Introduction
Lung cancer, the biggest contributor to
cancer-associated mortality worldwide, has a severe impact on
public health (1). At present, the
5-year survival rate for lung cancer is only 18%, which is in
contrast with the stable increase in the survival rates of other
types of cancer (2). Among all lung
cancer subtypes, non-small cell lung cancer (NSCLC) accounts for
~85%. Of note, lung adenocarcinoma (LUAD) is the most common and
malignant pathological type of NSCLC (3). Although the 5-year survival rate of
LUAD has increased with the emergence of targeted drugs, the
mortality rate remains high due to the lack of effective diagnostic
and prognostic biomarkers (4,5). To
reduce the mortality rate of patients with LUAD, it is therefore
essential to establish a good prognostic signature to guide the
patients' treatment and clinical management.
It has been reported that ~90% of mammalian genomes
are transcribed into non-coding RNA (ncRNA) (6). Long ncRNAs (lncRNAs) are one of the
most important classes of the ncRNA family and are >200
nucleotides in length (7).
Accumulating studies have suggested that certain lncRNAs have
mutations or changes in expression levels in various types of
cancer (8–10). Differentially expressed lncRNAs are
involved in the aberrant processes of cancer, including cell cycle,
apoptosis and chemoresistance (11).
These cancer-associated lncRNAs have a critical role in
tumorigenesis and metastasis through different mechanisms,
including regulating the gene expression by serving as a guide to
target chromatin-modifying complexes to a specific gene location or
acting as a competing endogenous (ce)RNA that competitively binds
to microRNA (miR) to regulate gene expression (12). With the importance of lncRNAs in
cancer recognized, an increasing number of studies have explored
the function of lncRNA in NSCLC. For instance, certain significant
lncRNAs with a gene regulatory mechanism in LUAD were discovered
through pathway crosstalk analysis (13) and several of them were identified to
have the potential to act as therapeutic targets or diagnostic
markers for NSCLC (14–16). It is also critical to explore the
association between lncRNAs and cancer prognosis. To date,
lncRNA-associated prognostic signatures have been established in
several types of cancer, including gastric cancer (17), urothelial carcinoma (18) and hepatocellular carcinoma (19). Numerous prognostic lncRNA signatures
have been reported for various lung cancer subtypes, including lung
squamous cell carcinoma (20), NSCLC
(21) and NSCLC in elderly subjects
(22). Of course, numerous studies
have explored the association between lncRNA and the prognosis of
LUAD. lncRNAs serving as prognostic biomarkers for LUAD were
identified through a ceRNA network analysis (23). A prognostic signature based on lncRNA
suggested the existence of a tumor protein 53-dependent subtype of
LUAD with poor survival (24).
Prognostic signatures for LUAD constructed from lncRNA or lncRNA
combined with mRNA have also been reported (25,26).
However, to date, no ideal lncRNA signature has been developed for
use in the clinical setting, possibly due to limited sample size
and lack of systematic investigation. The lncRNA signature
established in the present study may provide a reference value for
building the prognostic signature that may be applied in the
clinic.
In the present study, a 5-lncRNA signature with good
reliability and stability in the prognostication of patients with
LUAD was successfully established. The predictive ability of the
prognostic signature was independent of other clinical factors. The
results of the functional enrichment analysis demonstrated that the
5 lncRNAs may be involved in the tumorigenesis of LUAD. In short,
the present study provided an lncRNA signature that may be utilized
for survival prediction of patients with LUAD.
Materials and methods
LUAD database and clinical information
of patients
The lncRNA expression profiles of 535 LUAD tumor and
49 non-tumor tissues, as well as the clinical information of 504
patients with LUAD, were downloaded from the official website of
The Cancer Genome Atlas (TCGA; http://gdc-portal.nci.nih.gov/). After excluding those
patients with incomplete clinical information, the data of 486
patients were retained for analysis in the present study. The
correlative clinical information included overall survival (OS),
age, sex and TNM stage. The 486 patients were randomly divided into
two cohorts. Of these, 264 LUAD patients were used as a training
cohort to build a prognostic signature, while the 222 remaining
LUAD patients were used as the verifying cohort to test the
prognostic ability of the signature. Detailed information on the
cohorts used in the present study is provided in Table I.
 | Table I.Clinical characteristics of lung
adenocarcinoma patients in the present study. |
Table I.
Clinical characteristics of lung
adenocarcinoma patients in the present study.
|
Characteristics | Training cohort
(n=264) | Verifying cohort
(n=222) | Total cohort
(n=486) |
|---|
| Vital status |
|
Alive | 163 (61.7) | 145 (65.3) | 308 (63.4) |
|
Dead | 101 (38.3) | 77 (34.7) | 178 (36.6) |
| Age (years) |
|
<65 | 121 (45.8) | 95 (42.8) | 216 (44.4) |
|
≥65 | 143 (54.2) | 127 (57.2) | 270 (55.6) |
| Sex |
|
Female | 143 (54.2) | 120 (54.1) | 263 (54.1) |
|
Male | 121 (45.8) | 102 (45.9) | 223 (45.9) |
| Stage |
| I | 143 (54.2) | 120 (54.1) | 263 (54.1) |
| II | 58 (22.0) | 59 (26.6) | 117 (24.1) |
|
III/IV | 63 (23.8) | 43 (19.3) | 106 (21.8) |
Acquisition and processing of lncRNA
expression profiles for LUAD patients
The expression profiles were acquired for 17,109
mRNAs and 1,787 lncRNAs after adding annotation using the Ensemble
database (http://asia.ensembl.org/index.html). Next, the R
package ‘edgeR’ (27) was used to
log2-transform the RNA-sequencing expression values and
normalize the data and differential expression analysis, using
log2|fold change|>1 and adjusted P<0.05 as the
threshold to screen out differentially expressed RNAs. A total of
841 differentially expressed lncRNAs were screened.
Acquisition and processing of lncRNA
expression profiles for LUAD from the gene expression omnibus (GEO)
database
A total of three GEO datasets were downloaded, which
contained gene expression, clinical information and the platform
annotation file (GPL570-Affymetrix Human Genome U133 Plus 2.0
Array) from the National Center for Biotechnology Information
(NCBI) GEO database (http://www.ncbi.nlm.nih.gov/geo). The average
expression value of a gene was used when it corresponded to
multiple probes. After converting the probe information to gene
symbols, the three datasets were merged and the expression levels
of different batches were normalized using the R package ‘sva’. A
total of 418 patients with LUAD were included in the present study,
comprising 204 patients from the dataset GSE31210, 85 patients from
GSE30219 and 129 patients from GSE50081.
Construction of a prognostic lncRNA
signature
In the training cohort, univariate Cox regression
analysis was used to evaluate the association between the
expression of each differentially expressed lncRNA and the OS of
patients with LUAD. Considering the number of lncRNAs selected and
their association with prognosis, those lncRNAs with P<0.001
were considered as candidate lncRNAs. These candidate lncRNAs were
further subjected to multivariate Cox regression analysis to select
a set of lncRNAs, thereby establishing an RS model. The
multivariate Cox regression analysis was performed using a
mathematical model based on the Akaike Information Criterion (AIC)
(28). The model based on the AIC
was used to construct a prognostic signature with the best
predictive ability but the least number of lncRNAs. The calculation
formula of the RS was as follows:
RS=∑(i=1)N(ExpixCoei), where N represents
the total number of prognostic lncRNAs, Expi the expression
of a certain lncRNA and Coei the regression coefficient
obtained from the multivariate Cox regression analysis for a
certain lncRNA numbered as i. Based on this equation, each patient
with LUAD had an RS and the median RS was treated as a cut-off
point to stratify the patients into low- and high-risk groups.
Univariate and multivariate Cox regression analysis was performed
using the Survival R package from the CRAN package repository
(https://cran.r-project.org/web/packages/).
Statistical analysis
Kaplan-Meier survival analysis and two-sided
log-rank tests were used to evaluate the difference in OS between
low- and high-risk groups in each cohort. The Kaplan-Meier survival
analysis was performed using the Survival R package. After the
patients with LUAD were divided into multiple groups according to a
certain clinical factor, the Kruskal-Wallis test was used to
analyze whether a certain lncRNA was significantly influenced by
this clinical factor. The accuracy of the prognostic signature in
predicting the 5-year survival rate was assessed using
time-dependent receiver operating characteristic (ROC) analysis.
ROC analysis was performed using the R package ‘survivalROCR’
(29). The area under the ROC curve
(AUC) was calculated. Univariate Cox regression analysis was
performed in each cohort to test whether the prognostic signature
was associated with the survival of patients with LUAD.
Multivariate Cox regression and stratification analysis were
further performed in each cohort to test whether the prognostic
signature had an independent predictive value regarding survival.
At the same time, the hazard ratio (HR) and 95% confidence interval
(CI) were determined. At RT-qPCR data were analyzed using GraphPad
Prism 8.0 (GraphPad Software, Inc.). Significant differences of
reverse transcription-quantitative PCR (RT-qPCR) data were analyzed
using a unpaired Student's t-test, and P<0.05 was considered to
indicate a statistically significant difference.
