Introduction
The ear is one of the most pivotal sensory organs on
the face, such that congenital or acquired auricular abnormalities
have negative physical and mental impacts on the patients. Most of
these abnormalities, including microtia, anotia, cryptotia,
prominent ear and constricted ear, can be diagnosed by physical
observation. Surgical and non-surgical methods are selectively used
for different conditions (1,2). Although scales of satisfaction and
other subjective methods are important for the evaluation of
therapeutic efficacy (3),
anthropometric methods, designed to objectively appraise the
severity of abnormalities and outcomes of therapy, are also
indispensable (4).
The length and width of the auricle, cranioauricular
height, and cranioauricular angle are most frequently applied in
the evaluation of the ear (5,6). The arc
length of the auricle is also a suitable index for assessing the
size of the auricle but has not been fully determined previously.
Among the previous studies, manual measurements of straight-line
distances using rulers and calipers were applied most frequently
(5,7,8).
However, this method is inaccurate and unreliable. Although there
have been some attempts at measuring auricular angles, convenient
and accurate approaches to address the accuracy of this measurement
remain elusive (8,9).
Three-dimensional (3D) digital techniques, which can
be used to build models of high similarity, have been developing
rapidly in the past two decades (10–12). In
the present study, a standardized measurement procedure combining
Mimics software and a 3D digital device was used to evaluate five
indices for auricle measurements in 20 normal ears. Emphasis was
placed on the precision and reliability of this method.
Materials and methods
Patients
Ethical approval of the study was obtained from the
Institutional Review Board of Plastic Surgery Hospital of Peking
Union Medical College. Between August 2017 and January 2018, 20
patients (sex, 12 males and 8 females; age range, 5–15 years; mean
age, 7.9±2.88 years) with unilateral auricular abnormality at the
Department of the First Center of Auricular Reconstruction, Plastic
Surgery Hospital, Chinese Academy of Medical Sciences, Peking Union
Medical College who were subjected to surgery were randomly
selected and enrolled into the study (Beijing, China). All parents
or guardians of the patients granted informed consent to
participate in the study. Eight right normal ears and 12 left
normal ears were scanned and measured prior to surgery.
3D equipment
A surface 3D scanner (Artec Space Spider; Artec 3D)
with a stated resolution of 0.1 mm and a point accuracy of ≤0.03 mm
was used to capture 3D images of the normal auricles. The acquired
preliminary data were processed using the Artec Studio software
(version 9.0; Artec 3D) by following the surface scan workflow
(including rough serial registration, fine registration, global
registration, manual alignment and fast fusion). After preliminary
treatment, data were exported as stereolithography format files to
the Geomagic Studio 2012 software (3D Systems Corporation) for
further processing. Using this software, spike removal, filling of
holes matching the curvature of the surrounding mesh and
minimization of crease angles between the polygons were achieved to
obtain accurate 3D models displaying details and sizes of the ears.
Following the preparation of digital images, data were imported
into the Materialise Mimics software (version 20.0; Materialise NV)
for precise measurements.
Measurement of auricular
parameters
The auricular parameters measured included the
length of the auricle (LA), the width of the auricle (WA), arch
length of the auricle (ALA), cranioauricular height (CH) and
cranioauricular angle (CA). LA, WA, ALA, CH, and CA were calculated
in the measurement model of the Mimics software. The definitions
for these five parameters were as follows: LA, the maximum distance
from the sup-helix to the sub-lobe (a-b; Fig. 1A); WA, the maximum distance from the
pre-auricle to the post-auricle (c-d; Fig. 1A); ALA, the arc length between the
intersection of crus of helix and the tragus and the intersection
of earlobe and tragus (e-f; Fig.
1B); CH, the projection of the helical rim at the horizontal
plane of the prominent point of tragus to the mastoid (g-h;
Fig. 1C and E); and CA, the angle
formed between the plane of auricle and the plane of mastoid at the
horizontal level of the prominent point of tragus (g-h; Fig. 1D and F).
