Introduction
Allo-hematopoietic stem cell transplantation
(allo-HSCT) has become an essential part of the standard
therapeutic management for several hematological diseases and
malignancies, including acute or chronic leukemia. An estimated
10-40% of patients who undergo allo-HSCT develop significant
clinical acute graft-vs.-host disease (GVHD) (1). Gastrointestinal GVHD usually occurs ≥3
weeks after allo-HSCT and is characterized by profuse diarrhea,
anorexia, nausea, vomiting, abdominal pain and gastrointestinal
bleeding (2,3).
Accurate diagnosis of intestinal GVHD is required,
which is based on histological findings, including crypt
abnormalities, e.g. degeneration, dilatation, abscesses and crypt
loss, which accompany epithelial apoptosis in the ileum and colon
(4). Ileocolonoscopy is commonly
performed, as patients suspected to have acute GVHD complain of
gastrointestinal symptoms. Pathological examination is
indispensable for the confirmation of GVHD diagnosis; however,
treatment may be rapidly initiated after the preliminary endoscopic
diagnosis. Previous studies have reported that classic endoscopic
features, including orange-peel appearance, spotty redness, small
mucosa sloughing and diffuse mucosal defect, are useful in
diagnosing acute GVHD (5). It has
been previously reported that villous atrophy of the terminal ileum
is most useful for the diagnosis of GVHD (6). However, these previous studies did not
address details of the random sequence and were performed at a
single institution. Thus, the present study aimed to investigate