Predicting the functions and pathways
of lncRNAs
The Pearson's correlation coefficients for the
correlation between the prognostic lncRNAs and protein-coding genes
were calculated in order to select co-expressed PCGs. Genes
significantly co-expressed with at least one of the prognostic
lncRNAs were treated as lncRNA-associated PCGs (|Pearson's
correlation coefficient|>0.40 and P<0.01). Gene ontology (GO)
enrichment analysis for the co-expressed PCGs was performed using
the Database for Annotation, Visualization and Integrated Discovery
(DAVID) bioinformatics tool (https://david.ncifcrf.gov/) (30) and the GO terms were limited to
‘Biological Process’. Kyoto Encyclopedia of Genes and Genomes
(KEGG) pathway analysis for the co-expressed PCGs was performed
using the KO-based Annotation System bioinformatics tool
(http://kobas.cbi.pku.edu.cn/) (31) with the entire human genome as the
background. The results of the functional enrichment analysis with
a P<0.005 were regarded as the potential biological functions.
Enriched GO terms with similar function were clustered and the
major categories of clustering were visualized through the
Enrichment Map plugin (32) in
Cytoscape (33). Significantly
enriched KEGG pathways were visualized with the R package ‘ggplot2’
(34).
RT-qPCR verification of lncRNA
expression in LUAD tissues and cell lines
A total of 14 paired LUAD and adjacent non-tumor
tissue samples were used in the present study, which were collected
at the Second Affiliated Hospital of Xian Jiaotong University
(Xian, China) between March 2017 and December 2018. The study
protocol was approved by the Ethics Committee of the Second
Affiliated Hospital of Xian Jiaotong University (Xian, China) and
ethics consent had been received written informed consents from all
participating patients. Detailed clinical information of these
patients are presented in Table SI.
The human lung cancer cell lines A549, PC-9 and H1299 and the
normal human lung epithelial cell line BEAS-2B were purchased from
the Type Culture Collection Cell Bank of the Chinese Academy of
Sciences (Shanghai, China). All cell lines were cultured in
RPMI-1640 (Hyclone; GE Healthcare Life Sciences) containing 10% FBS
at 37°C in a 5% CO2 incubator. Total RNA was extracted
from lung tissues using Fast1000 (Xfyangbio) and from cell lines
using Fast 200 (Xfyangbio). The total RNA was reverse-transcribed
using the PrimerScript™ RT reagent kit (Takara Biotechnology Co.,
Ltd.). The reverse transcription mixture was incubated at 37°C for
15 min and 85°C for 5 sec. The TB Green® Premix Ex Taq™
II (Takara Biotechnology Co., Ltd.) was used for detecting the gene
amplification and qPCR was performed on the CFX96 Touch™ Real-Time
PCR Detection System (Bio-Rad Laboratories, Inc.). The qPCR
reaction mixture was incubated at 95°C for 30 sec, followed by 40
cycles of 95°C for 3 sec and 60°C for 30 sec. The PCR primers for
the 5 lncRNAs are listed in Supplemental Table SII. All experimental procedures were
performed according to the manufacturer's protocol and all
reactions were performed in triplicate. The 2−ΔΔCq
method (35) was used to calculate
the expression of lncRNAs and β-actin was used as an internal
reference.
Results
Construction of a 5-lncRNA signature
to predict the OS of patients with LUAD
First, each of the 841 differentially expressed
lncRNAs was subjected to univariate Cox regression analysis in the
training cohort. A total of 7 lncRNAs were selected as candidate
lncRNAs (P<0.001). These candidate lncRNAs were then further
subjected to multivariate Cox regression analysis. Finally, five
lncRNAs, including neuropeptide S receptor 1-antisense RNA 1
(NPSR1-AS1), opioid growth factor receptor pseudogene 1 (OGFRP1),
integrin subunit beta 1 divergent transcript (ITGB1-DT), LIM domain
7 downstream neighbor (LMOTDN) and protein kinase cyclic
GMP-dependent 1-antisense RNA 1 (PRKG1-AS1), were selected to
construct a risk model. According to the results of the
multivariate Cox regression analysis, an RS model was successfully
established, as per the following equation: RS=(0.155 × NPSR1-AS1
expression) + (0.419 × OGFRP1 expression) + (0.109 × ITGB1-DT
expression) + (−0.186 × LMOTDN expression) + (0.151 × PRKG1-AS1
expression). The 5 lncRNAs were differentially expressed in 535
tumor vs. 49 non-tumor tissues (P<0.0005; Fig. S1). Detailed information about the 5
lncRNAs is provided in Table
II.
| Table II.The five long non-coding RNAs
significantly associated with prognosis of lung adenocarcinoma
patients in the training cohort. |
Table II.
The five long non-coding RNAs
significantly associated with prognosis of lung adenocarcinoma
patients in the training cohort.
| Gene name | Ensemble ID | Chromosomal
position | Hazard
ratioa |
Coefficienta |
P-valuea |
|---|
| OGFRP1 |
ENSG00000182057.4 | chr22:
42,269,753-42,275,196 | 1.52
(1.18–1.97) | 0.419 | 0.001 |
| ITGB1-DT |
ENSG00000229656 | chr10:
32,958,845-33,082,102 | 1.12
(1.01–1.23) | 0.109 | 0.023 |
| LMO7DN |
ENSG00000178734 | chr13:
75,871,038-75,883,811 | 0.83
(0.72–0.96) | −0.186 | 0.014 |
| NPSR1-AS1 |
ENSG00000197085.7 | chr7:
34,346,512-34,871,582 | 1.17
(1.04–1.31) | 0.155 | 0.008 |
| PRKG1-AS1 |
ENSG00000236671 | chr10:
52,230,742-52,314,507 | 1.16
(1.13–1.31) | 0.151 | 0.015 |
The 5-lncRNA signature predicted the
OS of patients with LUAD in the training cohort
Based on the RS equation, the RS of each patient
with LUAD was calculated in the training cohort. The results
suggested that the median RS was 2.593. The 264 patients with LUAD
in the training cohort were divided into high-(n=132) and low-risk
groups (n=132) with RS=2.593 as the cut-off point. The Kaplan-Meier
survival analysis indicated that the median survival of LUAD
patients in the high-risk group was significantly shorter (1.63
years) than that in the low-risk group (1.91 years;
P=1.418×10−6; Fig. 1A).
Specifically, the 3-, 5- and 8-year survival rates were 47.5, 6.2
and 0.0% in the high-risk group, and 68.9, 45.1 and 31.6% in the
low-risk group, respectively. From the time-dependent ROC curve, it
was determined that the AUC value was 0.784 for the 5-lncRNA
signature to predict the 5-year survival rate in the training
cohort, indicating excellent reliability of the prognostic
signature in predicting survival. The ROC curve is presented in
Fig. 1B. The risk distribution and
vital status of 264 LUAD patients from the training cohort are
presented in Fig. 1C, and heatmap of
the 5 lncRNAs expression profiles in training cohort is presented
in Fig. 1D. Of these 5 lncRNAs, high
expression of NPAR1-AS1, OGFRP1, ITGB1-DT and PRKG1-AS1 indicated
to be associated with high RSs, while high expression of LMOTDN was
associated with a low RS. Furthermore, the number of mortalities in
the low-risk group was lower than that in the high-risk group.
Univariate Cox regression analysis was performed on the 5-lncRNA
signature in the training cohort. The results suggested that the
prognostic signature was significantly linked to the survival of
LUAD patients (P<0.001, HR=2.743, 95% CI=1.792–4.200). More
detailed results are provided in Table
III.
