Introduction
Posterior pilon fracture is a specific type of
fracture that manifests in a similar manner to either an ankle
fracture or a pilon fracture. Posterior pilon fractures are caused
by rotational or axial forces and lead to posterior distal tibial
fractures with displacement toward the proximal direction.
Posterior pilon fractures are also frequently accompanied by talus
dislocation (1,2). Notably, posterior articular fractures
of the distal tibia may be divided into posterior malleolus
fractures and posterior pilon fractures. Avulsion fractures caused
by torsion trauma are types of posterior malleolus fractures, which
are characterized by small fracture blocks and do not involve the
joint surface or a small part of the joint surface. If the injury
is associated with vertical trauma, it is a pilon fracture, and the
fracture fragment is generally large, involving the articular
surface and is displaced proximally (3). In clinical practice, posterior pilon
fractures are not uncommon. Post-operative articular function is
poor due to difficult reduction processes and complex ankle
ligament injury; post-operative traumatic arthritis, even failure
of internal fixation and fracture re-displacement, may occur
(3,4).
Regardless of the type of articular fracture,
anatomic reduction, reliable fixation and early functional exercise
are considered the basis of surgical treatment. Posterior tibial
fracture fragments, incarcerated tissue and die-punch fragments are
common (5). The reduction procedure
requires clear visualization of the surgical field and minimal
operative trauma. Therefore, it is required to select the
appropriate incision and approach. In addition, exposing the
fragments posterior to the tibia and the incarcerated tissue
between the bone fragments are key to a successful surgery
(5). In terms of selecting a
fixation technique, cannulated compression screws (from anterior to
posterior, and vice versa) and posterior tibia plates are commonly
