Introduction
Stroke is the second most common cause of death in
the world, accounting for 11.8% of all the reasons of deaths
(1). Cerebral infarction and CH are
two common cerebrovascular diseases, which usually lead to severe
disability and even death (2–5).
Although some neurological scales such as the National Institutes
of Health Stroke Scale (NIHSS) and the Modified Rankin Scale (MRS)
have the ability of predicting the prognosis of stroke patients,
the prognosis of patients with apraxia, aphasia or disorientation
is difficult to evaluate with scales (6).
According to relevant studies, cerebral infarction
will bring harmful incidents such as oxidative stress, neuronal
excitatory toxicity, blood-brain barrier dysfunction, microvascular
injury, and ischemic inflammation, resulting in irreversible damage
to brain tissue (7,8). In the early stage of CH, the toxicity
of plasma extravasation components including blood-derived
coagulation factors, complement, immunoglobulins, and other
bioactive molecules is considered to be one of the causes of
CH-induced tissue damage, and during CH, hematoma components are
the trigger of inflammatory response that can aggravate hemorrhagic
brain injury (9,10). Therefore, it is essential to actively
search for some specific serum markers such as peripheral
biomarkers of related inflammation and oxidative stress markers to
analyze the occurrence and prognosis of CH and cerebral
infarction.
However, there are few studies on the changes of
complement and oxidative stress parameters in patients with acute
cerebral infarction (ACI) or cerebral hemorrhage (CH) and their
clinical significance. Therefore, this study tested complement and
oxidative stress parameters in the serum of such patients and
analyzed their clinical significance, so as to provide certain
clinical guidance for the two diseases.
Patients and methods
General data
A total of 122 patients with ACI or CH admitted to
the People's Hospital of Zhangqiu Area (Jinan, China) from August
2018 to September 2019 were collected, among which 59 ACI patients
were assigned into a cerebral infarction group (CIG) and other 63
CH patients were assigned into a cerebral hemorrhage group (CHG).
Moreover, 53 healthy people in physical examination during the same
period were enrolled as a control group (CG), and the CG consisted
of people aged between 24 and 69 years, with an average age of
45.23±15.54 years.
Inclusion and exclusion criteria
The inclusion criteria of the CIG and the CHG were
as follows: Patients confirmed with cerebral infarction or CH based
on CT and magnetic resonance imaging (MRI), patients admitted to
the hospital within 24 h after the onset of the disease, patients
without shock or surgical indicators, patients who had not recently
taken any immune preparations or anti-inflammatory drugs. The
inclusion criterion of the CG was as follows: Patients judged as
healthy people based on their physical examination results. The
exclusion criteria were as follows: Patients with cardiopulmonary
insufficiency, hepatic or kidney function obstacle, or a malignant
tumor, patients comorbid with infection, and patients with
traumatic CH, or subarachnoid hemorrhage. The study was approved by
the Ethics Committee of the People's Hospital of Zhangqiu Area and
all patients and their families signed informed consent forms.
Treatment
Both the CIG and the CHG were comprehensively
treated with edaravone, Xueshuantong, brain protein hydrolysates,
aspirin and statin-related drugs.
Methods
The levels of complement C3 (C3), complement C4
(C4), superoxide dismutase (SOD), and total antioxidant capacity
(TAC) in the serum of the patients were determined, and the levels
in the patients with different nerve function deficits were also
determined. Receiver operating characteristic (ROC) curves were
employed to analyze the predictive value of C3, C4, SOD and TAG in
ACI and CH, and logistic regression was used to analyze the risk
factors of stroke.
Determination methods
Determination of serum C3, C4, SOD and
TAC levels
Fasting venous blood was sampled from the patients
on the morning of the third day after admission, and determined
using the immune scatter turbidity. The serum C3 and C4 levels were
determined using a ADVIA2400 automatic biochemistry analyzer and
corresponding kit, and the serum SOD and TAC levels were determined
using colorimetry with a SOD detection kit from Dojindo, a total
antioxidant capacity (T-AOC) determination kit from Nanjing
Jiancheng Bioengineering Institute, and a ADVIA2400 automatic
biochemistry analyzer.