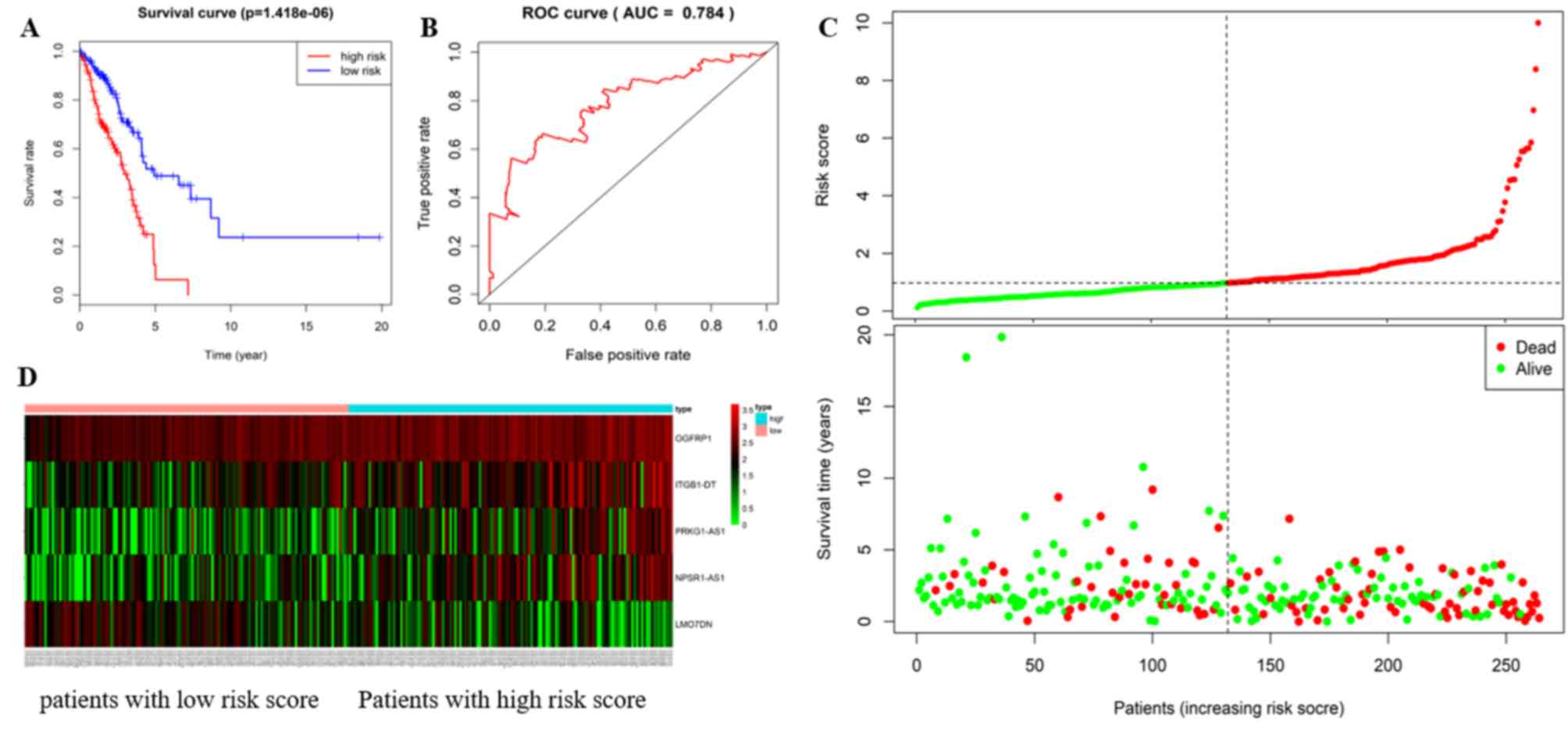 | Figure 1.The 5 lncRNAs are able to predict
overall survival in the training cohort. (A) Kaplan-Meier survival
curves, (B) ROC curve for the training cohort, and the AUC value
more than 0.7 is considered to be reliable. (C) risk distribution,
survival status of patients and (D) heatmap of the 5 lncRNAs
expression profiles in the training cohort. The ‘+’ on the survival
curves represents the censored data-points. lncRNA, long non-coding
RNA; ROC, receiver operating characteristic; AUC, area under ROC
curve; OGFRP1, opioid growth factor receptor pseudogene 1;
ITGB1-DT, integrin subunit beta 1 divergent transcript; LMO7DN, LIM
domain 7 downstream neighbor; NPSR1-AS1, neuropeptide S receptor
1-antisense RNA 1; PRKG1-AS1, protein kinase cyclic GMP-dependent
1-antisense RNA 1. |
| Table III.Univariate and multivariate Cox
regression analysis in each cohort. |
Table III.
Univariate and multivariate Cox
regression analysis in each cohort.
| A, Training cohort
(n=264) |
|---|
|
|---|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | HR | 95% CI of HR | P-value | HR | 95% CI of HR | P-value |
|---|
| Five-lncRNA risk
score (high/low risk) | 2.743 | 1.792–4.200 | <0.001 | 2.418 | 1.566–3.736 | <0.001 |
| Age (≥65/<65
years) | 1.006 | 0.680–1.490 | 0.975 | 1.013 | 0.681–1.508 | 0.949 |
| Sex
(female/male) | 1.078 | 0.724–1.603 | 0.712 | 1.026 | 0.682–1.542 | 0.903 |
| Stage |
|
|
|
|
|
|
| (II vs.
I) | 3.028 | 1.855–4.943 | <0.001 | 2.583 | 1.568–4.253 | <0.001 |
| (III/IV
vs. I) | 2.837 | 1.774–4.537 | <0.001 | 2.517 | 1.563–4.054 | <0.001 |
|
| B, Verification
cohort (n=222) |
|
|
| Univariate
analysis | Multivariate
analysis |
|
|
|
|
|
Variables | HR | 95% CI of
HR | P-value | HR | 95% CI of
HR | P-value |
|
| Five-lncRNA risk
score (high/low risk) | 1.962 | 1.232–3.127 | 0.005 | 1.925 | 1.201–3.085 | 0.007 |
| Age (≥65/<65
years) | 1.369 | 0.860–2.181 | 0.185 | 1.442 | 0.886–2.283 | 0.145 |
| Sex
(female/male) | 0.734 | 0.468–1.150 | 0.177 | 0.819 | 0.521–1.288 | 0.388 |
| Stage |
|
|
|
|
|
|
| (II vs.
I) | 1.655 | 0.944–2.902 | 0.079 | 1.692 | 0.948–3.020 | 0.075 |
| (III/IV
vs. I) | 4.297 | 2.458–7.429 | <0.001 | 4.515 | 2.571–7.929 | <0.001 |
|
| Total cohort
(n=486) |
|
|
| Univariate
analysis | Multivariate
analysis |
|
|
|
|
|
Variables | HR | 95% CI of
HR | P-value | HR | 95% CI of
HR | P-value |
|
| Five-lncRNA risk
score (high/low risk) | 2.225 | 1.636–3.027 | <0.001 | 2.117 | 1.550–2.891 | <0.001 |
| Age (≥65/<65
years) | 1.147 | 0.851–1.547 | 0.368 | 1.198 | 0.887–1.619 | 0.239 |
| Sex
(female/male) | 0.909 | 0.677–1.220 | 0.524 | 0.915 | 0.680–1.232 | 0.559 |
| Stage |
|
|
|
|
|
|
| (II vs.
I) | 2.318 | 1.606–3.347 | <0.001 | 2.204 | 1.520–3.197 | <0.001 |
| (III/IV
vs. I) | 3.371 | 2.370–4.795 | <0.001 | 3.284 | 2.301–4.687 | <0.001 |
Evaluation of the advantages of the
5-lncRNA signature
To evaluate the possible advantages of the 5-lncRNA
signature in predicting the survival of LUAD patients, the same
data and methods as those above were used to analyze the
differentially expressed mRNAs. A total of 25 mRNAs significantly
associated with OS (P<0.001) were obtained. The top 7 mRNAs were
subjected to multivariate Cox analysis and a 5-mRNA signature,
including family with sequence similarity 189 member A2, collagen
type XXII alpha 1 chain (COL22A1), C1q and tumor necrosis factor
related 6 (C1QTNF6), neurotensin receptor 1 (NTSR1) and cell death
inducing DNA fragmentation factor subunit alpha like effector c,
was obtained. The AUC value of the 5-mRNA signature to predict the
5-year survival rate of LUAD patients was 0.726 (Fig. S2). Subsequently, the same data and
methods were used to analyze the differentially expressed lncRNA
and mRNA together, and a total of 32 genes closely linked to
survival were obtained (P<0.001). The top 7 genes were subjected
to on multivariate COX analysis, and a 4-gene signature consisting
of 2 lncRNAs (OGFRP1 and LINC01322) and 2 mRNAs (COL22A1 and NTSR1)
was obtained. The AUC value of the 4-gene signature in predicting
the 5-year survival of LUAD patients was 0.738 (Fig. S3). It is worth mentioning that 16 of
the 25 mRNAs significantly associated with the prognosis were
included in the co-expressed PCGs of the 5 lncRNAs obtained in the
present study. The 5-lncRNA signature had a higher AUC value
compared with the 5-mRNA and 4-gene signatures, which indicated
that 5-lncRNA signature was more reliable in predicting prognosis.
Considering the accuracy and complexity of the predictive model,
the 5-lncRNA signature had certain advantages in predicting
survival.
Verification of the ability of the
5-lncRNA signature to predict the OS of patients with LUAD
The ability of the 5-lncRNA signature to predict
survival was further assessed in the verification and total
cohorts. Based on the RS equation, the RS of each patient with LUAD
in the verification and total cohort was calculated. With the
median RS of 2.539 as the cut-off point, 222 LUAD patients in the
verification cohort and 486 LUAD patients in the total cohort were
classified into high- and low-risk groups (n=113 and 109, and n=245
and 241, respectively). The results of the Kaplan-Meier survival
analysis for the verification and total cohorts were consistent
with those in for training cohort. In the verification cohort, the
median survival of LUAD patients in the high- and low-risk group
was 1.66 and 2.12 years, respectively (P=3.861×10−3;
Fig. 2A). The 3-, 5- and 8-year
survival rates were 44.3, 25.9 and 0.0% in the high-risk group, and
71.0, 45.1 and 30.1% in the low-risk group, respectively. In the
total cohort, the median survival of patients with LUAD in the
high- and low-risk groups was 1.64 and 1.95 years, respectively
(P=1.724×10−7; Fig. 2B).
The 3-, 5- and 8-year survival rates were 47.3, 22.4 and 0.0% in
the high-risk group, and 71.0, 47.4 and 37.6% in the low-risk
group, respectively.
