Introduction
Bronchiolitis, a common lower respiratory tract
infection in infants, is the primary reason of hospitalization of
infants in developed and developing countries (1). This disease is characterized by
wheezing, cough and tachypnea. Cases mostly present among the
infants aged 1–6 months. It usually occurs in early spring and
winter seasons (2).
It is estimated that 1 in 5 infants each year
suffers respiratory infection caused by respiratory syncytial virus
(RSV) (3). The mortality rate is
0.5–1.5% among hospitalized infants, but increases to 3–4% for
infants with potential pulmonary or cardiac diseases (4). This is a frustrating condition for
physicians managing bronchiolitis, as most cases are not responsive
to treatment (5). At present,
treatment for this disease is primarily supportive with the
administration of bronchodilators (6,7),
steroids (8,9) and antibiotics (10), which show little benefit.
It has been established that 3% hypertonic solution
(3% HS) solution absorbs water from the submucosa, subsequently
resolving edema and thereby improving mucociliary function
(11). Data from in vitro and
in vivo experiments have indicated that HS accelerates the
transport rates of mucus (12,13). It
has been demonstrated that inhalation of nebulized 3% HS may
improve immediate and long-term clearance of small airways in
infants with bronchiolitis (14–16).
However, the functional mechanism remains unknown. HS has been
suggested to facilitate the removal of inspissated mucus,
disruption of mucus strand and reduction of mucosal edema (17,18). HS
is usually administered with a bronchodilator to decrease the risk
of bronchospasm caused by HS (19).
Certain studies have suggested that nebulized 3% HS is useful for
infants with bronchiolitis (14,20–24);
however, certain studies have reported no beneficial efficacy of HS
in bronchiolitis (25–27).
The present meta-analysis was performed to
provideadditional insight on this topic. A total of 23 eligible
articles were selected. Duration of hospitalization, clinical
severity score (CSS) and re-admission rates were analyzed to
determine the efficacy of 3% HS compared with NS. The results
provided information regarding the clinical application of 3% HS in
bronchiolitis.
Materials and methods
Search strategy
Articles were accessed using the Pubmed (from 1966
to March 2018; http://www.ncbi.nlm.nih.gov/PubMed) and MEDLINE (from
1966 to March 2018; http://wwwcf.nlm.nih.gov/serials/journals/index.cfm)
databases. The Cochrane Central Register of Controlled Trials
(CENTRAL; http://www.cochranelibrary.com/central) was also used.
The following terms were used: ‘Bronchiolitis’ OR ‘respiratory
syncytial virus’ OR ‘RSV’ OR ‘acute wheezing’ AND ‘3% saline’. The
search focused on human studies and had no language restrictions.
Concurrently, additional articles were obtained via references of
obtained reviews.
Inclusion criteria
The included studies were selected based on the
following criteria: i) The studies were designed as randomized
controlled trials (RCTs); ii) the studies investigated the efficacy
of 3% HS in bronchiolitis; iii) they included a comparison in
efficacy between 3% HS and normal saline (NS; 0.9% saline) was
performed; and iv) they examined length of stay, CSS score, or
re-admission rates.
Data extraction
A total of 2 independent authors reviewed all
obtained articles, scanned the full texts, selected eligible
articles according to the inclusion criteria and carefully
extracted the data. Baseline characteristics of the included trials
were identified, including name of first author, publication year,
