Introduction
Crush syndrome (CS) is a systemic dysfunction
resulting from crush injuries and muscle compression. It is
characterized by an unpredictable clinical course and high
mortality due to cardiac arrest, shock, acute kidney injury (AKI),
and inflammatory disorders (1–3). Several
human and animal studies have included pathological analyses of CS.
In disaster management, massive fluid resuscitation is the
recommended initial management to prevent death due to cardiac
arrest and AKI. However, CS is known as rescue death because
approximately 20% of deaths occur shortly after extrication
(4), and at a hospital, these
patients are at an additional risk of systemic inflammatory
response syndrome and multi organ dysfunction syndrome secondary to
ischemia reperfusion due to the recommended therapy. We previously
reported that in a CS model involving rats (5), they died due to cardiac failure
following hyperkalemia; therefore, the outcomes in patients with CS
might be improved by improving the condition of the muscles
involved. Furthermore, improvements in the muscles are reported to
be due to the anti-inflammatory and anti-oxidative effects that
follow prevention of mitochondrial dysfunction (6).
Cryotherapy involves the cooling via ice packs or
similar methods of the skin overlying the respective muscles in
order to temporarily reduce muscle temperature, induce
vasoconstriction, and inhibit pain sensation. The potential
benefits of cryotherapy in the healing of the muscle following
various trauma-induced damages are controversial (7). In cryotherapy, icing technique is
general used in the emergency treatment of trauma in addition to
rehabilitation and surgery (8).
Furthermore, low tissue temperature is the most powerful
intervention towards limiting ischemia reperfusion injury (IRI),
which may subsequently prevent mitochondrial damage and, therefore,
reduce the severity of IRI (9).
Basic animal studies have proved the positive effect of icing
treatment over contusion injury (10) and crush injury in rats (11) in the early stages of attenuated
inflammation (during migration of inflammatory cells); however,
these effects were not sufficient to prevent effective muscle
regeneration at later stages. Furthermore, such studies did not
investigate and clarify the efficacy of icing intervention in
improving survival, electrolyte balance, vital signs, and
inflammation at early stages within 24 h.
In the present study involving CS model rats, we
hypothesized that treatment with icing will inhibit the influence
of potassium by vasoconstriction, exert anti-inflammatory effects
in the affected myocytes, and improve mitochondrial function.
Materials and methods
Animal model of CS
Male Wistar rats, weighing 250–300 g each, were
obtained from Japan SLC (Shizuoka, Japan) and housed in a room that
was maintained at a temperature of 23±3°C and relative humidity of
55±15% with 12:12-h light/dark cycle, with free access to food and
water. The animal experiments were carried out according to the
guidelines for animal use and were approved by the Life Science
Research Center of Josai University (approval no. H29030). In the
experimental periods, rats were anesthetized using sodium
pentobarbital (50 mg/kg body weight, intraperitoneal [i.p.]
administration). Anesthesia was maintained (confirmed by normal
rectal temperature, respiratory rate, and sleeping state) by the
i.p. administration of sodium pentobarbital (20 mg/kg body
weight/h). The body temperature was maintained uniformly throughout
the experiment using a heating pad. The CS rat model has been
previously described in detail (5).
Briefly, a rubber tourniquet was applied to both the hindlimbs of
each rat, which was wrapped five times around a 2.0 kg-metal
cylinder, and the end of the band was glued. After compression for
5 h, it was released by cutting the band and removing the rubber
tourniquet (i.e., reperfusion 0 h).
Experimental design
Experimental design-1 (survival rate): To examine
the survival period and the changes in the blood pressure and blood
gas parameters of CS rats, they were randomly divided into the
following six groups: i) Sham (n=10); ii) CS (n=10); iii) icing for
30 min over the entire hindlimb (CI-30)(n=10); iv) icing for 180
min over the entire hindlimb (CI-180)(n=10); v) local icing for 30
min over the hindlimb (CLI-30)(n=10); and (vi) local icing for 180
min over the hindlimb (CLI-180) (n=10). All the rats used in the
experiments were euthanized (confirmation by pupillary reflex to
light) by sodium pentobarbital overdose (100 mg/kg body weight,
intravenous administration) at 48 h after all measurements were
recorded.
Experimental design-2 (vital signs and blood gas
parameters): To examine the changes in the blood pressure and blood
gas parameters, the rats were randomly divided into the following
six groups (n=4 each):i) sham; ii) CS; iii) CI-30; iv) CI-180; v)
CL-30; and (vi) CLI-180 groups. Sequential sampling was performed
at 0.083, 0.5, 1, 3, 6, and 24 h after reperfusion.
Experimental design-3 (blood perfusion in the
crushed hindlimb): blood perfusion in the crushed hindlimb was
evaluated with the rats divided into the following four
experimental groups (n=6 each): i) sham; ii) CS; iii) CI-30; and
iv) CLI-30. Sequential measuring was performed at 0.083, 0.5, 1, 3,
6 and 24 h after reperfusion. All the rats used in the experiments
were euthanized (confirmation by pupillary reflex to light) by
sodium pentobarbital overdose (100 mg/kg body weight, intravenous
administration) at 24 h after all measurements were recorded.
Experimental design-4 (plasma potassium
(K+) and creatine phosphokinase (CPK) levels, and
anti-inflammatory and mitochondrial function parameters):
Biochemical analyses, serum cytokine levels, and mitochondrial
parameters were evaluated with the rats divided into the following
four experimental groups (n=6 each): i) Sham; ii) CS; iii) CLI-30;
and (iv) CLI-180. Samplings were performed at 1, 3, 6 and 24 h
after reperfusion. All the rats used in the experiments were
euthanized (confirmation by pupillary reflex to light) by sodium
pentobarbital overdose (100 mg/kg body weight, intravenous
administration) at each sampling time.
Vital signs, blood gas levels, and
biochemical parameters
The following vital signs were recorded using a
PowerLab data acquisition system (AD Instruments, Nagoya, Japan):
Mean blood pressure (MBP), heart rate (HR), and body temperature
(BT). One carotid artery was cannulated with a polyethylene
catheter (PE-50 tubing) and was connected to a pressure transducer.
Arterial blood samples from each group were obtained at 0.083, 0.5,
1, 3, 6, 12, and 24 h after reperfusion using the carotid artery
catheter (6). The arterial levels of
hematocrit (Hct), pH, base excess (BE), anion gap (AG), and lactate
were analyzed using i-STAT300F blood gas analyzer and CG4+ and EC8+
cartridges (FUSO Pharmaceutical Industries, Osaka, Japan). These
measurements were assess using experimental design-2.
