Introduction
Often featuring intensified cough in the morning and
at night and receiving no efficacy from antibiotics, cough variant
asthma, a special kind of chronic recurrent cough that is
characterized by the involvement of a variety of cells and cell
components, is one of the most prominent causes of chronic cough in
children (1,2). Approximately 30–54% of cough variant
asthma in children with this disease deteriorates further to
develop into typical bronchial asthma. With the changing society
and living habits, cough variant asthma is showing an increasing
incidence, greatly impacting the learning, physical and mental
health of children suffering from it (3,4).
Therefore, an active clinical treatment is required for children
with cough variant asthma.
According to the consensus of experts worldwide, the
treatment strategy of cough variant asthma is basically the same as
the treatment of bronchial asthma, mainly using montelukast sodium,
budesonide and loratadine in today's clinical practice (5–7).
Montelukast sodium is a highly specific and selective leukotriene
receptor antagonist, which can effectively improve airway
inflammation in children with cough variant asthma (8). Budesonide is a glucocorticoid that
enhances cell membrane stability, improves immune response, and
relieves bronchial muscle spasms (9). Loratadine, a piperidine antihistamine
commonly used in the treatment of allergic diseases, has also been
used in recent years to treat cough variant asthma (10). In some related studies, montelukast
sodium combined with budesonide or loratadine has been proven to
have a good efficacy in the treatment of cough variant asthma
(11,12). However, few comparative studies have
been made on the efficacy of these three drugs, montelukast sodium,
budesonide and loratadine in cough variant asthma. In addition,
tumor necrosis factor-α (TNF-α) and interleukin-4 (IL-4) are very
important indicators of inflammation. Many studies have reported
that the expression of these two factors in cough variant asthma
was increased (13,14).
This study retrospectively analyzed the medical
records of 72 child patients with cough variant asthma and compared
the clinical efficacy of montelukast sodium combined with
budesonide or loratadine in cough variant asthma to provide
reference in the drug treatment of cough variant asthma.
Patients and methods
Research subjects
A retrospective analysis of the medical records of
72 children with cough variant asthma who were treated in Xuzhou
Children's Hospital, Xuzhou Medical University (Xuzhou, China) from
April 2015 to August 2017 was performed and the 72 children were
divided into two groups: 35 children treated with montelukast
sodium combined with budesonide in Group A, and 37 children treated
with montelukast sodium combined with loratadine in Group B.
Inclusion criteria were: Child patients that met the following
diagnostic criteria (15): Cough, no
dyspnea or wheezing, relieved symptoms after the inhalation of
β2-adrenergic receptor agonists, a positive result of bronchial
hyperresponsiveness tested by methylcholine inhalation test or β2
agonist inhalation test, aged from 3 to 14 years, no history of
allergic diseases, no history of drug allergy, no history of
respiratory diseases, no infectious disease. Exclusion criteria
were: Children previously treated with leukotriene receptor
antagonists, glucocorticoids, antihistamines; children with chronic
cough; children with abnormal bleeding or coagulopathy combined
with cardiovascular diseases; children complicated with digestive
tract diseases; children who were transferred to another hospital
halfway; children whose families did not cooperate with the
treatment; children with incomplete medical records; children
without complete 24-week follow-up data.
This study was approved by the Ethics Committee of
Xuzhou Children's Hospital, Xuzhou Medical University, and the
parents of the child patients signed informed consents.
Treatment plan
Patients in Group A were treated with montelukast
sodium combined with budesonide, and patients in Group B were
treated with montelukast sodium combined with loratadine. In both
groups, patients under 6 years old were given montelukast sodium
(Hangzhou MSD Pharmaceutical Co., Ltd., medical product permitted
by the China Food and Drug Administration, code no. J20130047) 4.0
mg/time and once per day to chew before bedtime, while patients
under 6 years old were given montelukast sodium 5.0 mg/time and
once per day; in Group A, patients were given budesonide Aerosol
(Shanghai Sine Pharmaceutical Laboratories Co., Ltd., medical
product permitted by the China Food and Drug Administration, code
no. H20010552) 1 mg/time, once every 6–8 h; in Group B, patients
under 30 kilograms were given loratadine (Jiangsu Hengrui Medicine
Co., Ltd., medical product permitted by the China Food and Drug
Administration, code no. H20020436) 5.0 mg/time, while patients
above 30 kilograms were given loratadine 10 mg/time, once per day
to take orally before bedtime. All the drug treatments lasted 12
weeks. Then the clinical efficacy was evaluated in terms of the
lung function indexes and inflammatory markers before treatment and
at 4 and 12 weeks after treatment. The adverse reactions,
reoccurrence of disease and treatment compliance (the score of
treatment compliance ranged from 0 to 100 points, graded by 3
doctors who were either chief physicians or had more senior titles,
and a higher score indicated a better compliance) were also
recorded.
