Introduction
Chronic kidney disease (CKD) has a considerable
impact on health, by progressive loss of kidney functions up to
end-stage renal disease (ESRD) requiring renal replacement
treatment (RRT), either by dialysis or by kidney transplant.
Moreover, health and survival are endangered by the complications
associated with CKD, such as anemia, disturbances of bone and
mineral metabolism, high blood pressure (HBP), cardiovascular
disease, anxiety or depression and altered quality of life
(1,2).
Therefore, an early diagnosis is important, followed
by adequate assessment, monitoring, and treatment of patients with
CKD, because proper management may slow down the progression and
even prevent the occurrence of ESRD (1).
Referring these patients to the nephrologist is one
of the mainstays of the correct management of CKD. An early
assessment by the nephrologist may unravel the etiology of kidney
disease and may lead to prompt initiation of strategies able to
delay the progressive decline of kidney function, prevent and treat
the complications, and appropriately prepare for and timely
initiate RRT (3).
Materials and methods
This is a retrospective, unicentric study regarding
the status of patients with stage 5 CKD at the time of RRT
initiation. The evaluation included the clinical manifestations
leading to hemodialysis initiation, as well as the clinical and
laboratory features of the patients when hemodialysis was started,
including etiology of CKD, associated comorbidities, biological
status, previous nephrological monitoring, preparation of patients
by vascular access creation prior to the initiation of RRT. The
subjects of this study were patients with stage 5 CKD admitted to
the Nephrology Clinic of the Emergency University Hospital of
Bucharest (Romania), in whom hemodialysis was initiated between
January 1st, 2017 and March 31st, 2018. The inclusion criteria were
age over 18 years and hemodialysis initiation. The exclusion
criteria was acute kidney injury unresponsive to conservatory
treatment, but with recovery of the kidney function after several
hemodialysis sessions.
A total of 109 patients were included in the study.
Information was obtained regarding age, gender, socioeconomic
background, etiology and duration of CKD, risk factors, history,
including HBP, diabetes mellitus (DM), myocardial infarction, left
ventricular hypertrophy, ischemic heart disease (IHD), heart
failure (HF), stroke, peripheral arterial disease (PAD), and
cardiac arrhythmias. The assessment included also routine
laboratory tests. Glomerular filtration rate was calculated by
means of 2009 CKD-EPI Creatinine Equation. The statistical analysis
was performed by means of Chi-square test, Fisher's exact test,
ANOVA, and Kruskal-Wallis H test.
This study was approved by Ethics Committee of the
Emergency University Hospital of Bucharest. Written informed
consent was obtained from all patients prior to publication.
Results
Demographics
In our sample, there were 56 (51.38%) women and 53
men (48.62%). The mean age of the patients was 64.61±13.59 years,
with a minimum age of 25 and a maximum of 91 years. In women, the
average age was 66.46±14.09 years and in men 62.66±12.88 years. Of
the patients 69.72% lived in an urban setting.
Etiology
In our sample, the etiology of CKD was: i) vascular
nephropathies (28%); ii) DM (24%); iii) glomerular nephropathies
(10%); iv) obstructive nephropathy (9%); v) tubulointerstitial
nephropathy (5%); vi) other etiology including kidney polycystic
disease (6%); and vii) unknown etiology in 12% of the patients.
Gender predominance varied according to CKD etiology, with a female
preponderance in diabetic nephropathy, obstructive nephropathy,
tubulointerstitial nephropathy, and in kidney disease of unknown
cause. By contrast, there was a male preponderance for vascular and
glomerular nephropathies, and for polycystic kidney disease.
Comorbidities
Most of our patients (93 i.e., 85.32%) had HBP.
There was a mild female preponderance (48 out of 93) among our
hypertensive patients. There were 46 patients with left ventricular
hypertrophy (LVH), most of these patients being males (31 males vs.
15 females). The higher proportion of males was statistically
significant: Chi-squared with Yates correction = 3.87 with a
P=0.049, while the P-value yielded by Fisher's exact test was
0.036. HF was present in 41 (37.61%) patients. A history of stroke
was identified in 15 patients (7 females and 8 males). PAD was
present in 27 patients (13 females and 14 males). Atrial
fibrillation (AF) was present in 19.27% of the patients.
Duration of CKD
The duration of CKD prior to RRT was not known in 42
of our patients. In the other 67 patients, the mean duration of the
known evolution of CKD (from the moment of diagnosis until RRT
initiation) was 41.28±35.71 months.
