Introduction
Lichen planus (LP) is an idiopathic, cell-mediated
immune disorder, accompanied by itching, mucosal lesions and
characteristic skin lesions in most cases. The clinical
manifestations of LP have been described as the ‘6 Ps’ of LP,
namely: Pruritic, purple, polygonal, planar, papules and plaques,
encompassing the main manifestations of this disorder (1). Different subtypes of LP are more
prevalent in certain populations and sub groups, for example,
actinic, hypertrophic, pigmentosus and childhood variants are more
common in African American and darker-skinned populations. Of note,
childhood LP has a greater male prevalence, which is unusual for an
autoimmune disorder (1).
There is a potential for the development of
malignancy in association with mucosal lesions. Spontaneous
remission occurs. Topical and systemic therapies are utilized
including potent topical steroids, topical calcineurin inhibitors,
psoralen and ultraviolet A (PUVA), narrow band UVB, oral
corticosteroids and acitretin (2).
Since these therapies are not without complications
and may be ineffective in some cases, other treatment modalities
with potential are welcome. Complementary and alternative or
integrative therapies have been tried as a therapeutic possibility
and as a way of avoiding the side effects of conventional
therapies. A study of Ayurvedic medicine, combining herbs and diet
for LP therapy, reported 100% remission rates, although residual
post-inflammatory hyperpigmentation and dryness were seen (3).
Homeopathy is a therapeutic system developed by the
German physician, Samuel Hahnemann. It is based on the utilization
of infinitesimal concentrations (extremely high dilutions) of
substances to treat diseases and thus, is free of the side effects
associated with conventional therapy. Its exact mechanism of action
remains to be elucidated, but homeopathy enjoys increasing
popularity with growth rates of 25% per year in India (4) and in the US, homeopathy was one of the
most commonly used forms of CAM, used by 2.1% of the population
(5).
Four cases of recalcitrant, generalized LP with and
without mucosal involvement treated homeopathically are
presented.
This study was approved by the Ethics Committee of
Cabinet Medical Individual (Bucharest, Romania), and a written
informed consent was provided by all the patients included in this
study.
Case studies
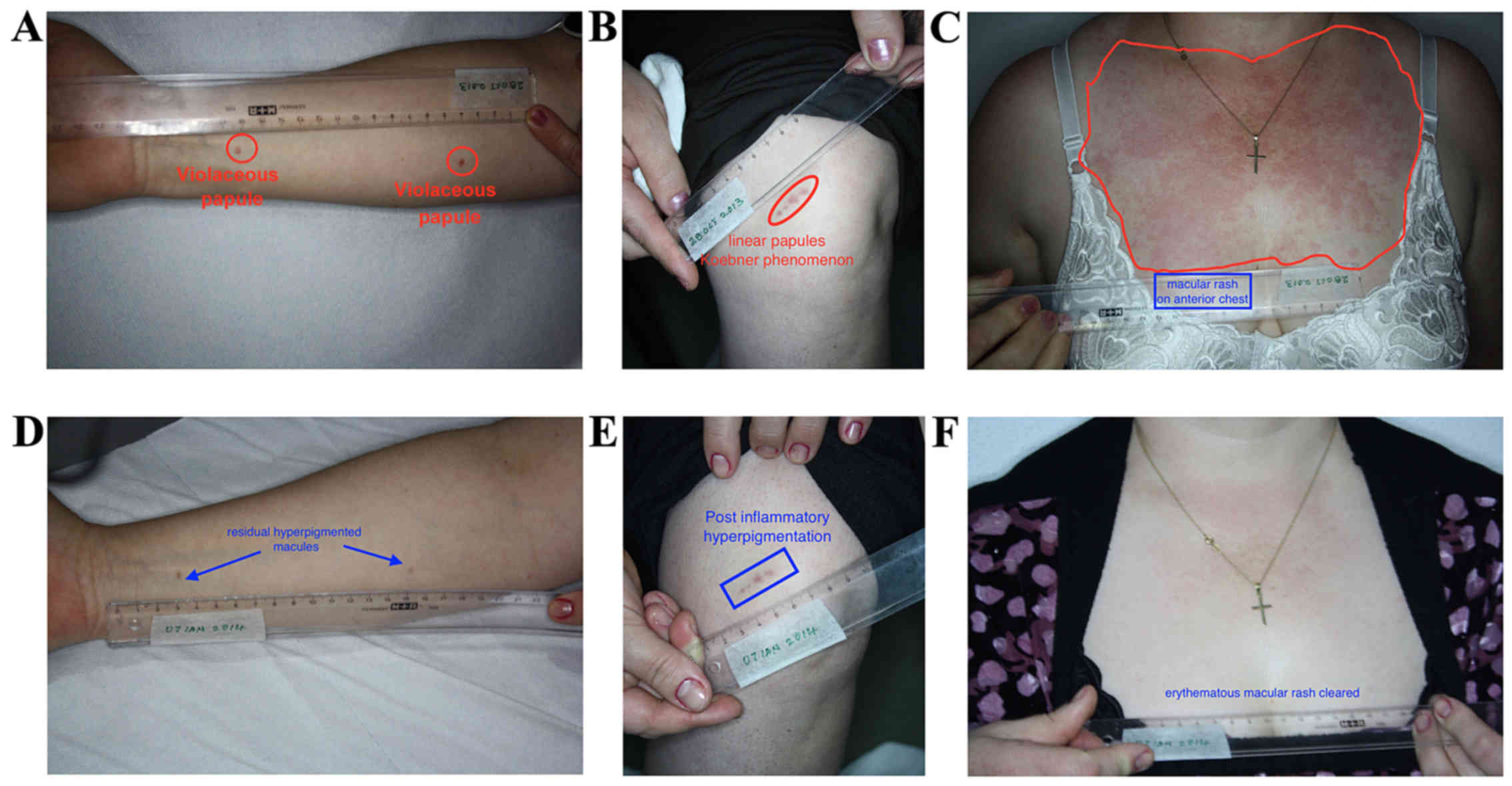
Case 1
A 48-year-old female presented with a 7-month
history of generalized LP. Topical corticosteroid treatment and
removal of dental fillings did not ameliorate the condition.
