Introduction
Silicosis, one of the most common and severe
pneumoconiosis, is characterized by extensive nodular fibrosis in
the lungs, which is caused by long-term exposure to silica dust in
industry (1). In China, 23,812 new
pneumoconiosis cases were reported in 2010, of which 9,870 were
silicosis, accounting for 41.45% (2). Silicosis has become a threat to the
occupational safety of workers worldwide (3). Therefore, it is particularly important
to find an effective treatment.
Tetrandrine is a traditional Chinese medicine
extracted from the root tuber of Stephania tetrandra, a type
of alkaloid, that can significantly improve the immune function of
patients (4,5). Moreover, it is widely used in the
treatment of silicosis, with anti-hypertensive, anti-inflammatory
and analgesic effects (6). In recent
years, acetylcysteine has been used extensively for treating
idiopathic pulmonary fibrosis (IPF) and chronic obstructive
pulmonary disease (COPD), since it is anti-oxidative stress,
anti-fibrosis and anti-inflammatory, and can effectively relieve
patients' condition (7,8).
Silicosis is the result of the interaction of many
factors and constraints, involving a variety of cells and bioactive
substances (9). Transforming growth
factor-β1 (TGF-β1), a strong fibrogenic factor, is secreted by a
variety of cells, including alveolar macrophages, endothelial
cells, fibroblasts, and epithelial cells (10,11). It
can regulate cell proliferation and differentiation, stimulate the
synthesis and secretion of various cytokines, inflammatory
mediators and other active substances, and participate in the
formation and degradation of extracellular matrix (11). By establishing silicosis rat models,
researchers (12) found that ursolic
acid retarded the development of silicosis by reducing the
expressions of TGF-β1 and IL-1. Matrix metalloproteinases (MMPs)
are potential biomarkers for diagnosing and monitoring the progress
of various fibrotic lung diseases (13). MMP-7, the smallest member of the MMPs
superfamily, degrades cytoplasmic matrix components (including
signal molecules and receptors) and is a key factor in fibrosis
(14,15). It has been reported that elevated
serum MMP-7 concentration is related to the severity of pulmonary
fibrosis and low survival rate of IPF patients (16). The effect of tetrandrine combined
with acetylcysteine on serum TGF-β1 and MMP-7 in silicosis patients
remains to be further studied. At present, the treatment outcomes
of silicosis patients are mainly reflected by pulmonary function
indexes (17). The 6-min walk test
(6MWT) is a safe detection method that has been widely used to
evaluate the degree of pulmonary function decline in patients with
pulmonary hypertension, IPF, and COPD (18,19).
The aim of the current study was to mainly evaluate
the therapeutic effect of tetrandrine combined with acetylcysteine
on silicosis through pulmonary function and exercise tolerance, and
explore its effect on the expression levels of serum TGF-β1 and
MMP-7.
Materials and methods
General information
A retrospective analysis was performed. The study
comprised 149 patients with silicosis who were admitted to the
Maternal and Child Health Care Hospital of Zhangqiu District
between August, 2015 and September, 2017. Of these patients, 70
patients treated with acetylcysteine comprised the control group,
including 51 males and 19 females, with an average age of
(52.09±5.78) years. The grade of silicosis was defined according to
a previous study (20). There were
42 silicosis patients in stage I, 23 in stage II and 5 in stage
III, with a dust exposure duration of (8.01±1.18) years. The
remaining 79 patients were treated with tetrandrine combined with
acetylcysteine and constituted the study group. This group included
55 males and 24 females, with an average age of (52.87±5.12) years.
There were 47 silicosis patients in stage I, 26 in stage II and 6
in stage III, with a dust exposure duration of (7.92±1.21)
years.
Inclusion criteria were: patients diagnosed with
silicosis by clinical manifestations, high KV chest radiography and
pulmonary function examination; patients with complete pathological
data and good compliance; patients who actively co-operated; and
patients with no blood diseases, diabetes, tumors, hypertension or
other diseases. Exclusion criteria were: patients with a history of
mental illness; pregnant women; patients complicated with active
pulmonary tuberculosis, pneumothorax, respiratory failure and other
complications; patients suffering from serious organic diseases
such as lung, liver, kidney and brain; and patients with cognitive
impairment and unable to communicate normally.
The study was approved by the Ethics Committee of
Maternal and Child Health Care Hospital of Zhangqiu District. The
subjects were informed of the experimental contents, and their
family members signed complete informed consent forms.
Treatment methods
Patients in the control group were given routine
treatment and comprehensive treatment, including anti-inflammatory,
antiasthmatic and antitussive treatment, and kept away from a
dust-exposed work environment. The nutrition and physical exercise
were increased to improve their immunity to actively prevent and
treat pulmonary tuberculosis and other complications.
Acetylcysteine effervescent tablets (600 mg; Zhejiang Conba
Biopharmaceutical Co., Ltd.; SFDA approval no. H20057334) were
administered twice a day, dissolved in warm boiled water. Twelve
days was a course of treatment, one course per month in the first
two months, then one course every 2 months, and patients received 4
courses. On the basis of the control group, patients in the study
group were given tetrandrine (Zhejiang Zhongyi Pharmaceutical Co.,
Ltd.; SFDA approval no. H33022163) orally, 60–100 mg each time,
three times a day, six days a week. After one course of treatment
(3 months), the drug was stopped for 1 month and then repeated for
one course.