Pre-dialysis monitoring
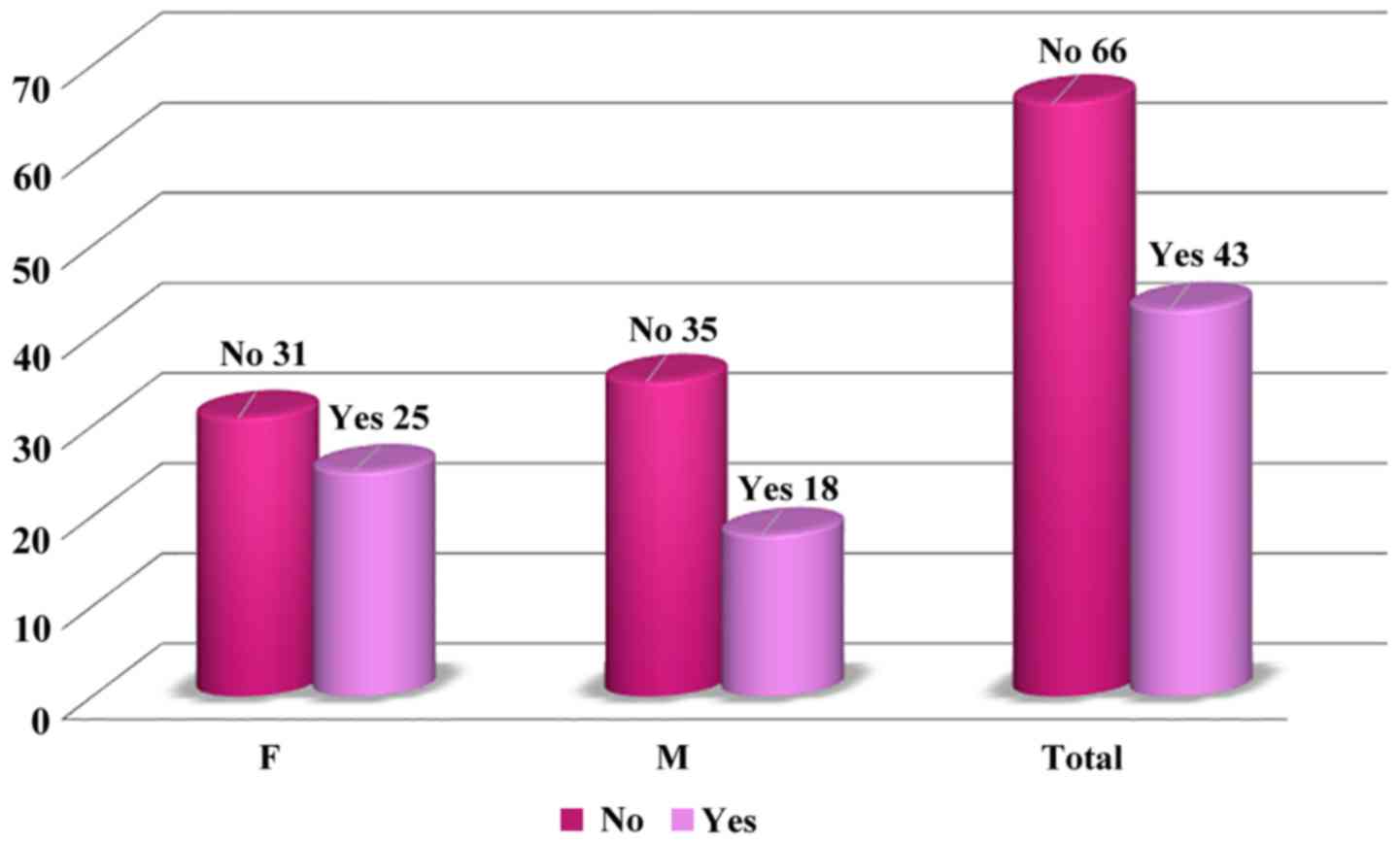
Only 43 (39.45%) of our patients were monitored
prior to hemodialysis initiation. Among these patients followed by
a nephrologist, there was a higher proportion of females (Table I; Fig.
1).
 | Table IThe characteristics of the study
group. |
Table I
The characteristics of the study
group.
| General
characteristics | Values |
|---|
| Total number of
patients | 109 |
| Sex | F: 51.38%; M:
48.62% |
| Socioeconomic
background | Urban: 69.72%; Rural:
30.28% |
| Mean age | 64.61±13.59
years |
| Duration of
CKD | 41.28±35.71
months |
| Body mass
index | 25.97±6.27
kg/m2 |
| CKD etiology
(%) |
|
Vascular
nephropathies | 28.44 |
|
Diabetic
nephropathy | 23.85 |
|
Glomerular
nephropathy | 10.09 |
|
Tubulointerstitial
nephropathy | 4.59 |
|
Polycystic
kidney disease | 6.42 |
|
Obstructive
nephropathy | 9.17 |
|
Unknown
etiology | 11.93 |
| Comorbidities
(%) |
|
High blood
pressure | 85.32 |
|
Ischemic
heart disease | 68.81 |
|
Left
ventricular hypertrophy | 42.20 |
|
Cardiac
failure | 37.61 |
|
Stroke | 13.76 |
|
Peripheral
arterial disease | 24.77 |
|
Atrial
fibrillation | 19.27 |
Vascular access and preparation for
hemodialysis
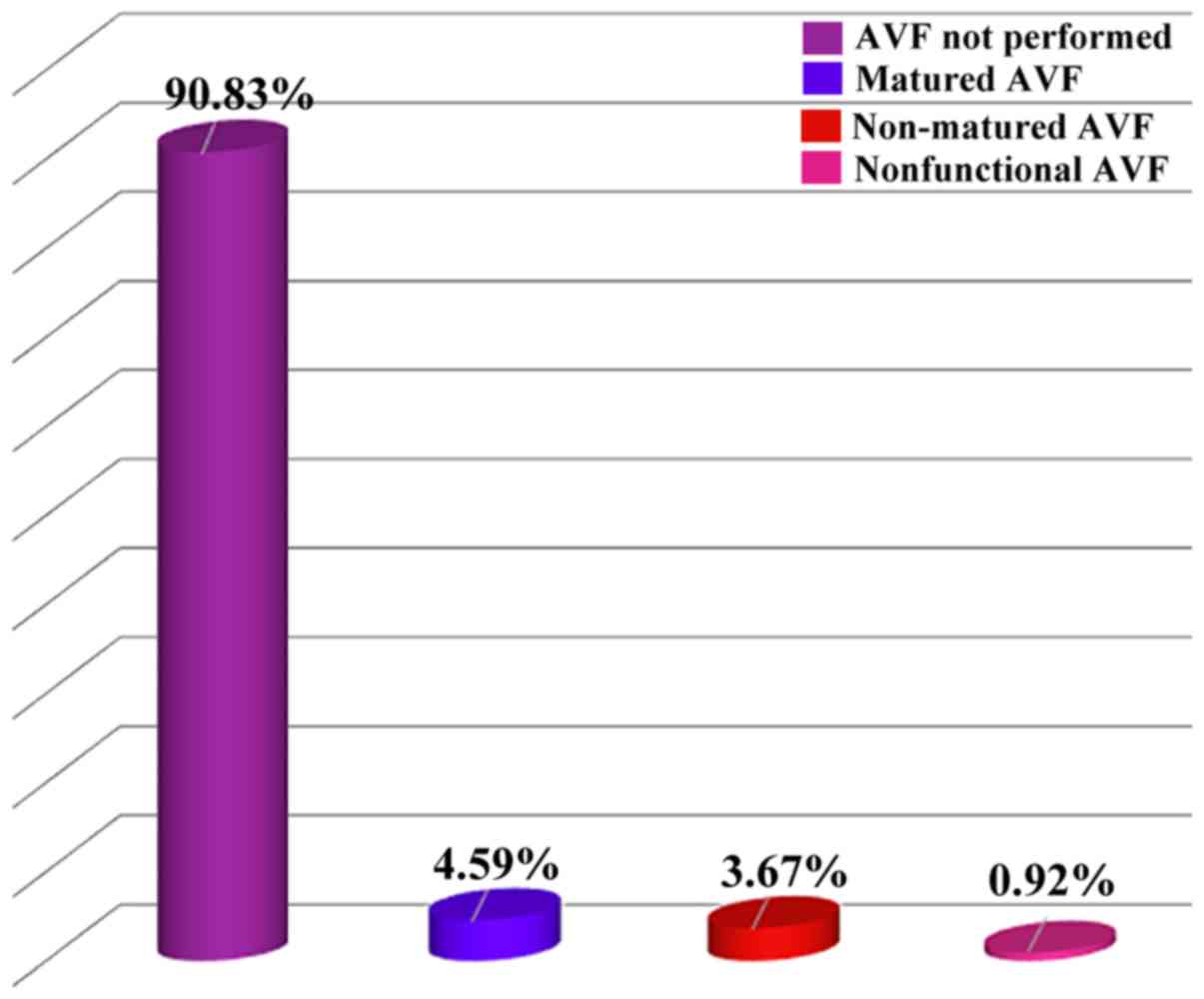
In our study, a low availability of arteriovenous
fistula (AVF) was identified for hemodialysis initiation: only 10
of or patients (9.17%) presented AVF, and only 5 of them had AVF
mature enough to be used for hemodialysis. Consequently,
hemodialysis was initiated on central venous catheter (CVC) (in
most cases non-tunneled) in 78.90% of the patients (Fig. 2).
