Introduction
Among the developments in surgical endourology
techniques in the past three decades, percutaneous nephrolithotomy
(PCNL) has become a standard treatment strategy with minimal
invasiveness for the treatment of large renal stones (1,2).
Conventionally, creating the nephrostomy tract is a fundamental
process in this technique. At present, there are four major
dilation methods for PCNL: Fascial Amplatz dilation (AD), metal
telescopic Alken type dilation (MTD), balloon dilation (BD) and
one-shot dilation (OSD). BD is generally considered as the most
modern and safest technique. It has advantages of reduced
complication rates and shorter durations of X-ray exposure
(3-5),
but its application is limited due to high cost. AD and MTD are
inexpensive, but longer durations of application and X-ray exposure
are required. The OSD technique, which was first proposed by
Frattini et al (6), may
achieve the same effects compared with the other three dilation
methods (7-13);
however, OSD may cause parenchymal damage (14). A previous meta-analysis compared the
four dilation methods (15), but
only four randomized clinical trials (RCTs) were included and three
combinations of tract dilation methods were analyzed. Therefore,
the most effective method for the selection of tract dilation
remains controversial; surgeons may select different methods
depending on their familiarity or experience with certain
techniques. Thus, a meta-analysis based on recent studies was
performed to systematically assess the effectiveness and safety of
each tract dilation method.
Materials and methods
Study search and selection
The PubMed, EMBASE, Web of Science and Cochrane
library databases were searched for relevant studies from database
inception to 1 April 2019. Analysis was performed using the
following MeSH key words: (‘percutaneous nephrolithotomy’,
‘percutaneous lithotripsy’, ‘PCNL’, ‘PNL’ or ‘PCN’) AND (‘one
shot’, ‘single step’, ‘one stage’, ‘one-shot’, ‘single-step’,
‘one-stage’, ‘tract dilators’, ‘AD’, ‘MTD’ or ‘BD’). The search was
restricted to RCTs published in English. The present study was
prepared based on the Cochrane Handbook for Systematic Reviews of
Interventions (16) and presented
based on the Preferred Reporting Items for Systematic Reviews and
Meta-analyses guidelines (17).
Inclusion and exclusion criteria
RCTs were selected for analysis according to the
following inclusion criteria: i) RCTs that compared ≥2 tract
dilation techniques for PCNL; ii) RCTs that included patients aged
>18 years; iii) the baseline characteristics were matched
between groups; iv) RCTs were published in English and their full
texts were available; v) at least one of the following types of
data was available: Hemoglobin decrease, X-ray exposure time,
stone-free rate, operation time, length of hospital stay and blood
transfusion rate. The exclusion criteria were as follows: i) RCTs
that were not comparative studies; ii) the full texts were not
accessible; and iii) RCTs that included patients aged <18
years.
Risk of bias assessments
The quality of the RCTs was assessed by two
independent researchers using the Cochrane risk-of-bias criteria
(16). Bias was evaluated based on
the criteria of random sequence generation, allocation concealment,
blinding of participants and personnel, blinding of outcome
assessment, incomplete outcome data, selective reporting and other
bias for each RCT, which allowed for grading of RCTs as low-risk,
high-risk or unclear risk of bias. Providing the randomized
sequence generation or allocation concealment indicated high risk
of bias, the RCT was regarded as being of low quality, whereas if
these factors were considered to be of low or unclear risk of bias,
then the RCT would be regarded as being of high quality. In
addition, intermediate risk of bias suggested that an RCT was of
moderate quality.
Data extraction
The following data were extracted by two independent
researchers (HLH and YCL): Name of first author, publication year,
participant characteristics, stone burden, operational history,
tract methods, hemoglobin decrease, X-ray exposure time, stone-free
rate, operation time, length of hospital stay, blood transfusion
rate and complications. Disagreements were resolved by consensus.
If any data were missing, attempts were made to contact the
authors. The X-ray exposure time was the primary outcome, while the
stone-free rate, blood transfusion rate, hemoglobin reduction and
complications were denoted as the secondary outcomes.
Statistical analysis
The present study employed the Mantel-Haenszel
statistical method to calculate risk ratios (RRs) and mean
difference (MD) with 95% confidence intervals (CIs) for dichotomous
data and continuous data to assess the overall outcomes of the four
tract dilation methods for PCNL procedures. A χ2 test
(P=0.05) and the I2 statistic were used to evaluate
statistical heterogeneity among the studies by two independent
researchers. P<0.05 was considered to indicate a statistically
significant difference and I2>50% was considered to
indicate heterogeneity. Fixed-effects and random-effect models were
generated to analyze homogeneous and heterogeneous data,
respectively. Sensitivity analysis was performed by excluding
trials with low quality or abnormal data. Possible publication bias
was assessed by generating funnel plots for the studies. All
meta-analyses were performed using RevMan version 5.2.
Results
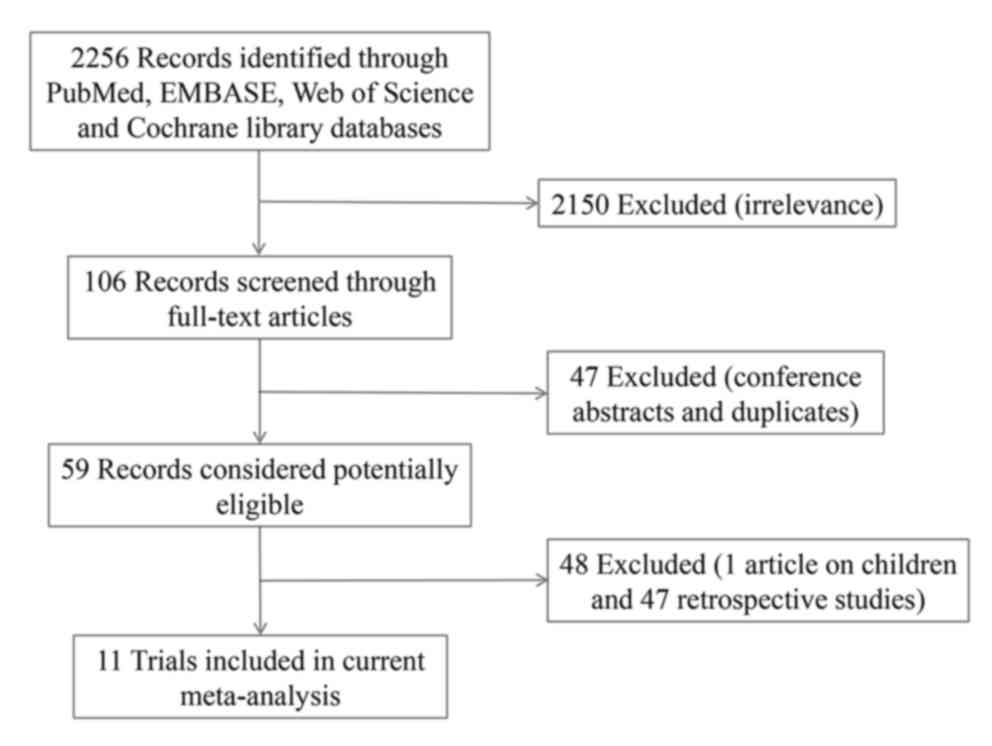
Eligible studies and
characteristics
A total of 110 potentially eligible reports were
identified from the databases following screening of the titles and
abstracts; 85 studies were excluded, as they were duplicates (37
articles) or retrospective trials (48 articles). In addition, 14
articles (13 conference abstracts and one study on pediatric
patients) were excluded from the remaining 25 RCTs during the
review of full-text articles based on the inclusion and exclusion
criteria. Finally, 11 RCTs, comprising 1,415 cases, were included
in the present meta-analysis (Fig.
