Introduction
Smoking has been recognized to cause serious health
problems. It is established that smoking is a risk factor of
diseases such as myocardial infarction (1,2), stroke
(3) and peripheral vascular diseases
(4). Smoking causes vascular
thrombosis by altering the hemostatic process via changes in the
function of endothelial cells and platelets affected by fibrinogen,
or coagulation factors (2).
Concerning the platelet function, the number of small aggregates of
platelets in smokers' plasma is significantly higher than in
non-smokers in the absence of chemical stimulants (5). Furthermore, acute smoking exposure in
habitual smokers increases the platelet aggregation and induces
greater resistance to thrombolysis than in non-smokers (5), and the mean platelet volume and
platelet distribution width, which are indicators of platelet
activation, are significantly higher in smokers than in non-smokers
(6). However, there are no
significant differences between smokers and non-smokers in platelet
aggregation induced by ADP (7).
Given these conflicting previous findings, the influence of smoking
on platelet activation has not been fully clarified.
Quitting of smoking is recommended in patients
undergoing surgery, because smoking increases the risk of
postoperative morbidity or mortality (8,9). Smoking
cessation reduces the rate of postoperative pulmonary complications
such as pneumonia (10) or
wound-healing complications such as surgical site infection
(9). At least eight weeks are
required for the disappearance of the cough-promoting effect of
smoking and reduction of postoperative pulmonary complications
(11) and more than four weeks are
required to reduce wound-healing complications (10). In addition, surgical patients are at
risk of developing venous thrombo-embolism (12). The main cellular components of
thrombo-embolism are platelets, endothelial cells, monocytes and
erythrocytes (12). However, the
influence of smoking cessation for surgery on platelet activation
is not fully known. Platelet aggregability in long-term smokers is
not reversible in four weeks (13).
However, only two weeks of smoking cessation reduced the ADP or
collagen-induced platelet aggregations through suppression of
oxidative stress (14).
Collagen initiates human platelet activation in the
process of thrombus formation. The interactions of platelet
glycoprotein VI with the collagen of the exposed vessel wall and
the complex of platelet glycoprotein Ib/IX/V with von Willebrand
factor (vWF) result in the adhesion of platelets to the site of
injury. After this adhesion, thromboxane A2 and ADP lead
to the activation of glycoprotein IIb/IIIa (αIIbβ3) and thrombosis
formation (15). Thrombus formation
is also associated with the secretion of granule contents, such as
platelet-derived growth factor (PDGF)-AB (16). In the plasma of smokers, platelet
α-granule constituents are increased, leading to platelet
aggregation (2). Smoking have higher
P2Y12 receptor expression on platelets, which increases the
ADP-induced platelet aggregation (2). However, the effects of smoking or
smoking cessation on platelet activation and the intracellular
mechanism are not fully clarified. Furthermore, the time-dependent
changes in the platelet function associated with smoking cessation
remain unclear.
We previously demonstrated that ADP (17,18) and
collagen (19,20) induce the secretion of PDGF-AB via the
activation of p38 mitogen-activated protein (MAP) kinase in human
platelets. In the present study, to investigate the effects of
smoking and the cessation of smoking on human platelet activation,
we examined the effects of collagen on platelet aggregation, the
secretion of PDGF-AB and the underlying mechanism in patients who
were quitting smoking for surgery over time for 12 weeks.
Materials and methods
Materials
Collagen was purchased from Takeda Austria GmbH
(Linz, Austria). A PDGF-AB enzyme-linked immunosorbent assay
(ELISA) kit was purchased from R&D System, Inc. (Minneapolis,
MN, USA). Phospho-specific p38 MAP kinase antibodies and p38 MAP
kinase antibodies were obtained from Cell Signaling, Inc. (Beverly,
MA, USA). GAPDH antibodies were purchased from Santa Cruz
Biotechnology (Santa Cruz, CA, USA). All other materials and
chemicals were obtained from commercial sources.
Subjects
This study was approved by the Ethics Committee of
Gifu University Graduate School of Medicine and Gifu Prefectural
General Medical Center. All participants signed an informed consent
agreement after receiving a detailed explanation of the study.
We enrolled 19 patients who visited smoking
cessation outpatient services at Gifu University Graduate School of
Medicine or Gifu Prefectural General Medical Center between January
2012 and November 2014. However, four patients were excluded from
the current study as they only visited outpatient services once. A
self-assessment was administered, and we examined the concentration
of carbon monoxide (CO) exhaled to confirm smoking cessation. Blood
samples were donated 4 times as follows: before smoking cessation,
and 4, 8 and 12 weeks after smoking cessation. We avoided drawing
blood except for at these time points in order to avoid influencing
the platelet function. Blood samples were drawn from the
antecubital vein by careful venipuncture in a 21-G sterile
syringe.
Human blood samples were combined with 1/10 volume
of a 3.8% sodium citrate. Platelet-rich plasma (PRP) was obtained
from blood samples by centrifugation at 155 × g for 12 min at room
temperature. Platelet-poor plasma (PPP) was prepared from the
residual blood by centrifugation at 2,500 × g for 5 min.
Two patients with severe hypertriglycemia (No. 10
and No. 12) were excluded because their PRP and PPP were highly
turbid and the samples are inappropriate for an analysis of
platelet function. Therefore, a total of 13 patients who ceased
smoking were analyzed in the current study.
Platelet aggregation
Platelet aggregation using citrated PRP was
monitored using a PA-200 aggregometer (Kowa Co., Ltd., Tokyo,
Japan), which can determine the size of platelet aggregates via
particle counting using laser scattering methods (small, 9–25 µm;
medium, 25–50 µm; large, 50–70 µm) (21) at 37°C with a stirring speed of 800
rpm. Platelet aggregation was monitored for 4 min after stimulation
with collagen (n=13 patients). The percentage of transmittance of
the isolated platelets was recorded as 0%, and that of the
appropriate PPP (blank) was recorded as 100%.
Determination of the ED50
value
We calculated the ED50 of collagen for
the platelet aggregation using an aggregometer with the laser
scattering system. The percentage of aggregation in each subject
was analyzed at a dose of 0, 1, 3 and 10 µg/ml collagen. Using the
ALOKA curve software program included in the ALOKA RIA programs
(ALOKA, Tokyo, Japan), a dose-response curve was plotted. From the
regression equation, the collagen dose corresponding to 50%
aggregation was calculated as the individual ED50 value
(22).