For the patients included in our study, hemodialysis
was initiated at a GFR of 4 to 5 ml/min/1.73 m2.
Hemodialysis was initiated at a higher GFR in males (5.32±2.14
ml/min/1.73 m²) than in females (4.25±1.96 ml/min/1.73 m²), a
statistically significant difference (P=0.007 on ANOVA, P=0.0013,
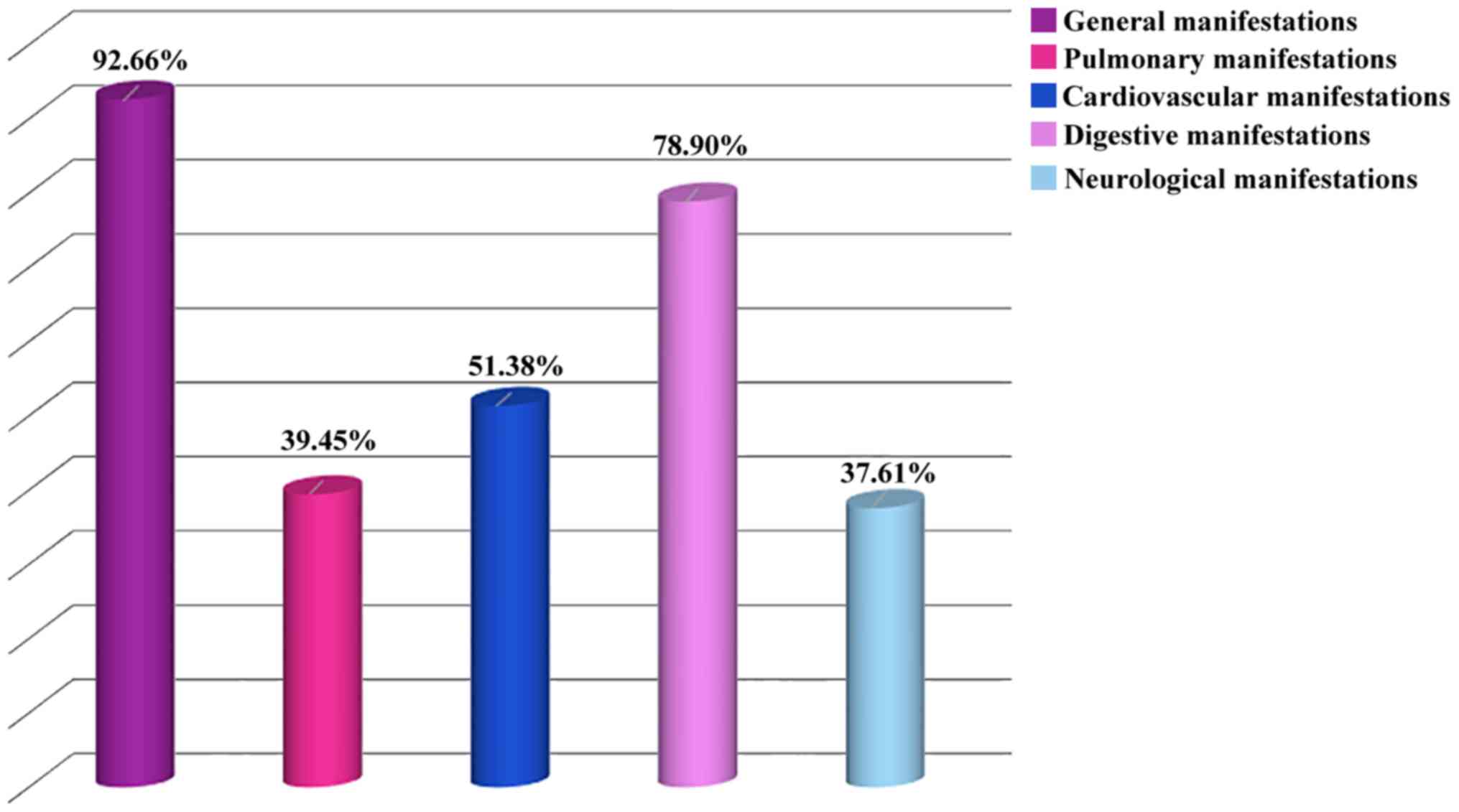
corresponding to a 10.34 statistic, on Kruskal-Wallis H test). Most
of the patients included in our study had an altered general status
and fatigue/tiredness with poor exercise capacity when started on
hemodialysis (Fig. 3).
Pulmonary manifestations
Pulmonary manifestations were present in 39.45% of
the patients and cardiovascular manifestations in more than half of
the cases. Acute pulmonary edema was present in 17.43% of the
patients, but 33.94% had clinical and/or laboratory signs of
hyperhydration. Digestive manifestations, such as loss of appetite,
nausea and vomiting were encountered in most of the patients
(78.90%) enrolled in our study. Only a low proportion of patients
(7.34%) had hemorrhagic events when hemodialysis was initiated, and
5.5% had an upper gastrointestinal bleeding.
Neurological manifestations
A proportion of 37.61% of the patients had
neurological manifestations, but only 1.83% had uremic
encephalopathy (Table II).
| Table IIBiological parameters of the study
group. |
Table II
Biological parameters of the study
group.
| Parameters | Values |
|---|
| Hemoglobin | 8.6±1.8 g/dl |
| Cholesterol | 173.14±47.14
mg/dl |
| Triglycerides | 164.04±91.32
mg/dl |
| Calcium | 7.7±1.11 mg/dl |
| Phosphorus | 6.55±2.43
mg/dl |
| Calcium x
Phosphorus | 33.2±27.2
