Introduction
Percutaneous coronary interventions (PCIs) are
widely performed as an invasive intervention to treat patients with
acute coronary syndromes (ACSs) including non-ST-elevation ACS
[including unstable angina (UA) and non-ST-elevation myocardial
infarction (NSTEMI)] and ST-elevated myocardial infarction (STEMI).
It is well-established that PCI induces elevated levels of
inflammatory mediators and pathophysiological levels of reactive
oxygen species (ROS) production, which leads to an occurrence of
restenosis, stent thrombosis and other adverse cardiovascular
events in patients with ACS after PCI (1–4).
Inflammatory markers have been implicated as the
most important risk indicators in the development of restenosis and
may be predictive of poor cardiovascular outcomes in ACS patients
undergoing coronary angiography (4–7). The
concentration of inflammatory cytokines also correlates with the
occurrence of stent restenosis. Furthermore, oxidative stress is
involved in the pathogenesis of cardiovascular diseases, which is
characterized by an imbalance between the generation of ROS and the
capacity of the intrinsic antioxidant defense system (8). Research has documented that oxidative
stress indicators released from stenotic and symptomatic lesions in
patients undergoing PCI participate in the development of new
lesions, and increase the risk of major adverse cardiovascular
events (MACE) such as cardiovascular death, myocardial infarction
(MI) and stroke (9–13).
Nicorandil is a hybrid agent with distinctive
pharmacological function as an ATP-sensitive potassium channel
(KATP) opener and a nitric oxide donor. The mechanism of
nicorandil includes not only dilation of both the macrovascular and
microvascular systems but also has potential cardio-protective
effects. Intracoronary (IC) injection of nicorandil has been
reported to be safe for patients with coronary artery disease (CAD)
during PCI (14–18). Additionally, it was found to improve
the prognosis of patients with acute heart failure (AHF) (16), and to ameliorate both early
functional defection (17) and
long-term complications of acute myocardial infarction (AMI).
However, the effects of intracoronary nicorandil injection on
inflammation and oxidative stress remain unclear in patients with
ACS undergoing PCI as no data are available at present. Thus, the
present study was performed to evaluate the feasibility and
efficacy of IC nicorandil injection for the improvement of
inflammation and oxidative stress in patients with ACS undergoing
PCI.
Materials and methods
Study population
This single-blinded, randomized prospective and
clinical trial was performed at the Department of Cardiology, Qilu
Hospital, Shandong University, Jinan, Shandong, China. Patients
were eligible if they were age 30 years or older and admitted to
our institution for ACS. The diagnosis of ACS was based on clinical
symptoms, electrocardiographic changes compatible with AMI, and
elevation of cardiac biomarkers (18). This study enrolled patients with AMI
and unstable angina pectoris. Clinical symptoms of ACS were as
follows: Angina pectoris including chest pain with or without
radiating to the neck, jaw, upper abdomen or shoulder. AMI was
defined as episodes of chest pain persisting >30 min and <24
h, ST-segment elevation in at least two continuous
electrocardiogram leads, and more than two-fold creatine kinase
(CK) elevation above the maximum peak in the normal range (19). The diagnosis of unstable angina
pectoris was based on typical precordial chest pain at rest,
angiographic evidence of a stenosis ≥75% according to the American
Heart Association (AHA) classification (11) and no elevation of cardiac
biomarkers.
Exclusion criteria were as follows: Age >90
years; patients with history of coronary artery bypass grafting
(CABG); systolic blood pressure (BP), 80 mmHg; known allergy to
aspirin, clopidogrel, ticagrelor or nicorandil; bleeding history
within the prior 3 months; cancer or other severe comorbidity
affecting life expectancy. NSTEMI patients are not eligible for
stent implantation, thus they were also excluded.
Finally, 65 consecutive participants with a
diagnosis of ACS were recruited to the trial after providing
written informed consent for angiography, PCI and blood extraction.
All patients were admitted to our hospital between March 2016 and
May 2017. This study was approved by the Qilu Hospital Ethics
Committee (KYLL-2015266). All procedures were performed as standard
interventional techniques following current guidelines at the time
of intervention.
Procedures
Sixty-five patients with ACS were randomly divided
into two groups: A nicorandil treatment group and a control group.
The 32 patients in the nicorandil group received an IC bolus of
nicorandil (2 mg/2 ml) before reperfusion with PCI and the 32
patients in the control group received the same volume of
physiological saline. PCIs were performed due to stenosis-related
coronary artery. Next, 3,000 units of heparin was injected after
the achievement of arterial access, and adjunctive injections of
7,000 units were needed for patients undergoing PCI. IC
administration of nitroglycerin was used to achieve the maximal
vasodilation for all patients before the initial and final
angiograms. PCI was performed following standard procedures.
A total dose of 12 mg nicorandil was dissolved in 12
ml of 0.9% saline. Two milliliters of nicorandil in the nicorandil
group and 2 ml saline in the control group were administered,
respectively, by IC bolus injection before percutaneous
transluminal coronary angioplasty (PTCA). All other procedures were
the same for both treatment groups. The cardiologist in-charge
performed PCI and IC injection of nicorandil or saline in the
catheter laboratory at the appropriate time. No angiographical
residual stenosis was detected in any patients and there were no
deaths during PCI. No follow-up data, such as complications,
mortality and long-term effect of nicorandil, were available in
this study. After all procedures, patients were maintained on
aspirin (100 mg once daily) plus clopidogrel (75 mg once daily) or
ticagrelor (90 mg twice daily) for at least 1 year after metal
stent placement followed by the physician's specific
directions.
Collection and preservation of
coronary blood
Approximately 10 ml of intracoronary blood was
collected from the distal coronary stenosis with a Finecross
micro-catheter (Asahi Intecc Co., Ltd.) before the injection of
nicorandil or saline prior to PTCA, and immediately after the stent
placement in patients undergoing PCI. The blood samples were
collected in vacutainer anticoagulant tubes at room temperature for
~30 min and then centrifuged for 10 min at 1,000 × g. Plasma and
serum were aliquoted and stored at −80°C until further
analysis.
Measurement of SOD and MDA
Superoxide dismutase (SOD) was examined using an SOD
determination kit (cat. no. 19160; Sigma-Aldrich; Merck KGaA)
following the manufacturer's instructions. Each sample was measured
with three replicates of four samples: Sample, Blank 1, Blank 2 and
Blank 3. The Sample subset consisted of 20 µl sample solution, 200
µl of WST working solution and 20 µl of enzyme working solution.
Then the sample solution was substituted by 20 µl of enzyme working
solution as Blank 1. Blank 2 consisted of 20 µl sample solution,
200 µl of WST working solution and 20 µl of dilution buffer.
Finally, 20 µl sample solution was substituted by 20 µl of enzyme
working solution in Blank 3 compared with Blank 2. The plates were
incubated at 37°C for 20 min and the absorbance was read at 450 nm
using a microplate reader. The SOD activity calculation formula is
as follows: SOD activity (inhibition rate %)={((ABlank 1-ABlank
3)-(ASample-ABlank 2))/(ABlank 1-ABlank3)} ×100.
Malondialdehyde (MDA) was measured with the Lipid
Peroxidation Assay Kit (cat. no. MAK085; Sigma-Aldrich; Merck KGaA)
according to the manufacturer's instructions. The MDA standard
solution was used to generate blank, 0.4, 0.8, 1.2, 1.6 and 2.0
nmol standards to create a standard curve. Plasma samples (10 µl)
were gently mixed with 500 µl of 42 mM sulfuric acid. Then 125 µl
of phosphotungstic acid solution was added and mixed by vortexing.
