Introduction
In 1895, the German surgeon Kummell first reported
on six patients with a vertebral body compression fracture after a
minor trauma, which led to delayed collapse of the vertebral body.
The disease later became known as ‘Kummell disease’. The incidence
of Kummell disease increases with age and the presence of
osteoporosis. Wang et al (1)
linked Kummell disease to infarction of the vertebral body, with
trauma and osteoporosis being the major factors responsible for the
infarction. Li et al (2)
divided Kummell disease into three stages (stage I, II and III). In
stage I, the vertebral body height loss is <20%, with or without
adjacent intervertebral disc degeneration, whereas the vertebral
body height loss in stage II is >20% and is usually accompanied
by adjacent intervertebral disc degeneration. Stage III Kummell
disease is characterized by posterior breakage combined with spinal
cord compression (2). Various
factors associated with Kummell disease, including neurological
deficits, back pain and spinal canal stenosis, may increase the
risk of disability and mortality, and reduce the quality of life
(3). Thus, the development of a
suitable surgical technique for use in Kummell disease is urgently
required.
Previous studies have indicated that percutaneous
kyphoplasty (PKP) in stage I, II and III Kummell disease achieved a
good curative effect (4,5). Compared with bone cement-augmented
short segmental fixation, PKP was associated with better early
clinical outcomes and reduced blood loss, as well as decreased
operative times and duration of stay at the hospital (6). PKP also immediately alleviated
vertebral body pain and restored the stiffness and strength of the
vertebral body via the use of polymethyl methacrylate (PMMA)
cement, which provided stability and support (7). PMMA is the most commonly used cement in
PKA, and the use of PMMA with improved viscosity and working times
as well as radiofrequency-targeted augmentation and implants, has
led to progress in the treatment of Kummell disease (7). The bilateral approach, which is
relatively safe and effective, is considered the mainstay of PKP
for Kummell disease (8,9). Certain studies have proposed that, as
compared with bilateral PKP, unilateral PKP may offer a number of
benefits, including a shorter operative time, lower complication
rate and less radiation exposure (10,11). A
comparison of bilateral and unilateral approaches may provide
evidence for surgeons in the selection of PKP.
In the present study, the efficacy of the unilateral
transverse process-pedicle and bilateral puncture technique in PKP
for patients with Kummell disease was retrospectively analyzed.
Materials and methods
Inclusion and exclusion criteria
The inclusion criteria were patients who met the
diagnostic criteria for Kummell disease, without a known history of
trauma or acute minor trauma and intractable chest and back pain,
which receded upon bed rest and worsened upon sitting and walking,
as well as kyphosis and local percussion pain, ineffective
conservative treatment for >3 months, and imaging revealing a
vacuum sign, fissure sign, pseudoarthrosis or fracture sclerosis.
Additional inclusion criteria were an age of >55 years, a
lesional segment of T11-L4, stage I or II
disease and a bone density T-value of <-2.5 on dual-energy X-ray
absorptiometry, which is in accordance with the diagnostic criteria
for osteoporosis (12).
The exclusion criteria were combined serious
internal medical diseases, a fresh fracture, or a pathological
fracture associated with a metastatic tumor or primary tumor of the
vertebral body.
Patients
A total of 63 patients with Kummell disease who met
the diagnostic criteria and underwent PKP between March 2015 and
June 2017 with one of the two puncture techniques were recruited
(registration number 2015-3-31-1). Due to the increased cost of
bilateral surgery, certain patients selected the unilateral method,
which is cheaper and theoretically safe. A total of 38 patients
were treated with the unilateral method and 25 patients were
treated with the bilateral method. In the unilateral group, there
were 7 males and 31 females aged 57–81 years, with an average age
of 69.7 years. The course of the disease was between 16 and 44
weeks, with an average duration of 19.5 weeks. The lesional segment
was classified as T11, T12, L1,
L2 and L3 in 3, 9, 14, 7 and 5 patients,
respectively. A total of 12 patients had stage I disease and 28
patients had stage II disease. The bone density T-value was between
−3.9 and −2.5, with an average T-value of −2.9. In the bilateral
group, there were 6 males and 19 females aged 56–84 years, with an
average age of 69.4 years. The course of the disease was between 14
and 51 weeks, with an average duration of 18.4 weeks. The lesional
segment was classified as T11, T12,
L1, L2, L3 and L4 in 2,
9, 8, 2, 2 and 2 patients, respectively. A total of 8 patients had
stage I disease and 17 patients had stage II disease. The bone
density T-value was between −3.7 to −2.6, with an average T-value
of −2.9.