used for fixation (1,2,5).
Compared with compression screws, fixation with a posterior tibia
plate is more secure and stable, and helps in the early functional
rehabilitation of the ankle (2,6). The aim
of the present study was to retrospectively review the procedure
and determine prognostic factors in patients with posterior pilon
fracture diagnosed at our hospital to provide recommendations for
its clinical treatment.
Patients and methods
Patient cohort
A total of 23 patients with posterior pilon
fractures were recruited at the First Affiliated Hospital of
Soochow University (Suzhou, China) between March 2013 and October
2017. The cohort comprised 9 males and 14 females with a mean age
of 46.7 years (range, 19–72 years). The causes of injury included
traffic accidents (n=11), falls when walking (n=6) and falls from a
high place (n=6). A total of 4 cases were accompanied by rib
fractures and lung contusion, 2 with open injuries, 2 with pelvic
fractures and 1 with traumatic subarachnoid hemorrhage.
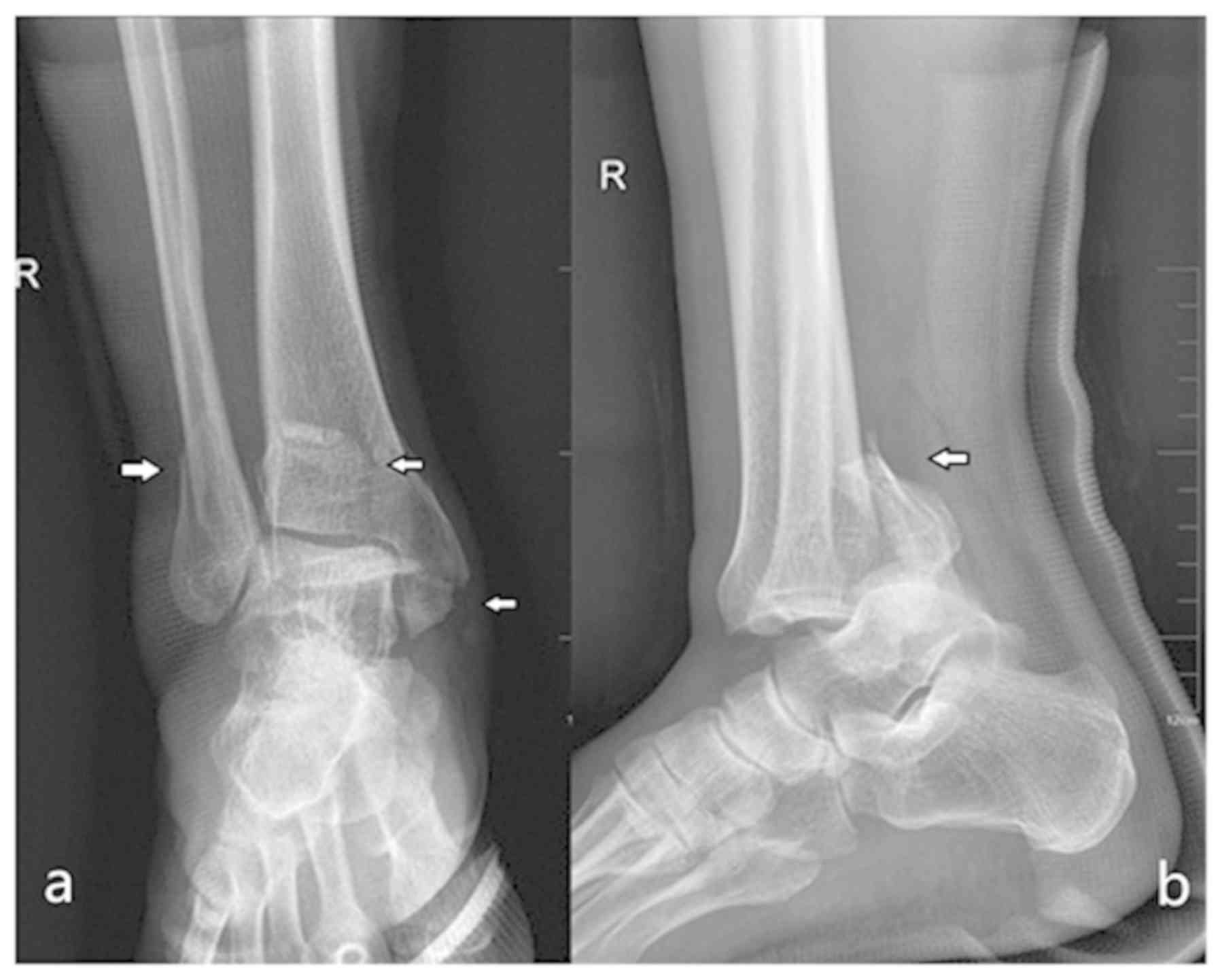
Pre-operative computed tomography (CT) plain scanning, coronal and
sagittal image reconstruction and articular surface image
reconstruction were performed in all patients. Klammer et al
classification system (1) was used
to divide posterior pilon fractures according to the shape of the
fracture line on the axial image into type I (5 patients), type II
(10 patients) and type III (8 patients) fractures. According to the
AO classification (7) of ankle
fractures, the patients in this group included 5 cases of the B3
type, 4 cases of the C1 type, 6 cases of the C2 type and 7 cases of
the C3 type. Following admission, the patients were evaluated based
on the swelling of the ankle. Of these patients, 4 underwent
emergency surgery within 8 h post-injury, 13 underwent cast
immobilization of the ankle in a neutral position, and 6 underwent
calcaneal traction and then received surgical treatment when the