number of patients in each group, the drugs used and their doses.
The primary outcomes were the re-admission rates, duration of
hospital stay and the CSS score.
Statistical analysis
All statistical analyses were completed with State
12.0 software (Stata Corp LLC, College Station, TX, USA). The
weighted mean difference (WMD) with 95% confidence interval (95%
CI) was used to pool continuous data of length of stay. Standard
mean difference (SMD) with 95% CI was used to pool data of CSS
score. Relative risk (RR) with 95% CI was calculated to examine the
association between 3% HS and re-admission. Heterogeneity was
evaluated by I2 and P-values. The potential publication
bias was assessed with the Begg's funnel plot method and Egger's
regression quality of included studies was evaluated according to
the modified Jadad scale score (28). P<0.05 was considered to indicate a
statistically significant difference.
Results
Literature search and study
selection
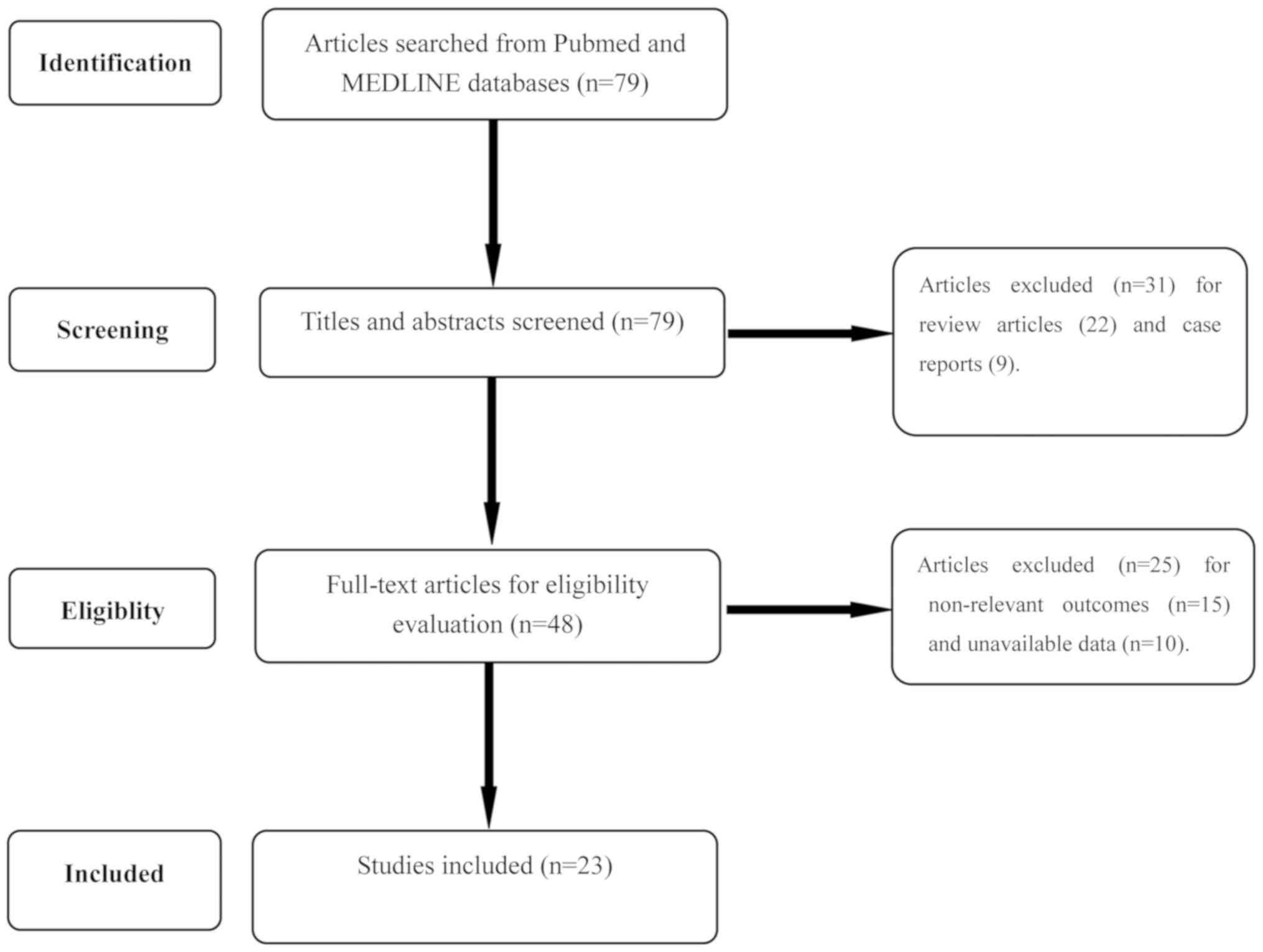
A total of 79 relevant articles were identified from
Pubmed and MEDLINE databases. CENTRAL was also used. Of these, 31
articles were excluded, as they were review articles (n=22) or case
reports (n=9). Then, the full-texts of the 48 remaining articles
were extracted and examined carefully. A total of 15 articles
revealed non-relevant outcomes and 10 articles provided no
available data; therefore, 23 articles were included. The detailed
selection process is demonstrated in Fig. 1. Information concerning the study
population, the intervention type, HS dosage, additional medication
and outcomes of each study are summarized in Table I. All 23 studies were double-blinded
RCTs (14,15,20–25,27,29–42).
Jadad scores of each study are presented in Table II.
 | Table I.Basic information of included
studies. |
Table I.
Basic information of included
studies.
| First author | Year | N (Intervention vs.
control) | HS dosage, % | Addition | Outcomes | (Refs.) |
|---|
| Gupta | 2016 | 33 vs. 33 | 3 vs. 0.9 | Salbutamol | LOS, CSS | (29) |
| Silver | 2015 | 111 vs. 111 | 3 vs. 0.9 | – | LOS,
Re-admission | (30) |
| Ojha | 2014 | 12 vs. 9 | 3 vs. 0.9 | – | LOS, CSS | (31) |
| Flores | 2016 | 33 vs. 35 | 3 vs. 0.9 | Salbutamol | LOS, CSS | (32) |
| Angoulvan | 2017 | 385 vs. 387 | 3 vs. 0.9 | – | LOS | (33) |
| Mandelberg | 2003 | 27 vs. 25 | 3 vs. 0.9 | Epinephrine | LOS, CSS | (20) |
| Tal | 2006 | 21 vs. 20 | 3 vs. 0.9 | Epinephrine | LOS | (21) |
| Kuzik | 2007 | 47 vs. 49 | 3 vs. 0.9 | – | LOS | (14) |
| Miraglia Del
Giudice | 2012 | 52 vs. 54 | 3 vs. 0.9 | Epinephrine | LOS, CSS | (24) |
| Al-Ansari | 2010 | 58 vs. 56 | 3 vs. 0.9 | Epinephrine | LOS,
Re-admission | (34) |
| Luo | 2011 | 57 vs. 55 | 3 vs. 0.9 | – | LOS, CSS | (22) |
| Sharma | 2013 | 125 vs. 123 | 3 vs. 0.9 | B2 agonist | LOS | (27) |
| Teunissen | 2014 | 84 vs. 80 | 3 vs. 0.9 | B2 agonist | LOS | (35) |
| Pandit | 2013 | 51 vs. 49 | 3 vs. 0.9 | Epinephrine | LOS | (36) |
| Everard | 2014 | 142 vs. 149 | 3 vs. 0.9 | – | LOS,
Re-admission | (37) |
| Mahesh Kumar | 2013 | 20 vs. 20 | 3 vs. 0.9 | B2 agonist | LOS | (38) |
| Luo | 2010 | 50 vs. 43 | 3 vs. 0.9 | B2 agonist | LOS, CSS | (23) |
| Wu | 2014 | 211 vs. 197 | 3 vs. 0.9 | – | LOS | (25) |
| Espelt | 2012 | 37 vs. 45 | 3 vs. 0.9 | B2 agonist | LOS | (41) |
| Sarrell | 2002 | 33 vs. 32 | 3 vs. 0.9 | Terbutaline | CSS | (15) |
| Grewal | 2009 | 23 vs. 23 | 3 vs. 0.9 | Epinephrine | Re-admission | (39) |
| Anil | 2010 | 75 vs. 74 | 3 vs. 0.9 | Epinephrine | Re-admission | (40) |
| Köse | 2016 | 35 vs. 35 | 3 vs. 0.9 | Salbutamol | CSS | (42) |
| Table II.Jadad score of each included
study. |
Table II.