Examination revealed violaceous papules on upper and lower limbs,
oral mucosal lesions and an irregular, erythematous, blanching,
macular rash on the chest. She received the homeopathic medicine
Ignatia amara at MK potency, weekly dosage and went into
remission at 3 months. The patient relapsed (after presentation of
the abstract of this work), following work-related stress and
dental work, at 2.5 years after the last visit. She presented with
only oral lesions, which responded to Ignatia amara MK
(Fig. 1A-F).
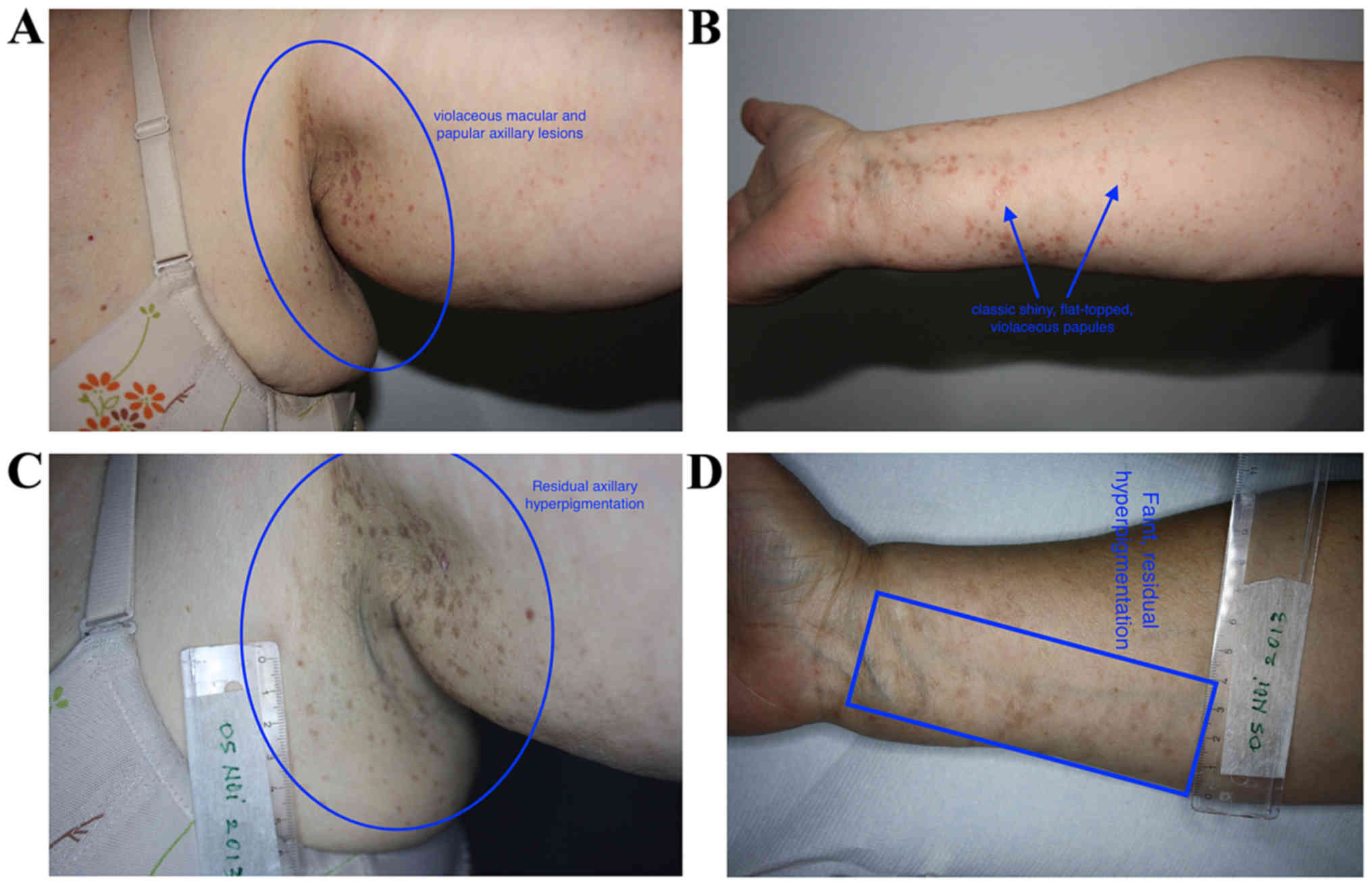
Case 2
A 65-year-old female presented with a 27-year
history of generalized, LP, which was unresponsive to topical
steroids. Examination showed generalized, violaceous papules, with
no mucosal involvement. She received homeopathic Aurum
metallicum, MK potency, weekly dosage, and went into remission.