Frontal and lateral chest X-ray, computed tomography
in cases of injured vertebrae and chest magnetic resonance imaging
were performed prior to surgery. There were no significant
inter-group differences in terms of sex, age, course of disease,
lesional segment, bone density T-value, pre-operative visual analog
scale (VAS) pain score, Oswestry disability index (ODI), vertebral
body height and Cobb angle (13)
(Table I).
 | Table I.Comparison of operation indices
between the two groups. |
Table I.
Comparison of operation indices
between the two groups.
| Group | n | Operation time
(min) | Intra-operative
fluoroscopy times (number of repeats) | Volume of bone cement
injection (ml) |
|---|
| Unilateral | 38 | 36.54±10.23 | 17.98±2.58 | 4.62±1.03 |
| Bilateral | 25 | 50.26±12.06 | 20.16±3.02 | 5.57±1.08 |
| Statistics |
| t=−4.253 | t=−3.019 | t=−3.275 |
|
|
| P<0.001 | P=0.005 | P=0.003 |
Surgical techniques
Surgery was performed in accordance with a previous
report with some modifications as listed below (14). Under general anesthesia, the patient
was placed in the prone position during the X-ray examination. The
C-arm was adjusted to ensure that there was no bilateral shadow on
the affected vertebral body and the puncture entry point was marked
(3-o'clock on the right side and 9-o'clock on the left side). When
the puncture point reached the anterior one-third of the posterior
margin of the vertebral body, a working tunnel was established
using a needle, dilated duct and working casing pipe. In the
present study, a balloon was then guided into the anterior
one-third of the affected vertebral body. A pressure injection
device was connected to the balloon and iohexol was injected to
monitor the balloon expansion. When the pressure reached 350 kPa, a
core needle in the balloon was extracted from the balloon to expand
to locations affected by osteoporosis. In the unilateral group,
prior to injection of the PMMA bone cement, the fluid and air in
the vertebral body were exhausted, and the bone cement was
injected, as described previously. In the bilateral group, a
puncture entry point was made on the other side. A tunnel was
established and the vertebral body was expanded through the working
tunnel. After vertebral body reduction, the bone cement was
injected into the vertebral body. When the bone cement had diffused
into the posterior one-third of the vertebral body, the bone cement
volume was reduced and the fluoroscopy time was increased. Once
bone cement leakage was detected or the bone cement filled the
cavity, the bone cement injection was stopped and the puncture
needle was removed. The wound was then covered by a sterile wound
dressing. Post-operative electrocardiograph monitoring was
performed for 2 h. All of the patients were fitted with a corset
and regained remobilization at 1 day after the operation.
Evaluation indices
The operative time, intra-operative fluoroscopy
time, volume of bone cement material and bone cement leakage were
recorded.
The VAS was used to assess the pain scores of the
patients prior to surgery, at 1 and 3 days post-surgery, and at 1,
6 and 12 months post-surgery. A 10-cm-long line, with ‘painless
(score = 0)’ and ‘severe pain (score = 10)’ marked at either end,
was used. According to the degree of pain, the patients marked a
point on the line to indicate the intensity and psychological
impact of the pain. The numeric value of the distance from the
starting point to the marked point in cm resembled the VAS score.
The higher the score, the more severe the pain was considered to
be.
The ODI was used to assess the ability of the
patients to pursue daily activities of life prior to surgery, at 1
and 3 days post-surgery, and at 1, 6 and 12 months post-surgery.
The ODI includes an assessment of pain (the degree of pain and the
effect of pain on sleep), single functions (lying down, sitting,
standing and walking) and comprehensive function (activities of
daily living, sexual life and social activities). Each item was
scored as 0–5 points. The corresponding scores of the answers to 10
items were accumulated and the ODI was calculated as the percentage
of the accumulated score/50 points. The higher the score, the more
severe the level of dysfunction was considered to be.
The vertebral body height was used to assess the
recovery of the vertebral body. The method of Pflugmacher (15) was used to measure the distance
between the upper and lower endplates of the anterior vertebral
body prior to surgery, at 1 and 3 days post-surgery, and at 1, 6
and 12 months post-surgery.
The Cobb angle was used to assess the recovery of
the vertebral body. Phillips's method (16) was used to measure the angle of the
intersection of the vertical line of the upper vertebral endplate
and lower vertebral endplate of injured vertebrae prior to surgery,
at 1 and 3 days post-surgery, and at 1, 6 and 12 months
post-surgery.