Protein preparation after
stimulation
After the stimulation with collagen, platelet
aggregation was terminated by the addition of an ice-cold EDTA (10
mM) solution. The mixture was centrifuged at 10,000 × g at 4°C for
2 min. To measure the secreted PDGF-AB as described below, the
supernatant was isolated and stored at −30°C for a subsequent
enzyme-linked immunosorbent assay (ELISA). For the Western blot
analysis, the pellet was washed twice with phosphate-buffered
saline, lysed, and immediately boiled in a lysis buffer containing
62.5 mM Tris/Cl, pH 6.8, 2% sodium dodecyl sulfate (SDS), 50 mM
dithiothreitol and 10% glycerol.
Western blotting
Western blot analysis was performed as described
previously (23). Briefly,
SDS-polyacrylamide gel electrophoresis (PAGE) was performed by the
method described by Laemmli (24)
using a 10% polyacrylamide gel. The proteins in the gel were
transferred onto a polyvinylidene fluoride (PVDF) membrane, which
was then blocked with 5% fat-free dry milk in Tris-buffered saline
with 0.1% Tween-20 (TBS-T, 20 mM Tris, pH 7.6, 137 mM NaCl, 0.1%
Tween-20) for 2 h before incubation with the indicated primary
antibodies. The primary antibodies used in this study were
phospho-specific p38 MAP kinase antibodies, p38 MAP kinase
antibodies or GAPDH antibodies. Peroxidase-labeled anti-rabbit IgG
antibodies or anti-goat IgG antibodies were used as secondary
antibodies. The primary and secondary antibodies were diluted to
the optimum concentration with 5% fat-free dry milk in TBS-T. The
peroxidase activity on the PVDF membranes was visualized on X-ray
film using an ECL Western blotting detection system as described in
the manufacturer's instructions.
Measurement of PDGF-AB
The PDGF-AB levels in the samples were determined
using a PDGF-AB ELISA kit in accordance with the manufacturer's
instructions.
Statistical analyses
The data are presented as box-and-whisker plots
representing the median ± 25 and 75 percentile values. Statistical
analyses were performed using the SPSS software program, ver. 23.0
(IBM Japan Ltd., Tokyo, Japan). The data were analyzed by Friedman
test followed by Wilcoxon signed-rank test for multiple comparisons
using the Bonferroni method. A P-value<0.05 was considered to
indicate statistical significance.
Results
Effects of smoking cessation on the
human platelet aggregation induced by collagen
Nineteen patients who intended to abstain from
smoking participated in this study, but four who stopped visiting
the hospital during the treatment period were excluded. The
characteristics of the patients are detailed in Table I. The concentration of exhaled CO
decreased after smoking cessation in all patients (Table I). We first examined the effect of
smoking cessation on the platelet aggregation stimulated by
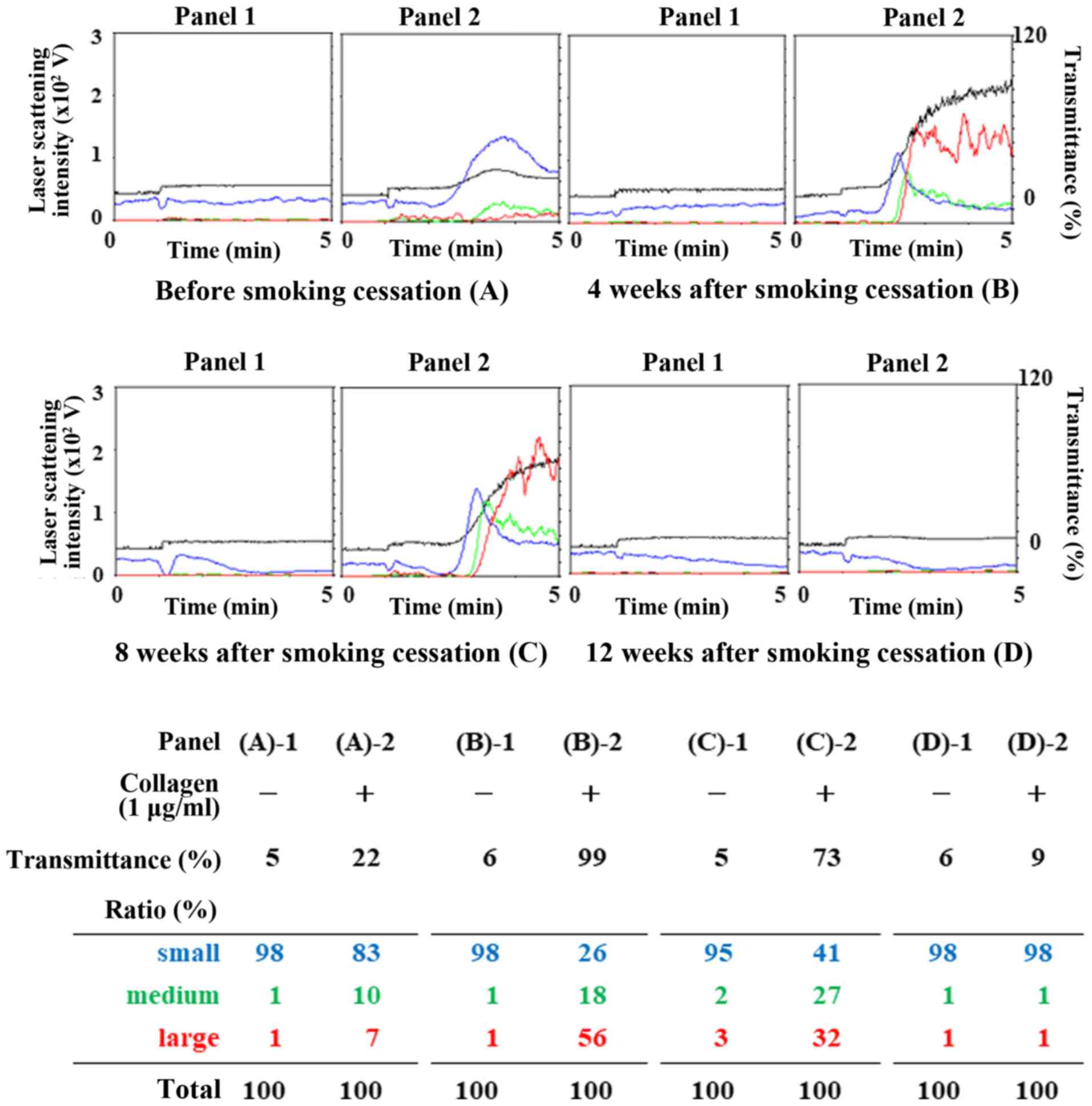
collagen. Before smoking cessation, collagen dose-dependently
elicited platelet aggregation between 1 and 10 µg/ml. For platelet
aggregation induced by a high dose of collagen (10 µg/ml), the
transmittance of aggregation was over 100% throughout the
observation periods. There were no significant differences between
the findings before and after smoking cessation (data not shown).