She relapsed at 8 months after onset of therapy, following a
stressful incident, but remitted again with repetition of Aurum
metallicum after 1 month of therapy. She remained in remission
for 3 years until the death of her mother, which triggered a
relapse for which she received Aurum metallicum again. This
helped put her into remission once more (Fig. 2A-D).
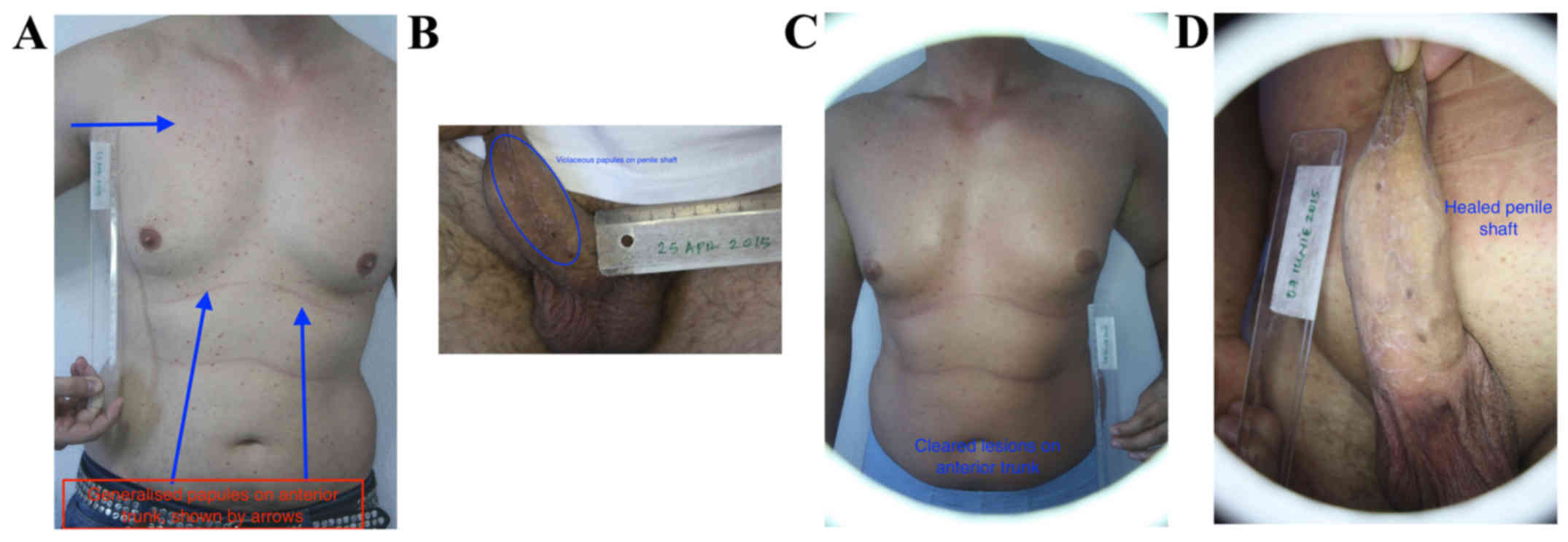
Case 3
A 38-year-old male presented with a 21-year history
of generalized LP. Medical history was significant for hepatitis B
and asthma. Topical clobetasol had been tried with only limited
success. Examination revealed generalized, violaceous papules, with
oral and genital involvement. He received homeopathic Lycopodium
clavatum at MK potency, weekly dosage, and remitted by 2
months. He remains in remission (Fig.
3A-D).