Statistical analysis
SPSS software, version 17 (SPSS Inc., Chicago, IL,
USA) was used for all the statistical analyses. Values are
expressed as the mean ± standard deviation. A comparative analysis
between the groups was performed using an independent two-samples
t-test. Repeated-measures analysis of variance was used to compare
different assessments in each group, followed by a Newman-Keuls
post-hoc test. Categorical variables were compared using the
χ2 test. P<0.05 was considered to indicate
statistical significance.
Results
Clinical outcomes
Various operation indices for the two groups are
provided in Table I. In the
unilateral group, there were six cases of bone cement leakage
(15.79%) and the leakage reached the anterior vertebrae in all
cases. In the bilateral group, there were four cases of bone cement
leakage (16.00%), with the leakage reaching the anterior vertebrae
in one case and the intervertebral disc in three cases. There was
no statistically significant inter-group difference in the
incidence of bone cement leakage (χ2=<0.001;
P<0.001). The operative time, intra-operative fluoroscopy time
and volume of bone cement injection in the unilateral group were
significantly lower than those in the bilateral group (P<0.05).
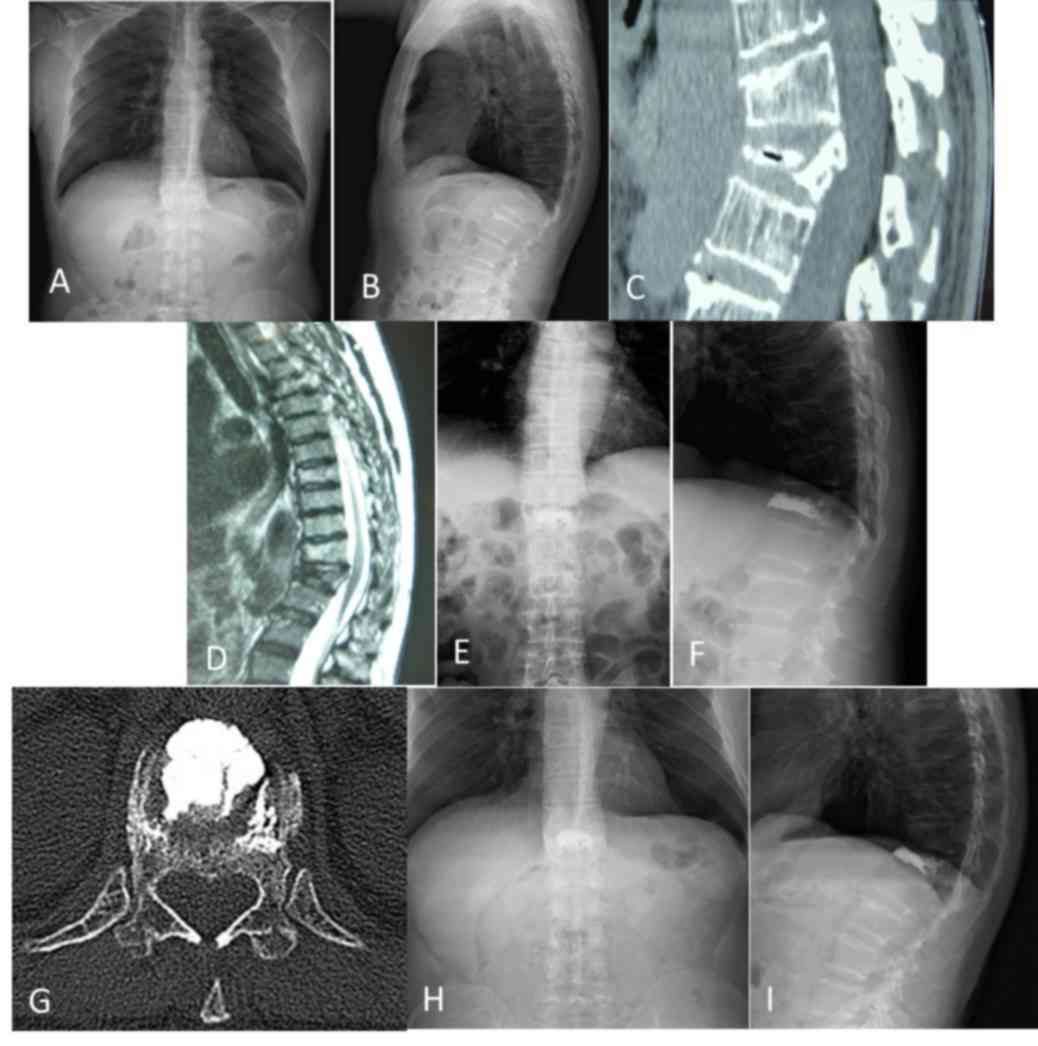
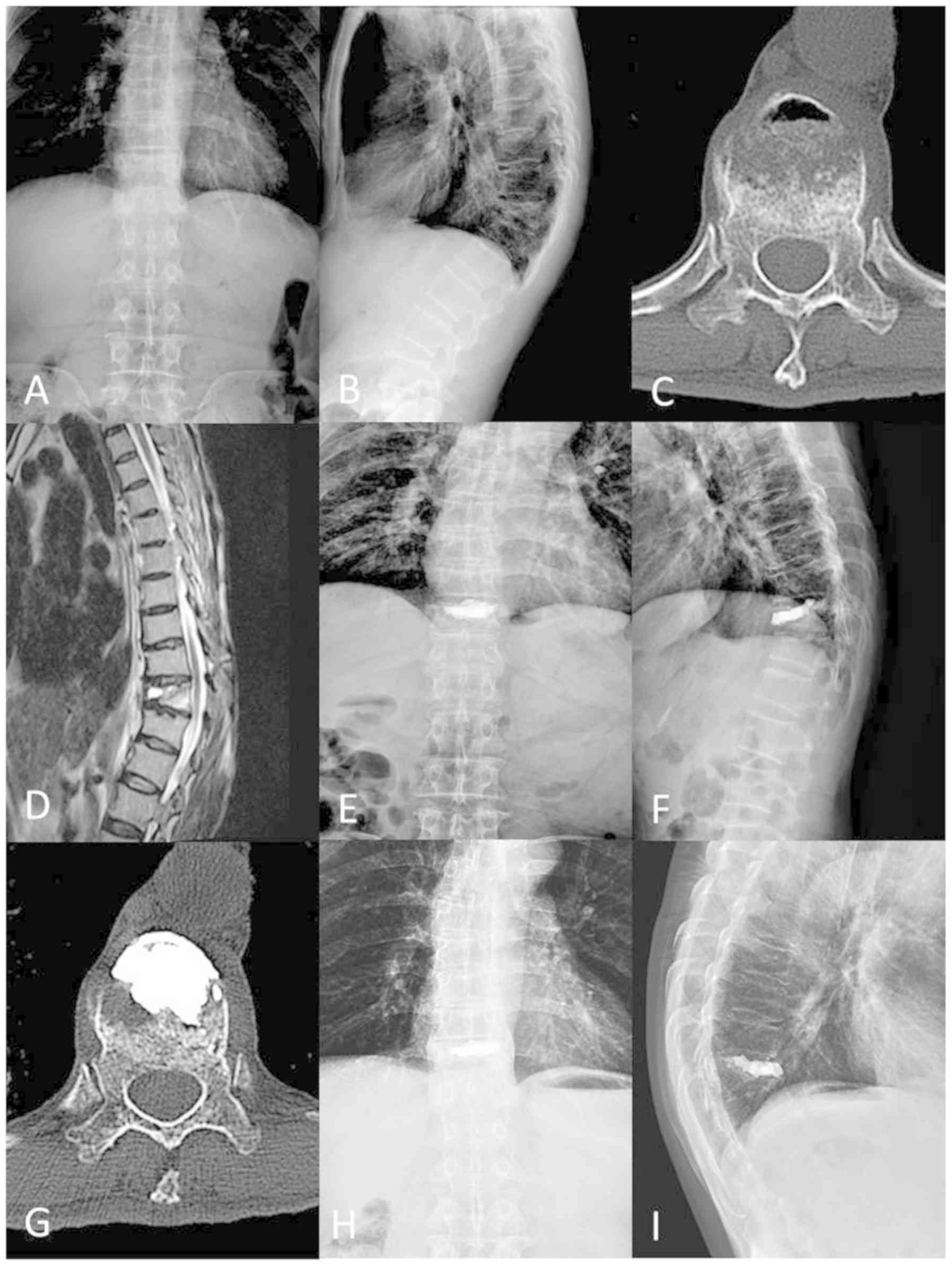
The chest X-ray examination exhibited no pulmonary embolism at 1
day post-surgery in the two groups. There were no complications,
including re-fracture of the vertebral body or displacement of bone
cement block, in either group, as exemplified by representative
cases, whose images are provided in Figs. 1 and 2.
