Introduction
Induction is recommended for all renal
transplantation (RT) recipients, except for haplo-identical living
related-donor transplantations (1).
Anti-T-lymphocyte globulins (ATGs), which may effectively attenuate
the risk of acute rejection and improve graft survival, is
frequently used for induction in solid organ transplantation
(2). ATG-Fresenius (ATG-F;
Neovii-Biotech), a highly purified rabbit polyclonal anti-human
T-lymphocyte immunoglobulin derived from immunizing rabbits with
the Jurkat T-Lymphoblast cell line, is one of the
best-characterized types of ATGs (3). Short-term induction is more preferable
due to the prominent toxicity associated with long-term
administration (4). However, the
optimal dose, the maximal tolerable cumulative dose and the dosing
frequency of ATG-F remain undefined despite the fact that ATG-F has
been in use for many years. Kaden et al (5,6)
attempted to re-schedule the timing of ATG-F induction from the
post-operative period to the pre-operative period and use a single
high dose (9 mg/kg) for induction, and they revealed that the
reschedule increased the rates of graft and patient survival
compared to those receiving routine triple-drug maintenance
therapy. However, Meier-Kriesche et al (7) indicated that ATG-F reduced the risk of
acute rejection but also caused serious adverse effects in the
renal graft recipients, including higher mortality linked to
cardiovascular or infectious episodes and a higher incidence of
advanced malignancy. In addition, Chen et al (8) reported that a regimen consisting of a
cumulative ATG-F dose of 6 mg/kg (2 mg/kg/day during the operation
and on post-operative days 1 and 2) provided adequate protection
from acute rejection.
At the Affiliated Hospital of Qingdao University
(Qingdao, China), a cumulative ATG-F dose of 7 mg/kg based on
actual body weight has been consistently used for the induction of
renal transplantation. However, doses are rounded to the nearest
vial size and the range of the dose lies between 400 and 600 mg;
this practice may result in administering a cumulative dose of
<7 mg/kg for overweight patients but ≥7 mg/kg for underweight
ones. The absence of randomized controlled trials and controversial
data from the existing literature points to the requirement for
data to facilitate the selection of optimal ATG-F induction doses
for recipients of kidney graft, particularly under the circumstance
of ATG-F provided with triple immunosuppressive maintenance.
Therefore, in the present study, the efficacy and safety associated
with different cumulative doses of ATG-F induction were assessed in
renal transplant recipients receiving a steroid-containing
maintenance regimen.
Materials and methods
Enrollment of participants
The present retrospective single-center cohort study
included adult renal transplant recipients who received a deceased
donor graft at the Affiliated Hospital of Qingdao University
(Qingdao, China) between August 2015 and July 2018. All
participants received ATG-F induction and were maintained on
tacrolimus, enteric-coated mycophenolate sodium (EC-MPS) and
prednisone. According to the institutional protocol, the
indications for ATG-F induction included the following: i) Chinese
ethnicity; ii) receipt of deceased donor renal transplant; iii)
panel reactive antibody (PRA) between 0 and 10%, or a negative
pre-operative PRA but a positive history in the waiting list; or
iv) a history of blood transfusion within 3 months prior to
surgery. Patients were excluded if they had a history of prior
non-renal transplantation, received a simultaneous non-renal
transplant, underwent desensitization, experienced primary graft
non-function, received a positively cross-matched renal graft, or
received any experimental medications or ATG-F for
non-protocol-based indications.