Venous blood from the jugular vein was collected and
centrifuged to measure plasma K+ and CPK (the
measurements were carried out by SRL Inc., Tokyo, Japan). These
measurements were performed using experimental design-3.
Blood perfusion parameters
Blood perfusion (BPF) of muscles and blood vessels
was measured using PeriScan PIM3 (PERIMED, Stockholm, Sweden) in
experimental design-3. BPF was assessed under the following
conditions: distance to hindlimb: 10–15 cm; measurement area: 10×10
cm; environmental temperature: 23±5°C; and relative humidity:
50±5%.
Determination of cytokines, reactive oxygen species
(ROS) production, and mitochondrial function. The serum high
mobility group box 1 (HMGB1), interleukin-6 (IL-6), and
interleukin-10 (IL-10) were measured using HMGB1 ELISA Kit II
(Shino-Test Co., Tokyo, Japan), Rat IL-6 Quantikine®
ELISA kit (R&D Systems, Inc., MN, USA), and Rat IL-10
Quantikine® ELISA kit (R&D Systems, Inc., MN, USA)
according to the manufacturer's instructions. ROS production in the
injured gastrocnemius muscle was determined by measuring the
concentration of thiobarbituric acid reactive substances (TBARS)
(6). Myeloperoxidase (MPO) activity
was determined by the method previously described by Murata et
al (6). Isolation of
mitochondria from the injured muscles for evaluation of
mitochondrial function was performed using a mitochondrial
isolation kit (Thermo Fisher Scientific K.K., Kanagawa, Japan). In
mitochondrial permeability transition, mitochondrial membrane
potential (i.e., mitochondrial inner membrane function) was
evaluated using JC-1 Mitochondrial Membrane Potential Assay Kit
(Cayman Chemical Company, Ann Arbor, MI, USA). To evaluate the
mitochondrial outer membrane function, cytochrome c (cyt c) in the
cytoplasm of the crushed myocytes from the samples that did not
include mitochondria was quantified using Quantikine®
cyt c Immunoassay (R&D Systems, Inc. MN, USA). These
measurements were performed using experimental design-4 with
samples collected from the hindlimb muscles at 1, 3, 6 and 24 h
after reperfusion.
Statistical analyses
Results are expressed as means ± standard error of
mean (SEM). Differences between the groups were assessed by
analysis of variance with Tukey's honest significant difference
test or Tukey's test. Survival curves were generated using the
Kaplan-Meier method, and survival was compared by the log-rank
test. P<0.05 was considered to indicate a statistically
significant difference (Statcel 2, 2nd ed. OMS Publishing Inc.,
Saitama, Japan).
Results
The impact of icing on CS rat
viability
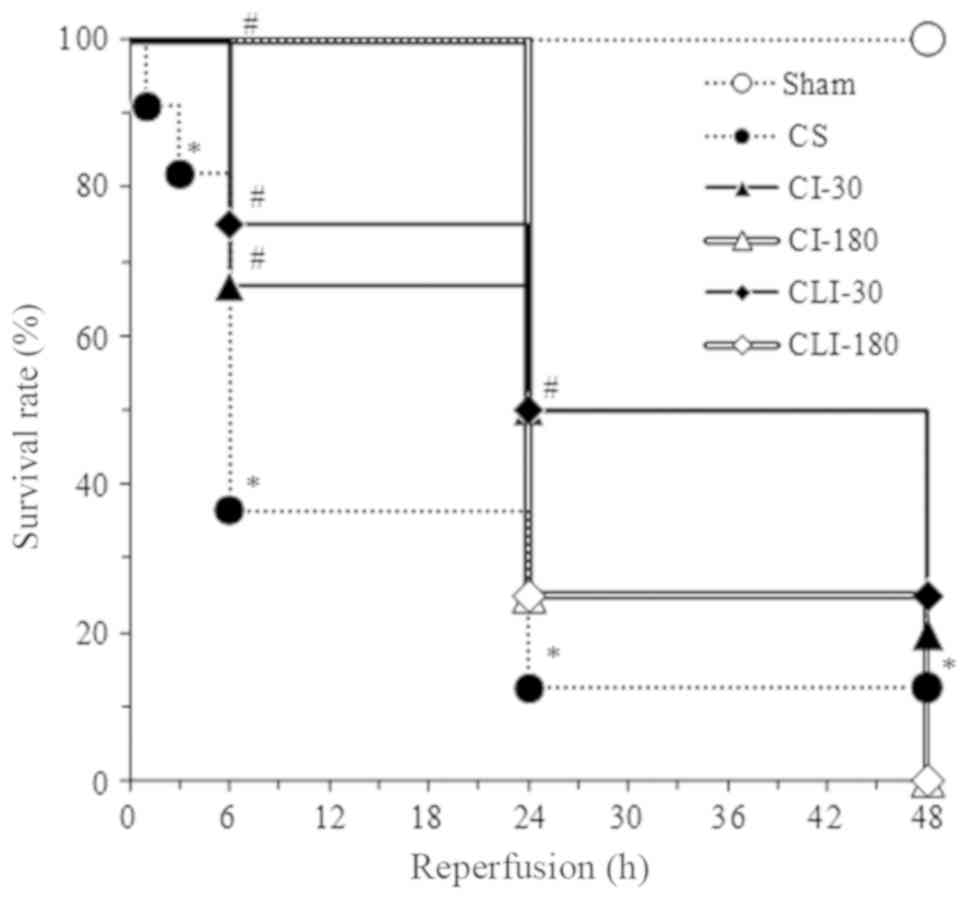
The survival rate is illustrated in Fig. 1. The survival rates of rats in the CS
group were 91%, 82%, 36%, 13%, and 13% at 1, 3, 6, 24, and 48 h
after reperfusion, respectively. Until 6 h after reperfusion, the
survival rates in CI-30, CI-180, CLI-30, and CLI-180 groups were
significantly higher than those in the CS group. Until 24 h after
reperfusion, the survival rates in the CI-30 and CLI-30 groups were
significantly higher than those in the CS group; however, 48 h
after reperfusion, the survival rates were not significantly
different. Furthermore, icing for 180 min (CI-180 and CLI-180
groups) demonstrated a tendency to extend the survival period when
compared with an icing period of 30 min (CI-30 and CLI-30 groups).
Furthermore, the survival rates following icing for 5 and 60 min
were similar to that following an icing period of 30 min (data not
shown).