After incubation at room temperature for 5 min and centrifugation
at 13,000 × g for 3 min, the pellet was resuspended on ice with a
water/BHT solution. TBA solution was added to each sample including
standards and they were incubated at 95°C for 1 h. Then, 200 µl of
each sample mixture and standard were pipetted into a 96-well plate
and the absorbance was measured at 532 nm. The concentrations of
MDA in samples were calculated using the previously determined
standard curve. Three replicates were conducted for each
sample.
Measurement of sCD40L, tumor necrosis
factor α (TNFα), high-sensitivity C-reactive protein (hs-CRP),
intercellular adhesion molecule-1 (ICAM-1) and vascular cell
adhesion molecule-1 (VCAM-1)
Enzyme-linked immunosorbent assay (ELISA) was used
to determine the inflammatory factors for each plasma sample
according to the manufacturer's instructions. A serial dilution of
purified standards was used to generate a standard curve to measure
the cytokine levels in a semi-quantitative way. Kits purchased from
R&D Systems were used to detect the plasma or serum levels of
soluble CD40L (cat. no. DCDL40, Human CD40 Ligand/TNFSF5 Quantikine
ELISA kit), TNFα (cat. no. DTA00D, Human TNF-α Quantikine ELISA
kit), hs-CRP (cat. no. DCRP00, Human C-Reactive Protein/CRP
Quantikine ELISA kit), I-CAM (cat. no. DCD540, Human ICAM-1/CD54
Allele-specific Quantikine ELISA kit) and V-CAM (Cat. no. PDVC00,
Human sVCAM-1/CD106 Quantikine ELISA kit). Three replicates were
examined for each sample.
Statistical analysis
Data are shown as the mean ± SD and three replicates
were conducted for each analysis. Differences between the
nicorandil and placebo groups were analyzed by the two-tailed
paired t-test for continuous outcome variables. This test was used
for comparing the pre-PCI and post-PCI values within the nicorandil
and control groups. The comparisons between non-continuous
variables were performed using the χ2 test. SPSS
statistical software package, version 17.0 (SPSS Inc.) was used for
analysis. A P-value <0.05 was considered statistically
significant.
Results
Patient baseline characteristics
In this study, a total of 65 consecutive patients
were enrolled with 32 randomly allocated to the nicorandil and 33
to placebo groups. The baseline characteristics of the two groups
are shown in Table I. There were no
significant differences in age, sex, BMI, incidence of coronary
risk factors, serum creatinine or urea nitrogen levels, ejection
fraction (EF), previous MI history, culprit lesions or quantitative
angiographic data between the two groups. Clinically, 5 patients
(15.6%) and 3 patients (9.1%) were diagnosed with myocardial
infarction (MI) in the nicorandil group and placebo group,
respectively. Other patients were diagnosed with unstable angina
(UA). There were no significant differences in the use of oral
medications at discharge among all patients.
 | Table I.Patients and characteristics of the
lesion. |
Table I.
Patients and characteristics of the
lesion.
|
| Groups |
|---|
|
|
|
|---|
|
Characteristics | Nicorandil
(n=32) | Placebo (n=33) | P-value |
|---|
| Age, in years | 60.0±10.0 | 61.8±9.7 | 0.466 |
| Male, n (%) | 21 (65.6) | 21 (63.6) | 0.869 |
| BMI,
kg/m2 | 26.7±4.1 | 26.0±3.3 | 0.459 |
| Cardiovascular risk
factors, n (%) |
|
Hypertension | 23 (71.9) | 22 (66.7) | 0.655 |
|
Diabetes mellitus | 8 (25) | 11 (34.4) | 0.468 |
|
Hyperlipidemia | 12 (37.5) | 13 (39.4) | 0.878 |
|
Smoking | 16 (50) | 15 (45.5) | 0.719 |
| Cr, µmol-/l | 72.91±11.63 | 69.94±17.75 | 0.430 |
| BUN, mg/dl | 5.22±1.88 | 8.89±15.93 | 0.198 |
| Previous MI, n
(%) | 3 (9) | 3 (9) | 0.968 |
| Number
of vessels occluded | 1.33±0.58 | 1.33±0.58 | 1.000 |
| EF, % | 62.8±6.4 | 60.1±8.7 | 0.157 |
| Clinical diagnosis,
n (%) |
| MI | 5
(15.6) | 3 (9.1) | 0.431 |
| UA | 28 (84.4) | 30 (90.9) | 0.431 |
| Quantitative
coronary angiography |
| Percent
diameter stenosis, % | 89.3±7.1 | 87.0±7.5 | 0.236 |
| Vessel undergoing
PCI, n |
| Left
anterior descending artery | 21 | 19 | 0.681 |
| Left
circumflex artery | 3 | 4 | 0.726 |
| Right
coronary artery | 8 | 10 | 0.468 |
| Vessel diameter,
mm | 23.06±7.52 | 26.79±9.04 | 0.07 |
| Therapy, % |
|
Aspirin | 100 | 100 | 1.000 |
|
Clopidogrel | 90.9 | 93.8 | 0.378 |
|
ACEI | 93.75 | 93.94 | 0.975 |
|
ARB | 6.25 | 6.06 | 0.975 |
|
β-blocker | 100 | 100 | 1.00 |
|
Statin | 100 | 100 | 1.00 |
|
Glycoprotein IIb/IIIa
inhibitor | 9.1 | 6.2 | 0.623 |
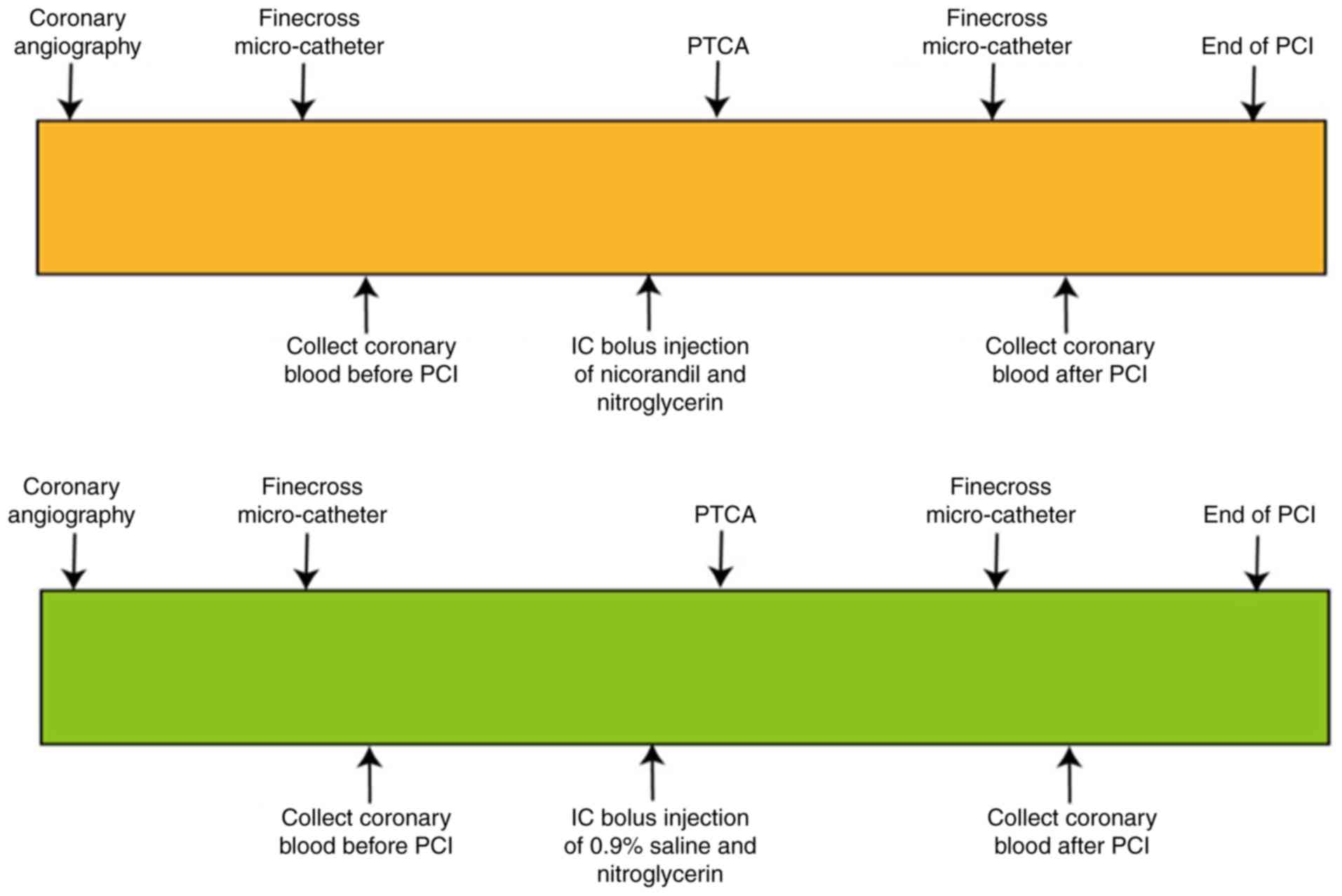
Outline of the PCI procedures
Coronary angiography was performed to visualize the
severity of coronary stenosis. The subsequent treatment of PTCA was
followed up if the residual diameter stenosis was greater than or
equal to 75% of the coronary artery stenosis diameter. The
Finecross micro-catheter reached the distal coronary stenosis
guided by a coronary guide-wire, and 10 ml of coronary blood was
collected before PCI. Then 2 ml nicorandil (1 mg/ml) or placebo (2
ml of 0.9% saline) was IC bolus injected into coronary ostia. After
nicorandil (or placebo) injection, PCI was performed according to
standard techniques. Another 10 ml of coronary blood was collected
immediately after stent implantation (Figs. 1 and S1).