Criteria of the efficacy
evaluation
The evaluation of efficacy was divided into four
degrees: Complete recovery, significant efficacy, certain efficacy,
and no efficacy. Complete recovery means that the symptoms of cough
and asthma totally disappeared with no complications, significant
efficacy means that the symptoms of cough and asthma were basically
improved, and the incidence rate of complications was ≤5%; certain
efficacy means that the symptoms of cough and asthma were partly
improved, and the incidence rate of complications was ≤10%; no
efficacy refers to no improvement of symptoms and even worsen
symptoms (12).
Detection of lung function
indexes
The lung function indexes include the forced
expiratory volume in the first second (FEV1), the ratio of the
forced expiratory volume in the first second to the forced vital
capacity (FEV1/FVC), and the peak expiratory flow (PEF). The Master
Screen series lung function spirometer was purchased from
Jaeger.
Detection of inflammatory markers
The inflammatory markers in this study included
TNF-α and IL-4, which were measured by enzyme-linked immunosorbent
assay. Operation guide for blood collection: The peripheral blood
was collected by professional nurses in the morning and sent for
examination within 1 h. After centrifugation of the blood sample at
4,000 × g for 15 min at 4°C, serum was taken to be tested in strict
accordance with the manufacturers instructions. All test kits were
purchased from Shanghai Jingkang Biological Engineering Co., Ltd.,
and the article numbers of TNF-α and IL-4 detection kits were
JLC7047 and JLC6419, respectively.
Detection of eosinophil
granulocyte
The automatic hematology analyzer purchased from
Beckman Coulter Commercial Enterprise (China) Co., Ltd. (article
no. N/A) was used to detect the eosinophil granulocyte.
Detection of IgE
Enzyme-linked immunosorbent assay was used to detect
IgE guided by the manufacturers instructions. The detection kit for
IgE was purchased from Shanghai Yanhui Biotechnology Co. Ltd.
(article no. KA0216).
Statistical analysis
The software SPSS 19.0 (Asia Analytics Formerly SPSS
China) was used. The enumeration data were expressed as [n(%)], and
the ratio was compared using the χ2 test. The
measurement data were expressed with mean ± SD, and the t-test was
used for comparison between the two groups. Comparison of different
time-points within each group was performed with the repeated test
of variance measurement. LSD test was used for post hoc test.
Statistical significance was set at P<0.05.
Results
General information
No significant difference in the sex ratio and age
between the two groups existed as the Group A consisted of 17 males
and 18 females, with an average age of 6.7±0.8 years, and Group B
consisted of 17 males and 20 females, with an average age of
6.5±0.7 (P>0.05). The height and weight of patients from the two
groups were not statistically different (P>0.05). With regard to
the duration of cough, proportion of eosinophils, proportion of
basophils, and total serum IgE levels, the difference between the
two groups was not statistically significant (P>0.05) (Table I).
 | Table I.General information. |
Table I.
General information.
| Characteristics | Group A (n=35) | Group B (n=37) | χ2/t
value | P-value |
|---|
| Sex |
|
| 0.050 | 0.824 |
| Male | 17 (48.57) | 17 (45.95) |
|
|
| Female | 18 (51.43) | 20 (54.05) |
|
|
| Age (year) | 6.7±0.8 | 6.5±0.7 | 1.131 | 0.262 |
| Height (cm) | 112.35±23.57 | 118.42±24.73 | 1.065 | 0.291 |
| Weight (kg) | 26.13±4.32 | 27.59±4.73 | 1.365 | 0.177 |
| Duration of cough
(month) | 4.68±0.84 | 4.75±0.92 | 0.337 | 0.737 |
| Eosinophils (%) | 7.21±2.31 | 7.56±2.62 | 0.551 | 0.600 |
| White blood cells
(109/l) | 6.89±1.67 | 7.02±1.83 | 0.314 | 0.754 |
| Neutrophil
granulocytes (%) | 58.75±8.96 | 61.77±9.11 | 1.417 | 0.161 |
| Basophils (%) | 0.083±0.034 | 0.095±0.029 | 1.614 | 0.111 |
| Monocytes (%) | 6.33±1.45 | 6.41±1.62 | 0.220 | 0.826 |
| Lymphocytes (%) | 32.75±9.62 | 30.83±9.24 | 0.864 | 0.391 |
| Total serum IgE level
(IU/ml) | 638.74±84.57 | 613.85±78.69 | 1.294 | 0.200 |
| Score of the
frequency of gastroesophageal reflux | 9.65±6.32 | 10.12±6.96 | 0.299 | 0.766 |
| Airway
hyper-reactivity | Positive | Positive |
|
|
| Score of the
childhood asthma control test | 16.34±2.13 | 17.25±2.42 | 1.690 | 0.096 |
| Methacholine
challenge test | Positive | Positive |
|
|
Evaluation of efficacy
The evaluation of the efficacy of the two groups at
the 12 week after treatment showed no significant difference in the
rate of complete recovery, the rate of significant efficacy, the
rate of certain efficacy, the rate of no efficacy and the total
effective rate between the two groups (P>0.05) (Table II).
| Table II.Efficacy evaluation. |
Table II.