In contrast, a low dose of collagen (1 µg/ml) accelerated platelet
aggregation at 4 or 8 weeks after smoking cessation compared with
that before cessation (Fig. 1). In
addition, 12 weeks after smoking cessation, the levels of platelet
aggregation induced by collagen (1 µg/ml) had nearly returned to
the levels before smoking cessation. Representative patterns of
low-dose collagen (1 µg/ml)-induced platelet aggregation are shown
in Fig. 1.
 | Table I.Characteristics of 15 patients who
ceased smoking and participated in the present study. |
Table I.
Characteristics of 15 patients who
ceased smoking and participated in the present study.
|
|
|
|
|
|
|
|
| Concentration of CO
(ppm) |
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| Pt | Age (years) | Sex | Height/Weight
(cm/kg) | HTN | DM | HL | Platelet
(×104/µl) | (before) | (12 weeks
after) | Brinkman Index | Anti-platelet
medication |
|---|
| 1 | 44 | F | 170/58 | − | − | − | 20.5 | 20 | 0 | 480 | − |
| 2 | 71 | M | 160/76 | + | + | + | 20.3 | 11 | 2 | 1375 | + |
| 3 | 49 | M | 167/58 | − | − | − | 27.7 | 66 | 2 | 2040 | − |
| 4 | 35 | F | 162/44 | − | − | − | 35.1 | 38 | 6 | 300 | − |
| 5 | 63 | M | 168/59 | − | + | − | 21.6 | 25 | 1 | 1350 | + |
| 6 | 62 | M | 156/64 | − | − | − | 27.5 | 30 | 2 | 840 | − |
| 7 | 53 | M | 170/65 | − | − | − | 22.2 | 24 | 3 | 600 | − |
| 8 | 46 | M | 163/80 | − | − | + | 25.4 | 13 | 1 | 780 | − |
| 9 | 75 | M | 165/54 | − | − | − | 16.6 | 2 | 0 | 900 | − |