ankle swelling subsided and ankle skin striae appeared. In the
patients who underwent non-emergency surgery, the average
pre-operative duration was 8.5 days (range, 5–24 days).
Surgical technique
General anesthesia via inhalation and intravenous
routes was used for surgery. The patients were placed in either the
prone or the prone float position with elevation of the affected
lower extremity with a slightly bent knee. This position allowed
for the extreme extension of the ankle during the reduction
procedure. A longitudinal incision was made between the lateral
margin of the Achilles tendon and the posterior margin of the
fibula. The distal incision was curved forward and the incision was
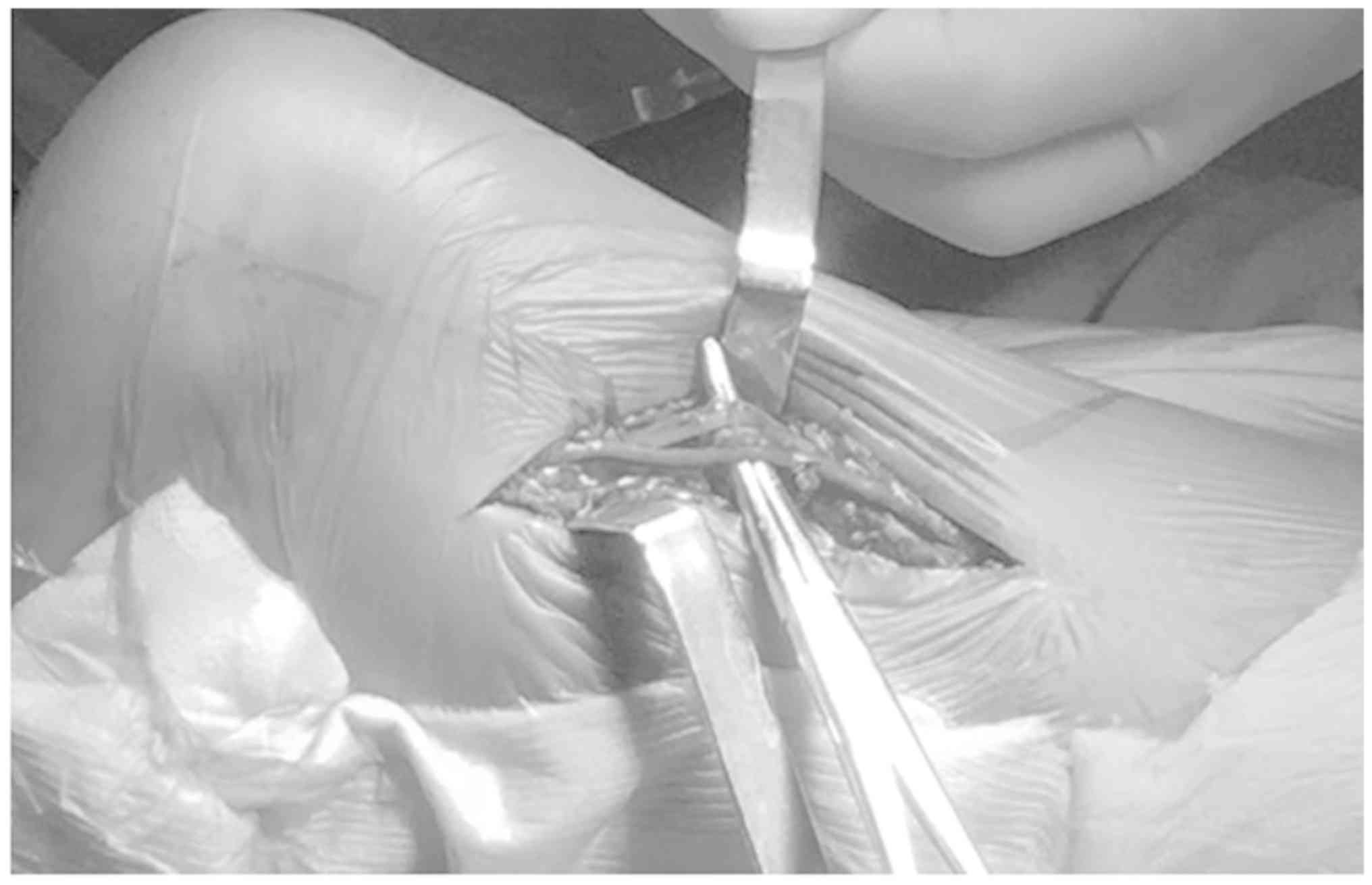
free for extension in either direction as required (Fig. 1). The sural nerve and the small
saphenous vein were identified, exposed and protected by skin flap
traction (Fig. 2). The posterior and
lateral fibula was visualized via the anterior space of the
peroneus longus and brevis muscles. At the site posterior to the
peroneus longus and brevis muscles, the muscle belly of the flexor
hallucis longus muscle was separated by blunt dissection between
the interosseous membrane and the lateral tibia. Care was taken to
protect the peroneal artery when operating through this access. The
flexor hallucis longus muscle was retracted medially to expose the
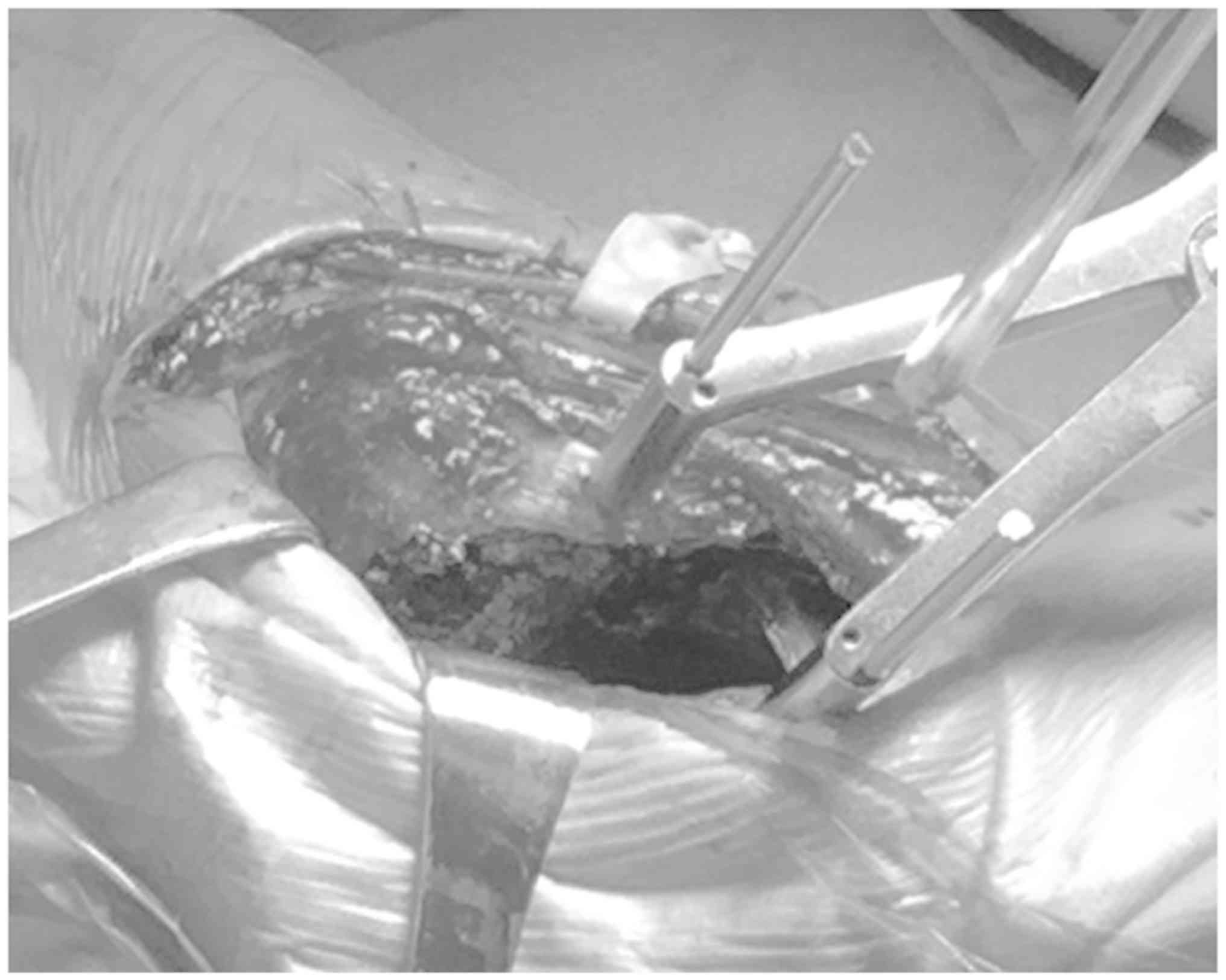
posterior tibial fracture fragments. In cases with incarcerated
soft tissue and die-punch fragments between the fracture fragments,
Kirschner wires were placed on either side of the fracture line; a
Kirschner wire retractor was then used to retract the Kirschner
wires to allow for the separation of the fractured bone. At this
point, it was possible to fully visualize the fibular fracture
fragments as well as the incarcerated soft tissue and bone
fragments in the fracture gap (Fig.
3). A small curette was used to remove the incarcerated tissue
