II score as an internationally recognized
system for evaluating the condition of critically ill patients can
be used to perform more comprehensive assessments of the severity
of the illness (27). The higher the
APACHE II score is, the more severe the patient condition is and
the higher the mortality rate will be. On the contrary, the lower
the APACHE II score is, the less severe the patient's condition is,
and the better the prognosis of such a patient is (28). Therefore, APACHE II score is
positively related to the severity and mortality of the disease
(29), so it is widely used
clinically. The second grouping method in this study was based on
the median APACHE II score. Eighty-one patients were divided into
group A (APACHE II score ≤13 points) and group B (APACHE II score
>13 points), and statistical analysis was performed on TEG
scores at the time of ICU entry and 6 h after ICU entry. At the
time of ICU entry, compared with group A, the K time was
significantly prolonged, MA value, and CI were significantly
decreased in group B. At 6 h after ICU entry, compared with sepsis
group, R value and K time were significantly increased, while MA
value, CI and α angle were significantly decreased in septic shock
group. These data suggest that as the APACHE II score increases,
the body's hypocoagulable state becomes more pronounced, and fibrin
and platelet function declines. This shows that the severity of the
disease is positively correlated with the APACHE II score, and as
the disease progresses, the extent of coagulation disorders
worsens. In this process, TEG test can reflect whether there is
consumption of coagulation factors and whether the function of
clotting factors is reduced, thereby more fully reflecting the
overall coagulation state of the patient.
Coagulation dysfunction in patients with sepsis is
complicated and changeable, and there are many influencing factors.
Patients with sepsis are prone to DIC and, in the event of DIC, the
prognosis is usually poor. However, DIC is not an independent
disease, but is an intermediate link in the pathological process of
multiple complex diseases. This dynamic change of process is rapid,
clinical symptoms are hidden, and the evaluation ability of
diagnostic indicators is limited, which brings great difficulties
to the clinical identification of DIC. Primary disease and clinical
manifestations are the basis of the diagnosis of DIC. On this
basis, laboratory indicators need to be comprehensively evaluated.
Any single laboratory index used to evaluate the process of
coagulation and diagnosis of DIC has great limitations (30–33).
Gold standard for the diagnosis of DIC is lacking. In recent years,
experts from Japan, Europe, and the United States have successively
proposed multi-indicator DIC integral diagnostic systems, those
systems mainly include Japanese Society of Emergency Medicine
system, the Japanese Ministry of Health and Welfare system, and the
International Thrombosis and Hemostasis Association system.
However, the accuracy and practicality of these three standards are
still widely controversial. The scope of current diagnostic scoring
system, inclusion criteria, and the boundary value classification
of indicators are still open to question, and accurate diagnosis of
DIC is still a difficult task.
In 2017, the Chinese Medical Association Hematology
Branch Thrombosis and Hemostasis Group established the China
Disseminated Intravascular Coagulation Diagnosis Score System
(CDSS) through a multi-center, large-scale retrospective and
prospective study, making the DIC diagnostic criteria more in line
with conditions in China. The third grouping method in this study
was to collect laboratory indicators of 81 patients when they
entered the ICU. According to the CDSS, they were divided into
non-DIC group (CDSS <7 points) and DIC group (CDSS ≥7 points).
TEG indicators were compared and results showed that compared with
the non-DIC group, R time was prolonged and CI decreased in DIC
group suggesting a hypocoagulable state. Besides, decreased MA
values suggested decreased platelet function and prolonged K time
and decreased α angle suggest FIB dysfunction. As known, the
current CIs required for the diagnosis of DIC are mainly PT, APTT,
PLT, FIB, FDP and D-dimer. These are quantitative indicators and do
not reflect the functional status of clotting factors, but TEG
detection can reflect the function of clotting factors. TEG showed
a decrease in platelet function and FIB function in DIC group, and
it indicated that the body showed a hypocoagulable state, which was
not possible with traditional coagulation parameters. However, this
does not mean that the TEG test can replace the traditional
coagulation function test. In clinical work, traditional blood
coagulation testing methods can be combined with TEG testing to
comprehensively evaluate the patient's coagulation status, thereby
assisting diagnosis and guiding treatment.