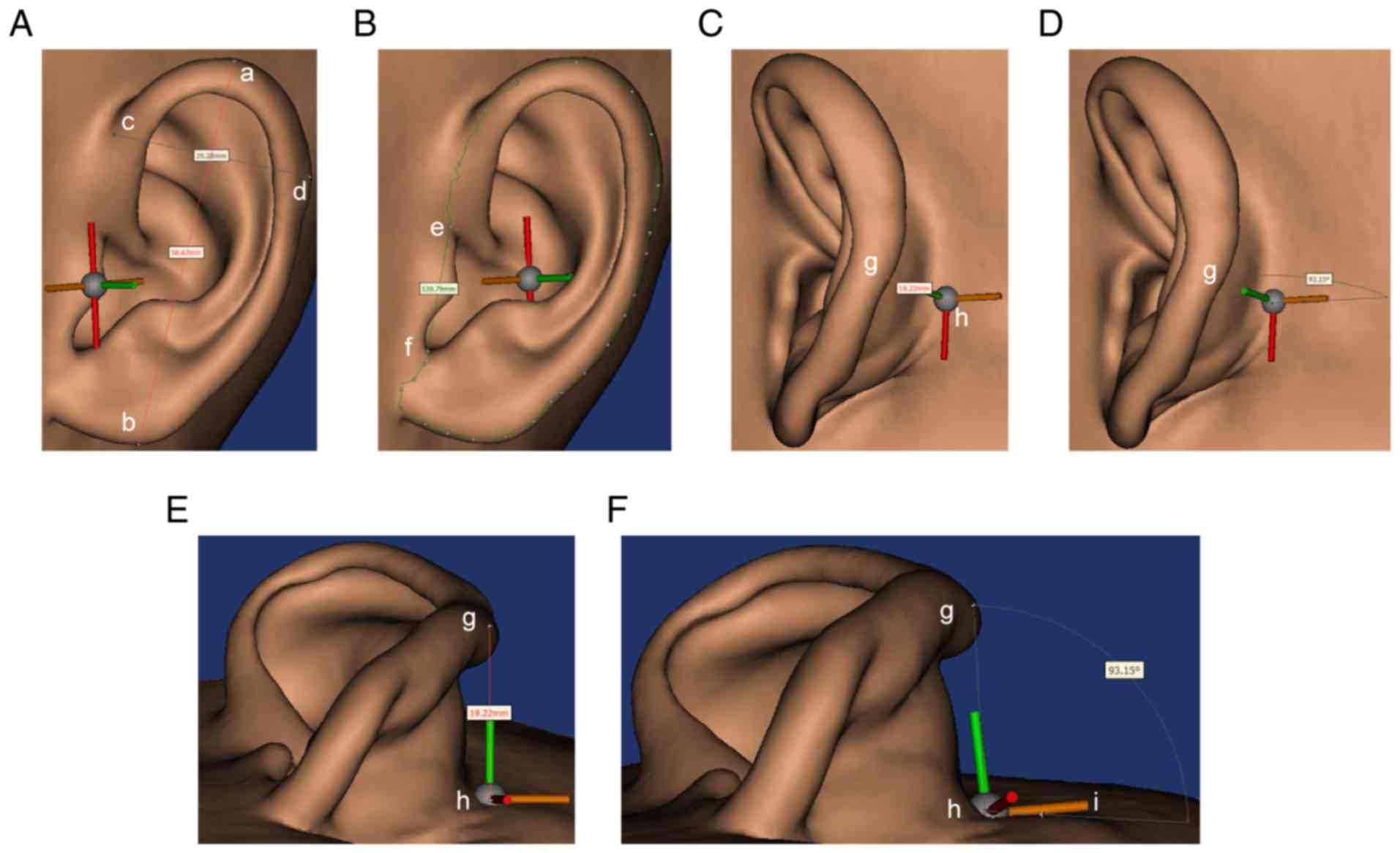 | Figure 1.Measurement of length and width of the
auricle, arch length of the auricle and cranioauricular height and
angle from Mimics software. (A) Anterior view of the auricle
indices used for the measurement of the length of the auricle,
which is the maximum distance from the sup-helix ‘a’ to the
sub-lobe ‘b’, and the width of the auricle, which is the maximum
distance from the pre-auricle ‘c’ to the post-auricle ‘d’. (B)
Anterior view of the auricle and indices used for the measurement
of the arch length of the auricle, which is the arc length between
the intersection of crus of helix and tragus ‘e’ and the
intersection of earlobe and tragus ‘f’. (C) Lateral view of the
auricle and indices used for the measurement of cranioauricular
height, which is the projection of the helical rim at the
horizontal plane of the prominent point of tragus ‘g’ to the
mastoid ‘h’. (D) Lateral view of the cranioauricular angle
measurement. (E) Low angle view of the auricle with the indices
used for the measurement of cranioauricular height. (F) Low angle
view of the indices used for the measurement of the cranioauricular
angle (angle ghi), which is the angle between the plane of the
auricle and the plane of the mastoid at the horizontal level of the
prominent point of tragus. a, the sup-helix; b, the sub-lobe; c,
the pre-auricle; d, the post-auricle; e, the intersection of crus
of helix and tragus; f, the intersection of earlobe and tragus; g,
the prominent point of tragus; h, the projection of the point p at
the horizontal plane to the mastoid; i, a random point at the
horizontal plane across the point h. |
Surgeons 1 and 2 independently measured all 20
normal ears using the digital measurement method with an Artec
Spider Device and the measurement points designated on the
software, whilst surgeons 3 and 4 independently measured all 20
normal ears using a flexible tape and protractor, without using the
standardized indices. Measurement points were chosen subjectively
by surgeons 3 and 4 according to prior experience.