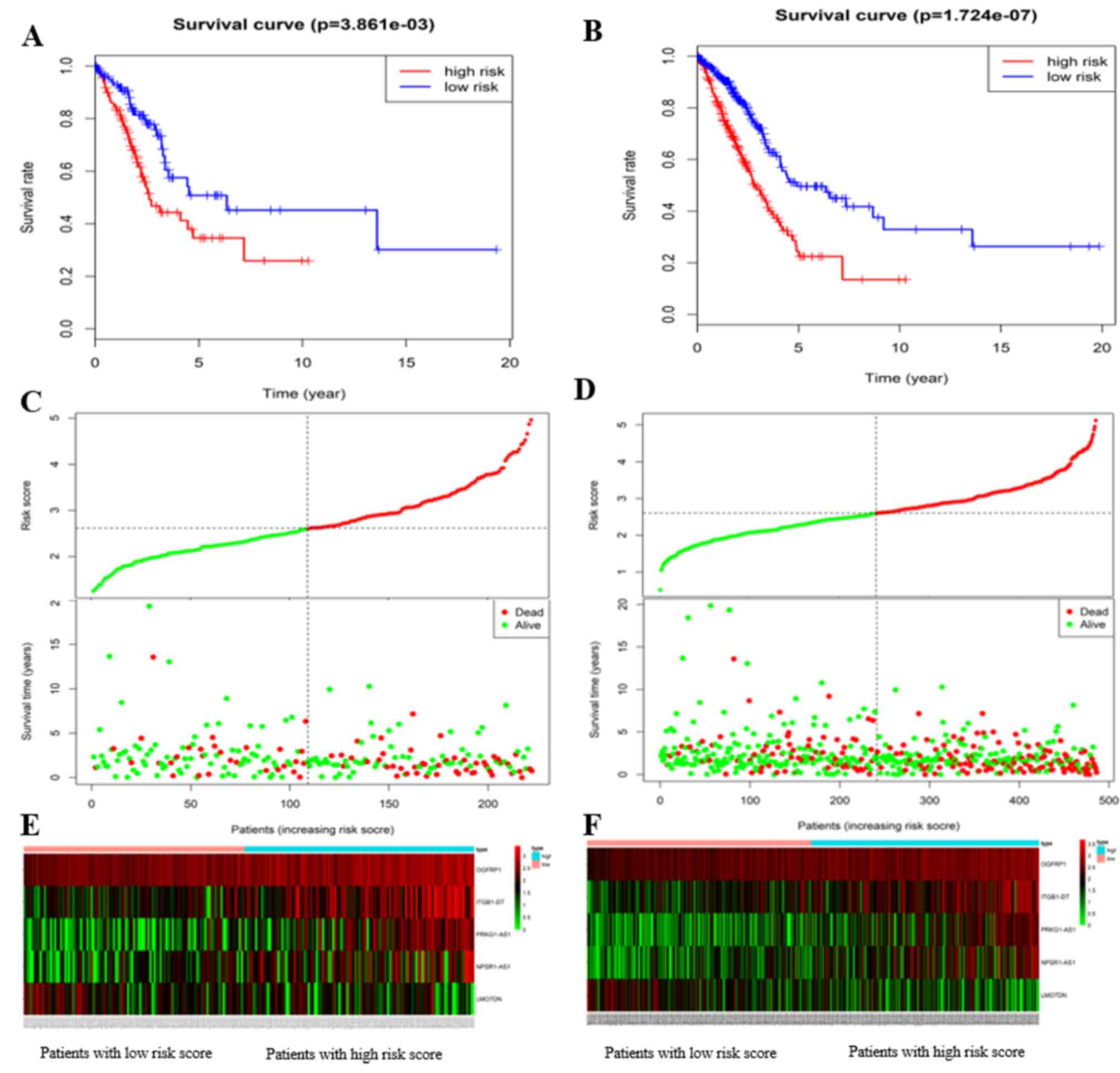
The risk distribution and vital status in LUAD
patients from the verification and total cohorts are presented in
Fig. 2C and D, the heatmap of the 5
lncRNAs expression profiles in verification and total cohorts are
presented in Fig. 2E and F,
respectively. As expected, the patients with high-risk LUAD had the
tendency to express the high-risk lncRNAs, while the protective
lncRNA was upregulated in low-risk patients. Mortality rate in the
high-risk group was higher than that in the low-risk group
(verification cohort: 41.6% vs. 27.5%; total cohort: 44.9% vs.
28.2%). Univariate Cox regression analysis was performed on the
5-lncRNA signature in these two cohorts. Similar results to those
obtained in the training cohort were obtained: The prognostic
signature was closely associated with survival (verification
cohort: P=0.005, HR=1.962, 95% CI=1.232–3.127; total cohort:
P<0.001, HR=2.225, 95% CI=1.636–3.027). More detailed results
are listed in Table III. In short,
the results indicated that the 5-lncRNA signature had good
reliability and stability in predicting the survival of patients
with LUAD.
The 5-lncRNA signature is an
independent predictor of survival
Multivariate Cox regression analysis was performed
on the 5-lncRNA signature in each cohort to assess whether the
predictive ability of the prognostic signature was independent of
other clinical factors, including sex age and TNM stage. In the
multivariate Cox regression analysis, the OS was used as a
dependent variable and the other clinical factors were regarded as
covariates. The results indicated that the 5-lncRNA signature was
significantly associated with the OS of patients with LUAD after
adjustment by the other clinical factors in all cohorts (HR=2.418,
95% CI, 1.566–3.736, P<0.001 in the training cohort; HR=1.925,
95% CI, 1.201–3.085, P=0.007 in the verification cohort; HR=2.117,
95% CI, 1.550–2.891, P<0.001 in the total cohort). More detailed
results are listed in Table III.
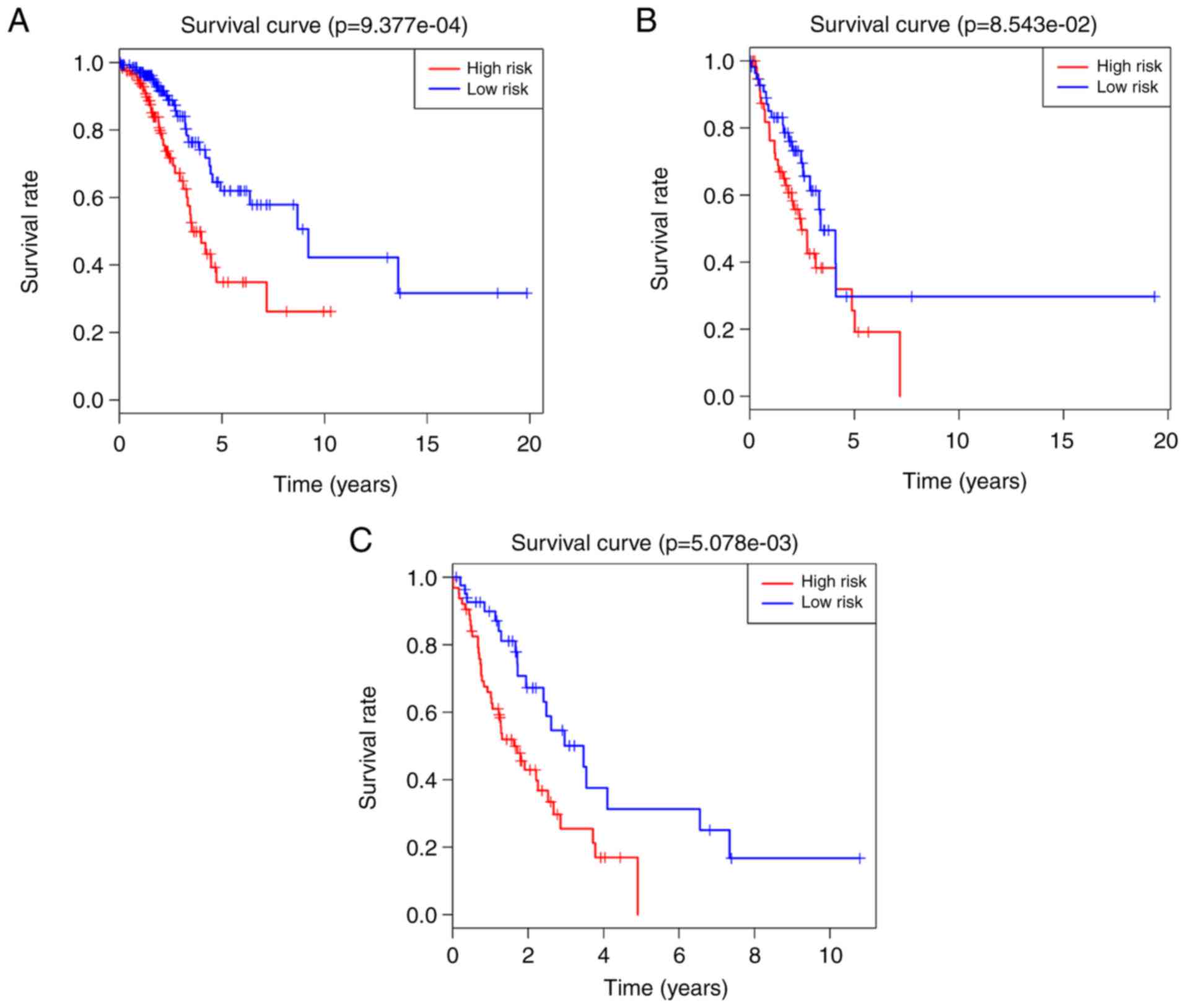
However, it was indicated that the TNM stage was also significantly
associated with survival. Therefore, a data stratification analysis
was performed to evaluate whether the prognostic signature still
had a predictive value at the same TNM stage. All 486 patients with
LUAD were stratified into three groups according to their TNM
stage: The stage I (n=263), stage II (n=117) and stage III/IV
(n=106) groups. With the median RS derived from the training cohort
as a cut-off point, the stage I, II and III/IV groups were divided
into high- (n=122, n=59 and n=64) and low-risk groups (n=141, n=58
and n=42), respectively. Significant differences in OS were
observed between the high- and low-risk groups (log-rank test
P=9.377×10−4, median survival: 1.67 vs. 2.08 years in
the stage I group, Fig. 3A; log-rank
test P=8.543×10−2; median survival: 1.73 vs. 1.90 years
in the stage II group, Fig. 3B;
log-rank test P=5.078×10−3; median survival: 1.25 vs.
