Introduction
The majority of patients with avascular necrosis
(AVN) of the femoral head (hip) experience collapse of the
subchondral bone, leading to osteoarthritis (1,2). Due to
this, the preservation of the femoral head in the early stages of
osteonecrosis is a primary objective. However, to the best of our
knowledge, a consensus regarding the best approach to this is
lacking.
Surgical intervention is more effective when it is
performed prior to the collapse of the femoral head, especially in
patients <48 years old (3). For
AVN, treatment strategies include subchondral bone drilling, core
decompression, vascularized bone-grafting, femoral osteotomy,
surface replacement and total hip arthroplasty (THA) (4). However, these treatment options have a
number of limitations. Core decompression results in a deficiency
of subchondral plate support for the weight load, leading to
inconsistent outcomes (5).
Vascularized fibular grafting is limited by the morbidity
associated with graft harvest and additional time required for
surgery and potential complications during rehabilitation (6). Pain, infection and a loose association
with a prosthetic are limiting factors for hip arthroplasty
(7).
A proposed alternative for AVN is a porous tantalum
rod, which is a biomaterial used to support the subchondral bone of
the femoral head, providing advantageous physical and mechanical
properties. The modulus of elasticity of the implant is 3 GPa,
which is between that of subchondral bone (1.5 GPa) and cortical
bone (15 GPa) (8). Additionally, it
is significantly less than that of a titanium alloy (110 GPa),
which minimizes stress shielding (8). The surface of the rod has a high-volume
porosity (75-80%) with interconnected pores (mean; 430 µm) similar
to bone, allowing for primary stability and rapid bone in-growth
(9). Soft tissue has been indicated
to grow on the rod for 4 weeks post-implantation in an animal model
(10). Additionally, a biomechanical
fatigue test demonstrated that the rod can bear 4-fold the
bodyweights of humans and has an intensity that is 9.3-fold greater
than the pressure it resists post-implantation, permitting
physiological load-bearing (11,12). A
previous study has suggested that beneficial results can be
achieved in patients with an integral head outline (13).
Therefore, the purpose of the present study was to
evaluate the clinical results and survival rates of patients fitted
with the porous tantalum rod system, which was used to treat
early-stage osteonecrosis of the femoral head.
Materials and methods
Demographics
The present study was approved by the Ethics
Committee of the Institutional Review Board of the Affiliated
Hospital of Qingdao University. Written informed consent was
obtained from all patients whose specimens and clinical information
were used for the present study.
The inclusion criteria were as follows: i) Diagnosis
of early non-traumatic AVN of the femoral head; and ii) the ability
to withstand surgery. The exclusion criteria were as follows: i) A
history of metal allergy; ii) an infection in the hip or another
part of the body; and/or iii) previous hip surgery.
A total of 60 patients (82 hips) who had received
treatment between June 2010 and March 2015 in the Affiliated
Hospital of Qingdao University were retrospectively selected for
analysis. Patients included in the study had AVN of the femoral
head with normal morphology and joint space and were classified as
Ficat stage I or II (14,15). The patients' reported symptoms
included hip pain, limp, limited range of motion and hip
dysfunction. Changes in the density of the subchondral bone was
discernible by radiographic evaluation and the configuration of the
femoral heads were intact. None of the patients had undergone any
prior treatment for osteonecrosis. The risk factors for AVN
included corticosteroid application, excessive alcohol consumption
and trauma.
X-ray and MRI scans of the hip joint were used to
diagnose and stage AVN of the femoral head according to the Ficat
classification. Considering economic cost, all patients were
evaluated by x-ray during the follow-up.
The patients were classified into two groups based
on the treatment they requested: The non-surgical treatment group
and the surgical treatment group. The non-surgical treatment group
included 30 patients (41 hips; 26 males and 4 females) with a mean
age of 48.1 years (31-61 years). A total of 7 patients exhibited
Ficat stage I and 23 exhibited stage II. A total of 19 cases (8
left side, 11 right side) exhibited ipsilateral disease and 11
patients exhibited bilateral disease. The surgical group included
30 patients (41 hips; 26 males and 4 females) with a mean age of
44.2 years (23-68 years). Of these patients, 10 were classified as
Ficat stage I and 20 as stage II. A total of 21 patients received a
porous tantalum implant on one side (9 left side, 12 right side)
and 9 received the implant bilaterally.