Determination of serum C3, C4, SOD and
TAC levels in patients with different nerve function deficits
Patients in the CIG and the CHG were divided into a
NIHSS <4 group and a NIHSS ≥4 group according to their nerve
function deficits based on NIHSS (11). NIHSS indicates mild disease with a
score <4 points, moderate disease with a score between 4–15
points, and severe disease with a score >15 points.
Statistical analysis
SPSS 19.0 (Asia Analytics Formerly SPSS China) was
used for statistical analysis. Measurement data were expressed as
mean ± SD, and comparison was performed using the Students t-test,
while enumeration data were expressed by rate, and comparison was
performed using the χ2 test. Comparison among multiple
groups was carried out by the Analysis of variance. ROC curves were
adopted to analyze the predicative value of C3, C4, SOD and TAC in
stroke, and Logistic regression to analyze risk factors of
stroke.
Results
General clinical data
There was no significant difference in sex, age,
body mass index (BMI), smoking, drinking, and place of residence
among the three groups (all P>0.05), while there were
differences in hyperlipidemia and hypertension among them (both
P<0.05) (Table I).
 | Table I.Primer sequences. |
Table I.
Primer sequences.
|
| Upstream
sequence | Downstream
sequence |
|---|
| U6 |
5′-TCTCTGCTCCTCGTTCGA-3′ |
5′-GCGCCCATACGACCAAATC-3′ |
| miR-122a |
5′-CAAGCGTTGGAGTGTGACA-3′ |
5′-CGTCCTACCATTCTCCAGC-3′ |
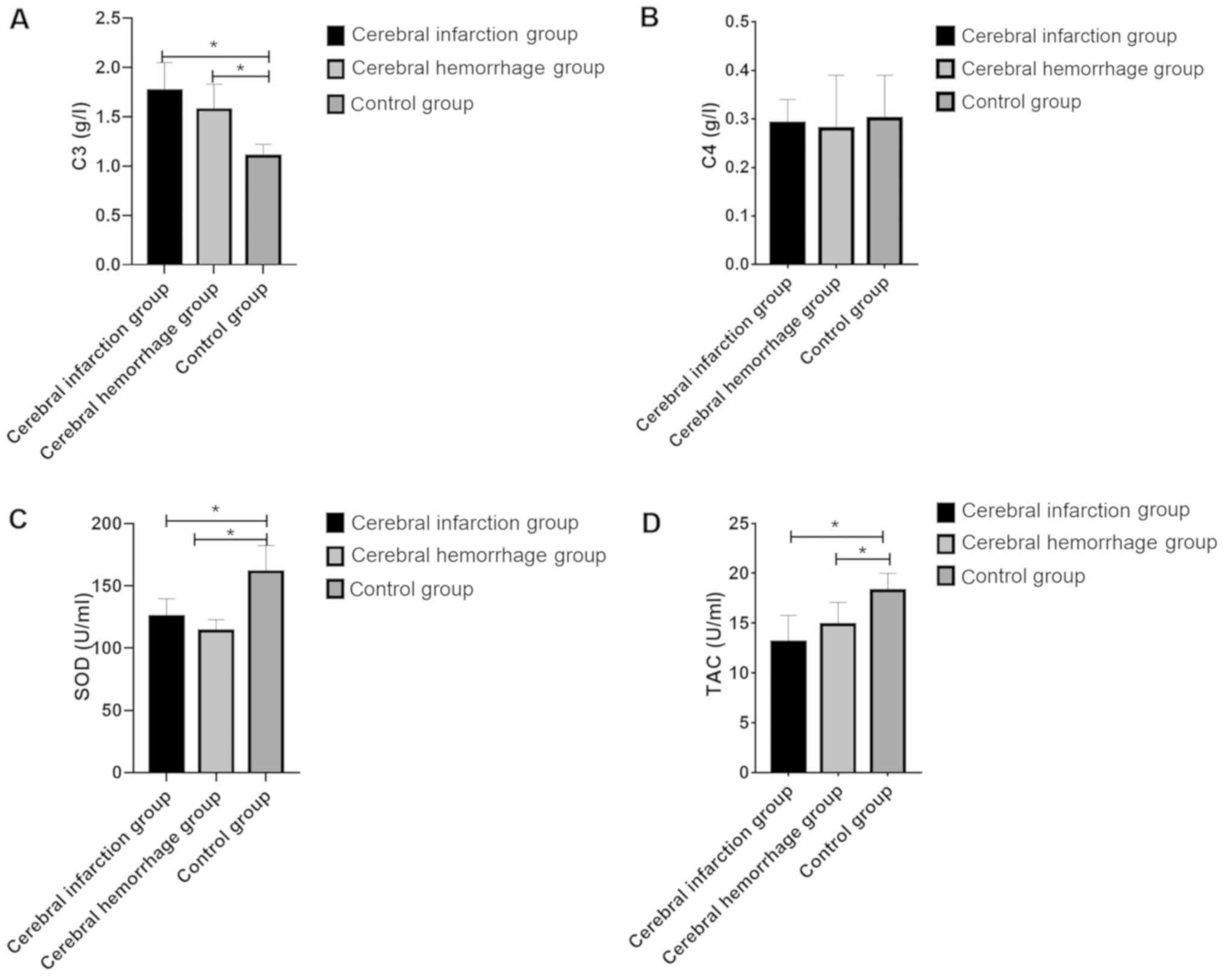
Determination of serum C3, C4, SOD and
TAC levels
The C3, C4, SOD and TAC levels in the CIG were
1.76±0.2 g/l, 0.29±0.05 g/l, 125.35±14.23 U/ml and 13.07±2.69 U/ml,
respectively; those of the CHG were 1.57±0.26 g/l, 0.28±0.1 g/l,
113.62±9.14 U/ml and 14.83±2.25 U/ml, respectively, and those of
the CG were 1.10±0.12 g/l, 0.30±0.09 g/l, 161.20±21.12 U/ml and
18.24±1.75 U/ml, respectively. It was apparent that the CIG and the
CHG showed significantly higher C3 level and significantly lower
C4, SOD and TAC levels than the CG (all P<0.05). It was also
shown that there were significant differences in C3, SOD and TAC
levels among the three groups (all P<0.05), but no significant