Icing treatment improves vital
signs
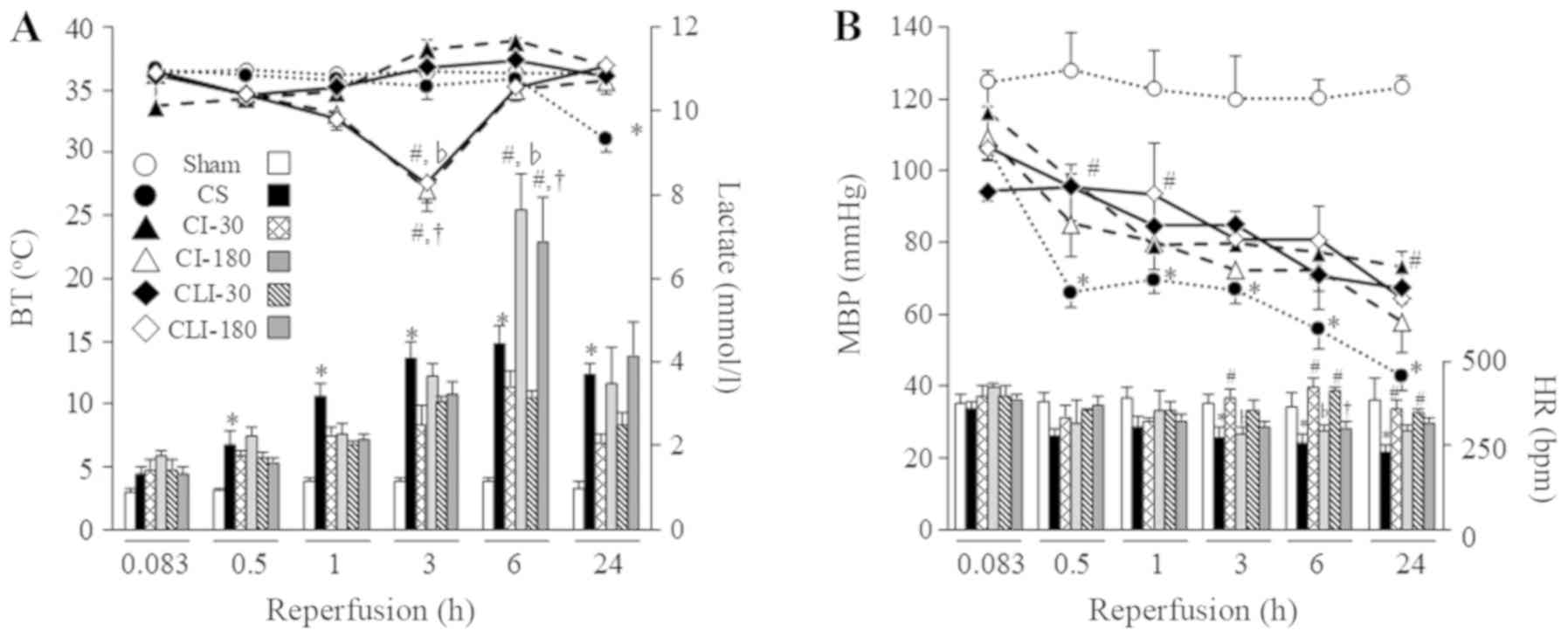
The relationship between BT and lactate levels, and
MBP and HR is illustrated in Fig. 2.
BT in the CS group was significantly lower than that in the sham
group at 24 h after reperfusion (31±1.4 vs. 36±0.5°C,
P<0.05), and the lactate level in the CS group was
significantly higher than that in the sham group throughout the
experimental period. In the CI-30 and CLI-30 groups, BT levels were
not significantly different when compared with that in the CS group
until 6 h after reperfusion, and similarly than the sham group
(37±0.2 and 36±0.4°C), and lactate levels were not showed
significantly changes compared that the CS group. In the CI-180 and
CLI-180 groups, the BT levels were significantly lower than that in
the CS groups at 3 h after reperfusion (27±0.9 and 28±2.3 vs.
35±0.5°C, P<0.05), and the lactate levels were
significantly higher (7.6±0.9 and 6.9±1.0 vs. 4.5±0.4 mmol/l,
P<0.05). In the CS group, MBP and HR levels were
significantly lower than that in the sham group until 24 h after
reperfusion (MBP, 42.8±3.8 vs. 123.2±3.1 mmHg; HR, 231±20 vs.
390±64 bpm; P<0.05 at 24 h after reperfusion). In the
CI-30, CLI-30, CI-180, and CLI-180 groups, MBP levels were
significantly higher than that in the CS group until 24 h after
reperfusion (CI-30, 57.9±8.9; CLI-30, 64.4±7.7; CI-180, 73.3±4.1;
CLI-180, 67.2±4.2 mmHg), and the HR levels were the CI-30 and
CLI-30 group has similarly than the sham group until 24 h after
reperfusion (CI-30, 362±25; CLI-30, 352±7 bpm) however that the
CI-180 and CLI-180 group were similar in the CS group at 6 h after
reperfusion (CI-180, 293±18; CLI-180, 322±9 bpm) and significantly
decreased compared to the CI-30 and CLI-30 groups.
Blood gas parameters and Hct levels of all the
experimental groups are presented in Table I. pH and BE levels in the CS groups
were significantly lower than that in the sham group, while the Hct
level was significantly higher than that in the sham group. In the
CI-30 and CLI-30 groups, pH level significantly increased compared
to the CS group at 6 and 24 h after reperfusion; however, the
CI-180 and CLI-180 groups had worse outcomes compared with the CS
group until 0.083 to 1 h after reperfusion.
 | Table I.Effects of CS and icing therapy on
blood gas parameters. |
Table I.
Effects of CS and icing therapy on
blood gas parameters.