1). Of note, six studies compared MTD with OSD (8-12,14),
one article compared MTD, OSD and BD (6); one compared MTD, OSD, BD and AD
(13), two studies compared AD with
OSD (18,19), and one article compared MTD, BD and
AD (20). The baseline
characteristics and quality ratings of the studies included are
presented in Table I.
 | Table IBaseline characteristics of the
studies included. |
Table I
Baseline characteristics of the
studies included.
| First author | Year | Design | Intervention | M/Fa | Mean
agea (years) | Stone burden | Stone
sitea (R/L) | Sheath size
(F) | Quality | (Refs.) |
|---|
| Nour | 2014 | RCT | MTD/OSD | (16/9)/(17/7) | 38.2/48.3 | 30.2±6.9/30.7±7.2
mm |
(15/10)/(14/10) | 30/30 | High | (8) |
| Aminsharifi | 2011 | RCT | MTD/OSD | (9/10)/(19/10) | 42.5/44.1 | 30.9±12.9/26.9±9.7
mm | (8/11)/(11/18) | 30/30 | Moderate | (14) |
| Khorrami | 2017 | RCT | MTD/OSD |
(74/46)/(76/44) | 44.4/44.6 | NA/NA | NA/NA | 28/28 | Low | (9) |
| Amirhassani | 2014 | RCT | MTD/OSD |
(27/23)/(28/22) | 45.6/44.8 | NA/NA | NA/NA |
(28/30)/(28/30) | Moderate | (10) |
| Falahatkar | 2009 | RCT | MTD/OSD |
(62/50)/(56/46) | 51/57 | 3.4±1.2/3.9±1.6
mm |
(68/44)/(52/50) | 30/30 | Moderate | (11) |
| Amjadi | 2008 | RCT | MTD/OSD | (12/2)/(10/7) | 44/42 | 3.2±1.1/3.7±1.0
cm | (6/8)/(8/9) | 28/28 | Moderate | (12) |
| Frattini | 2001 | RCT | MTD/OSD/BD |
(15/12)/(17/9)/(8/17) | 54/59/52 |
2.9±0.9/2.3±0.7/2.1±0.5 cm |
(14/13)/(15/11)/(11/14) | 34/34/34 | Moderate | (6) |
| Srivastava | 2017 | RCT | MTD/OSD/BD/AD |
(62/58)/(59/61)/(59/59)/(60/59) |
40.1/38.9/42.1/41.2 |
29.7±5.2/30.5±3.9/31.1±4.0/30.1±4.1
mm2 |
(55/65)/(56/64)/(56/62)/(59/60) | 30/30/30/30/ | High | (13) |
| Thiruvarul | 2015 | RCT | AD/OSD |
(18/12)/(14/16) | 40.5/43.3 | NA/NA |
(17/13)/(11/19) | 30/30/ | Moderate | (18) |
| Wen | 2007 | RCT | AD/OSD | NA/NA | 44.6/45.2 | NA/NA | NA/NA | NA/NA | Moderate | (19) |
| Unsal | 2010 | RCT | BD/MTD/AD |
(8/4)/(11/3)/(18/6) | 42.4/45.5/43.2 |
3.5±2.7/4.1±5.2/3.8±4.3 cm |
(6/6)/(6/8)/(10/14) |
(28/30)/(28/30)/(28/30) | Moderate | (20) |
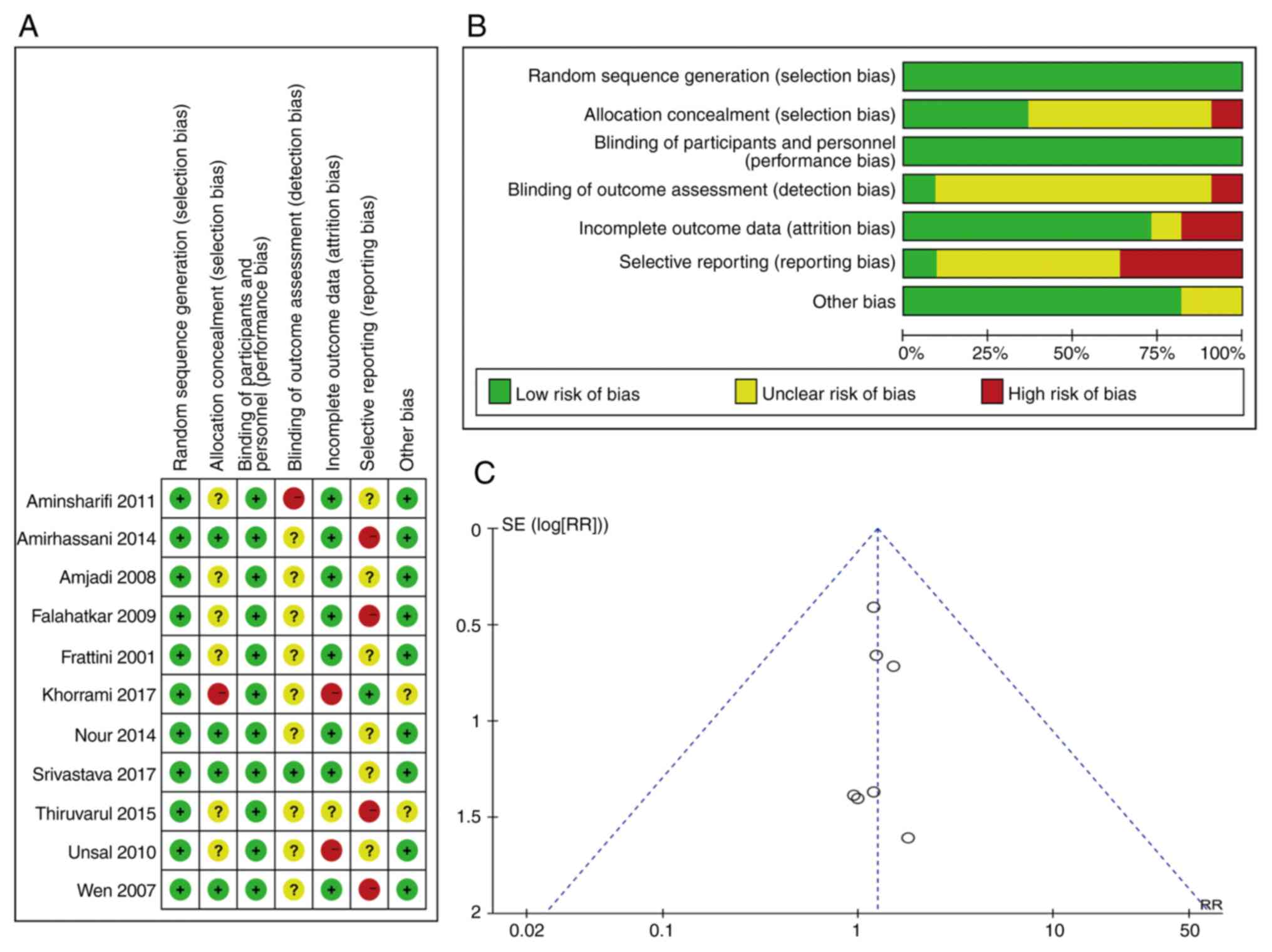
Quality assessment and publication
bias
Based on the Cochrane risk-of-bias criteria
(16), two articles were graded as
being of high quality and eight articles were graded as being of
moderate quality, while one article was of low quality. The details
of the quality assessment are presented in Fig. 2A and B. A lack of publication bias was
demonstrated via the funnel plots for hemoglobin decrease, and the
transfusion rate, successful dilation rate, one access rate and
stone-free rate. The publication bias of the transfusion rate was
also determined (Fig. 2C; data not
shown for other items).
