Introduction
Neonatal jaundice is a common disease in
neonatology. Due to the immature liver function in neonates leading
to abnormal bilirubin metabolism and causing an abnormal increase
in bilirubin levels of blood, also called neonatal
hyperbilirubinemia. According to etiology, it can be divided into
physiological jaundice and pathological jaundice (1,2).
Neonatal jaundice occurs mostly in premature infants, and the main
clinical manifestations are yellow stains on the sclera, skin and
mucosa membranes of infants. However, the symptoms are painless, so
it is unnoticeable for parents (3–5).
Currently, the incidence of neonatal pathological jaundice is still
high, and the incidence rates of jaundice in ABO hemolytic neonates
is extremely high (6). Neonatal ABO
is a neonatal homologous immune hemolytic disease, due to the
incompatibility of maternal and infant ABO blood type, an extremely
fast hemolysis rate during the process of hemolysis in children
will lead to a direct rise in blood bilirubin levels, and will
gradually develop into pathological ABO hemolytic jaundice
(7,8). ABO hemolytic jaundice has an extremely
severe effect, which can cause neonatal bilirubin encephalopathy if
treatment is not given in an appropriate time, and further causes
damage to the neonatal nervous system, intelligence and/or hearing
loss. In severe cases, it can threaten the life of a newborn
(3,9). Therefore, early and active treatment is
very important for neonatal ABO hemolytic jaundice, and it is also
a topic that is currently highly valued in medical studies.
Currently, phototherapy treatment is a widely used
method for treating neonatal jaundice. It is easy to use, has a low
cost and good effect, so it is accepted by most of the medical
staff (10). It's easier for serum
bilirubin molecules to absorb blue light than green and ultraviolet
light. Therefore, blue light irradiation has become the preferred
treatment. Also it rapidly reduces the serum bilirubin content in
children by converting indirect bilirubin into a non-toxic
water-soluble derivative light-bilirubin isomer (11,12).
Continuous irradiation is mostly used clinically, however, there
are documents showing that a long irradiation time can cause many
adverse reactions (13). According
to the research by Maisels (14),
reducing the duration of phototherapy can decrease the adverse
reactions caused by phototherapy and helps the nurse care and
treatment of children. Therefore, this study retrospectively
analyzed neonatal ABO hemolytic jaundice in Qilu Hospital of
Shandong University (Qingdao, China) for continuous and
intermittent blue light irradiation. Serum bilirubin levels were
measured before and after treatment in children, and all the
indicators between the groups were recorded and compared. This
study provides a reference for the clinical treatment of neonatal
ABO hemolytic jaundice.
Patients and methods
Patient information
Retrospective analysis of 307 patients with neonatal
ABO hemolytic jaundice admitted to Qilu Hospital of Shandong
University (Qingdao) from January 2010 to December 2017 was
performed. A total of 165 children treated with continuous blue
light irradiation were the continuous phototherapy group, including
89 males, and 76 females, average age 5.87±0.65 days, average
weight 3.92±0.27 kg and mean disease duration 5.22±0.86 days. A
total of 142 children treated with intermittent blue light
irradiation were the intermittent phototherapy group, with 74
males, and 68 females, average age 5.79±0.84 days, average weight
3.88±0.38 kg and mean disease duration 5.17±0.62 days.
Inclusion criteria: i) Children diagnosed with
neonatal ABO hemolytic jaundice; ii) age <1 week, disease
duration 1–7 days; iii) total serum bilirubin levels of children
>220.60 µmol/l; iv) with complete cases; and v) never received
treatments from other hospitals. Exclusion criteria: i) Children
with contraindications for treatment with blue light irradiation;
ii) parents who refused to treat children with blue light
radiation; and iii) children with serious infections and
diseases.
This study was approved by the Ethics Committee of
Qilu Hospital of Shandong University (Qingdao). Patients who
participated in this research had complete clinical data. Signed
informed consents were obtained from the parents of the child
patients.