Statistical analysis
Each patient was measured three times by each
surgeon and the mean value was calculated. All data were imported
into Statistical Package for Social Sciences (SPSS) software
(version 20.0; IBM Corp.) and analyzed. Distribution of data was
analyzed using the Shapiro-Wilk normality test (P>0.05). Paired
samples t-test and Wilcoxon signed rank test were used and
P<0.05 was considered to indicate a statistically significant
difference. Five sets of data were analyzed using intra-class
correlation coefficients (ICC). The level of clinical significance
is considered poor, fair, good and excellent when ICC <0.40,
0.40<ICC<0.59, 0.60<ICC<0.74, and 0.75<ICC<1.00,
respectively (13). Pearson product
moment correlation was calculated to reflect the correlation
between LA and WA, and between CH and CA.
Results
Summary of data
Age, sex, measured side and measured data of the
five parameters of all 20 patients are listed in Tables I and II. The mean value of LA measured by
surgeon 1 to 4 was 8.64±4.07, 58.59±3.95, 60.02±4.30 and 56.83±3.65
mm, respectively, while that of WA was 31.80±2.92, 31.82±2.71,
32.51±2.69, and 31.41±3.01 mm. The mean value of LA was
135.70±6.56, 135.57±7.13, 139.69±7.27 and 134.56±7.48 mm,
respectively. The mean value of CH was 19.43±2.51, 19.67±2.62,
18.35±2.02 and 20.32±2.78 mm, respectively. The mean value of CA
was 85.91±14.54°, 86.55±15.18°, 90.6±3.43° and 81.8±13.86°,
respectively.
 | Table I.Clinical characteristics and measured
data from the digital measurement. |
Table I.
Clinical characteristics and measured
data from the digital measurement.
|
|
|
|
| LA (mm) | WA (mm) | ALA (mm) | CH (mm) | CA (°) |
|---|
|
|
|
|
|
|
|
|
|
|
|---|
| Patient number | Sex | Age | Measured side | Surgeon 1 | Surgeon 2 | Surgeon 1 | Surgeon 2 | Surgeon 1 | Surgeon 2 | Surgeon 1 | Surgeon 2 | Surgeon 1 | Surgeon 2 |
|---|
| 1 | M | 6 | Right | 58.89 | 58.66 | 33.15 | 34.10 | 121.93 | 122.66 | 21.72 | 21.00 | 103.27 | 102.12 |
| 2 | M | 12 | Left | 60.38 | 59.86 | 25.26 | 24.86 | 149.24 | 148.12 | 24.2 | 24.29 | 74.93 | 72.15 |
| 3 | F | 7 | Right | 57.92 | 59.16 | 26.31 | 28.36 | 140.31 | 137.60 | 18.86 | 20.14 | 100.41 | 107.78 |
| 4 | M | 7 | Left | 53.35 | 52.25 | 31.11 | 32.55 | 132.00 | 130.36 | 16.63 | 18.56 | 83.43 | 84.03 |
| 5 | F | 5 | Left | 56.90 | 56.56 | 29.02 | 28.99 | 135.01 | 130.68 | 19.10 | 19.10 | 102.99 | 105.35 |
| 6 | M | 6 | Left | 58.77 | 57.73 | 28.59 | 28.48 | 131.44 | 132.69 | 13.42 | 12.24 | 58.81 | 60.90 |
| 7 | M | 5 | Left | 51.10 | 53.34 | 34.18 | 33.19 | 127.51 | 127.18 | 19.67 | 23.24 | 99.30 | 101.40 |
| 8 | M | 8 | Right | 57.75 | 57.54 | 34.24 | 33.61 | 138.03 | 132.19 | 17.58 | 19.60 | 80.20 | 82.55 |
| 9 | F | 10 | Left | 60.70 | 60.43 | 31.29 | 31.72 | 137.47 | 138.26 | 18.69 | 18.26 | 76.10 | 72.71 |
| 10 | F | 6 | Right | 57.36 | 57.19 | 28.85 | 28.53 | 133.86 | 131.11 | 19.97 | 19.47 | 71.73 | 72.48 |
| 11 | M | 10 | Left | 59.36 | 59.03 | 31.39 | 31.97 | 140.99 | 142.76 | 20.77 | 20.30 | 105.42 | 103.16 |
| 12 | M | 9 | Left | 55.24 | 56.08 | 33.51 | 34.25 | 134.32 | 135.61 | 24.27 | 23.92 | 97.34 | 98.72 |
| 13 | F | 5 | Left | 57.61 | 57.24 | 32.30 | 31.95 | 133.15 | 133.53 | 21.31 | 20.80 | 86.17 | 85.85 |
| 14 | M | 6 | Right | 55.98 | 56.07 | 32.07 | 32.33 | 134.54 | 136.30 | 17.71 | 17.66 | 74.14 | 77.77 |
| 15 | F | 6 | Left | 63.84 | 63.57 | 32.95 | 32.75 | 134.78 | 134.99 | 21.35 | 21.59 | 104.01 | 105.69 |
| 16 | M | 13 | Right | 65.71 | 66.75 | 34.52 | 34.31 | 140.06 | 143.84 | 18.82 | 19.00 | 97.55 | 97.96 |
| 17 | M | 9 | Right | 59.43 | 58.91 | 33.41 | 32.69 | 133.68 | 134.00 | 20.27 | 19.50 | 86.46 | 86.54 |
| 18 | M | 8 | Right | 55.95 | 56.09 | 34.71 | 34.08 | 138.99 | 141.24 | 18.33 | 18.16 | 65.11 | 65.22 |
| 19 | F | 15 | Left | 69.12 | 68.57 | 36.77 | 36.24 | 148.95 | 151.09 | 18.69 | 19.36 | 69.24 | 67.90 |
| 20 | M | 5 | Left | 57.50 | 56.78 | 32.31 | 31.43 | 127.72 | 127.21 | 17.24 | 17.29 | 81.49 | 80.72 |
| Table II.Clinical characteristics and measured
data from the manual measurement. |
Table II.