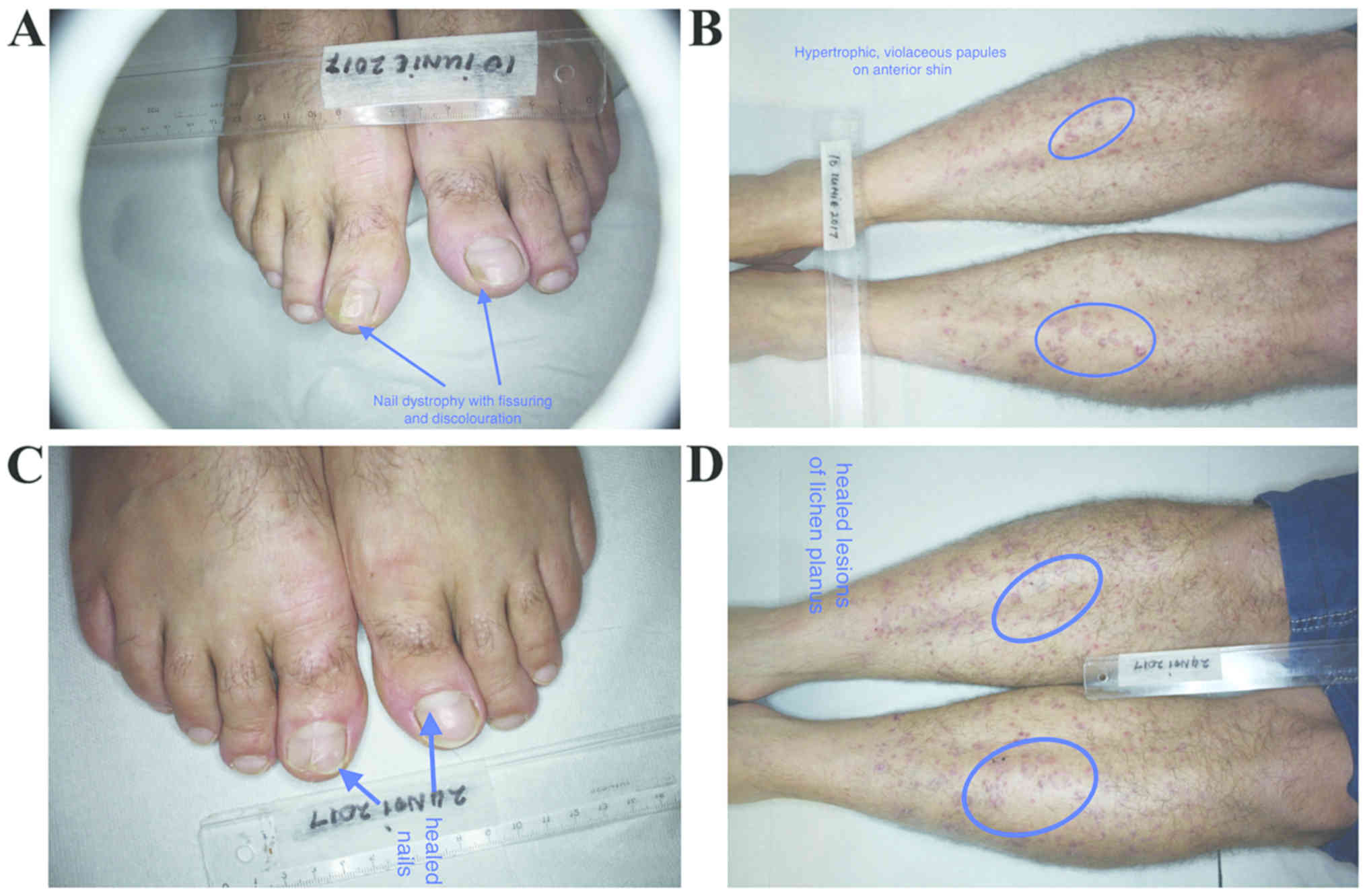
Case 4
A 41-year-old male presented with a 12-year history
of itchy rash, which had responded partially to topical steroids
and UVA therapy. Medical history was significant for reduced sense
of smell. Examination revealed generalized, violaceous,
hypertrophic papules, with dystrophic nails. He also had palmar and
plantar hyperkeratosis. No mucosal lesions were observed. He
received homeopathic Carcinosinum at MK potency and remitted
at 6 months, with improved sense of smell (Fig. 4A-D).
Discussion
LP is an idiopathic, autoimmune disorder primarily
involving the cell-mediated immune system. It constituted 0.38 and
5% of dermatology patients (6,7) in India
and Nigeria respectively, as well as 32–38/100,000 patients
(8) in a UK review of GP
practices.
Differential diagnosis of LP includes prurigo,
eczema, psoriasis, drug eruption, oral leukoplakia, candida
infection, Queyrat erythroplasia and genital lichen sclerosus
(2,9,10).
Distinguishing these conditions from LP is essential, as some of
these conditions are not as benign as LP itself (11). In spite of this, the diagnosis of LP
is often straightforward as the violaceous lesions of LP tend to be
characteristic and histopathology is reserved for difficult cases
(9–11).
Histopathology of LP is characteristic, comprising a
hyperkeratotic epidermis with irregular acanthosis and focal
thickening of the granular layer. Colloid or civatte bodies, which
are degenerative keratinocytes can be found in the lower epidermis.
Other colloid bodies comprising IgM (occasionally IgG and IgA) with
complement can also be seen. There are fibrin and fibrinogen
deposits in the basement membrane zone. A band-like lymphocytic
infiltrate (mostly helper T cells), Langhans cells and histiocytes
can be seen.