Jadad score of each included
study.
|
| Study
characteristics |
|---|
|
|
|
|---|
| First author,
year | Generation of
allocation sequence | Allocation
concealment | Blindness | Withdrawal and
drop-out | Jadad score | (Refs.) |
|---|
| Gupta, 2016 | 1 | 0 | 0 | 0 | 1 | (29) |
| Silver, 2015 | 2 | 2 | 2 | 1 | 7 | (30) |
| Ojha, 2014 | 2 | 2 | 2 | 1 | 7 | (31) |
| Flores, 2016 | 2 | 2 | 2 | 1 | 7 | (32) |
| Angoulvan,
2017 | 2 | 2 | 2 | 1 | 7 | (33) |
| Mandelberg,
2003 | 1 | 0 | 1 | 1 | 3 | (20) |
| Tal, 2006 | 1 | 0 | 1 | 1 | 3 | (21) |
| Kuzik, 2007 | 2 | 2 | 2 | 1 | 7 | (14) |
| Giudice, 2012 | 2 | 2 | 2 | 0 | 6 | (24) |
| Al-Ansari,
2010 | 2 | 2 | 2 | 1 | 7 | (34) |
| Luo, 2011 | 2 | 2 | 2 | 1 | 7 | (22) |
| Sharma, 2013 | 2 | 2 | 2 | 1 | 7 | (27) |
| Teunissen,
2014 | 2 | 1 | 2 | 1 | 6 | (35) |
| Pandit, 2013 | 2 | 2 | 0 | 1 | 5 | (36) |
| Everard, 2014 | 2 | 2 | 2 | 1 | 7 | (37) |
| Mahesh Kumar,
2013 | 2 | 1 | 0 | 1 | 3 | (38) |
| Luo, 2010 | 1 | 2 | 2 | 1 | 6 | (23) |
| Wu, 2014 | 2 | 2 | 1 | 1 | 6 | (25) |
| Espelt, 2012 | 2 | 2 | 2 | 1 | 7 | (41) |
| Sarrell, 2002 | 1 | 0 | 1 | 0 | 2 | (15) |
| Grewal, 2009 | 2 | 2 | 2 | 1 | 7 | (39) |
| Anil, 2010 | 2 | 2 | 2 | 1 | 7 | (40) |
| Köse, 2016 | 1 | 0 | 1 | 1 | 3 | (42) |
Effects on the length of stay
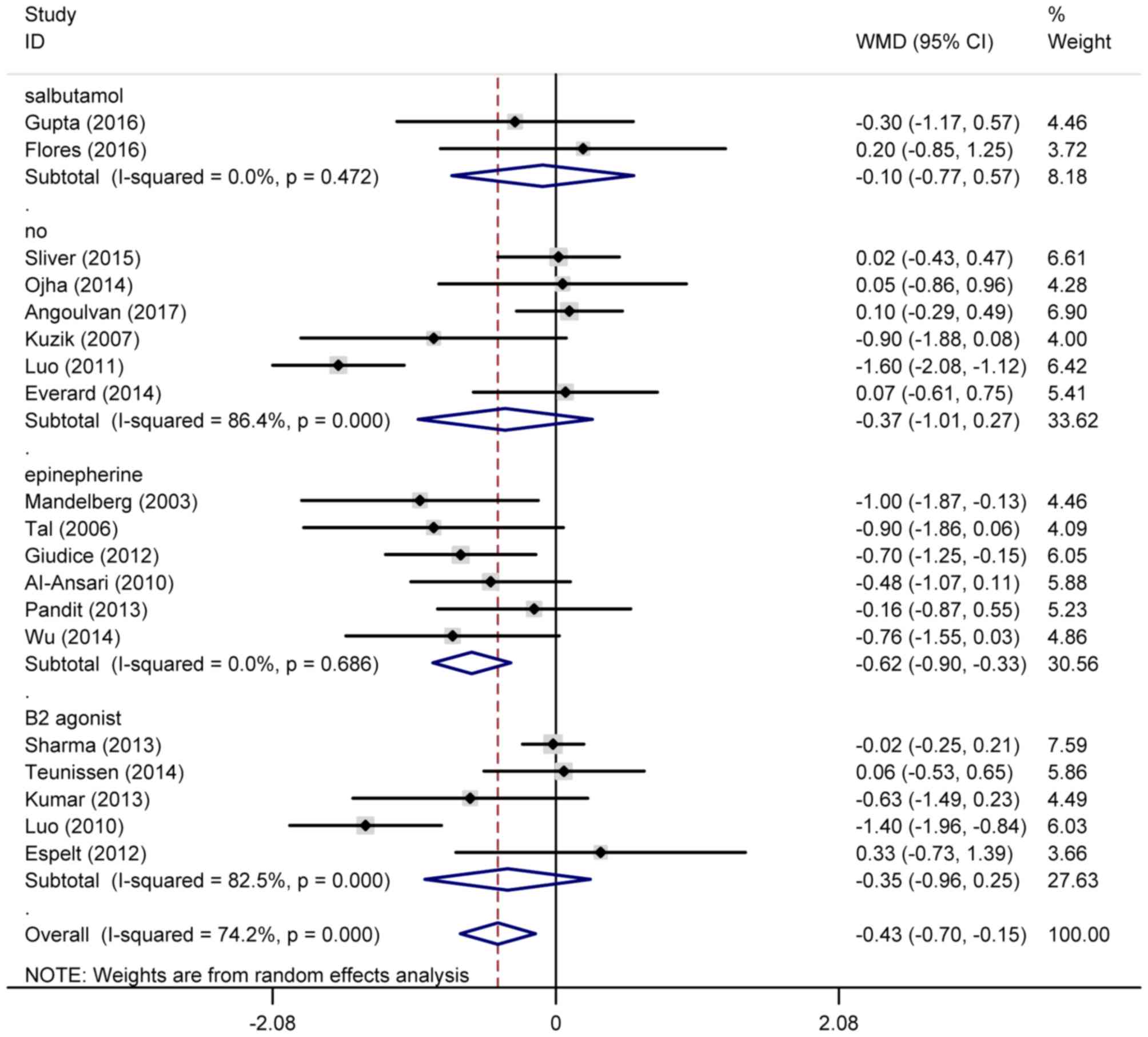
A total of 14RCTs were included to analyze the
duration of hospitalization (Fig.
2). The pooled data revealed that infants treated with HS
nebulizers exhibited shorter periods of hospitalization compared
with those treated by NS nebulizers (WMD=−0.43; 95% CI=−0.70,
−0.15). Subgroup analysis of additional medications demonstrated
that HS nebulizer with epinephrine may significantly decrease the
length of hospital stay, with a WMD=−0.62 (95% CI=−0.90,
−0.33).