|
| Reperfusion
(h) |
|---|
|
|
|
|---|
| Parameter | 0.083 | 0.5 | 0.1 | 3 | 6 | 24 |
|---|
| pH |
|
sham | 7.48±0.02 | 7.46±0.01 | 7.46±0.03 | 7.48±0.00 | 7.50±0.01 | 7.45±0.01 |
| CS | 7.44±0.02 | 7.51±0.03 | 7.43±0.02 |
7.38±0.02a |
7.31±0.02a |
7.22±0.05a |
|
CI-30 | 7.45±0.04 | 7.42±0.03 | 7.44±0.02 | 7.43±0.03 |
7.40±0.00b |
7.37±0.03b |
|
CI-180 | 7.42±0.01 |
7.31±0.06b |
7.33±0.03b | 7.31±0.03 | 7.29±0.03 | 7.26±0.03 |
|
CLI-30 | 7.42±0.03 | 7.38±0.01 | 7.38±0.02 | 7.38±0.03 |
7.40±0.04b |
7.37±0.03b |
|
CLI-180 |
7.38±0.01b |
7.37±0.02b |
7.35±0.02b | 7.30±0.03 | 7.27±0.03 | 7.30±0.04 |
| BE (mmol/l) |
|
sham | 2.3±0.6 | 2.3±1.0 | 2.8±0.9 | 3.0±1.1 | 2.5±0.3 | 2.8±1.0 |
| CS | 2.0±0.5 | 2.3±0.7 | 2.0±1.4 | 0.0±2.1 |
−5.0±0.7a |
−7.8±1.5a |
|
CI-30 | 0.5±0.7 | −2.3±1.0 | −3.3±1.7 | −5.0±2.0 | −7.5±1.4 | −6.3±1.2 |
|
CI-180 | 0.5±0.6 | −2.0±1.2 | −1.5±1.1 | −5.5±1.4 | −6.0±0.8 | −6.5±1.1 |
|
CLI-30 | 0.5±2.5 | 0.0±1.6 | 0.0±2.4 | −4.8±3.5 | −5.8±2.2 | −4.8±1.7 |
|
CLI-180 | −0.5±0.7 | −1.8±0.7 | −0.8±0.3 | −3.8±0.3 |
−10.0±0.9b | −9.5±0.3 |
| AG (mmol/l) |
|
sham | 15.3±1.5 | 13.0±1.6 | 14.0±0.8 | 13.0±1.7 | 13.7±1.5 | 15.0±1.2 |
| CS | 19.3±1.0 | 15.5±1.4 | 15.0±1.2 | 15.8±1.6 | 17.3±1.9 | 19.6±1.0 |
|
CI-30 | 16.0±2.3 | 18.8±1.3 | 18.5±1.5 | 18.5±1.1 | 19.0±0.7 | 19.5±0.7 |
|
CI-180 | 20.8±1.5 | 18.5±0.6 | 16.3±0.9 | 18.5±1.4 | 19.3±1.1 | 18.8±0.6 |
|
CLI-30 | 18.0±1.6 | 15.8±1.8 | 15.8±1.4 | 17.8±1.2 | 19.8±1.7 | 21.0±1.7 |
|
CLI-180 | 20.8±1.7 | 16.8±1.1 | 14.5±2.0 | 16.5±1.7 | 19.8±0.6 | 21.5±1.7 |
| Hct (%) |
|
sham | 45.0±1.2 | 46.8±1.3 | 47.3±1.7 | 46.5±1.4 | 46.3±1.3 | 46.0±1.7 |
| CS | 45.0±1.2 | 46.5±0.3 | 47.5±0.3 | 52.0±1.2 |
56.0±1.8a |
60.5±1.1a |
|
CI-30 | 46.5±1.7 | 45.5±1.5 | 45.8±2.2 | 49.5±1.5 | 52.3±2.2 | 51.8±0.3 |
|
CI-180 | 47.0±0.7 | 48.3±0.7 | 51.3±0.9 | 52.8±0.7 | 54.8±0.7 | 53.8±1.2 |
|
CLI-30 | 45.0±2.4 | 47.0±2.4 | 47.3±2.3 | 51.3±2.8 | 52.3±2.1 | 51.3±1.7 |
|
CLI-180 | 46.3±2.0 | 50.0±0.8 | 50.3±0.7 | 53.5±1.1 | 56.0±1.4 | 55.3±1.4 |
Icing treatment attenuated
hyperkalemia by controlling BPF
The survival rates, vital signs, and blood gas
parameters improved when the the icing period was over 30 min.
Further, an icing period of 180 min induces hypothermia; therefore,
we decided that the icing period should be 30 min.
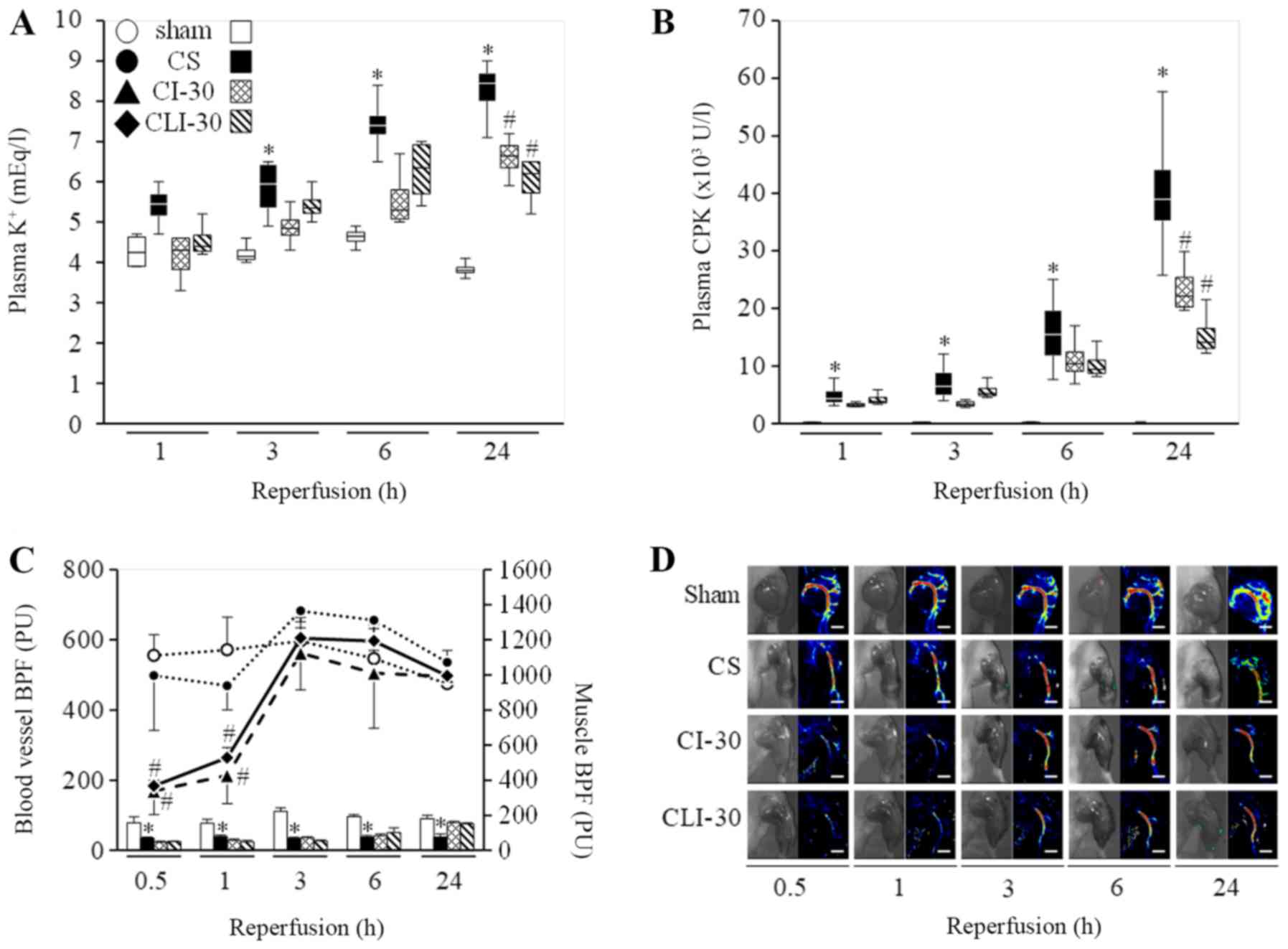
The plasma K+ and CPK levels and BPF of
the crushed limbs is presented in Fig.