Clinical characteristics and measured
data from the manual measurement.
|
|
|
|
| LA (mm) | WA (mm) | ALA (mm) | CH (mm) | CA (°) |
|---|
|
|
|
|
|
|
|
|
|
|
|---|
| Patient number | Sex | Age | Measured side | Surgeon 3 | Surgeon 4 | Surgeon 3 | Surgeon 4 | Surgeon 3 | Surgeon 4 | Surgeon 3 | Surgeon 4 | Surgeon 3 | Surgeon 4 |
|---|
| 1 | M | 6 | Right | 60.5 | 57.4 | 35.2 | 33.1 | 128.2 | 121.5 | 19 | 22.1 | 110 | 95 |
| 2 | M | 12 | Left | 62.5 | 56.7 | 27.1 | 23.4 | 152.3 | 147.4 | 22.5 | 25.2 | 85 | 70 |
| 3 | F | 7 | Right | 59.2 | 56.8 | 28.2 | 29.7 | 145.2 | 135.4 | 17.4 | 21.1 | 105 | 100 |
| 4 | M | 7 | Left | 55.4 | 51.2 | 31.8 | 34.4 | 135.8 | 129.4 | 15.3 | 18.4 | 85 | 82 |
| 5 | F | 5 | Left | 57.1 | 53.2 | 29.9 | 31.6 | 138 | 129.6 | 18.5 | 18.9 | 104 | 100 |
| 6 | M | 6 | Left | 59.8 | 55.5 | 31.3 | 27.2 | 134.3 | 129.7 | 14.2 | 12.2 | 70 | 60 |
| 7 | M | 5 | Left | 53.1 | 51 | 35 | 32.8 | 130.2 | 125.1 | 18.4 | 23 | 105 | 95 |
| 8 | M | 8 | Right | 60.3 | 57.2 | 36.2 | 31.2 | 139.5 | 133.4 | 17 | 21.3 | 88 | 78 |
| 9 | F | 10 | Left | 62 | 58.2 | 31.4 | 33.5 | 140.2 | 139 | 18.8 | 18.5 | 85 | 73 |
| 10 | F | 6 | Right | 59.5 | 55.2 | 28.5 | 29.6 | 136.4 | 131.1 | 18.7 | 20.5 | 80 | 71 |
| 11 | M | 10 | Left | 60.2 | 57.2 | 32.4 | 34.5 | 146.4 | 142.1 | 17.8 | 21 | 108 | 98 |
| 12 | M | 9 | Left | 56.3 | 55.2 | 35.2 | 32.5 | 138 | 136.4 | 21.4 | 23.8 | 99 | 90 |
| 13 | F | 5 | Left | 59.6 | 55.9 | 33.9 | 29.8 | 134.8 | 131.1 | 20.4 | 23.1 | 87 | 80 |
| 14 | M | 6 | Right | 55 | 57.2 | 32.8 | 34.5 | 138 | 135.2 | 15.7 | 19.8 | 78 | 70 |
| 15 | F | 6 | Left | 65.3 | 60.2 | 34.7 | 30.1 | 138.3 | 132.9 | 20.1 | 22.4 | 108 | 102 |
| 16 | M | 13 | Right | 67.6 | 61.2 | 35.5 | 31.8 | 149 | 143.1 | 18.24 | 19 | 100 | 93 |
| 17 | M | 9 | Right | 62.7 | 57.5 | 31.2 | 29.4 | 138.7 | 133.5 | 20.5 | 19.5 | 90 | 80 |
| 18 | M | 8 | Right | 55.2 | 58.1 | 31.1 | 31.2 | 145.2 | 142 | 18 | 18.8 | 70 | 62 |
| 19 | F | 15 | Left | 70.3 | 67.9 | 35.6 | 37.4 | 155.3 | 149.2 | 17.6 | 20 | 70 | 63 |
| 20 | M | 5 | Left | 58.8 | 53.8 | 33.2 | 30.5 | 129.9 | 124.1 | 17.4 | 17.8 | 85 | 74 |
The reliability of ratings or
measurements