Comparison of indices in the follow-up
period
The duration of follow-up was between 12 and 24
months for all of the patients, with an average period of 16.4
months. There were no significant differences in the VAS scores
between the unilateral and bilateral groups (P>0.05), although
the VAS score in the bilateral group was lower than that in the
unilateral group (Table II). The
VAS scores were significantly decreased in the unilateral and
bilateral groups at 1 day post-surgery as compared with those
pre-surgery (Table II). With the
increase in the follow-up time, the VAS scores of the two groups
gradually decreased, and there was a statistically significant
difference in the scores between the first day post-surgery and the
later time-points (P<0.05).
| Table II.Comparison of visual analog scale
score between the two groups at different time-points. |
Table II.
Comparison of visual analog scale
score between the two groups at different time-points.
|
|
|
| Following
surgery |
|---|
|
|
|
|
|
|---|
| Group | N | Prior to surgery | 1 day | 3 days | 1 month | 6 months | 12 months |
|---|
| Unilateral | 38 | 6.73±1.00 |
3.50±0.91a |
3.12±0.87a,b |
2.35±0.94a,b |
1.70±0.85a,b |
1.38±0.82a,b |
| Bilateral | 25 | 6.37±0.96 |
3.42±1.07a |
3.08±0.93a,b |
2.31±0.98a,b |
1.65±0.79a,b |
1.32±0.75a,b |
| Statistics |
| t=1.213 | t=0.270 | t=0.148 | t=0.138 | t=0.201 | t=0.251 |
|
|
| P=0.232 | P=0.788 | P=0.883 | P=0.891 | P=0.842 | P=0.803 |
There were no significant inter-group differences in
the ODI scores (P>0.05), although the ODI scores of the
bilateral group were higher than those of the unilateral group
(Table III). In each of the two
groups, the ODI scores had decreased significantly at 1 day
post-surgery as compared with those prior to surgery (Table III). With the increase in the
follow-up time, the ODI scores of the two groups gradually
decreased, and there was a statistically significant difference
between the scores at day 1 post-surgery and the later time-points
(P<0.05).
| Table III.Comparison of Oswestry disability
index between the two groups at different time-points. |
Table III.
Comparison of Oswestry disability
index between the two groups at different time-points.
|
|
|
| Following
surgery |
|---|
|
|
|
|
|
|---|
| Group | N | Prior to
surgery | 1 day | 3 days | 1 month | 6 months | 12 months |
|---|
| Unilateral | 38 | 68.00±6.70 |
32.73±5.05a |
28.54±5.78a,b |
22.78±5.47a,b |
18.84±5.05a,b |
15.34±4.14a,b |
| Bilateral | 25 | 68.16±7.67 |
33.74±7.05a |
29.23±6.64a,b |
23.28±5.75a,b |
18.25±5.36a,b |
14.62±4.36a,b |
| Statistics |
| t=0.074 | t=0.561 | t=0.371 | t=0.296 | t=0.377 | t=0.563 |
|
|
| P=0.941 | P=0.578 | P=0.712 | P=0.769 | P=0.708 | P=0.576 |
As presented in Table
IV, there were no significant inter-group differences in the
vertebral body height (P>0.05). In either of the two groups, the
vertebral body height was significantly increased at 1 day
post-surgery as compared with that prior to surgery
(P<0.05).
| Table IV.Comparison of vertebral body height
between the two groups at different time-points. |
Table IV.
Comparison of vertebral body height
between the two groups at different time-points.
|
|
|
| Following
surgery |
|---|
|
|
|
|
|
|---|
| Group | N | Prior to
surgery | 1 day | 3 days | 1 month | 6 months | 12 months |
|---|
| Unilateral | 38 | 16.08±1.96 |
20.62±1.64a |
20.62±1.62a,b |
20.60±1.64a,b |
20.58±1.60a,b |
20.56±1.57a,b |
| Bilateral | 25 | 15.61±1.24 |
20.04±1.21a |
20.04±1.24a,b |
20.02±1.20a,b |
20.00±1.25a,b |
20.00±1.16a,b |
| Statistics |
| t=0.983 | t=1.303 | t=1.305 | t=1.306 | t=1.313 | t=1.313 |
|
|
| P=0.331 | P=0.199 | P=0.199 | P=0.198 | P=0.196 | P=0.196 |
There were no significant differences in the Cobb
angles of the unilateral and bilateral groups (P>0.05), as
indicated in Table V. In the
unilateral and bilateral groups, the Cobb angle was significantly
decreased at 1 day post-surgery as compared with that prior to
surgery (P<0.05; Table V).
| Table V.Comparison of Cobb angle between the
two groups at different time-points. |
Table V.