Categorization of study participants
based on ATG-F doses
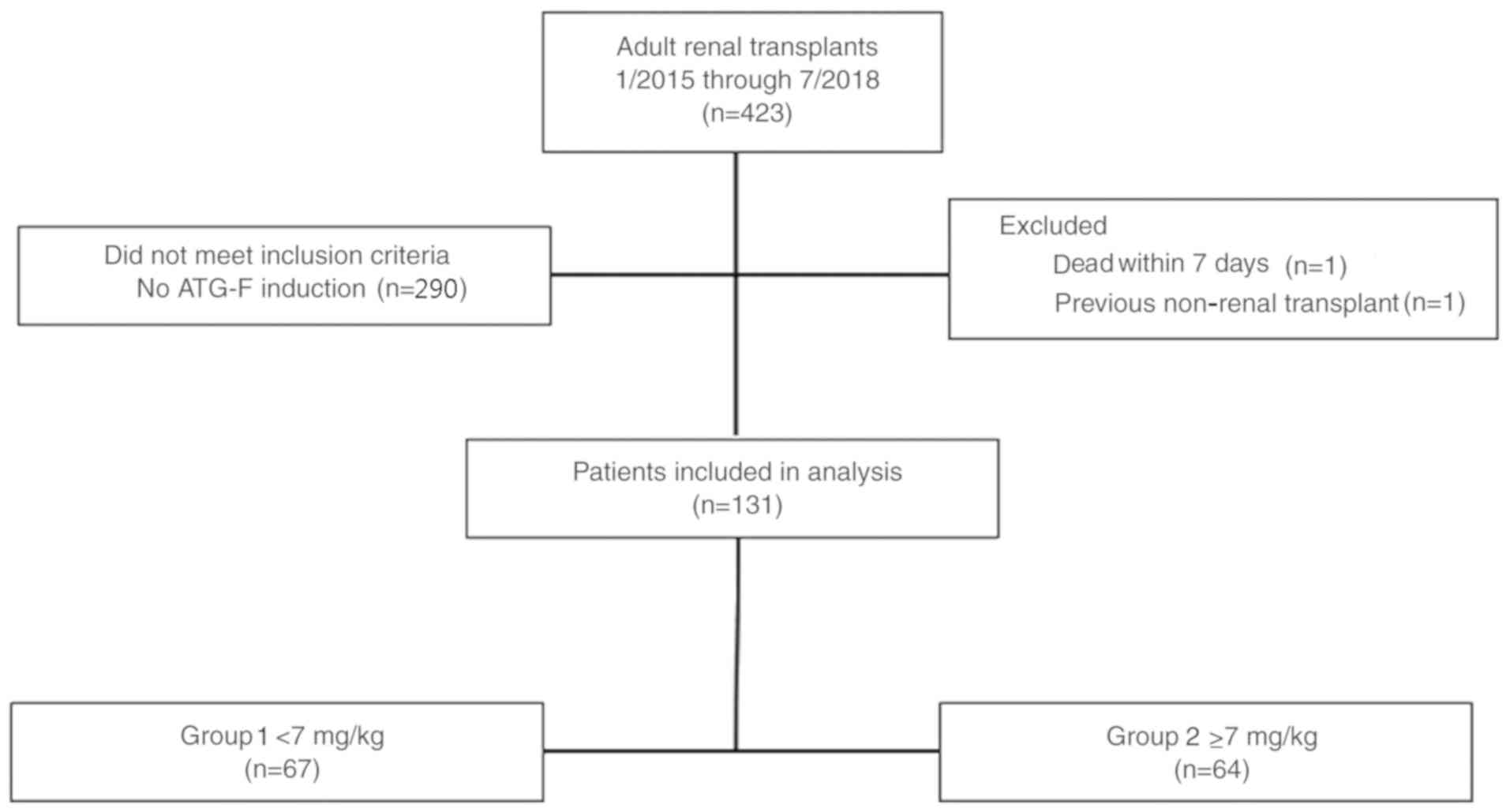
Eligible patients were divided into 2 groups,
including the cumulative ATG-F dose <7 mg/kg group (group 1) and
the ≥7 mg/kg group (group 2) based on the pre-operative actual body
weight.
The induction regimen of ATG-F consisted of 2 mg/kg
administered on post-operative day (POD) 0 and POD 1, followed by
another 1.5 mg/kg on POD 2 and POD 3, for a cumulative dose of 7
mg/kg. Doses were rounded to the nearest vial size (100 mg) and
capped at 200 mg based on the 2 mg/kg schedule on POD 0 and 1, and
100 mg based on the 1.5 mg/kg schedule on POD 2 and 3. Dose
modifications were not allowed for patients with leukopenia or
thrombocytopenia. The cumulative ATG-F dosages for group 1 and 2
were 442.19±77.08 mg (400–600 mg) and 485.93±58.27 mg (400–600 mg),
respectively (P<0.001). Corticosteroids were administered
according to the following schedule: Intravenous methylprednisolone
500 or 750 mg given intra-operatively followed by another 500 mg on
POD 1 and 2, and oral prednisone starting at 16 mg on POD 3 with
gradual tapering to 4 mg by POD 90. In addition, oral tacrolimus
0.05–0.06 mg/kg every 12 h was initiated within 24 h of renal
transplantation, with the trough levels set at 8–10 ng/ml between
POD 0 and 30, 6–8 ng/ml between POD 31 and 180, and 5–7 ng/ml after
POD 181. Oral EC-MPS 540 or 720 mg was administered every 12 h on
POD 0. All patients received prophylaxis for Pneumocystis
jiroveci infection using trimethoprim/sulfamethoxazole for 6–12
months, except those presenting with severe leukopenia or having a
serum creatinine level exceeding 2 mg/dl. Prophylaxis against
cytomegalovirus (CMV) was not routinely administered.