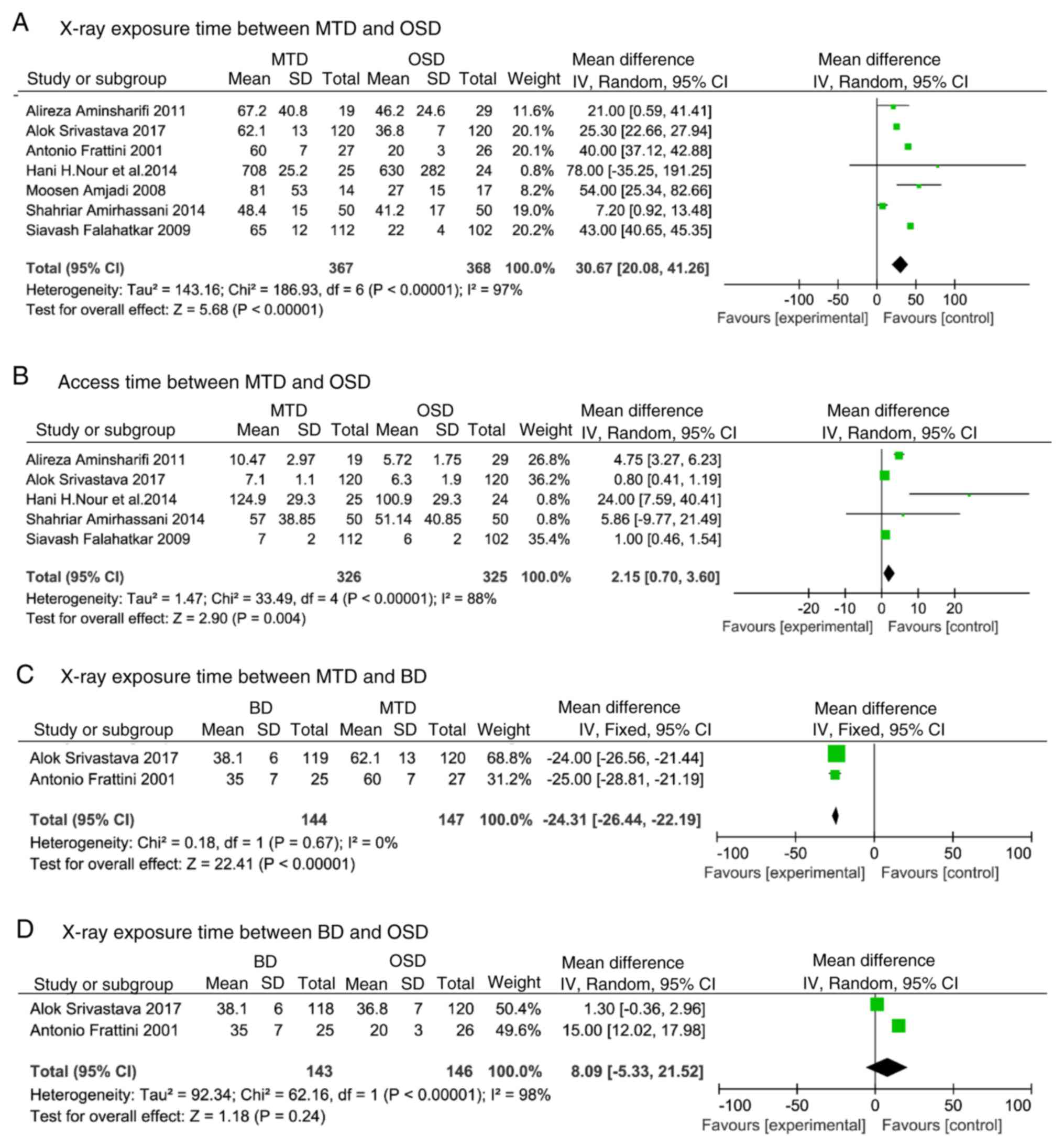
X-ray exposure time and access
time
A total of eight studies compared MTD with OSD. The
data were pooled for analysis with the random-effect model due to
the significant heterogeneity among these studies (P<0.001;
I2=97%). Significantly longer X-ray exposure times for
tract creation were determined for MTD compared with OSD (WMD,
30.67; 95%CI, 20.08-41.26; P<0.001; Fig. 3A). Sensitivity analysis after
exclusion of the trial by Nour et al (8) due to the inaccuracy of the definition
of the X-ray exposure time and the access time compared to other
studies revealed the same results [random-effects model; WMD,
30.27; 95%CI, 19.63-40.92; P<0.001; I2=97% (result
not shown)]. Similarly, for access time, heterogeneity was high
(P<0.001; I2=88%), revealing that the access time for
MTD was longer compared with that for OSD (random-effects model;
WMD, 2.15; 95%CI, 0.70-3.60; P<0.004; Fig. 3B). Following exclusion of the trial
by Nour et al (8), the same
results [random-effects model; WMD, 1.93; 95%CI, 0.62-3.23;
P<0.001; I2=88% (result not shown)] were obtained.
Heterogeneity of X-ray exposure times was low (P<0.67;
I2=0%), revealing that the X-ray exposure time for MTD
was longer compared with that for OSD [fixed-effects model; WMD,
-24.31; 95%CI, -(26.44-22.19); P<0.001; Fig. 3C], but the
heterogeneity of X-ray exposure time was high (P<0.001;
I2=98%) between BD and OSD. Similar X-ray exposure time
was observed between these groups (random-effects model; WMD, 8.09;
95%CI, -5.33-21.52; P<0.24; Fig.
3D).