Serum collection and index
detection
In the two groups, 2 ml of fasting peripheral blood
collected 1 day before treatment and the morning after treatment
were loaded into anticoagulation tubes, respectively, and sent to
the clinical laboratory. Then the blood was coagulated for 60 min
(20–25°C) and centrifuged at 2,600 × g for 10 min (4°C). The
supernatant was collected and stored at −80°C. The concentrations
of serum TGF-β1 and MMP-7 in the two groups before and after
treatment were detected by enzyme-linked immunosorbent assay
(ELISA). The microplate reader was purchased from Bio-Rad Company
(450 nm), and the serum TGF-β1 and MMP-7 kits were provided by
Shanghai Yuanmu Biotechnology Co., Ltd. (YM-S0090 and YM-S1007).
Standard, testing sample and blank wells (without sample and ELISA
reagent, the remaining steps were the same) were respectively
established. Then, 50 µl of standard sample was added accurately to
the microELISA strip plate (Shanghai, Yuanmu Biotechnology, Ltd.)
followed by the addition of 40 µl of diluent and 10 µl of sample to
the testing sample well. The plate was sealed with a closure plate
membrane and incubated at 37°C for 30 min. After uncovering the
membrane, the liquid was discarded and patted dry. Each well was
filled with PBS washing buffer (Beyotime), which was discarded
after standing. This step was repeated five times, then the well
was dried. ELISA reagent (50 µl) was added to each well, except for
blank well, then incubated and washed. Then, 50 µl of substrate A
and 50 µl of substrate B were added to each well, gently mixed and
incubated at 37°C for 10 min in the dark. The microplate reader was
removed, and 50 µl of termination solution 2 M sulphuric acid
(Shanghai, Yuanmu Biotechnology, Ltd.) was added. The optical
density (OD) value of each well at 450 mm was measured within 15
min.
Outcome measures
The improvement rates of chest distress, chest pain,
cough, expectoration, dyspnea and other clinical symptoms in the
two groups were recorded. The 6MWT and lung function indexes
[maximal voluntary ventilation (MVV) per minute, percentage of FEV1
and vital capacity percentage (FEV1/FVC%), forced expiratory volume
in 1 second (FEV1), peak expiratory flow (PEF) per second] in the
two groups were compared. The changes of serum TGF-β1 and MMP-7
before and after treatment were observed.
Statistical treatment
SPSS 19.0 software system (IBM, SPSS, Chicago, IL,
USA) was used for statistical analysis of experimental data.
Counting data were expressed as [n (%)], and the Chi-square test
was used for inter-group comparisons. Measurement data were
expressed as (mean ± SD). Inter-group comparisons were conducted by
an independent sample t-test, and comparisons between groups were
conducted by the paired t-test. P<0.05 indicated statistically
significant differences.
Results
Comparison of general data
The general data of patients in the two groups were
collected (Table I). There was no
significant differences between the two groups in terms of sex,
age, average age, dust exposure duration, smoking and silicosis
stage (P>0.05).
 | Table I.Comparison of general data between
the two groups (mean ± SD) [n (%)]. |
Table I.
Comparison of general data between
the two groups (mean ± SD) [n (%)].
| Characteristic | Study group | Control group | Chi-square
test | P-value |
|---|
| Sex |
|
| 0.189 | 0.663 |
|
Male | 55 | 51 |
|
|
|
Female | 24 | 19 |
|
|
| Age (years) |
|
| 0.502 | 0.479 |
| ≤50 | 44 | 43 |
|
|
| >50 | 35 | 27 |
|
|
| Average age
(years) | 52.87±5.12 | 52.09±5.78 | 0.874 | 0.384 |
| Dust exposure
duration (years) |
7.92±1.21 |
8.01±1.18 | 0.458 | 0.647 |
| Smoking |
|
| 0.237 | 0.626 |
| Yes | 42 | 40 |
|
|
| No | 37 | 30 |
|
|
| Stage |
|
| 0.012 | 0.994 |
| I | 47 | 42 |
|
|
| II | 26 | 23 |
|
|
| III | 6 | 5 |
|
|
Comparison of clinical symptoms
between the two groups before and after treatment
Cough, expectoration, chest distress, chest pain and
dyspnea in the two groups were relieved after treatment (Table II). The improvement rates of chest
distress, chest pain and dyspnea in the study group were
significantly higher than those in the control group, with
statistically significant difference (P<0.05).
| Table II.Comparison of clinical symptoms
between two groups before and after treatment/cases. |
Table II.
Comparison of clinical symptoms
between two groups before and after treatment/cases.