Efficacy evaluation.
| Factors | Group A (n=35) | Group B (n=37) | χ2
value | P-value |
|---|
| Complete
recovery | 20 (57.14) | 23 (62.16) | 0.188 | 0.664 |
| Significant
efficacy | 10 (28.57) | 9 (24.32) | 0.167 | 0.683 |
| Certain efficacy | 2 (5.71) | 3 (8.11) | 0.159 | 0.690 |
| No efficacy | 3 (8.57) | 2 (5.41) | 0.279 | 0.597 |
| Overall effective
rate | 32 (91.43) | 35 (94.59) | 0.279 | 0.597 |
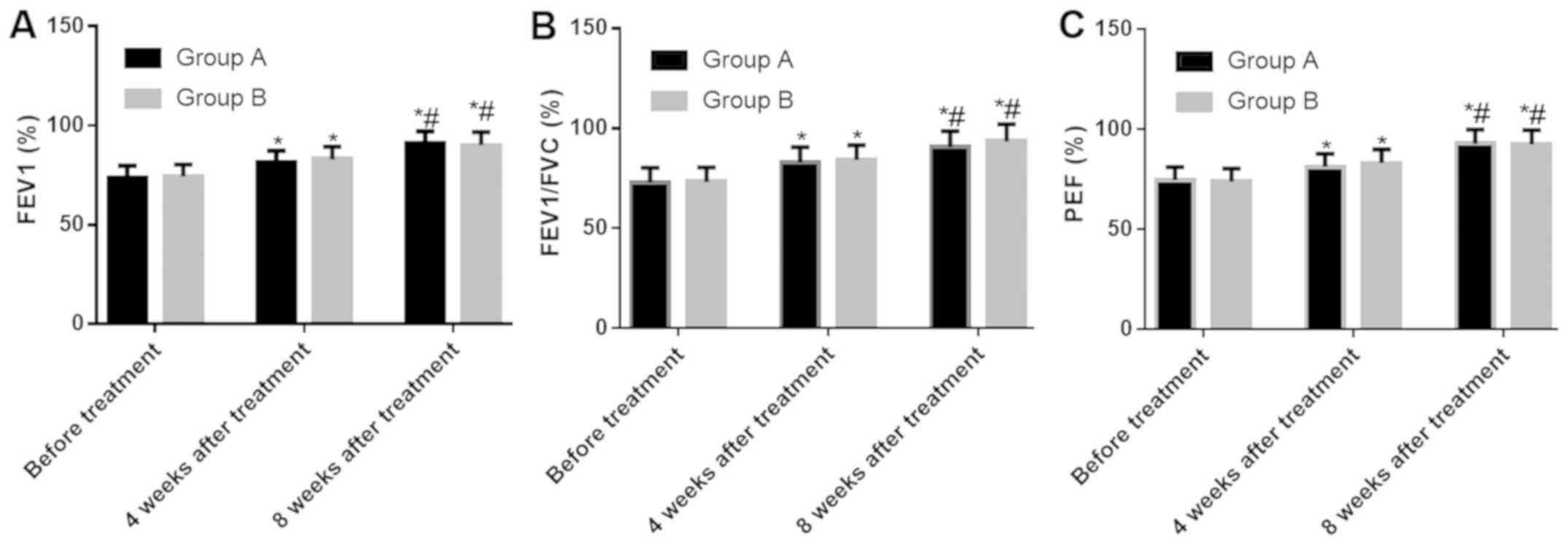
Changes in lung function indexes in
the two groups
The results of lung function tests in the two groups
showed no significant difference in the FEV1, FEV1/FVC and PEF
between the two groups at three time-points: Before treatment, the
4th week after treatment, and the 12th week after treatment
(P>0.05). According to the comparison within each group, the
levels of FEV1, FEV1/FVC and PEF at the 4th and 12th week after
treatment were higher than those before treatment (both P<0.05),
and the levels of FEV1, FEV1/FVC and PEF at the 12th week after
treatment in the two groups were higher than those at the 4th week
after treatment (both P<0.05) (Fig.
1).