Endpoint definitions
The primary endpoint was incident biopsy-confirmed
acute rejection (BCAR) within 12 months after transplantation,
based on the Banff histologic criteria (9). Secondary endpoints included incident
infections (all), pneumonia, urinary tract infection; CMV or BK
viruria and viremia, BK virus nephropathy (BKVN), hematologic
adverse effects including anemia, leukopenia, thrombocytopenia and
lymphopenia; delayed graft function, as well as overall patient and
graft survival. Graft function was assessed via measuring serum
creatinine levels at 12 months. BK virus was screened by PCR-based
assays at 1, 3, 6, 9 and 12 months after transplantation, or as
required when serum creatinine increased for unknown reasons. PCR
assays for CMV were performed at 1, 3, 6 and 12 months after
transplantation in the presence of symptoms and signs suggestive of
CMV infection. Delayed graft function was defined according to a
urine output level of <0.5 ml/kg/h, a decline in serum
creatinine <10% from pre-transplant levels within 24 h, or a
requirement for hemodialysis within 1 week after transplantation.
Primary non-function of renal grafts was defined as recipients
requiring maintenance dialysis or re-transplantation, excluding
those who died with functional grafts.
Statistical analysis
The Student's t-test and one-way analysis of
variance were used to compare continuous variables. Categorical
variables were compared using the χ2 test. Continuous
variables are expressed as the mean ± the standard deviation. A
P-value <0.05 was deemed significant. All statistical analyses
were performed using SPSS 21 (IBM Corp.).
Results
Clinical characteristics of study
participants
Of the 423 renal transplantations performed between
August 2015 and July 2018, 131 cases were included in the final
analysis (Fig. 1). Participants in
the two dose groups were well matched with regard to demographics
and immunological risk factors aside from by body weight and body
mass index (Table I). The clinical
features of the donors are presented in Table II. There was no significant
difference between groups 1 and 2 in terms of age, sex, cause of
death or duration of ischemia. The mean ATG-F dose in group 1 was
significantly lower than that in group 2 (5.90±0.93 vs. 8.24±1.05
mg/kg, P<0.001). The cumulative ATG-F dosages in groups 1 and 2
were 442.19±77.08 mg (400–600) and 485.93±58.27 mg (400–600),
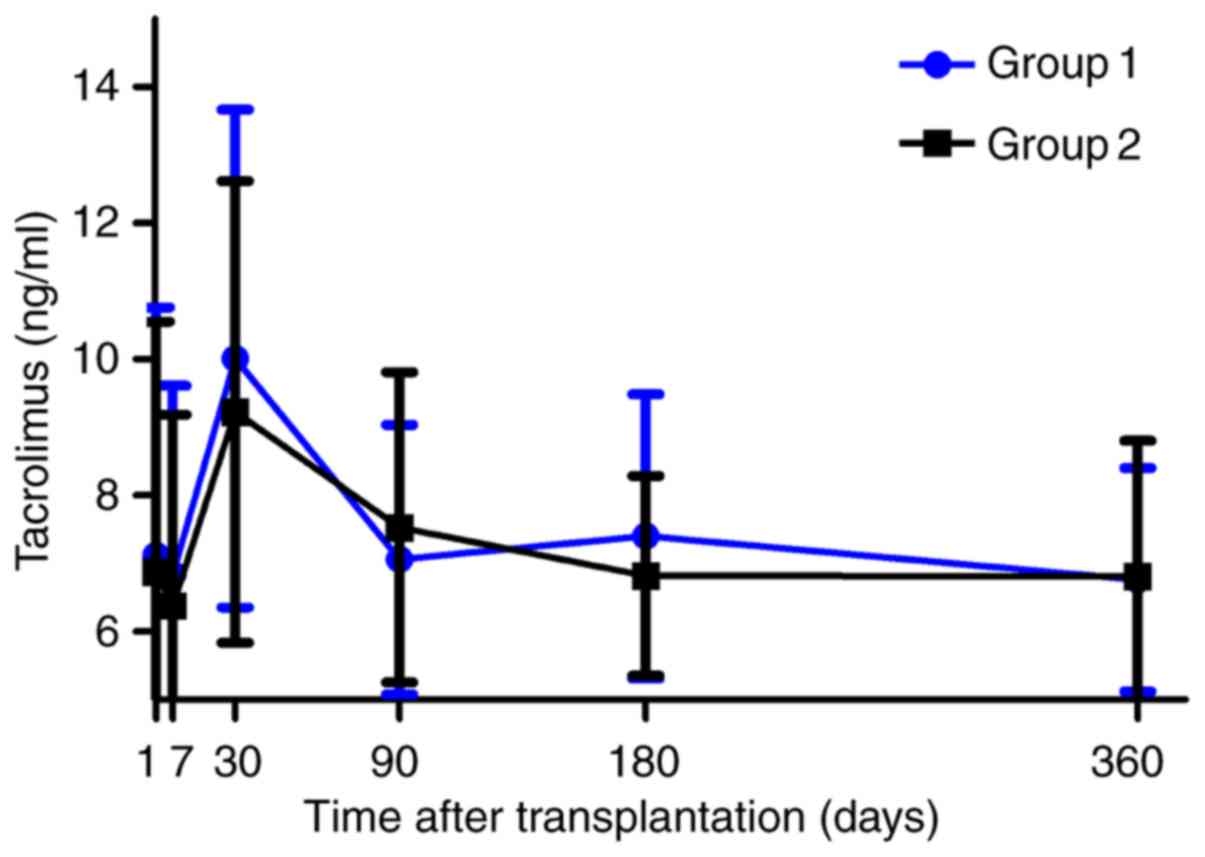
respectively (P<0.001). The trough levels of tacrolimus were
similar between the two groups during the follow-up period
(Fig. 2 and Table III). All participants were
maintained on a steroid-containing regimen and continued the triple
maintenance immunosuppression for 12 months (Table III). The overall incidence of
delayed graft function was 6.1% and the incidence did not differ
between the two groups (7.4 vs. 4.7%, P=0.766; Table II).