| Item | Chest distress | Chest pain | Cough | Expectoration | Dyspnea |
|---|
| Study group
(n=79) |
| Before
treatment | 69 | 73 | 77 | 72 | 65 |
| After
treatment | 7 | 9 | 11 | 13 | 6 |
|
Improvement rate | 78.5% | 81.0% | 83.5% | 74.7% | 74.7% |
| Control group
(n=70) |
| Before
treatment | 63 | 68 | 70 | 67 | 60 |
| After
treatment | 19 | 21 | 19 | 15 | 17 |
|
Improvement rate | 62.9%a | 67.1%a | 72.9a | 74.3% | 61.4%a |
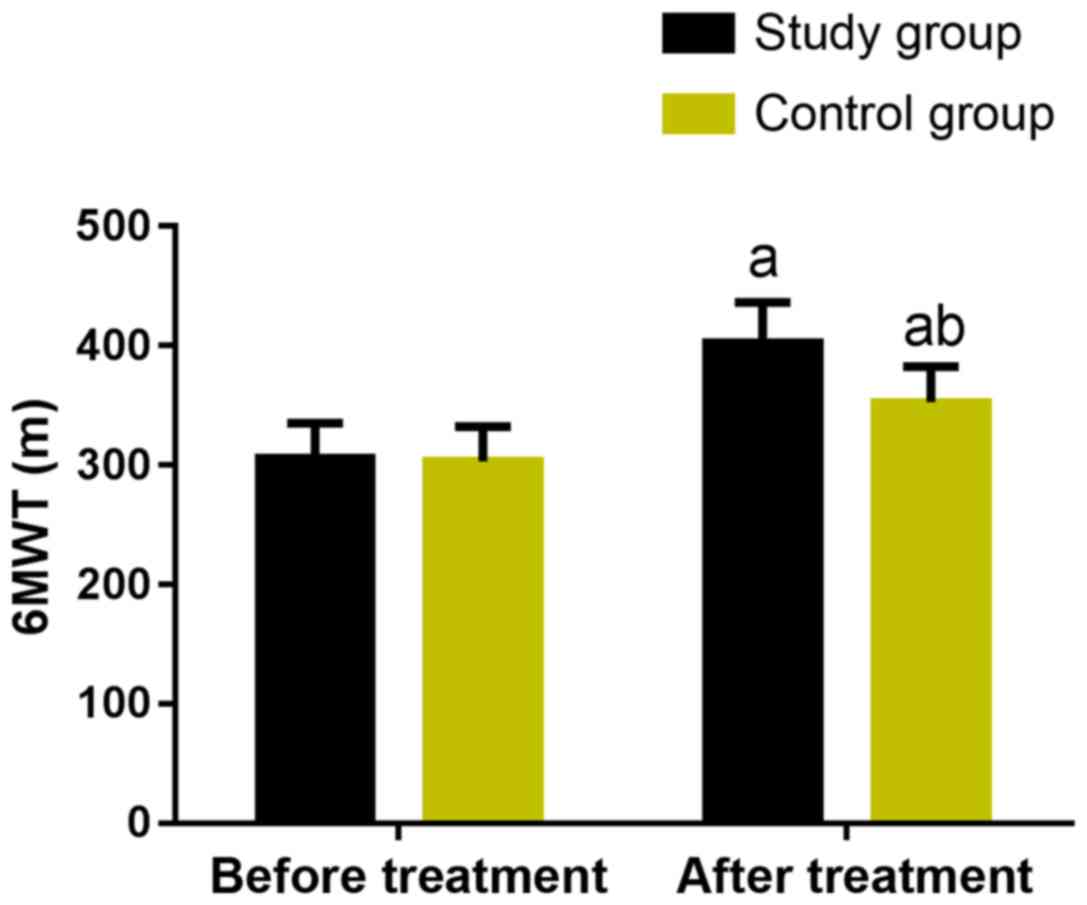
Comparison of exercise tolerance
between two groups
Exercise tolerance was compared between the two
groups, as shown in Fig. 1. Before
treatment, there was no significant difference in the results of
6MWT between the two groups (P>0.05). After treatment, the 6MWT
in the two groups was significantly increased (P<0.05), and the
improvement effect in the study group was more marked than that in
the control group (P<0.05).
Comparison of pulmonary function
between the two groups
There was no significant difference in pulmonary
function indexes between the two groups before treatment
(P>0.05). By contrast, the indexes in the two groups were
significantly increased after treatment (P<0.05), including MVV,
PEF, FEV1, FEV1/FVC%. Specifically, the indexes in the study group
were significantly higher than those in the control group
(P<0.05) (Fig. 2).
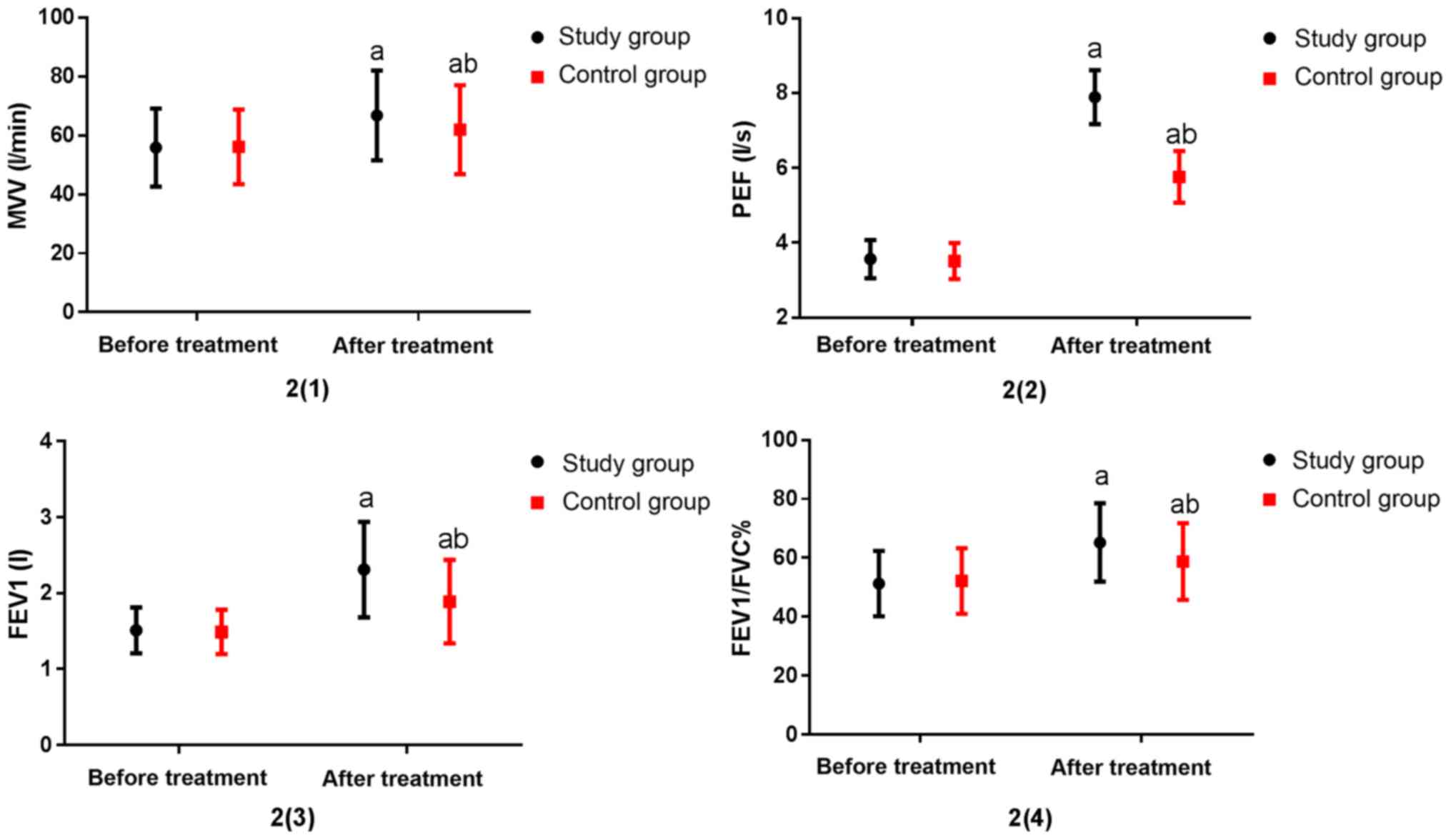 | Figure 2.Comparison of lung function between
the two groups. Before treatment, there was no significant
difference in lung function between the two groups (P>0.05).
After treatment, the lung function indexes MVV, PEF, FEV1,
FEV1/FVC% were significantly higher than those before treatment (P
<0.05). MVV, PEF, FEV1, FEV1/FVC% in the study group were
significantly higher than those in the control group, with