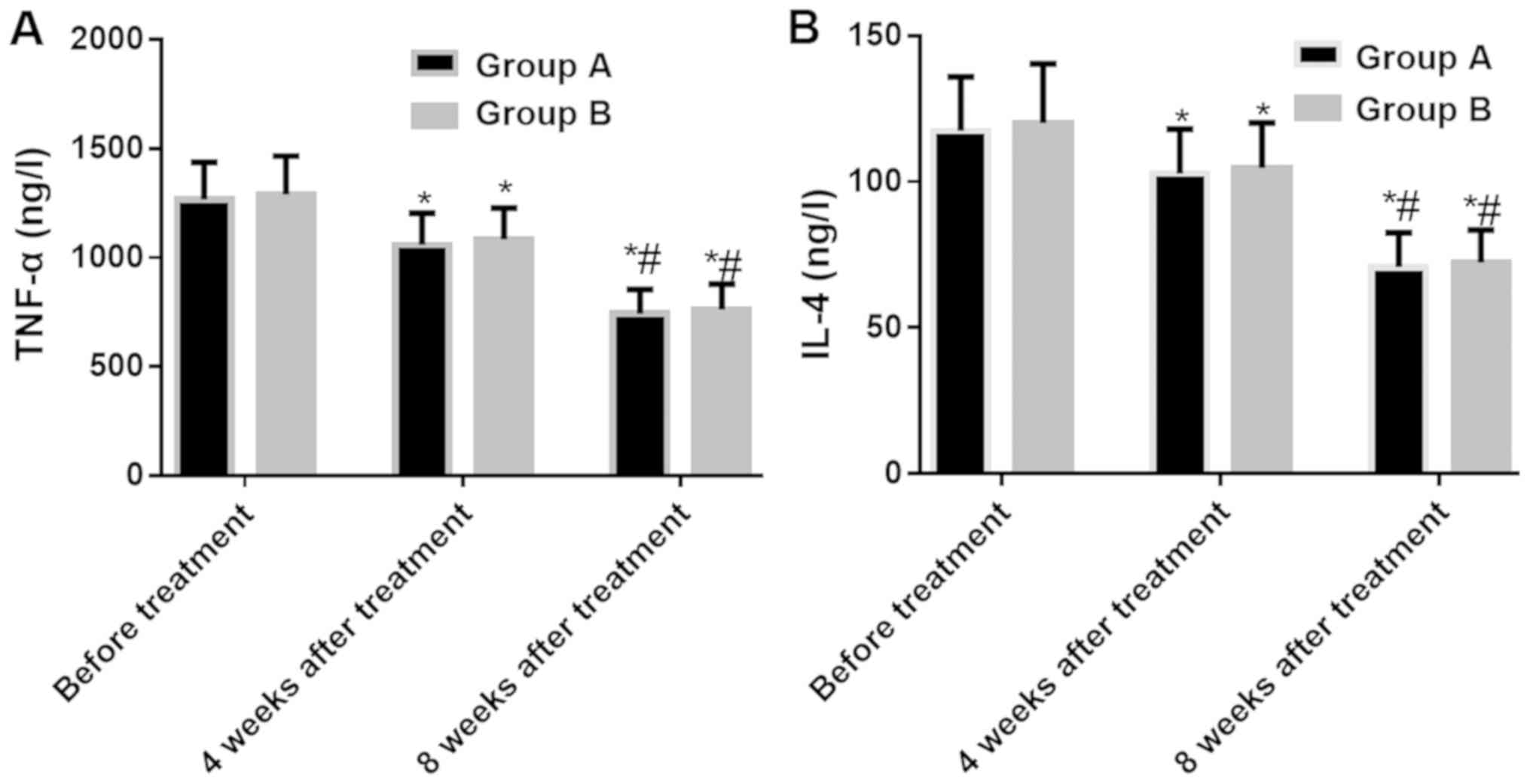
Changes in inflammatory markers in the
two groups
The tests of the inflammatory markers in the two
groups showed that there was no significant difference in the TNF-α
and IL-4 between the two groups at three time-points: Before
treatment, the 4th week after treatment, and the 12th week after
treatment (P>0.05). According to the comparison within each
group, the TNF-α and IL-4 levels were significantly decreased after
treatment and the inflammatory reaction was under effective
control. The TNF-α and IL-4 levels at the 4th and 12th week after
treatment were lower than those before treatment (both P<0.05),
and the levels of TNF-α and IL-4 at the 12th week after treatment
in the two groups were lower than those at the 4th week after
treatment (both P<0.05) (Fig.
2).
Changes in the eosinophil granulocytes
in the two groups
In both groups, the eosinophil granulocyte levels at
three time-points (before treatment, at the 4th week after
treatment, and at the 12th week after treatment) were not
statistically different (P>0.05). According to the comparison
within each group, no statistical difference was detected between
the eosinophil granulocyte level before treatment and the
eosinophil granulocyte level at the 4th week after treatment
(P>0.05), but the eosinophil granulocyte level at the 12th week
after treatment was lower than that at the 4th week after treatment
(P<0.05) (Table III).
| Table III.Changes in the eosinophil
granulocytes in the two groups (%). |
Table III.