The P-values and ICC of the five sets of data from
two different measurement methods were presented in Tables III and IV. No significant differences were
observed in all five sets of measured parameters using the digital
method between different investigators (P>0.05; Table III). However, significant
differences were observed in the same sets of measured data using
the manual method between different investigators (P<0.01;
Table IV). ICCs between the two
surgeons for LA, WA, ALA, CH and CA measured using standardized
methods were 0.98, 0.962, 0.944, 0.901 and 0.987, respectively
(Table III), indicating high
precision and observer independence. By contrast, ICC of LA, WA and
CH were calculated to be 0.630, 0.526 and 0.546, respectively
(ICC<0.7; Table IV), and 0.790
and 0.807 for ALA and CA, respectively (0.75<ICC<0.9;
Table IV) for measurements obtained
using the manual method. These results indicated that manual
measurements exhibited a lower clinical significance compared with
digital measurements.
| Table III.P-values and ICCs of the data
obtained using the digital measurement method. |
Table III.
P-values and ICCs of the data
obtained using the digital measurement method.
| Statistical
item | LA | WA | ALA | CH | CA |
|---|
| t value | −0.256 | −0.126 | 0.242 | −0.949 | −1.183 |
| P-value | 0.801 | 0.901 | 0.812 | 0.355 | 0.252 |
| ICC | 0.98 | 0.962 | 0.944 | 0.901 | 0.987 |
| Table IV.P-value and ICCs of the data obtained
using the manual measurement method. |
Table IV.
P-value and ICCs of the data obtained
using the manual measurement method.
| Statistical
item | LA | WA | ALA | CH | CA |
|---|
| Z-value | −3.585 | −1.999 | N/A | N/A | N/A |
| t value | n/a | n/a | 11.188 | −4.845 | 12.471 |
| P-value | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 |
| ICC | 0.630 | 0.526 | 0.790 | 0.546 | 0.807 |
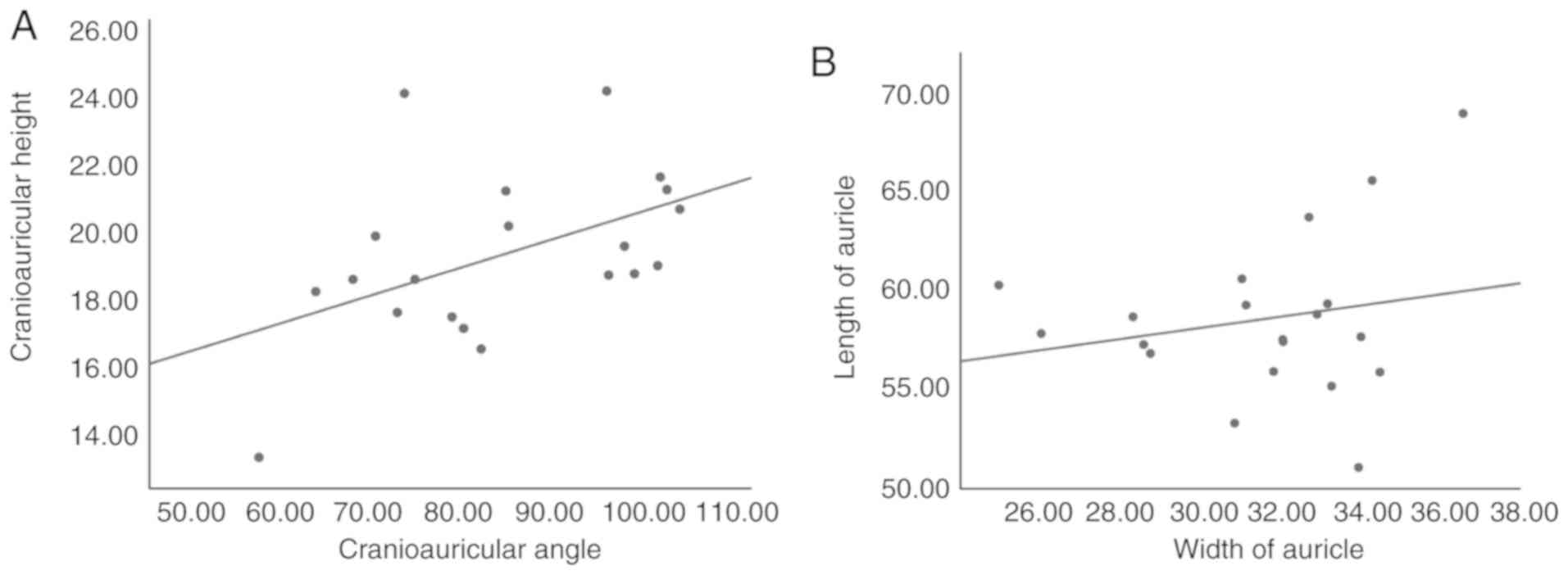
Linear association between two
indices
Pearson product-moment correlation analysis
(r=0.479; P<0.05) showed that a moderate but significant
positive correlation was observed between CH and CA, whilst the
same analysis (r=0.206; P>0.05) did not demonstrate a
significant correlation between LA and WA (Fig. 2).