Treatment
In the non-surgical treatment group, celecoxib,
salvia miltiorrhiza and tetramethylypyrazine were applied.
The total course of the treatment was 6 weeks. Celecoxib (Pfizer,
Inc.) was orally administered at a dose of 200 mg/day for 6 weeks
for analgesia during the entire course. Additionally, 10 ml
Salvia miltiorrhiza (Sanhome Pharmaceutical Co, Ltd.) and 20
mg tetramethylypyrazine (Zhengzhou Cheuk-Fung pharmaceutical Co.,
Ltd.) diluted with 500 ml of 10% glucose was concurrently
administered intravenously daily for 10 days. After another 2 weeks
of celecoxib treatment only, the regimen of Salvia
miltiorrhiza and 20 mg tetramethylypyrazine injection was
repeated for an additional 10 days. Patients were advised to walk
with two crutches to avoid full weight-bearing for at least three
months and to walk <1,000 m/day. Furthermore, patients were
asked to reduce their daily activities to limit hip movement.
In the surgical treatment group, necrotic bone was
located using x-ray prior to surgery. Epidural anaesthesia was
administered to 20 patients with ropivacaine (Humanwell Healthcare
Co., Ltd.) while the remaining 10 underwent endotracheal
anaesthesia with sevoflurane (Lunan Pharmaceutical Group, Co.,
Ltd.). Patients were placed in a supine position, where the
affected hip joint was disinfected with tincture of iodine followed
by deiodination with alcohol. A 4 cm longitudinal mid-lateral
incision was made from the tip of the greater trochanter towards
the femoral shaft. A 3.22 mm guidewire was drilled into the centre
of the osteonecrotic lesion to the level of subchondral bone using
fluoroscopic guidance, under which core compression was conducted
using cannulated reamers to enlarge the diameter of the tunnel to a
diameter of 10 mm. The osteonecrotic bone was removed with a
curette and the tunnel was irrigated. Following this, the length of
the guidewire was measured and the tunnel was tapped. A porous
tantalum rod (Trabecular Metal; Zimmer Biomet) with a diameter of
10 mm and a length of 70-140 mm was then inserted into the tunnel
reaching the subchondral bone with the lateral portion of the rod
abutting the lateral femoral cortex. The incision was closed in
layers and no drainage tube was inserted.
Rehabilitation protocol began the day following
surgery. To avoid weight-bearing, patients were allowed to walk
with crutches for 48 h post-surgery. Hips could be flexed to ~90˚
after three weeks. Patients were permitted to start physiotherapy
protocol and progress to full weight-bearing after fluoroscopic
confirmation of the integration of the implant and host bone.
Functional assessment
Patients received regular follow-up at the clinic.
Harris score (16), Ficat
classification (15), symptoms,
range of motion, activity and radiography were performed/determined
pre-operatively and during the follow-up period. Additionally, hip
survivorship, implant status and any complications were also
recorded during the follow-up period. Follow-up was performed once
every three months for the first year and twice per year following
that. In cases where the follow-up time of the patients were <24
months, for example 18 months, then Harris scores would be recorded
at 6 and 12 months up until the final follow-up time. Harris scores
would not be recorded at 24 and 36 months in which case, as these
patients are considered lost to follow up. Failure of the implant
and hips in the non-surgical treatment group served as an
indication for THA. Indications for THA included sustained pain and
dysfunction of the hips or dissatisfaction with either the surgical
or non-surgical treatment.
Statistical analysis
Statistical analysis of the data was performed using
SPSS 17.0 software (SPSS, Inc.). All continuous variables were
expressed as mean ± standard deviation (SD). An unpaired
t-test was used for the comparison of two groups. The
Kaplan-Meier method was used to analyse hip survivorship. The
difference between groups was determined using the log-rank test.