Changes in the eosinophil
granulocytes in the two groups (%).
| Time-points | Group A (n=35) | Group B (n=37) | t value | P-value |
|---|
| Before
treatment | 7.21±2.31 | 7.56±2.62 | 0.551 | 0.600 |
| The 4th week after
treatment | 6.86±1.14 | 6.75±1.17 | 0.404 | 0.688 |
| The 12th week after
treatment |
6.32±0.97a,b |
6.44±0.85a,b | 0.559 | 0.578 |
Changes in the IgE in the two
groups
The tests of the IgE in the two groups showed that
there was no significant difference in the IgE levels between the
two groups at three time-points: before treatment, at the 4th week
after treatment, and at the 12th week after treatment (P>0.05).
According to the comparison within each group, the IgE levels at
the 4th and 12th week after treatment were lower than those before
treatment (both P<0.05), and the IgE levels at the 12th week
after treatment in the two groups were lower than those at the 4th
week after treatment (both P<0.05) (Table IV).
| Table IV.Changes in the IgE in the two groups
(IU/ml). |
Table IV.
Changes in the IgE in the two groups
(IU/ml).
| Time-points | Group A (n=35) | Group B (n=37) | t value | P-value |
|---|
| Before
treatment | 638.74±84.57 | 613.85±78.69 | 1.294 | 0.200 |
| The 4th week after
treatment |
582.64±70.51a |
574.35±70.51a | 0.506 | 0.614 |
| The 12th week after
treatment | 495.22
aftera,b | 483.87
aftera,b | 0.812 | 0.420 |
The incidence of adverse reactions in
the two groups
The two groups had 3 cases each of adverse reactions
(not very severe) which were healed after receiving the
corresponding treatment intervention. No statistically significant
difference in the incidence of complications and the incidence of
respiratory tract infection between the two groups was found as
there was 1 case of respiratory tract infection, 1 case of
pneumonia, and 1 case of drowsiness in Group A, while 2 cases of
respiratory tract infection and 1 case of fatigue in Group B (both
P>0.05) (Table V).
| Table V.The incidence of adverse reactions in
the two groups of children. |
Table V.
The incidence of adverse reactions in
the two groups of children.
| Factors | Group A (n=35) | Group B (n=37) |
|---|
| Respiratory tract
infection | 1 (2.86) | 2 (5.41) |
| Pneumonia | 1 (2.86) | 0 (0.00) |
| Fatigue | 0 (0.00) | 1 (2.70) |
| Drowsiness | 1 (2.86) | 0 (0.00) |
| Overall incidence
rate | 3 (8.57) | 3 (8.11) |
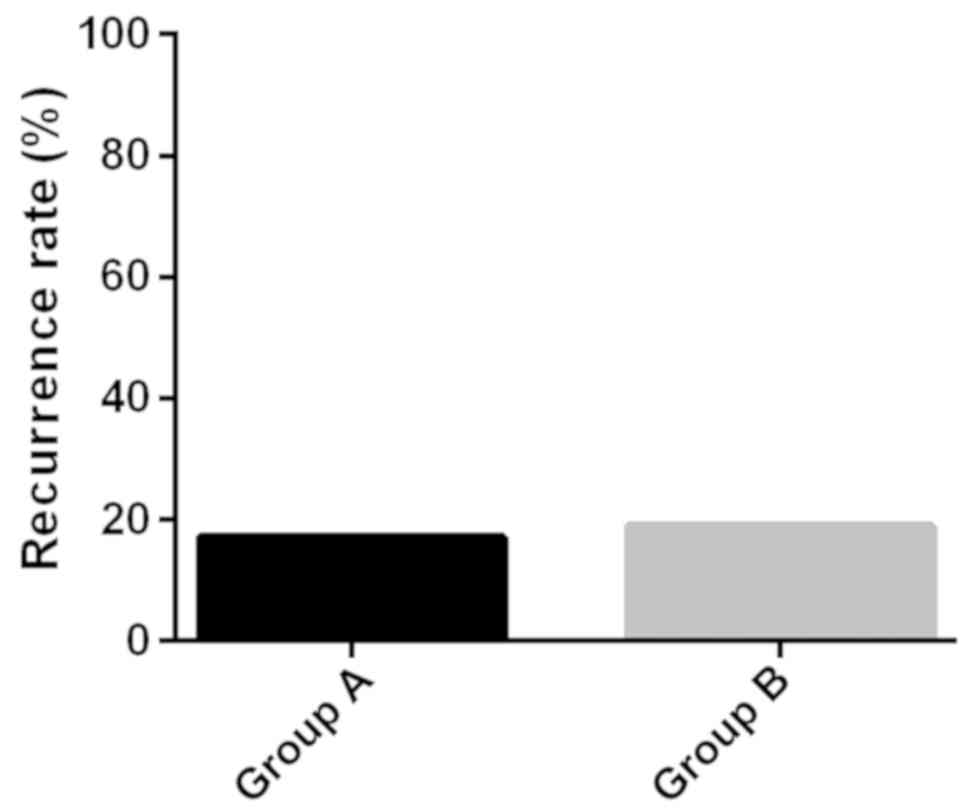
Recurrence of the disease in the two
groups
The follow-up continued for 24 weeks after the
completion of treatment. During the follow-up, 6 patients in Group
A had recurrence, with a recurrence rate of 17.14%, and 7 patients
in Group B had recurrence, with a recurrence rate of 18.92%, the
difference between the two groups was not statistically significant
(P>0.05) (Fig. 3).