difference among them in C4 level (P>0.05), and there was no
significant difference between the CIG and the CHG in C3, C4, SOD
and HCY levels (all P>0.05) (Fig.
1).
Determination of serum C3, SOD and TAC
levels in the patients with different nerve function deficits
According to the NIHSS, 71 patients were assigned
into the NIHSS <4 group, and 51 patients were assigned into the
NIHSS ≥4 group. Both groups showed higher hs-C3 level, and lower
SOD and TAC levels than the CG, and the NIHSS <4 group showed
lower C3, SOD and TAC levels than the NIHSS ≥4 group (all
P<0.05) (Table II).
| Table II.Clinical basic data [n (%)]. |
Table II.
Clinical basic data [n (%)].
|
| Research group
(32) | Control group
(30) | χ2 or t
value | P-value |
|---|
| Age (years) | 50.8±10.6 | 51.2±10.3 | 0.151 | 0.881 |
| Sex |
|
| 0.209 | 0.647 |
| Male | 21 (65.63) | 18 (60.00) |
|
|
|
Female | 11 (34.38) | 12 (40.00) |
|
|
| BMI
(kg/m2) | 22.26±0.37 | 22.21±0.25 | 0.618 | 0.538 |
| Marital status |
|
| 0.242 | 0.623 |
|
Married | 29 (90.63) | 26 (86.67) |
|
|
|
Unmarried | 3 (9.38) | 4 (13.33) |
|
|
| Ethnicity |
|
| 0.011 | 0.915 |
| Han | 22 (68.75) | 21 (70.00) |
|
|
| Ethnic
minorities | 10 (31.25) | 9 (30.00) |
|
|
| Place of
residence |
|
| 0.501 | 0.479 |
| Cities
and towns | 18 (56.25) | 19 (63.33) |
|
|
|
Countryside | 14 (43.75) | 11 (36.67) |
|
|
| History of
smoking |
|
| 29.370 | 0.001 |
| Yes | 30 (93.75) | 8 (26.67) |
|
|
| No | 2 (6.25) | 22 (73.33) |
|
|
| History of
drinking |
|
| 25.930 | 0.001 |
| Yes | 4 (12.50) | 23 (76.67) |
|
|
| No | 28 (87.50) | 7 (23.33) |
|
|
| Exercise habits |
|
| 0.047 | 0.829 |
| Yes | 13 (40.63) | 13 (43.33) |
|
|
| No | 19 (59.38) | 17 (56.67) |
|
|
The predictive value of C3, C4, SOD
and TAC for stroke
The area-under-the-curve (AUC), critical value,
sensitivity, and specificity of C3 in predicting stroke were 0.687,
36.48, 63.49 and 71.19, respectively; those of C4 were 0.540,
23.49, 31.75 and 89.83, respectively; those of SOD were 0.750,
41.65, 85.71 and 54.24, and those of TAC were 0.714, 38.36, 82.54
and 54.24, respectively (Table III
and Fig. 2).