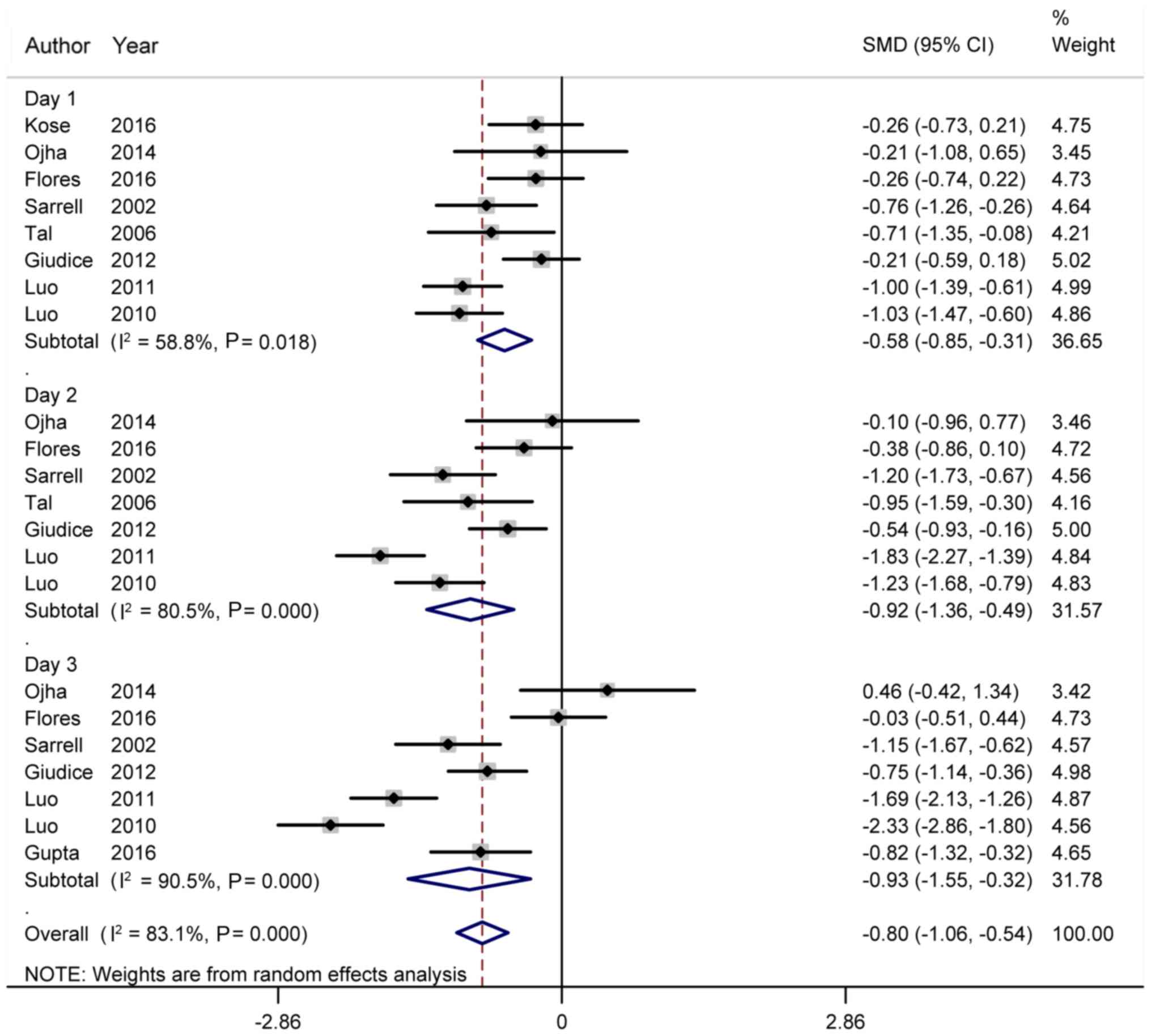
Effects on CSS score
A total of 8RCTs provided data of CSS scores on the
first day of treatment (Fig. 3).
Compared with the NS nebulizer, HS nebulizers significantly
decreased CSS scores on the first day of treatment (SMD=−0.58; 95%
CI=−0.85, −0.31). Then, 7RCTs provided data of CSS scores on the
second day of treatment. The results demonstrated that there was
statistically significant difference in CSS scores between HS and
NS nebulizers on the second day (SMD=−0.92; 95% CI=−1.36, −0.49). A
total of 7RCTs provided data of CSS scores on the third day of
treatment. The pooled results indicated a lower CSS score in the 3%
HS group compared with the control group (SMD=−0.93; 95% CI=−1.55,
−0.32).