Comparison of Cobb angle between the
two groups at different time-points.
|
|
|
| Following
surgery |
|---|
|
|
|
|
|
|---|
| Group | N | Prior to
surgery | 1 day | 3 days | 1 month | 6 months | 12 months |
|---|
| Unilateral | 38 | 14.53±3.96 |
8.66±2.51a |
8.66±2.54a,b |
8.66±2.48a,b |
8.67±2.52a,b |
8.69±2.57a,b |
| Bilateral | 25 | 14.93±3.66 |
8.46±2.66a |
8.46±2.65a,b |
8.46±2.63a,b |
8.48±2.62a,b |
8.51±2.68a,b |
| Statistics |
| t=0.345 | t=0.257 | t=0.256 | t=0.260 | t=0.246 | t=0.228 |
|
|
| P=0.732 | P=0.798 | P=0.799 | P=0.796 | P=0.807 | P=0.821 |
Discussion
Kummell disease is a complication of osteoporosis,
osteogenesis decline, intervertebral disc degeneration,
microfractures, fatigue fractures, inadequate blood flow and
pseudoarthrosis (17); it is caused
by vertebral body infarction, with trauma and osteoporosis thought
to be the major factors responsible for the infarction (1). Usually, Kummell disease is diagnosed
based on an intravertebral vacuum cleft sign (18). The affected vertebral body exhibits
marked mobility, with a decreased height, which increases during
hyperextension. There are no neurological symptoms in stage I and
II Kummell disease. Thus, at these stages, the major aim is to
eliminate the mobility of the fractured vertebrae and restore
spinal stability (15). By contrast,
stage III disease is characterized by rupture of the posterior
vertebral wall, together with severe kyphosis and neurospinal
symptoms, for which open surgery is recommended (19).
As a treatment for Kummell disease, PKP may
immediately alleviate pain and restore the stiffness and strength
of the vertebral body through the stability and support provided by
PMMA (20). Kim et al
(21) reported that a bone cement
volume of 30% of the vertebral body volume restored the level of
stiffness to that of normal bone. However, if the bone cement
volume exceeded 30% of the vertebral body volume, the stiffness
exceeded that of normal bone. Thus, an appropriate bone cement
volume is vital for restoration of the vertebral body. In the
present study, although the volume of bone cement in the unilateral
group was significantly lower than that in the bilateral group, a
unilateral puncture may result in an uneven distribution of bone
cement in the vertebral body, unilateral weight bearing, lateral
compression and collapse of the non-operative side of the vertebral
body (22,23).
In a previous biomechanical analysis, unipedicular
kyphoplasty and bipedicular kyphoplasty restored the strength and
stiffness of the vertebral body, and unipedicular kyphoplasty did
not increase the risk of lateral compression based on a comparison
of the vertebral body height (5).
The present results indicated that the operative time,
intra-operative fluoroscopy time and volume of bone cement
injection in the unilateral group were significantly lower than
those in the bilateral group, indicating that unilateral PKP was
beneficial in decreasing the operative time, X-ray radiation dose
and the puncture wound size. In the follow-up period, none of the
patients experienced refracture around the vertebral body,
suggesting that the unilateral puncture method was able to restore
the strength and stiffness of the affected vertebral body. Studies
by Yan et al (24,14) reported that pain and the kyphotic
angle were reduced in their unilateral and bilateral groups,
whereas the volume of the injected cement and radiation dose in the
unilateral group were lower than those in the bilateral group.
Hence, the current study demonstrated that unilateral PKP had a
similar curative effect as bilateral PKP, and the radiation dose,
operative time and complication rate were all lower than those in
the bilateral PKP group, which was consistent with the results of
previous studies (13)
In the unilateral puncture approach, the inclined
angle of the puncture is increased to distribute the bone cement to
the opposite side, which increases puncture-associated risks. To
address these issues, the balloon must be placed in the anterior
one-third of the vertebral body to allow the bone cement to diffuse
into the midline and contralateral vertebral body (25). The balloon may be extended and
expanded twice during surgery, which aids in the recovery of the
vertebral body height. To avoid rupture of the vertebral body wall
and balloon and the risk of bone cement leakage, the pressure
achieved by balloon dilatation should not be excessively high
(26). In certain patients with
acute fractures, the vertebral body contains a large amount of
fluid. In such cases, prior to bone cement injection, the fluid in
the vertebral body should be removed to reduce the injection
pressure and facilitate bone cement diffusion and anchorage of the
bone cement to the vertebral wall (26).