 | Table I.Comparison of clinical features
between groups 1 and 2. |
Table I.
Comparison of clinical features
between groups 1 and 2.
| Parameter | Group 1 (n=67) | Group 2 (n=64) | P-value |
|---|
| Age (years) | 41.9±10.1 | 39.5±10.5 | 0.751 |
| Sex, Male (n, %) | 59 (88.1) | 43 (67.2) | 0.330 |
| ABW (kg) | 73.4±13.5 | 59.6±9.3 | 0.009 |
| BMI
(kg/m2) | 24.3±3.69 | 20.7±2.85 | 0.047 |
| Follow up (days) | 480 (90–1140) | 610 (125–1145) | 0.584 |
| Indication for
transplant (n, %) |
|
| 0.632 |
| CGN | 45 (67.2) | 48 (75.0) |
|
| IgAN | 6 (9.0) | 5 (7.8) |
|
| DN | 8
(11.8) | 6 (9.4) |
|
| HTN | 2 (3.0) | 1 (1.6) |
|
| PCKD | 3 (4.5) | 1 (1.6) |
|
|
Other | 3 (4.5) | 3 (4.6) |
|
| Dialysis mode (n,
%) |
|
| 0.655 |
|
Preemptive | 3 (4.5) | 5 (7.8) |
|
| HD | 57 (85.1) | 54 (84.4) |
|
| PD | 7 (10.4) | 5 (7.8) |
|
| Dialysis
duration | 12 | 12 | 0.268 |
| HLA mismatch | 2.8±1.3 | 3.0±1.2 | 0.363 |
| Table II.Clinical features of the donors. |
Table II.
Clinical features of the donors.
| Parameter | Group 1 (n=34) | Group 2 (n=32) | P-value |
|---|
| Age (years) | 39.1±9.9 | 40.7±13.1 | 0.576 |
| Sex, Male (n, %) | 28 (82.4) | 26 (81.3) | 0.908 |
| Cause of death (n,
%) |
|
| 0.972 |
| Traumatic
brain injury | 18 (52.9) | 16 (50.0) |
|
|
Encephalorrhagia | 14 (41.2) | 14 (43.8) |
|
|
Other | 2 (5.9) | 2 (6.2) |
|
| Warm ischemic time
(min) |
8.2±4.3 |
8.7±4.6 | 0.650 |
| Cold ischemic time
(h) |
7.6±2.7 |
7.7±2.3 | 0.872 |
| Mean ATG-F dose
(mg/kg) |
5.90±0.93 |
8.24±1.05 | <0.001 |
| Cumulative ATG-F dose
(mg) | 442.19±77.08 | 485.93±58.27 | <0.001 |
| Incidence of delayed
graft function (%) | 7.4% | 4.7% | 0.766 |
| Mean serum creatinine
at 12 months (mg/dl) | 1.23±0.64 | 1.19±0.58 | 0.165 |
| Table III.Mean trough tacrolimus levels in
subjects on maintenance immunosuppression and immunosuppression at
12 months. |
Table III.
Mean trough tacrolimus levels in
subjects on maintenance immunosuppression and immunosuppression at
12 months.