Methods
Children in the continuous and the intermittent
phototherapy group received prompt correction of the acid-base
imbalance, anti-infection treatment, nutritional support, and heat
preservation. Both groups of children were treated with blue
double-sided light irradiation (YLG-1 type; Shanghai Medical
Thermostat Equipment Factory, Shanghai, China) on the basis of
conventional treatment. The perineum of children was protected by
black cotton diapers, and the eyes were protected by a black eye
mask, and children were appropriately constrained. The temperature
was set to 30–32°C and the humidity was set to 55–65%. In order to
ensure that the skin of children receives light evenly, the light
distance was adjusted to 25 cm, and the blue light wavelength was
set as 425–475 nm and the power to 160 W. Children in the
phototherapy group were treated with continuous 12–18 h of blue
light irradiation with a stop of 8–12 h in between. Children in the
intermittent phototherapy group were treated with intermittent blue
light: 3–5 h of blue light of irradiation and a stop of 2–4 h in
between. The course of treatment for each group was 72 h. During
the treatment, yellow staining on the skin and sclera as well as
all the vital signs were closely monitored. The bilirubin level of
children was measured by bilirubin measuring instrument (Beckman
automatic biochemical analyzer) before and after 24, 48 and 72 h of
treatment. The bilirubin levels, time of phototherapy, phototherapy
frequency, treatment efficiency and adverse reaction rates were
recorded and compared between the groups.
Total efficiency evaluation criteria in clinic.
Efficacy judgment criteria: i) Fully healed: The yellow stains on
the skin, sclera and entire body of children completely
disappeared; ii) the serum bilirubin level of children was at a
normal content of 3–25 µmol/l; iii) effective: after the treatment,
the yellow stains on the skin, sclera and entire body of children
has partially gone and the serum bilirubin level of children has
decreased significantly, however, it still did not return to the
normal value; and iv) ineffective: after the treatment, the yellow
stains on the skin, sclera and entire body of the children did not
disappear at all and the serum bilirubin level of children did not
decrease. Clinical total effective rate = (effective number of
cases + number of effective cases) / total number of cases
×100%.
Statistical analysis
Statistical analysis was carried out using the
software system of SPSS 17.1 (SPSS, Inc., Chicago, IL, USA). The
data counting was expressed as a percentage [n (%)]. The difference
between the groups was compared by Chi-square test. Measurement of
data were expressed as mean ± standard deviation, the difference
between the groups was compared by t-test. Comparison of multiple
time points used repeated measures of analysis of variance with
Least Significant Difference test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Comparison of patients' clinical
data
In order to make the experimental results accurate
and credible, sex, age, weight, duration of disease and delivery
period between groups were compared. The difference was not
statistically significant (P>0.05). It shows that there is
comparability between the groups of patients (Table I).
 | Table I.Basic information of patients between
the continuous and the intermittent phototherapy groups [n
(%)]. |
Table I.
Basic information of patients between
the continuous and the intermittent phototherapy groups [n
(%)].
| Variables | Continuous
phototherapy group (n=165) | Intermittent
phototherapy group (n=142) | t/Chi-square
test | P-value |
|---|
| Sex |
|
| 0.102 | 0.749 |
| Male | 89
(53.94) | 74
(52.11) |
|
|
|
Female | 76
(46.06) | 68
(47.89) |
|
|
| Age (days) | 5.87±0.65 | 5.79±0.84 | 0.940 | 0.348 |
| Weight (kg) | 3.92±0.27 | 3.88±0.38 | 1.074 | 0.284 |
| Disease duration
(days) | 5.22±0.86 | 5.17±0.62 | 0.576 | 0.565 |
| With or without
deformity |
|
| 0.204 | 0.652 |
| With
deformity | 2
(1.12) | 1
(0.70) |
|
|
| Without
deformity | 163 (98.79) | 141 (99.30) |
|
|
| Maternity period |
|
| 1.202 | 0.548 |
|
Premature | 115 (69.70) | 91
(64.08) |
|
|
|
Full-term | 43
(26.06) | 45
(31.69) |
|
|
|
Exceeded | 7
(4.24) | 6
(4.23) |
|
|
Comparison of phototherapy time and
frequency in children between continuous and intermittent
phototherapy groups
Phototherapy time of children in continuous
phototherapy group was significantly higher than the intermittent
phototherapy group, and the difference was statistically
significant (t=26.800, P<0.001). There was no significant
difference in the number of phototherapy between phototherapy and
intermittent phototherapy groups (P>0.050; Table II).
| Table II.Comparison of phototherapy time and
frequency in children between the phototherapy and the intermittent
phototherapy groups (mean ± standard deviation). |
Table II.