| 10 | 72 | M | 169/52 | − | − | + | 22.5 | 23 | 0 | 1040 | − |
| 11 | 49 | M | 168/61 | − | − | − | 21.0 | 27 | 2 | 1240 | − |
| 12 | 47 | F | 149/40 | − | − | − | 28.0 | 23 | 8 | 580 | − |
| 13 | 75 | M | 151/61 | − | − | − | 18.6 | 22 | 3 | 500 | − |
| 14 | 47 | M | 178/77 | − | − | − | 20.3 | 14 | 0 | 600 | − |
| 15 | 46 | M | 176/90 | − | − | − | 24.9 | 8 | 2 | 405 | − |
Based on the analysis of the size of platelet
aggregates using laser scattering methods, after 4 or 8 weeks
smoking cessation, the ratio of large aggregates (50–70 µm)
stimulated by 1 µg/ml collagen was significantly increased while
the ratio of small aggregates (9–25 µm) was significantly decreased
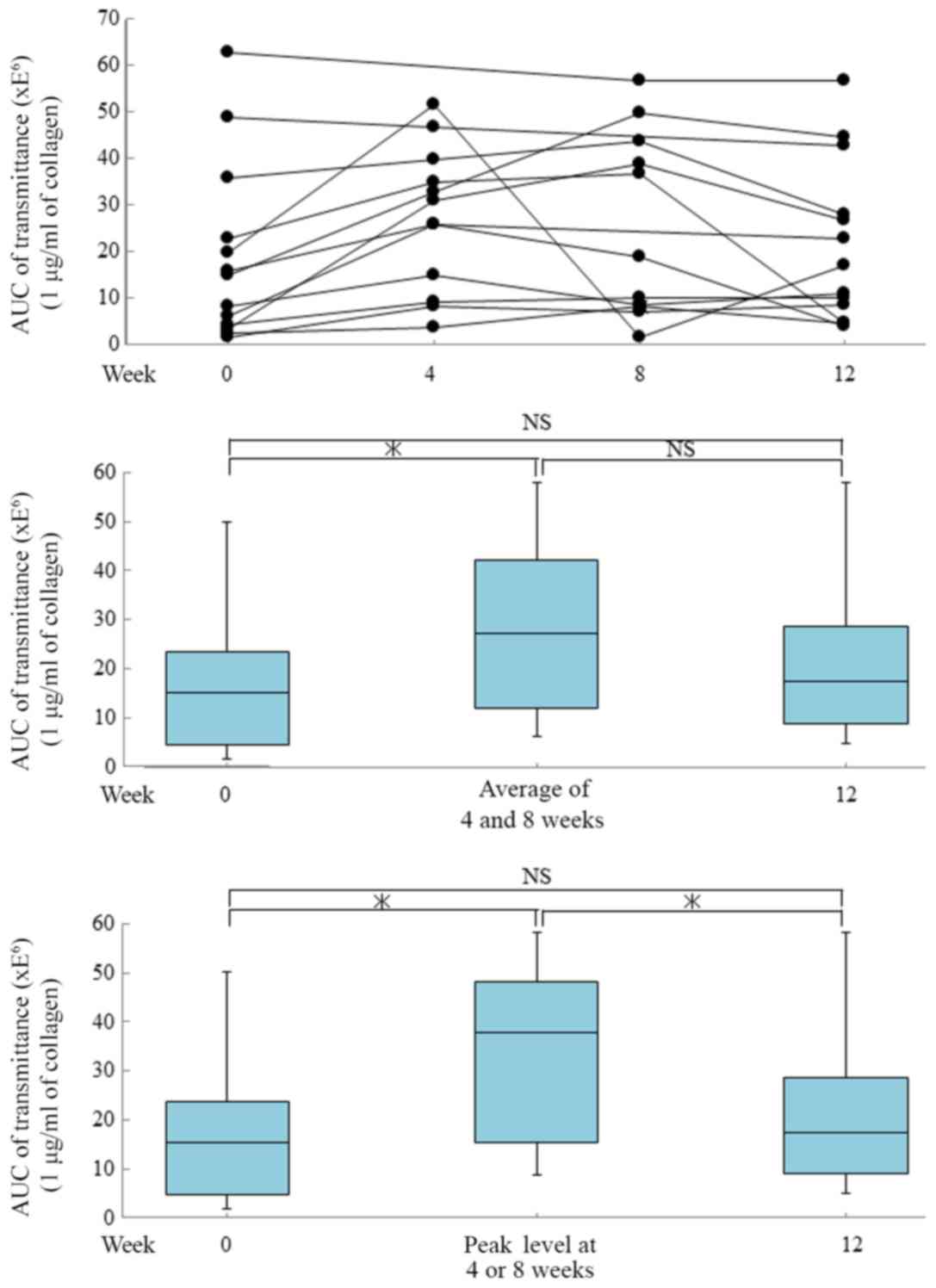
(data not shown). The peak value of the areas under the curve
(AUCs) of transmittance stimulated by low-dose collagen (1 µg/ml)
at 4 or 8 weeks after smoking cessation were significantly higher
than the respective AUCs before smoking cessation (Fig. 2). In addition, the AUC of
transmittance stimulated by 1 µg/ml collagen at 12 weeks after
smoking cessation returned to levels similar to those before the
cessation of smoking.
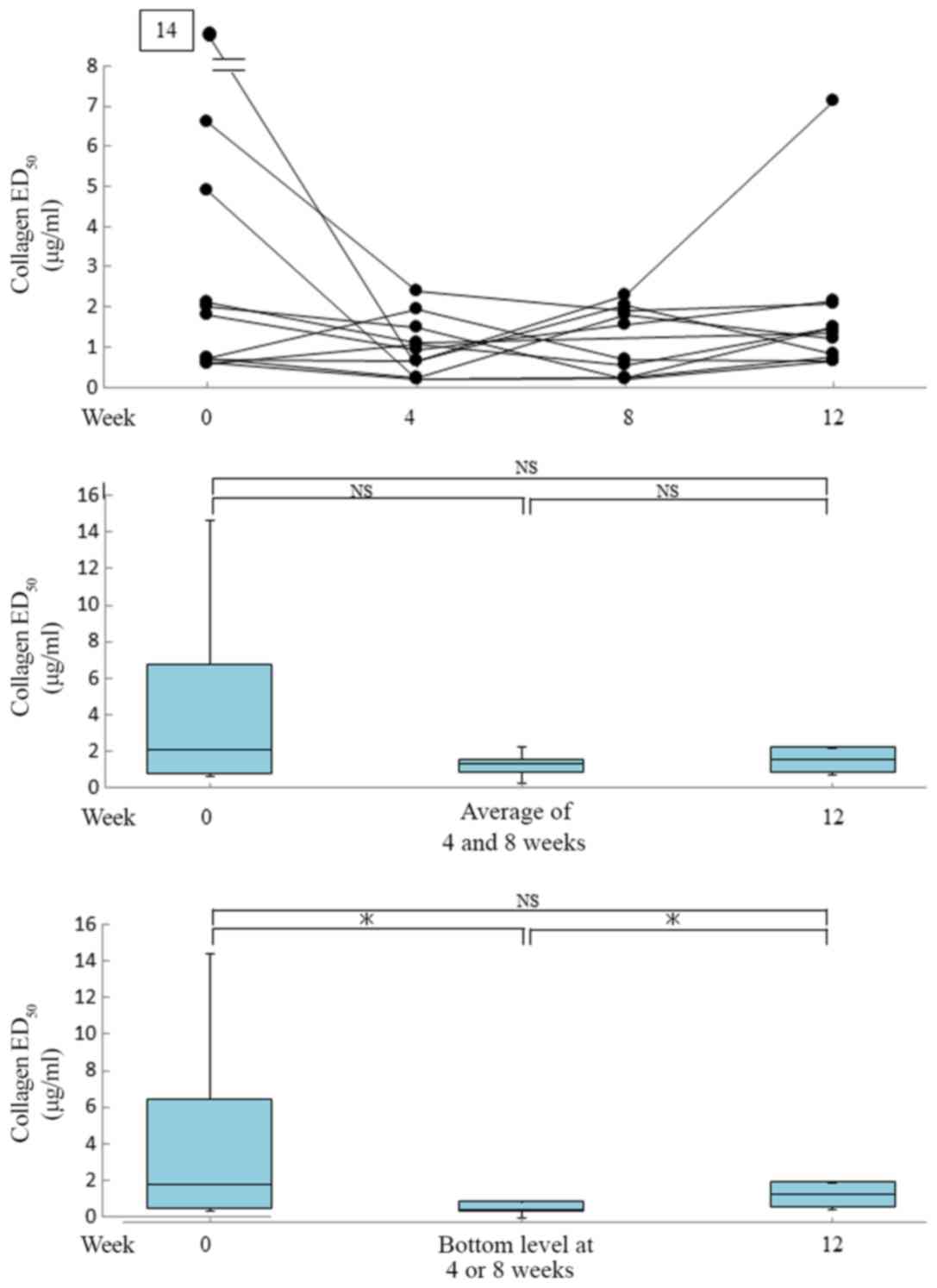
The bottom ED50 values of collagen (1
µg/ml) at 4 or 8 weeks after smoking cessation were significantly
lower the respective ED50 values before smoking
cessation, and at 12 weeks after the cessation, these values
returned to levels similar to those observed before the cessation
(Fig. 3).