Newer techniques, such as confocal microscopy, which
is useful in other papulosquamous disorders, may also be of value
in diagnosing LP (12).
Therapy of LP is aimed at controlling and
suppressing the disorder, as curative treatment is not documented
in the literature. This includes topical and oral steroids, topical
and oral calcineurin inhibitors, PUVA, metronidazole, itraconazole,
griseofulvin, hydroxychloroquine, dapsone and thalidomide (2,13). These
options are fraught with side effects, some of which are
potentially severe (13).
Complementary therapies have been tried for LP,
including traditional Chinese medicine and herbs, such as Aloe vera
(14). Some small studies have shown
Aloe vera to be more effective than triamcinolide for oral LP
(14).
Homeopathy is a complementary and alternative
therapeutic method begun by the German physician Samuel Hahnemann.
It utilizes infinitesimal quantities of medication to treat
disease, thus, side effects such as allergies or potential
teratogenicity are obviated.
A randomized controlled trial using the homeopathic
medicine Ignatia amara, which is obtained by making a very
high dilution of the plant, was carried out. The study group had 30
patients, with histopathologically confirmed erosive and/or
atrophic LP. The follow-up period was 4 months. The patients were
randomized to either placebo or Ignatia 30c. Mean lesion
size and pain scores were significantly in favour of homeopathic
treatment (15).
Homeopathic therapies are individualized, as
homeopaths believe that personal traits produce individualized
predispositions to disease. As a result, a homeopathic consultation
is often like a psychological consultation, with the aim being to
ascertain personality traits in the patient that can be matched by
the profile of the homeopathic medicine. It is this match, rather
than the physical pathology the patient presents with, that
determines what homeopathic medicine may be used in each case. The
homeopathic medicines used in these cases were of vegetable origin
(Lycopodium and Ignatia), chemical origin (Aurum
metallicum) and human origin (Carcinosinum). The
posology is determined by the intensity of the manifestation of the
disease and whether it is acute or chronic.
Psychosomatic dermatology supports this mode of
thinking and these psychosomatic skin disorders have been
classified in such a way as to ease discomfort of dermatologists,
via increased knowledge (16). This
mode of thinking appears to mirror and support the theory of
locus minoris resistentiae that has been posited in order to
explain the occurrence of cutaneous disorders in various locations
(17,18). Some of these disease locations have
included unilateral occurrence of rosacea, nasal spinulosis,
pityriasis folliculorum, unilateral blepharitis and endosymbiont
proliferation (19–25). Various side effects such as skin
atrophy, telangiectasia, acne, pustules, scaling, contact allergy,
weight gain, sleep disturbances and localized proliferation of
endosymbionts have been reported with conventional medications such
as corticosteroids (26–33), but not with homeopathic therapies.
Concerns regarding these side effects, including the carcinogenic
potential of drugs used also for their anti-inflammatory properties
have been raised and alternatives suggested (34–37).
Of note, nanomedicine has been associated with the
mode of action of homeopathy and recent research suggests that
homeopathic medicines may work by inducing the production of
nanomolecules, which may then influence physiopathologic processes
in the human body (38–40).
Although this case series is small (n=4), these
cases were generalized, recalcitrant cases of LP, often with
mucosal involvement. Dermatologists are aware that these are
characteristically difficult to treat in daily clinical,
dermatological practice. Thus, therapies that could potentially
place the patient in remission would always be welcome. Homeopathy
has been found to be useful in lichen striatus, psoriasis, atopic
dermatitis, acne, dermatitis herpetiformis, cutaneous T-cell
lymphoma, amongst others (41–47). It
is also a very cheap form of treatment, that is well tolerated by
all categories of patients and can be used in pregnancy, for which
there are many potential applications (48,49).
Complementary and alternative medical therapies, including plant
extracts have been used for the treatment of various diseases since
ancient times, even during periods of economic downturn and their
characteristics have been analysed in detail (50–60).
Informed consent obliges us to fully disclose all positive and
potential adverse effects of the therapies we propose to our
patients. This ethical approach means that patients sometimes
refuse to take the treatments offered to them for fear of adverse
reactions as well as in resistance to the use of animals in
biomedical research (61–63). This may cause them to turn to other
therapeutic systems for help, even without consulting their primary
physician thus, in order to properly educate our patients and
bridge this gap, research into the usefulness of complementary
therapies has been recommended (64,65).
Our results suggest that recalcitrant,
long-standing, generalized LP, with mucosal involvement may respond
to individualized homeopathy. Randomised controlled trials also
support the potential role of homeopathy in the therapy of LP
(11). Larger studies are needed to
confirm these assertions and these may finally clarify homeopathy's
place in LP therapy.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used during the present study are
available from the corresponding author upon reasonable
request.