from the tibial and fibular fracture gaps. First, the fractured
fibula was reduced via temporary Kirschner wire fixation. The
fracture fragment posterior to the tibia was exposed. The fracture
fragment could not be turned over due to the limited exposure of
the posterior tibia and the intact inferior tibiofibular ligament
during all the surgical procedures; however, the incarcerated
tissue between the fragments was removed via the fibular fracture
gap. This posterior fragment was then slightly elevated to separate
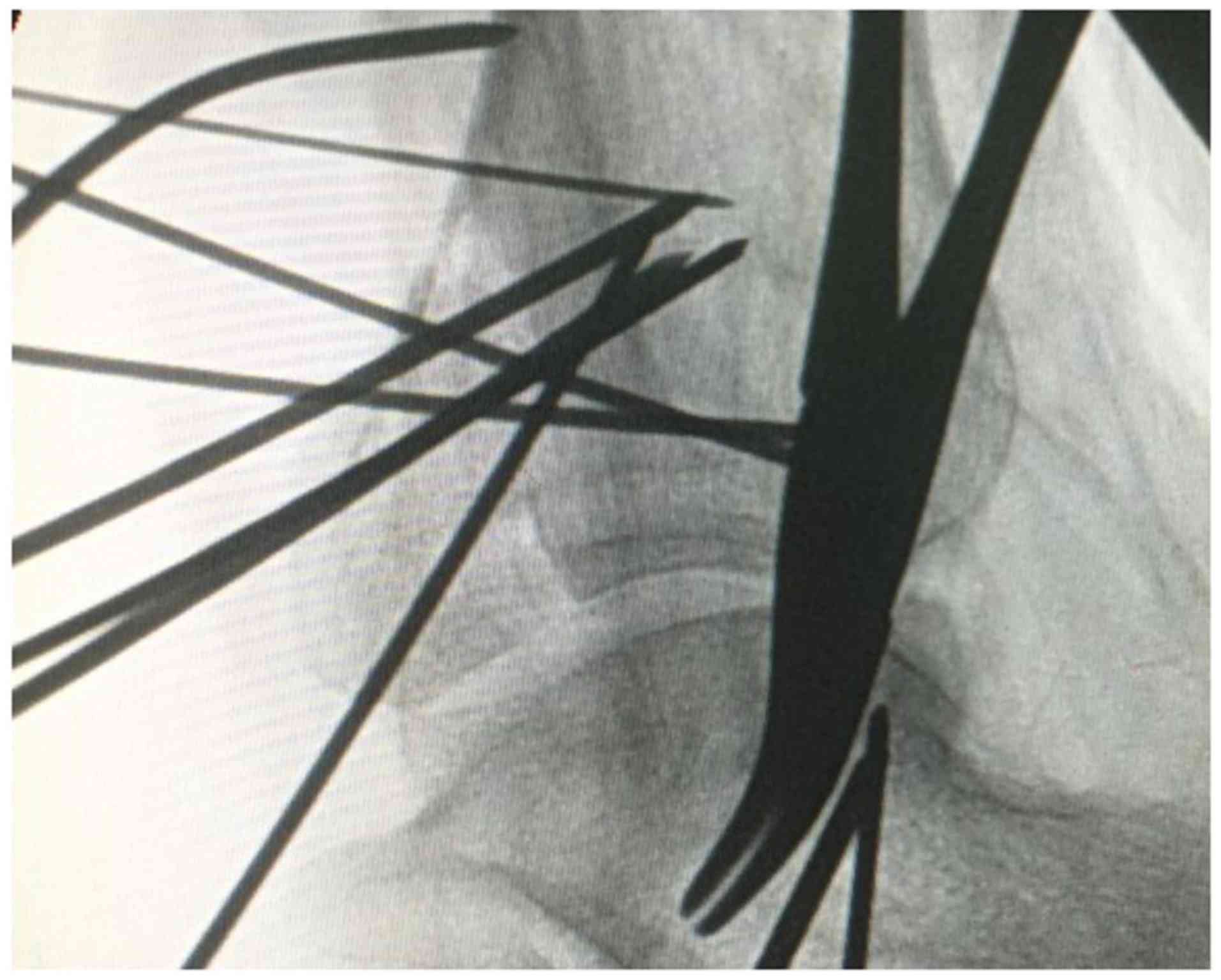
it from the tibia. The ankle was then subjected to extreme
extension to facilitate complete anatomical reduction. A Kirschner
wire was then used to temporarily fix the posterior fragment of the
ankle. Intra-operative fluoroscopy was performed to assess whether
the articular surface was smooth (Figs.
4 and 5). A posterior-lateral
plate and screws were used to fix the fibula. A specific anatomic
locked plate or a pre-bent distal radius plate was used to fix the
posterior fragments of the tibia. According to the conditions of
the medial malleolus fracture, a posterior-medial or medial
incision was made for medial malleolus fracture reduction and
fixation. The tourniquet was then released and adequate hemostasis
was achieved; subsequently, the incision was closed in layers.
Drainage of the incision was not required and the incision was
dressed with sterile dressings. The ankle was fixed via cast
immobilization in a neutral position. A total of 15 patients had
die-punch fragments between the tibia fracture fragments, and 10
patients received posterior-medial or medial incisions for medial
malleolus fracture reduction and fixation; this combination was
utilized as the medial malleolus fracture and the fracture
involving the posterior malleolus colliculus require the posterior
medial incision for reduction. It was difficult to expose the