Comparison of phototherapy time and
frequency in children between the phototherapy and the intermittent
phototherapy groups (mean ± standard deviation).
| Items | Continuous
phototherapy group (n=165) | Intermittent
phototherapy group (n=142) | t | P-value |
|---|
| Time of phototherapy
(h) | 29.54±3.28 | 20.18±2.76 | 26.800 | <0.001 |
| Number of
phototherapy (times) |
2.61±0.18 |
2.65±0.24 |
1.665 |
0.097 |
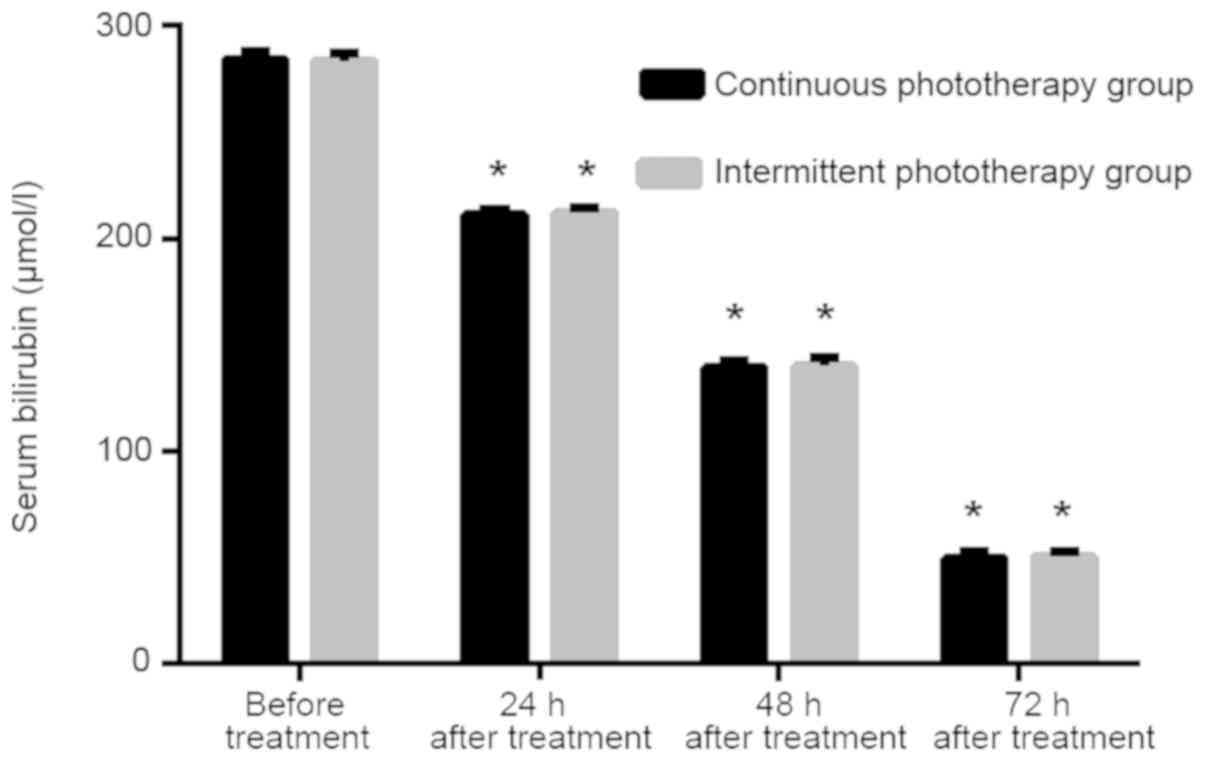
Comparison of serum bilirubin levels
in children between continuous and intermittent phototherapy groups
before and after 24, 48 and 72 h of treatment
Before treatment, there was no significant
difference in serum bilirubin levels between continuous and
intermittent phototherapy groups (P>0.050). There was no
significant difference in serum bilirubin levels between continuous
and intermittent phototherapy groups at 24, 48 and 72 h after
treatment (P>0.050). The serum bilirubin levels of patients in
the continuous and the intermittent phototherapy groups were lower
than both previous period and before treatment (P<0.001;
Table III and Fig. 1).
| Table III.Comparison of serum bilirubin (µmol/l)
levels in children between the continuous and the intermittent
phototherapy groups before and after 24, 48 and 72 h of
treatment. |
Table III.