| A, Mean trough
tacrolimus levels in subjects on maintenance immunosuppression
(ng/ml) |
|---|
|
|---|
| Post-operative
day | Group 1 (n=67) | Group 2 (n=64) | P-value |
|---|
| 7 | 6.9±2.8 | 6.8±3.3 | 0.255 |
| 30 | 9.9±3.7 | 9.7±3.7 | 0.397 |
| 90 | 7.1±2.0 | 7.4±2.3 | 0.196 |
| 360 | 6.8±1.6 | 6.9±1.9 | 0.175 |
|
| B,
Immunosuppressive drug use at 12 months |
|
| Regimen | Group 1
(n=67) | Group 2
(n=64) | P-value |
|
| TMP | 65 | 62 | 0.645 |
| CMP | 2 | 2 |
|
Comparison of endpoints between the
two dose groups
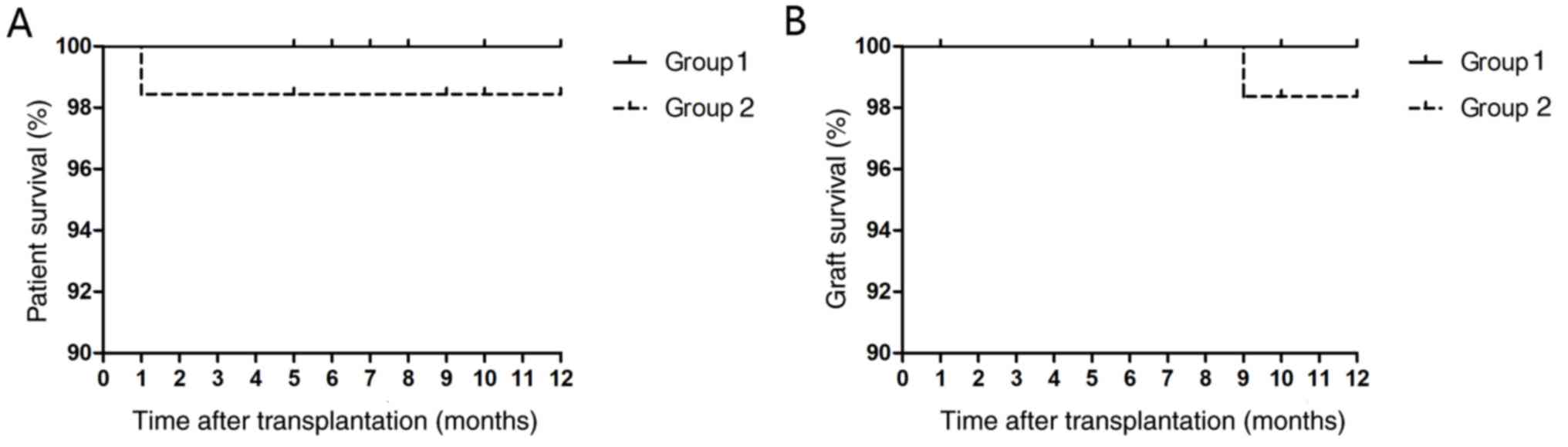
There was no significant difference with regard to
overall patient and graft survival between the 2 groups. At 12
months after transplantation, all patients in group 1 were alive,
whereas 98.4% of patients were alive in group 2 (P=0.306; Fig. 3A). One patient from group 2 died
during the follow-up period due to pulmonary infection. Graft
survival was 100 and 98.4% in group 1 and 2, respectively (P=0.374;
Fig. 3B). Allograft loss occurred in
1 patient from group 2 during follow-up due to T cell-mediated
acute rejection. There was no difference regarding creatinine-based
graft function between groups 1 and 2 (1.23 vs. 1.19 mg/dl,
P=0.165; Table II) or the primary
endpoint BCAR at 12 months between the two groups. The cumulative
ATG-F dose did not influence the rates of BCAR within the first 12
months after transplantation (Table
IV).
| Table IV.Rates of BCAR at 12 months. |
Table IV.
Rates of BCAR at 12 months.
| BCAR grade (n,
%) | Group 1 (n=67) | Group 2 (n=64) | P-value |
|---|
| ≥1A | 5 (7.4) | 3 (4.7) | 0.766 |
| 1 | 4 (6.0) | 2 (3.1) | 0.718 |
| 2 | 1 (1.5) | 1 (1.6) | 0.496 |
Comparison of side effects between the
two dose groups
Regarding adverse effects, no differences in CMV
infection rates (60.5 vs. 66.6%, P=0.560), CMV-associated diseases
(7.4 vs. 7.8%; P=0.800) or BKVN (1.6 vs. 3.0%, P=0.968) were
observed between groups 1 and 2. Group 1 had a lower incidence of
BK viremia (7.5 vs. 23.3%, P=0.022) and BK viruria (50.0 vs. 76.7%,
P=0.023) than group 2. The overall incidence of infection (26.9 vs.
50.0%, P=0.006) and urinary tract infection (7.5 vs. 20.3%,
P=0.033) within 12 months was significantly lower in group 1 than
in group 2. In addition, the incidence of pneumonia within 12
months was similar in groups 1 and 2 (10.4 vs. 20.3%, P=0.117).
Similarly, the incidence of anemia, lymphopenia, thrombocytopenia
and leukopenia did not differ between the two groups (Fig. 4). Induction using ATG-F depleted
circulating lymphocytes to <500 cells/mm3, and
lymphocyte depletion persisted until POD 90 in 3.2% of patients.
However, the degree and the duration of lymphopenia did not differ
between the two groups.