Of note, the present study has certain limitations.
The number of patients with Kummell disease was relatively small,
and the length of the follow-up period was not sufficient. In the
present study, spinal cord damage, operative time and
intra-operative fluoroscopy time, as well as the volume of bone
cement injection, were lower in the unilateral group than those in
the bilateral group, and the VAS scores, ODI scores, vertebral body
height and Cobb angle were measured during the follow-up period to
indicate the curative effect between uni- and bilateral groups. A
study with a larger patient population (200 or more patients) and a
longer follow-up period (24 months post-surgery) will be performed
in the future.
In conclusion, the present study indicated that
bilateral and unilateral PKP are able to efficiently relieve pain,
restore the vertebral body height, reduce the Cobb angle and
restore spinal stability. As compared with bilateral PKP,
unilateral PKP was associated with shorter operative times and
intraoperative fluoroscopy times. However, as indicated by previous
studies, the risk of unevenly distributed bone cement with
unilateral PKP may be higher than that with bilateral PKP.
Therefore, unilateral PKP may be a priority on the basis of
proficiency in PKP.
Acknowledgements
Not applicable.
Funding
No funding received.
Availability of data and materials
The datasets used during the present study are
available from the corresponding author on reasonable request.
Authors' contributions
XX and YS conceived and designed the current study,
prepared the manuscript and performed statistical analysis. SS and
MY acquired the data. JZ and DW contributed to the quality control
of data and algorithms. XD and HS analyzed and interpreted the
data. All authors read and approved the final version of the
manuscript.
Ethical approval and consent to
participate
The study was approved by the ethics committee of
Sichuan Orthopaedic Hospital (Sichuan, China) and informed consent
was obtained from all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Wang G, Yang H, Meng B, Zhu X, Zou J, Gan
M, Mei X, Chen K and Tang T: Post-traumatic osteoporotic vertebral
osteonecrosis treated using balloon kyphoplasty. J Clin Neurosci.
18:664–668. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Li K, Wong T, Kung F, Li A and Hsieh C:
Staging of Kümmell's disease. J Musculoskelet Res. 8:43–55. 2004.
View Article : Google Scholar
|
|
3
|
Zhang X, Hu W, Yu J, Wang Z and Wang Y: An
effective treatment option for Kümmell disease with neurological
deficits: Modified transpedicular subtraction and disc osteotomy
combined with long-segment fixation. Spine (Phila Pa 1976).
41:E923–E930. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Huang Y, Peng M, He S, Tang X, Dai M and
Tang C: Clinical efficacy of percutaneous kyphoplasty at the
hyperextension position for the treatment of osteoporotic kümmell
disease. Clin Spine Surg. 29:161–166. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen B, Li Y, Xie D, Yang X and Zheng Z:
Comparison of unipedicular and bipedicular kyphoplasty on the
stiffness and biomechanical balance of compression fractured
vertebrae. Eur Spine J. 20:1272–1280. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Huang YS, Hao DJ, Feng H, Zhang HP, He SM,
Ge CY and Niu XB: Comparison of percutaneous kyphoplasty and bone
cement-augmented short-segment pedicle screw fixation for
management of kümmell disease. Med Sci Monit. 24:1072–1079. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Filippiadis DK, Marcia S, Masala S,
Deschamps F and Kelekis A: Percutaneous vertebroplasty and
kyphoplasty: Current status, new developments and old
controversies. Cardiovasc Intervent Radiol. 40:1815–1823. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Garfin SR, Yuan HA and Reiley MA: New
technologies in spine: Kyphoplasty and vertebroplasty for the
treatment of painful osteoporotic compression fractures. Spine
(Phila Pa 1976). 26:1511–1515. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lieberman IH, Dudeney S, Reinhardt MK and
Bell G: Initial outcome and efficacy of ‘kyphoplasty’ in the
treatment of painful osteoporotic vertebral compression fractures.