1.72 years in the stage III/IV group, Fig. 3C). Although the P-value of the stage
II group was above the significance level, a significant difference
in median survival was observed between the high- and low-risk
groups. These results demonstrated that the 5-lncRNA signature was
an independent survival predictor for patients with LUAD.
Verification of the 5-lncRNA signature
in GEO datasets
In order to determine the value of the 5-lncRNA
signature in predicting survival, GEO datasets were analyzed.
However, when the 5 lncRNAs were searched in GEO datasets, the
expression data of ITGB1-DT appeared not to be available. The 4
remaining lncRNAs were analyzed in a cohort composed of three GEO
datasets (GSE30210, GSE30219 and GSE50081). As expected, the
results indicated that OGFRP1, PRKG1-AS1 and LMO7DN were closely
associated with the survival of patients with LUAD (P<0.001;
Fig. 4). Among them, OGFRP1 and
PRKG1-AS1 were risk factors for patients with LUAD, as their high
expression was associated with poor survival, while LMO7DN acted as
a protective factor, whose high expression was associated with a
favorable outcome. Although there was no significant association
between NPSR1-AS1 and survival in this cohort, the median survival
in the high-expression group (4.54 years) was lower than that in
the low-expression group (5.09 years) when the LUAD patients were
divided into two groups with the median value of its expression
used as a cut-off point. Based on the expression of the 4 lncRNAs
in the GEO datasets, the reliability of the 5-lncRNA signature was
further confirmed.
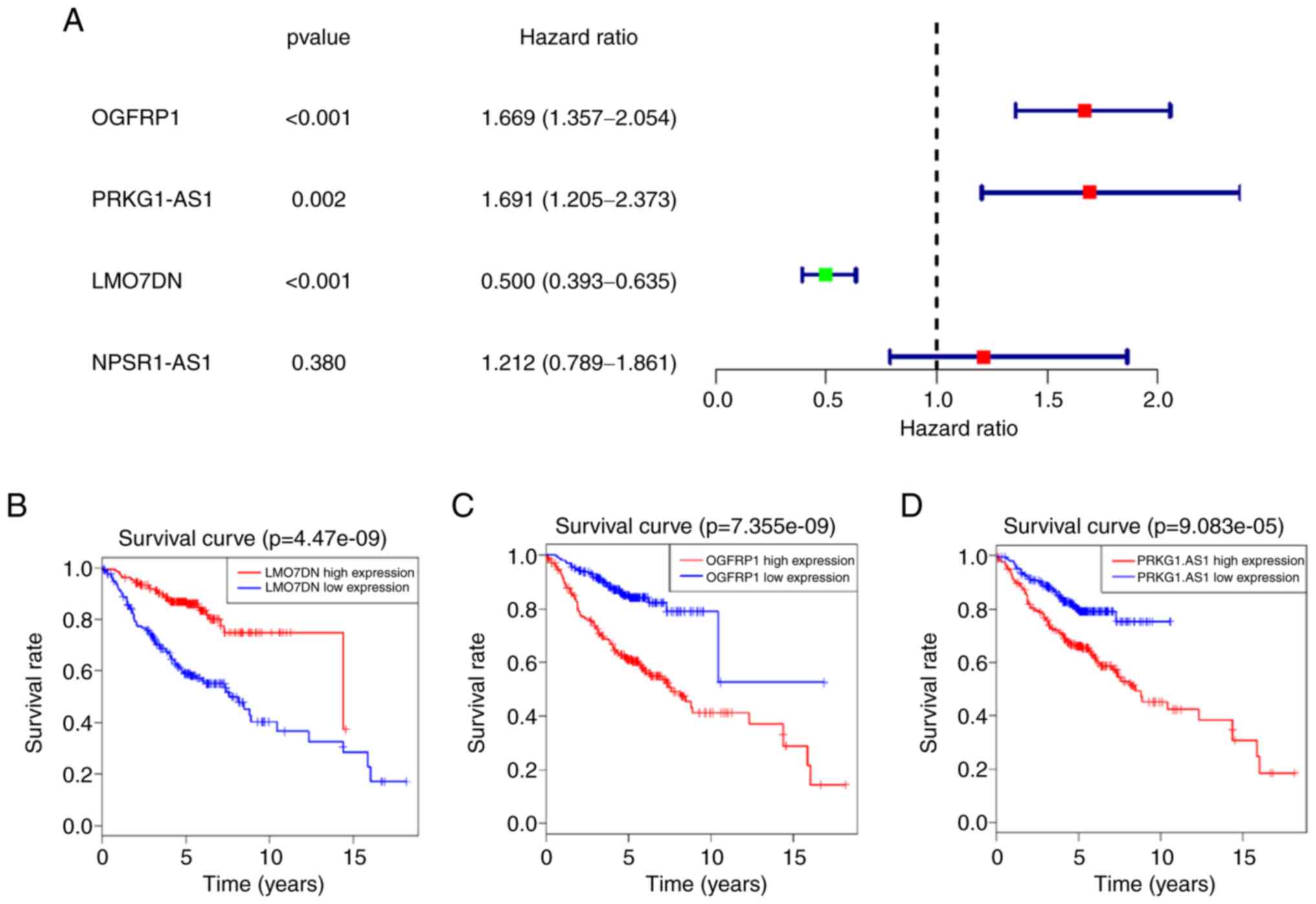 | Figure 4.Analysis of GEO datasets for LMO7DN,
NPSR1-AS1, OGFRP1 and PRKG1-AS1. (A) Results of the univariate Cox
regression analysis of the 4 lncRNAs. Kaplan-Meier survival curves
for (B) LMO7DN, (C) OGFRP1 and (D) PRKG1-AS1 in the GEO datasets,
and the ‘+’ on the survival curves represents the censored
data-points. GEO, gene expression omnibus; lncRNA, long non-coding
RNA; OGFRP1, opioid growth factor receptor pseudogene 1; LMO7DN,
LIM domain 7 downstream neighbor; NPSR1-AS1, neuropeptide S
receptor 1-antisense RNA 1; PRKG1-AS1, protein kinase cyclic
GMP-dependent 1-antisense RNA 1. |
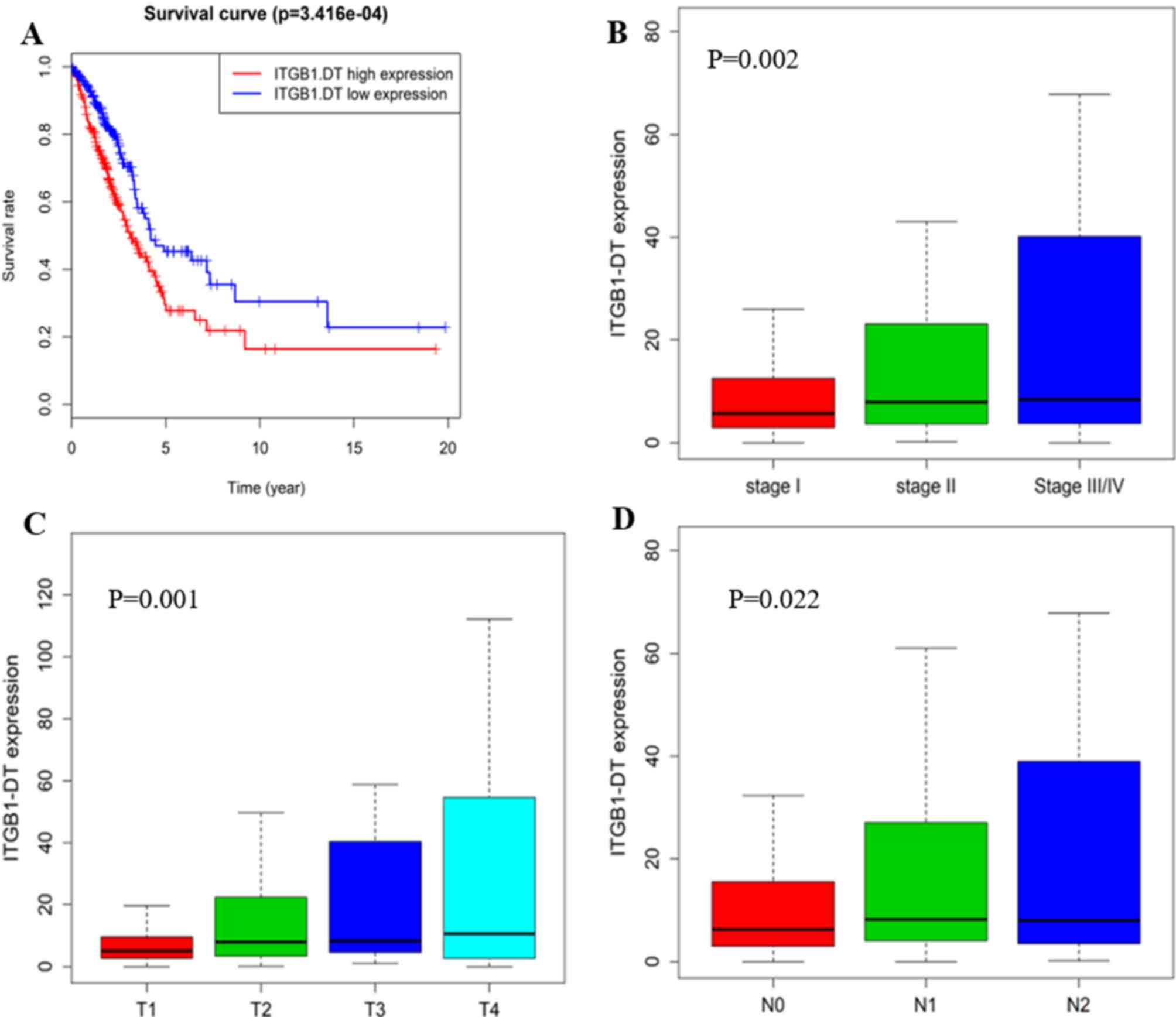
Role of ITGB1-DT in LUAD
Since the lncRNA ITGB1-DT was not present in the GEO
datasets examined and no literature is currently available for it,
it was assumed that this lncRNA has remained largely unexplored.