statistically significant differences (P<0.05). a vs. before
treatment, aP<0.05; b vs. the study group after
treatment, bP<0.05. |
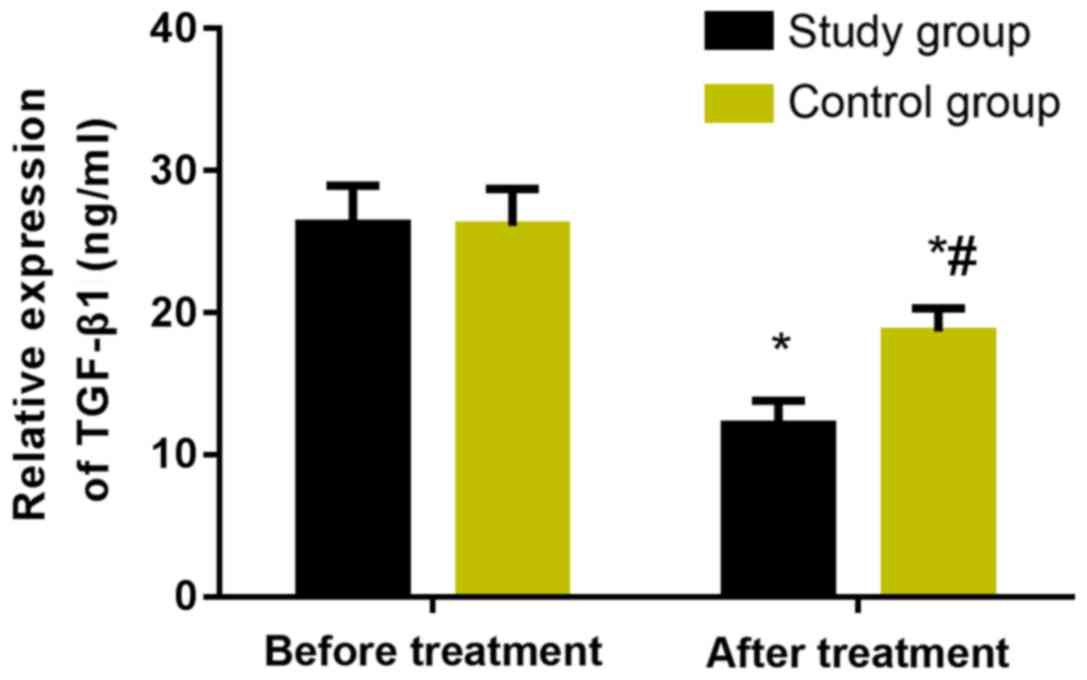
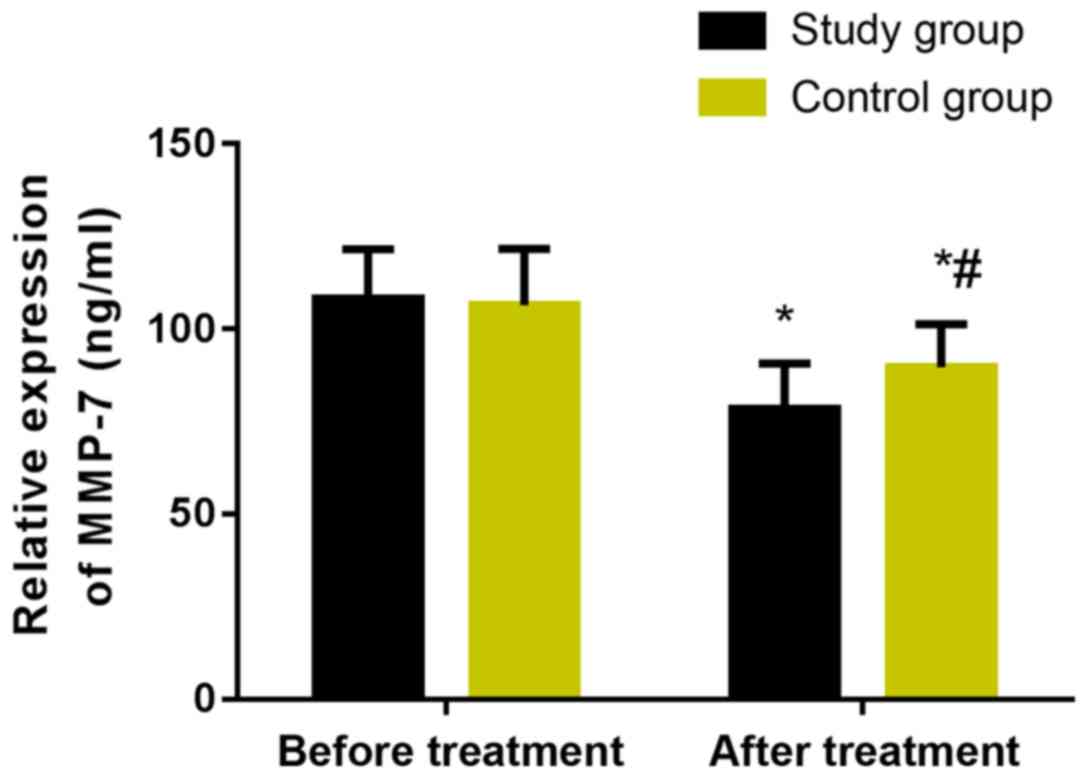
Changes of serum TGF-β1 and MMP-7
before and after treatment in the two groups
The levels of serum TGF-β1 and MMP-7 in the two
groups were measured before and after treatment (Figs. 3 and 4). Before treatment, there was no
significant difference in serum TGF-β1 and MMP-7 expression levels
between the two groups (P>0.05). However, after treatment, the
levels in the two groups were significantly decreased, and the
study group was statistically significantly lower than the control
group (P<0.05).
Discussion
Silicosis is a systemic disease characterized by
pulmonary fibrosis, mainly caused by long-term inhalation of dust
containing free silica (21). The
gradual development of pulmonary fibrosis may lead to gas exchange
area reduction, lung function damage, thus resulting in respiratory
failure, or even lung cancer in severe cases (22). Therefore, effective clinical
treatment should be taken to improve the pulmonary function of
patients to prevent the deterioration of the condition.
Tetrandrine is a strong calcium antagonist and
affects the transmembrane transport of calcium ions by acting on
calcium channels, thus playing a blocking effect on calcium
channels of lung fibroblasts. Moreover, it can also promote the
loosening and degradation of lung collagen fibers, the
disappearance and depolymerization of microtubule structures, thus
hindering the transformation of procollagen and preventing
pulmonary fibrosis (23). Modern
pharmacology shows that tetrandrine improves phagocytosis of
macrophages and enhances excretion by acting on collagen
macromolecules and combining with them, effectively preventing