the incidence of villous atrophy in the terminal ileum and the
inter- and intra-observer agreement for this finding among
experienced endoscopists in multiple centers.
Materials and methods
Patients
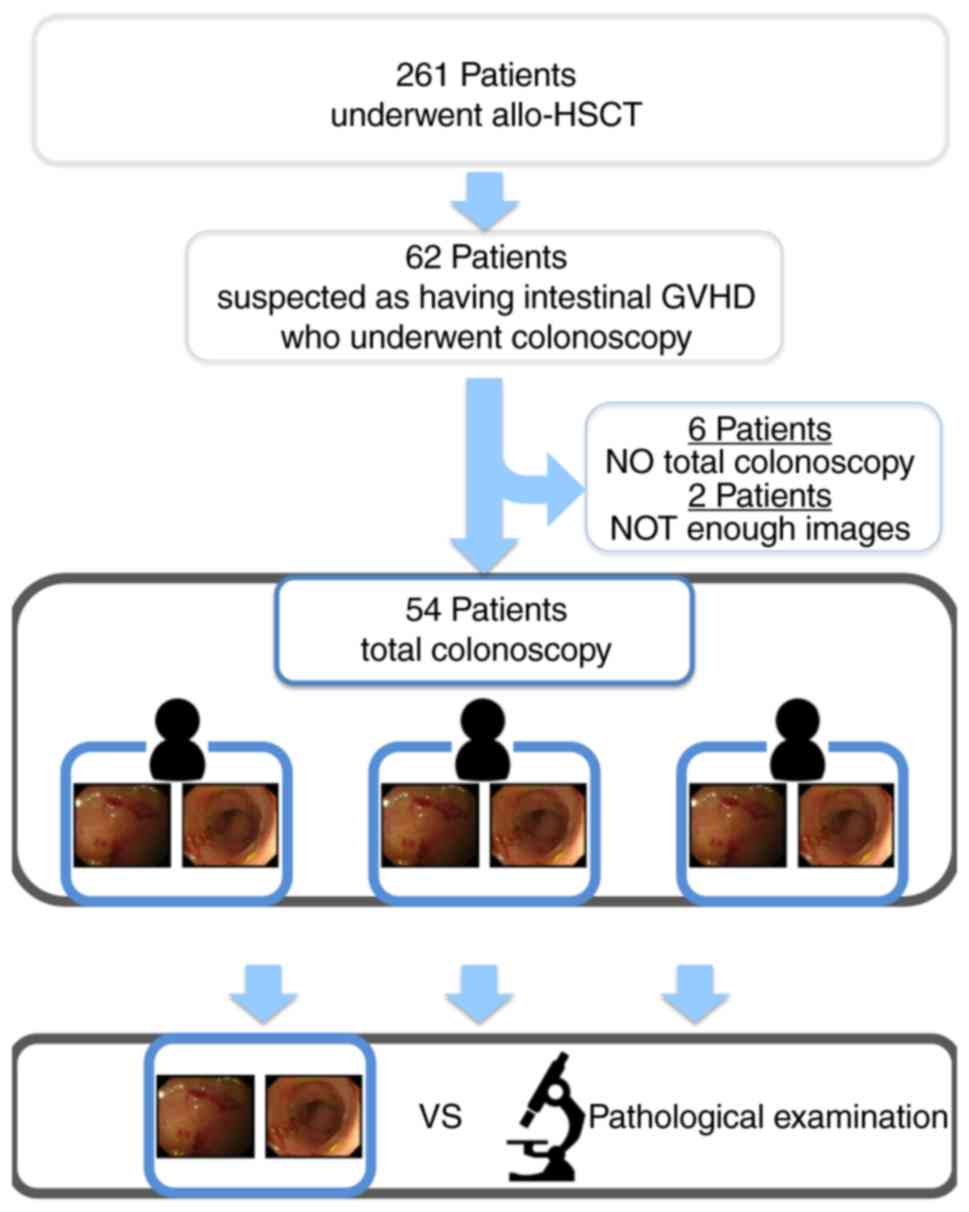
The present retrospective study comprised 261
consecutive patients who underwent allo-HSCT and were referred to
the Okayama University Graduate School of Medicine (Okayama, Japan)
between May 2008 and September 2015. Among them, 62 patients
underwent colonoscopy and had symptoms suggestive of
gastrointestinal GVHD, including anorexia, nausea, vomiting, watery
diarrhea and abdominal pain. All patients underwent biopsies in
each of the following segments regardless of the presence or
absence of abnormalities that may be indicative of intestinal GVHD:
Terminal ileum, right hemi-colon, left hemi-colon and rectum. A
total of 6 patients who were unable to undergo total
ileocolonoscopy due to incomplete preparation or unbearable pain
were excluded from the study. In addition, two patients with
inadequate imaging information following ileocolonoscopy were
excluded (Fig. 1). Demographic
information, details on the hematological condition, symptoms and
histological findings were retrospectively obtained from the
patients' medical records. All study participants provided informed
consent. The study was approved by the local ethics review
committee (approval no. 1610-013) and was registered at the
University Hospital Medical Network Clinical Trials Registry
(UMIN-CTR; registration no. UMIN000025390).