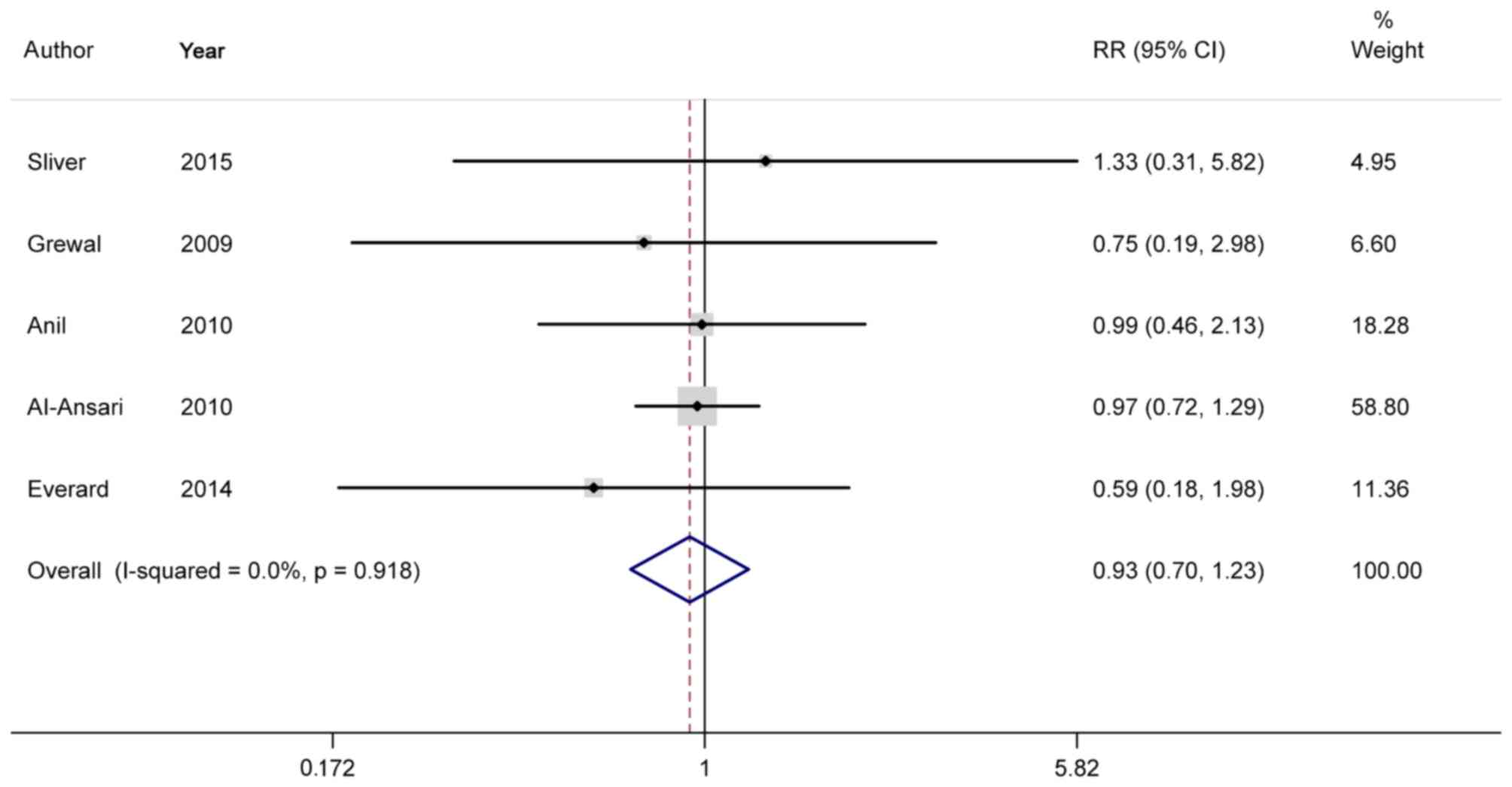
Effects on re-admission
A total of 5RCTs analyzed the effects of HS
nebulizers on the re-admission rate. The pooled outcome indicated a
beneficial effect of HS nebulizers on decreasing re-admission rate
compared with NS nebulizers (RR=0.93; 95% CI=0.70, 1.23; Fig. 4).
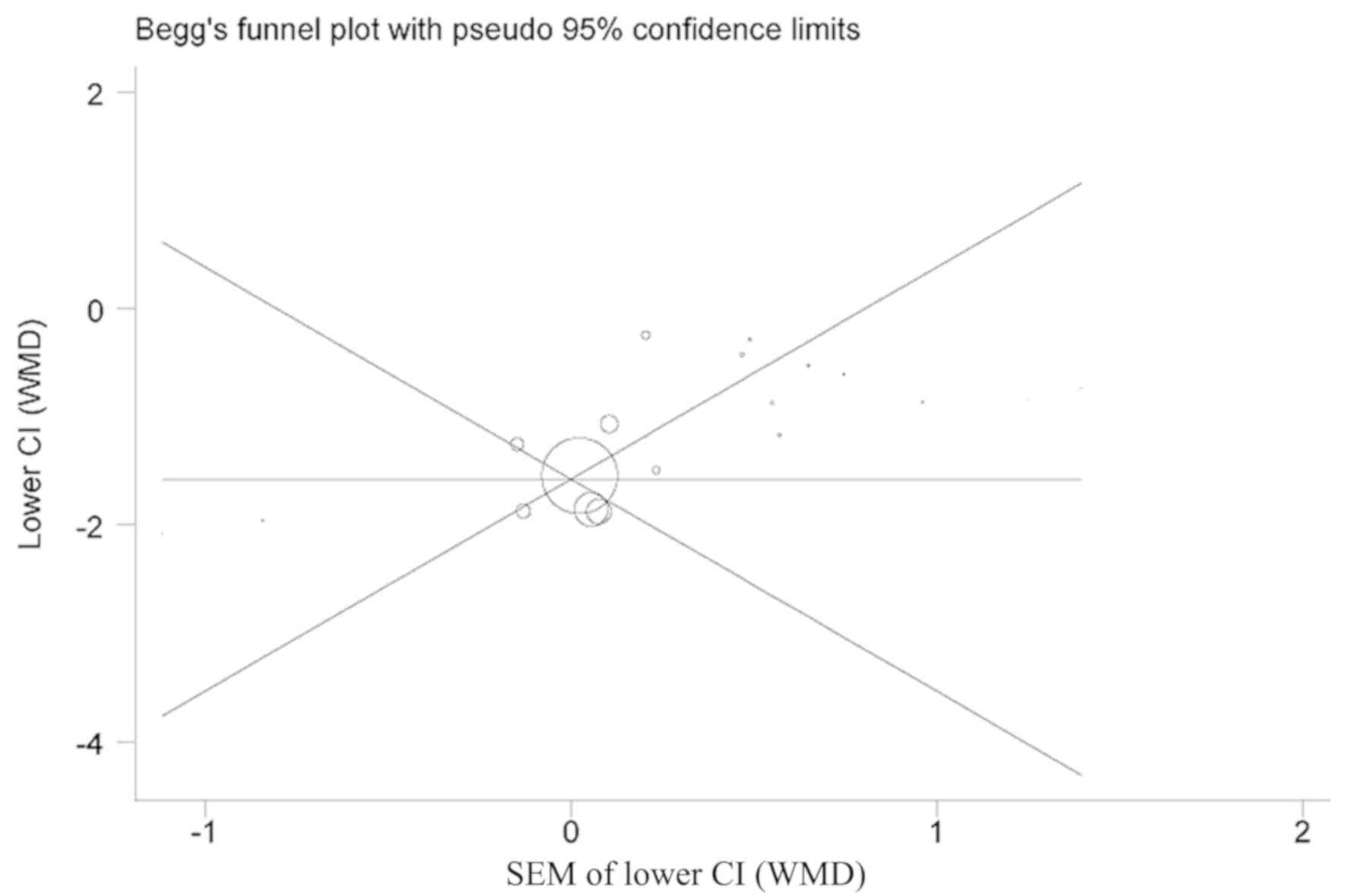
Sensitivity analysis and publication
bias
A sensitivity analysis was performed to evaluate the
effects of the methodological quality of each trial on the pooled
results. The results indicated that the pooled results were robust.