inflammation and pulmonary fibrosis (24). It has been shown that a free
radical-mediated oxidation/antioxidation imbalance plays an
important role in the occurrence and development of silica-induced
pulmonary fibrosis (25).
Acetylcysteine, a precursor of reduced glutathione with an
antioxidant effect, can reduce the level of free radicals,
antagonize pulmonary fibrosis caused by free radicals, and delay
the process of pulmonary fibrosis induced by silicosis (25–27).
The occurrence and progression of silicosis is an
interweaving process of inflammation and fibrosis, in which
cytokines play an important role (28). TGF-β1 is considered the strongest
extracellular matrix precipitation promoter and the most direct
cytokine to promote pulmonary fibrosis (29). It may promote the increase of
extracellular matrix by up-regulating the expressions of
fibronectin and collagen, and may inhibit the degradation of
extracellular matrix by increasing the secretion of protease
inhibitor and decreasing the secretion of matrix metalloproteinase,
eventually participating in the process of pulmonary fibrosis
(30). MMP-7 is a matrix
metalloproteinase, which has local inflammatory regulatory effects
(31,32), and is highly up-regulated in alveolar
epithelial cells of idiopathic pulmonary fibrosis (IPF) (32,33). In
addition, MMP-7 knockout mice were relatively unaffected by
bleomycin (a fibrosis inducer), suggesting that MMP-7 may promote
fibrosis in IPF (33). Moreover,
MMP-7 may stimulate epithelial cells by lysis of E-cadherin
(34) and activate heparin-binding
epidermal growth factor-like growth factor (proHB-EGF) by
proteolysis, leading to the release of activated HB-EGF and the
proliferation of human lung fibroblasts (35), thus promoting pulmonary fibrosis.