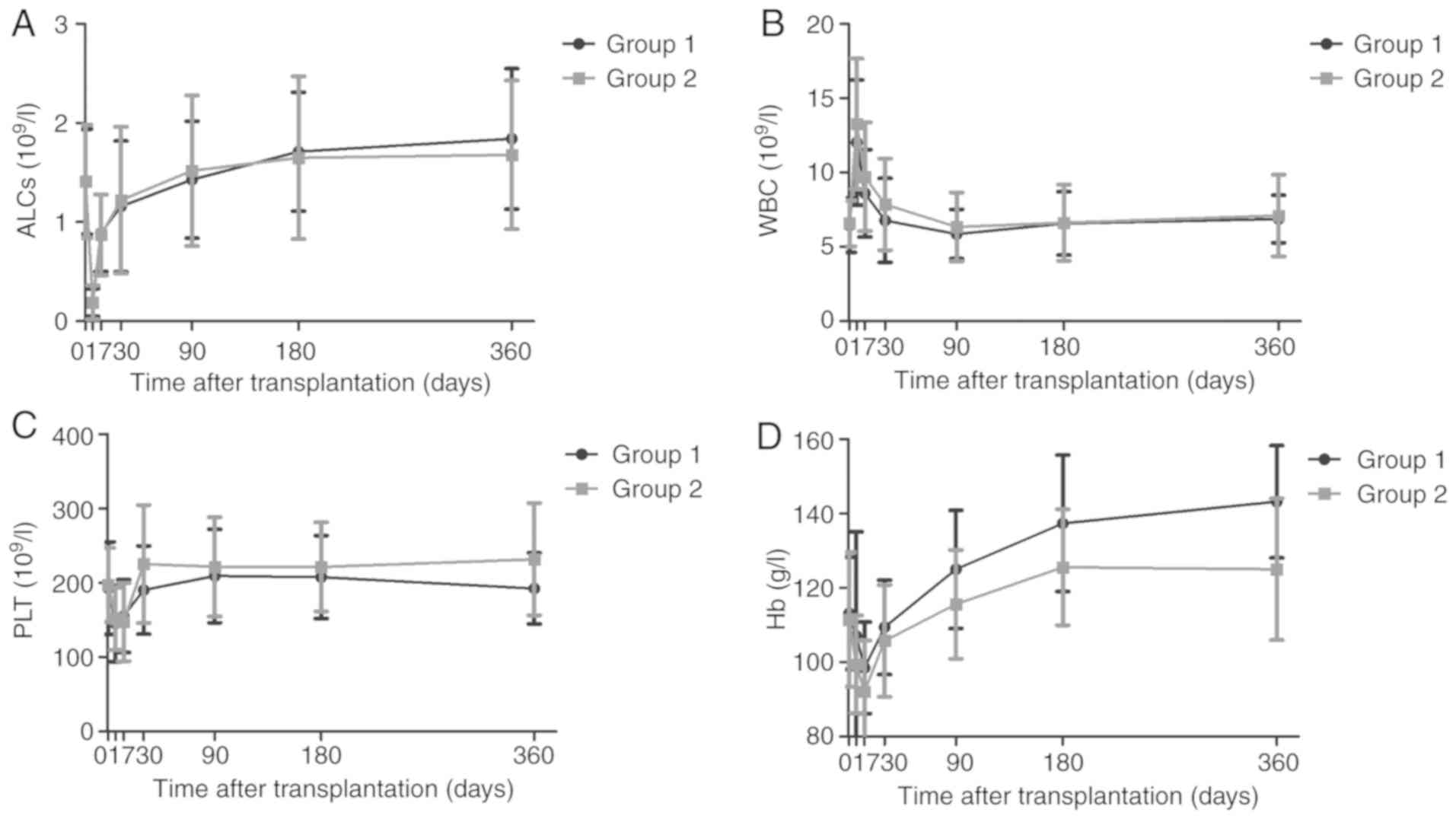 | Figure 4.Hematologic effects of ATG-F induction
following renal transplantation. (A) ALC, (B) total WBC count, (C)
PTL counts and (D) Hb. The Student's t-test was used to analyze the
differences in ALC, WBCs, PTLs and Hb levels. Group 1, <7 mg/kg
ATG-F; group 2, ≥7 mg/kg ATG-F. ATG-F, anti-T-lymphocyte
globulin-Fresenius; ALC, absolute lymphocyte count; WBC, white
blood cell; PLT, platelet; Hb, hemoglobin. |
Discussion
The dose of ATG-F used for induction in renal
transplantation that is able to provide adequate protection against
acute rejection with a low incidence of complications is a subject
under intense investigation. The present results provide additional
evidence regarding weight-based dosing strategies of ATG-F
induction in adult patients receiving renal transplantation with
moderate immunologic risk.