The funnel plot appeared to be symmetric and no potential
publication bias was observed (Fig.
5; Begg's, P=0.133; Egger's, P=0.576, hospital stay).
Discussion
Bronchiolitis is one of the most common lower
respiratory tract infections in infants (43,44). The
pathophysiology of bronchiolitis is different from that of asthma.
It involves infection of the bronchiolar epithelium, characterized
by the sloughing and necrosis of epithelial cells, edema,
peribronchiolar mononuclear infiltration and secretion of mucus.
These changes result in the obstruction of flow in the small and
large airways, causing hyperinflation, wheezing and atelectasis
(45,46).
Antiviral agents are available for bronchiolitis;
however, they are not routinely prescribed due to unconfirmed
efficacy. Ribavirin is the only specific drug used to treat RSV
infection; however, its efficacy was not been significant (47–50).
Studies using glucocorticoids to treat bronchiolitis demonstrated
negative effects (51,52). In addition, the application of
β2-agonists may confer short-term improvement in infants
with bronchiolitis, in particular the application of epinephrine
(53–55). However, no significant effects have
been observed in other types of β2-agonists (46,56).
Previous studies have demonstrated that inhaled HS
is a promising therapy (24,26). As stated previously, RSV infection
results in edema, necrosis and sloughing of the respiratory
epithelium, causing obstruction of the small and large airways. HS
may decrease the edema extent of airways through drawing fluid from
adventitial and submucosal spaces. This increased fluid may
contribute to a loosening of inspissated mucous and improvement of
mucociliary clearance. The patients with bronchiectasis
demonstrated a significant increase in weight of expectorated
sputum and decrease in sputum viscosity (57,58).
Concurrently, it has been suggested that nasal HS may alleviate the
symptoms of chronic rhinosinusitis. Previously, certain studies
revealed the benefit of HS in decreasing respiratory distress
(15,20,34,59) and
length of stay (21,22–24)
among infants with bronchiolitis.
However, there are inconsistent data concerning the
efficacy of 3% HS in bronchiolitis. The study by Teunissen et
al (35) demonstrated that 3% HS
was safe for bronchiolitis; however, it did not decrease the length
of stay orduration of supplemental oxygen required in infant
hospitalization due to bronchiolitis. Sharma et al (27) revealed that the CSS in 3 and 0.9%
saline groups were not significantly different. The mean length of
hospital stay was 63.93±22.43 h in the 3% saline group and
63.51±21.27 h in 0.9% saline group (P=0.878). Therefore, nebulized
3% HS was not superior to 0.9% saline in infants with diagnosed
bronchiolitis. Pandit et al (36) reached a similar conclusion:
Nebulization with HS + adrenaline and normal saline +adrenaline
were equally effective in the treatment of bronchiolitis in
infants. Our analysis, based on 23 studies, demonstrated that 3% HS
was more effective compared with 0.9% NS in decreasing the length
of hospitalization, CSS score and rate of re-admission. Compared
with individual articles, the pooled results were much more
credible.
However, there were limitations in the present
study. Firstly, significant heterogeneity was observed in the
analysis of length of stay. Although subgroup analysis of
supplemental medication was performed, heterogeneity was observed
in subgroup analysis of β2 agonists (P<0.001) and 3%
HS-only treatment (P<0.001). This may be due to the differences
in patient characteristics, severity of bronchiolitis and
performance of individual physicians. Secondly, only 3% HS was
analyzed and other concentrations of HS were not considered;
comprehensive analysis should therefore be preformed to confirm the
efficacy of HS.
In conclusion, 3% HS is superior to normal saline
(0.9% saline) in decreasing length of stay, CSS score and rate of
re-admission in cases of infant bronchiolitis.
Acknowledgements
The authors would like to thank the authors of the
original studies included in this meta-analysis.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
ZYW designed the study. ZYW and XDL screened the
literature. ZYW and ALS extracted the data from the literature. ZYW
and XQF conducted the meta-analysis and wrote the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Klassen TP: Recent advances in the
treatment of bronchiolitis and laryngitis. Pediatr Clin North Am.
44:249–261. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kabra SK and Ghai OP: Respiratory
disorders. In: Ghai Essentials Pediatrics. 6th edition. CBS
Publishers and Distributors; New Delhi: pp. 352–354. 2004
|
|
3
|
Hall CB, Weinberg GA, Iwane MK, Blumkin
AK, Edwards KM, Staat MA, Auinger P, Griffin MR, Poehling KA,
Erdman D, et al: The burden of respiratory syncytial virus
infection in young children. N Engl J Med. 360:588–598. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dennis MM: Bonchiolitis. Arch Dis Child
Educ Pract. 90:81–86. 2005.
|
|
5
|
Mathew JL: Hypertonic saline nebulization
for bronchiolitis. Indian Pediatr. 45:987–989. 2008.PubMed/NCBI
|
|
6
|
Gadomski AM and Scribani MB:
Bronchodilators for bronchiolitis. Cochrane Database Syst Rev.
6:CD0012662014.
|
|
7
|
Skjerven HO, Hunderi JO, Brügmann-Pieper
SK, Brun AC, Engen H, Eskedal L, Haavaldsen M, Kvenshagen B, Lunde
J, Rolfsjord LB, et al: Racemic adrenaline and inhalation
strategies in acute bronchiolitis. N Engl J Med. 368:2286–2293.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Farley R, Spurling GK, Eriksson L and Del
Mar CB: Antibiotics for bronchiolitis in children under two years
of age. Cochrane Database Syst Rev. 10:CD0051892014.
|
|
9
|
Hartling L, Fernandes RM, Bialy L, Milne
A, Johnson D, Plint A, Klassen TP and Vandermeer B: Steroids and
bronchodilators for acute bronchiolitis in the first two years of
life: Systematic review and meta-analysis. BMJ. 342:d17142011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fernandes RM and Hartling L:
Glucocorticoids for acute viralbronchiolitis in infants and young
children. JAMA. 311:87–88. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wabnitz DA and Wormald PJ: A blind,
randomized, controlled study on the effect of buffered 0.9 and 3%
sodium chloride intranasal sprays on ciliary beat frequency.