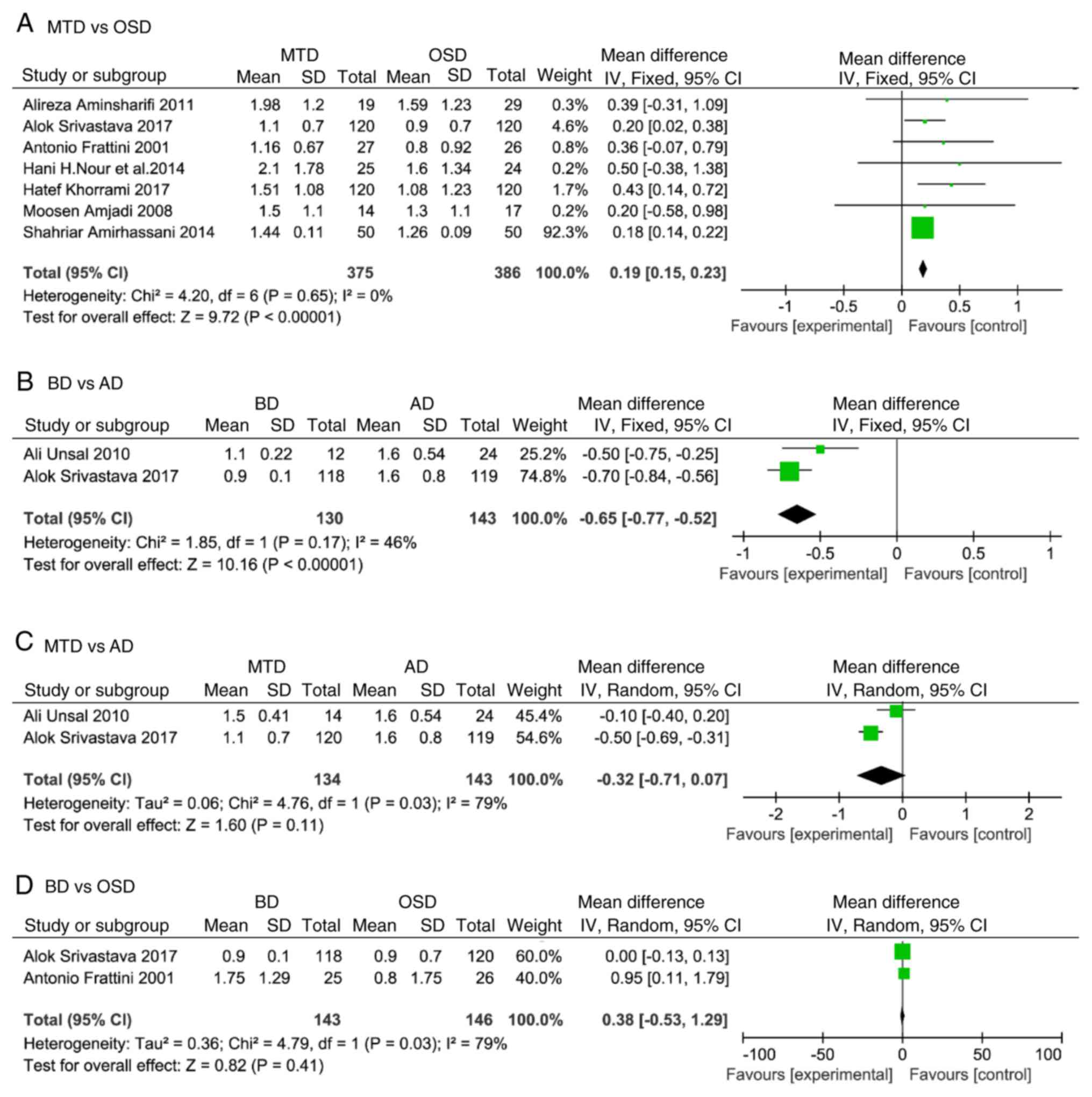
Hemoglobin decrease
A total of eight articles compared MTD with OSD. The
data were pooled for analysis with fixed-effect models (P=0.65;
I2=0%). A significant reduction in hemoglobin was
determined for the MTD group compared with that in the OSD group
(WMD, 0.19; 95%CI, 0.15-0.23; P<0.001; Fig. 4A). In addition, two studies compared
BD and AD. The heterogeneity of hemoglobin decrease was low
(P=0.17; I2=46%) and there was a significantly smaller
decrease in hemoglobin in the BD group compared with that in the AD
group [fixed-effects model; WMD, -0.65; 95%CI, -(0.77-0.52);
P<0.001; Fig. 4B]. The heterogeneity of hemoglobin decrease was
high (P<0.03; I2=79%) between MTD and AD. Similar
hemoglobin decrease was determined between these groups
(random-effects model; WMD, -0.32; 95% CI, -0.71-0.07; P=0.11;
Fig. 4C). The heterogeneity of
hemoglobin decrease was high (P<0.03; I2=79%) and no
statistically significant difference was determined in hemoglobin
decrease between BD and OSD (random-effects model; WMD, 0.38;
95%CI, -0.53-1.29; P=0.41; Fig.
4D).
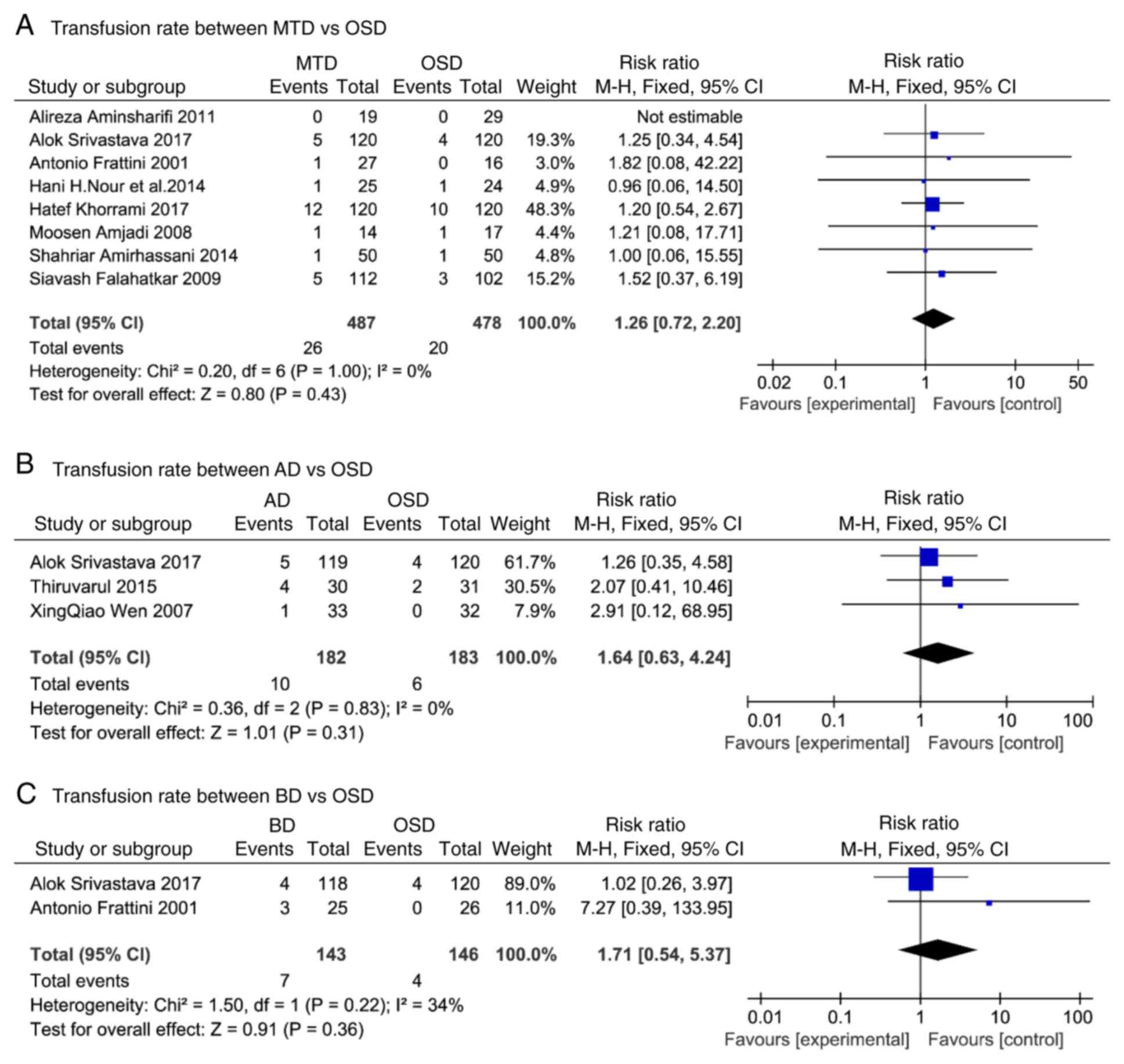
Transfusion rate
The heterogeneity of transfusion rate between MTD
and OSD (P=1.00; I2=0%), AD and OSD (P=0.83;
I2=0%), and BD and OSD (P=0.22; I2=34%) was
low, revealing that MTD (fixed-effects model; RR, 1.26; 95%CI,
0.72-2.20; P=0.43; Fig. 5A), AD
(fixed-effects model; RR, 1.64; 95%CI, 0.63-4.24; P=0.31; Fig. 5B) and BD (fixed-effects model; RR,
1.71; 95%CI, 0.54-5.37; P=0.36; Fig.