Effect of smoking cessation on the
collagen-induced PDGF-AB secretion in human platelets
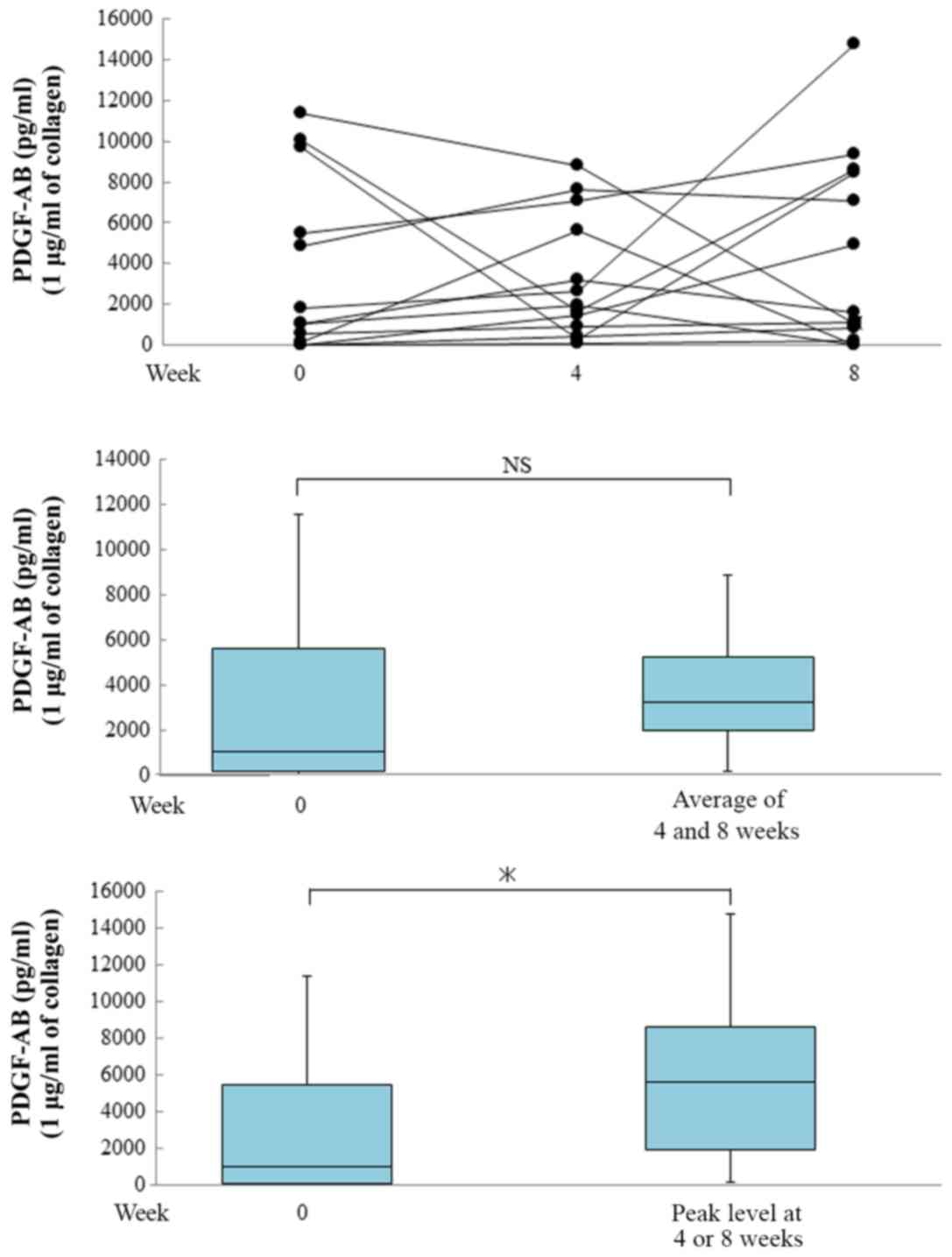
We previously reported that collagen induces PDGF-AB
secretion from human platelets (25). We further examined whether smoking
cessation affects the collagen-induced PDGF-AB secretion from human
platelets or not. The peak values of PDGF-AB at 4 or 8 weeks after
the cessation of smoking were significantly higher than before the
cessation (Fig. 4).
Considering the measured individual data, the peak
or bottom value seems to be at 4 or 8 weeks. However, there is a
trend but no statistically significant difference between 0, 4, 8
and 12 weeks (data not shown). We'd like to clarify the tendency of
short-term hyperactivation of human platelets at 4 or 8 weeks.
Therefore, we presented some plots weeks 4 and 8 together (Figs. 2–4).