P<0.05 was considered to indicate a statistically significant
difference.
Results
In the non-surgical treatment group, 27 cases (37
hips) were followed up and 3 cases (4 hips) were lost to follow-up.
In the surgery group, 26 cases (36 hips) were followed up and 4
cases (5 hips) were lost to follow-up. The mean follow-up time was
33.5 months (range: 18-83 months). No difference in age was noted
between groups (P>0.05). The average surgical time for tantalum
rod implantation was 53 min (range; 40-80 min). The mean blood loss
was 80 ml (range; 50-150 ml) and no infusion was required. No
intra-operative or immediate post-operative complications occurred.
The mean total hospitalization time, including those recorded
before and after surgery, was 5 days (range; 3-7 days). No
complications, such as infection of the incision, delayed healing,
fracture or trochanteric bursitis, were recorded.
No difference in Harris score was identified between
the non-surgical treatment and tantalum rod implant groups before
treatment (P>0.05). Harris score increased at six months in the
surgical group and then gradually decreased until the final
follow-up (Table I). Significant
differences in Harris score existed between the two groups at each
stage of the follow-up (P<0.05).
 | Table IComparison of Harris scores before
and after treatmentsa. |
Table I
Comparison of Harris scores before
and after treatmentsa.
| Group | Prior to
surgery | 6 months | 12 months | 24 months | 36 months | Final
follow-upb |
|---|
| Non-surgical
group | 60.50±5.20 | 69.45±13.92 | 67.87±14.42 | 64.34±11.29 | 60.72±11.93 | 57.50±10.25 |
| Surgery | 61.20±5.00 | 86.06±11.59 | 83.83±10.61 | 78.95±12.34 | 72.71±13.15 | 68.63±17.11 |
| P-value | >0.05 | <0.05 | <0.05 | <0.05 | <0.05 | <0.05 |
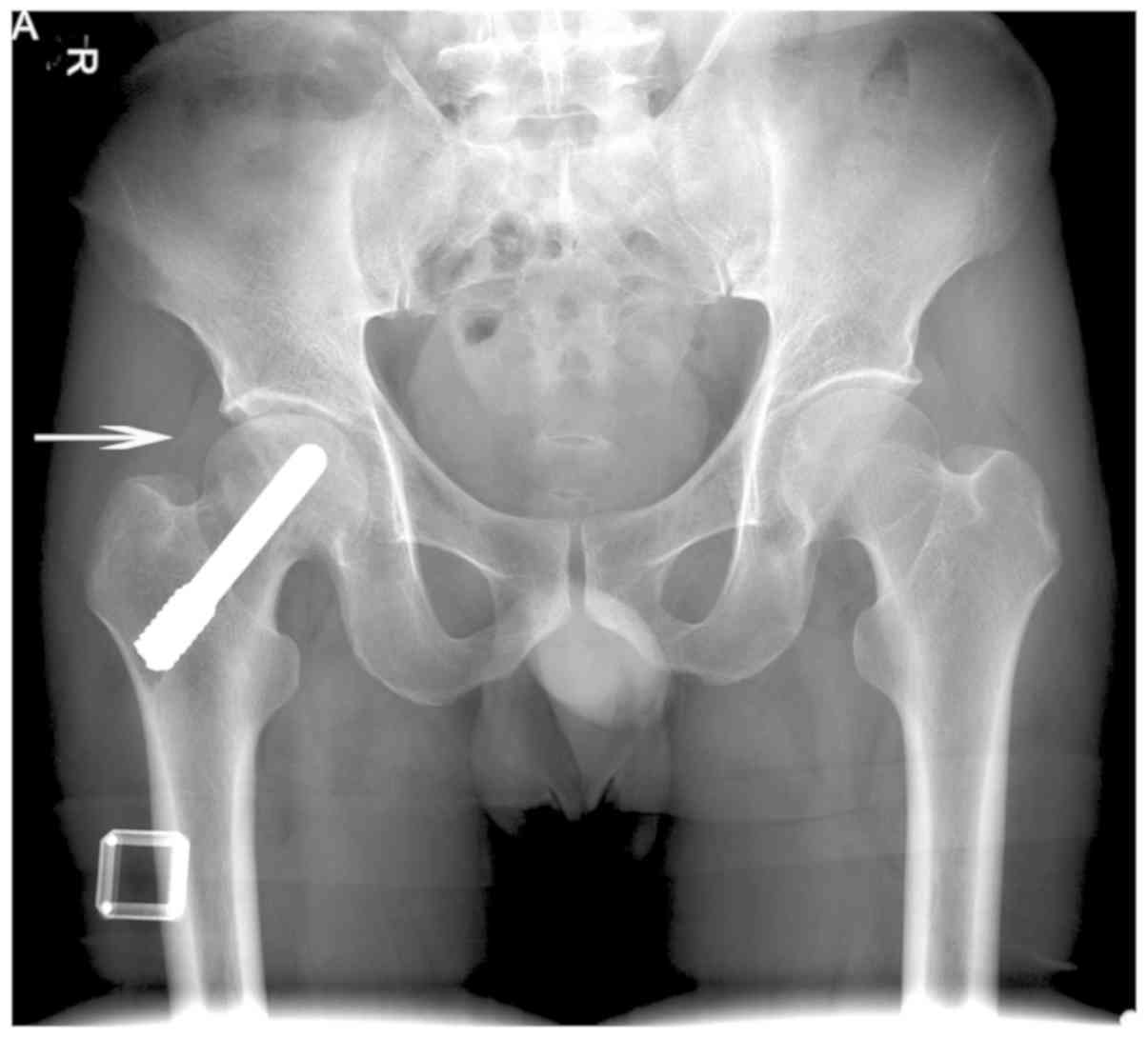
Radiographic results at 12 months post-treatment
revealed that 21 hips in the non-surgical treatment group exhibited
an intact femoral head outline and a normal joint gap (Fig. 1A). The head appeared to have
collapsed in the remaining 20 hips. In the surgical treatment
group, the position of the tantalum rod in 31 hips was unchanged 12
months post-operatively, with a normal femoral head outline
(Fig. 1B). However, partial collapse
of the head was noted in the remaining 10 hips. At the final
follow-up, only 5 hips in the non-surgical treatment group retained
a normal femoral head outline and collapse of the head and
narrowness of the joint gap were noted in the remaining 36
patients. THA was performed in 25 patients (28 hips) with Ficat
stage IV due to accelerated pain, collapse of the femoral head and
enlargement of the cyst region. In the surgical treatment group, 15
hips continued to exhibit normal implantation and a normal femoral
head (Fig. 2A). The femoral head
collapsed in the remaining 26 patients (Fig. 2B), including 4 patients (5 hips) who
later underwent THA (Fig. 2C).