The newly proposed Sepsis-3 concept leads to the
emergence of qSOFA concept. qSOFA can help to quickly determine the
severity of the patient's condition, and it is easier to get qSOFA
score in the clinic. However, SOFA score may be more accurate in
reflecting the severity of sepsis. SOFA score can be used to assess
the evolution of functional impairment in various organ systems.
The higher the total score is, the greater the number of organ
system failures are, which indicates that more severe condition and
higher mortality rate. SOFA scoring system is mainly based on six
systems including respiratory system, nervous system, circulatory
system, liver function, coagulation system and kidney function,
among which the evaluation of coagulation system is based on PLT,
and there is no traditional CI and TEG index available for the
evaluation of coagulation system. It is well known that the
coagulation state of patients with sepsis is extremely complicated
and changeable. It is impossible to represent coagulation function
by a certain CI, but a comprehensive analysis of the condition and
test results is required to evaluate coagulation function. A number
of studies have shown that there is a correlation between TEG index
and the PLT (34–36). The same conclusion was made in this
study (Fig. 6). Therefore, it is
proposed to analyze the relationship between the TEG index and the
SOFA score to analyze the coagulation status of patients with
sepsis. The fourth grouping method of this study was to collect the
SOFA scores of 81 patients and the TEG index at the time of
admission. The correlation between SOFA scores and TEG parameters
was analyzed. Results showed that, as the score of SOFA increases,
R value increases, and CI decreases significantly, suggesting that
the body exhibits a hypocoagulable state; K value increases
significantly and angle of α decreases, suggesting a decrease in
FIB function; and the decrease in MA value indicates reduced
function of platelet. Evaluation of the coagulation system by the
SOFA score is based on the number of platelets. This study found
that number of platelets was closely correlated with TEG
indicators. Therefore, it can be concluded that TEG can reflect the
functional status of clotting factors in patients with sepsis, as
well as the overall blood coagulation, and it is in accordance with
the occurrence and development of sepsis. It also shows that TEG
can be used to determine severity of sepsis.
Eighty-one patients were divided into the survival
and death groups. Statistical analysis was performed on the TEG
indicators at the time of admission and 6 h after admission. No
correlation was found between the TEG indicators and the prognosis.
The consideration may be associated with the sample size. In
addition, the pathogenesis of sepsis is extremely complicated and
remains unclear. Coagulation dysfunction is one of the factors in
the occurrence and development of sepsis, and its own mechanism is
also very complicated and affected by many factors. Therefore, a
single index may not directly reflect the prognosis of patients
with sepsis.
In conclusion, coagulation disorders in patients
with sepsis have been confirmed, but the mechanism is still not
fully understood. Indicators in TEG testing, such as R value, K
time, α angle, MA value and CI, can help determine the severity of
the patient's condition. Although the advantage of TEG in detecting
the function of the coagulation system is more prominent, it still
cannot replace the traditional coagulation test and PLT test. It is
necessary to combine these three methods to make a comprehensive
analysis and accurately reflect the coagulation status of patients
with sepsis, thereby achieving timely and effective treatment.
Close attention should be paid on changes in the blood coagulation
system in patients with sepsis. Traditional coagulation tests,
routine blood tests, and TEG tests should be combined to
comprehensively determine coagulation status in patients with
sepsis, so as to make early, comprehensive, accurate, and objective
diagnosis.
The patient experienced obvious hypocoagulable
state, FIB function and platelet function decline according to TEG,
from the sepsis to septic shock process, and those conditions
became worse with the increase of the severity of disease.
Moreover, platelet function and FIB function of DIC patients were
significantly reduced, and the body showed hypocoagulability.
Acknowledgements
Not applicable.
Funding
This study was supported by the funding project of
Ningxia Medical University Fund for Scientific Research (no.
XM2015054, no. XM2016027), Ningxia Natural Science Foundation (no.
NZ17151) and the regional project of National Science Foundation of
China (no. 81260583).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
WenyanZ and WenjieZ collected and analyzed the
general information of patients. JB recorded coagulation function
indicators. SM analyzed thrombo-elastogram parameters. QL and XM
interpreted normal reference values. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
General Hospital of Ningxia Medical University (Yinchuan, China).