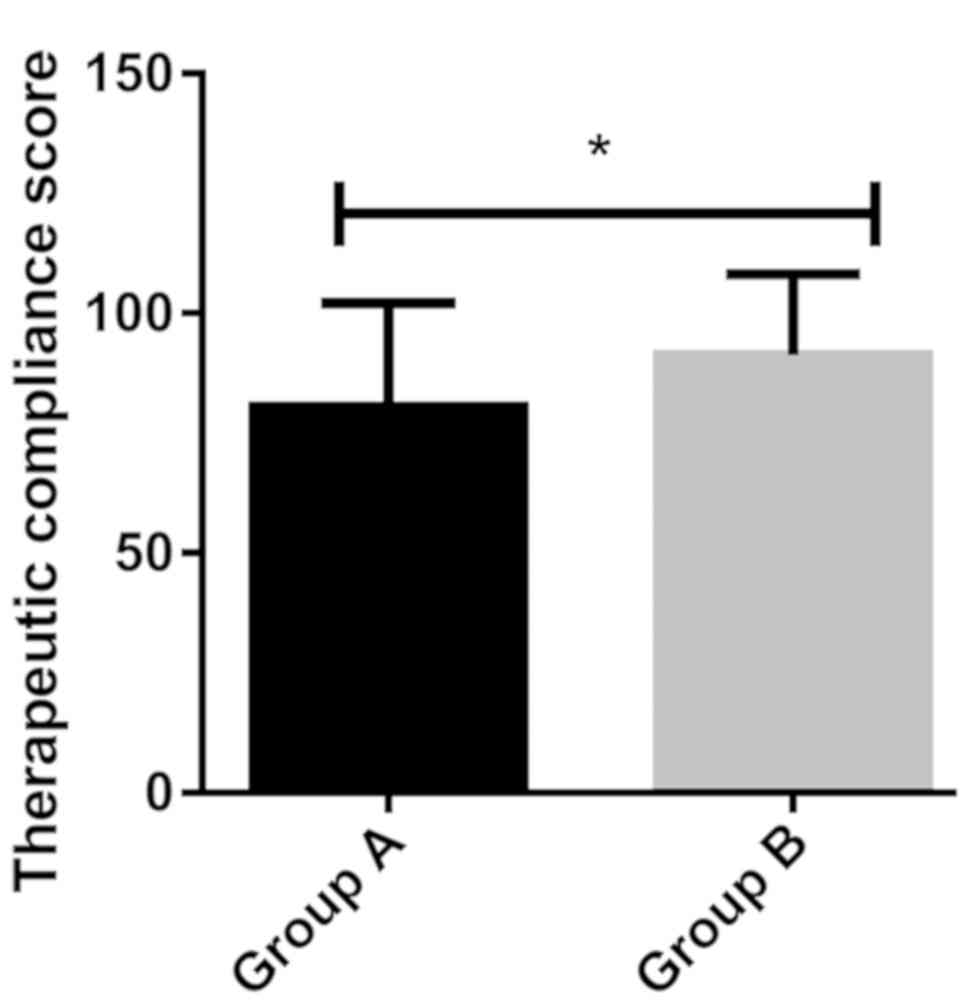
Analysis of the treatment
compliance
The treatment compliance analysis of the two groups
showed that the treatment compliance score of Group A (80.42±21.75)
was significantly lower than that of Group B (91.36±16.78)
(P<0.05) (Fig. 4).
Discussion
Considering the fact that cough variant asthma has
similar clinical symptoms to clinical typical asthma such as
respiratory remodeling, inflammatory cell infiltration and
generally airway hyperresponsiveness, a consensus has been reached
worldwide that the principles of treating cough variant asthma are
consistent with that of treating typical asthma (15,16).
However, different countries or regions lack a unified opinion on
the choice of therapeutic drugs, and there is no relevant
evidence-based medical basis for the choice of treatment options.
This study retrospectively analyzed the efficacy of montelukast
sodium combined with budesonide or loratadine in cough variant
asthma in order to provide a reference for clinical treatment.