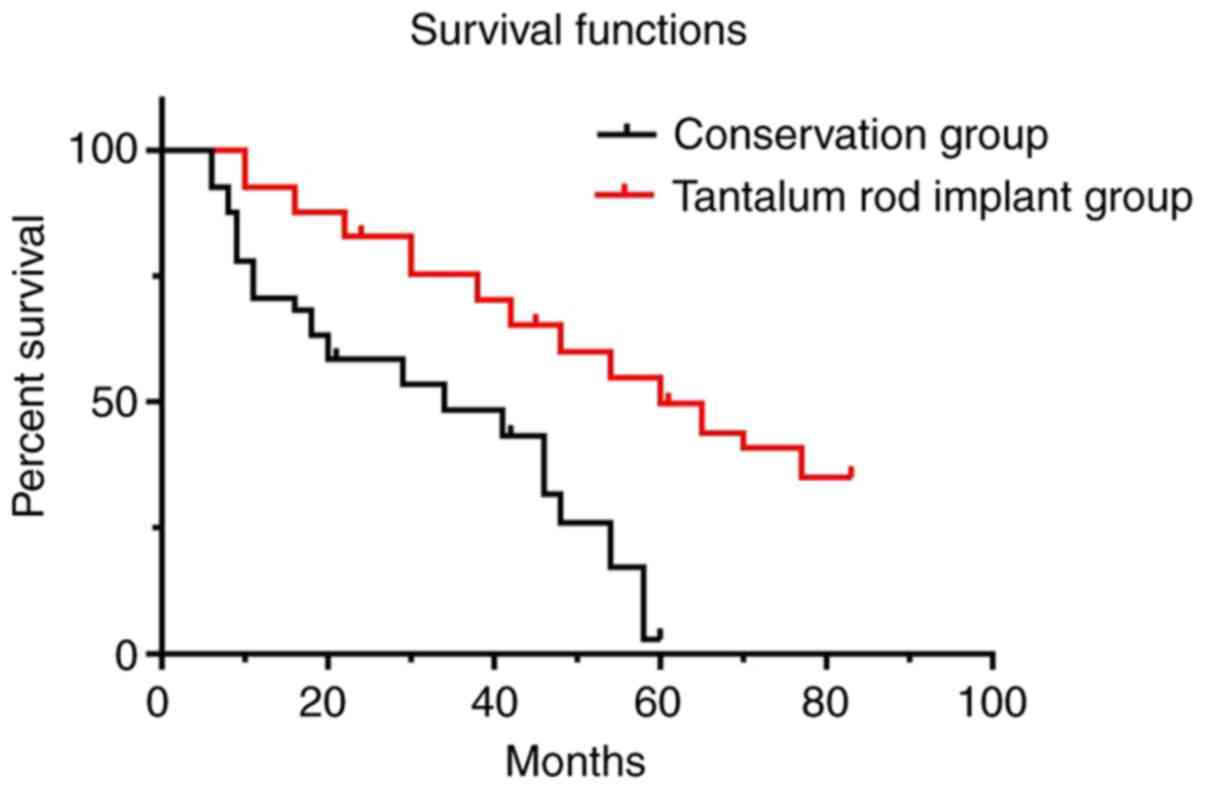
The significant differences between the two groups
were verified using the log-rank test (log rank=20.330;
P<0.001). The survival curve revealed that the survival rate of
the patients in the non-surgical treatment group and surgical
treatment group was 70.7 and 92.7% in the first year, respectively
and 48.8 and 75.6% after 3 years, respectively. Final follow-up
demonstrated a survival rate of 4.9% in the non-surgical treatment
group and 36.7% in the surgical treatment group (Fig. 3).
The mean delay from the first treatment to THA was
17.64±5.82 months (SD, months) in the non-surgical treatment group
and 42.38±9.35 months in the tantalum implantation group (Table II).
| Table IIMean delay from the first treatment
to THA. |
Table II
Mean delay from the first treatment
to THA.
| Group | Non-surgical
group | Surgical group | P-value |
|---|
| Time (months) | 17.64±5.85 | 42.38±9.35 | <0.001 |
Discussion
In the present study, the follow-up data of patients
with early AVN of the femoral head who received either non-surgical
treatment or tantalum rod implantation was retrospectively
analysed. The results indicated that porous tantalum rod
implantation improved hip joint function to a certain extent,
effectively delaying the requirement for THA caused by collapse of
the femoral head and the narrowing of the joint gap and did not
increase the risk of associated surgical complications.
Indications for THA treatment include collapse of
the femoral head and narrowing of the joint space, demonstrating
the importance of the outline of the femoral head (17). Therefore, the outline of the femoral
head and hip joint must be preserved prior to collapse of the
femoral head and subchondral plate, especially in patients <48
years old (18). Previous research
has indicated that a subchondral bone buttress may be effective in
halting or preventing the progression of osteonecrosis of the
femoral head (19). Due to their
minimally invasive characteristics, subchondral bone drilling and
decompression were popular means of treatment despite their
potential to weaken the cancellous bone within and adjacent to the
necrotic area (20).