Endoscopic protocol
Experienced endoscopists performed the
ileocolonoscopy in all patients using Olympus endoscopes (CF-H260I,
CF-Q260I, PCF-Q260AI, CF-HQ-290I, CF-H290I or PCF-290I; Olympus
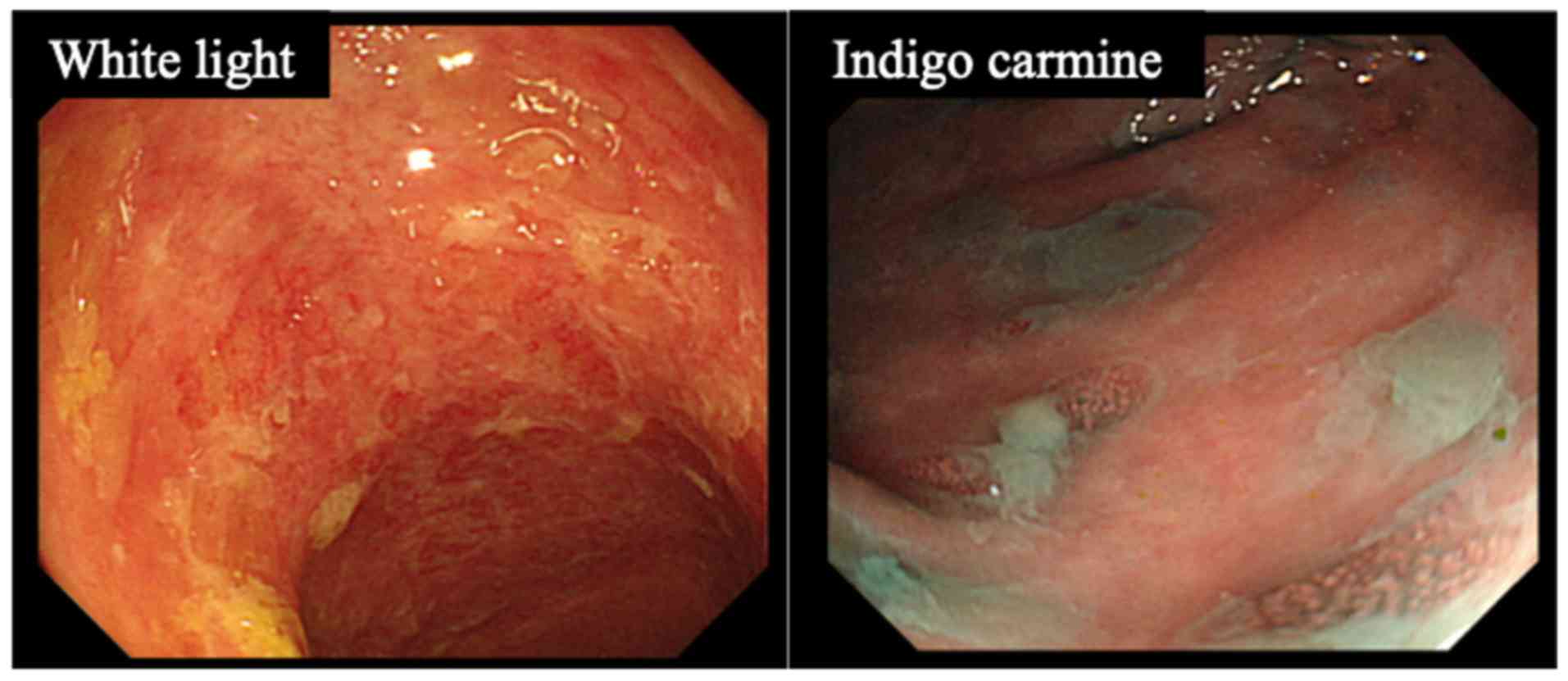
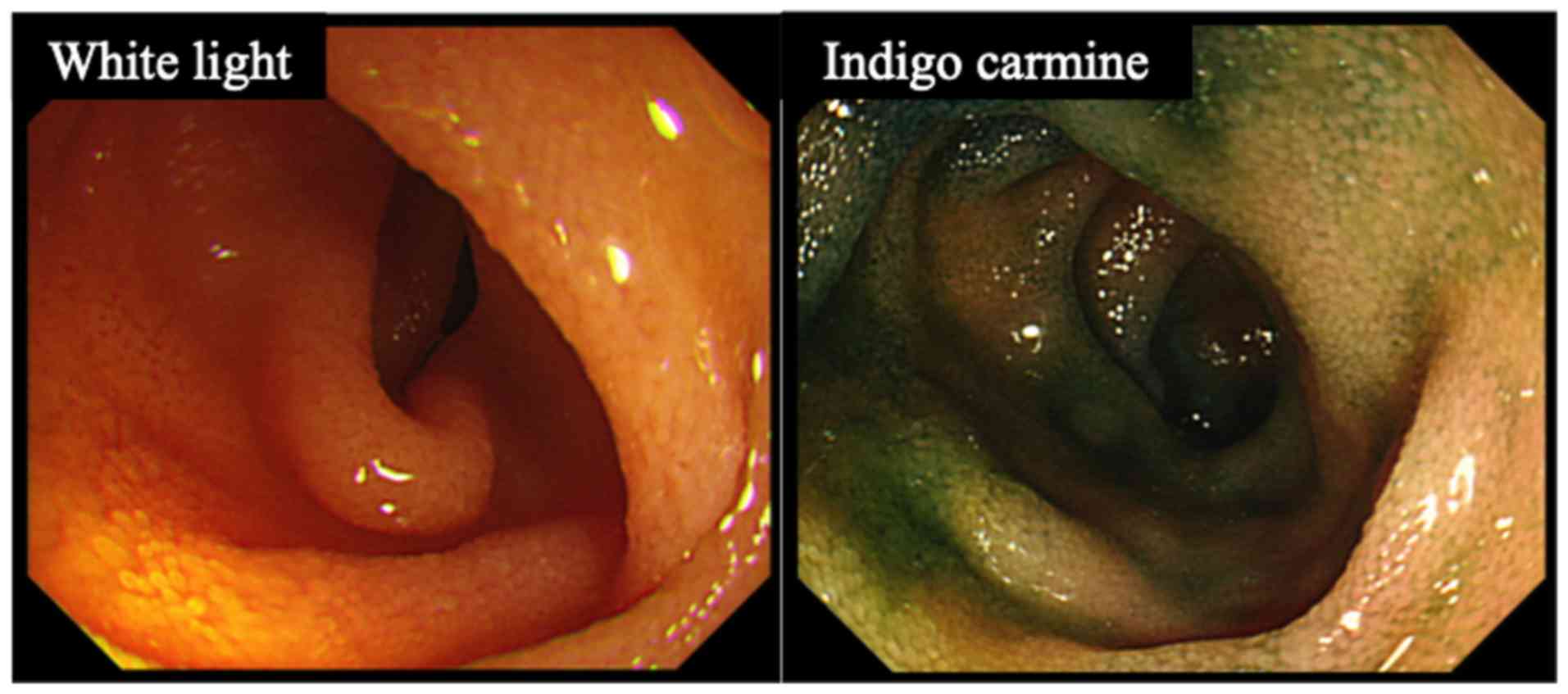
Optical). Ileocolonoscopic images were evaluated based on the
presence of villous atrophy observed in the terminal ileum
(Figs. 2 and 3). Regarding the preparation for
ileocolonoscopy, all patients were administered polyethylene glycol
(PEG) if oral ingestion was possible.
A total of 3 experienced endoscopists (>10 years
as a gastroenterologist) from multiple institutions (Okayama
University, Kagawa Prefectural Central Hospital, and Hiroshima
Citizens Hospital) served as observers (A,B,C) and examined the
images for the presence of villous atrophy in the terminal ileum.
They were blinded to any patient information, including
pathological diagnosis of GVHD, during the determination of
atrophy. The 3 endoscopists were blindly evaluated to check for
inter- and intra-observer agreement.