Authors' contributions
LCN examined the test subjects and evaluated the
in vivo effects. MM performed the acquisition analysis and
interpretation of the data. ALT contributed to the writing of the
manuscript, as well as all revisions for intellectual content and
scientific quality. All authors contributed to the conception and
design of the study, as well as revising it. All authors read and
approved the final manuscript to be published and agreed to be
accountable for all aspects of the work in ensuring that questions
related to the accuracy or integrity of any part of the work are
appropriately investigated and resolved.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Cabinet Medical Individual (Bucharest, Romania), and a written
informed consent was provided by all the patients included in this
study.
Patient consent for publication
A written informed consent for the publication of
the images was provided by all the participants.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gorouhi F, Davari P and Fazel N: Cutaneous
and mucosal lichen planus: a comprehensive review of clinical
subtypes, risk factors, diagnosis, and prognosis.
ScientificWorldJournal. 2014:7428262014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Usatine RP and Tinitigan M: Diagnosis and
treatment of lichen planus. Am Fam Physician. 84:53–60.
2011.PubMed/NCBI
|
|
3
|
Narahari SR, Prasanna KS and Sushma KV:
Evidence-based integrative dermatology. Indian J Dermatol.
58:127–131. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Prasad R: Homoeopathy booming in India.
Lancet. 370:1679–1680. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dossett ML, Davis RB, Kaptchuk TJ and Yeh
GY: Homeopathy use by US adults: Results of a National Survey. Am J
Public Health. 106:743–745. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Alabi GO and Akinsanya JB: Lichen planus
in tropical Africa. Trop Geogr Med. 33:143–147. 1981.PubMed/NCBI
|
|
7
|
Bhattacharya M, Kaur I and Kumar B: Lichen
planus: A clinical and epidemiological study. J Dermatol.
27:576–582. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pannell RS, Fleming DM and Cross KW: The
incidence of molluscum contagiosum, scabies and lichen planus.
Epidemiol Infect. 133:985–991. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Brănișteanu DE, Pintilie A, Dimitriu A,
Cerbu A, Ciobanu D, Oanţă A and Tatu AL: Clinical, laboratory and
therapeutic profile of lichen planus. Rev Med Chir Soc Med Nat
Iasi. 121:25–32. 2017.
|
|
10
|
Brănişteanu DE, Pintilie A, Andreş LE,
Dimitriu A, Oanţă A, Stoleriu G and Brănişteanu DC: Ethiopatogenic
hypotheses in lichen planus. Rev Med Chir Soc Med Nat Iasi.
120:760–767. 2016.PubMed/NCBI
|
|
11
|
Brănişteanu DE, Brănişteanu DC, Stoleriu
G, Ferariu D, Voicu CM, Stoica LE, Căruntu C, Boda D,
Filip-Ciubotaru FM, Dimitriu A, et al: Histopathological and
clinical traps in lichen sclerosus: A case report. Rom J Morphol
Embryol. 57 (Suppl):817–823. 2016.PubMed/NCBI
|
|
12
|
Batani A, Brănișteanu DE, Ilie MA, Boda D,
Ianosi S, Ianosi G and Caruntu C: Assessment of dermal papillary
and microvascular parameters in psoriasis vulgaris using in
vivo reflectance confocal microscopy. Exp Ther Med.
15:1241–1246. 2018.PubMed/NCBI
|
|
13
|
Manousaridis I, Manousaridis K, Peitsch WK
and Schneider SW: Individualizing treatment and choice of
medication in lichen planus: A step by step approach. J Dtsch
Dermatol Ges. 11:981–991. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Reddy RL, Reddy RS, Ramesh T, Singh TR,
Swapna LA and Laxmi NV: Randomized trial of aloe vera gel vs
triamcinolone acetonide ointment in the treatment of oral lichen
planus. Quintessence Int. 43:793–800. 2012.PubMed/NCBI
|
|
15
|
Mousavi F, Sherafati S and Mojaver YN:
Ignatia in the treatment of oral lichen planus. Homeopathy.
98:40–44. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Nwabudike LC: Knowledge removes
discomfort. JAMA Dermatol. 154:738–739. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Happle R and Kluger N: Answer to Tatu AL,
Nwabudike LC: Koebner's sheep in Wolf's clothing - does the
isotopic response exist as a distinct phenomenon? J Eur Acad
Dermatol Venereol. 32:e336–337. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Nwabudike LC, Tatu AL, Gambichler T, et
al: Altered epigenetic pathways and cell cycle dysregulation in
healthy appearing skin of patients with koebnerized squamous cell
carcinomas following skin surgery. J Eur Acad Dermatol Venereol.
33:e3–e4. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tatu AL, Ionescu MA and Cristea VC:
Demodex folliculorum associated Bacillus pumilus in lesional areas
in rosacea. Indian J Dermatol Venereol Leprol. 83:610–611. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tatu AL, Clatici VG and Nwabudike LC:
Rosacea-like demodicosis (but not primary demodicosis) and
papulopustular rosacea may be two phenotypes of the same disease -
a microbioma, therapeutic and diagnostic tools perspective. J Eur
Acad Dermatol Venereol. 33:e46–e47. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tatu AL: Nasal Spinulosis. J Cutan Med
Surg. 21:3392017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tatu AL and Cristea VC: Pityriasis
folliculorum of the back thoracic area: Pityrosporum, keratin
plugs, or demodex involved? J Cutan Med Surg. 21:4412017.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tatu AL and Cristea VC: Unilateral
blepharitis with fine follicular scaling. J Cutan Med Surg.