posterior fracture fragment of the tibia via the fibula fracture
gap when the fracture lines of the tibia and fibula were not at the
same height. In such cases, it was necessary to extend the incision
and expose the fracture from behind the fibula. Images of typical
cases are presented in Figs.
6–8.
Post-operative treatment and
follow-up
Based on the fracture conditions, patients started
non-weight-bearing functional exercise on the second day
post-surgery if no ligament damage was present. Otherwise, the
patients were placed in a cast boot or a splint for 3 weeks and
started performing active range of motion exercises. The patients
were allowed full weight bearing following 6 weeks. Imaging
evaluation was performed using the Burwell-Charnley scoring system,
which focused on the degree of displacement of the medial and
lateral malleolus (8). Fractures
were considered clinically healed when the patient was able to bear
proper weight and experience no pain in the affected extremity and
no pain upon palpation/percussion. The mean American Orthopedic
Foot and Ankle Score (AOFAS) was 82.3 points (range, 44–97 points)
at the final follow-up visit.
Results
Preoperative treatment
The mean follow-up period was 14.5 months (range,
6–24 months). Following surgery, 17 patients were placed in a cast
boot for immobilization. 6 patients were free from post-operative
immobilization and allowed to start early motion exercises of the
ankle. The mean fracture recovery time was 2.1 months (range, 2–3
months). The mean time to full weight-bearing walking was 2.4
months.
Clinical and radiological
outcomes
Post-operative fracture reductions were evaluated
using Burwell-Charnley scores. Anatomical reduction was confirmed
in 17 patients (73.9%) and an acceptable reduction was observed in
6 patients (26%). At the final follow-up visit, the mean AOFAS was
82.3 points (range, 44–97 points). Good AOFASs (>75 points) were
reported in 20 patients, accounting for 86.9% of all patients.