The study collected the medical records of two
groups of children with cough variant asthma strictly according to
the inclusion and exclusion criteria. No statistical difference
between the two groups of patients existed in the general data,
indicating that the two groups were comparable in this study and
the results of this study had certain credibility. Leukotriene
receptor antagonists, glucocorticoids, and antihistamines are the
three major types of drugs for the treatment of cough variant
asthma (17,18). Leukotriene can induce spasms of
bronchial smooth muscle, increase of vascular permeability and
infiltration of inflammatory cells. Montelukast sodium, one of the
most frequently mentioned leukotriene receptor antagonists in the
treatment of cough variant asthma, is reported worldwide with
excellent efficacy, low adverse reactions and high patient
compliance (8,19). Studies have reported that the main
cause of cough variant asthma is airway hyperresponsiveness caused
by abnormal inflammatory reactions which can be effectively
improved by glucocorticoids such as budesonide, especially through
the dosing method of atomization inhalation (20,21).
Loratadine, a piperidine antihistamine that antagonizes peripheral
H1 receptors over a long time efficiently, can greatly improve the
airway hyperresponsiveness, inhibit the degranulation of
eosinophils and mast cells, and reduce the release of leukotrienes
(22). The good complementarity and
synergistic therapeutic effects of montelukast sodium combined with
budesonide or loratadine in cough variant asthma have been reported
in many studies (11,12). According to the results of this
study, both methods of drug treatments had a good therapeutic
effect with an effective rate of >90%, and improved eosinophil
granulocyte level and IgE level, similarly to previous research
results (11,12). The two methods of drug treatment both
had similar efficacy in improving the lung function indexes and the
inflammation symptoms, slight adverse reactions, and not
statistically different incidence rates of recurrence, proving that
montelukast sodium combined with budesonide or loratadine were
equivalent in the treatment efficacy of cough variant asthma.
However, the atomization inhalation therapy's requiring special
inhalation techniques and shortage of aerosol devices usually
causes low compliance in patients (23,24)
which was reflected in this study. Therefore, for younger patients
with poor compliance, montelukast sodium combined with loratadine
can be a better choice.
However, this study also had some defects. In this
study, we did not find any differences between the two combination
therapies, which may be related to our exclusion criteria or the
number of our cases, or due to the 12 weeks of treatment time,
while the follow-up time was 24 weeks after the completion of the
treatment. Both were relatively short. The long-term efficacy of
the two treatment methods still needs to be further studied and
determined, and continued follow-up will be needed in the future.
Also, the age range of the patients included in this study was
large, and because TNF-α and IL-4 are the most commonly detected
inflammatory factors in our hospital, in order to avoid the
occurrence of fewer cases, we did not include other inflammatory
indicators, such as IL-5, IL-13, which might lead to bias in the
results of compliance analysis, so more clinical data and narrowed
age range will be asked in future studies to make further analysis.
This study aimed to inspire more scholars to conduct large-scale,
multi-center experiments for in-depth research.
In summary, both the combination of montelukast
sodium and budesonide and the combination of montelukast sodium and
loratadine had similar efficacy in cough variant asthma to
effectively improve the lung function and inflammatory response in
patients without causing more adverse reactions and higher
recurrence rate, both worthy of clinical promotion. For patients
with younger age and poor compliance, the method of using
montelukast sodium combined with loratadine is preferably
advised.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
HW and WL helped with detection of lung function
indexes. HW and ZJ worked on detection of inflammatory markers. XX
and GQ collected, analyzed and interpreted the general data of
patients, and revised the manuscript critically for important
intellectual content. HW was involved in the writing of this
manuscript. All the authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Xuzhou Children's Hospital, Xuzhou Medical University (Xuzhou,
China). Signed informed consents were obtained from the parents of
the child patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hossain SS, Islam MS, Rahman MM, Dey S and
Mahmud K: Clinical and demographic profiles of patients diagnosed
as cough variant asthma attended at Tertiary Referral Hospital.
JNINB. 2:12016.
|
|
2
|
Kanemitsu Y, Niimi A, Matsumoto H, Iwata
T, Ito I, Oguma T, Inoue H, Tajiri T, Nagasaki T, Izuhara Y, et al:
Gastroesophageal dysmotility is associated with the impairment of
cough-specific quality of life in patients with cough variant
asthma. Allergol Int. 65:320–326. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tagaya E, Kondo M, Kirishi S, Kawagoe M,
Kubota N and Tamaoki J: Effects of regular treatment with
combination of salmeterol/fluticasone propionate and salmeterol
alone in cough variant asthma. J Asthma. 52:512–518. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tajiri T, Niimi A, Matsumoto H, Ito I,
Oguma T, Otsuka K, Takeda T, Nakaji H, Inoue H, Iwata T, et al:
Prevalence and clinical relevance of allergic rhinitis in patients
with classic asthma and cough variant asthma. Respiration.