Comparison of serum bilirubin (µmol/l)
levels in children between the continuous and the intermittent
phototherapy groups before and after 24, 48 and 72 h of
treatment.
| Items | Continuous
phototherapy group (n=165) | The intermittent
phototherapy group (n=142) | t | P-value |
|---|
| Before treatment | 284.25±3.68 | 283.67±3.59 | 1.392 | 0.165 |
| 24 h after
treatment |
211.54±2.50a |
212.02±2.34a | 1.728 | 0.085 |
| 48 h after
treatment |
139.49±3.28a |
140.23±3.75a | 1.844 | 0.066 |
| 72 h after
treatment |
49.98±2.64a |
50.54±2.66a | 1.847 | 0.066 |
| F | 176534.000 | 142991.000 |
|
|
| P-value | <0.001 | <0.001 |
|
|
Comparison of overall efficiency in
children between continuous and intermittent phototherapy groups
after treatment
The number of partially-effective,
significantly-effective and ineffective in continuous phototherapy
group was 41, 107 and 17, respectively. The number of
partially-effective, significantly-effective and ineffective in the
intermittent phototherapy group was 38, 88 and 16, respectively.
The overall effective rate was 89.70% in the continuous
phototherapy group and 88.73% in the intermittent phototherapy
group. There was no significant difference between the groups
(P>0.050; Table IV).
| Table IV.Comparison of overall efficiency in
children between the continuous and the intermittent phototherapy
groups after treatment. |
Table IV.
Comparison of overall efficiency in
children between the continuous and the intermittent phototherapy
groups after treatment.
| Items |
Partially-effective |
Significantly-effective | Ineffective | Overall
efficiency |
|---|
| Continuous
phototherapy group (n=165) | 41 | 107 | 17 | 148 (89.70) |
| Intermittent
phototherapy group (n=142) | 38 | 88 | 16 | 126 (88.73) |
| Chi-square
test | – | – | – | 0.074 |
| P-value | – | – | – | 0.786 |
Comparison of adverse reaction rates
in children between continuous and intermittent phototherapy groups
after treatment
The adverse reaction rates of patients in continuous
phototherapy group was 41.21%, which was significantly higher than
intermittent phototherapy group (24.65%). The difference was
statistically significant (P<0.050). Adverse reactions of
children ceased after the symptomatic treatment (Table V).
| Table V.Comparison of adverse reactions of
children between the continuous and the intermittent phototherapy
groups after treatment [n (%)]. |
Table V.
Comparison of adverse reactions of
children between the continuous and the intermittent phototherapy
groups after treatment [n (%)].
| Groups | Continuous
phototherapy group (n=165) | Intermittent
phototherapy group (n=142) | Chi-square
test | P-value |
|---|
| Fever | 27
(16.36) | 11 (7.75) | – | – |
| Skin rash | 22
(13.33) | 13 (9.15) | – | – |
| Diarrhea | 12 (7.27) | 7
(4.93) | – | – |
| Others | 7
(4.24) | 4
(2.82) | – | – |
| Adverse reaction
rates | 68
(41.21) | 35
(24.65) | 9.393 | 0.002 |
Discussion
Approximately 60% of full-term infants and 80% of
premature infants develop jaundice due to hyperbilirubinemia during
neonatal period. Also 5–10% of them require treatment by
phototherapy (15), and 60% of
newborns have clinical jaundice symptoms in the first week after
birth. Also ABO-incompatibility is the most common cause of
hemolytic disease in newborns, occuring commonly in maternal type O
blood and type A or B blood in newborns as well as in the ABO
hemolytic jaundice (16,17). ABO hemolytic jaundice is a serious
pathological jaundice, which can cause neonatal growth and
development disorders and irreversible effects on the nervous
system if patients receive inappropriate or not well-timed
treatment (18). Some documents have
shown that phototherapy irradiation can make bilirubin from the
serum of children absorb certain wavelength of light, resulting in
the transformation of its structure and properties. Excreting from
the body through the biliary tract or urethra and reducing the
serum bilirubin levels in children. However, there are also
documents showing that the phototherapy exposure can cause related
complications (19,20).
Our study reviewed 307 patients with neonatal
hemolytic jaundice admitted to Qilu Hospital of Shandong University
(Qingdao) from January 2010 to December 2017. A total 165 patients
with continuous blue light irradiation and 142 patients with
intermittent blue light irradiation were analyzed. Also the serum
bilirubin levels, phototherapy time and frequency, treatment
efficiency and adverse reactions were compared between the groups.