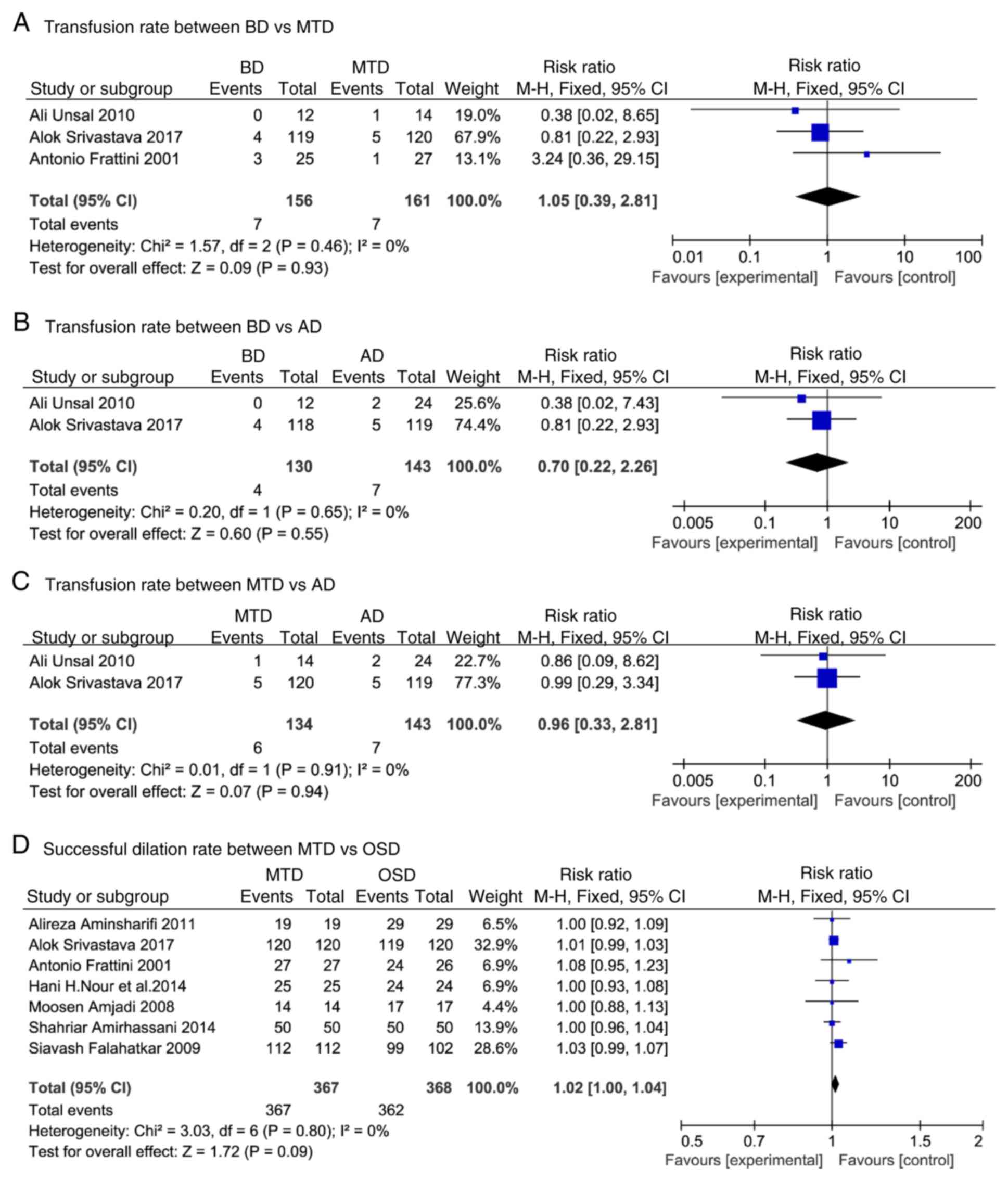
5C) had higher transfusion rates compared with OSD. The
heterogeneity of transfusion rate between BD and MTD (P=0.46;
I2=0%), BD and AD (P=0.65; I2=0%), and MTD
and AD (P=0.91; I2=0%) was low. The transfusion rate was
similar between BD and MTD (fixed-effects model; RR, 1.05; 95%CI,
0.39-2.81; P=0.93; Fig. 6A), BD and
AD (fixed-effects model; RR, 0.70; 95%CI, 0.22-2.26; P=0.55;
Fig. 6B), and MTD and AD
(fixed-effects model; RR, 0.96; 95%CI, 0.33-2.81; P=0.94; Fig. 6C).