Complications
Postoperative complications occurred in 5 patients
(21.7%). One patient had a post-operative wound infection (no
osteomyelitis and no plate exposure), and the wound healed
following localized treatment. One patient had post-operative
numbness around the incision and the dorsum of the foot that was
caused by intra-operative nerve retraction; these symptoms
gradually subsided 4 months following treatment with a neurotrophic
agent.3 patients complained of persistent pain and discomfort
following surgery even though their fractures had been clinically
healed. Their internal fixations were removed at 10, 13 or 14
months post-surgery, and they recovered well following the removal
of the internal fixation.
Discussion
Posterior pilon fractures are a specific type of
intra-articular fracture in the distal tibia and are caused by
low-energy rotational forces (posterior ankle fractures) or
high-energy axial forces (pilon fractures). Amorosa et al
(2) summarized the characteristics
of posterior pilon fractures as follows: i) The posterior fracture
fragment is large; ii) multiple fracture fragments may be present;
iii) a ‘stair’ phenomenon is observed; and iv) fracture fragments
are displaced toward the proximal direction. In clinical practice,
posterior pilon fractures are not uncommon. Switaj et al
(3) revealed that posterior pilon
fractures accounted for 20% of fractures in a series of 270
patients with ankle fractures who underwent surgical treatment.
Topliss et al (4) analyzed
the fracture lines of the distal tibia on axial views of CT images;
posterior pilon fractures, presenting with coronal fracture lines
and longitudinal displacement, accounted for 5.6% of all types of
fracture. Forberger et al (5)
performed a retrospective analysis of 45 patients with ankle
fractures and reported that proximal displacement of the posterior
fracture fragment was present in 73% of all ankle fractures. These
results indicated that longitudinal forces were involved the
fractures, and that they may be classified as posterior fractures.
As displacement of the posterior fragment in the distal tibia is
usually accompanied by posterior subluxation of the talus and
posterior ligament complex damage, this type of fracture has a poor
prognosis, with high probabilities of internal fixation failure and
traumatic arthritis. In the literature, this particular type of
fracture has drawn increasing attention (3,4).
Multiple classifications of posterior pilon fracture
have been used. Based on the location of the fracture line, Wang
et al (6) divided posterior
pilon fractures into two types. In type I fractures, two separated
posterior fracture fragments, a posterior-medial fracture fragment
and a medial malleolus fracture fragment are present, with the
fracture line located above the lower syndesmosis. In type II
fractures, the posterior-medial fracture fragment is adjacent to
the medial malleolus fracture fragment; the fragments are displaced
proximally, small incarcerated bones may be present and the
fracture line is located beneath the lower syndesmosis. Klammer
et al (1) retrospectively
analyzed patients with posterior pilon fracture and divided those
fractures into 3 types according to their increasing degree of
complexity. In type I fractures, a single posterior malleolar
fragment is present, and a long oblique fracture line runs through
the posterior colliculus (coronal view); type I fractures may be
fixed via a posterolateral approach alone. In type II fractures,
the posterior fragment is split into 2 pieces, a posterolateral
fragment and a posteromedial fragment involving the medial
malleolus; type II fractures may require an additional
posteromedial approach to assist in the reduction and fixation of
the posteromedial fragment. In type III fractures, a long oblique
fracture line divides the fragment into 2 pieces and runs through
the anterior portion of the medial malleolus; based on the
procedure for type II fractures, a posteromedial approach is always
required for the reduction and fixation of medial malleolus
fragments. This classification system cannot only describe the
severity of posterior pilon fractures but also guide the selection
of an appropriate surgical approach and internal fixation strategy.
The current classification system is based on CT images, which are
required for the diagnosis of posterior pilon fractures (9,10).
Posterior pilon fractures are frequently associated
with injury of the lower syndesmosis ligament. This ligament
originates from the posterior malleolus, attaches to the posterior
portion of the lateral malleolus and is an important structure for
maintaining ankle stability (11,12). In
addition, posterior pilon fractures may be accompanied by the
dislocation of the talus or comminuted lateral (medial) malleolus
fractures. Thus, posterior pilon fractures are a fracture pattern
between typical posterior malleolus fractures and pilon fractures,
and are considered unstable. Thus, it is necessary to select a
reliable reduction and fixation technique in clinical treatments.
Longer ankle immobilization is required in these cases, and 2 or 3
weeks of cast immobilization is recommended. The patients may start
weight-bearing exercise at week 6–12 and walk while bearing full
weight at 3 months (2,6,9).
Anatomic reduction is the first principle in the
treatment of posterior pilon fractures. Following reduction, the
residue step in the articular surface of the distal tibia should
not exceed 1 mm. Verhage et al (13) performed a follow-up study in 52
patients with trimalleolar fractures, in the surgery of which
patients were placed in the prone position. The posterolateral
approach to the ankle provides adequate access to the posterior
malleolus, allowing its anatomical reduction and stable fixation.