The total ATG-F dosage for induction therapy was
relatively constant for all patients at the Affiliated Hospital of
Qingdao University. The mean ATG-F dosage was calculated using
total dosages divided by the mean body weight. As a result, the
mean ATG-F dosage was lower in patients with higher body weight. In
the present study, transplant recipients were effectively protected
from acute rejection based on ATG-F induction using a cumulative
dose of <7 mg/kg in combination with a tacrolimus-based
steroid-containing triple maintenance immunosuppression. The mean
ATG-F dose in the study participants was 7.05±1.54 mg/kg. Overall
patient survival and death-censored graft survival at 12 months
were 99.2%, whereas the incidence of BCAR ≥1A at 12 months was only
6.1% (8/131). The present results clearly indicate that an
induction regimen consisting of a lower ATG-F dose did not increase
the risk of acute rejection.
Kaden et al (10,11)
indicated that a single pre-operative ATG bolus (ATG-F at 9 mg/kg)
for prophylaxis against rejection induced a drastic reduction in
T-cell counts that lasted for at least 5 days, and this regimen
resulted in a lower risk of rejection compared with that in graft
recipients receiving a regimen of triple immunosuppressants only.
Yussim and Shapira (12) reported a
higher acute rejection rate when graft recipients were given the
same dose of ATG-F and a triple maintenance immunosuppression
regimen consisting of a calcineurin inhibitor, an
anti-proliferative agent and steroids. Similarly, Samsel et
al (13) studied the effect of
high-dose ATG bolus administration on revascularization among renal
graft recipients receiving a triple maintenance immunosuppression
regimen consisting of steroids, mycophenolate mofetil (converted to
azathioprine 4 months later) and cyclosporine. The incidence of
acute rejection at 12 months in that study was 22.5%. Earlier
studies also examined the efficacy of different ATG-F doses in
combination with a triple maintenance immunosuppression regimen in
these patients. Chen et al (8) compared the efficacy and safety between
rabbit anti-thymocyte globulin and anti-T lymphocyte globulin in
renal transplant patients receiving allografts from donors who had
suffered cardiac death, and indicated a higher rate of acute
rejection (19.4%) but similar 1-year graft (97%) and patient
survival (100%) in those receiving ATG-F compared with those
determined in the present study. Shang et al (14) indicated that the rate of acute
rejection at 12 months was 15.4% but the 1-year patient and graft
survival was 94.9% among recipients who received ATG-F 1.5 mg/kg
daily for 4 days in combination with a standard triple
immunosuppression regimen. In that study, the incidence of
post-operative infection was 35.9% (14).
The results of the present study indicated that
differences in the dose of ATG-F were not associated with changes
in the risk of opportunistic infections, hematologic toxicities or
the duration of lymphopenia. A total of 10 patients developed
CMV-associated diseases, including diarrhea, abdominal pain or
fever, and all had good outcomes. In China, CMV is an endemic
disease and most individuals are positive for CMV IgG. Considering
the fact that CMV-associated pneumonia is rare at our institute,
preemptive therapy for CMV instead of routine prophylaxis with
valgancyclovir or ganciclovir was preferred for all recipients,
although all patients tested positive for CMV IgG.
ATG-F has been widely used in the induction phase of
solid-organ transplantation for decades, but the optimal dosage and
duration remain elusive. Most existing studies have used rabbit
ATG, a drug that completely differs from ATG-F with regard to the
production process, usage, dosage and treatment efficacy. A number
of studies used ATG-F as the induction regimen and a single ATG
bolus (9 mg/kg) was the most common approach (10,11).
Although the present study was retrospective, a comparison group
was present, and important results regarding the optimal dosage and
outcomes of ATG-F were obtained.
Acute rejection remains one of the major causes of
graft loss after solid organ transplantation (15). The proliferation of leukocytes is one
of the underlying mechanisms that increase acute rejection after
initial reperfusion injury (16).
ATGs are immunosuppressive agents widely used in the induction of
immunosuppression after renal transplantation. The efficacy of ATG
preparations relies on its potent capacity to deplete T lymphocytes
of the graft, thereby preventing or treating episodes of acute
rejection in transplantation (3). In
the present study, patients from the low-dose group exhibited a
similar degree of lymphocyte depletion compared with those in the
high-dose group. In addition, the incidence of acute rejection did
not differ between the two groups.
The present study is limited by its retrospective
design and its non-randomized single-center nature. Confounding
factors, including adherence to the maintenance immunosuppression
regimen or adjustment of mycophenolate dose, were not collected for
analysis. Recipients at the highest immunologic risk were excluded
from the present study, including those who were ABO incompatible,
had a positive cross-match result and those who received
desensitization or steroid avoidance. The results of the present
study suggested that a modest reduction in the ATG-F dose for
induction is associated with a lower risk of infection and does not
increase the risk of acute rejection when used in combination with
tacrolimus-based steroid-containing triple maintenance
immunosuppression in graft recipients with low immunologic
risk.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YXC, HYW and ZD conceived and designed the study;
JLJ, SJL and YWC collected data; XXS, QHW and TH analyzed and
interpreted the data; YXC drafted the manuscript; ZD and HYW
revised the manuscript; ZD had primary responsibility for the final
content. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
the Affiliated Hospital of Qingdao University (Qingdao, China; no.