Successful dilation and one-access
rates
The heterogeneity of successful dilation rate was
low (P=0.80; I2=0%), revealing that MTD had a markedly
higher successful dilation rate compared with OSD (fixed-effect
model; RR, 1.02; 95%CI, 1.00-1.04; P=0.09; Fig. 6D); however, no statistical
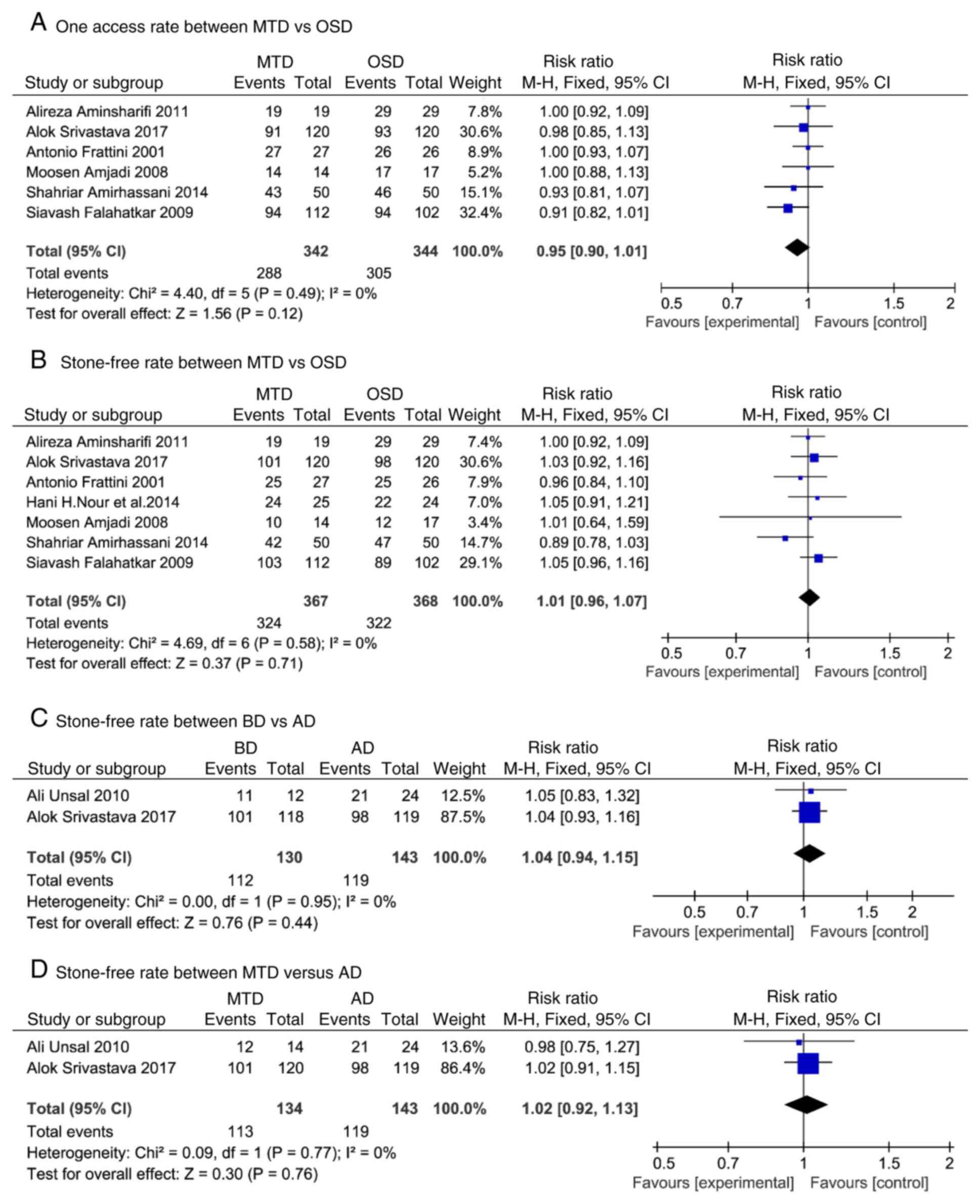
significance was obtained. The heterogeneity of one-access rate was
low (P=0.49; I2=0%), and the one-access rate was similar
between MTD and OSD (fixed-effects model; RR, 0.95; 95%CI,
0.90-1.01; P=0.12; Fig. 7A).
Stone-free rate
The heterogeneity of stone-free rate between MTD and
OSD (P=0.58; I2=0%), BD and AD (P=0.95;
I2=0%), and MTD and AD (P=0.77; I2=0%) was
low. No statistically significant differences were observed in the
stone-free rate between MTD and OSD (fixed-effects model; RR, 1.01;
95%CI, 0.96-1.07; P=0.71; Fig. 7B),
BD and AD (fixed-effects model; RR, 1.04; 95%CI, 0.94-1.15; P=0.44;
Fig. 7C), and MTD and AD
(fixed-effects model; RR, 1.02; 95%CI, 0.9-1.13; P=0.76;
I2=0%; Fig. 7D).
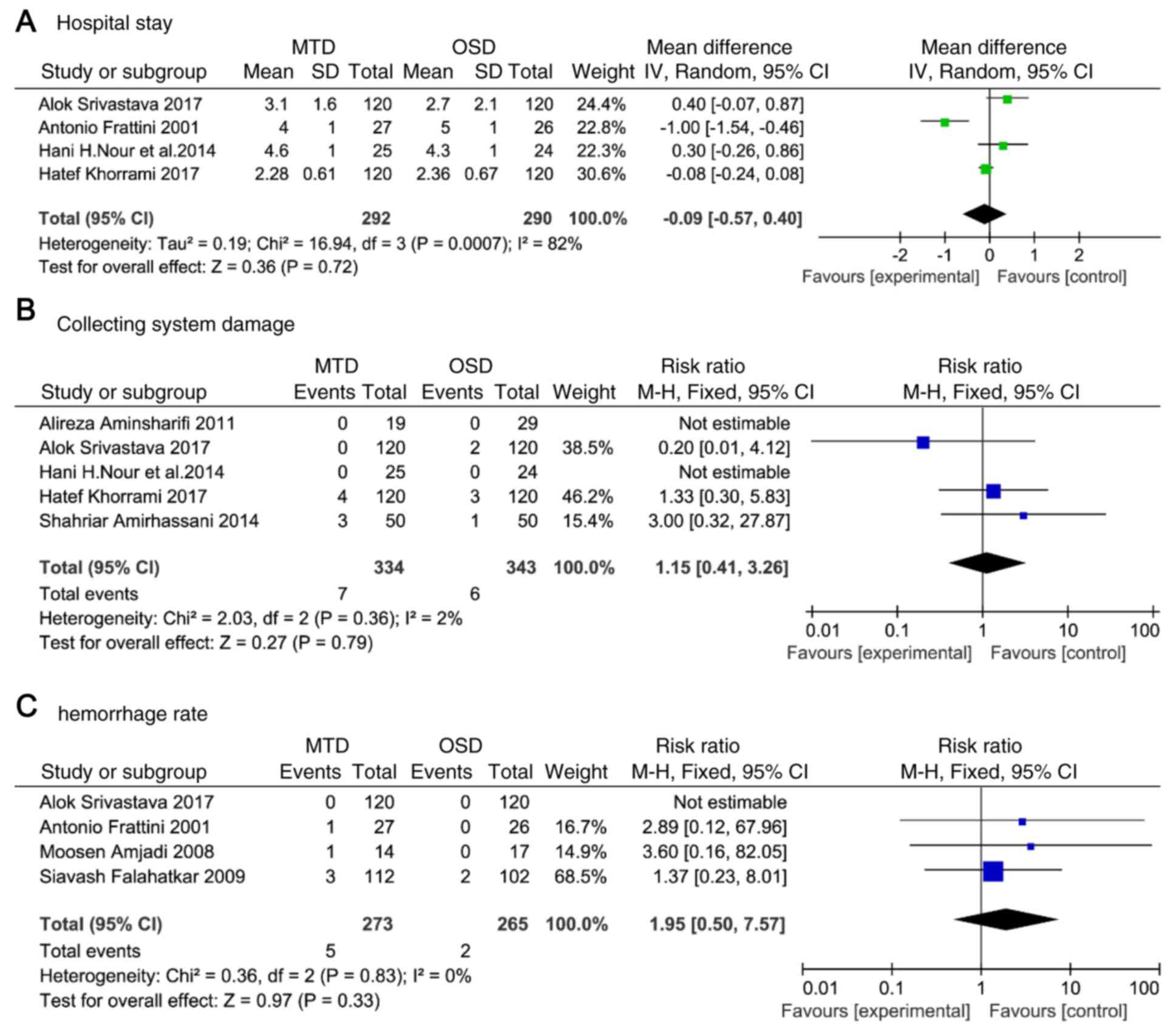
Hospital stay
A significant degree of heterogeneity between MTD
and OSD was determined (P<0.001, I2=82%), and the
data were pooled for analysis with a random-effects model. Similar
lengths of hospital stay were determined between these groups
(random-effects model; WMD, -0.09; 95%CI, -0.57-0.40; P<0.72;
Fig. 8A).