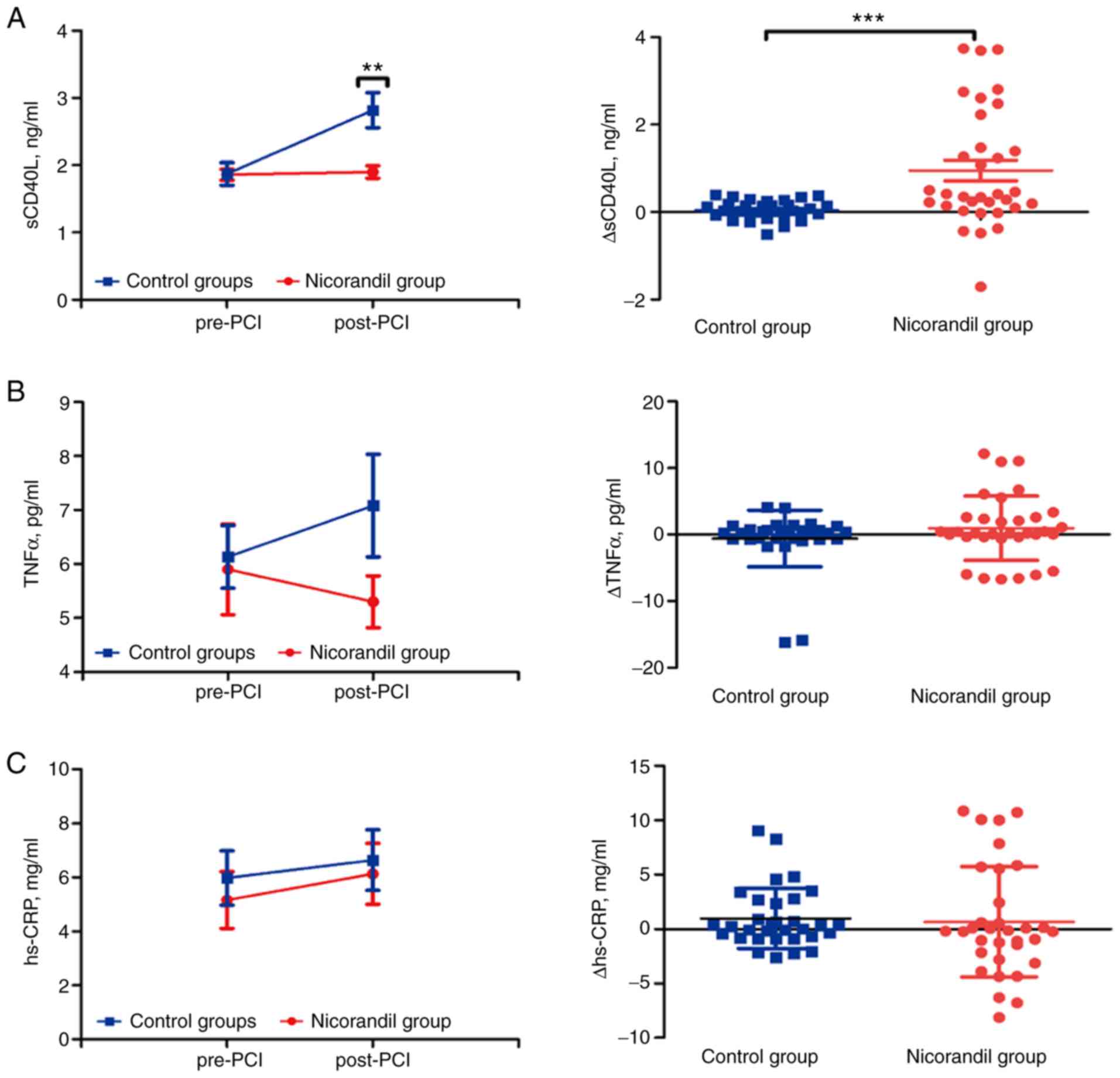
Effect of nicorandil on markers of
inflammation
There was a significant increase in soluble CD40
ligand (sCD40L) levels in the plasma of post-PCI compared with
pre-PCI in the control group (1.87±0.17 vs. 2.82±0.26 ng/ml,
P<0.001), but no difference in the nicorandil group in both pre-
and post-PCI (1.86±0.08 vs. 1.90±0.09 ng/ml, P=0.12) (Fig. 2A). Compared with post-PCI in the
control group, there was a significant reduction in sCD40L levels
in the nicorandil group (P=0.001) (data not shown). The amount of
change (Δ value) for sCD40L was significantly increased in the
control group with no difference in the nicorandil group (0.04±0.04
vs. 0.95±0.23 ng/ml, P<0.001; Fig.
2A). No significant change was found in pre- and post-PCI
levels of TNFα in the nicorandil group (5.90±0.84 vs. 5.3±2.73
pg/ml, P=0.43) and control group (6.13±0.58 vs. 7.08±0.95 pg/ml,
P=0.29) (Fig. 2B). In comparison,
there was no difference between pre-PCI and post-PCI in levels of
IC plasma hs-CRP in the nicorandil group (5.16±1.05 vs. 6.13±1.13
mg/ml, P=0.054) and in the control group (5.98±1.01 vs. 6.64±1.12
mg/ml, P=0.458) (Fig. 2C). The Δ
value of both TNFα (−0.60±0.75 vs. 0.95±0.84 pg/ml, P=0.405) and
hs-CRP (0.98±0.49 vs. 0.66±0.88 mg/ml, P=0.246) remained
statistically unchanged (Fig. 2B and
C). Thus, the inflammatory sCD40L marker was significantly
improved during PCI due to the intracoronary bolus injection of
nicorandil.