Mechanical support of the femoral head is necessary
for weight-bearing and to delay disease progression, especially in
patients with early-stage disease (21). This understanding has led to the
development of bone transplant with or without blood supply and
free fibular transplantation to prevent femoral head collapse
(22). However, inconsistent effects
and clinical results, shortage of mechanical support and aggressive
secondary trauma has limited the achievement of satisfactory
results (23).
An advantage of the porous tantalum rod is that the
implant is minimally invasive and avoids the morbidity associated
with vascularized and non-vascularized bone-grafting strategies,
such as extensive surgical procedures, protected weight-bearing or
risk of disease transmission (24).
Veillette et al (25)
evaluated the results of the tantalum rod in 44 patients (60 hips;
mean age; 35 years) with a mean follow-up period of 24 months.
According to the Steinberg classification (26), 1 hip (2%) was classified as stage I,
49 hips (84%) were classified as stage II and 8 (14%) hips were
classified as stage III. The overall survivorship rates were 91.8%
at 12 months, 81.7% at 24 months and 68.1% at 48 months. A total of
9 hips (15.5%) were converted to THA. Shuler et al (27) compared the results between
vascularized fibular grafts and tantalum rod implants. No patient
required patient-controlled analgesia or transfusion. In the
tantalum implant group, the mean blood loss and operative time were
reduced compared with those in the fibular graft group. All
surviving implants (86%) resulted in good to excellent outcomes.
Kaplan-Meier analysis at 39 months revealed 86 and 67% survivorship
rates for implant and fibular grafts, respectively. A modified
technique, including bone marrow mesenchymal stem cells and
vascularized iliac grafting with a tantalum rod, was used in 24
patients with end-stage necrosis of the femoral head. After 64.35
months of follow-up, only five hips were converted to THA. The
success rate of this method was 89.47% for the Association Research
Circulation Osseous (ARCO) stage III and 75% for ARCO stage IV
(28). A further study used a 3D
finite element method to compare the tantalum rod with fibula
implantation and the core decompression model (29). When the tantalum rod was inside the
osteonecrotic area, shortening the implant or fibula implant
reduced the collapse values of the femoral head when the necrotic
area was large (120˚). A meta-analysis of clinical trials for
porous tantalum rod implantation, including six randomized
controlled trials and controlled clinical trials with 256 patients,
was performed to analyse the efficacy and safety of the procedure
compared with vascularized or non-vascularized bone grafting
(30). The results revealed that
this less invasive method was more effective and tolerable in
early-stage patients with a necrotic femoral head, with the
advantages of a better Harris score, a significantly reduced
incidence of femoral head collapse and reduced blood loss (30). These data demonstrated that a
tantalum rod can provide structural support for the subchondral
bone, in addition to core decompression and bone growth, due to the
porous nature of the tantalum.
In the present study, the terminal time point for
the final follow-up was established as collapse of the femoral
head, indicating failure of the mechanical support by the tantalum
implants and subchondral bone (31).
THA was not selected as the criterion because certain patients
would not accept the surgery, despite the presence of symptoms
including pain and hip dysfunction, due to the fear of surgery or
financial reasons. Due to this, the actual clinical results of the
tantalum rod implant could have been overestimated if THA was
selected as the failure criterion for survivorship analysis. In
fact, the mechanical role of the tantalum rod in supporting the
head was not applicable when collapse occurred.