Collecting-system damage and
hemorrhage rate
The heterogeneity of collecting system damage was
low (P=0.36; I2=2%), no statistically significant
differences were reported in damage to the collecting system
between MTD and OSD (fixed-effects model; RR, 1.15; 95%CI,
0.41-3.26; P=0.79; Fig. 8B). The
heterogeneity of hemorrhage rate was low (P=0.83;
I2=0%), revealing that a markedly increased hemorrhage
rate was reported for MTD compared with OSD (fixed-effects model;
RR, 1.95; 95CI%, 0.50-7.57; P=0.33; Fig.
8C).
Discussion
Tract creation and dilation are fundamental steps in
percutaneous renal surgery and are required for three traditional
types of dilation, including MTD, AD and BD (21-23).
OSD was first introduced by Frattini et al (6); several studies have investigated the
safety and effectiveness of OSD compared with those of other
methods (7-13).
Numerous RCTs on these methods have been reported and a previous
meta-analysis has been published by Cao et al (15). Of note, this previous meta-analysis
included only four RCTs and analyzed three combinations of tract
dilation methods without comparing the associated complications.
Therefore, an integrated analysis of the four tract dilation
techniques was required.
The present meta-analysis revealed that OSD was safe
and effective for almost every adult patient, including those who
previously underwent renal surgery. Significant differences were
reported in X-ray exposure time and access time between MTD and
OSD. Sensitivity analysis was performed by excluding a study that
was abnormal due to inaccuracy of the definition of the X-ray
exposure time and the access time, leading to marked differences in
the data from other studies, and the same results were obtained.
The hemoglobin decrease, transfusion rate and hemorrhage rate in
the MTD and OSD groups were also compared, as hemorrhage was
characterized by blood drain within the nephrostomy tube,
intermittent or continuous hematuria or gross hematuria with or
without a decrease in hemoglobin and rarely required blood
transfusion, and these three variables were linked but different.
OSD was determined to significantly decrease the transfusion rate,
hemorrhage rate and the extent of hemoglobin decrease compared with
those of MTD. These results support the results of previous studies
(6,8-14,18-20).
In addition, no statistically significant differences were observed
between the two groups regarding the stone-free rate. By contrast,
Falahatkar et al (11) and
Srivastava et al (13)
reported that OSD required more auxiliary procedures. This may be
due to the higher proportion of complex stones in the OSD; it may
also indicate that OSD has limited efficacy in managing complex
stones. The present meta-analysis revealed that, as compared with
MTD, OSD was associated with a lower rate of complications,
including damage to the collecting system and hemorrhage. These
results indicated that the OSD technique may be widely used;
however, Srivastava et al (13) reported on two patients with minor
pelvic perforations and injuries to the collecting system. These
patients had a similar history of ipsilateral open surgery. OSD
benefits from increased radial force and reduced axial force, yet
the high resistance of fascial dilation requires more radial force,
which may be the cause of complications. In addition, several
studies reported on a number of unsuccessful procedures in patients
who underwent open surgery (6,11,13),
whereas OSD was determined to be as effective as MTD in previously
operated patients (10,12,24,25).
Frattini et al (6) and
Falahatkar et al (11)
suggested that the high resistance of perirenal scar tissue due to
previous kidney surgery, which prevented fascial dilator passage,
or renal supermotility and rotation during dilation, may lead to
avulsion of the entire organ. In the present meta-analysis, the
rates of successful dilation and one access were compared. OSD was
determined to have a markedly lower successful dilation rate.
Advancements in equipment and the experience of surgeons in
employing various techniques may also account for the differences
determined. In addition, Aminsharifi et al (14) demonstrated that OSD caused more
parenchymal damage than MTD. The difference between the two
methods, an insufficient number of patients and inadequate
follow-up time may have influenced the results. Furthermore, it is
uncertain whether the formation of small new scars affects renal
function. Lee and Stoller (26)
suggested that the differences reported may be explained by the
surgeon's familiarity and experience rather than the dilator
systems. The hemoglobin decrease associated with MTD was previously
determined to not be significantly different compared with that
resulting from AD (13,27); however, in the present study, MTD was
reported to lead to a lower hemoglobin decrease compared with AD.
This could be due to trauma as a result of the cycle of insertion
and removal of the dilator in and out of the tract during
sequential exchange, increasing the risk of bleeding. However, the
transfusion rate and stone-free rate were similar between the two
groups. AD and MTD are used to create the tract by using axial and
radial forces, which have a higher chance of successful tract
creation compared with OSD. The spinning movement of the sheath
during tract creation serves an important role in decreasing the
risk of kidney or guidewire shift (28). Thus, these methods, particularly AD,
are frequently used in patients who have previously undergone
kidney surgery. As of the small tip of these dilators, it is easy
to guide along smaller tracts from previous dilations, regardless
of the density of scar tissue (25).
A number of studies reported that BD had reduced X-ray exposure
time and hemoglobin decrease compared with AD and MTD (13,20,29), as
the inflated balloon provides constant pressure and tamponades the
small injured vessels. In addition, BD was previously proposed to
be more likely to fail in patients who underwent kidney surgery
(13,30). This may be due to the low axial force
in BD and the lack of constant dilation. Kijvikai and de la Rosette
(31) reported that BD was not
suitable for complete staghorn calculus. The space between these
stones and the collecting system may be inadequate and the tapered
end of the dilator may create a small tract into the collecting
system or split the calix.
Of note, the present study has certain limitations.
A variety of factors, including the stone burden, body mass index,
hydronephrosis grade or the number of previous surgeries may have
influenced the results; subgroup analyses were not performed due to
limitations of the studies included. In addition, other
complications were not compared, including the presence of pleural
effusion, post-operative urinary tract infections or post-operative
fever due to a lack of data. Furthermore, the heterogeneity of the
data may have affected the results of X-ray exposure time and
access time; the high heterogeneity may have been due to the
different definitions among the studies included. Despite these
limitations, there are certain advantages of the present study
regarding the quality and quantity of articles analyzed, and the
results of comparisons with previous meta-analyses in terms of both
quality and quantity (15), as
results from the present study were more comprehensive.
In the present meta-analysis, OSD was determined to
be a safer method in almost every adult patient, including those
who underwent renal surgery previously, compared to AD and MTD;
however, OSD has a considerable risk of serious complications if
the surgeon is inexperienced. Therefore, the present study proposed
that surgeons with technical expertise in OSD should perform this
procedure. BD was also determined to be more effective and safer
than AD and MTD in patients that had not undergone renal surgery
previously. By contrast, BD is an expensive procedure and
unsuitable for patients with a history of renal surgery. For
patients who have undergone kidney surgery, AD and MTD are safer
methods of dilation. However, additional RCTs are required to
determine the best method for PCNL.
Acknowledgements
Contents of this study were previously presented as
a poster at the 37th World Congress of Endourology (1st November
2019; Abu Dhabi, United Arab Emirates; abstract no. MP23-04).
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
YW performed the statistical analysis and wrote the
manuscript. YX and HLH performed the literature search. HLH and YCL
extracted the data. BLQ performed the quality assessment. YW and YX
performed the meta-analysis and interpreted the results. SGW was a
major contributor in conceiving and designing the manuscript. SGW
also calibrated the final version and revised the manuscript. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Türk C, Petřík A, Sarica K, Seitz C,
Skolarikos A, Straub M and Knoll T: EAU guidelines on diagnosis and
conservative management of urolithiasis. Eur Urol. 69:468–474.