Pathological examination
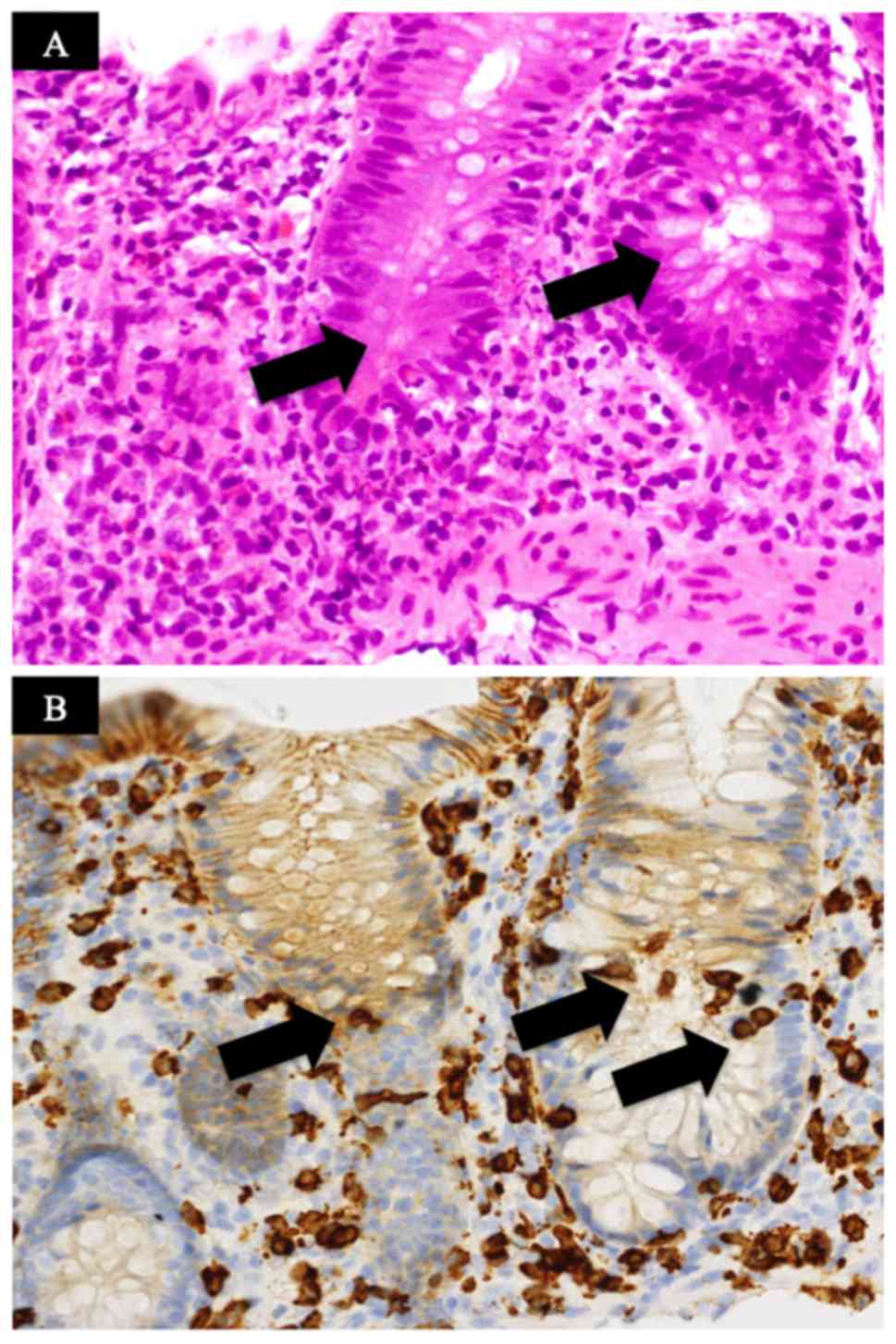
Biopsy specimens from all patients were subjected to
routine HE staining for pathological examination. The pathological
diagnosis of GVHD was based on the following criteria: i) The
presence of apoptotic bodies in the epithelium of the ileum, colon
or rectum; ii) crypt abnormalities of degeneration, dilatation,
abscesses or loss; iii) all histological findings were determined
by HE staining and CD8 immunostaining (Fig. 4). In the present study, GVHD was
diagnosed when all of these three previously listed criteria were
met. The gold standard of GVHD diagnosis is positive pathological
detection. A patient was diagnosed with GVHD if the pathological
findings of any ileocolonoscopic samples met these criteria.