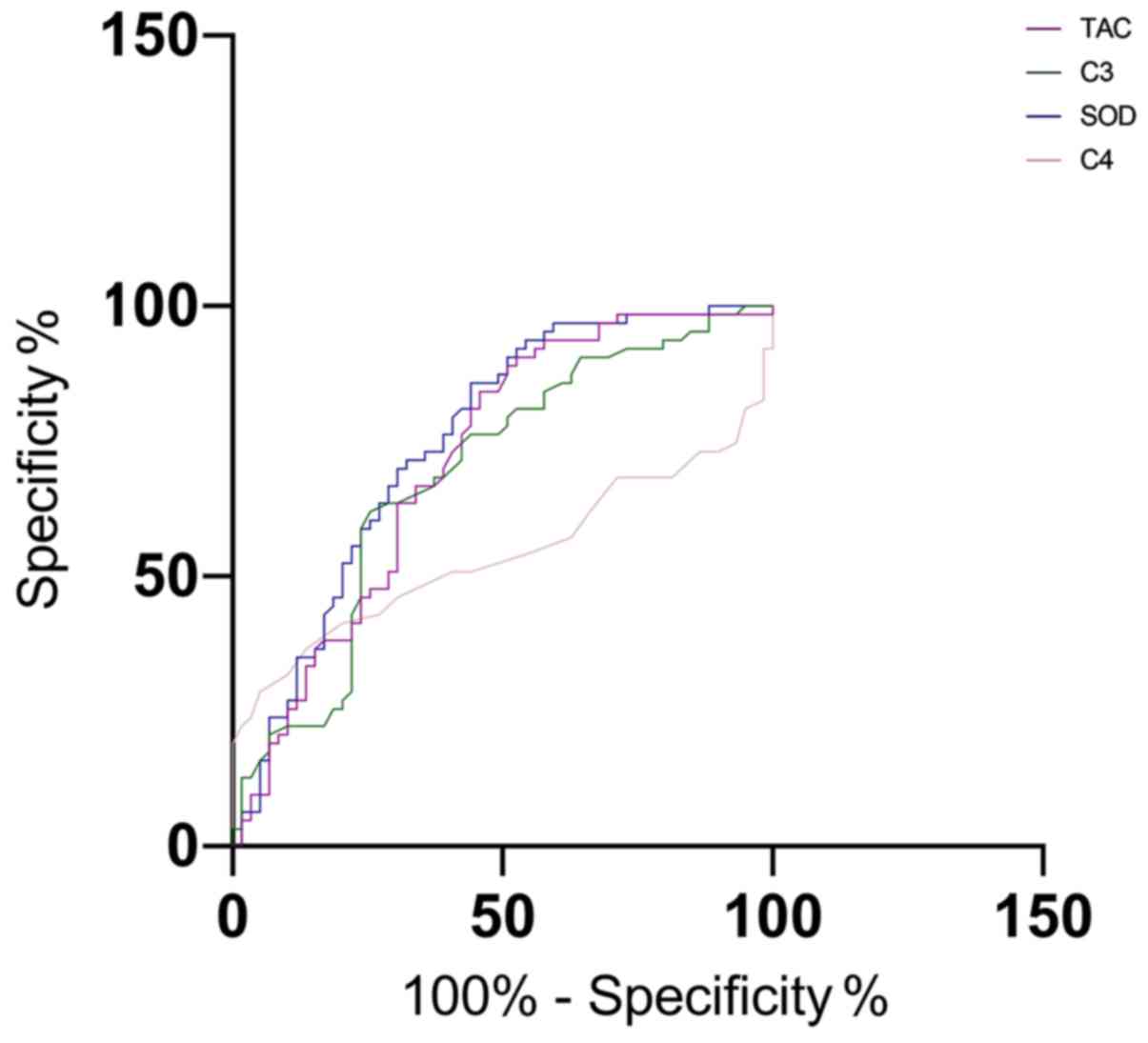 | Figure 2.The predictive value of C3, C4, SOD
and TAC for stroke. The AUC of C3, C4, SOD and TAC for predicting
stroke were 0.687, 0.540, 0.750 and 0.714, respectively. SOD,
superoxide dismutase; TAC, total antioxidant capacity; AUC,
area-under-the-curve. |
| Table III.ROC diagnosis. |
Table III.