mg/dl |
| Potassium | 5.06±1.32
mmol/dl |
| Uric acid | 7.4±2.7 mg/dl |
| Albumin | 3.35±0.70 g/dl |
Anemia
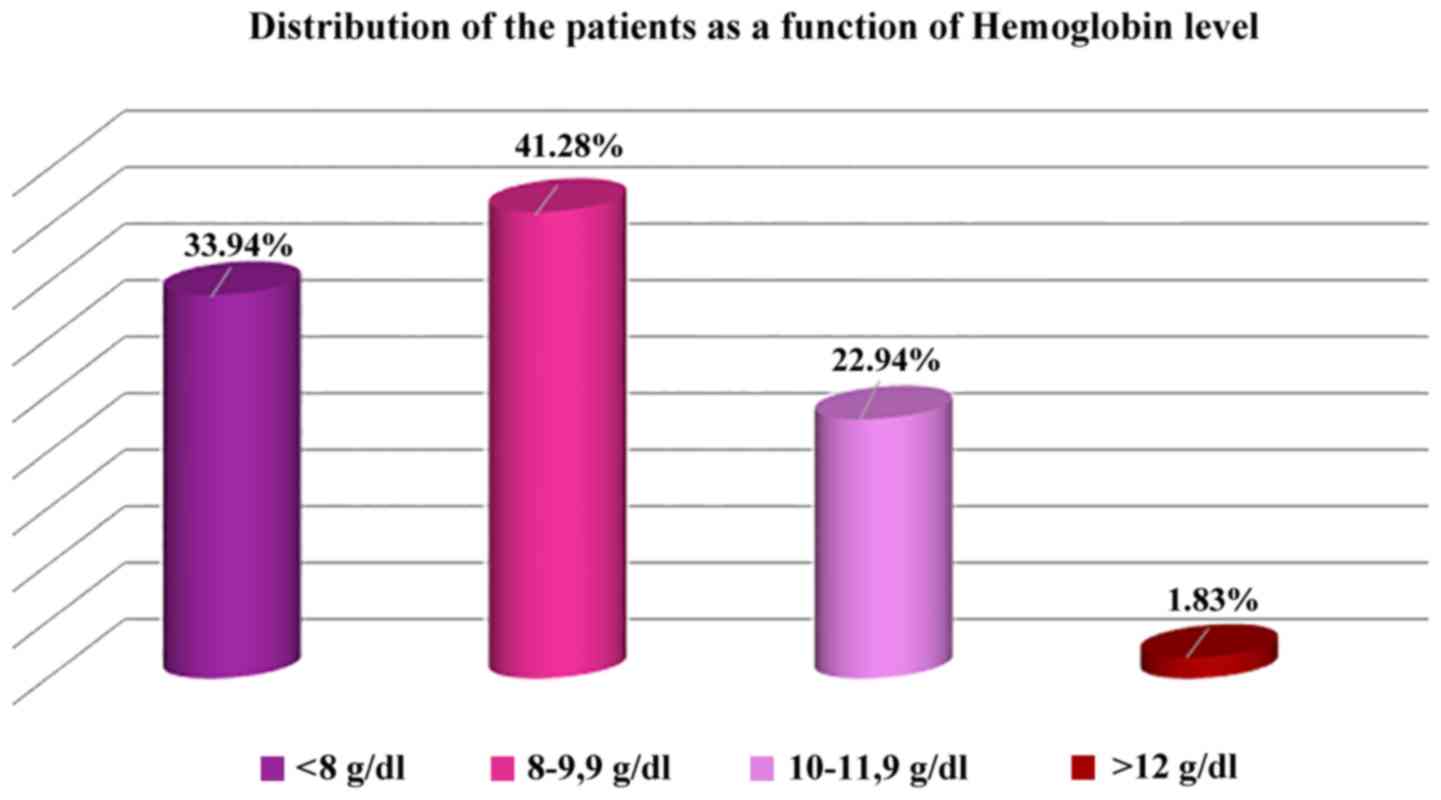
Most of the patients (98.17%) had anemia, the mean
level of hemoglobin being 8.69±1.85 g/dl. Dividing the patients in
three categories based on the level of hemoglobin (10-12 g/dl,
8-9.9 g/dl, and less than 8 g/dl), the middle category was the most
numerous (41.28%).
In our study, the hemoglobin level did not differ
significantly between the patients monitored by a nephrologist
(8.71±1.65 g/dl) and the unmonitored ones (8.67±1.98 g/dl)
(Fig. 4).
Nutritional status
The mean serum albumin level was 3.35±0.70 g/dl and
mean serum uric acid 7.44±2.7 mg/dl, while the mean body mass index
was 25.97±6.27 kg/m2.
Bone and mineral metabolism
The mean serum calcium level was 7.70±1.11 mg/dl and
mean serum phosphorus 6.55±2.43 mg/dl. Most of the patients had
hypocalcemia.
Discussion
In our study group there were slightly more females,
although most of the currently available studies agree on a higher
prevalence of CKD in males than in females, and also on a slower
progression of CKD in females than in males (3). The fact that most of the patients
included in the study lived in an urban setting may be explained by
healthcare facilities being more readily available to the urban
population. The poor access to medical care in the countryside is a
consequence of the low socioeconomic level (4,5).
Vascular nephropathies and DM were the dominant etiology of CKD, in
agreement with available data pointing out HBP and DM as the main