3. CS group had significantly higher plasma K+ and
CPK levels than the sham group at all experimental periods, while
the same in the CI-30 and CLI-30 groups were significantly lower
than that in the CS group at 24 h after reperfusion. In the CS
group, BPF level within the blood vessels was not significantly
different from that in the sham group, and the muscle BPF level was
significantly lower than that in the sham group at all experimental
periods. In the CI-30 and CLI-30 groups, BPF within the blood
vessels was significantly lower than that in the CS group at 0.5
and 1 h after reperfusion, while the muscle BPF level was similar
to that in the CS group between 0.5–6 h after reperfusion.
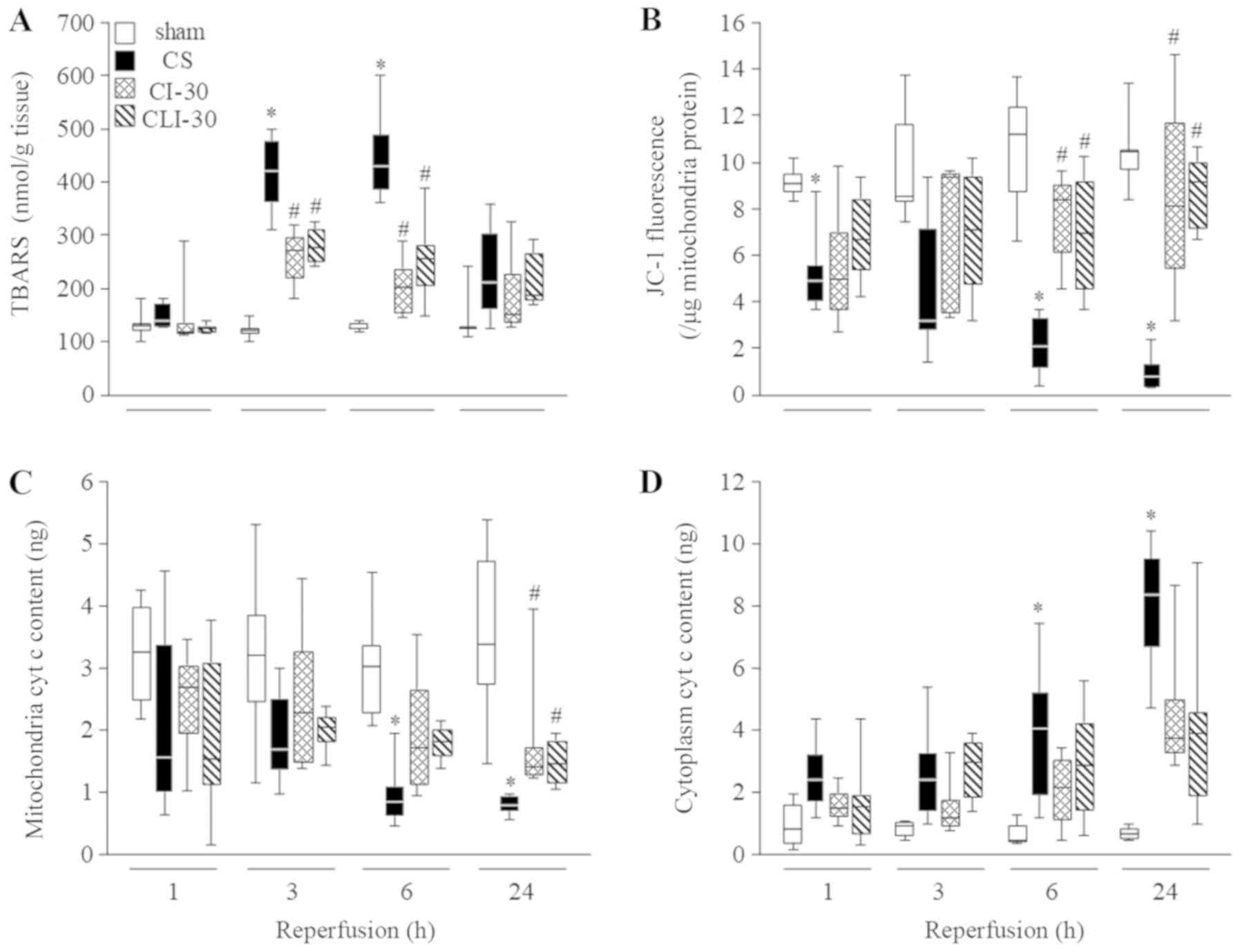
Icing treatment attenuated
inflammation through prevention of mitochondrial dysfunction
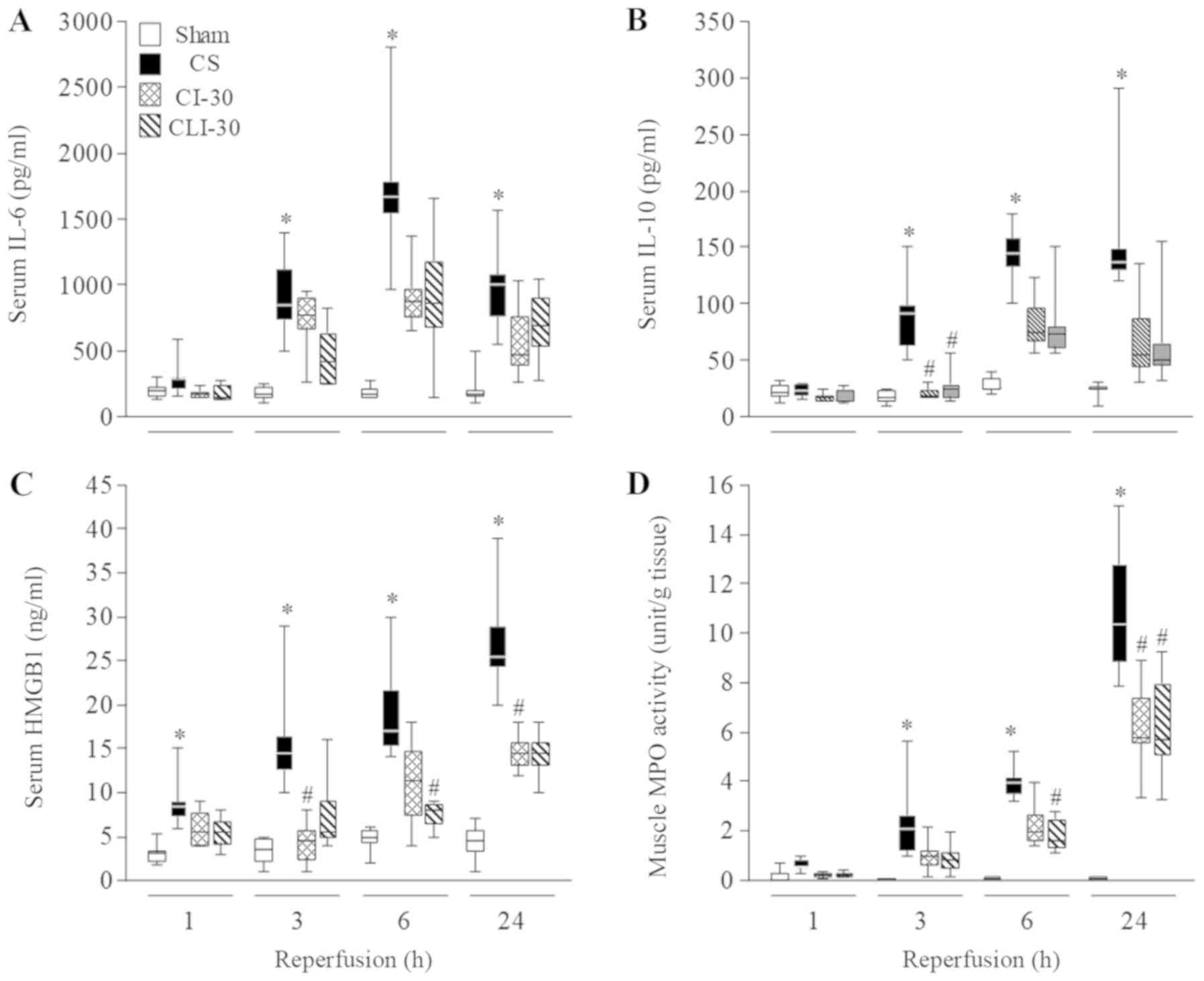
The serum cytokine levels, and TBARS (i.e., ROS
generation level) due to mitochondrial dysfunction is presented in
Figs. 4 and 5. The CS group had significantly higher
serum IL-6 and IL-10 levels than the sham group at 3, 6, and 24 h
after reperfusion, and showed maximum levels at 6 h after
reperfusion. Serum HMGB1 and MPO levels in the CS group were
significantly higher than that in the sham group at 3–24 h after
reperfusion. Their levels in the CI-30 and CLI-30 groups were
significantly lower than that in the CS group (Fig. 4). While evaluating the mitochondrial
function, TBARS level in the CS group was maximum at 6 h after
reperfusion and was significantly higher than that in the sham
group at 3 and 6 h after reperfusion. Furthermore, JC-1
fluorescence (mitochondrial membrane potential) and mitochondrial
cyt c content in the CS group was significantly lower than that in
the sham group at all experimental timepoints, and cytoplasm cyt c
content of the CS group was lower than that in the sham group. In
the CI-30 and CLI-30 groups, TBARS levels were significantly lower
than that in the CS group at 3 and 6 h after reperfusion, JC-1
fluorescence was significantly higher than that in the CS group at
6 and 24 h after reperfusion, and mitochondrial cytochrome C
contents were significantly increased and cytoplasm cytochrome C
contents tended to be decreased compared with those in the CS group
(Fig. 5).
Discussion
A variety of modalities are used to treat muscle
injuries including (7) cryotherapy,
massage therapy, and hyperbaric oxygen therapy; however, icing is
the mainstay treatment for several types of acute musculoskeletal
injuries (12,13).
We selected the icing method since icing periods of
both 30 and 180 min decrease the average temperature of the skin