ROC diagnosis.
|
| miR-122a |
|---|
| AUC | 0.770 |
| Std. error | 0.057 |
| 95% CI | 0.659–0.881 |
| P-value | 0.001 |
| Cut-off | 4.105 |
| Sensitivity
(%) | 82.22 |
| Specificity
(%) | 68.75 |
Univariate analysis
The patients were divided into a stroke group
(n=122) and a healthy group (n=53) according the occurrence of
stroke. Their clinical data were collected and analyzed through
univariate analysis. The two groups had no differences in sex, age,
BMI, smoking, drinking, place of residence, COPD or C4 (all
P>0.05). There were differences in hyperlipidemia, hypertension,
C3, SOD and TAC (all P<0.05) (Table
IV).
| Table IV.Univariate analysis. |
Table IV.
Univariate analysis.
|
| Stroke group
(n=122) | Healthy group
(n=53) | χ2
value | P-value |
|---|
| Sex [n (%)] |
|
| 0.073 | 0.788 |
|
Male | 71 (58.20) | 32 (60.38) |
|
|
|
Female | 51 (41.80) | 21 (39.62) |
|
|
| Age (years) |
|
| 0.138 | 0.710 |
|
<40 | 47 (38.52) | 22 (41.51) |
|
|
|
≥40 | 75 (61.48) | 31 (58.49) |
|
|
| BMI
(kg/m2) |
|
| 0.251 | 0.616 |
|
≥25 | 39 (31.97) | 19 (35.85) |
|
|
|
<25 | 83 (68.03) | 34 (64.15) |
|
|
| Smoking [n
(%)] |
|
| <0.001 | 0.978 |
|
Yes | 78 (63.93) | 34 (64.15) |
|
|
| No | 44 (36.07) | 19 (35.85) |
|
|
| Drinking [n
(%)] |
|
| 0.142 | 0.707 |
|
Yes | 84 (68.85) | 38 (71.70) |
|
|
| No | 38 (31.15) | 15 (28.30) |
|
|
| Hyperlipidemia [n
(%)] |
|
| 10.790 | 0.001 |
|
Yes | 87 (71.31) | 24 (45.28) |
|
|
| No | 35 (28.69) | 29 (54.72) |
|
|
| Hypertension [n
(%)] |
|
| 12.690 | <0.001 |
|
Yes | 95 (77.87) | 27 (50.94) |
|
|
| No | 27 (22.13) | 26 (49.06) |
|
|
| Place of residence
[n (%)] |
|
| 0.081 | 0.776 |
| Urban
area | 57 (46.72) | 26 (49.06) |
|
|
| Rural
area | 65 (53.28) | 27 (50.94) |
|
|
| COPD [n (%)] |
|
| 0.011 | 0.916 |
|
Yes | 54 (44.26) | 23 (43.40) |
|
|
| No | 68 (55.74) | 30 (56.60) |
|
|
| C3 (g/l) | 1.63±0.27 | 1.10±0.12 | 13.700 | <0.001 |
| C4 (g/l) | 0.28±0.15 | 0.30±0.09 | 0.902 | 0.368 |
| SOD (U/ml) | 119.22±12.42 | 161.20±21.12 | 16.400 | <0.001 |
| TAC (U/ml) | 14.17±2.48 | 18.24±1.75 | 10.830 | <0.001 |
Multivariate analysis of stroke in the
patients
We performed assignment to indexes with differences
in univariate analysis (Table V) and
performed logistic regression analysis. The results revealed that
hypertension and hyperlipidemia were independent risk factors of
stroke (Table VI).
| Table V.Valuation. |
Table V.