Signed informed consent was obtained from the patients or the
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Azkárate I, Sebastián R, Cabarcos E,
Choperena G, Pascal M and Salas E: A prospective, observational
severe sepsis/septic shock registry in a tertiary hospital in the
province of Guipuzcoa (Spain). Med Intensiva. 36:250–256. 2012.(In
Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Samuels JM, Moore HB and Moore EE:
Coagulopathy in severe sepsis: Interconnectivity of coagulation and
the immune system. Surg Infect (Larchmt). 19:208–215. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wang Y, Ouyang Y, Liu B, Ma X and Ding R:
Platelet activation and antiplatelet therapy in sepsis: A narrative
review. Thromb Res. 166:28–36. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang Y, Wang D, Fu J and Liu Y: Predictive
value of SOFA, qSOFA score and traditional evaluation index on
sepsis prognosis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue.
29:700–704. 2017.(In Chinese). PubMed/NCBI
|
|
5
|
Wang L, Bastarache JA and Ware LB: The
coagulation cascade in sepsis. Curr Pharm Des. 14:1860–1869. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Reikvam H, Steien E, Hauge B, Liseth K,
Hagen KG, Størkson R and Hervig T: Thrombelastography. Transfus
Apheresis Sci. 40:119–123. 2009. View Article : Google Scholar
|
|
7
|
Kozek-Langenecker S: Management of massive
operative blood loss. Minerva Anestesiol. 73:401–415.
2007.PubMed/NCBI
|
|
8
|
Salooja N and Perry DJ:
Thrombelastography. Blood Coagul Fibrinolysis. 12:327–337. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kunio NR, Differding JA, Watson KM, Stucke
RS and Schreiber MA: Thrombelastography-identified coagulopathy is
associated with increased morbidity and mortality after traumatic
brain injury. Am J Surg. 203:584–588. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ren J, Zhao Y, Yuan Y, Han G, Li W, Huang
Q, Tong Z and Li J: Complement depletion deteriorates clinical
outcomes of severe abdominal sepsis: A conspirator of infection and
coagulopathy in crime? PLoS One. 7:e470952012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sivula M, Pettilä V, Niemi TT, Varpula M
and Kuitunen AH: Thromboelastometry in patients with severe sepsis
and disseminated intravascular coagulation. Blood Coagul
Fibrinolysis. 20:419–426. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ostrowski SR, Windeløv NA, Ibsen M, Haase
N, Perner A and Johansson PI: Consecutive thrombelastography clot
strength profiles in patients with severe sepsis and their
association with 28-day mortality: A prospective study. J Crit
Care. 28:317.e1–317.e11. 2013. View Article : Google Scholar
|
|
13
|
Haase N, Ostrowski SR, Wetterslev J, Lange
T, Møller MH, Tousi H, Steensen M, Pott F, Søe-Jensen P, Nielsen J,
et al: Thromboelastography in patients with severe sepsis: A
prospective cohort study. Intensive Care Med. 41:77–85. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Braber A and van Zanten AR: Unravelling
post-ICU mortality: Predictors and causes of death. Eur J
Anaesthesiol. 27:486–490. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Namendys-Silva SA, Texcocano-Becerra J and
Herrera-Gómez A: Prognostic factors in critically ill patients with
solid tumours admitted to an oncological intensive care unit.
Anaesth Intensive Care. 38:317–324. 2010.PubMed/NCBI
|
|
16
|
Jianmin Q, Xueliang Y, Liqin L, Yongsheng
W, Licang H and Yuanxin H: Value of continuous video EEG and EEG
responses to thermesthesia stimulation in prognosis evaluation of
comatose patients after cardiopulmonary resuscitation. Open Med
(Wars). 13:35–40. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Singh RK, Poddar B, Baronia AK, Azim A,
Gurjar M, Singhal S, Srivastava S and Saigal S: Audit of patients
with severe acute pancreatitis admitted to an intensive care unit.
Indian J Gastroenterol. 31:243–252. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Qiao Q, Lu G, Li M, Shen Y and Xu D:
Prediction of outcome in critically ill elderly patients using
APACHE II and SOFA scores. J Int Med Res. 40:1114–1121. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Goulden R, Hoyle MC, Monis J, Railton D,
Riley V, Martin P, Martina R and Nsutebu E: qSOFA, SIRS and NEWS
for predicting inhospital mortality and ICU admission in emergency
admissions treated as sepsis. Emerg Med J. 35:345–349. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mato A, Fuchs BD, Heitjan DF, Mick R,
Halpern SD, Shah PD, Jacobs S, Olson EM, Schuster SJ, Ujjani C, et
al: Utility of the systemic inflammatory response syndrome (SIRS)
criteria in predicting the onset of septic shock in hospitalized
patients with hematologic malignancies. Cancer Biol Ther.