However, the main mechanism of TGF-β1 and MMP-7 in silicosis
patients needs to be further proved.
Findings of this study showed that chest distress,
chest pain, cough, expectoration and dyspnea in the two groups were
relieved after treatment, and the improvement rates of chest
distress, chest pain and dyspnea in the study group were
significantly higher than those in the control group, with
statistically significant difference (P<0.05). Thus, tetrandrine
combined with acetylcysteine effervescent tablets improves the
occurrence of adverse respiratory symptoms, and its effect is
better than that of single drug. Li et al (36) compared the clinical effects of
tetrandrine combined with acetylcysteine effervescent tablets
(observation group) and conventional treatment (control group) on
silicosis. The results showed that there was no significant
difference in respiratory symptoms between the two groups before
treatment. After treatment, the symptoms in the two groups were
significantly improved, and the improvement rates of cough,
expectoration, chest pain, chest distress and other symptoms in the
observation group were significantly better than those in the
control group. This is similar to the study in this paper, but
probably due to the small sample size, there was no significant
difference between the two groups in the improvement rates of cough
and expectoration. In this study, the exercise tolerance in the two
groups was compared. The results showed that there was no
significant difference in the results of 6MWT before treatment
(P>0.05). After treatment, the 6MWT in the two groups was
significantly increased (P<0.05), and the improvement effect in
the study group was more marked than that in the control group
(P<0.05). Previous findings showed that the 6MWT of patients
treated with high-dose N-acetylcysteine was significantly higher
than that with conventional dose in treating silicosis (37). Combined with this study, it has been
shown that tetrandrine combined with high-dose acetylcysteine can
significantly improve exercise tolerance of silicosis patients.
There was no significant difference in pulmonary function indexes
between the two groups before treatment (P>0.05). After
treatment, pulmonary function indexes MVV, PEF, FEV1, FEV1/FVC% in
the two groups were significantly increased, and those indexes in
the study group were significantly higher than those in the control
group. It was also reported that tetrandrine combined with
acetylcysteine can significantly improve FVC and FEV and lung
ventilation function of silicosis patients (38). Xiao et al (39) used silicosis models to show that
tetrandrine combined with acetylcysteine can significantly delay
and inhibit the process of pulmonary fibrosis, and the therapeutic
effect was better than that of single drug. Therefore, tetrandrine
and acetylcysteine can both achieve good therapeutic effects, but
the combination is better. It was reported that the high expression
of MMP-7 in plasma of IPF patients was positively correlated with
the severity of the disease (40),
and that the expression of TGF-β1 was upregulated in the peripheral
blood of silicosis patients (41).
In this study, there was no significant difference in serum TGF-β1
and MMP-7 expression levels between the two groups before
treatment. By contrast, after treatment, the levels in the two
groups were significantly decreased, and the levels in the study
group were significantly lower than those in the control group.
This suggests that tetrandrine combined with acetylcysteine can
significantly reduce the expressions of TGF-β1 and MMP-7 in serum
of silicosis patients. A study found that tetrandrine can inhibit
the expression of MMP-2 protein in human umbilical vein endothelial
cells (HUVEC) cultured in vitro (42). Combined with the results of this
study, it is suggested that tetrandrine may inhibit MMP-7
expression by the same mechanism. The effects of N-acetylcysteine
on pulmonary fibrosis, endothelial injury and vasoactive factor in
patients with chronic pulmonary heart disease were studied
(43), and it was found that
N-acetylcysteine can significantly reduce the expression levels of
TGF-β1 and MMP-7 in serum of those patients.
The results of the present study mainly explored the
curative effect of tetrandrine combined with acetylcysteine on
silicosis patients and its influence on TGF-β1 and MMP-7
expressions. The prognosis and influencing factors of silicosis and
the mechanism of tetrandrine combined with acetylcysteine in
silicosis patients will be further explored, so as to provide more
definite references for the pathogenesis, clinical diagnosis and
treatment of silicosis. To sum up, tetrandrine combined with
acetylcysteine can improve pulmonary function and exercise
tolerance of patients with silicosis by inhibiting the expressions
of TGF-β1 and MMP-7, thus improving the clinical efficacy.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
JZ and YW was responsible for ELISA. SZ analyzed and
interpreted the patients' data. JL and HF helped with statistical
analysis. JZ wrote the manuscript. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Maternal and Child Health Care Hospital of Zhangqiu District.
Patients who participated in this research, signed the informed
consent and had complete clinical data. Signed written informed
consents were obtained from the patients and/or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chen S, Yuan J, Yao S, Jin Y, Chen G, Tian
W, Xi J, Xu Z, Weng D and Chen J: Lipopolysaccharides may aggravate
apoptosis through accumulation of autophagosomes in alveolar
macrophages of human silicosis. Autophagy. 11:2346–2357. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Castranova V and Vallyathan V: Silicosis
and coal workers' pneumoconiosis. Environ Health Perspect.