Statistical analysis
All analyses were performed using JMP version 11.2
(StataCorp). Statistical comparisons were performed using the
Student's t-test. P<0.05 was considered to indicate statistical
significance. Reproducibility coefficients were analyzed using the
kappa agreement coefficient. Intra- and inter-observer agreement
values were classified as follows: Poor (≤0.20), slight
(0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80) and
excellent (0.81-1.00). Diagnostic values, the diagnostic value of
the ileocolonoscopy observation result compared with the
pathological result as a gold standard, were compared among
observers and for each observer in terms of sensitivity,
specificity, positive predictive value (PPV) and negative
predictive value (NPV) by a 2x2 contingency Table using the
Student's t-test.
Results
Patient demographics
The characteristics of the 54 patients are presented
in Table I. Definitive pathological
and non-pathological GVHDs were identified in 22 and 32 patients,
respectively. The mean patient age was 46 years and the youngest
patient was aged 10 years (range, 10-67) years. The most common
diagnosis was acute myeloid leukemia.
 | Table ICharacteristics of patients suspected
to have gastrointestinal GVHD who underwent colonoscopy. |
Table I
Characteristics of patients suspected
to have gastrointestinal GVHD who underwent colonoscopy.
| Item | Value |
|---|
| Pathological
result | |
|
GVHD | 22 |
|
No GVHD | 32 |
| Age (years), mean
(range) | 46 (10-67) |
| Sex | |
|
Male | 32 |
|
Female | 22 |
| Disease requiring
transplantation | |
|
Acute
myeloid leukaemia | 15 |
|
Myelodysplastic
syndromes | 11 |
|
Acute
lymphoblastic leukaemia | 8 |
|
Adult T-cell
leukemia/lymphoma | 4 |
|
T
lymphoblastic leukemia/lymphoma | 4 |
|
B
lymphoblastic leukemia/lymphoma | 3 |
|
Chronic
myelogenous leukaemia | 3 |
|
Diffuse
large B-cell lymphoma | 1 |
|
Myelofibrosis | 1 |
|
Non-Hodgkin
lymphoma | 1 |
|
Extranodal
NK/T-cell lymphoma | 1 |
|
Polycythaemia | 1 |
|
Severe
combined immunodeficiency | 1 |
| Stem cell source | |
|
Bone
marrow | 39 |
|
Cord
blood | 9 |
|
Peripheral
blood stem cell | 6 |
The results of examining whether villous atrophy
could predict GVHD in all 54 sets of images were as follows. The
sensitivity (which examines whether villous atrophy could predict
GVHD) was 86.4, 77.3 and 79.2%, respectively, and the specificity
was 62.5, 62.5 and 86.7%, respectively, for the three observers (A,
B and C). Furthermore, the PPV was 61.3, 58.6 and 82.6%,
respectively, whereas the NPV was 87.0, 80.0 and 83.9%,
respectively (Tables
II-IV).
Inter-observer agreement
Table V displays the inter-observer reliability of
each observer. Kappa coefficients among observers A and B, A and C
and B and C were 0.85, 0.63 and 0.63, respectively (Table V).
| Table VParameters of intraobserver and
interobserver agreement regarding villous atrophy. |
Table V
Parameters of intraobserver and
interobserver agreement regarding villous atrophy.
| A, Inter-observer
agreement (Kappa coefficient) |
|---|
| Observer | A | B | C |
|---|
| A | 1 | 0.85 | 0.63 |
| B | 1 | 0.63 | |
| C | 1 | | |
| B, Intra-observer
agreement |
| Observer | A | B | C |
| Kappa value | 0.88 | 0.73 | 0.75 |
| 95% CI | 0.83-0.94 | 0.65-0.81 | 0.70-0.81 |
Intra-observer agreement
When analyzing the villous atrophy in all patients,
the intra-observer kappa coefficient was determined to be 0.88 (95%
CI 0.83-0.94) for observer A, 0.73 (95% CI 0.65-0.81) for observer
B and 0.75 (95% CI 0.70-0.81) for observer C (Table IV).
| Table IVAssociation between the number of
patients with GVHD and villous atrophy by Observer C. |
Table IV
Association between the number of
patients with GVHD and villous atrophy by Observer C.
| | GVHD | |
|---|
| Villous atrophy | Positive | Negative | Total |
|---|
| Positive | 19 | 4 | 23 |
| Negative | 5 | 26 | 31 |
| Total | 24 | 30 | 54 |
Discussion
The present study was the first, to the best of our
knowledge, to investigate the inter- and intra-observer agreement
for the ileocolonoscopic finding of villous atrophy in the terminal
ileum to detect acute intestinal GVHD in multiple institutions.