The phototherapy time of children in the continuous phototherapy
group was significantly higher than the intermittent phototherapy
group, and the difference was statistically significant. Based on
the comparison of phototherapy time, we compared the serum
bilirubin levels and the efficacy of patients between the
continuous and the intermittent phototherapy groups before and
after treatment. Our results showed that there was no statistically
significant difference in serum bilirubin levels between the
continuous and the intermittent phototherapy groups at 24, 48 and
72 h before and after treatment. The serum bilirubin levels of
patients between the continuous and the intermittent phototherapy
groups were lower than the previous period and before treatment,
and the differences were statistically significant. The overall
effective rate in the continuous phototherapy group was 89.70%, and
the overall effective rate in the intermittent phototherapy group
was 88.73%. The difference between the groups was not statistically
significant. According to Sachdeva et al (21) in the neonatal intensive care unit of
jaundice neonatal irradiation treatment study, it was found that
the clinical efficacy between intermittent single-light irradiation
in the treatment of neonatal hyperbilirubinemia and continuous
single-light irradiation were consistent. However, Lamola et
al (22) found that there was no
significant difference in serum bilirubin levels between the
intermittent and continuous phototherapy at 12, 24, 36 and 48 h
after treatment (P>0.05), which further proved our research
results. Moreover, in the case of small difference in efficacy,
intermittent phototherapy can save medical costs and reduce the
anxiety of family members (22). In
the later stage, we found that the adverse reaction rates in the
continuous phototherapy group was 41.21% after treatment, which was
significantly higher than the intermittent phototherapy group
(24.65%). The difference was statistically significant.
Furthermore, there are documents showing that the continuous
phototherapy exposure can cause skin rash in children (23). According to Hansen (24), phototherapy may be harmful and the
time of phototherapy is the factor for determination. Therefore, we
can speculate that long exposure time of phototherapy can lead to
increased adverse reactions in children. Currently, there is no
relevant data on the adverse reaction rates in the continuous or
intermittent blue light irradiation. However, there is increasing
evidence showing that long-term exposure of phototherapy for the
treatment of jaundice can be harmful to children, and should be
used as minimally as possible with the same efficacy (25,26).
In this experiment, due to the small number of ABO
hemolytic jaundice patients in Qilu Hospital of Shandong University
(Qingdao), the selected subjects are limited and there may have
certain contingency within our results. Also due to the large bases
of our neonatal research variables, a longer follow-up
investigation on these subjects will be conducted.
In summary, the treatment effect of the intermittent
blue light irradiation on neonatal ABO hemolytic jaundice is
consistent with the continuous blue light irradiation treatment.
Also the intermittent blue irradiation has a low adverse reaction
rate, so it is worthy of promotion in clinical practice.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
SZ wrote the manuscript. SZ and YZ and MZ conceived
and designed the study and worked on total efficiency evaluation.
XW and AM collected the patient data. MZ and YL analyzed and
interpreted the patient data regarding the neonatal hemolytic. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by The Ethics Committee of
Qilu Hospital of Shandong University (Qingdao, China). Patients who
participated in this research had complete clinical data. Signed
informed consents were obtained from the parents of the child
patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chang PF, Lin YC, Liu K, Yeh SJ and Ni YH:
Identifying term breast-fed infants at risk of significant
hyperbilirubinemia. Pediatr Res. 74:408–412. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Moncrieff G: Bilirubin in the newborn:
Physiology and pathophysiology. Br J Midwifery. 26:362–370. 2018.
View Article : Google Scholar
|
|
3
|
Christensen RD, Nussenzveig RH, Yaish HM,
Henry E, Eggert LD and Agarwal AM: Causes of hemolysis in neonates
with extreme hyperbilirubinemia. J Perinatol. 34:616–619. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bjerre JV, Petersen JR and Ebbesen F:
Surveillance of extreme hyperbilirubinaemia in Denmark. A method to
identify the newborn infants. Acta Paediatr. 97:1030–1034. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Olusanya BO, Teeple S and Kassebaum NJ:
The contribution of neonatal jaundice to global child mortality:
findings from the GBD 2016 study. Pediatrics. 141:e201714712018.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lee BK, Le Ray I, Sun JY, Wikman A, Reilly
M and Johansson S: Haemolytic and nonhaemolytic neonatal jaundice
have different risk factor profiles. Acta Paediatr. 105:1444–1450.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Christensen RD and Yaish HM: Hemolytic
disorders causing severe neonatal hyperbilirubinemia. Clin
Perinatol. 42:515–527. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Agarwal V, Singh V, Goel SP and Gupta B:
Maternal and neonatal factors affecting physiological jaundice in
western U.P. Indian J Physiol Pharmacol. 51:203–206.