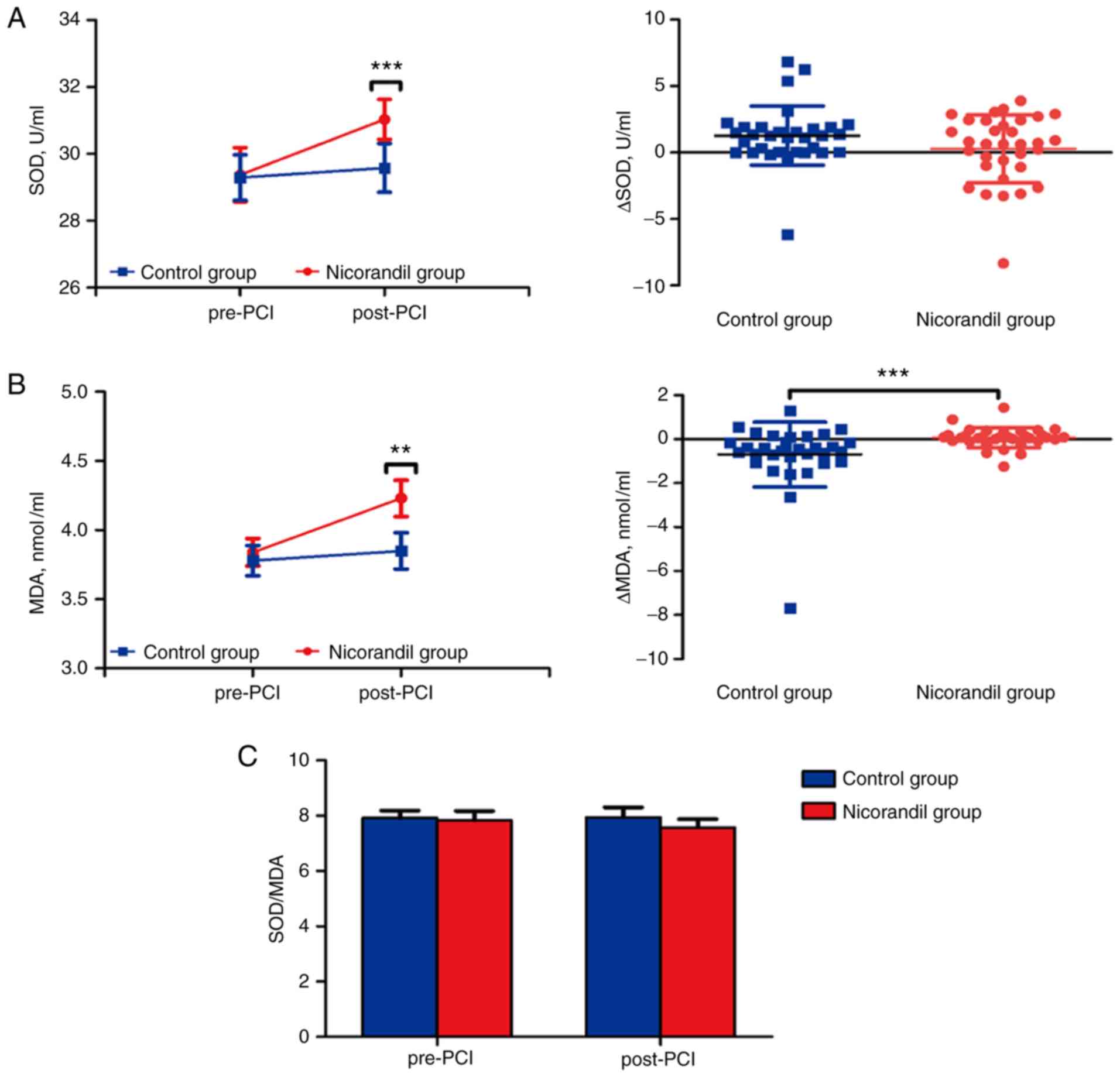
Effect of nicorandil on indicators of
oxidative stress
SOD and MDA indicators were measured to investigate
the effect of nicorandil on oxidative stress. SOD was significantly
increased in the plasma of post-PCI compared with pre-PCI in
nicorandil group (29.37±0.81 vs. 31.03±0.60 U/ml, P<0.001), and
no difference was observed between time-points in the control group
(29.29±0.68 vs. 29.58±0.73 U/ml, P=0.519) (Fig. 3A). Additionally, MDA was
significantly increased in plasma of post-PCI compared to pre-PCI
in the nicorandil group (3.84±0.10 vs. 4.230±0.13 mmol/ml,
P=0.001), and no difference was observed between time-points in the
control group (3.78±0.11 vs. 3.85±0.13 mmol/ml, P=0.402) (Fig. 3B). Surprisingly, the ratio of SOD and
MDA was unchanged in four time-point subgroups of both the
nicorandil (7.84±0.33 vs. 7.58±0.30, P=0.241) and control
(7.92±0.27 vs. 7.95±0.35, P=0.888) group (Fig. 3C). There also was no difference in
the Δ value of SOD (1.28±0.39 vs. 0.29±0.45 U/ml, P=0.328) in the
control vs. nicorandil group, but a significant increase in levels
of MDA (−0.70±0.26 vs. 0.07±0.08 mmol/ml, P<0.001) in the
control group compared with the nicorandil group (Fig. 3A and B).
These results indicated that nicorandil may relieve
oxidative stress via increased levels of SOD, but the levels of MDA
were also subsequently increased. The possible change in ratio
between SOD and MDA during PCI may be based on operational injury
and the delayed reaction of the plasma levels to oxidative stress
indicators.
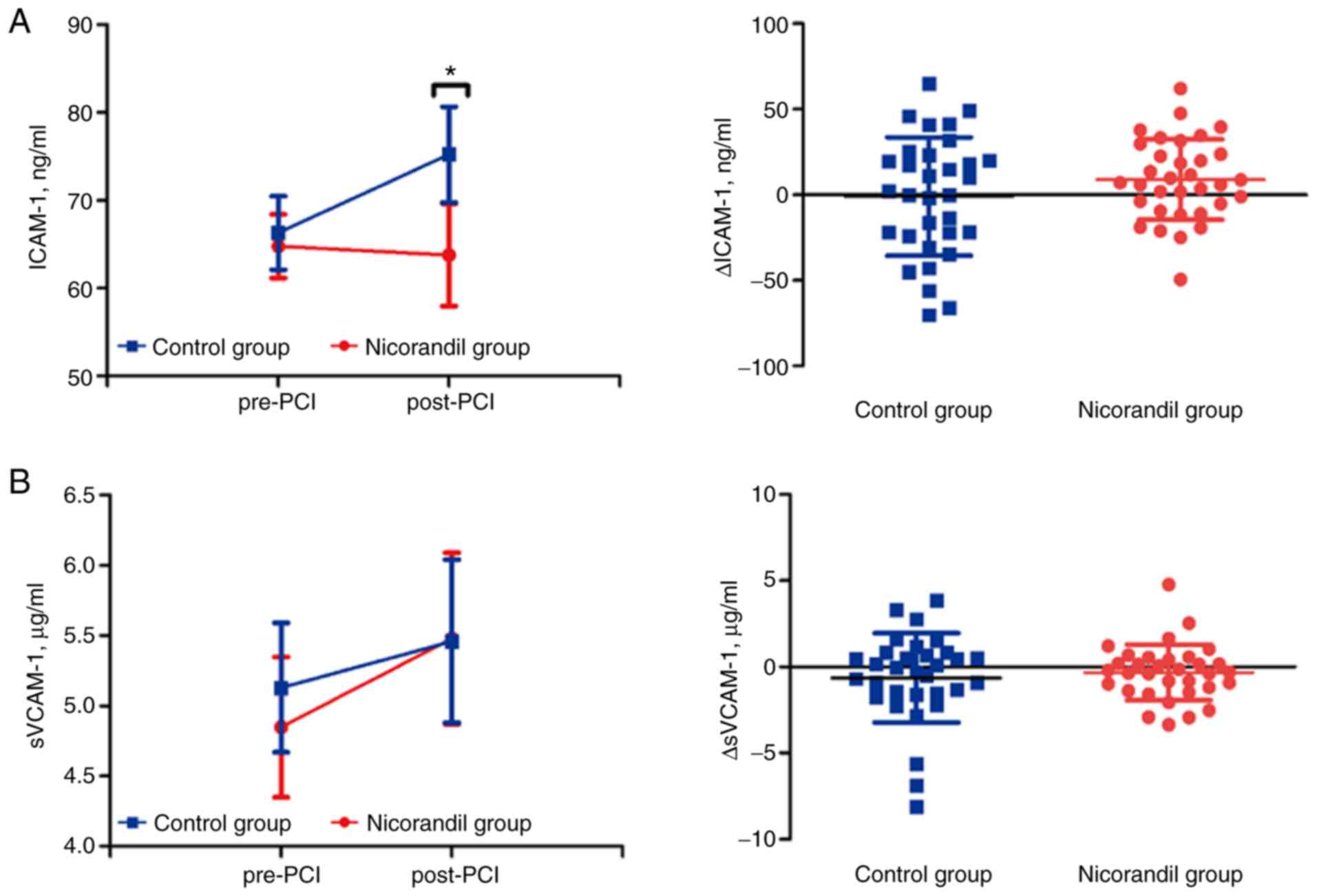
Effect of nicorandil on angiokinetic
factors
To further explore the effects of bolus injection of
nicorandil during PCI, we also measured two different functional
angiokinetic factors, ICAM-1 and sVCAM-1 post-PCI compared with
pre-PCI. The results showed no significant differences in ICAM-1 in
the nicorandil group (64.79±3.63 vs. 63.80±5.85 ng/ml, P=0.827).