causes of CKD (6,7). However, it should be noted that HBP may
also be the result of CKD, not only the cause (8).
Regarding gender predominance for diabetic
nephropathy, a recent study concluded that female gender should be
counted among the unmodifiable risk factors for diabetic
nephropathy, while male gender is one of the factors incriminated
for its progression (7). It is
common knowledge that HBP is one of the major risk factors for
glomerulosclerosis (9). Both
systolic and diastolic arterial pressure were higher in males
(10). These observations may
explain the higher percentage of male patients in our study, with
HBP as etiology for CKD. In our study, the patients with CKD
secondary to a glomerular disease were more frequently males. As
reported in the literature, the gender predominance differs
according to the type of glomerular disease: females in lupus
nephritis and males in acute post infectious nephritis, focal
segmental glomerulosclerosis and IgA nephropathy (11). In our study, information was lacking
about the exact type of glomerular disease responsible for ESRD,
therefore we could not find an explanation for the higher
percentage of males in the subset defined by glomerular disease
etiology. The female predominance among the patients with
obstructive nephropathy as the cause of ESRD in our sample is at
odds with the data in the literature, where male gender dominates
this particular etiology of ESRD (12). For autosomal dominant polycystic
kidney disease, the data in the literature indicate that RRT is
initiated in males earlier than in females, which may explain the
results of our study (13).