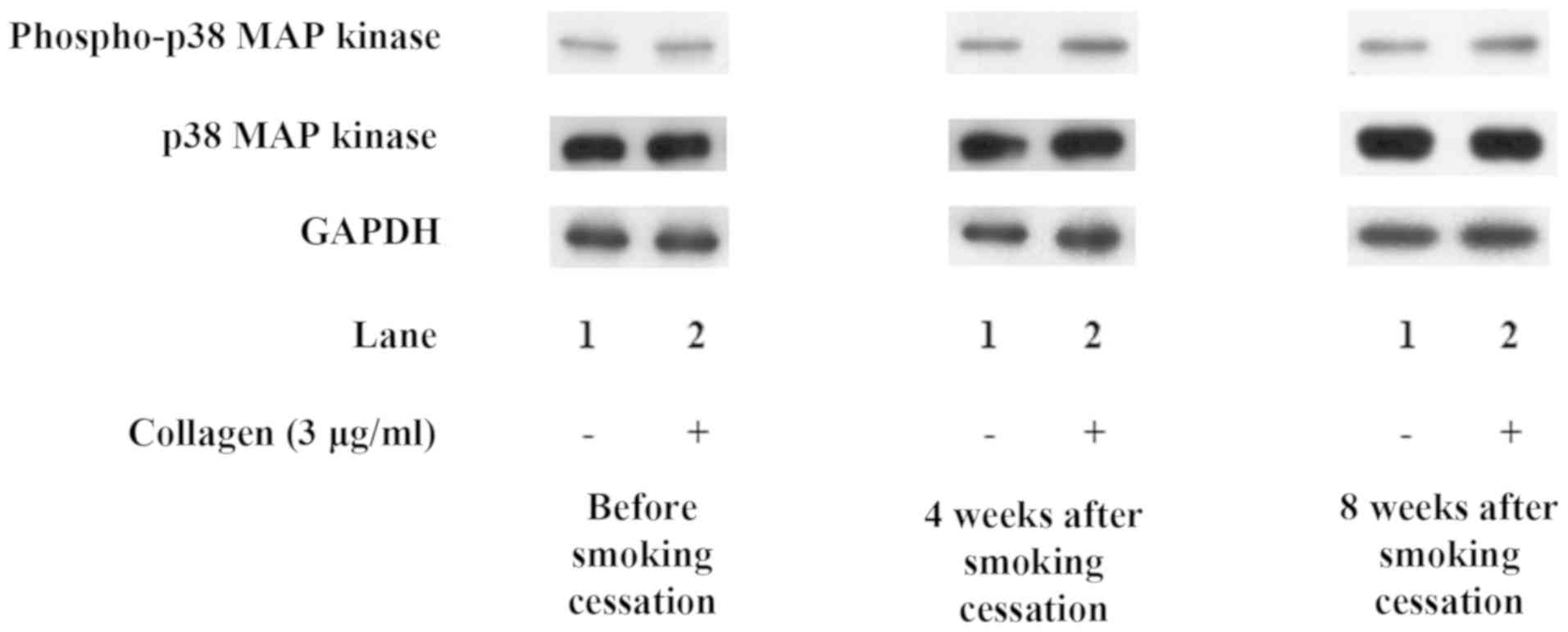
Effect of smoking cessation on the
collagen-induced phosphorylation of p38 MAP kinase in human
platelets
In our previous studies (17–20), we
demonstrated that collagen-induced PDGF-AB secretion is associated
with the activation of p38 MAP kinase in human platelets.
Therefore, we examined whether smoking cessation affects the
collagen-induced phosphorylation of p38 MAP kinase or not. Smoking
cessation markedly enhanced the levels of collagen-induced
phosphorylation of p38 MAP kinase at 4 weeks compared to before
smoking cessation, whereas the total p38 MAP kinase levels were not
affected. Though, there is no significant difference of the levels
of the collagen-induced phosphorylation of p38 MAP kinase between 4
and 8 weeks. Representative results are shown in Fig. 5.
Discussion
In the present study, we investigated the effect of
smoking cessation on human platelet activation. We showed that
cessation for 4 and 8 weeks induced a significantly increase in the
AUC (transmittance) of collagen (1 µg/ml)-induced platelet
aggregation and a decrease in the ED50 of collagen
compared with the values before smoking cessation. In addition,
smoking cessation affected the distribution of aggregated particle
sizes of human platelets as evaluated using laser scattering
methods. These results suggest that the platelet aggregation
induced by low-dose collagen (1 µg/ml) was temporarily up-regulated
by the smoking cessation. We also found that the collagen-induced
PDGF-AB secretion after cessation was temporarily amplified. In our
previous studies (18–20), we demonstrated that collagen or ADP
induces the secretion of PDGF-AB from human platelets associated
with the activation of p38 MAP kinase. From this viewpoint, we
focused on the effect of smoking cessation on the p38 MAP kinase
activation. We found that smoking cessation remarkably enhanced the
collagen-induced phosphorylation of p38 MAP kinase. Therefore,
smoking cessation may up-regulate the secretion of PDGF-AB by
collagen from human platelets associated with the enhancement of
p38 MAP kinase activation. These results newly suggest that smoking
cessation temporary causes hyper-reactivity of human platelets,
which is observed relatively short-term from 4 to 8 weeks after
cessation.
Platelet activation and aggregability are more
augmented in smokers than in non-smokers (5,6,26–29). A
previous report found that chronic exposure to cigarette smoke
sustains the activation of the endothelial-coagulative system, such
as by increasing vWF antigen, D-dimer, prothrombin fragment F1+2,
platelet factor-4 and beta-thromboglobulin, and smoking abstinence
may result in the improvement of several endothelial-coagulative
system abnormalities (30).
vWF activity decreases as early as 2 months after
starting smoking abstinence, and other circulating
endothelial-coagulative activation markers are substantially
modified at 6 and 12 months after smoking abstinence in regular
smokers (30). The mean platelet
volume, which is known to be a simple and convenient indicator for
platelet activation, is significantly higher in regular smokers
than in non-smokers (6,28) and decreases significantly at three
months after smoking cessation (28). In contrast, Morita et al
(14) reported that only two weeks
of smoking cessation in long-term smokers was able to ameliorate
the enhanced platelet aggregability and intraplatelet redox
imbalance. In present study, we examined the time-course changes in
the platelet function including the mechanism over 12-week at
4-week intervals. Our present findings showing that the
hyper-reactivity in human platelet was transient, occurring
relatively short-term after 4 to 8 weeks of smoking cessation, is
inconsistent with these previous reports. While we did not gather
data at very early timing (e.g. 1 and 2 weeks) of the smoking
cessation, smoking cessation might cause extremely complicated
changes in the platelet function. At the very least, our present
findings suggest that the time-dependent changes in the platelet
function through the persistence of smoking cessation require
physicians to monitor the temporary augmentation of the platelet
aggregability.
Smoking cessation is recommended before surgery. A
systematic review showed that the incidence of postoperative
complications, such as general morbidity, wound complications,
general infections and pulmonary or neurological complications, was
significantly higher in smokers than in non-smokers (31). It has been reported that current
smokers undergoing coronary artery bypass surgery have higher rates
of pulmonary complications, such as postoperative pneumonia,
pleural effusion and adult respiratory distress syndrome, than
non-smokers, with the risk declining in patients after more than
four weeks smoking cessation (32).
In addition, four weeks of preoperative smoking cessation reduced
the incidence of pulmonary complications after pulmonary surgery
(33). Turan et al (34) demonstrated that in non-cardiac
surgical patients, smoking was associated with a statistically
significant increase in cardiovascular complications: In their
large data set, there was a 57% increased chance of experiencing
30-day postoperative cardiac arrest, an 80% increased chance of
experiencing a myocardial infarction, and a 73% increase chance of
experiencing stroke.