(32-28°C) by 3–5°C (data not shown). In this study, BT
significantly decreased only with an icing period of 180 min.
Previous studies reported that ice application of 30 min over the
Achilles (14) and patellar
(15) tendons decreased the skin
temperature to approximately 17–20°C. Furthermore, Dewhurst et
al (16) reported that ice pack
application over the thigh decreases skin temperature by 6°C and
muscle temperature by 4°C. Similarly, in our study, the icing
procedure was able to be cool the injured muscle. Knight et
al (8), suggested that the
effects of local cooling were limited to local effects; however, it
appears to be not so according to this study. An icing period of 30
min did not decreased BT; however, an icing period of 180 min did
significantly decrease BT. This might be because of additional
factors such as increased lactate and decrease HR because the
gastrocnemius is a relatively large muscle in the rat.
Additionally, the vasoconstriction in the affected part induced by
icing would decrease the release of potassium into the systemic
circulation. We demonstrated that hyperkalemia can be improved from
blocking the blood flow to the crushed limbs (data not shown). In
the present study, we demonstrated that the blood flow to the
affected limb temporarily decreases with icing treatment (Fig. 3D), and that these changes had similar
effects on decreasing serum potassium in the experimental period
(Fig. 3A). In contrast, Nakayama
et al (17) reported that
warming of the hindlimbs to 40°C during compression resulted in a
much lower survival rate and significantly enhanced hyperkalemia,
leading to cardiac arrest. Therefore, lower BT and temperature of
the affected muscle are believed to be necessary in improving
hyperkalemia. However, icing treatment for 30 min significantly
increased the survival rate within 24 h from the injury; however,
that with icing treatment for 180 min did not vary significantly
despite a temporary decrease in serum potassium. The CS model rat
in our study died from cardiac insufficiency following rapidly
progressing (within an injured 3 h) hyperkalemia (5); nevertheless, the decreased survival
period following hypothermia by the icing treatment for 180 min
could not provide this reason. We believe that survival with CS
state may be affected by various factors, such as hypovolemic shock
and inflammation. Therefore, our findings suggest that icing
therapy for 30 min effectively prolonged the viability in
situations where the risk of hypothermia could be controlled,
although, cooling of the affected limb is a simple therapy in
difficult clinical situations with ongoing CS.