Discussion
The present study reported a standardized method
combining 3D scanning technique and Mimics software for the
evaluation of auricular size. Measurement of auricular size is one
of the key elements in the diagnosis, pre-operation design and
therapeutic effect assessment of ear abnormalities (14). However, uniform and standardized
objective methodology is currently unavailable (7,9,14) and variations exist in the measurement
results obtained by different investigators. These differences
could lead to errors in surgical or non-surgical therapy for the
correction of auricular abnormalities, especially in multiple stage
surgery. In previous studies, manual measurement was utilized in
the pre- and post-therapy appraisal of auricular abnormalities,
where low accuracy and high error rates were reported (5,15). In
particular, in the measurement of cranioauricular angle, there are
a number of reliable methods, including alginate mold (7). In a previous study, visual inspection
was chosen for ear similarity, leading to imprecise outcomes
(16). Although innovative
methodologies providing auricular measurements have been previously
proposed, this method is inconvenient and time-consuming (7,9). In
addition, another essential factor that influences the outcome of
manual measurement is that contact with the ears results in ear
distortion and introduces further variation to the data. To the
best of our knowledge, this is the first study that attempted to
unify the indices for the measurement of auricles using a highly
precise and reliable digital method.
CT scans are widely used to collect data for 3D
reconstruction (10,17). It has been previously reported that
exposure to radiation is a risk factor for the development of
malignant tumors (18). Since
clinical benefits should be considered for patients, especially for
children, an alternative for CT scans would be beneficial. In the
present study, a 3D surface scanner digitizing the intricate
details of the auricle was used. A previous study has demonstrated
minimal differences in the screenshots of specimen surfaces
obtained using a CT scan and an Artec Space Spider scanner
(19). Blue light 3D scanning
technology used in the Artec Spider does not emit radiation during
the scanning process and is therefore harmless to patients
(20).
Digitizing software is frequently applied in 3D
reconstruction and measurement, and other aspects in the field of
surgery (21,22). In the present study, Mimics software
was used for the measurement of straight-line distance, arc length
and angle with an accuracy of 0.01 mm and 0.01°, which was markedly
higher compared with previous reports (6,9). Mimics
software is an image processing software that can create 3D models,
measurements and analysis of 3D images (23), but was mostly applied in oral and
maxillofacial surgery (10,22). Manual measurements and digital
measurement has been compared previously. Some previous reports
have drawn the conclusion that manual and digital measurements are
similar and that they were both reliable (24,25),
while in another study the authors deemed the digital approach more
reliable (26).
As the auricle can become easily deformed during
manual measurement, error derived from distortion is common. The 3D
scanning requires no ear contact, and therefore, introduces no
distortion to the auricle, suggesting that digital measurement may
be more accurate compared with manual measurement. The position of
the measured subject and the perspective of the observer may also
influence the measurements, as previously described (27). Following data collection and
processing, all operations were performed in silico, where
the 3D images could be scrutinized at will to expose details if
necessary, especially for the selection of measurement points of
the auricle. Therefore, combined with traditional tools, this
method can provide a highly precise auricular measurements without
contact-mediated distortion.
Results from the present demonstrated the digital
measurement method is replicable and reliable, which carries
advantages over the manual method. No significant differences were
found between measurements of the five auricular parameters made by
the two surgeons using the digital method. However, significant
differences were found between measurements made by the two
surgeons using the manual method with non-uniformed indices. An
important indicator for the assessment of a new measurement method
is the reproducibility (28). In the
present study, ICC using a scale of 0–1 was calculated for this
purpose. The ICC values calculated from digital measurements ranged
from 0.901 to 0.987 demonstrating excellent reproducibility by
independent investigators. In comparison, ICC values from manual
measurements ranged from 0.526 to 0.807. This finding suggests that
the standardized digital measurement method is more repeatable and
reliable compared with the traditional manual method. Subsequently,
Pearson's product moment correlation analysis was utilized to
assess the correlation between CH and CA in addition to the
correlation between LA and WA. A moderate but significant positive
correlation was observed between CH and CA (0.4<r<0.7),
suggesting that higher ear location is correlated with a larger CA.