However, levels of ICAM-1 in the control group were increased after
PCI (66.30±4.17 vs. 75.24±5.46 ng/ml, P=0.002) (Fig. 4A). There was also no change in levels
of sVCAM-1 in the nicorandil group (4.85±0.61 vs. 5.48±0.61 µg/ml,
P=0.175) compared to placebo group (5.13±0.46 vs. 5.46±0.58 µg/ml,
P=0.255) (Fig. 4B). The Δ values
both for ICAM-1 (−0.99±6.12 vs. 8.94±4.10 ng/ml, P=0.285) and
sVCAM-1 (−0.63±0.46 vs. −0.33±0.28 µg/ml, P=0.927) also showed no
difference between the two groups (Fig.
4A and B). Nicorandil may improve the angiokinetic factor of
ICAM-1 to hinder any inflammatory reaction during PCI in ACS
patients.
Discussion
The present study presents for the first time the
effects of intracoronary (IC) bolus injection of nicorandil or
placebo on markers of inflammation and oxidative stress in patients
with acute coronary syndrome (ACS) undergoing percutaneous coronary
interventions (PCIs). In this randomized, single-blinded and
placebo-controlled study, it was confirmed in a brief period that
percutaneous transluminal coronary angioplasty (PTCA) results in
the upregulation of inflammation and oxidative stress. Coronary
blood, which has a greater impact on the coronary artery compared
with the peripheral blood, was used to evaluate serum as well as
plasma levels of inflammatory and oxidative markers to precisely
investigate temporal changes during PCI. It was also demonstrated
that an IC bolus injection of nicorandil in patients with ACS is
safe and significantly reduced soluble CD40 ligand (sCD40L),
superoxide dismutase (SOD), malondialdehyde (MDA) and intercellular
adhesion molecule-1 (ICAM-1) levels after PCI. However, no changes
in other systemic inflammation markers, such as high-sensitivity
C-reactive protein (hs-CRP), tumor necrosis factor α (TNFα) and
soluble vascular cell adhesion molecule-1 (sVCAM-1) levels were
observed in the nicorandil or control groups. This finding could
possibly be due to delayed inflammatory responses.
PCI has become a standard revascularization
procedure and the main management option for patients with ACS.
However, PTCA induces vascular injury and wreaks damage on the
endothelium which is associated with pro-inflammatory responses and
platelet-activating effects with adhesion (20,21).
This damage also elicits an inflammatory response via the
activation of platelets and leukocytes (22). PCI-induced vascular injury and
ischemia/reperfusion injury was found to result from both
intracellular calcium loading due to ATP depletion and
intracellular acidification (23),
and the occurrence of oxidative stress with the mitochondrial
respiratory chain as the main source of reactive oxygen species
(ROS) (24).
Nicorandil, as a hybrid nitrate and ATP-sensitive
potassium channel opener agent (25), has been shown not only to dilate
systemic veins, but also to exert a vaso-dilative effect on
arteries, including peripheral arteries (16). Moreover, IC bolus injection of
nicorandil is safe and efficacious for myocardial protection,
ameliorating fractional flow reserve (FFR) and ischemia/reperfusion
injury (26,27). Kawai et al found that
intravenous administration of nicorandil could prevent slow
coronary flow phenomenon compared with that of 0.9% saline before
PCI in patients with ACS or non-ACS (28). Previous research further found that
IC bolus injection of nicorandil is safe and effective compared
with IC adenosine to induce hyperemia in patients with an
angiographically intermediate lesion (27). Lee et al compared IC bolus
injection of nicorandil with intravenous infusion of adenosine
(26). Different from previous
studies, we firstly IC injected the same volume of saline in ACS
patients since no placebo effect was observed in those studies
which further increased the importance of our study. We also
collected coronary blood to perform ELISA to evaluate the levels of
inflammatory or oxidative indicators during PCI. A previous study
also showed that nicorandil improves microvascular dysfunction as
assessed by the index of microcirculatory resistance after PCI
(29).
The soluble CD40 ligand (sCD40L), as a member of the
TNF family, is expressed widely on monocytes, dendritic cells,
endothelial cells and epithelial cells (30). Activation of platelets was shown to
result in the release of sCD40L, accelerating the inflammatory
process and promoting coagulation (31–34). A
previous study showed that sCD40L may be a predictor of coronary
artery disease in patients undergoing PCI (35). Thus, we evaluated the level of sCD40L
in pre-PCI and post-PCI subgroups in the nicorandil and control
groups. Its expression level in intracoronary plasma increased
after the stent implantation compared with pre-PCI in the placebo
group which is consistent with other trials (35,36). The
IC bolus injection of nicorandil also improved the alleviation of
sCD40L in the post-PCI subgroup immediately as there were no
significant changes compared with the post-PCI and pre-PCI
subgroup. Our trial further confirmed that nicorandil has the
ability to improve the inflammatory reaction of sCD40L during PCI
in ACS patients.
Other inflammation indicators, such as TNFα and
hs-CRP, had no significant differences in both nicorandil and
placebo groups and their subgroups. Although PCI led to a
platelet-activating effect with adhesion and sCD40L participates in
the promotion of coagulation, the adhesion molecule sVCAM-1 also
exhibited no difference in the different groups although ICAM-1 was
clearly induced in the control group after PCI. The reasons for
this finding may be as follows. Firstly, Aströmolsson et al
demonstrated that TNFα increased during the 24 h of reperfusion
(37). Hs-CRP, an acute-phase
reactant, increased markedly at 6 h after PCI and reached a peak
value at 48 h which indicates that there is a delayed reaction of
these inflammatory markers after PCI (37,38).