A previous study by our group suggested that villous
atrophy in the terminal ileum is a useful endoscopic finding in
acute intestinal GVHD (6). Of note,
the pathological diagnosis is indispensable for the final diagnosis
of acute intestinal GVHD; however, the study by our group reported
that villous atrophy in the terminal ileum is an important
indicator for the estimation using ileocolonoscopy. Comparing this
finding and the diagnosis of acute intestinal GVHD, the sensitivity
of villous atrophy observed in the terminal ileum was 86.4, 77.3
and 79.2%, whereas the specificity was 62.5, 62.5 and 86.7%, for
observers A, B and C, respectively. In a previous study, Altun
et al (7) reported that lower
endoscopic findings had a sensitivity and specificity of 40 and 0%,
respectively. However, this study only examined a low number of
patients in only one facility and did not emphasize the importance
of terminal ileum observation. According to the previous study by
our group, villous atrophy in the terminal ileum is an important
finding (6); therefore, the terminal
ileum should be visualized during colonoscopy.
To the best of our knowledge, the present study was
the first to examine the inter-observer agreement of
ileocolonoscopic findings for predicting GVHD. The kappa value for
inter-observer agreement was 0.85 for observers A and B, 0.63 for A
and C, and 0.63 for B and C. Based on these results, the
inter-observer agreement was substantial to excellent in clinical
practice. If an endoscopist has a certain amount of clinical
experience, villous atrophy in the terminal ileum may be considered
to have an excellent inter-observer agreement, even if the
observers are from different institutions.
Certain endoscopists may argue that complete
ileocolonoscopy, which requires insertion into the terminal ileum,
is not widely accepted, as it is completely invasive and associated
with a high risk of complications (8). However, we believe that careful
endoscopic insertion techniques will enable rapid endoscopic
diagnosis of acute intestinal GVHD. It may be speculated that
pathological examination of acute intestinal GVHD is required for
the diagnosis; however, endoscopic evaluation is also important, as
the results may be obtained faster compared with pathological
examination. In a previous study, endoscopic and histological
findings of distal colonoscopy were indicated to be clinically
significant in diagnosing patients who had intestinal GVHD with a
poor general condition and who were at high risk of developing
endoscopy-associated complications (9). Depending on the patient's condition, it
is possible to prepare a testable condition by carefully prepping
patients with PEG and enema. The method is to reduce the amount of
food taken by patients and taking PEG on the day before the
examination. On the day of examination, patients should take PEG
carefully while paying attention to their symptoms. Prepping of
patients is complete when the patient has taken ~2,000 ml of PEG
and solid excretion has almost disappeared. Enema is performed if
patients are not adequately prepped before examination
The present study had several limitations. First,
since it was a retrospective study, images of the terminal ileum
were already acquired. The location and angle of images were
different for each endoscopist, which may have had an influence on
the results of the present study. Furthermore, only 54 cases were
screened by three observers, and it was not evaluated whether this
number of patients and the number of observers were appropriate.
Finally, the present study does not consider GVHD with
cytomegalovirus or thrombotic microangiopathy. To the best of our
knowledge, no studies have been performed on how the mucosa at the
terminal ileum changes in GVHD with the above diseases. The study
on the ileal mucosa of these diseases is an important theme for the
future.