Therefore, the role of ITGB1-DT in the tumorigenesis of LUAD was
further investigated. Kaplan-Meier survival analysis for ITGB1-DT
was performed, revealing that its expression levels are closely
linked to the survival of patients with LUAD
(P=3.416×10−4; Fig. 5A).
Next, the association between ITGB1-DT and the TNM stage, tumor
stage and lymph node metastasis were analyzed, and the results
indicated that ITGB1-DT was significantly associated with the tumor
node metastasis (TNM stage; P<0.005; Fig. 5B), tumor stage (P<0.005; Fig. 5C) and lymph node metastasis
(P<0.05; Fig. 5D). The LUAD
patients with a higher TNM stage, tended to have a higher
expression of ITGB1-DT.
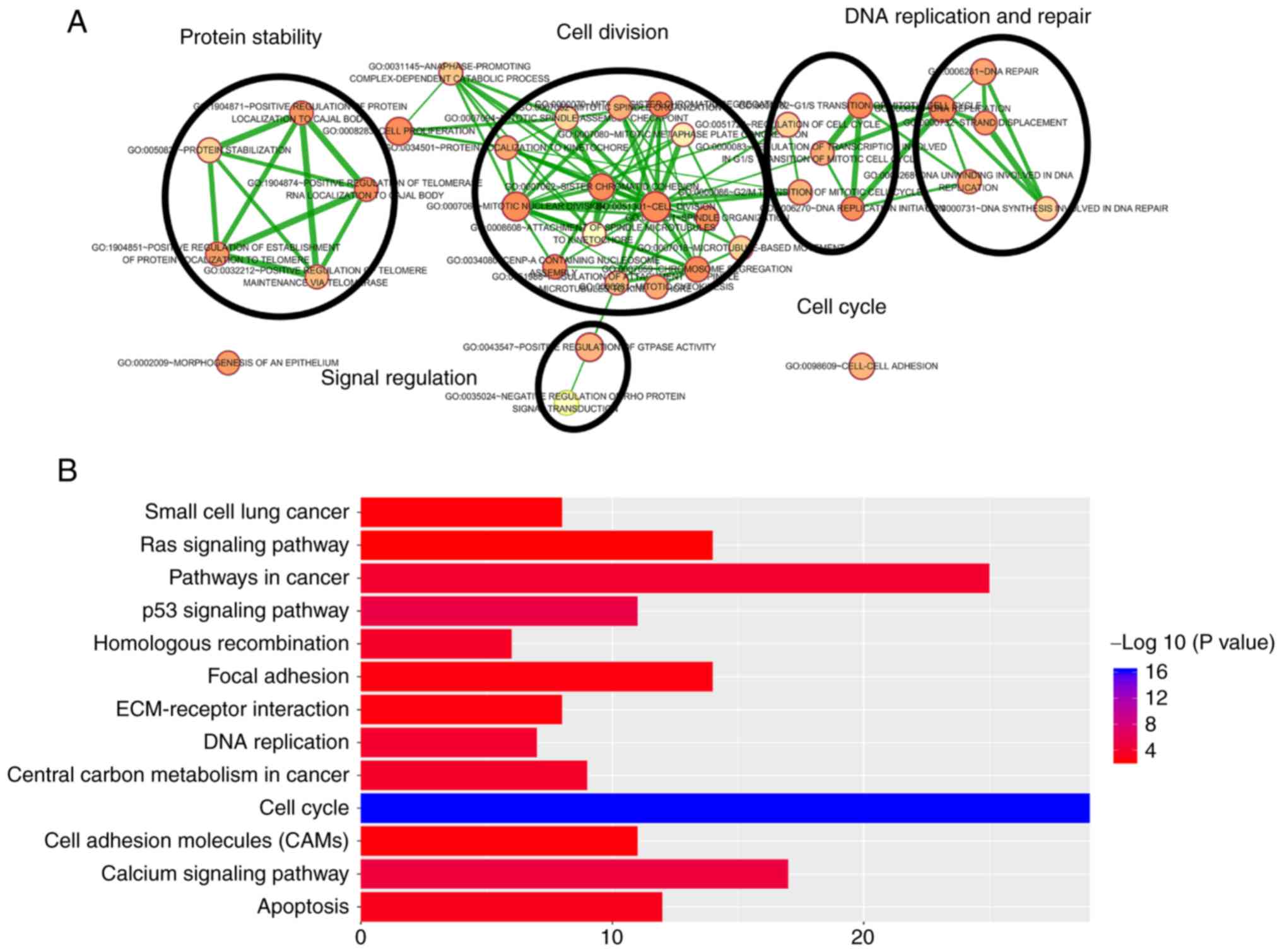
Functional enrichment analysis for 5
prognostic lncRNAs
Pearson's correlation coefficients between the 5
lncRNAs and PCGs were calculated in the total cohort in order to
further investigate the potential biological processes and pathways
of these lncRNAs in LUAD. The results indicated that a total of
1,068 PCGs were closely associated with at least one of the 5
prognostic lncRNAs (|Pearson's correlation coefficient|>0.40 and
P<0.01). According to the functional enrichment analysis, the
1,068 PCGs were mainly enriched in 51 GO terms and 37 KEGG pathways
(P<0.005). These GO terms were clustered into 5 major
categories, including protein stability regulation, DNA replication
and repair, signal regulation, cell division and cell cycle
(Fig. 6A). A total of thirteen
pathways were regarded as being most closely associated with
tumorigenesis, including cell cycle, calcium signaling pathway, p53
signaling pathway, pathways in cancers, DNA replication, central
carbon metabolism in cancer, homologous recombination, apoptosis
and ras signaling pathway (Fig. 6B).
Most of these GO terms and KEGG pathways have been indicated to be
closely linked to the occurrence and development of LUAD,
suggesting that the 5 lncRNAs may be involved in the
LUAD-associated biological functions through co-expressed PCGs.
Expression levels of 5 lncRNAs in LUAD
patients and cell lines
The expression levels of the 5 lncRNAs of the
signature were detected in 14 paired LUAD tissues and adjacent
non-tumor tissues using RT-qPCR. Among these LUAD patients, six
were female and eight were male; the average age was 58 years and
the median age was 59 years (range, 40–80 years). The expression
levels of the 5 lncRNAs in lung cancer cell lines and a normal lung
epithelial cell line were also detected by RT-qPCR. The expression
levels of the 5 lncRNAs in LUAD tissues and cell lines were
consistent with the results obtained with the TCGA dataset. The
results revealed that ITGB1-DT, NPSR1-AS1, OGFRP1 and PRKG1-AS1
were significantly upregulated in LUAD tissues and cell lines,
while LMO7DN was downregulated in the LUAD tissues and cell lines
compared with the normal control tissues and the normal cell line,
respectively. The detailed information is provided in Fig. 7A-J.