Most of our patients had HBP, which is in agreement
with the data from the literature indicating a 90% prevalence of
HBP among ESRD patients at the time when hemodialysis is initiated
(14). Of our patients 68.81% had
IHD at the time when hemodialysis was started. IHD is an important
comorbidity in patients started on hemodialysis, as it is
associated with a higher mortality (15). Other identifiable comorbidities were
left ventricular hypertrophy (LVH), HF, stroke, PAD and AF. The
available studies confirm the presence of LVH in patients with
ESRD, and associate it with an increased risk of sudden death,
highlighting the need that the practitioners should pay particular
attention to therapeutic strategies aimed at reducing LVH (16). Like IHD, HF is an important risk
factor for death in ESRD patients started on hemodialysis, both on
short and long-term (17). Stroke
seems to occur with increased frequency in the 3 months preceding
the onset of chronic hemodialysis, the highest risk being in the
month preceding the initiation of RRT. However, after starting
hemodialysis, the stroke risk declines (18). A history of PAD in patients started
on chronic hemodialysis is associated with a higher need of either
revascularization or amputation (19). Patients with AF are known to have a
bad prognosis because of a higher risk of cardiovascular events
(20-23).
According to literature, the evolution of CKD to
more advanced stages is slower in elderly patients (24).
The patient with CKD needs specialized care. The
guidelines state that specialized nephrological care is preferable
for patients with a GFR <60 ml/min/1.73 m2 and
mandatory for those with a GFR <30 ml/min/1.73 m2
(25). The occurrence of
complications typical for CKD (HBP, cardiovascular disease, anemia,
bone and mineral metabolism disturbances, anxiety or depression)
has an important impact on the health status and on the survival of
these patients (1). Early monitoring
and implementation of therapeutic strategies aimed at slowing down
the progressive decline of kidney function, as well as adequate
preparation for and timely initiation of RRT, are important for
ameliorating the prognosis of these patients (2). Delaying the referral to a nephrologist
is one of the major issues leading to suboptimal care of a CKD
patient. A patient not included soon enough in a monitoring program
lead by a nephrologist is more likely to be started on RRT on an
emergency basis, which may be deleterious for the outcome of the
patient, resulting in lower quality of life and increased
morbidity, mortality, and healthcare costs (26).
When RRT is required, the clinician together with
the patient have to choose between hemodialysis, peritoneal
dialysis and kidney transplant. The first option for treatment of
choice (in Romania and in most other countries) is hemodialysis
(27). Performing hemodialysis
requires vascular (venous) access. The conclusion of most of the
studies and the current recommendation in most of the guidelines is
that the preferred vascular access for hemodialysis initiation is
an arteriovenous fistula (AVF). However, in most ESRD patients
hemodialysis is initiated on a CVC, either untunneled or tunneled
(28). The data collected in our
study are consistent with the literature. Suboptimal preparation of
the patients is the result of poor referral to the specialist.
Regarding GFR, there is no optimal level for hemodialysis
initiation defined by the guidelines. The symptoms and the general
lack of well-being of the patient, rather than a certain GFR are
major criteria for starting hemodialysis (27). However, the occurrence of certain
manifestations recommend earlier initiation of hemodialysis, even
at a GFR of 15 ml/min/1.73 m2, including hyperkalemia,
hyper hydration, weight loss and malnutrition, cognitive decline
(29,30). The identified symptomatology of our
patients is in line with specialty literature: pulmonary,
cardiovascular and digestive manifestations, acute pulmonary
edema.
CKD patients are known to have a higher risk of
bleeding, gastrointestinal tract being frequently involved
(31).
However, our study identified an unacceptably high
number of patients with a hemoglobin level below 8 g/dl, which is
an important issue because a level of hemoglobin below 8 g/dl is
associated with higher mortality. This increased death risk
persists even if the hemoglobin level is restored to above 10 g/dl
after 4 months of dialysis (32).
The most probable explanation is that among the 43 patients
monitored by a nephrologist only a few (23.26%) received an
erythropoiesis stimulating agent, and none of them reached the
targeted level of hemoglobin, a sobering fact that underlines the
necessity of improving anemia management in predialysis patients
(32).
Both in predialysis and in chronically hemodialysis
patients there is a close relation between the nutritional status
and mortality (33). The nutritional
status was assessed by means of the body mass index and the serum
albumin level, lipid fractions, and uric acid. In most of the
subjects the serum cholesterol level was below 150 mg/dl, while the
serum triglycerides level was normal, which differs from the
results of other studies in which the serum triglycerides level was
increased (34,35). In our study, we evaluated markers of
nutritional status (albumin, uric acid, body mass index), as well
as bone and mineral metabolism (calcium, phosphorus) markers.
Unfortunately, data regarding the serum PTH level
were not available. Assessing for bone and mineral metabolism
disorders is of paramount importance for the survival of the
patients on chronic hemodialysis, because these complications have
a great impact on both morbidity and mortality (36,37), due
to their close association with cardiovascular complications
(38).
In conclusion, increasing the number of monitored
patients in early stages of CKD and improving their management
result in lower morbidity and mortality. These objectives may be
achieved by implementing screening programs and early
interventions. In the advanced stages of the disease, when RRT is
needed, choosing the optimal moment and the type of treatment are
decisions that should be taken by the physician together with the
patient and his/her family members and individually adapted to the
needs of each patient.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Due to confidentiality reasons data generated or
analyzed during this study are not included in this published
article.