Valuation.
| Dependent
variable | Assignment |
|---|
| Hyperlipidemia | Yes=0, No=1 |
| Hypertension | Yes=0, No=1 |
| C3 | Raw data of those
belonging to continuous variable were used for analysis. |
| SOD | Raw data of those
belonging to continuous variable were used for analysis. |
| TAC | Raw data of those
belonging to continuous variable were used for analysis. |
| Table VI.Logistic multivariate analysis of
stroke. |
Table VI.
Logistic multivariate analysis of
stroke.
|
|
|
|
|
|
| 95% CI of Exp
(B) |
|---|
|
|
|
|
|
|
|
|
|---|
|
| B | SE | Wals | Sig. | Exp (B) | Lower limit | Upper limit |
|---|
| Hyperlipidemia | −0.045 | 0.343 | 0.017 | 0.006 | 0.956 | 0.489 | 1.872 |
| Hypertension | −0.005 | 0.359 | 0 | 0.014 | 0.995 | 0.493 | 2.01 |
| C3 | −1.147 | 0.428 | 5.575 | 0.723 | 0.409 | 0.117 | 0.819 |
| SOD | −1.114 | 0.446 | 5.876 | 0.267 | 0.310 | 0.120 | 0.799 |
| TAC | −1.157 | 0.489 | 5.387 | 0.457 | 0.315 | 0.118 | 0.835 |
Discussion
ACI and CH are common diseases that endanger life
and health of the middle-aged and the elderly. Vascular
atherosclerosis is a common reason, and it is an inflammatory
process of plaque formation, development and deposition (12). Cerebral infarction indicates the
injury degree of microvascular endothelial cells and brain
parenchyma cells due to ischemia, which is closely related to
oxygen free radicals. The main reason for the aggravation of
cerebral ischemia-induced brain injury is the abnormal increase of
oxygen free radicals, and the enhancement of oxygen free radical
reactions is an important reason for cerebral edema secondary to CH
(13). Stroke treatment is currently
limited by lack of accurate and reliable blood biomarkers, and its
identification will be helpful for early diagnosis and risk
prediction (14).
C3 and C4, as key factors in the complement system,
play an important role in various inflammation-related diseases
(15,16). In this study, the C3 level in the CIG
and the CHG was higher than that in the CG, suggesting that C3
level would increase in ACI and CH, and may be used as a routine
serum marker to evaluate the two diseases. In contrast, the C4
level in the former two groups was lower than that in the latter
group, which may be due to the decrease of consumption caused by
the stress state of the body at the initial stage of the disease. A
study by Anrather and Iadecola (17)
pointed out that complement system was a humoral branch of natural
immunity, which was always related to the pathobiology of stroke,
and its activation was linked to the adverse outcomes of stroke.
The study also indicated that C3a receptor antagonists could
alleviate ischemic brain injury and improve brain function. It was
consistent with our experimental results. Based on these results,
we speculated that the detection of relevant complement levels in
stroke diseases could play a certain clinical guiding role in the
clinical diagnosis and prognosis of the diseases.
SOD and TAC are commonly used oxidative stress
parameters to eliminate excess oxygen free radicals and avoid cell
damage (18,19). In this study, SOD and TAC levels in
the CIG and the CHG were lower than those in the CG, indicating
that SOD and TAC levels were related to ACI and CH. Relevant
studies have pointed out that oxidative stress is one of the main
pathophysiological mechanisms of inflammation in the central
nervous system and neurodegenerative diseases, and was related to
stroke diseases (20,21). A study by Milanlioglu et al
(22) concluded that patients with
acute ischemic stroke showed enhanced oxidative stress reaction,
and weakened antioxidant enzyme activity, suggesting that imbalance
of oxidant/antioxidant status may be a part of the pathogenesis of
acute ischemic stroke. It further proves that the detection of SOD
level is effective in evaluating ACI and CH to a certain
degree.