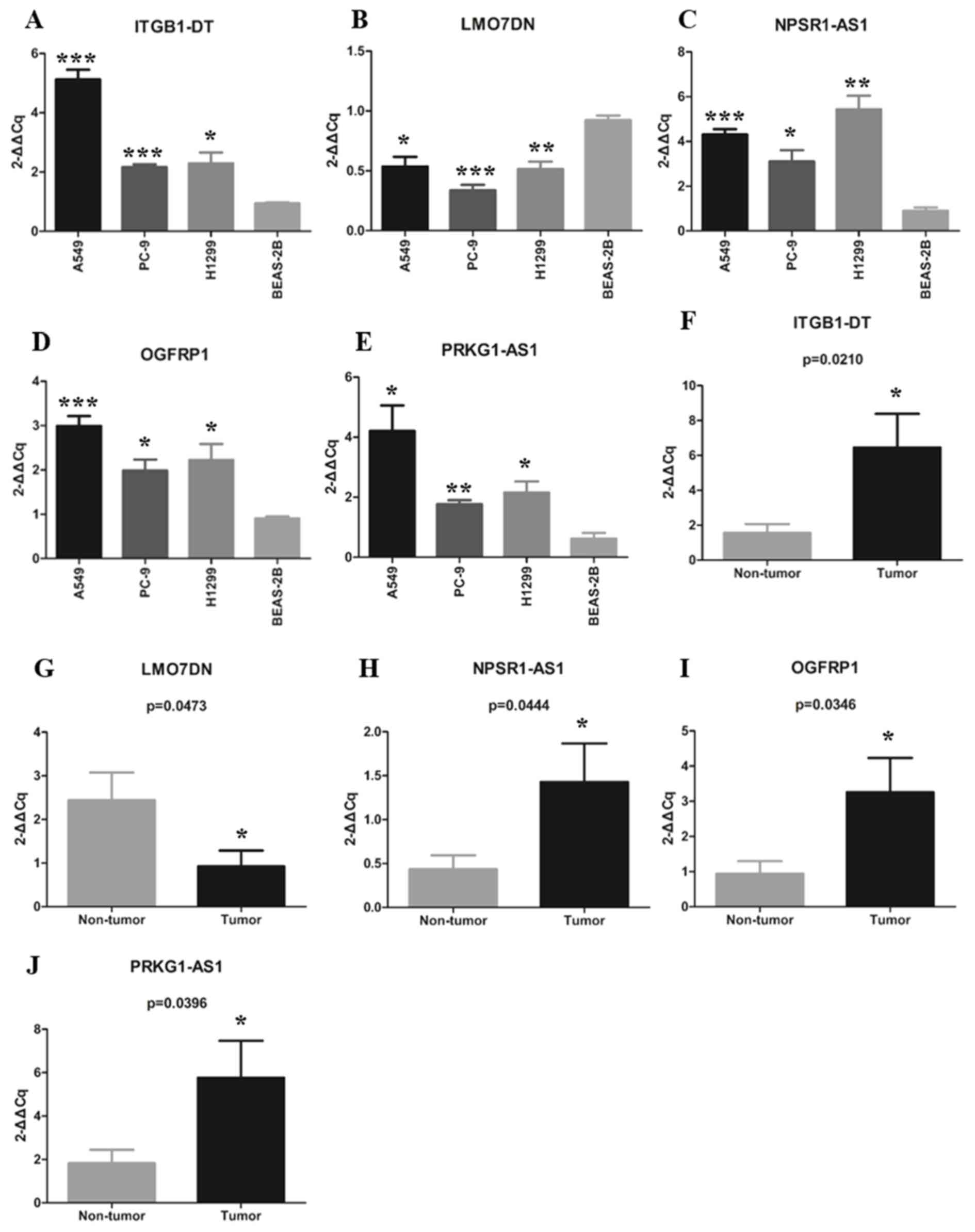 | Figure 7.Expression of the 5 long non-coding
RNAs in lung adenocarcinoma tissues and cell lines. (A-E)
Differential expression of (A) ITGB1-DT, (B) LMO7DN, (C) NPSR1-AS1,
(D) OGFRP1 and (E) PRKG1-AS1 between tumor and non-tumor tissues.
(F-J) Differential expression of (F) ITGB1-DT, (G) LMO7DN, (H)
NPSR1-AS1, (I) OGFRP1 and (J) PRKG1-AS1 between lung cancer cell
lines and a normal human lung epithelial cell line. *P<0.05,
**P<0.01, ***P<0.001 vs. non-tumor or BEAS-2B. OGFRP1, opioid
growth factor receptor pseudogene 1; ITGB1-DT, integrin subunit
beta 1 divergent transcript; LMO7DN, LIM domain 7 downstream
neighbor; NPSR1-AS1, neuropeptide S receptor 1-antisense RNA 1;
PRKG1-AS1, protein kinase cyclic GMP-dependent 1-antisense RNA
1. |
Discussion
In recent years, a growing body of evidence has
suggested that abnormal expression of lncRNAs is involved in
various cancer-associated processes (36,37). In
addition, certain lncRNAs have been indicated to be specific to
tissues, disease types and developmental stages (38,39). An
in-depth study of the association between lncRNAs and cancer is
crucial for obtaining a better understanding of cancer. At present,
although a large number of lncRNAs have been reported to have the
potential to act as diagnostic, prognostic and therapeutic targets,
the clinical application of lncRNAs remains limited. In the present
study, a 5-lncRNA signature was determined in order to provide a
reference for identifying the ideal prognostic signature for
clinical application.
In the present study, the top 7 lncRNAs were
selected as candidate lncRNAs by analyzing the association between
differentially expressed lncRNAs and the survival of LUAD patients
using univariate Cox regression analysis in the training cohort.
Next, multivariate Cox regression analysis, which used a model
based on AIC, was performed on candidate lncRNAs. The model based
on AIC was applied to construct a prognostic signature with the
best predictive ability and the least number of lncRNAs. The
prognostic signature that contained fewer genes is more likely to
be applied in clinical practice. An RS model consisting of 5
lncRNAs, including OGFRP1, ITGB1-DT, LMO7DN, NPSR1-AS1 and
PRKG1-AS1 was successfully established. The 5-lncRNA signature was
proven to have good reliability and stability in predicting the
prognosis of patients with LUAD through testing in the verification
and total cohorts. Using multivariate Cox regression and data
stratification analysis in each cohort, it was found that the
5-lncRNA signature could independently predict the prognosis of
LUAD patients. The results suggested that the 5-lncRNA signature
has a high potential to act as a prognostic biomarker.
Among the 5 lncRNAs, OGFRP1, NPSR1-AS1, ITGB1-DT and
PRKG1-AS1 were indicated to be risk factors for the survival of
patients with LUAD, while LMO7DN was a protective factor. Of note,
except for OGFRP1, these lncRNAs have remained largely unexplored
and they were identified as prognostic cancer biomarkers for the
first time in the present study, to the best of our knowledge. The
expression of the 5 lncRNAs was then verified in LUAD tissues and
cell lines. As expected, ITGB1-DT, NPSR1-AS1, OGFRP1 and PRKG1-AS1
were upregulated in LUAD tumor tissues and cell lines, while LMO7DN
expression was downregulated compared with that in non-cancerous
tissues and cell line. Of note, no expression data for ITGB1-DT
were available in the GEO datasets examined. Further study on
ITGB1-DT indicated that it was significantly associated with tumor
size, lymph node metastasis and stage. In short, ITGB1-DT was
indicated to have a key role in the occurrence and development of
LUAD, and its in-depth study may provide novel insight into LUAD. A
previous study suggested that OGFRP1 may be involved in the
progression of hepatocellular carcinoma through the AKT/mTOR and
Wnt/β-catenin signaling pathways (40). Different studies demonstrated that
OGFRP1 may influence the development of endometrial cancer
(41) and NSCLC (42) by regulating miR-124-3p. OGFRP1 has
also been identified as one of the lncRNA-associated signatures for
predicting the survival of patients with LUAD (26), which further confirmed the potential
value of the 5-lncRNA signature in predicting patient prognosis.
Further research into the function of the other 4 lncRNAs may
provide a better understanding of LUAD.
To date, an increasing number of lncRNAs have been
identified due to the development of various technologies (6). However, the great majority of lncRNAs,
including the 5 lncRNAs identified in the present study, have not
been well characterized in terms of their functions. It has been
reported that lncRNAs may be involved in the biological processes
by interacting PCGs (43), which
implied that the biological functions of lncRNAs may be predicted
by analyzing the co-expressed PCGs. In the present study, a total
of 1,068 PCGs were considered to be closely associated with at
least one of the 5 lncRNAs. A total of 5 functional categories and
13 KEGG pathways were obtained by performing functional enrichment
analysis on these PCGs. These functional categories and KEGG
pathways were all closely associated with tumorigenesis. For
instance, the p53 signaling pathway has been indicated to be a key
pathway in the process of tumorigenesis (44) and the cell cycle is a key biological
process in tumorigenesis (45). The
present results indicated that the 5 prognostic lncRNAs have an
important role in LUAD via their involvement in these known
cancer-associated biological functions.
In conclusion, a 5-lncRNAs signature with the
ability to effectively predict the survival of LUAD patients was
successfully established in the present study. The prognostic
signature was proven to have good reliability and stability in
predicting survival and maintain an independent predictive ability
from other clinical factors. Furthermore, the 5 lncRNAs were
indicated to involved in the tumorigenesis of LUAD through
cancer-associated biological processes and pathways. Overall, the
present results suggested that the 5-lncRNAs signature has the
potential to act as an independent prognostic biomarker for LUAD
and provide novel insight into the potential mechanisms of
LUAD.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was funded by the National Natural
Science Foundation of China (grant no. 81672300).
Availability of data and materials
The data used in this study were obtained from The
Cancer Genome Atlas database (https://portal.gdc.cancer.gov) and Gene Expression
Omnibus database (http://www.ncbi.nlm.nih.gov/geo).