Interestingly, low tissue temperature can help in
resisting hypoxia because chemical reactions in vivo are
catalyzed by enzymes (18).
Furthermore, this anti-inflammation effect prevents leukocyte
migration and edema by reducing vascular permeability (19). Icing treatment is not considered to
be beneficial in the repair process of damaged tissue (8,20,21);
however, uncontrolled inflammation is also harmful for homeostasis.
We evaluated the overall balance between inflammatory and
anti-inflammatory factors by assessing the serum levels of
cytokines IL-6 and IL-10 (22),
which are markedly induced in CS rats. Additionally, we evaluated
the serum levels of HMGB1, which is lethally involved in
constitutive expression and vascular endothelial cell interactions
(23,24), and is a lethal inflammation mediator
(25). Extracellular release of
HMGB1 induces the expression of adhesion factors of intravascular
cells such as vascular cell adhesion molecule 1, intercellular
adhesion molecule 1, and E-selectin, and inflammatory reactions
involving production of cytokines due to the extravasation of
neutrophils and monocytes (23,26). As
demonstrated by the MPO activity level in the muscle tissue, icing
treatment suppresses both neutrophil infiltration and HMGB1
expression. The reduction in HMGB1, in turn, suppresses
inflammation as indicated by lowered levels of IL-6 and IL-10,
which can also be due to inhibition of cell rupture. However,
although IL-10 is an anti-inflammation cytokine, lowered levels of
it seemed to be secondary to no expression due to suppression of
inflammation. Additionally, icing treatment affects mitochondrial
function after a long period of time. One of the characteristics of
CS is that ROS production is enhanced in a relatively short time
along with decreased mitochondrial function (6). In this study, ROS production peaked 6 h
after the compression injury and was reduced by icing treatment. It
is believed that this result is because of normalization of
mitochondrial function and mitochondrial injury secondary to
decreased cell temperature, as demonstrated by maintenance of the
mitochondrial membrane potential (Fig.
5B) as well as cytoplasmic of cyt c (Figs. 5C and D). Therapeutic hypothermia may
also alleviate bursts of reactive oxygen species and calcium
overload and activate the cell survival signaling pathways
(26–30), which are believed to be involved in
permeability transition pore (PTP) regulation (31–33).
Furthermore, some reports have suggested that therapeutic
hypothermia limits calcium-induced mitochondrial dysfunction,
including opening of PTP (26,34,35).
In emergency situations, icing treatment following
crush injury temporarily prolonged the viability by suppressing
potassium elevation; however, this could not improve the overall
outcomes dramatically because CS involves simultaneous and rapid
worsening of multiple symptoms. Icing was suggested to be effective
in suppressing the inflammatory reactions; therefore, the
effectiveness of icing therapy can be enhanced by combining it with
other infusion therapies.
Acknowledgments
The authors thank Dr. Hiroyuki Uchida and Dr. Junta
Ito for advice, and Mr. Ryo Kawanishi and Ms. Chikako Murata for
technical assistance. These members were affiliated Laboratory of
Drug Safety Management or Division of Pathophysiology, Department
of Clinical Dietetics and Human Nutrition, Faculty of Pharmacy and
Pharmaceutical Science, Josai University.
Funding
The present study was supported by JSPS KAKENHI
(grant no. 16K20397).
Availability of data and material
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
IM led the project, and designed and performed most
of the experiments. MI and MK assisted with the survival and
biochemical marker analyses. JK, YI, and IK conceived the study,
participated in its design and coordination, and helped draft the
manuscript. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Life Science
Research Center of Josai University (approval no. H29030).
Patient consent for publication
Not applicable.
Competing interests
The all authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CS
|
crush syndrome
|
|
CI-30
|
icing for 30 min over the entire
hindlimb on CS rats
|
|
CI-180
|
icing for 180 min over the entire
hindlimb on CS rats
|
|
CLI-30
|
local icing for 30 min over the
affected area on CS rats
|
|
CLI-180
|
local icing for 180 min over the
affected area on CS rats
|
|
AKI
|
acute kidney injury
|
|
IRI
|
ischemia reperfusion injury
|
|
K+
|
plasma potassium
|
|
CPK
|
creatine phosphokinase
|
|
MBP
|
mean blood pressure
|
|
HR
|
heart rate
|
|
BT
|
body temperature
|
|
Hc
|
hematocrit
|
|
BE
|
base excess
|
|
AG
|
anion gap
|
|
BPF
|
Blood perfusion
|
|
ROD
|
reactive oxygen species
|
|
HMGB1
|
high mobility group box 1
|
|
IL-6
|
interleukin-6
|
|
IL-10
|
interleukin-10
|
|
TBARS
|
thiobarbituric acid reactive
substances
|
|
MPO
|
myeloperoxidase
|
|
cyt c
|
cytochrome c
|
|
SEM
|
standard error of mean
|
|
PTP
|
permeability transition pore
|
References
|
1
|
Smith J and Greaves I: Crush injury and
crush syndrome: A review. J Trauma. 54((5 Suppl)): S226–S230.
2003.PubMed/NCBI
|
|
2
|
Sever MS and Vanholder R; RDRTF of ISN
Work Group on Recommendations for the Management of Crush Victims
in Mass Disasters, : Recommendation for the management of crush
victims in mass disasters. Nephrol Dial Transplant. 27 (Suppl
1):i1–i67. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gonzalez D: Crush syndrome. Crit Care Med.
33((1 Suppl)): S34–S41. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ashkenazi I, Isakovich B, Kluger Y, Alfici
R, Kessel B and Better OS: Prehospital management of earthquake
casualties buried under rubble. Prehosp Disaster Med. 20:122–133.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Murata I, Ooi K, Sasaki H, Kimura S,
Ohtake K, Ueda H, Uchida H, Yasui N, Tsutsui Y, Yoshizawa N, et al:
Characterization of systemic and histologic injury after crush
syndrome and intervals of reperfusion in a small animal model. J
Trauma. 70:1453–1463. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Murata I, Abe Y, Yaginuma Y, Yodo K,
Kamakari Y, Miyazaki Y, Baba D, Shinoda Y, Iwasaki T, Takahashi K,
et al: Astragaloside-IV prevents acute kidney injury and
inflammation by normalizing muscular mitochondrial function
associated with a nitric oxide protective mechanism in crush
syndrome rats. Ann Intensive Care. 7:902017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tiidus PM: Alternative treatments for
muscle injury: Massage, cryotherapy, and hyperbaric oxygen. Curr
Rev Musculoskelet Med. 8:162–167. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Merrick MA, Rankin JM, Andres FA and
Hinman CL: A preliminary examination of cryotherapy and secondary
injury in skeletal muscle. Med Sci Sports Exerc. 31:1516–1521.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jahandiez V, Cour M, Bochaton T, Abrial M,
Loufouat J, Gharib A, Varennes A, Ovize M and Argaud L: Fast
therapeutic hypothermia prevents post-cardiac arrest syndrome
through cyclophilin D-mediated mitochondrial permeability
transition inhibition. Basic Res Cardiol. 112:352017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Singh DP, Barani Lonbani Z, Woodruff MA,
Parker TJ, Steck R and Peake JM: Effects of topical icing on
inflammation, angiogenesis, revascularization, and myofiber
regeneration in skeletal muscle following contusion injury. Front
Physiol. 8:932017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Takagi R, Fujita N, Arakawa T, Kawada S,
Ishii N and Miki A: Influence of icing on muscle regeneration after
crush injury to skeletal muscles in rats. J Appl Physiol (1985).