This study additionally employed NIHSS to score the
neurological function injury of stroke patients, and determined
their serum hs-C3, SOD and TAC levels, finding that patients with a
more severe neurological function injury showed a higher C3 level,
and lower SOD and TAC levels. A study by Zhang et al
(23) reported that the high
sensitivity C-reactive protein (hs-CRP) of the NIHSS >5 group
was dramatically higher than that of the NIHSS ≤5 group, and hs-CRP
has been proved to be related to stroke by many studies (24). Therefore, we speculated that C3, SOD
and TAC levels were related to the severity of ACI and CH, and they
were expected to be biomarkers of evaluating prognosis. We also
studied the predictive value of the four markers of stroke in this
study, finding that SOD had a relatively good predictive value
among the four markers, but further exploration is needed in this
direction. In this study, the Logistic regression analysis revealed
that hypertension and hyperlipidemia were independent risk factors
of stroke. Moreover, studies by Li et al (25) and Hsieh and Chiou (26) also reported that hypertension and
hyperlipidemia were risk factors of stroke. Therefore, it is a
reminder of the importance to actively control blood pressure and
blood lipid level in daily life to avoid ACI and CH to some
extent.
In conclusion, the serum complement and oxidative
stress parameters in patients with ACI or CH can be determined
through routine examination, and the nerve function deficit could
be assessed by determining the complement and oxidative stress
parameters in clinical practice.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MZ was responsible for the determination of serum
C3, C4, SOD and TAC levels, and wrote the manuscript. XW and JY
conceived and designed the study. SM and YW were responsible for
the collection and analysis of the experimental data. SL and SM
interpreted the data and drafted the manuscript. MZ and XW revised
the manuscript critically for important intellectual content. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
the People's Hospital of Zhangqiu Area (Jinan, China). Patients who
participated in this research had complete clinical data. Signed
informed consents were obtained from the patients and/or
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Feigin VL, Norrving B and Mensah GA:
Global burden of stroke. Circ Res. 120:439–448. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nogueira RG, Jadhav AP, Haussen DC, Bonafe
A, Budzik RF, Bhuva P, Yavagal DR, Ribo M, Cognard C, Hanel RA, et
al DAWN Trial Investigators, : Thrombectomy 6 to 24 hours after
stroke with a mismatch between deficit and infarct. N Engl J Med.
378:11–21. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Keep RF, Andjelkovic AV, Xiang J,
Stamatovic SM, Antonetti DA, Hua Y and Xi G: Brain endothelial cell
junctions after cerebral hemorrhage: Changes, mechanisms and
therapeutic targets. J Cereb Blood Flow Metab. 38:1255–1275. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
An SJ, Kim TJ and Yoon BW: Epidemiology,
risk factors, and clinical features of intracerebral hemorrhage: An
update. J Stroke. 19:3–10. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lai M, Wang D, Lin Z and Zhang Y: Small
molecule copper and its relative metabolites in serum of cerebral
ischemic stroke patients. J Stroke Cerebrovasc Dis. 25:214–219.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang W, Gao C, Yu C, Liu S, Hou D, Wang Y,
Wang C, Mo L and Wu J: No association between elevated total
homocysteine levels and functional outcome in elderly patients with
acute cerebral infarction. Front Aging Neurosci. 9:702017.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fanning JP, See Hoe LE, Passmore MR,
Barnett AG, Rolfe BE, Millar JE, Wesley AJ, Suen J and Fraser JF:
Differential immunological profiles herald magnetic resonance
imaging-defined perioperative cerebral infarction. Ther Adv Neurol
Disorder. Mar 13–2018.(Epub ahead of print). doi:
10.1177/1756286418759493. View Article : Google Scholar
|
|
8
|
Ono H, Nishijima Y, Ohta S, Sakamoto M,
Kinone K, Horikosi T, Tamaki M, Takeshita H, Futatuki T, Ohishi W,
et al: Hydrogen gas inhalation treatment in acute cerebral
infarction: A randomized controlled clinical study on safety and
neuroprotection. J Stroke Cerebrovasc Dis. 26:2587–2594. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Aronowski J and Zhao X: Molecular
pathophysiology of cerebral hemorrhage: Secondary brain injury.