Authors' contributions
LZ analyzed the data and wrote the manuscript. WW
and YC were responsible for downloading the data. XL, JY and RS
were responsible for selecting the literature. SY was responsible
for the conception and experimental guidance of the study. All
authors approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
OS
|
overall survival
|
|
LUAD
|
lung adenocarcinoma
|
|
TCGA
|
the cancer genome atlas
|
|
RS
|
risk score
|
|
lncRNA
|
long non-coding RNA
|
|
NSCLC
|
non-small-cell lung cancer
|
|
GEO
|
Gene Expression Omnibus
|
|
AIC
|
akaike information criterion
|
|
ROC
|
receiver operating characteristic
|
|
AUC
|
area under the ROC curve
|
|
HR
|
hazard ratio
|
|
RT-qPCR
|
reverse transcription-quantitative
PCR
|
|
PCGs
|
protein-coding genes
|
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2019. CA Cancer J Clin. 69:7–34. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sholl LM: The molecular pathology of lung
cancer. Surg Pathol Clin. 9:353–378. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mao Y, Yang D, He J and Krasna MJ:
Epidemiology of lung cancer. Surg Oncol Clin N Am. 25:439–445.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Puri T: Targeted therapy in nonsmall cell
lung cancer. Indian J Cancer. 54:83–88. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jathar S, Kumar V, Srivastava J and
Tripathi V: Technological developments in lncRNA biology. Adv Exp
Med Biol. 1008:283–323. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jarroux J, Morillon A and Pinskaya M:
History, discovery, and classification of lncRNAs. Adv Exp Med
Biol. 1008:1–46. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bhan A, Soleimani M and Mandal SS: Long
noncoding RNA and cancer: A New Paradigm. Cancer Res. 77:3965–3981.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Liu Y, Sharma S and Watabe K: Roles of
lncRNA in breast cancer. Front Biosci (Schol Ed). 7:94–108. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Thin KZ, Liu X, Feng X, Raveendran S and
Tu JC: LncRNA- DANCR: A valuable cancer related long non-coding RNA
for human cancers. Pathol Res Pract. 214:801–805. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gibb EA, Brown CJ and Lam WL: The
functional role of long non-coding RNA in human carcinomas. Mol
Cancer. 10:382011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Balas MM and Johnson AM: Exploring the
mechanisms behind long noncoding RNAs and cancer. Noncoding RNA
Res. 3:108–117. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Qi G, Kong W, Mou X and Wang S: A new
method for excavating feature lncRNA in lung adenocarcinoma based
on pathway crosstalk analysis. J Cell Biochem. 120:9034–9046. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Peng W, Wang J, Shan B, Peng Z, Dong Y,
Shi W, He D, Cheng Y, Zhao W, Zhang C, et al: Diagnostic and
prognostic potential of circulating long non-coding RNAs in non
small cell lung cancer. Cell Physiol Biochem. 49:816–827. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dai SP, Jin J and Li WM: Diagnostic
efficacy of long non-coding RNA in lung cancer: A systematic review
and meta-analysis. Postgrad Med J. 94:578–587. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pan X, Zheng G and Gao C: LncRNA PVT1: A
novel therapeutic target for cancers. Clin Lab. 64:655–662. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Song P, Jiang B, Liu Z, Ding J, Liu S and
Guan W: A three- lncRNA expression signature associated with the
prognosis of gastric cancer patients. Cancer Med. 6:1154–1164.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bao Z, Zhang W and Dong D: A potential
prognostic lncRNA signature for predicting survival in patients
with bladder urothelial carcinoma. Oncotarget. 8:10485–10497. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gu JX, Zhang X, Miao RC, Xiang XH, Fu YN,
Zhang JY, Liu C and Qu K: Six-long non-coding RNA signature
predicts recurrence-free survival in hepatocellular carcinoma.
World J Gastroenterol. 25:220–232. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Luo D, Deng B, Weng M, Luo Z and Nie X: A
prognostic 4-lncRNA expression signature for lung squamous cell
carcinoma. Artif Cells Nanomed Biotechnol. 46:1207–1214. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lu T, Wang Y, Chen D, Liu J and Jiao W:
Potential clinical application of lncRNAs in non-small cell lung
cancer. Onco Targets Ther. 11:8045–8052. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Miao R, Ge C, Zhang X, He Y, Ma X, Xiang
X, Gu J, Fu Y, Qu K, Liu C, et al: Combined eight-long noncoding
RNA signature: A new risk score predicting prognosis in elderly
non-small cell lung cancer patients. Aging (Albany NY). 11:467–479.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Li X, Li B, Ran P and Wang L:
Identification of ceRNA network based on a RNA-seq shows prognostic
lncRNA biomarkers in human lung adenocarcinoma. Oncol Lett.
16:5697–5708. 2018.PubMed/NCBI
|
|
24
|
Kumar P, Khadirnaikar S and Shukla SK: A
novel LncRNA- based prognostic score reveals TP53-dependent subtype
of lung adenocarcinoma with poor survival. J Cell Physiol. Feb
10–2019.doi: 10.1002/jcp.28260 (Epub ahead of print). View Article : Google Scholar
|
|
25
|
Songyang Y, Zhu W, Liu C, Li LL, Hu W,
Zhou Q, Zhang H, Li W and Li D: Large-scale gene expression
analysis reveals robust gene signatures for prognosis prediction in
lung adenocarcinoma. PeerJ. 7:e69802019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Li YY, Yang C, Zhou P, Zhang S, Yao Y and
Li D: Genome-scale analysis to identify prognostic markers and
predict the survival of lung adenocarcinoma. J Cell Biochem.
119:8909–8921. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Robinson MD, McCarthy DJ and Smyth GK:
edgeR: A Bioconductor package for differential expression analysis
of digital gene expression data. Bioinformatics. 26:139–140. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Huang PH: Asymptotics of AIC, BIC, and
RMSEA for model selection in structural equation modeling.
Psychometrika. 82:407–426. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sing T, Sander O, Beerenwinkel N and
Lengauer T: ROCR: Visualizing classifier performance in R.
Bioinformatics. 21:3940–3941. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Huang DW, Sherman BT, Tan Q, Kir J, Liu D,
Bryant D, Guo Y, Stephens R, Baseler MW, Lane HC and Lempicki RA:
DAVID bioinformatics resources: Expanded annotation database and
novel algorithms to better extract biology from large gene lists.
Nucleic Acids Res. 35:W169–W175. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wu J, Mao X, Cai T, Luo J and Wei L: KOBAS
server: A web-based platform for automated annotation and pathway
identification. Nucleic Acids Res. 34:W720–W724. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Merico D, Isserlin R, Stueker O, Emili A
and Bader GD: Enrichment map: A network-based method for gene-set
enrichment visualization and interpretation. PLoS One.
5:e139842010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Shannon P, Markiel A, Ozier O, Baliga NS,
Wang JT, Ramage D, Amin N, Schwikowski B and Ideker T: Cytoscape: A
software environment for integrated models of biomolecular
interaction networks. Genome Res. 13:2498–2504. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ito K and Murphy D: Application of ggplot2
to pharmacometric graphics. CPT Pharmacometrics Syst Pharmacol.
2:e792013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Forrest ME and Khalil AM: Review:
Regulation of the cancer epigenome by long non-coding RNAs. Cancer
Lett. 407:106–112. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Yang G, Lu X and Yuan L: LncRNA: A link
between RNA and cancer. Biochim Biophys Acta. 1839:1097–1109. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Schmitz SU, Grote P and Herrmann BG:
Mechanisms of long noncoding RNA function in development and
disease. Cell Mol Life Sci. 73:2491–2509. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Zhang H, Chen Z, Wang X, Huang Z, He Z and
Chen Y: Long non-coding RNA: A new player in cancer. J Hematol
Oncol. 6:372013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chen W, You J, Zheng Q and Zhu YY:
Downregulation of lncRNA OGFRP1 inhibits hepatocellular carcinoma
progression by AKT/mTOR and Wnt/β-catenin signaling pathways.
Cancer Manag Res. 10:1817–1826. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Lv Y, Chen S, Wu J, Lin R, Zhou L, Chen G,
Chen H and Ke Y: Upregulation of long non-coding RNA OGFRP1
facilitates endometrial cancer by regulating miR-124-3p/SIRT1 axis
and by activating PI3K/AKT/GSK-3beta pathway. Artif Cells Nanomed
Biotechnol. 47:2083–2090. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Tang LX, Chen GH, Li H, He P, Zhang Y and
Xu XW: Long non-coding RNA OGFRP1 regulates LYPD3 expression by
sponging miR-124-3p and promotes non-small cell lung cancer
progression. Biochem Biophys Res Commun. 505:578–585. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Ferré F, Colantoni A and Helmer-Citterich
M: Revealing protein-lncRNA interaction. Brief Bioinform.
17:106–116. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Joerger AC and Fersht AR: The p53 pathway:
Origins, inactivation in cancer, and emerging therapeutic
approaches. Annu Rev Biochem. 85:375–404. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Williams GH and Stoeber K: The cell cycle
and cancer. J Pathol. 226:352–364. 2012. View Article : Google Scholar : PubMed/NCBI
|