Authors' contributions
DT, DD, AEBS, DGB, OS and DI designed the study,
analysed and interpreted datasets and wrote the manuscript. MDT and
LM collected the data and analysed the datasets. DT, DD, AEBS, DGB,
OS, DI, LR and CRJ performed a literature search and selected the
studies to be included. DT, DD, AEBS, DGB, OS and DI critically
revised the manuscript. All authors read and approved the final
manuscript. The contributions of all the authors on this article
are greatly valued and appreciated.
Ethics approval and consent to
participate
This study was approved by Ethics Committee of the
Emergency University Hospital of Bucharest (Romania). Written
informed consent was obtained from all patients prior to
publication.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Zilisteanu DS: Chronic kidney disease, a
major public health problem. Rom Med J. 70:18–26. 2013.
|
|
2
|
Piccoli GB, Alrukhaimi M, Liu ZH,
Zakharova E and Levin A: World Kidney Day Steering Committee. What
we do and do not know about women and kidney diseases; questions
unanswered and answers unquestioned: Reflection on World Kidney Day
and International Woman's Day. BMC Nephrol. 19(66)2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Wavamunno MD and Harris DC: The need for
early nephrology referral. Kidney Int Suppl. 67:S128–S132.
2005.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Balcangiu-Stroescu AE, Tanasescu MD,
Diaconescu A, Raducu L, Constantin AM, Balan DG, Tarmure V and
Ionescu D: Cardiovascular comorbidities, inflammation and serum
albumin levels in a group of hemodialysis patients. Rev Chim
Buchar. 69:926–929. 2018.
|
|
5
|
Francu V: Inequities in addressability and
accessibility of vulnerable groups to health care services.
Transilv Acta Med. 2:174–176. 2013.
|
|
6
|
Balan DG, Balcangiu Stroescu AE, Tanasescu
MD, Diaconescu A, Raducu L, Mihai A, Tanase M, Stanescu II and
Ionescu D: nutritional intervention in patients with diabetic renal
disease - A brief presentation. Rev Chim Buchar. 69:4078–4082.
2018.
|
|
7
|
Balcangiu Stroescu AE, Tanasescu MD,
Diaconescu A, Raducu L, Balan DG, Mihai A, Tanase M, Stanescu II
and Ionescu D: Diabetic nephropathy: A concise assessment of the
causes, risk factors and implications in diabetic patients. Rev
Chim Buchar. 69:4018–4021. 2018.
|
|
8
|
Mandita A, Timofte D, Balcangiu-Stroescu
AE, Balan D, Raducu L, Tanasescu MD, Diaconescu A, Dragos D,
Cosconel CI, Stoicescu SM, et al: Treatment of high blood pressure
in patients with chronic renal disease. Rev Chim Buchar.
70:993–995. 2019.
|
|
9
|
Fervenza FC: Nephrosclerosis. Medscape,
2018. https://emedicine.medscape.com/article/244342-overview.
Accessed September 19, 2019.
|
|
10
|
August P: Hypertension in men. J Clin
Endocrinol Metab. 84:3451–3454. 1999.PubMed/NCBI View Article : Google Scholar
|
|
11
|
O'Shaughnessy MM, Hogan SL, Thompson BD,
Coppo R, Fogo AB and Jennette JC: Glomerular disease frequencies by
race, sex and region: Results from the International Kidney Biopsy
Survey. Nephrol Dial Transplant. 33:661–669. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Klahr S: Obstructive nephropathy. Intern
Med. 39:355–361. 2000.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ishikawa I, Maeda K, Nakai S and Kawaguchi
Y: Gender difference in the mean age at the induction of
hemodialysis in patients with autosomal dominant polycystic kidney
disease. Am J Kidney Dis. 35:1072–1075. 2000.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Malliara M: The management of hypertension
in hemodialysis and CAPD patients. Hippokratia. 11:171–174.
2007.PubMed/NCBI
|
|
15
|
Inaguma D, Koide S, Takahashi K, Hayashi
H, Hasegawa M and Yuzawa Y: Relationship between history of
coronary heart disease at dialysis initiation and onset of events
associated with heart disease: A propensity-matched analysis of a
prospective cohort study. BMC Nephrol. 18(79)2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Charytan D: Is left ventricular
hypertrophy a modifiable risk factor in end-stage renal disease.
Curr Opin Nephrol Hypertens. 23:578–585. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Segall L, Nistor I and Covic A: Heart
failure in patients with chronic kidney disease: A systematic
integrative review. BioMed Res Int. 2014(937398)2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Murray AM, Seliger S, Lakshminarayan K,
Herzog CA and Solid CA: Incidence of stroke before and after
dialysis initiation in older patients. J Am Soc Nephrol.