Complications rarely occur when using this approach. In terms of
fixation, the majority of clinicians prefer the posterolateral
approach and supportive plate fixation, particularly in patients
with osteoporosis (14–16). Certain clinicians have opted for
cannulated compression screw fixation (from posterior to anterior)
and have achieved satisfactory results (2,6). In
addition, a plate and screws may be used to fix the posterolateral
and posteromedial bone fragments, respectively, depending on the
condition of each case (17).
In certain cases, the peroneal tendon is entrapped
between the fibula fracture fragment and the posterior fragments of
the tibia, and is the major case of reduction failure in this
pattern of fracture with posterior dislocation of the talus. Lu
et al (18). Reported a rare
case of posterior pilon fracture combined with irreducible
dislocation and proposed a radiological characteristic, ‘tongues of
flame sign’, which indicates peroneal tendon entrapment between the
fibula and the posterior tibial fracture gap. All types of
posterior pilon fracture require open reduction. However, the
fracture fragment cannot be turned over due to the limited exposure
of the posterior tibia and the intact inferior tibiofibular
ligament. In addition, only the posterior tibial fracture line may
be visualized in the incision. An attempt to turn the fragment may
result in greater tissue damage. In the present study, the
posterior fracture fragment of the tibia was exposed via the fibula
fracture gap. Kirschner wires were used to retract the fibula
fracture fragment to expose the posterior edge of the tibia. This
method may clearly expose the incarcerated soft tissue and the
fracture fragments between the tibia fracture fragments. All
incarcerated tissues should be removed. Following the reduction of
the fibular fractures, K-wires may be used for temporary fixation
rather than using a plate, which may interfere with the obtainment
of satisfactory fluoroscopic images during surgery. If additional
posteromedial fragments are present, a posteromedial incision is
required to assist fixation. Either a plate or screws may be
selected for fixation.
There is a risk of damaging the sural nerve or
posterior tibial neurovascular bundles when using posterolateral or
additional posteromedial incisions, particularly in patients
requiring removal of internal fixations. The scars and adhesions in
the healed incision may be a challenge in secondary surgeries, and
an inexperienced surgeon may be more likely to cause intraoperative
damage during internal fixation removal. Post-operative
complications include wound infection, restrictions in ankle
mobility, hardware irritability and re-displacement of the
fracture. The incidence of postoperative complications was reported
as 11–47% (5,13–15). In
the present study, postoperative complications occurred in 5
patients (21.7%), and 1 patient had a post-operative wound
infection; the wound was healed following local treatment. One
patient had post-operative numbness around the incision and the
dorsum of the foot. The numbness gradually subsided after 4 months
of treatment with a neurotrophic agent. A total of 3 patients
complained of persistent pain, which improved following the removal
of their internal fixations. At the final follow-up in the present
study, the functional results were favorable with a mean AOFAS
score of 87.3, the anatomical reduction rate was 73.9%, which was
similar to the results of other studies (13,14).
Furthermore, their ankle mobility recovered well. Based on the
AOFAS, the average score for flexion and extension was 6.3 points
(maximum of 8 points), and the mean score for inversion and
eversion was 5.2 points (maximum of 6 points). A multicenter
randomized controlled study including 110 patients with unstable
ankle fractures undergoing surgical treatment reported that early
(2 weeks) ankle weight-bearing and motion exercise may improve the
functional prognosis of the ankle without increasing the incidence
of complications (19).
With the popularity of CT equipment in clinical
settings, patients who are diagnosed with ankle fracture by X-ray
examinations may be confirmed by CT. Therefore, it is not difficult
to make a definitive diagnosis of posterior pilon fracture.
Anatomical reduction and proper fixation of posterior fracture
fragments are essential for favorable prognoses. However,
conventional ankle fracture reductions, in which lateral malleolus
fractures are first reduced to achieve a reduction of the posterior
malleolus fracture via inferior tibiofibular ligament retraction,
may not restore a smooth articular surface. Therefore, it is
important to understand the definitions, classifications and
treatment guidelines of posterior fractures to develop a suitable
and reasonable treatment plan.
Notably, there were some limitations in the present
study. Limitations of the present study included the intrinsic
weakness of a retrospective study and lack of powerful statistical
data to reveal the advantage of the plate fixation method. In
addition, the incidence of the specific type of fracture is low, so
sample limitation is inevitable.
In conclusion, posterior pilon fractures are a
common pattern of ankle fractures. Achieving good clinical efficacy
requires the selection of an appropriate surgical approach and
proper post-operative rehabilitation. In the present study, a
posterolateral incision approach was employed that was able to
clearly expose the operative field without requiring the turning
over of the posterior fracture fragment of the tibia. The fibula
fracture gap was used to expose the incarcerated tissues between
the tibial fracture fragments and to reduce the fractures with
minimal trauma. Posterior placement of a plate may be employed to
maintain the stability of the anatomical reduction of the fracture
and promote early functional rehabilitation. Therefore, this
procedure may reduce the complication rate and is helpful in
post-operative recovery; thus, it is a safe and effective internal
fixation method.