Laryngoscope. 115:803–805. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wills PJ, Hall RL, Chan W and Cole PJ:
Sodium chloride increases the ciliary transportability of cystic
fibrosis and bronchiectasis sputum on the mucusdepleted bovine
trachea. J Clin Invest. 99:9–13. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sood N, Bennett WD, Zeman K, Brown J, Foy
C, Boucher RC and Knowles MR: Increasing concentration of inhaled
saline with or without amiloride: Effect on mucociliary clearence
in normal subjects. Am J Respir Crit Care Med. 167:158–163. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kuzik BA, Al-Qadhi SA, Kent S, Flavin MP,
Hopman W, Hotte S and Gander S: Nebulized hypertonic saline in the
treatment of viral bronchiolitis in infants. J Pediatr.
151:266–270, 270.e1. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sarrell EM, Tal G, Witzling M, Someck E,
Houri S, Cohen HA and Mandelberg A: Nebulized 3% hypertonic saline
solution treatment in ambulatory children with viral bronchiolitis
decreases symptoms. Chest. 122:2015–2020. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang L, Mendoza-Sassi RA, Wainwright C
and Klassen TP: Nebulized hypertonic saline solution for acute
bronchiolitis in infants. Cochrane Database Syst Rev.
4:CD0064582008.
|
|
17
|
Robinson M, Hemming AL, Regnis JA, Wong
AG, Bailey DL, Bautovich GJ, King M and Bye PT: Effect of
increasing doses of hypertonic saline on mucociliary clearance in
patients with cystic fibrosis. Thorax. 52:900–903. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tomooka LT, Murphy C and Davidson TM:
Clinical study and literature review of nasal irrigation.
Laryngoscope. 110:1189–1193. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Delvaux M, Henket M, Lau L, Kange P,
Bartsch P, Djukanovic R and Louis R: Nebulised salbutamol
administered during sputum induction improves bronchoprotection in
patients with asthma. Thorax. 59:111–116. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mandelberg A, Tal G, Witzling M, Someck E,
Houri S, Balin A and Priel IE: Nebulized 3% hypertonic saline
solution treatment in hospitalized infants with viral
bronchiolitis. Chest. 123:484–487. 2003. View Article : Google Scholar
|
|
21
|
Tal G, Cesar K, Oron A, Houri S, Ballin A
and Mandelberg A: Hypertonic saline epinephrine treatment in
hospitalized infants with viral bronchiolitis reduces
hospitalization stay: 2 years experience. Isr Med Assoc J.
8:169–173. 2006.PubMed/NCBI
|
|
22
|
Luo Z, Fu Z, Liu E, Xu X, Fu X, Peng D,
Liu Y, Li S, Zeng F and Yang X: Nebulized hypertonic saline
treatment in hospitalized children with moderate to severe viral
bronchiolitis. Clin Microbiol Infect. 17:1829–1833. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Luo Z, Liu E, Luo J, Li S, Zeng F, Yang X
and Fu Z: Nebulized hypertonic saline/salbutamol solution treatment
in hospitalized children with mild to moderate bronchiolitis.
Pediatr Int. 52:199–202. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Miraglia Del Giudice M, Saitta F, Leonardi
S, Capasso M, Niglio B, Chinellato I, Decimo F, Maiello N, Capristo
C, Perrone L and Peroni D: Effectiveness of nebulized hypertonic
saline and epinephrine in hospitalized infants with bronchiolitis.
Int J Immunopathol Pharmacol. 25:485–491. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wu S, Baker C, Lang ME, Schrager SM, Liley
FF, Papa C, Mira V, Balkian A and Mason WH: Nebulized hypertonic
saline for bronchiolitis: A randomized clinical trial. JAMA
Pediatr. 168:657–663. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Florin TA, Shaw KN, Kittick M, Yakscoe S
and Zorc JJ: Nebulized hypertonic saline for bronchiolitis in the
emergency department: A randomized clinical trial. JAMA Pediatr.
168:664–670. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sharma BS, Gupta MK and Rafik SP:
Hypertonic (3%) saline vs. 0.93% saline nebulization for acute
viral bronchiolitis: A randomized controlled trial. Indian Pediatr.
50:743–747. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhang Y, Ding S, Li C, Wang Y, Chen Z and
Wang Z: Effects of N-acetylcysteine treatment in acute respiratory
distress syndrome: A meta-analysis. Exp Ther Med. 14:2863–2868.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gupta HV, Gupta VV, Kaur G, Baidwan AS,
George PP, Shah JC, Shinde K, Malik R, Chitkara N and Bajaj KV:
Effectiveness of 3% hypertonic saline nebulization in acute
bronchiolitis among Indian children: A quasiexperimental study.
Perspect Clin Res. 7:88–93. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Silver AH, Esteban-Cruciani N, Azzarone G,
Douglas LC, Lee DS, Liewehr S, Nazif JM, Agalliu I, Villegas S,
Rhim HJ, et al: 3% hypertonic saline versus normal saline in
inpatient bronchiolitis: A randomized controlled trial. Pediatrics.
136:1036–1043. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ojha AR, Mathema S, Sah S and Aryal UR: A
comparative study on use of 3% saline versus 0.9% saline
nebulization in children with bronchiolitis. J Nepal Health Res
Counc. 12:39–43. 2014.PubMed/NCBI
|
|
32
|
Flores P, Mendes AL and Neto AS: A
randomized trial of nebulized 3% hypertonic saline with salbutamol
in the treatment of acute bronchiolitis in hospitalized infants.
Pediatr Pulmonol. 51:418–425. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Angoulvant F, Bellêttre X, Milcent K,
Teglas JP, Claudet I, Le Guen CG, de Pontual L, Minodier P, Dubos
F, Brouard J, et al: Effect of nebulized hypertonic saline
treatment in emergency departments on the hospitalization rate for
acute bronchiolitis: A randomized clinical trial. JAMA Pediatr.
171:e1713332017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Al-Ansari K, Sakran M, Davidson BL, El
Sayyed R, Mahjoub H and Ibrahim K: Nebulized 5 or 3% hypertonic or
0.9% saline for treating acute bronchiolitis in infants. J Pediatr.