110:382–388. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Meeusen R and Lievens P: The use of
cryotherapy in sports injuries. Sports Med. 3:398–414. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Swenson C, Swärd L and Karlsson J:
Cryotherapy in sports medicine. Scand J Med Sci Sports. 6:193–200.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Alegre LM, Hasler M, Wenger S, Nachbauer W
and Csapo R: Does knee joint cooling change in vivo patellar tendon
mechanical properties? Eur J Appl Physiol. 116:1921–1929. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Warren TA, McCarty EC, Richardson AL,
Michener T and Spindler KP: Intra-articular knee temperature
changes: Ice versus cryotherapy device. Am J Sports Med.
32:441–445. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dewhurst S, Macaluso A, Gizzi L, Felici F,
Farina D and De Vito G: Effects of altered muscle temperature on
neuromuscular properties in young and older women. Eur J Appl
Physiol. 108:451–458. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nakayama T, Fujita M, Ishihara M, Ishihara
M, Ogata S, Yamamoto Y, Shimizu M, Maehara T, Kanatani Y and
Tachibana S: Improved survival rate by temperature control at
compression sites in rat model of crush syndrome. J Surg Res.
188:250–259. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Merrick MA: Secondary injury after
musculoskeletal trauma: A review and update. J Athl Train.
37:209–217. 2002.PubMed/NCBI
|
|
19
|
Deal DN, Tipton J, Rosencrance E, Curl WW
and Smith TL: Ice reduces edema. A study of microvascular
permeability in rats. J Bone Joint Surg Am. 84:1573–1578. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tidball JG and Wehling-Henricks M: Damage
and inflammation in muscular dystrophy: Potential implications and
relationships with autoimmune myositis. Autoimmune myositis. Curr
Opin Rheumatol. 17:707–713. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Barnett A: Using recovery modalities
between training sessions in elite athletes: Does it help? Sports
Med. 36:781–796. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Murata I, Ooi K, Shoji S, Motohashi Y, Kan
M, Ohtake K, Kimura S, Ueda H, Nakano G, Sonoda K, et al: Acute
lethal crush-injured rats can be successfully rescued by a single
injection of high-dose dexamethasone through a pathway involving
PI3K-Akt-eNOS signaling. J Trauma Acute Care Surg. 75:241–249.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Scaffidi P, Misteli T and Bianchi ME:
Release of chromatin protein HMGB1 by necrotic cells triggers
inflammation. Nature. 418:191–195. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lotze MT and Tracey KJ: High-mobility
group box 1 protein (HMGB1): Nuclear weapon in the immune arsenal.
Nat Rev Immunol. 5:331–342. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang H, Bloom O, Zhang M, Vishnubhakat JM,
Ombrellino M, Che J, Frazier A, Yang H, Ivanova S, Borovikova L, et
al: HMG-1 as a late mediator of endotoxin lethality in mice.
Science. 285:248–251. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Huang CH, Tsai MS, Chiang CY, Su YJ, Wang
TD, Chang WT, Chen HW and Chen WJ: Activation of mitochondrial
STAT-3 and reduced mitochondria damage during hypothermia treatment
for post-cardiac arrest myocardial dysfunction. Basic Res Cardiol.
110:592015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tissier R, Chenoune M, Pons S, Zini R,
Darbera L, Lidouren F, Ghaleh B, Berdeaux A and Morin D: Mild
hypothermia reduces per-ischemic reactive oxygen species production
and preserves mitochondrial respiratory complexes. Resuscitation.
84:249–255. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yang X, Liu Y, Yang XM, Hu F, Cui L,
Swingle MR, Honkanen RE, Soltani P, Tissier R, Cohen MV and Downey
JM: Cardioprotection by mild hypothermia during ischemia involves
preservation of ERK activity. Basic Res Cardiol. 106:421–430. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yenari MA and Han HS: Neuroprotective
mechanisms of hypothermia in brain ischemia. Nat Rev Neurosci.
13:267–278. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhao H, Shimohata T, Wang JQ, Sun G,
Schaal DW, Sapolsky RM and Steinberg GK: Akt contributes to
neuroprotection by hypothermia against cerebral ischemia in rats. J
Neurosci. 25:9794–9806. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Alam MR, Baetz D and Ovize M: Cyclophilin
D and myocardial ischemia-reperfusion injury: A fresh perspective.
J Mol Cell Cardiol. 78:80–89. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Baines CP, Kaiser RA, Purcell NH, Blair
NS, Osinska H, Hambleton MA, Brunskill EW, Sayen MR, Gottlieb RA,
Dorn GW, et al: Loss of cyclophilin D reveals a critical role for
mitochondrial permeability transition in cell death. Nature.
434:658–662. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bochaton T, Crola-Da-Silva C, Pillot B,
Villedieu C, Ferrera L, Alam MR, Thibault H, Strina M, Gharib A,
Ovize M and Baetz D: Inhibition of myocardial reperfusion injury by
ischemic postconditioning requires sirtuin 3-mediated deacetylation
of cyclophilin D. J Mol Cell Cardiol. 84:61–69. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Liu J, Wang Y, Zhuang Q, Chen M, Wang Y,
Hou L and Han F: Protective effects of cyclosporine A and
hypothermia on neuronal mitochondria in a rat asphyxial cardiac
arrest model. Am J Emerg Med. 34:1080–1085. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Patil KD, Halperin HR and Becker LB:
Cardiac arrest: Resuscitation and reperfusion. Circ Res.
116:2041–2049. 2015. View Article : Google Scholar : PubMed/NCBI
|