Consequently, the underlying improvement of inflammatory indicators
with nicorandil may not react and reflect changes immediately after
operation. Secondly, Bayata et al measured VCAM-1 and
sICAM-1 serum levels in patients before and after stent
implantation and found no difference in VCAM-1 and ICAM-1 levels
(39). Similarly, Wexberg et
al found increased levels of VCAM-1 after stent implantation
(40). Thus, the differences between
the above trials and our results may be due to different sourcing
of serum or plasma as our samples came from the intracoronary blood
drawn by the micro-catheter. Another reason may be a difference in
patient ethnicity and the reactivity to PTCA. The small sample size
may also be one of the reasons for this difference.
Reactive oxygen species (ROS) are involved in
physiological cell regulation and redox signaling (41). SOD, which catalyzes the metabolism of
the superoxide anion (O2−) into hydrogen
peroxide and molecular oxygen, is one of the most important
antioxidative enzymes. MDA, the major end product of lipid
peroxidation, is one of the markers indicating partial levels of
oxidative stress. The production of MDA is initiated promptly after
the generation of ROS (42). Both
molecules directly reflect the expression levels of oxygen-free
radicals. Our results showed that both SOD and MDA levels have the
tendency to rise but there were no significant differences in both
subgroups of the control group. An investigation by Ekeløf et
al indicated that SOD was reduced significantly at 2 h after
PTCA (42), which suggests that the
consumption of SOD may require a series of processes. However, a
study by Demircan et al indicated that SOD was immediately
reduced after PCI compared to the pre-PCI subgroup (43). These controversial results require
further investigation due to the limited sample sizes employed.
In the present study, it was demonstrated that the
SOD levels in the post-PCI subgroup of the nicorandil group
significantly increased compared with the pre-PCI subgroup.
However, the MDA levels were also unexpectedly increased. The ratio
of SOD and MDA exhibited no significant change in the post-PCI
nicorandil group compared with the control groups. These results
showed that nicorandil reduced oxidative stress significantly as a
supplement to PCI. The over-production of free radicals at the
beginning of the ischemic phase is thought to be due to
mitochondrial depolarization. Nicorandil reduces ROS formation by
mitochondria by opening the mitochondrial KATP (44). Due to its free radical scavenging
properties and inhibition of oxidative respiratory bursting of
neutrophils (45), IC bolus
injection of nicorandil could function by reducing oxidative
stress. Furthermore, nicorandil plays a role in ameliorating
myocardial damage as well as improving cardiac function and
clinical outcomes.
The inflammatory response evoked by vascular damage
during angioplasty and the subsequent reaction are thought to be
the main contributors to the development of restenosis. Oxidative
stress also contributes to clinical outcomes such as adverse
cardiac events. IC bolus injection of nicorandil before
implantation of the coronary artery stent was associated with
better suppression of various inflammatory cytokines, and further
reduced the oxidative stress in patients who suffered from ACS
undergoing PCI. However, there were no definite clinical benefits
detected in the amelioration of adhesion molecules and inflammatory
mediators. Our findings suggest that IC bolus injection of
nicorandil is a simple, safe, and effective way to reduce the
levels of inflammation and oxidation during PCI which may be
attributable to improved outcomes for such ACS patients.
There were several limitations to the present study.
Firstly, the sample size of this study was small. It was necessary
to perform a power analysis before conducting the study. However,
no similar data could be found in the published articles which made
it difficult for us to assess the sample size. Thus, we enrolled 65
patients to ensure the normality of the data distribution. We
surprisingly found significant differences of sCD40L, SOD, MDA and
ICAM-1 between the two groups. Then, we performed the power
analysis through PASS based on our expression levels of sCD40L,
SOD, MDA and ICAM-1. We found that the value of 1-β was beyond 0.8.
Secondly, since nicorandil was only used during PCI and only 20 of
the enrolled patients took nicorandil regularly post-discharge, no
long-term observations of nicorandil was obtained. We followed up
the enrolled patients for only one month after PCI. No difference
in complications and mortality was found in the two groups after
one month. After surgery, the patients recovered well after regular
intake of the standard medicine. Finally, according to the new
guidelines of ECS for ACS patients, ticagrelor is recommended for
Class IA. However, ticagrelor is recommended for Class IB in China
at present. According to the 2016 Ticagrelor Expert Consensus in
China (46), ticagrelor should be
used as early as possible in NSTE-ACS patients who have a moderate
or high risk of ischemia and plan for early invasive treatment. We
previously used clopidogrel more often during our experimental
period according to our previous guidelines. More than 50% patients
now use ticagrelor instead of clopidogrel at present. We still need
to consider our clinical practice, Chinese national conditions,
individual differences and implement specific antithrombotic
strategies to choose the antiplatelet drugs. We will also follow up
the patients taking nicorandil after PCI for a longer period to
explore its long-term effect when we carry out a larger sample
study in future studies.
In conclusion, our trial showed that IC bolus
injection of nicorandil as part of therapy for patients with ACS
undergoing PCI reduced soluble CD40 ligand levels, increased MDA
and SOD levels, and decreased ICAM-1. However, none of the other
subclinical markers of inflammation were altered after the
injection of nicorandil and PCI surgery. These findings within the
context of this clinical trial suggest a solitary anti-oxidative
and anti-inflammatory effect of nicorandil. A larger sample size
and a longer treatment period with nicorandil are needed for
further investigation of the underlying and long-term beneficial
effects of this therapy.
The prospective, randomized design and use of
coronary angiography to diagnose ACS patients are the strengths of
this study. The percutaneous transluminal coronary angioplasty
(PTCA) showed that a residual stenosis diameter ≥75% of the
coronary artery combined with clinical symptoms are the gold
standard for identifying ACS patients.
Coronary blood was used to test serum or plasma
levels of inflammatory and oxidative markers, which was a better
measure of the coronary artery compared with peripheral blood as it
precisely reflected the effect on markers after stent
deployment.
The limitations of this study included a limited
sample size of 65 subjects, inflammatory or oxidative indicators
influenced by PTCA and limited time period for extraction of
coronary blood during PCA and stent deployment.
Supplementary Material
Supporting Data
Acknowledgements
This study was facilitated with the assistance of
many colleagues in the Department of Cardiology and Cardiac
Intervention Department of Shandong University Qilu Hospital. In
addition to the dedicated workers, the authors would especially
like to thank Professor Gui-Peng An, Wen-Qiang Chen and Qing Zhu
who helped in collecting and analyses of the blood samples. We also
thank the Professor Lu Wang for his help in English writing. Trial
registration: This study was approved by the Qilu Hospital Ethics
Committee (KYLL-2015266). Trial registration: Current Controlled
Trials ChiCTR1800019349, retrospectively registered on November 7,
2018.
Funding
The financial support received from different funds
was essential to conduct the blood investigations, finance the
staff who interviewed the patients, collection of the blood
samples, registration and analysis of the data. This work was
funded by the National 973 Basic Research Program of China (grant
no. 2015CB553604), the Program of Introducing Talents of Discipline
to Universities (grant no. B07035), the State Key Program of
National Natural Science of China (grant nos. 61331001 and
81530014), and the grants of the Shandong Province Natural Science
Fund (grant no. ZR2014CM010). All authors have reported that they
have no relationships relevant to the contents of this paper to
disclose.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MN, XX and XL conceived, designed and performed the
experiments. MN performed the PCI procedures and extracted coronary
blood at the appropriate time. XX, JM, SY and LY collected and
analyzed the data. All authors contributed to the interpretation of
data, drafted or revised the paper. All authors read and approved
the manuscript and agree to be accountable for all aspects of the
research in ensuring that the accuracy or integrity of any part of
the work are appropriately investigated and resolved.