157:630–634, 634.e1. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Teunissen J, Hochs AH, Vaessen-Verberne A,
Boehmer AL, Smeets CC, Brackel H, van Gent R, Wesseling J,
Logtens-Stevens D, de Moor R, et al: The effect of 3 and 6%
hypertonic saline in viral bronchiolitis: A randomised controlled
trial. Eur Respir J. 44:913–921. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Pandit S, Dhawana N and Thakur D: Utility
of hypertonic saline in the management of acute bronchiolitis in
infants: A randomised controlled study. Int J Clin Pediatr.
2:24–29. 2013.
|
|
37
|
Everard ML, Hind D, Ugonna K, Freeman J,
Bradburn M, Cooper CL, Cross E, Maguire C, Cantrill H, Alexander J
and McNamara PS: SABRE: A multicentrerandomised control trial of
nebulised hypertonic saline in infants hospitalised with acute
bronchiolitis. Thorax. 69:1105–1112. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Mahesh Kumar KB, Karunakara BP, Manjunath
MN and Mallikarjuna HB: Aerosolised hypertonic saline in
hospitalized young children with acute bronchiolitis: A randomized
controlled clinical trial. J Pediatr Sci. 5:e1742013.
|
|
39
|
Grewal S, Ali S, McConnell DW, Vandermeer
B and Klassen TP: A randomized trial of nebulized 3% hypertonic
saline with epinephrine in the treatment of acute bronchiolitis in
the emergency department. Arch Pediatr Adolesc Med. 163:1007–1012.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Anil AB, Anil M, Saglam AB, Cetin N, Bal A
and Aksu N: High volume normal saline alone is as effective as
nebulized salbutamol-normal saline, epinephrine-normal saline, and
3% saline in mild bronchiolitis. Pediatr Pulmonol. 45:41–47. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Espelt MI; Hospital General de Niños Pedro
de Elizalde, : Efficacy of nebulized hypertonic saline in the
treatment of acute bronchiolitis (Hypertonic). ClinicalTrials.gov
Identifier: NCT01238848. http://www.clinicaltrials.gov/ct2/show/NCT01238848?term=espelt+bronchiolitis&rank=1November
11–2010
|
|
42
|
Köse S, Şehriyaroğlu A, Esen F, Özdemir A,
Kardaş Z, Altuğ U, Karakuş E, Özcan A, Kısaarslan AF, Elmalı F, et
al: Comparing the efficacy of 7, 3 and 0.9% saline in moderate to
severe bronchiolitis in infants. Balkan Med J. 33:193–197. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Coffen SE: Bronchiolitis: Inpatient focus.
Pediatr Clin North Am. 52:1047–1057. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Hall CB: Respiratory syncytial virus. In:
Textbook of Pediatric Infectious Diseases. 3rd. Philadelphia;
Saunders: pp. pp1633–1656. 1991
|
|
45
|
Hall CB: Respiratory syncytial virus and
parainfluenza virus. N Engl J Med. 344:1917–1928. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Darville T and Yamauchi T: Respiratory
syncytial virus. Pediatr Rev. 19:55–61. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Meert KL, Sarnaik AP, Gelmini MJ and
Lieh-Lai MW: Aerosolized ribavirin in mechanically ventilated
children with respiratory syncytial virus lower respiratory tract
disease: A prospective double-blind, randomized trial. Crit Care
Med. 22:566–572. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Moler FW, Steinhart CM, Ohmit SE and
Stidham GL: Effectiveness of ribavirin in otherwise well infants
with respiratory syncytial virus-associated respiratory failure. J
Pediatr. 128:442–448. 1996. View Article : Google Scholar
|
|
49
|
Guerguerian AM, Gauthier M, Lebel MH,
Farrell CA and Lacroix J: Ribavirin in ventilated respiratory
syncytial virus bronchiolitis: A randomized, placebo-controlled
trial. Am J Respir Crit Care Med. 160:829–834. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Wheeler JG, Wofford J and Turner RB:
Historical cohort evaluation of ribavirin efficacy in respiratory
syncytial virus infection. Pediatr Infect Dis J. 12:209–213. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
van Woensel JB, Wolfs TF, van Aalderen WM,
Brand PL and Kimpen JL: Randomized double blind placebo controlled
trial of prednisolone in children admitted to hospital with
respiratory syncytial virus bronchiolitis. Thorax. 52:634–637.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Cade A, Brownlee KG, Conway SP, Haigh D,
Short A, Brown J, Dassu D, Mason SA, Phillips A, Eglin R, et al:
Randomised placebo controlled trial of nebulised corticosteroids in
acute respiratory syncytial viral bronchiolitis. Arch Dis Child.
82:126–130. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Menon K, Sutcliffe T and Klassen TP: A
randomized trial comparing the efficacy of epinephrine with
salbutamol in the treatment of acute bronchiolitis. J Pediatr.
126:1004–1007. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Barr FE, Patel NR and Newth CJ: The
pharmacologic mechanism by which inhaled epinephrine reduces airway
obstruction in respiratory syncytial virus associated
bronchiolitis. J Pediatr. 136:699–700. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Bertrand P, Araníbar H, Castro E and
Sánchez I: Efficacy of nebulized epinephrine vs salbutamol in
hospitalized infants with bronchiolitis. Pediatr Pulmonol.
31:384–288. 2001. View Article : Google Scholar
|
|
56
|
Flores G and Horwitz RI: Efficacy of
2-agonists in bronchiolitis: A reappraisal and meta-analysis.
Pediatrics. 100:233–239. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Patterson JE, Bradley JM and Elborn JS:
Airway clearance in bronchiectasis: A randomized crossover trial of
active cycle of breathing techniques (incorporating postural
drainage and vibration) versus test of incremental respiratory
endurance. Chron Respir Dis. 1:127–130. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Charman J and Reid L: Sputum viscosity in
chronic bronchitis, bronchiectasis, asthma and cystic fibrosis.
Biorheology. 9:185–199. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Ipek IO, Yalcin EU, Sezer RG and Bozaykut
A: The efficacy of nebulized salbutamol, hypertonic saline and
salbutamol/hypertonic saline combination in moderate bronchiolitis.
Pulm Pharmacol Ther. 24:633–637. 2011. View Article : Google Scholar : PubMed/NCBI
|