87:211–218. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Evans DJ, Taylor DA, Zetterstrom O, Chung
KF, O'Connor BJ and Barnes PJ: A comparison of low-dose inhaled
budesonide plus theophylline and high-dose inhaled budesonide for
moderate asthma. N Engl J Med. 337:1412–1418. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bao W, Chen Q, Lin Y, Liu H, Zhao G, Chen
Z and Zhou X: Efficacy of procaterol combined with inhaled
budesonide for treatment of cough-variant asthma. Respirology. 18
(Suppl 3):53–61. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Frølund L: Efficacy of an oral
antihistamine, loratadine, as compared with a nasal steroid spray,
beclomethasone dipropionate, in seasonal allergic rhinitis. Clin
Otolaryngol Allied Sci. 16:527–531. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wang X, Liu B, Lu B, Zhang Y, Wang L, Li
H, Han X and Ding D: Micro-invasive embedding combined with
montelukast sodium for children cough variant asthma: A randomized
controlled trial. Zhongguo Zhen Jiu. 37:259–264. 2017.(In Chinese).
PubMed/NCBI
|
|
9
|
Zhou X, Hong J, Cheng H, Xie J, Yang J,
Chen Q, He S, Li Y, Zhou X and Li C: Budesonide suspension
nebulization treatment in Chinese pediatric patients with cough
variant asthma: A multi-center observational study. J Asthma.
53:532–537. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Steffey EP, Mama KR, Galey FD, Puschner B
and Woliner MJ: Effects of sevoflurane dose and mode of ventilation
on cardiopulmonary function and blood biochemical variables in
horses. Am J Vet Res. 66:606–614. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wei Y, Li DS, Liu JJ, Zhang J and Zhao HE:
Therapeutic effect and safety of montelukast sodium combined with
budesonide in children with cough variant asthma: A meta analysis.
Zhongguo Dang Dai Er Ke Za Zhi. 18:1100–1105. 2016.(In Chinese).
PubMed/NCBI
|
|
12
|
Wang XP, Yang LD and Zhou JF: Montelukast
and budesonide combination for children with chronic cough-variant
asthma. Medicine (Baltimore). 97:e115572018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Xiao Q and Qin X: Effects of salmeterol
xinafoate and fluticasone propionate powder in combination with
montelukast on pulmonary function and serum inflammatory cytokines
in children with cough variant asthma. Zhongguo Jiceng Yiyao.
25:182–185. 2018.(In Chinese).
|
|
14
|
Jiao HY, Su WW, Li PB, Liao Y, Zhou Q, Zhu
N and He LL: Therapeutic effects of naringin in a guinea pig model
of ovalbumin-induced cough-variant asthma. Pulm Pharmacol Ther.
33:59–65. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Takemura M, Niimi A, Matsumoto H, Ueda T,
Yamaguchi M, Matsuoka H, Jinnai M, Chin K and Mishima M: Atopic
features of cough variant asthma and classic asthma with wheezing.
Clin Exp Allergy. 37:1833–1839. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Saito N, Itoga M, Tamaki M, Yamamoto A and
Kayaba H: Cough variant asthma patients are more depressed and
anxious than classic asthma patients. J Psychosom Res. 79:18–26.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dicpinigaitis PV: Chronic cough due to
asthma: ACCP evidence-based clinical practice guidelines. Chest.
129 (Suppl 1):75S–79S. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Usta Guc B, Asilsoy S and Durmaz C: The
assessment and management of chronic cough in children according to
the British Thoracic Society guidelines: Descriptive, prospective,
clinical trial. Clin Respir J. 8:330–337. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Matsuse H and Kohno S: Leukotriene
receptor antagonists pranlukast and montelukast for treating
asthma. Expert Opin Pharmacother. 15:353–363. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sun LH, Chen AH and Zhang Y: Therapeutic
efficacy and follow-up study of inhaled corticosteroids vs. oral
montelukast in treatment of cough variant asthma. Zhonghua Er Ke Za
Zhi. 46:85–88. 2008.(In Chinese). PubMed/NCBI
|
|
21
|
Peng QF and Kong LF: The levels of nerve
growth factor and IL-4 in induced sputum and characteristics of
airway inflammation in cough variant asthma. Zhonghua Nei Ke Za
Zhi. 50:221–224. 2011.(In Chinese). PubMed/NCBI
|
|
22
|
Fujimura M, Ogawa H, Nishizawa Y and Nishi
K: Comparison of atopic cough with cough variant asthma: Is atopic
cough a precursor of asthma? Thorax. 58:14–18. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sanchis J, Gich I and Pedersen S; Aerosol
Drug Management Improvement Team (ADMIT), : Systematic review of
errors in inhaler use: Has patient technique improved over time?
Chest. 150:394–406. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Deuse T, Hua X, Stubbendorff M, Spin JM,
Neofytou E, Taylor V, Chen Y, Park G, Fink JB, Renne T, et al: The
selective JAK1/3-inhibitor R507 mitigates obliterative airway
disease both with systemic administration and aerosol inhalation.
Transplantation. 100:1022–1031. 2016. View Article : Google Scholar : PubMed/NCBI
|