8:1095–1100. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rhodes A, Evans LE, Alhazzani W, Levy MM,
Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally
ME, et al: Surviving Sepsis Campaign: International Guidelines for
Management of Sepsis and Septic Shock: 2016. Crit Care Med.
45:486–552. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Knoebl P: Blood coagulation disorders in
septic patients. Wien Med Wochenschr. 160:129–138. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Levi M and Schultz M: The
inflammation-coagulation axis as an important intermediate pathway
in acute lung injury. Crit Care. 12:144–147. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lissalde-Lavigne G, Combescure C, Muller
L, Bengler C, Raillard A, Lefrant JY and Gris JC: Simple
coagulation tests improve survival prediction in patients with
septic shock. J Thromb Haemost. 6:645–653. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Luddington RJ:
Thrombelastography/thromboelastometry. Clin Lab Haematol. 27:81–90.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nakae H, Endo S, Inada K, Takakuwa T,
Kasai T and Yoshida M: Relationship between thromboxane B2 and
6-keto-prostaglandin F1 alpha in sepsis. Res Commun Chem Pathol
Pharmacol. 83:297–302. 1994.PubMed/NCBI
|
|
27
|
Alarcón G, Fardella P, Conte G, Vargas V,
Parada X and Cuneo M: Changes in coagulation in patients with
sepsis. Rev Med Chil. 121:537–541. 1993.(In Spanish). PubMed/NCBI
|
|
28
|
Wang H, Li Z, Yin M, Chen XM, Ding SF, Li
C, Zhai Q, Li Y, Liu H and Wu DW: Combination of Acute Physiology
and Chronic Health Evaluation II score, early lactate area, and
N-terminal prohormone of brain natriuretic peptide levels as a
predictor of mortality in geriatric patients with septic shock. J
Crit Care. 30:304–309. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chen FG and Koh KF: Septic shock in a
surgical intensive care - validation of multiorgan and APACHE II
scores in predicting outcome. Ann Acad Med Singapore. 23:447–451.
1994.PubMed/NCBI
|
|
30
|
Levi M and Scully M: How I treat
disseminated intravascular coagulation. Blood. 131:845–854. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Di Nisio M, Baudo F, Cosmi B, D'Angelo A,
De Gasperi A, Malato A, Schiavoni M and Squizzato A; Italian
Society for Thrombosis and Haemostasis, : Diagnosis and treatment
of disseminated intravascular coagulation: Guidelines of the
Italian Society for Haemostasis and Thrombosis (SISET). Thromb Res.
129:e177–e184. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Louw SJ, Mayne ALH and Mayne ES:
Evaluation of the diagnostic utility of individual parameters in
the disseminated intravascular coagulation (DIC) panel for use in
under resourced settings. Int J Lab Hematol. 40:e46–e48. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Masuda T, Shoko T and Deguchi Y: Clinical
investigation of coagulation markers for early detection of
sepsis-induced disseminated intravascular coagulation: A
single-center, prospective observational study. Clin Appl Thromb
Hemost. 24:1082–1087. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Dorman BH, Spinale FG, Bailey MK, Kratz JM
and Roy RC: Identification of patients at risk for excessive blood
loss during coronary artery bypass surgery: Thromboelastography
versus coagulation screen. Anesth Analg. 76:694–700. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Rocha LL, Pessoa CM, Neto AS, do Prado RR,
Silva E, de Almeida MD and Correa TD; POCKET Trial Investigators, :
Thromboelastometry versus standard coagulation tests versus
restrictive protocol to guide blood transfusion prior to central
venous catheterization in cirrhosis: Study protocol for a
randomized controlled trial. Trials. 18:852017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Bowbrick VA, Mikhailidis DP and Stansby G:
Influence of platelet count and activity on thromboelastography
parameters. Platelets. 14:219–224. 2003. View Article : Google Scholar : PubMed/NCBI
|