QYFY WZLL 22519). All procedures involving human participants were
in accordance with the ethical standards of the institutional and
national research committee and with the 1964 Helsinki Declaration
and its later amendments or comparable ethics standards. Written
informed consent was obtained from all individual participants
included in this study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Yilmaz M, Sezer TO, Kir O, Öztürk A,
Hoşcoşkun C and Töz H: Use of ATG-fresenius as an induction agent
in deceased-donor kidney transplantation. Transplant Proc.
49:486–489. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pennington CA, Tischer SM, Lee E, Lee S,
Sindelar J Jr and Park JM: Evaluation of a weight-based rabbit
anti-thymocyte globulin induction dosing regimen for kidney
transplant recipients. Pharmacotherapy. 35:748–754. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Beiras-Fernandez A, Thein E and Hammer C:
Induction of immunosuppression with polyclonal antithymocyte
globulins: An overview. Exp Clin Transplant. 1:79–84.
2003.PubMed/NCBI
|
|
4
|
Morton RL, Howard K, Webster AC, Wong G
and Craig JC: The cost-effectiveness of induction immunosuppression
in kidney transplantation. Nephrol Dial Transplant. 24:2258–2269.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kaden J, Strobelt V and May G: Short and
long-term results after pretransplant high-dose single
ATG-fresenius bolus in cadaveric kidney transplantation. Transplant
Proc. 30:4011–4014. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kaden J, Völp A and Wesslau C: High graft
protection and low incidences of infections, malignancies and other
adverse effects with intra-operative high dose ATG-induction: A
single centre cohort study of 760 cases. Ann Transplant. 18:9–22.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Meier-Kriesche HU, Arndorfer JA and Kaplan
B: Association of antibody induction with short- and long-term
cause-specific mortality in renal transplant recipients. J Am Soc
Nephrol. 13:769–772. 2002.PubMed/NCBI
|
|
8
|
Chen GD, Lai XQ, Ko DS, Qiu J, Wang CX,
Han M, Li J, Huang G, He XS and Chen LZ: Comparison of efficacy and
safety between rabbit anti-thymocyte globulin and anti-T lymphocyte
globulin in kidney transplantation from donation after cardiac
death: A retrospective cohort study. Nephrology (Carlton).
20:539–543. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Solez K, Colvin RB, Racusen LC, Haas M,
Sis B, Mengel M, Halloran PF, Baldwin W, Banfi G, Collins AB, et
al: Banff 07 classification of renal allograft pathology: Updates
and future directions. Am J Transplant. 8:753–760. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kaden J, May G, Müller P, Groth J,
Strobelt V, Eger E and Wohlfahrt L: Intraoperative high-dose
anti-T-lymphocyte globulin bolus in addition to triple-drug therapy
improves kidney graft survival. Transplant Proc. 27:1060–1061.
1995.PubMed/NCBI
|
|
11
|
Kaden J, May G, Strobelt V, Groth J and
Müller P: Intraoperative T-cell depletion prior to completion of
anastomoses by high-dose single ATG bolus as a new approach to
improve long-term results after kidney transplantation. Transplant
Proc. 29:344–347. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yussim A and Shapira Z: Single-bolus
high-dose ATG for prophylaxis of rejection in renal transplantation
- a prospective, randomized study. Transpl Int. 13 (Suppl
1):S293–S294. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Samsel R, Pliszczyński J, Chmura A,
Korczak G, Włodarczyk Z, Cieciura T, Lagiewska B, Glyda M, Wyzgal
J, Paczek L, et al: Safety and efficacy of high dose ATG bolus
administration on rewascularization in kidney graft patients - long
term results. Ann Transplant. 13:32–39. 2008.PubMed/NCBI
|
|
14
|
Shang W, Feng G, Gao S, Wang Z, Pang X, Li
J, Liu L, Feng Y, Xie H, Zhang S, et al: Reduced ATG-F dosage for
induction in pediatric renal transplantation: A single-center
experience. Pediatr Transplant. 18:240–245. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Brennan DC, Daller JA, Lake KD, Cibrik D
and Del Castillo D; Thymoglobulin Induction Study Group, : Rabbit
antithymocyte globulin versus basiliximab in renal transplantation.
N Engl J Med. 355:1967–1977. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Beiras-Fernandez A, Chappell D, Hammer C,
Beiras A, Reichart B and Thein E: Impact of polyclonal
anti-thymocyte globulins on the expression of adhesion and
inflammation molecules after ischemia-reperfusion injury. Transpl
Immunol. 20:224–228. 2009. View Article : Google Scholar : PubMed/NCBI
|