In the process of costal cartilage carving, increasing base
thickness would increase the cranioauricular angle. However, no
positive correlation between LA and WA was found (r=0.206).
A comprehensive auricular measurement method should
specifically analyze the main characteristics of the ear shape. The
significance of the LA and WA, which are used widely, is well known
(5). Some diagnosis of ear
deformations such as the prominent ear is dependent on
cranioauricular angles (7). In
addition, CH and CA are the key indices in diagnosing microtia
(20). The ALA is becoming a very
promising index in the diagnosis of constricted ear and other
abnormalities which are associated with substantial helix changes
(29). Therefore, in the present
study, a total of five parameters were measured, which contain
almost all the necessary data for the diagnosis, pre-operation
design and outcome evaluation of a variety of auricular
abnormalities.
This study has a number of limitations. No matter
which measurement method is used, inconsistent measurement points
can occur on different ears, resulting in the value measured to not
be representative of the maximum value. For instance, in the
measurement of the WA, many investigators choose the intersection
of the helix and the skull surface as the origin, but these
intersections can vary markedly in different cases (5). However, in the evaluation of therapy
outcomes, it is paramount that the same measurement points are
chosen before and after therapy for precise measurements to be
achieved.
In conclusion, measurement of LA, WA, ALA, CH and CA
using the standardized digital method combining 3D scanning
technology and Mimics software is more precise, convenient,
reproducible and reliable compared with the traditional manual
method. The LA, WA, ALA, CH and CA measured for the evaluation of
different auricle abnormalities and healthy auricles are
comprehensive, efficient and simple, and a positive correlation
between CH and CA was found in the present study.
Acknowledgements
Not applicable.
Funding
The research reported in this publication was
supported by the CAMS Innovation Fund for Medical Sciences (grant
nos. CAMS-I2M-1-007 and CIFMS 2016-12M-2-006), PUMC Graduate
Innovation Fund (grant no. 2018-1002-02-20), the Beijing Municipal
Science & Technology Commission (grant no. Z161100000516098)
and PUMC Youth Fund and the Fundamental Research Funds for the
Central Universities (grant no. 33320140171).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
DW, HYJ, BP and LL designed the current study. DW,
HYS and XBY contributed to acquisition and analysis of patient
data. LL, HYJ, QHY and LRH supervised and managed the study. HYJ,
QHY and LRH performed the surgeries. DW and LL wrote the
manuscript. HYJ, QHY, LRH, HYS, XBY and BP revised the manuscript.
DW, HYJ and LL contributed to the acquisition of funding. All
authors gave their approval to the final version of this
manuscript.
Ethics approval and consent to
participate
Ethical approval of the study was obtained from the
Institutional Review Board of Plastic Surgery Hospital of Peking
Union Medical College. All parents or guardians of the patients
granted informed consent to participate in the present study.
Patient consent for publication
Informed consents from all patients included in the
current study were obtained for publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Pawar SS, Koch CA and Murakami C:
Treatment of prominent ears and otoplasty: A contemporary review.
JAMA Facial Plast Surg. 17:449–454. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mohammadi AA, Imani MT, Kardeh S, Karami
MM and Kherad M: Non-surgical management of congenital auricular
deformities. World J Plast Surg. 5:139–147. 2016.PubMed/NCBI
|
|
3
|
Akter F, Mennie JC, Stewart K and
Bulstrode N: Patient-reported outcome measures in microtia surgery.
J Plast Reconstr Aesthet Surg. 70:416–424. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Farkas LG: Anthropometry of the normal and
defective ear. Clin Plast Surg. 17:213–221. 1990.PubMed/NCBI
|
|
5
|
Zhao H, Lin G, Seong YH, Shi J, Xu J and
Huang W: Anthropometric research of congenital auricular
deformities for newborns. J Matern Fetal Neonatal Med.
32:1176–1183. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Leclère FM, Trelles M and Mordon SR:
Cartilage reshaping for protruding ears: A prospective long term
follow-up of 32 procedures. Lasers Surg Med. 43:875–880. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
da Silva Freitas R, Sanchez ME, Manzotti
MS, Baras F, Ono MC and de Oliveira e Cruz GA: Comparing
cephaloauricular and scaphaconchal angles in prominent ear patients
and control subjects. Aesthetic Plast Surg. 32:620–623. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kobayashi S and Maegawa J: Ear elevation
using 2-tiered costal cartilage on the same side as the
reconstructed framework. J Craniofac Surg. 22:1796–1799. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jiafeng L, Jiaming S and Xiaodan L:
Auricular reconstruction using a novel three-flap technique
improves the auriculocephalic angle. J Plast Reconstr Aesthet Surg.