2007.PubMed/NCBI
|
|
9
|
Wei CC, Chang CH, Lin CL, Chang SN, Li TC
and Kao CH: Neonatal jaundice and increased risk of
attention-deficit hyperactivity disorder: A population-based cohort
study. J Child Psychol Psychiatry. 56:460–467. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Maisels MJ and McDonagh AF: Phototherapy
for neonatal jaundice. N Engl J Med. 358:920–928. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Itoh S, Okada H, Kuboi T and Kusaka T:
Phototherapy for neonatal hyperbilirubinemia. Pediatr Int (Roma).
59:959–966. 2017. View Article : Google Scholar
|
|
12
|
Ebbesen F, Madsen PH, Vandborg PK,
Jakobsen LH, Trydal T and Vreman HJ: Bilirubin isomer distribution
in jaundiced neonates during phototherapy with LED light centered
at 497 nm (turquoise) vs. 459 nm (blue). Pediatr Res. 80:511–515.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mreihil K, Benth JS, Stensvold HJ, Nakstad
B and Hansen TWR; Norwegian NICU Phototherapy Study Group;
Norwegian neonatal network, : Phototherapy is commonly used for
neonatal jaundice but greater control is needed to avoid toxicity
in the most vulnerable infants. Acta Paediatr. 107:611–619. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Maisels MJ: Phototherapy in the neonatal
intensive care unit-quantity and quality. Acta Paediatr.
107:551–553. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bhutani VK and Wong R: Bilirubin-induced
neurologic dysfunction (BIND). Semin Fetal Neonatal Med. 20:12015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zecca E, Barone G, De Luca D, Marra R,
Tiberi E and Romagnoli C: Skin bilirubin measurement during
phototherapy in preterm and term newborn infants. Early Hum Dev.
85:537–540. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kaplan M, Hammerman C, Renbaum P, Klein G
and Levy-Lahad E: Gilbert's syndrome and hyperbilirubinaemia in
ABO-incompatible neonates. Lancet. 356:652–653. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jiao Y, Jin Y, Meng H and Wen M: An
analysis on treatment effect of blue light phototherapy combined
with Bifico in treating neonatal hemolytic jaundice. Exp Ther Med.
16:1360–1364. 2018.PubMed/NCBI
|
|
19
|
Mreihil K, Madsen P, Nakstad B, Benth JS,
Ebbesen F and Hansen TW: Early formation of bilirubin isomers
during phototherapy for neonatal jaundice: effects of single vs.
double fluorescent lamps vs. photodiodes. Pediatr Res. 78:56–62.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Oláh J, Tóth-Molnár E, Kemény L and Csoma
Z: Long-term hazards of neonatal blue-light phototherapy. Br J
Dermatol. 169:243–249. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sachdeva M, Murki S, Oleti TP and Kandraju
H: Intermittent versus continuous phototherapy for the treatment of
neonatal non-hemolytic moderate hyperbilirubinemia in infants more
than 34 weeks of gestational age: a randomized controlled trial.
Eur J Pediatr. 174:177–181. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lamola AA, Bhutani VK, Wong RJ, Stevenson
DK and McDonagh AF: The effect of hematocrit on the efficacy of
phototherapy for neonatal jaundice. Pediatr Res. 74:54–60. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Maisels MJ, Ramaswamy D and Kring EA: Does
phototherapy cause benign skin rashes in newborn infants? Acta
Paediatr. 103:e133–e135. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hansen TW: Let there be light - but should
there be less? J Perinatol. 32:649–651. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Mills JF and Tudehope D: Fibreoptic
phototherapy for neonatal jaundice. Cochrane Database Syst Rev.
1:CD0020602001.
|
|
26
|
Stokowski LA: Fundamentals of phototherapy
for neonatal jaundice. Adv Neonatal Care. 11 (Suppl 5):S10–S21.
2011. View Article : Google Scholar : PubMed/NCBI
|