Stroke. 42:1781–1786. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lattanzi S, Brigo F, Trinka E, Cagnetti C,
Di Napoli M and Silvestrini M: Neutrophil-to-lymphocyte ratio in
acute cerebral hemorrhage: A system review. Transl Stroke Res.
10:137–145. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bravata DM, Sico J, Vaz Fragoso CA, Miech
EJ, Matthias MS, Lampert R, Williams LS, Concato J, Ivan CS, Fleck
JD, et al: Diagnosing and treating sleep apnea in patients with
acute cerebrovascular disease. J Am Heart Assoc. 7:e0088412018.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Qu S and Guo J: Clinical significance and
difference of some biochemical indexes in patients with cerebral
infarction and cerebral hemorrhage. Xiandai Jianyan Yixue Zazhi.
33:114–117. 2018.(In Chinese).
|
|
13
|
Qi FM, Yuan X and Dong Y: Analysis of SOD
and HCY in acute cerebral infarction and acute cerebral hemorrhage
patients. Int J Lab Med. 10:1323–1324. 2015.(In Chinese).
|
|
14
|
Zhou J and Zhang J: Identification of
miRNA-21 and miRNA-24 in plasma as potential early stage markers of
acute cerebral infarction. Mol Med Rep. 10:971–976. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lin Z, Lin H, Li W, Huang Y and Dai H:
Complement component C3 promotes cerebral ischemia/reperfusion
injury mediated by TLR2/NFκB activation in diabetic mice. Neurochem
Res. 43:1599–1607. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Simats A, García-Berrocoso T and Montaner
J: Neuroinflammatory biomarkers: From stroke diagnosis and
prognosis to therapy. Biochim Biophys Acta. 1862:411–424. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Anrather J and Iadecola C: Inflammation
and stroke: An overview. Neurotherapeutics. 13:661–670. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ighodaro OM and Akinloye OA: First line
defence antioxidants-superoxide dismutase (SOD), catalase (CAT) and
glutathione peroxidase (GPX): Their fundamental role in the entire
antioxidant defence grid. Alexandria J Med. 54:287–293. 2018.
View Article : Google Scholar
|
|
19
|
Gonullu H, Aslan M, Karadas S, Kati C,
Duran L, Milanlioglu A, Aydin MN and Demir H: Serum prolidase
enzyme activity and oxidative stress levels in patients with acute
hemorrhagic stroke. Scand J Clin Lab Invest. 74:199–205. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Estevez AY, Stadler B and Erlichman JS:
In-vitro analysis of catalase-, oxidase-and SOD-mimetic activity of
commercially available and custom-synthesized cerium oxide
nanoparticles and assessment of neuroprotective effects in a
hippocampal brain slice model of ischemia. FASEB J. 31:693.5.
2017.
|
|
21
|
Llull L, Amaro S and Chamorro Á:
Administration of uric acid in the emergency treatment of acute
ischemic stroke. Curr Neurol Neurosci Rep. 16:42016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Milanlioglu A, Aslan M, Ozkol H, Çilingir
V, Nuri Aydın M and Karadas S: Serum antioxidant enzymes activities
and oxidative stress levels in patients with acute ischemic stroke:
Influence on neurological status and outcome. Wien Klin Wochenschr.
128:169–174. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang X, Huang WJ and Yu ZG: Relationship
between the hypersensitive C-reactive protein (hs-CRP) level and
the prognosis of acute brainstem infarction. Cell Biochem Biophys.
72:107–110. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lee JH, Kwon KY, Yoon SY, Kim HS and Lim
CS: Characteristics of platelet indices, neutrophil-to-lymphocyte
ratio and erythrocyte sedimentation rate compared with C reactive
protein in patients with cerebral infarction: A retrospective
analysis of comparing haematological parameters and C reactive
protein. BMJ Open. 4:e0062752014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Li W, Jin C, Vaidya A, Wu Y, Rexrode K,
Zheng X, Gurol ME, Ma C, Wu S and Gao X: Blood pressure
trajectories and the risk of intracerebral hemorrhage and cerebral
infarction: A prospective study. Hypertension. 70:508–514. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hsieh FI and Chiou HY: Stroke: Morbidity,
risk factors, and care in Taiwan. J Stroke. 16:59–64. 2014.
View Article : Google Scholar : PubMed/NCBI
|