Acknowledgements
Not applicable.
Funding
No funding received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
MG and NL collected clinical samples and wrote the
manuscript. YC and WS performed the experiments and statistical
analyses. HY designed the present study and revised the manuscript.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the First Affiliated Hospital of Soochow University
(Suzhou, China). Written informed consent was obtained from all
patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Klammer G, Kadakia AR, Joos DA, Seybold JD
and Espinosa N: Posterior pilon fractures: A retrospective case
series and proposed classification system. Foot Ankle Int.
34:189–199. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Amorosa LF, Brown GD and Greisberg J: A
surgical approach to posterior pilon fractures. J Orthop Trauma.
24:188–193. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Switaj PJ, Weatherford B, Fuchs D,
Rosenthal B, Pang E and Kadakia AR: Evaluation of posterior
malleolar fractures and the posterior pilon variant in operatively
treated ankle fractures. Foot Ankle Int. 35:886–895. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Topliss CJ, Jackson M and Atkins RM:
Anatomy of pilon fractures of the distal tibia. J Bone Joint Surg
Br. 87:692–697. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Forberger J, Sabandal PV, Dietrich M,
Gralla J, Lattmann T and Platz A: Posterolateral approach to the
displaced posterior malleolus: functional outcome and local
morbidity. Foot Ankle Int. 30:309–314. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang L, Shi ZM, Zhang CQ and Zeng BF:
Trimalleolar fracture with involvement of the entire posterior
plafond. Foot Ankle Int. 32:774–781. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fonseca LLD, Nunes IG, Nogueira RR,
Martins GEV, Mesencio AC and Kobata SI: Reproducibility of the
Lauge-Hansen, Danis-Weber, and AO classifications for ankle
fractures. Rev Bras Ortop. 53:101–106. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Burwell HN and Charnley AD: The treatment
of displaced fractures at the ankle by rigid internal fixation and
early joint movement. J Bone Joint Surg Br. 47:634–640. 1965.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li M, Collier RC, Hill BW, Slinkard N and
Ly TV: Comparing different surgical techniques for addressing the
posterior malleolus in supination external rotation ankle fractures
and the need for syndesmotic screw fixation. J Foot Ankle Surg.
56:730–734. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Evers J, Barz L, Wähnert D, Grüneweller N,
Raschke MJ and Ochman S: Size matters: The influence of the
posterior fragment on patient outcomes in trimalleolar ankle
fractures. Injury. 46 (Suppl 4):S109–S113. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Golanó P, Vega J, de Leeuw PA, Malagelada
F, Manzanares MC, Götzens V and van Dijk CN: Anatomy of the ankle
ligaments: A pictorial essay. Knee Surg Sports Traumatol Arthrosc.
24:944–956. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Evers J, Fischer M, Zderic I, Wähnert D,
Richards RG, Gueorguiev B, Raschke MJ and Ochman S: The role of a
small posterior malleolar fragment in trimalleolar fractures: A
biomechanical study. Bone Joint J 100-B. 95–100. 2018. View Article : Google Scholar
|
|
13
|
Verhage SM, Boot F, Schipper IB and
Hoogendoorn JM: Open reduction and internal fixation of posterior
malleolar fractures using the posterolateral approach. Bone Joint J
98-B. 812–817. 2016. View Article : Google Scholar
|
|
14
|
Chen DW, Li B, Aubeeluck A, Yang YF, Zhou
JQ and Yu GR: Open reduction and internal fixation of posterior
pilon fractures with buttress plate. Acta Ortop Bras. 22:48–53.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang Y, Wang J and Luo CF: Modified
posteromedial approach for treatment ofposterior pilon variant
fracture. BMC Musculoskelet Disord. 17:3282016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Abdelgawad AA, Kadous A and Kanlic E:
Posterolateral approach for treatment of posterior malleolus
fracture of the ankle. J Foot Ankle Surg. 50:607–611. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mak MF, Stern R and Assal M: Repair of
syndesmosis injury in ankle fractures: Current state of the art.
EFORT Open Rev. 3:24–29. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lu J, Maruo Holledge M, Trappel J and
Mayank M: A radiological sign (which we are calling the ‘tongues of
flame’ sign) in irreducible trimalleolar fractures of the ankle.
Foot Ankle Surg. 22:e6–e9. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dehghan N, McKee MD, Jenkinson RJ,
Schemitsch EH, Stas V, Nauth A, Hall JA, Stephen DJ and Kreder HJ:
Early weightbearing and range of motion versus non-weightbearing
and immobilization after open reduction and internal fixation of
unstable ankle fractures: A randomized controlled trial. J Orthop
Trauma. 30:345–352. 2016. View Article : Google Scholar : PubMed/NCBI
|