However, conflicting findings have also been
reported; for example, a meta-analysis shows that the preoperative
smoking status was not associated with cardiovascular complications
(31). Surgical patients are at risk
of developing thrombo-embolism during the post-operative period
with and without smoking (12).
However, to our knowledge, there are no clinical reports describing
an increase in perioperative thrombus formation due to smoking
cessation. In the present study, we found that more than 4 to 8
weeks are needed to restore the human platelet function; however,
the precise duration required remains unclear. Although the
incidence of cardiovascular complications tended to decrease, no
statistically significant decrease (P=0.08) was observed after 6 to
8 weeks of smoking cessation in those who had undergone hip or knee
arthroplasty (35). In addition, we
could not elucidate the benefits of smoking cessation regarding the
prevention of cardiovascular complications (10,36). Our
present findings, which show the non-linear recovery of the human
platelet function according to smoking cessation, might provide a
possible explanation for the phenomenon in which postoperative
cardiovascular complications do not obviously decrease immediately
after smoking cessation. Physicians should take measures to avoid
thrombus formation in the perioperative period because smoking
cessation can induce temporary hyper-activation of platelets in the
short term. A longer duration of preoperative smoking cessation is
likely to be desirable, and anesthesiologists should recommend the
cessation of smoking as soon as possible before surgery. In
addition, the incidence of complications such as mortality or
pulmonary complications does not increase with short-term smoking
cessation (36,37), so it is not necessary to postpone an
operation even if patients have only stopped smoking for a short
while.
Several limitations associated with the present
study warrant mention. Both the self-assessment of patients and the
CO concentration of breathing were used for the confirmation of
smoking cessation. However, the expired CO concentration in smokers
who have refrained from smoking for >8 h is almost as low as
that in non-smokers. Therefore, the confirmation of complete
quitting smoking during the 12-week period depended largely on the
self-report of patients. Some patients had remarkable medical
histories, such as hypertension, diabetes and hyperlipidemia or
anti-platelet medication, which may have affected the platelet
aggregation.
In conclusion, our results strongly suggest that
smoking cessation causes the temporary hyper-activation of human
platelets in the short term (4 to 8 weeks). Our present findings
suggest that the incidence of complications due to hyper-reactivity
of human platelets can be reduced by paying attention to the
smoking abstinence period. We should give preoperative patients
clear and strong advice to quit smoking as soon as possible and
provide educational messages about the impact of smoking on
surgery.
Acknowledgments
The authors would like to thank Yumiko Kurokawa
(Department of Pharmacology, Gifu University Graduate School of
Medicine, Gifu, Japan) for her technical assistance.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YK and TO performed in vitro experiments and
collected the data. MI, KT and TI drafted the manuscript and
acquired the data. KN and MT performed statistical analysis. HT
constructed the in vivo model and the associated
experiments. OK and HI designed the present study, and drafted and
revised the manuscript. All authors critically reviewed the
manuscript and approved the final version for publication.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Gifu University Graduate School of Medicine (approval
no. 23-209) and Gifu Prefectural General Medical Center (approval
no. 30) All participants signed an informed consent agreement after
receiving a detailed explanation of the study protocol.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ambrose JA and Barua RS: The
pathophysiology of cigarette smoking and cardiovascular disease: An
update. J Am Coll Cardiol. 43:1731–1737. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Barua RS and Ambrose JA: Mechanisms of
coronary thrombosis in cigarette smoke exposure. Arterioscler
Thromb Vasc Biol. 33:1460–1467. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shinton R and Beevers G: Meta-analysis of
relation between cigarette smoking and stroke. BMJ. 298:789–794.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Price JF, Mowbray PI, Lee AJ, Rumley A,
Lowe GD and Fowkes FG: Relationship between smoking and
cardiovascular risk factors in the development of peripheral
arterial disease and coronary artery disease. Euro Heart J.
20:344–353. 1999. View Article : Google Scholar
|
|
5
|
Barua RS, Sy F, Srikanth S, Huang G, Javed
U, Buhari C, Margosan D and Ambrose JA: Effects of cigarette smoke
exposure on clot dynamics and fibrin structure an ex vivo
investigation. Arterioscler Thromb Vasc Biol. 30:75–79. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Swaminathan A, Amitkumar K, Ganapathy S
and Ayyavoo S: Evaluation of the impact of cigarette smoking on
platelet parameters. Natl J Physiol Pharm Pharmacol. 5:426–430.
2015. View Article : Google Scholar
|
|
7
|
Fusegawa Y, Goto S, Handa S, Kawada T and
Ando Y: Platelet spontaneous aggregation in platelet-rich plasma is
increased in habitual smokers. Thromb Res. 93:271–278. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Musallam KM, Rosendaal FR, Zaatari G,
Soweid A, Hoballah JJ, Sfeir PM, Zeineldine S, Tamim HM, Richards
T, Spahn DR, et al: Smoking and the risk of mortality and vascular
and respiratory events in patients undergoing major surgery. JAMA
Surg. 148:755–762. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hawn MT, Houston TK, Campagna EJ, Graham
LA, Singh J, Bishop M and Henderson WG: The attributable risk of
smoking on surgical complications. Ann Surg. 254:914–920. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wong J, Lam DP, Abrishami A, Chan MT and
Chung F: Short-term preoperative smoking cessation and
postoperative complications: A systematic review and meta-analysis.
Can J Anaesth. 59:268–279. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yousefzadeh A, Chung F, Wong DT, Warner DO
and Wong J: Smoking cessation: The role of the anesthesiologist.
Anesth Analg. 122:1311–1320. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bombeli T and Spahn DR: Updates in
perioperative coagulation: Physiology and management of
thromboembolism and haemorrhage. Br J Anaesth. 93:275–287. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chiang VL, Castleden WM and Leahy MF:
Detection of reversible platelet aggregates in the blood of smokers
and ex-smokers with peripheral vascular disease. Med J Aust.