Ethics approval and consent to
participate
This study was approved by the Regional Ethics
Committee of Shandong University Qilu Hospital, China (Reference
no. KYLL-2015266). All members of the operation team and patients
were informed of the PCI operation, stent implantation, nicorandil
injection and coronary blood extraction. Written consent was
obtained before PCI and PTCA. This was approved by the Regional
Ethics Committee.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ACS
|
acute coronary syndrome
|
|
AHF
|
acute heart failure
|
|
CABG
|
coronary artery bypass grafting
|
|
CAD
|
coronary artery disease
|
|
ELISA
|
enzyme-linked immunosorbent assay
|
|
FFR
|
fractional flow reserve
|
|
IC
|
intracoronary
|
|
MACE
|
major adverse cardiovascular
events
|
|
MDA
|
malondialdehyde
|
|
MI
|
myocardial infarction
|
|
NSTEMI
|
non-ST-elevation myocardial
infarction
|
|
PCI
|
percutaneous coronary intervention
|
|
PTCA
|
percutaneous transluminal coronary
angioplasty
|
|
ROS
|
reactive oxygen species
|
|
sCD40L
|
soluble CD40 ligand
|
|
SOD
|
superoxide dismutase
|
|
STEMI
|
ST-elevated myocardial infarction
|
|
TNFα
|
tumor necrosis factor α
|
|
hs-CRP
|
high-sensitivity C-reactive
protein
|
|
ICAM-1
|
intercellular adhesion molecule 1
|
|
VCAM-1
|
vascular cell adhesion molecule 1
|
|
UA
|
unstable angina
|
References
|
1
|
Ajtay Z, Németh A, Sulyok E, Cziráki A,
Szabados S, Martens-Lobenhoffer J, Awiszus F, Szabó C and
Bode-Böger SM: Effects of stent implementation on plasma levels of
asymmetric dimethylarginine in patients with or without ST-segment
elevation acute myocardial infarction. Int J Mol Med. 25:617–624.
2010.PubMed/NCBI
|
|
2
|
Kochiadakis GE, Arfanakis DA, Marketou ME,
Skalidis EI, Igoumenidis NE, Nikitovic D, Giaouzaki A, Chlouverakis
G and Vardas PE: Oxidative stress changes after stent implantation:
A randomized comparative study of sirolimus-eluting and bare metal
stents. Int J Cardiol. 142:33–37. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
O'Donoghue ML, Morrow DA, Cannon CP,
Jarolim P, Desai NR, Sherwood MW, Murphy SA, Gerszten RE and
Sabatine MS: Multimarker risk stratification in patients with acute
myocardial infarction. J Am Heart Assoc. 5(pii):
e0025862016.PubMed/NCBI
|
|
4
|
Mcclelland RL, Jorgensen NW, Budoff M,
Blaha MJ, Post WS, Kronmal RA, Bild DE, Shea S, Liu K, Watson KE,
et al: 10-year coronary heart disease risk prediction using
coronary artery calcium and traditional risk factors: Derivation in
the MESA (Multi-Ethnic Study of Atherosclerosis) with validation in
the HNR (Heinz Nixdorf Recall) study and the DHS (Dallas Heart
Study). J Am Coll Cardiol. 66:1643–1653. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Liuzzo G, Buffon A, Biasucci LM, Gallimore
JR, Caligiuri G, Vitelli A, Altamura S, Ciliberto G, Rebuzzi AG,
Crea F, et al: Enhanced inflammatory response to coronary
angioplasty in patients with severe unstable angina. Circulation.
98:2370–2376. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kubica J, Kozinski M, Krzewina-Kowalska A,
Zbikowska-Gotz M, Dymek G, Sukiennik A, Piasecki R, Bogdan M,
Grzesk G, Chojnicki M, et al: Combined periprocedural evaluation of
CRP and TNF-alpha enhances the prediction of clinical restenosis
and major adverse cardiac events in patients undergoing
percutaneous coronary interventions. Int J Mol Med. 16:173–180.
2005.PubMed/NCBI
|
|
7
|
Buffon A, Liuzzo G, Biasucci LM,
Pasqualetti P, Ramazzotti V, Rebuzzi AG, Crea F and Maseri A:
Preprocedural serum levels of C-reactive protein predict early
complications and late restenosis after coronary angioplasty. J Am
Coll Cardiol. 34:1512–1521. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ikeda U, Ito T and Shimada K:
Interleukin-6 and acute coronary syndrome. Clin Cardiol.
24:701–704. 2010. View Article : Google Scholar
|
|
9
|
Liuzzo G, Biasucci LM, Gallimore JR,
Grillo RL, Rebuzzi AG, Pepys MB and Maseri A: The prognostic value
of c-reactive protein and serum amyloid a protein in severe
unstable angina. N Engl J Med. 331:417–424. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fefer P, Tsimikas S, Segev A, Sparkes J,
Otsuma F, Kolodgie F, Virmani R, Juliano J, Charron T and Strauss
BH: The role of oxidized phospholipids, lipoprotein (a) and
biomarkers of oxidized lipoproteins in chronically occluded
coronary arteries in sudden cardiac death and following successful
percutaneous revascularization. Cardiovasc Revasc Med. 13:11–19.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Segev A, Strauss BH, Witztum JL, Lau HK
and Tsimikas S: Relationship of a comprehensive panel of plasma
oxidized low-density lipoprotein markers to angiographic restenosis
in patients undergoing percutaneous coronary intervention for
stable angina. Am Heart J. 150:1007–1014. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tsimikas S, Kiechl S, Willeit J, Mayr M,
Miller ER, Kronenberg F, Xu Q, Bergmark C, Weger S, Oberhollenzer F
and Witztum JL: Oxidized phospholipids predict the presence and
progression of carotid and femoral atherosclerosis and symptomatic
cardiovascular disease: Five-year prospective results from the
Bruneck study. J Am Coll Cardiol. 47:2219–2228. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Juni RP, Duckers HJ, Vanhoutte PM, Virmani
R and Moens AL: Oxidative stress and pathological changes after
coronary artery interventions. J Am Coll Cardiol. 61:1471–1481.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Miyazawa A, Ikari Y, Tanabe K, Nakajima H,
Aoki J, Iijima R, Nakayama T, Hatori M, Nakazawa G, Tanimoto S, et
al: Intracoronary nicorandil prior to reperfusion in acute
myocardial infarction. Eurointervention. 2:211–217. 2006.PubMed/NCBI
|
|
15
|
Kim SJ and Kim W, Woo JS, Ha SJ, Kang WY,
Hwang SH, Kang DG, Lee SU, Cho SK, Im JS and Kim W: Effect of
myocardial protection of intracoronary adenosine and nicorandil
injection in patients undergoing non-urgent percutaneous coronary
intervention: A randomized controlled trial. Int J Cardiol.
158:88–92. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chen C, Fu X, Li W, Jia X, Bai S, Geng W
and Xing K and Xing K: Intracoronary administration of anisodamine
and nicorandil in individuals undergoing primary percutaneous
coronary intervention for acute inferior myocardial infarction: A
randomized factorial trial. Exp Ther Med. 10:1059–1065. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ito H, Taniyama Y, Iwakura K, Nishikawa N,
Masuyama T, Kuzuya T, Hori M, Higashino Y, Fujii K and Minamino T:
Intravenous nicorandil can preserve microvascular integrity and
myocardial viability in patients with reperfused anterior wall
myocardial infarction. J Am Coll Cardiol. 33:654–660. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vilalta V, Asmarats L, Ferreira-Neto AN,
Maes F, de Freitas Campos Guimarães L, Couture T, Paradis JM,
Mohammadi S, Dumont E, Kalavrouziotis D, et al: Incidence, clinical
characteristics and impact of acute coronary syndrome following
transcatheter aortic valve replacement. JACC Cardiovasc Interv.