21:4422017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tatu AL, Nwabudike LC, Kubiak K..et al:
Endosymbiosis and its significance in dermatology. J Eur Acad
Dermatol Venereol. 32:e346–e347. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tatu AL, Clatici V and Cristea V:
Isolation of Bacillus simplex strain from Demodex
folliculorum and observations about Demodicosis
spinulosa. Clin Exp Dermatol. 41:818–820. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tatu AL: Topical steroid induced facial
rosaceiform dermatitis. Acta Endocrinol (Buch). 12:232–233. 2016.
View Article : Google Scholar
|
|
27
|
Tatu AL and Clătici VG: Some correlations
between the clinical and dermoscopic features of steroid induced
facial dermatitis. J Am Acad Dermatol. 72 (Suppl):AB912015.
View Article : Google Scholar
|
|
28
|
Tatu AL, Ionescu MA, Clatici VG and
Cristea VC: Bacillus cereus strain isolated from Demodex
folliculorum in patients with topical steroid-induced
rosaceiform facial dermatitis. An Bras Dermatol. 91:676–678. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Tatu AL, Ionescu MA and Nwabudike LC:
Contact allergy to topical mometasone furoate confirmed by
rechallenge and patch test. Am J Ther. 25:e497–e498. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tatu AL and Nwabudike LC: The treatment
options of male genital Lichen sclerosus et atrophicus: Treatments
of genital Lichen sclerosus. In: Proceedings of the 14th National
Congress of Urogynecology and the National Conference of the
Romanian Association for the Study of Pain. Eforie; Romania: pp.
262–264. 2017
|
|
31
|
Tatu AL and Nwabudike LC: Male genital
lichen sclerosus - a permanent therapeutic challenge. J Am Acad
Dermatol. 79 (Suppl 1):AB1852018. View Article : Google Scholar
|
|
32
|
Tatu AL and Nwabudike LC: Bullous
reactions associated with COX-2 inhibitors. Am J Ther.
24:e477–e480. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gheorghe I, Tatu AL, Lupu I, Thamer O,
Cotar AI, Pircalabioru GG, Popa M, Cristea VC, Lazar V and
Chifiriuc MC: Molecular characterization of virulence and
resistance features in Staphylococcus aureus clinical
strains isolated from cutaneous lesions in patients with drug
adverse reactions. Rom Biotechnol Lett. 22:12321–12327. 2017.
|
|
34
|
Tatu AL and Nwabudike LC:
Metoprolol-associated onset of psoriatic arthropathy. Am J Ther.
24:e370–e371. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Nwabudike LC and Tatu AL: Response to -
chronic exposure to tetracyclines and subsequent diagnosis for
non-melanoma skin cancer in a large Mid-Western US population. J
Eur Acad Dermatol Venereol. 32:e1592018. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Tatu AL, Ciobotaru OR, Miulescu M, Buzia
OD, Elisei AM, Mardare N, Diaconu C, Robu S and Nwabudike LC:
Hydrochlorothiazide: Chemical structure, therapeutic, phototoxic
and carcinogenetic effects in dermatology. Revista de Chimie.
69:2110–2114. 2018.
|
|
37
|
Nwabudike LC, Elisei AM, Buzia OD,
Miulescu M and Tatu AL: Statins. A review on structural
perspectives, adverse reactions and relations with non-melanoma
skin cancer. Revista de Chimie. 69:2557–2562. 2018.
|
|
38
|
Montagnier L, Aïssa J, Ferris S,
Montagnier JL and Lavallée C: Electromagnetic signals are produced
by aqueous nanostructures derived from bacterial DNA sequences.
Interdiscip Sci. 1:81–90. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ion R and Boda D: Porphyrin-based
supramolecular nanotubes generated by aggregation processes.
Revista de Chimie. 59:205–207. 2008.
|
|
40
|
Chikramane PS, Suresh AK, Bellare JR and
Kane SG: Extreme homeopathic dilutions retain starting materials: A
nanoparticulate perspective. Homeopathy. 99:231–242. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Signore RJ: Treatment of lichen striatus
with homeopathic calcium carbonate. J Amer Ost College of Derm.
21:432011.
|
|
42
|
Nwabudike LC: Palmar and plantar psoriasis
and homeopathy Case reports. Our Dermatol Online. 8:66–69. 2017.