156:601–603. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Morita H, Ikeda H, Haramaki N, Eguchi H
and Imaizumi T: Only two-week smoking cessation improves platelet
aggregability and intraplatelet redox imbalance of long-term
smokers. J Am Coll Cardiol. 4:589–594. 2005. View Article : Google Scholar
|
|
15
|
Stegner D and Nieswandt B: Platelet
receptor signaling in thrombus formation. J Mol Med (Berl).
89:109–121. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
André P, Nannizzi-Alaimo L, Prasad SK and
Phillips DR: Platelet-derived CD40L: The switch-hitting player of
cardiovascular disease. Circulation. 106:896–899. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Doi T, Adachi S, Matsushima-Nishiwaki R,
Kato H, Enomoto Y, Minamitani C, Otsuka T, Tokuda H, Akamatsu S,
Iwama T, et al: Antithrombin III suppresses ADP-induced platelet
granule secretion: Inhibition of HSP27 phosphorylation. Arch
Biochem Biophys. 489:62–67. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Enomoto Y, Adachi S, Matsushima-Nishiwaki
R, Niwa M, Tokuda H, Akamatsu S, Doi T, Kato H, Yoshimura S, Ogura
S, et al: AlphaB-crystallin extracellularly suppresses ADP-induced
granule secretion from human platelets. FEBS Lett. 583:2464–2468.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hanai Y, Adachi S, Yasuda I, Takai S,
Matsushima-Nishiwaki R, Kato H, Enomoto Y, Akamatsu S, Sakakibara
S, Ogura S, et al: Collagen-induced p38 MAP kinase activation is a
biomarker of platelet hyper-aggregation in patients with diabetes
mellitus. Life Sci. 85:386–394. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kato H, Adachi S, Doi T,
Matsushima-Nishiwaki R, Minamitani C, Akamatsu S, Enomoto Y, Tokuda
H, Otsuka T, Iwama T, et al: Mechanism of collagen-induced release
of 5-HT, PDGF-AB and sCD40L from human platelets: Role of HSP27
phosphorylation via p44/p42 MAPK. Thromb Res. 126:39–43. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tohgi H, Takahashi H, Watanabe K, Kuki H
and Shirasawa Y: Development of large platelet aggregates from
small aggregates as determined by laser-light scattering: Effects
of aggregant concentration and antiplatelet medication. Thromb
Haemost. 75:838–843. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tokuda H, Kato K, Kasahara S,
Matsushima-Nishiwaki R, Mizuno T, Sakakibara S and Kozawa O:
Significant correlation between the acceleration of platelet
aggregation and phosphorylation of HSP27 at Ser-78 in diabetic
patients. Int J Mol Med. 30:1387–1395. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kato K, Ito H, Hasegawa K, Inaguma Y,
Kozawa O and Asano T: Modulation of the stress-induced synthesis of
hsp27 and αB-crystallin by cyclic AMP in C6 rat glioma cells. J
Neurochem. 66:946–950. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Laemmli UK: Cleavage of structural
proteins during assembly of the head of bacteriophage T4. Nature.
227:680–685. 1970. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Rendu F and Brohard-Bohn B: The platelet
release reaction: Granules' constituents, secretion and functions.
Platelets. 12:263–271. 2001. View Article : Google Scholar
|
|
26
|
Ichiki K, Ikeda H, Haramaki N, Ueno T and
Imaizumi T: Long-term smoking impairs platelet-derived nitric oxide
release. Circulation. 94:3109–3114. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Haramaki N, Ikeda H, Takajo Y, Katoh A,
Kanaya S, Shintani S, Haramaki R, Murohara T and Imaizumi T:
Long-term smoking causes nitroglycerin resistance in platelets by
depletion of intraplatelet glutathione. Arterioscler Thromb Vasc
Biol. 21:1852–1856. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Varol E, Icli A, Kocyigit S, Erdogan D,
Ozaydin M and Dogan A: Effect of smoking cessation on mean platelet
volume. Clin Appl Thromb Hemost. 19:315–319. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Takajo Y, Ikeda H, Haramaki N, Murohara T
and Imaizumi T: Augmented oxidative stress of platelets in chronic
smokers. Mechanisms of impaired platelet-derived nitric oxide
bioactivity and augmented platelet aggregability. J Am Coll
Cardiol. 38:1320–1327. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Caponnetto P, Russo C, Di Maria A,
Morjaria JB, Barton S, Guarino F, Basile E, Proiti M, Bertino G,
Cacciola RR and Polosa R: Circulating endothelial-coagulative
activation markers after smoking cessation: A 12-month
observational study. Eur J Clin Invest. 41:616–626. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Grønkjær M, Eliasen M, Skov-Ettrup LS,
Tolstrup JS, Christiansen AH, Mikkelsen SS, Becker U and
Flensborg-Madsen T: Preoperative smoking status and postoperative
complications: A systematic review and meta-analysis. Ann Surg.
259:52–71. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Al-Sarraf N, Thalib L, Hughes A, Tolan M,
Youn V and McGovern E: Effect of smoking on short-term outcome of
patients undergoing coronary artery bypass surgery. Ann Thorac
Surg. 86:517–523. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nakagawa M, Tanaka H, Tsukuma H and Kishi
Y: Relationship between the duration of the preoperative smoke-free
period and the incidence of postoperative pulmonary complications
after pulmonary surgery. Chest. 120:705–710. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Turan A, Mascha EJ, Roberman D, Turner PL,
You JY, Kurz A, Sessler DI and Saager L: Smoking and perioperative
outcomes. Anesthesiology. 114:837–846. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Møller AM, Villebro N, Pedersen T and
Tønnesen H: Effect of preoperative smoking intervention on
postoperative complications: A randomised clinical trial. Lancet.
359:114–117. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Myers K, Hajek P, Hinds C and McRobbie H:
Stopping smoking shortly before surgery and postoperative
complications: A systematic review and meta-analysis. Arch Intern
Med. 171:983–989. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Mason DP, Subramanian S, Nowicki ER, Grab
DJ, Murthy SC, Rice TW and Blackstone EH: Impact of smoking
cessation before resection of lung cancer: A Society of Thoracic
Surgeons General Thoracic Surgery Database study. Ann Thorac Surg.
88:362–371. 2009. View Article : Google Scholar : PubMed/NCBI
|