11:2523–2533. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ishii H, Ichimiya S, Kanashiro M, Amano T,
Imai K, Murohara T and Matsubara T: Impact of a single intravenous
administration of nicorandil before reperfusion in patients with
ST-segment-elevation myocardial infarction. Circulation.
112:1284–1288. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Breuss JM, Cejna M, Bergmeister H, Kadl A,
Baumgartl G, Steurer S, Xu Z, Koshelnick Y, Lipp J, De Martin R, et
al: Activation of nuclear factor-kappa B significantly contributes
to lumen loss in a rabbit iliac artery balloon angioplasty model.
Circulation. 105:633–638. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
van Dijk RA, Kolodgie F, Ravandi A,
Leibundgut G, Hu PP, Prasad A, Mahmud E, Dennis E, Curtiss LK,
Witztum JL, et al: Differential expression of oxidation-specific
epitopes and apolipoprotein(a) in progressing and ruptured human
coronary and carotid atherosclerotic lesions. J Lipid Res.
53:2773–2790. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tschoepe D, Schultheiss HP, Kolarov P,
Schwippert B, Dannehl K, Nieuwenhuis HK, Kehrel B, Strauer B and
Gries FA: Platelet membrane activation markers are predictive for
increased risk of acute ischemic events after PTCA. Circulation.
88:37–42. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Scholz W and Albus U:
Na+/h+ exchange and its inhibition in cardiac
ischemia and reperfusion. Basic Res Cardiol. 88:443–455. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Carreira RS, Monteiro P, Kowaltowski AJ,
Gonçalves LM and Providência LA: Nicorandil protects cardiac
mitochondria against permeability transition induced by
ischemia-reperfusion. J Bioenerg Biomembr. 40:95–102. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhu F, Zhong X, Zhou Y, Hou Z, Hu H, Liang
L, Chen J, Chen Q, Ji X and Shang D: Protective effects of
nicorandil against cerebral injury in a swine cardiac arrest model.
Exp Ther Med. 16:37–44. 2018.PubMed/NCBI
|
|
26
|
Lee JM, Kato D, Oi M, Toyofuku M,
Takashima H, Waseda K, Amano T, Kurita A, Ishihara H, Lim WH, et
al: Safety and efficacy of intracoronary nicorandil as hyperaemic
agent for invasive physiological assessment: A patient-level pooled
analysis. EuroIntervention. 12:e208–e215. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jang HJ, Koo BK, Lee HS, Park JB, Kim JH,
Seo MK, Yang HM, Park KW, Nam CW, Doh JH and Kim HS: Safety and
efficacy of a novel hyperaemic agent, intracoronary nicorandil, for
invasive physiological assessments in the cardiac catheterization
laboratory. Eur Heart J. 34:2055–2062. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kawai Y, Hisamatsu K, Matsubara H, Dan K,
Akagi S, Miyaji K, Munemasa M, Fujimoto Y, Kusano KF and Ohe T:
Intravenous administration of nicorandil immediately before
percutaneous coronary intervention can prevent slow coronary flow
phenomenon. Eur Heart J. 30:765–772. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ota S, Nishikawa H, Takeuchi M, Nakajima
K, Nakamura T, Okamoto S, Setsuda M, Makino K, Yamakado T and
Nakano T: Impact of nicorandil to prevent reperfusion injury in
patients with acute myocardial infarction: Sigmart multicenter
angioplasty revascularization trial (SMART). Circ J. 70:1099–1104.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Van KC and Banchereau J: Cd40-cd40 ligand.
J Leukocyte Biol. 67:2–17. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Henn V, Steinbach S, Büchner K, Presek P
and Kroczek RA: The inflammatory action of CD40 ligand (CD154)
expressed on activated human platelets is temporally limited by
coexpressed CD40. Blood. 98:1047–1054. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lee Y, Lee WH, Lee SC, Ahn KJ, Choi YH,
Park SW, Seo JD and Park JE: CD40L activation in circulating
platelets in patients with acute coronary syndrome. Cardiology.
92:11–16. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mach F, Schönbeck U, Bonnefoy JY, Pober JS
and Libby P: Activation of monocyte/macrophage functions related to
acute atheroma complication by ligation of CD40: Induction of
collagenase, stromelysin, and tissue factor. Circulation.
96:396–399. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cipollone F, Ferri C and Desideri G:
Preprocedural level of soluble CD40l is predictive of enhanced
inflammatory response and restenosis after coronary angioplasty.
Circulation. 13:54–55. 2004.
|
|
35
|
Rondina MT, Lappé JM, Carlquist JF,
Muhlestein JB, Kolek MJ, Horne BD, Pearson RR and Anderson JL:
Soluble CD40 ligand as a predictor of coronary artery disease and
long-term clinical outcomes in stable patients undergoing coronary
angiography. Cardiology. 109:196–201. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Dündar C, Kızılırmak F, Tigen K, Izgi A,
Karaahmet T, Pala S, Oduncu V, Erkol A, Bulut M and Kırma C:
Soluble CD40 ligand release in patients with stable coronary artery
disease during elective stent implantation: Effect of drug-eluting
stent over bare metal stent. Turk Kardiyol Dern Ars. 41:675–682.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Aströmolsson K, Hedström E, Hultén LM,
Wiklund O, Arheden H, Ohlin AK, Gottsäter A and Ohlin H:
Dissociation of the inflammatory reaction following PCI for acute
myocardial infarction. J Invasive Cardiol. 19:452–456.
2007.PubMed/NCBI
|
|
38
|
Gaspardone A, Crea F, Versaci F, Tomai F,
Pellegrino A, Chiariello L and Gioffrè PA: Predictive value of
C-reactive protein after successful coronary-artery stenting in
patients with stable angina. Am J Cardiol. 82:515–518. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Bayata S, Arıkan E, Yeşil M, Postacı N,
Taş A and Köseoğlu M: An important role for VCAM-1, but not for
ICAM-1 in restenosis following coronary stent implantation. Anadolu
Kardiyol Der. 10:405–409. 2010. View Article : Google Scholar
|
|
40
|
Wexberg P, Jordanova N, Strehblow C, Syeda
B, Meyer B, Charvat S, Zorn G, Scheinig D, Wojta J, Huber K, et al:
Time course of prothrombotic and proinflammatory substance release
after intracoronary stent implantation. Thromb Haemost. 99:739–748.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Tullio F, Angotti C, Perrelli MG, Penna C
and Pagliaro P: Redox balance and cardioprotection. Basic Res
Cardiol. 108:3922013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ekeløf S, Jensen SE, Rosenberg J and
Gögenur I: Reduced oxidative stress in STEMI patients treated by
primary percutaneous coronary intervention and with antioxidant
therapy: A systematic review. Cardiovasc Drug Ther. 28:173–181.
2014. View Article : Google Scholar
|
|
43
|
Demircan S, Yazici M, Diraman E, Demircan
G, Kilicaslan F, Durna K, Acar Z and Eren Z: The effect of
glucose-insulin-potassium treatment on myocardial oxidative stress
in patients with acute coronary syndromes undergoing percutaneous
coronary intervention. Coron Artery Dis. 19:99–104. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Li W, Wu N, Shu W, Jia D and Jia P:
Pharmacological preconditioning and postconditioning with
nicorandil attenuates ischemia/reperfusion-induced myocardial
necrosis and apoptosis in hypercholesterolemic rats. Exp Ther Med.
10:2197–2205. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Wang H, Zuo X, Wang Q, Yu Y, Xie L, Wang
H, Wu H and Xie W: Nicorandil inhibits hypoxia-induced apoptosis in
human pulmonary artery endothelial cells through activation of
mitoKATP and regulation of eNOS and the NF-κB pathway. Int J Mol
Med. 32:187–194. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Han Y: Chinese expert consensus on
clinical application of ticagrelor. Clin J Med Offic. 44:444–453.
2016.
|