2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Sivalingam S, Al-Essawi T and Hosking D:
Percutaneous nephrolithotomy with retrograde nephrostomy access: A
forgotten technique revisited. J Urol. 189:1753–1756.
2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Handa RK, Matlaga BR, Connors BA, Ying J,
Paterson RF, Kuo RL, Kim SC, Lingeman JE, Evan AP and Willis LR:
Acute effects of percutaneous tract dilation on renal function and
structure. J Endourol. 20:1030–1040. 2006.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Stoller ML, Wolf JS Jr and St Lezin MA:
Estimated blood loss and transfusion rates associated with
percutaneous nephrolithotomy. J Urol. 152:1977–1981.
1994.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Davidoff R and Bellman GC: Influence of
technique of percutaneous tract creation on incidence of renal
hemorrhage. J Urol. 157:1229–1231. 1997.PubMed/NCBI
|
|
6
|
Frattini A, Barbieri A, Salai P, Sebastio
N, Ferretti S, Bergamaschi E and Cortellini P: One shot: A novel
method to dilate the nephrostomy access for percutaneous
lithotripsy. J Endourol. 15:919–923. 2001.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Rusnak B, Castañeda-Zuñiga W, Kotula F,
Herrera M and Amplatz K: An improved dilator system for
percutaneousnephrostomies. Radiology. 144(174)1982.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Nour HH, Kamal AM, Zayed AS, Refaat H,
Badawy MH and El-Leithy TR: Single-step renal dilatation in
percutaneous nephrolithotomy: A prospective randomised study. Arab
J Urol. 12:219–222. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Khorrami MH, Izadpanahi MH, Mohammadi M,
Alizadeh F, Zargham M, Khorrami F and Isfahani FF: Comparison of
two treatment methods ‘one shot’ and ‘sequential’ on reduction the
level of hemoglobin in patients with percutaneous nephrolithotripsy
in Al Zahra hospital in 2012-2013. Adv Biomed Res.
6(84)2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Amirhassani S, Mousavi-Bahar SH, Iloon
Kashkouli A and Torabian S: Comparison of the safety and efficacy
of one-shot and telescopic metal dilatation in percutaneous
nephrolithotomy: A randomized controlled trial. Urolithiasis.
42:269–273. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Falahatkar S, Neiroomand H, Akbarpour M,
Emadi SA and Khaki N: One-shot versus metal telescopic dilation
technique for tract creation in percutaneous nephrolithotomy:
Comparison of safety and efficacy. J Endourol. 23:615–618.
2009.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Amjadi M, Zolfaghari A, Elahian A and
Tavoosi A: Percutaneous nephrolithotomy in patients with previous
open nephrolithotomy: One-shot versus telescopic technique for
tract dilatation. J Endourol. 22:423–425. 2008.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Srivastava A, Singh S, Dhayal IR and Rai
P: A prospective randomized studycomparing the four tract dilation
methods of percutaneous nephrolithotomy. World J Urol. 35:803–807.
2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Aminsharifi A, Alavi M, Sadeghi G, Shakeri
S and Afsar F: Renal parenchymal damage after percutaneous
nephrolithotomy with one-stage tract dilation technique: A
randomized clinical trial. J Endourol. 25:927–931. 2011.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Cao DH, Liu LR, Liu HW and Wei Q: A
comparison among four tract dilation methods of percutaneous
nephrolithotomy: A systematic review and meta-analysis.
Urolithiasis. 41:523–530. 2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Higgins JPT and Green S (eds): Cochrane
Handbook for Systematic Reviews of Interventions. Version 5.1.0
(updated March 2011). The Cochrane Collaboration, 2011. http://www.cochrane-handbook.org.
Accessed November 22, 2017.
|
|
17
|
Liberati A, Altman DG, Tetzlaff J, Mulrow
C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J
and Moher D: The PRISMA statement for reporting systematic reviews
and meta-analyses of studies that evaluate healthcare
interventions: Explanation and elaboration. BMJ.
339(b2700)2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Thiruvarul PV, Periasamy P and Pitchai BK:
Single step vs serial dilatation for tract creation in percutaneous
nephrolithotomy: A randomized controlled trial. J Evolution Med
Dental Sci. 91:15669–15672. 2015.
|
|
19
|
Wen X, Gao X, Li X, Lu M, Cai Y, Qiu J and
Xiao C: One-step percutaneous nephrostomy in patients with a
history of open nephrolithotomy: Comparison with the fascial
dilator system. J Endourol. 21:1281–1285. 2007.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Unsal A, Koca G, Reşorlu B, Bayindir M and
Korkmaz M: Effect of percutaneous nephrolithotomy and tract
dilatation methods on renal function: Assessment by quantitative
single-photon emission computed tomography of
technetium-99m-dimercaptosuccinic acid uptake by the kidneys. J
Endourol. 24:1497–1502. 2010.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Alken P, Hutschenreiter G and Günther R:
Percutaneous kidney stone removal. Eur Urol. 8:304–311.
1982.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Kessaris DN, Bellman GC, Pardalidis NP and
Smith AG: Management of hemorrhage after percutaneous renal
surgery. J Urol. 153:604–608. 1995.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Roth RA and Beckmann CF: Complications of
extracorporeal shockwave lithotripsy and percutaneous
nephrolithotomy. Urol Clin North Am. 15:155–166. 1988.
|
|
24
|
Ziaee SA, Karami H, Aminsharifi A, Mehrabi
S, Zand S and Javaherforooshzadeh A: One-stage tract dilation for
percutaneous nephrolithotomy: Is it justified? J Endourol.
21:1415–1420. 2007.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Lojanapiwat B: Previous open
nephrolithotomy: Does it affect percutaneous nephrolithotomy
techniques and outcome? J Endourol. 20:17–20. 2006.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lee KL and Stoller ML: Minimizing and
managing bleeding after percutaneous nephrolithotomy. Curr Opin
Urol. 17:120–124. 2007.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ozok HU, Sagnak L, Senturk AB, Karakoyunlu
N, Topaloglu H and Ersoy H: A comparison of metal telescopic
dilators and Amplatz dilators for nephrostomy tract dilation in
percutaneous nephrolithotomy. J Endourol. 26:630–634.
2012.PubMed/NCBI View Article : Google Scholar
|
|
28
|
McDougall EM, Liatsikos EN, Dinlenc CZ, et
al: Percutaneous approaches to the upper urinary tract. In: Walsh
PC, Vaughan ED, Wein AJ, Retik AB, eds. Campbell's Urology. 8th ed.
Philadelphia: WB Saunders. pp 3320-3369. 2002>.
|
|
29
|
Safak M, Gögüş C and Soygür T: Nephrostomy
tract dilation using a balloon dilator in percutaneous renal
surgery: Experience with 95 cases and comparison with the fascial
dilator system. Urol Int. 71:382–384. 2003.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Joel AB, Rubenstein JN, Hsieh MH, Chi T,
Meng MV and Stoller ML: Failed percutaneous balloon dilation for
renal access: Incidence and risk factors. Urology. 66:29–32.
2005.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Kijvikai K and de la Rosette J: Surgical
challenges of percutaneous nephrolithotomy. Business Briefing:
European Kidney & Urological Disease. 82-84. 2006.
|