View Article : Google Scholar
|
|
43
|
Witt CM, Lüdtke R and Willich SN:
Homeopathic treatment of patients with psoriasis - a prospective
observational study with 2 years follow-up. J Eur Acad Dermatol
Venereol. 23:538–543. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Nwabudike LC: Atopic dermatitis and
homeopathy. Our Dermatol Online. 3:217–220. 2012. View Article : Google Scholar
|
|
45
|
Nwabudike LC: Case reports of acne and
homeopathy. Complement Med Res. 25:52–55. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Nwabudike LC: Homeopathy in the treatment
of dermatitis herpetiformis - a case presentation. Homeopathic
Links. 28:44–46. 2015. View Article : Google Scholar
|
|
47
|
Nwabudike LC: Cutaneous T-cell lymphoma
(Mycosis fungoides) treated by homeopathy: A 3-case report. J Am
Acad Dermatol. 76:AB922017. View Article : Google Scholar
|
|
48
|
Tatu AL: The skin and nevi pigmentation
during pregnancy. J Am Acad Dermatol. 66 (Suppl 1):AB 1482012.
|
|
49
|
Tatu AL: Melasma and pregnancy. Australas
J Dermatol. 53 (Suppl 2):372011.PubMed/NCBI
|
|
50
|
Tatu AL: Dermoscopic structural changes of
nevi during pregnancy related to location. J Am Acad Dermatol. 64
(Suppl 1):AB752011.
|
|
51
|
Tatu AL: Skin tags and pregnancy.
Australas J Dermatol. 51 (Suppl 1):A48–A50. 2010.
|
|
52
|
Buzia OD, Fasie V, Mardare N, Diaconu C,
Gurau G and Tatu AL: Formulation, preparation, physico-chimical
analysis, microbiological peculiarities and therapeutic challenges
of extractive solution of Kombucha. Revista de Chimie. 69:720–724.
2018.
|
|
53
|
Zălaru C, Crişan C, Călinescu I, Moldovan
Z, Ţârcomnicu I, Litescu S, Tatia R, Moldovan L, Boda D and Iovu M:
Polyphenols in Coreopsis tinctoria Nutt. fruits and the
plant extracts antioxidant capacity evaluation. Open Chem.
12:858–867. 2014.
|
|
54
|
Mihăilă B, Dinică RM, Tatu AL and Buzia
OD: New insights in vitiligo treatments using bioactive compounds
from Piper nigrum. Exp Ther Med. 15:1241–1246.
2018.PubMed/NCBI
|
|
55
|
Buzia OD, Mardare N, Florea A, Diaconu C,
Dinica RM and Tatu AL: Formulation and preparation of
pharmaceuticals with anti-rheumatic effect using the active
principles of capsicum annuum and piper nigrum. Revista de Chimie.
69:2854–2857. 2018.
|
|
56
|
Tatu AL and Ionescu MA: Multiple
autoimmune syndrome type III - thyroiditis, vitiligo and alopecia
areata. Acta Endocrinol (Buch). 13:124–125. 2017. View Article : Google Scholar
|
|
57
|
Nwabudike LC and Tatu AL: Magistral
prescription with silver nitrate and Peru balsam in difficult to
heal diabetic foot ulcers. Am J Ther. 25:e679–e680. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Ionescu C, Țârcomnicu I, Ionescu MA,
Nicolescu TO, Boda D and Nicolescu F: Identification and
characterization of the methanolic extract of hellebrigenin
3-acetate from helleborirhizomes. Mass spectrometry. Revista de
Chimie. 1:972–975. 2014.
|
|
59
|
Boda D and Ion R-M: Synthesis, spectral
and photodynamic properties of lithium phthalocyanine. Revista de
Chimie. 65:1271–1274. 2014.
|
|
60
|
Raţiu MP, Purcărea I, Popa F, Purcărea VL,
Purcărea TV, Lupuleasa D and Boda D: Escaping the economic turn
down through performing employees, creative leaders and growth
driver capabilities in the Romanian pharmaceutical industry.
Farmacia. 59:119–130. 2011.
|
|
61
|
Robu S, Chesaru BI, Diaconu C, Dumitriu
BO, Tutunaru D, Stanescu U and Lisa EL: Lavandulahybrida:
Microscopic characterization and the evaluation of the essential
oil. Farmacia. 64:914–917. 2016.
|
|
62
|
Rogozea LM, Diaconescu DE, Dinu EA, Badea
O, Popa D, Andreescu O and Leaşu FG: Bioethical dilemmas in using
animal in medical research. Challenges and opportunities. Rom J
Morphol Embryol. 56:1227–1231. 2015.PubMed/NCBI
|
|
63
|
Purcaru D, Preda A, Popa D, Moga MA and
Rogozea L: Informed consent: How much awareness is there? PLoS One.
9:e1101392014. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Jou J and Johnson PJ: Nondisclosure of
complementary and alternative medicine use to primary care
physicians: Findings from the 2012 national health interview
survey. JAMA Intern Med. 176:545–546. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Nwabudike LC: Pustular eruption
(iododerma?) in a patient with cancer treated with complementary
and alternative medicine. JAMA Dermatol. 154:495–496. 2018.
View Article : Google Scholar : PubMed/NCBI
|