108:675–684. 2000. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Murtha LA, Morten M, Schuliga MJ,
Mabotuwana NS, Hardy SA, Waters DW, Burgess JK, Ngo DT, Sverdlov
AL, Knight DA, et al: The role of pathological aging in cardiac and
pulmonary fibrosis. Aging Dis. 10:419–428. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mei L, Chen Y, Wang Z, Wang J, Wan J, Yu
C, Liu X and Li W: Synergistic anti-tumour effects of tetrandrine
and chloroquine combination therapy in human cancer: A potential
antagonistic role for p21. Br J Pharmacol. 172:2232–2245. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kolahian S, Fernandez IE, Eickelberg O and
Hartl D: Immune mechanisms in pulmonary fibrosis. Am J Respir Cell
Mol Biol. 55:309–322. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liu T, Liu X and Li W: Tetrandrine, a
Chinese plant-derived alkaloid, is a potential candidate for cancer
chemotherapy. Oncotarget. 7:40800–40815. 2016.PubMed/NCBI
|
|
7
|
Wynn TA: Integrating mechanisms of
pulmonary fibrosis. J Exp Med. 208:1339–1350. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Strieter RM and Mehrad B: New mechanisms
of pulmonary fibrosis. Chest. 136:1364–1370. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sun W, Tang H, Gao L, Sun X, Liu J, Wang
W, Wu T and Lin H: Mechanisms of pulmonary fibrosis induced by core
fucosylation in pericytes. Int J Biochem Cell Biol. 88:44–54. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Warburton D, Shi W and Xu B: TGF-β-Smad3
signaling in emphysema and pulmonary fibrosis: An epigenetic
aberration of normal development? Am J Physiol Lung Cell Mol
Physiol. 304:L83–L85. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Aono Y, Ledford JG, Mukherjee S, Ogawa H,
Nishioka Y, Sone S, Beers MF, Noble PW and Wright JR: Surfactant
protein-D regulates effector cell function and fibrotic lung
remodeling in response to bleomycin injury. Am J Respir Crit Care
Med. 185:525–536. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Doyle TJ, Pinto-Plata V, Morse D, Celli BR
and Rosas IO: The expanding role of biomarkers in the assessment of
smoking-related parenchymal lung diseases. Chest. 142:1027–1034.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Morrison MI, Pither TL and Fisher AJ:
Pathophysiology and classification of primary graft dysfunction
after lung transplantation. J Thorac Dis. 9:4084–4097. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pei JS, Chou AK, Hsu PC, Tsai CW, Chang
WS, Wu MF, Wu MH, Hsia TC, Cheng SP and Bau DT: Contribution of
matrix metalloproteinase-7 genotypes to the risk of non-solid
tumor, childhood leukemia. Anticancer Res. 37:6679–6684.
2017.PubMed/NCBI
|
|
15
|
Martinez FJ, Chisholm A, Collard HR,
Flaherty KR, Myers J, Raghu G, Walsh SL, White ES and Richeldi L:
The diagnosis of idiopathic pulmonary fibrosis: Current and future
approaches. Lancet Respir Med. 5:61–71. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Song JW, Do KH, Jang SJ, Colby TV, Han S
and Kim DS: Blood biomarkers MMP-7 and SP-A: predictors of outcome
in idiopathic pulmonary fibrosis. Chest. 143:1422–1429. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rosas IO, Goldberg HJ, Collard HR,
El-Chemaly S, Flaherty K, Hunninghake GM, Lasky JA, Lederer DJ,
Machado R, Martinez FJ, et al: A phase II clinical trial of
low-dose inhaled carbon monoxide in idiopathic pulmonary fibrosis.
Chest. 153:94–104. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Flaherty KR, Andrei AC, Murray S, Fraley
C, Colby TV, Travis WD, Lama V, Kazerooni EA, Gross BH, Toews GB,
et al: Idiopathic pulmonary fibrosis: Prognostic value of changes
in physiology and six-minute-walk test. Am J Respir Crit Care Med.
174:803–809. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Miyamoto S, Nagaya N, Satoh T, Kyotani S,
Sakamaki F, Fujita M, Nakanishi N and Miyatake K: Clinical
correlates and prognostic significance of six-minute walk test in
patients with primary pulmonary hypertension. Comparison with
cardiopulmonary exercise testing. Am J Respir Crit Care Med.
161:487–492. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ma J, Zhou Y, Li W, Xiao L, Yang M, Tan Q,
Xu Y and Chen W: Association between plasma HMGB-1 and silicosis: A
case-control study. Int J Mol Sci. 19:40432018. View Article : Google Scholar
|
|
21
|
Wang SX, Liu P, Wei MT, Chen L, Guo Y,
Wang RY, Tu ZG and Liang XC: Roles of serum clara cell protein 16
and surfactant protein-D in the early diagnosis and progression of
silicosis. J Occup Environ Med. 49:834–839. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Racanelli AC, Kikkers SA, Choi AMK and
Cloonan SM: Autophagy and inflammation in chronic respiratory
disease. Autophagy. 14:221–232. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Dong J and Ma Q: Macrophage polarization
and activation at the interface of multi-walled carbon
nanotube-induced pulmonary inflammation and fibrosis.