69:1430–1435. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
You W, Liu LJ, Chen HX, Xiong JY, Wang DM,
Huang JH, Ding JL and Wang DP: Application of 3D printing
technology on the treatment of complex proximal humeral fractures
(Neer3-part and 4-part) in old people. Orthop Traumatol Surg Res.
102:897–903. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhao X, Yu RT, Li JS, Xu K and Li X:
Clinical value of multi-slice 3-dimensional computed tomographic
angiography in the preoperative assessment of meningioma. Exp Ther
Med. 6:475–478. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Glittenberg C and Binder S: Using 3D
computer simulations to enhance ophthalmic training. Ophthalmic
Physiol Opt. 26:40–49. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li L, Zeng L, Lin ZJ, Cazzell M and Liu H:
Tutorial on use of intraclass correlation coefficients for
assessing intertest reliability and its application in functional
near-infrared spectroscopy-based brain imaging. J Biomed Opt.
20:508012015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Thorne CH and Wilkes G: Ear deformities,
otoplasty, and ear reconstruction. Plast Reconstr Surg.
129:e701–e716. 2012. View Article : Google Scholar
|
|
15
|
Lee BM, Kang SJ and Sun H: Simple
aesthetic correction for patients with acute auriculocephalic
angle. Arch Craniofac Surg. 16:24–28. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jiang H, Pan B, Zhao Y, Lin L, Liu L and
Zhuang H: A 2-stage ear reconstruction for microtia. Arch Facial
Plast Surg. 13:162–166. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Shinohara H, Matsuo K, Hataya Y and Taki
K: Correlation between projection of the ear, the inferior crus,
and the antihelical body: Analysis based on computed tomography.
Scand J Plast Reconstr Surg Hand Surg. 41:288–292. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Johns AL, Lucash RE, Im DD and Lewin SL:
Pre and post-operative psychological functioning in younger and
older children with microtia. J Plast Reconstr Aesthet Surg.
68:492–497. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
DellaCroce FJ, Green S and Aguilar EF III:
Framework growth after reconstruction for microtia: Is it real and
what are the implications? Plast Reconstr Surg. 108:1479–1486.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhou J, Pan B, Yang Q, Zhao Y, He L, Lin
L, Sun H, Song Y, Yu X, Sun Z and Jiang H: Three-dimensional
autologous cartilage framework fabrication assisted by new additive
manufactured ear-shaped templates for microtia reconstruction. J
Plast Reconstr Aesthet Surg. 69:1436–1444. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Khamaisy S, Zuiderbaan HA, Thein R, Nawabi
DH, Joskowicz L and Pearle AD: Coronal tibiofemoral subluxation: A
new measurement method. Knee. 21:1069–1071. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Huang JW, Shan XF, Lu XG and Cai ZG:
Preliminary clinic study on computer assisted mandibular
reconstruction: The positive role of surgical navigation technique.
Maxillofac Plast Reconstr Surg. 37:202015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Asif MK, Nambiar P, Mani SA, Ibrahim NB,
Khan IM and Sukumaran P: Dental age estimation employing CBCT scans
enhanced with Mimics software: Comparison of two different
approaches using pulp/tooth volumetric analysis. J Forensic Leg
Med. 54:53–61. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Leifert MF, Leifert MM, Efstratiadis SS
and Cangialosi TJ: Comparison of space analysis evaluations with
digital models and plaster dental casts. Am J Orthod Dentofacial
Orthop. 136:16.e1–e4; discussion 16. 2009. View Article : Google Scholar
|
|
25
|
Bootvong K, Liu Z, McGrath C, Hägg U, Wong
RW, Bendeus M and Yeung S: Virtual model analysis as an alternative
approach to plaster model analysis: Reliability and validity. Eur J
Orthod. 32:589–595. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Santoro M, Galkin S, Teredesai M, Nicolay
OF and Cangialosi TJ: Comparison of measurements made on digital
and plaster models. Am J Orthod Dentofacial Orthop. 124:101–105.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Correia GD, Habib FA and Vogel CJ:
Tooth-size discrepancy: A comparison between manual and digital
methods. Dental Press J Orthod. 19:107–113. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Nawi N, Mohamed AM, Marizan Nor M and
Ashar NA: Correlation and agreement of a digital and conventional
method to measure arch parameters. J Orofac Orthop. 79:19–27. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang D, Pan B, Lin L, Yang Q, He L, Song
Y, Zhou J and Jiang H: New methods for specialized subjective and
high-precision objective evaluation of constricted ears: A pilot
study. Medicine (Baltimore). 97:e129972018. View Article : Google Scholar : PubMed/NCBI
|