24:1166–1173. 2013.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Plantinga LC, Fink NE, Coresh J, Sozio SM,
Parekh RS, Melamed ML, Powe NR and Jaar BG: Peripheral vascular
disease-related procedures in dialysis patients: Predictors and
prognosis. Clin J Am Soc Nephrol. 4:1637–1645. 2009.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Tanaka A, Inaguma D, Shinjo H, Murata M
and Takeda A: Aichi Cohort Study of Prognosis in Patients Newly
Initiated into Dialysis (AICOPP) Study Group. Asami Takeda the
Aichi cohort study of prognosis in patients newly initiated into
dialysis (AICOPP) study group, presence of atrial fibrillation at
the time of dialysis initiation is associated with mortality and
cardiovascular events. Nephron. 132:86–92. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Laslo C, Pantea Stoian A, Socea B,
Paduraru D, Bodean O, Socea L, Neagu TP, Stanescu AMA, Marcu D and
Diaconu C: New oral anticoagulants and their reversal agents. J
Mind Med Sci. 5:195–201. 2018.
|
|
22
|
Tica OA, Tica O, Antal L, Hatos A, Popescu
MI, Pantea Stoian A, Bratu OG, Gaman MA, Pituru SM and Diaconu CC:
Modern oral anticoagulant treatment in patients with atrial
fibrillation and heart failure: Insights from the clinical
practice. Farmacia. 66:972–976. 2018.
|
|
23
|
Gaman MA, Dobrica EC, Pascu EG, Cozma MA,
Epingeac ME, Gaman AM, Pantea Stoian A, Bratu OG and Diaconu CC:
Cardiometabolic risk factors for atrial fibrillation in type 2
diabetes mellitus: Focus on hypertension, metabolic syndrome and
obesity. J Mind Med Sci. 6:157–161. 2019.
|
|
24
|
Giannelli SV, Graf CE, Herrmann FR, Michel
JP, Patel KV, Pizzarelli F, Ferrucci L and Guralnik J: Natural
history of older adults with impaired kidney function: The
InCHIANTI study. Rejuvenation Res. 14:513–523. 2011.PubMed/NCBI View Article : Google Scholar
|
|
25
|
European Best Practice Guidelines for
Haemodialysis. (Part 1). Section I. Measurement of renal function,
when to refer and when to start dialysis. Nephrol Dial Transplant.
17:7–15. 2002.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Jones C, Roderick P, Harris S and Rogerson
M: Decline in kidney function before and after nephrology referral
and the effect on survival in moderate to advanced chronic kidney
disease. Nephrol Dial Transplant. 21:2133–2143. 2006.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Chan CT, Blankestijn PJ, Dember LM,
Gallieni M, Harris DCH, Lok CE, Mehrotra R, Stevens PE, Wang AY,
Cheung M, et al: Conference Participants: Dialysis initiation,
modality choice, access, and prescription: conclusions from a
Kidney Disease: Improving Global Outcomes (KDIGO) Controversies
Conference. Kidney Int. 96:37–47. 2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Xue H, Ix JH, Wang W, Brunelli SM, Lazarus
M, Hakim R and Lacson E Jr: Hemodialysis access usage patterns in
the incident dialysis year and associated catheter-related
complications. Am J Kidney Dis. 61:123–130. 2013.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Kurella Tamura M, O'Hare AM, McCulloch CE
and Johansen KL: Signs and symptoms associated with earlier
dialysis initiation in nursing home residents. Am J Kidney Dis.
56:1117–1126. 2010.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Abra G and Kurella Tamura M: Timing of
initiation of dialysis: Time for a new direction? Curr Opin Nephrol
Hypertens. 21:329–333. 2012.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Liang CC, Chou CY, Chang CT, Wang IK and
Huang CC: Upper gastrointestinal bleeding as a risk factor for
dialysis and all-cause mortality: A cohort study of chronic kidney
disease patients in Taiwan. BMJ Open. 6(e010439)2016.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Karaboyas A, Morgenstern H, Waechter S,
Fleischer NL, Vanholder R, Jacobson SH, Sood MM, Schaubel DE, Inaba
M, Pisoni RL, et al: Low hemoglobin at hemodialysis initiation: An
international study of anemia management and mortality in the early
dialysis period. Clin Kidney J. sfz065:2019.
|
|
33
|
Kwon YE, Kee YK, Yoon CY, Han IM, Han SG,
Park KS, Lee MJ, Park JT, Han SH, Yoo TH, et al: Change of
nutritional status assessed using subjective global assessment is
associated with all-cause mortality in incident dialysis patients.
Medicine (Baltimore). 95(e2714)2016.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Pandya V, Rao A and Chaudhary K: Lipid
abnormalities in kidney disease and management strategies. World J
Nephrol. 4:83–91. 2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Yang WL, Zhu XY, Zhu N, Su CY, Han QF,
Wang T and Zhang AH: What's the optimal lipids level for dialysis
patients? A cohort study from a Chinese dialysis center in a
university hospital. PLoS One. 11(e0167258)2016.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Hafeez E, Raza H, Khan RU, Anwar MA,
Hussain T and Beg MA: CKD-MBD spectrum at the time of initiation of
hemodialysis in Pakistani chronic kidney disease patients. Saudi J
Kidney Dis Transpl. 26:823–826. 2015.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Soohoo M, Feng M, Obi Y, Streja E, Rhee
CM, Lau WL, Wang J, Ravel VA, Brunelli S, Kovesdy CP, et al:
Changes in markers of mineral and bone disorders and mortality in
incident hemodialysis patients. Am J Nephrol. 43:85–96.
2016.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Komaba H, Igaki N, Takashima M, Goto S,
Yokota K, Komada H, Takemoto T, Kohno M, Kadoguchi H, Hirosue Y, et
al: Calcium, phosphorus, cardiovascular events and all-cause
mortality in hemodialysis patients: A single-center retrospective
cohort study to reassess the validity of the Japanese Society for
Dialysis Therapy guidelines. Ther Apher Dial. 12:42–48.
2008.PubMed/NCBI View Article : Google Scholar
|