Spine (Phila Pa 1976). 26:1631–1638. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Huang Z, Wan S, Ning L and Han S: Is
unilateral kyphoplasty as effective and safe as bilateral
kyphoplasties for osteoporotic vertebral compression fractures? A
meta-analysis. Clin Orthop Relat Res. 472:2833–2842. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Feng H, Huang P, Zhang X, Zheng G and Wang
Y: Unilateral versus bilateral percutaneous kyphoplasty for
osteoporotic vertebral compression fractures: A systematic review
and meta-analysis of RCTs. J Orthop Res. 33:1713–1723. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sun Z, Qiu G and Zhao Y: Application and
research advances of metabolomics in the field of orthopedics.
Zhonghua Wai Ke Za Zhi. 53:476–480. 2015.(In Chinese). PubMed/NCBI
|
|
13
|
Chang X, Lv YF, Chen B, Li HY, Han XB,
Yang K, Zhang W, Zhou Y and Li CQ: Vertebroplasty versus
kyphoplasty in osteoporotic vertebral compression fracture: A
meta-analysis of prospective comparative studies. Int Orthop.
39:491–500. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yan L, He B, Guo H, Liu T and Hao D: The
prospective self-controlled study of unilateral transverse
process-pedicle and bilateral puncture techniques in percutaneous
kyphoplasty. Osteoporos Int. 27:1849–1855. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pflugmacher R, Schroeder RJ and
Klostermann CK: Incidence of adjacent vertebral fractures in
patients treated with balloon kyphoplasty: Two years' prospective
follow-up. Acta Radiol. 47:830–840. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Phillips FM, Isaacs RE, Rodgers WB,
Khajavi K, Tohmeh AG, Deviren V, Peterson MD, Hyde J and Kurd M:
Adult degenerative scoliosis treated with XLIF: Clinical and
radiographical results of a prospective multicenter study with
24-month follow-up. Spine (Phila Pa 1976). 38:1853–1861. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kim YC, Kim YH and Ha KY: Pathomechanism
of intravertebral clefts in osteoporotic compression fractures of
the spine. Spine J. 14:659–666. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wu AM, Chi YL and Ni WF: Vertebral
compression fracture with intravertebral vacuum cleft sign:
Pathogenesis, image, and surgical intervention. Asian Spine J.
7:148–155. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Li H, Liang CZ and Chen QX: Kümmell's
disease, an uncommon and complicated spinal disorder: A review. J
Int Med Res. 40:406–414. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chen GD, Lu Q, Wang GL, Zou J, Yang HL,
Yang Y and Luo ZP: Percutaneous kyphoplasty for kummell disease
with severe spinal canal stenosis. Pain Physician. 18:1021–1028.
2015.
|
|
21
|
Kim JM, Shin DA, Byun DH, Kim HS, Kim S
and Kim HI: Effect of bone cement volume and stiffness on
occurrences of adjacent vertebral fractures after vertebroplasty. J
Korean Neurosurg Soc. 52:435–440. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hu M, Ma H, Shi H, Liang Y, Zeng Y and
Wang J: Early clinical outcome of manual reduction combined with
uni-lateral percutaneous kyphoplasty to treat osteoporotic
vertebral compression fracture. Zhongguo Xiu Fu Chong Jian Wai Ke
Za Zhi. 24:1092–1096. 2010.(In Chinese). PubMed/NCBI
|
|
23
|
Deng XQ, Wu YS and Wang HM: Application of
contralateral supplementary puncture in unilateral percutaneous
vertebroplasty for poor bone cement dispersion. Zhongguo Gu Shang.
31:1168–1171. 2018.(In Chinese). PubMed/NCBI
|
|
24
|
Yan L, Jiang R, He B, Liu T and Hao D: A
comparison between unilateral transverse process-pedicle and
bilateral puncture techniques in percutaneous kyphoplasty. Spine
(Phila Pa 1976). 39:B19–B26. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Dalton BE, Kohm AC, Miller LE, Block JE
and Poser RD: Radiofrequency-targeted vertebral augmentation versus
traditional balloon kyphoplasty: Radiographic and morphologic
outcomes of an ex vivo biomechanical pilot study. Clin Interv
Aging. 7:525–531. 2012.PubMed/NCBI
|
|
26
|
Guo J, Ding W, Shen Y, Li B, Wu H, Cao L
and Li P: Selective treatment of aged osteoporosis thoracolumbar
vertebrae burst fracture with balloon kyphoplasty. Zhongguo Xiu Fu
Chong Jian Wai Ke Za Zhi. 24:1341–1344. 2010.(In Chinese).
PubMed/NCBI
|