Nanotoxicology. 12:153–168. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Raha S, Kim SM, Lee HJ, Lee SJ, Heo JD,
Venkatarame Gowda Saralamma V, Ha SE, Kim EH, Mun SP and Kim GS:
Essential oil from Korean Chamaecyparis obtusa leaf
ameliorates respiratory activity in Sprague Dawley rats and
exhibits protection from NF-κB-induced inflammation in WI38
fibroblast cells. Int J Mol Med. 43:393–403. 2019.PubMed/NCBI
|
|
25
|
Zeidler P, Hubbs A, Battelli L and
Castranova V: Role of inducible nitric oxide synthase-derived
nitric oxide in silica-induced pulmonary inflammation and fibrosis.
J Toxicol Environ Health A. 67:1001–1026. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Duru N, Wolfson B and Zhou Q: Mechanisms
of the alternative activation of macrophages and non-coding RNAs in
the development of radiation-induced lung fibrosis. World J Biol
Chem. 7:231–239. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Liu L, Carron B, Yee HT, Yie TA, Hajjou M
and Rom W: Wnt pathway in pulmonary fibrosis in the bleomycin mouse
model. J Environ Pathol Toxicol Oncol. 28:99–108. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang X and Khalil RA: Matrix
metalloproteinases, vascular remodeling, and vascular disease. Adv
Pharmacol. 81:241–330. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gharib SA, Johnston LK, Huizar I, Birkland
TP, Hanson J, Wang Y, Parks WC and Manicone AM: MMP28 promotes
macrophage polarization toward M2 cells and augments pulmonary
fibrosis. J Leukoc Biol. 95:9–18. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Mohammed FF, Smookler DS and Khokha R:
Metalloproteinases, inflammation, and rheumatoid arthritis. Ann
Rheum Dis. 62:ii43–ii47. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Li Q, Park PW, Wilson CL and Parks WC:
Matrilysin shedding of syndecan-1 regulates chemokine mobilization
and transepithelial efflux of neutrophils in acute lung injury.
Cell. 111:635–646. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
McGuire JK, Li Q and Parks WC: Matrilysin
(matrix metalloproteinase-7) mediates E-cadherin ectodomain
shedding in injured lung epithelium. Am J Pathol. 162:1831–1843.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zuo F, Kaminski N, Eugui E, Allard J,
Yakhini Z, Ben-Dor A, Lollini L, Morris D, Kim Y, DeLustro B, et
al: Gene expression analysis reveals matrilysin as a key regulator
of pulmonary fibrosis in mice and humans. Proc Natl Acad Sci USA.
99:6292–6297. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Datta A, Scotton CJ and Chambers RC: Novel
therapeutic approaches for pulmonary fibrosis. Br J Pharmacol.
163:141–172. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Craig VJ, Zhang L, Hagood JS and Owen CA:
Matrix metalloproteinases as therapeutic targets for idiopathic
pulmonary fibrosis. Am J Respir Cell Mol Biol. 53:585–600. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Lee SH, Yeo Y, Kim TH, Lee HL, Lee JH,
Park YB, Park JS, Kim YH, Song JW, Jhun BW, et al Korean
Interstitial Lung Diseases Study Group, : Korean guidelines for
diagnosis and management of interstitial lung diseases: Part 2.
Idiopathic pulmonary fibrosis. Tuberc Respir Dis (Seoul).
82:102–117. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Benjamin MM and Khalil RA: Matrix
metalloproteinase inhibitors as investigative tools in the
pathogenesis and management of vascular disease. Exp Suppl.
103:209–279. 2012.PubMed/NCBI
|
|
38
|
Miao RM, Sun XF, Zhang YY, Wu W, Fang ZH,
Zhao R, Zhao DK, Qian GL and Ji J: Clinical efficacy of tetrandrine
combined with acetylcysteine effervescent tablets in treatment of
silicosis. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi.
31:857–858. 2013.(In Chinese). PubMed/NCBI
|
|
39
|
Xiao Y, Xia H, Zhu L, Li X, Chen R, Yin X,
Jiang Z, Feng L, Chen J, Yu M, et al: Study on the therapeutic
effects of tetrandrine combined with N-acetylcysteine on
experimental silicosis of rats. Zhonghua Lao Dong Wei Sheng Zhi Ye
Bing Za Zhi. 33:519–522. 2015.(In Chinese). PubMed/NCBI
|
|
40
|
Ning JX, Zhang LP and Cui Y: Evaluation of
clinical efficacy of tretrandrine combined with acetylcysteine
effervescent tablets in the treatment of silicosis. Zhonghua Lao
Dong Wei Sheng Zhi Ye Bing Za Zhi. 35:298–299. 2017.(In Chinese).
PubMed/NCBI
|
|
41
|
Miao RM, Zhang XT, Yan YL, He EQ, Guo P,
Zhang YY, Zhao DK, Yang ZG, Chen J, Yao MY, et al: Change of serum
TGF-beta1 and TNF-alpha in silicosis patients. Zhonghua Lao Dong
Wei Sheng Zhi Ye Bing Za Zhi. 29:606–607. 2011.(In Chinese).
PubMed/NCBI
|
|
42
|
Sadikot RT, Blackwell TS, Christman JW and
Prince AS: Pathogen-host interactions in Pseudomonas
aeruginosa pneumonia. Am J Respir Crit Care Med. 171:1209–1223.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Hill MR, Briggs L, Montaño MM, Estrada A,
Laurent GJ, Selman M and Pardo A: Promoter variants in tissue
inhibitor of metalloproteinase-3 (TIMP-3) protect against
susceptibility in pigeon breeders' disease. Thorax. 59:586–590.
2004. View Article : Google Scholar : PubMed/NCBI
|