In conclusion, substantial inter- and intra-observer
agreement was achieved for the detection of villous atrophy in the
terminal ileum and the inter-observer agreement for the predictive
histological diagnosis was also substantial to excellent, whereas
the intra-observer agreement ranged from substantial to excellent
for villous atrophy in the terminal ileum and acute intestinal
GVHD. Based on the results of the present study, villous atrophy in
the terminal ileum was a clinically effective diagnostic parameter
even if different endoscopists from multiple institutions were
involved in the diagnosis.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study available from the corresponding author on reasonable
request.
Authors' contributions
YS, SH, FO, and HO made substantial contributions to
conception and design. YS, EY, SO, YY, TI, HK, MT and TT were
involved in the acquisition of data. YS, YM, ST and KH analysed and
interpretated the data. YS and SH were involved in drafting the
manuscript and revising it critically for important intellectual
content. All authors approved the final manuscript and agreed to be
accountable for all aspects of the work.
Ethics approval and consent to
participate
The Ethics Review Committee of Okayama University
Graduate School of Medicine granted ethical approval for the study
(approval no. 1013) and was registered in the University Hospital
Medical Information Network Clinical Trials Registry (reference no.
UMIN000025390). All participants provided written informed
consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Iqbal N, Salzman D, Lazenby AJ and Wilcox
CM: Diagnosis of gastrointestinal graft-versus-host disease. Am J
Gastroenterol. 95:3034–3038. 2000.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Strasser SI and McDonald GB:
Gastrointestinal and hepatic complications. Hematopoietic cell
transplant. 4th ed. Oxford, UK: Wiley, Blackwell Publishing.
2009.
|
|
3
|
Nevo S, Enger C, Swan V, Wojno KJ, Fuller
AK, Altomonte V, Braine HG, Noga SJ and Vogelsang GB: Acute
bleeding after allogeneic bone marrow transplantation: Association
with graft versus host disease and effect on survival.
Transplantation. 67:681–689. 1999.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Epstein RJ, McDonald GB, Sale GE, Shulman
HM and Thomas ED: The diagnostic accuracy of the rectal biopsy in
acute graft-versus-host disease: A prospective study of 13
patients. Gastroenterology. 8:764–771. 1980.PubMed/NCBI
|
|
5
|
Endo K, Fujishima F, Kuroha M, Moroi R,
Onodera M, Naito T, Kanazawa Y, Kimura T, Shiga H, Kakuta Y, et al:
Effective and less invasive diagnostic strategy for
gastrointestinal GVHD. Endosc Int Open. 6:E281–E291.
2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sugihara Y, Hiraoka S, Fujii N, Takashima
S, Yamasaki Y, Inokuchi T, Takahara M, Kuwaki K, Harada K, Tanaka T
and Okada H: Villous atrophy in the terminal ileum is a specific
endoscopic finding correlated with histological evidence and poor
prognosis in acute graft-versus-host disease after
allo-hematopoietic stem cell transplantation. BMC Gastroenterol.
18(111)2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Altun R, Gökmen A, Tek İ, Soydan E and
Kurt Yüksel M: Endoscopic evaluation of acute intestinal
graft-versus-host disease after allogeneic hematopoietic cell
transplantation. Turk J Gastroenterol. 27:312–316. 2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Daniel F, Hassoun L, Husni M, Sharara A,
Soweid A, Barada K, Haffar B, Massoud R, Shaib Y, Al-Hashash J, et
al: Site specific diagnostic yield of endoscopic biopsies in
gastrointestinal graft-versus-host disease: A tertiary care center
experience. Curr Res Transl Med. 67:16–19. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Oomori S, Takagi S, Kikuchi T, Utsunomiya
K, Yokoyama H, Negoro K, Tohmiya Y, Aihara H, Yamada M, Takahashi
S, et al: Significance of colonoscopy in patients with intestinal
graft-versus-host disease after hematopoietic stem cell
transplantation. Endoscopy. 37:346–350. 2005.PubMed/NCBI View Article : Google Scholar
|