Core decompression may be helpful to alleviate
symptoms after surgery (32). A
meta-analysis was employed to identify 22 studies using a single
surgical core decompression technique (33). A similar procedure identified 8
studies that treated patients non-surgically (34). The success rates for core
decompression were 84, 63 and 29% for Steinberg stages I, II and
III, respectively. Non-surgically treated patients with stage 0, I,
II and III (AVN) demonstrated success rates of 86, 61, 59 and 25%,
respectively. χ2-analysis revealed that the success rate
of core decompression was significantly increased compared with
that of non-surgical treatment for stage I hips only. A prospective
study compared core decompression with tantalum rod insertion in 60
patients. No favourable results were observed for the tantalum rod
compared with multiple small drill holes (35). An additional study assessed
survivorship and prognostic factors for radiographic progression
and conversion to THA after tantalum rod implantation (36). After a mean follow-up period of 44.8
months, 29.82% of the hips exhibited radiographic progression and
19.30% were converted to THA. The overall survivorship rate was
72.49% at 60 months post-operatively. Corticosteroid use and bone
marrow oedema were predictors of radiographic progression and bone
marrow oedema was an independent prognostic factor for conversion
to THA (36). Tantalum rods have
also been used in combination with intra-arterial infusion of
peripheral blood stem cells mobilized by granulocyte-colony
stimulating factor via the medial circumflex femoral artery
(37). The results revealed that
targeted intra-arterial infusion of stem cells could enhance the
efficacy of the tantalum rod.
In the present study, patient symptoms were
completely or partially alleviated after tantalum rod implantation,
indicating a benefit of core decompression prior to rod
implantation. Positive early clinical results were associated with
the survivorship of femoral head, reduced complications, sufficient
strength to allow physiological load-bearing capabilities and short
hospital stay. Transparent line, loosening, translocation or
abnormal bone density were not noted around the implant during the
follow-up, demonstrating the primary and secondary stability of the
rods. These results may be attributed to the notion that the
modulus of elasticity in the rod was similar to that of donor bone
and the distal threads of the rods and high frictional stability of
the implant prevent loosening. In addition, all the patients
included in the current study were classified as Ficat stage I or
II, indicating that the shape of the femoral head was relatively
normal without collapse. Collapse was not considered to be a
rational indication for tantalum rod implantation, given that the
rod itself does not provide the characteristics necessary for
repair or reconstruction.
The non-surgical treatments used in the present
study included medication and reduction in weight bearing. However,
it was difficult for certain patients to strictly follow the
strategy due to their reduced quality of life and daily activities,
especially walking with double crutches. Salvia miltiorrhiza
is thought to increase peripheral vascular flow, improve
microcirculation, inhibit thrombosis and enhance soft tissue repair
(38). This agent has been used in
TCM to treat hypertension, cervical spondylosis and AVN of the
femoral head (39). Similar
pharmacological activity has been reported for tetramethylpyrazine,
an ingredient derived from Ligusticum wallichii (40). This agent acts as a calcium channel
blocker and has been used in TCM to treat cerebral embolism,
insufficient cerebral blood supply and AVN of the femoral head with
positive results (41,42). However, the protective mechanism of
this drug in osteonecrosis remains unclear. Survivorship of the
affected femoral head in the non-surgical treatment group of the
current study was lower compared with that in the surgical
treatment group, indicating the poor results of non-surgical
treatment and the protective advantage of subchondral support.
However, the short- or mid-term protection for this implant and the
difficulties of prosthesis re-implantation requires further
analysis.
It was demonstrated in the present study that a
porous tantalum rod could, to some extent, preserve the structural
integrity of the femoral head and protect the subchondral bone
plate from collapse. However, there are a number of limitations to
tantalum rod implantation. Porous tantalum rod implantation is
suitable for patients with a small femoral head necrosis area.
Considering that a tantalum rod can only serve a point supporting
role (diameter; 10 mm), it is not suitable for patients with
multiple foci and a large necrosis area (43). Another disadvantage of the tantalum
rod is that it is expensive and as a foreign body implant, it may
require removal when deep tissue infection occurs which will
increase the risk of fracture (35).
After the failure of tantalum rod implantation, it was converted to
THA. Extracting a rod is technically demanding due to strong
osseointegration of the porous tantalum rod (10). Challenges inclu0de increased blood
loss, longer operative time, bone loss along the trajectory of the
rod and the subsequent potential increased risk of femoral fracture
(44,45). For this reason, additional data and
further prospective studies are required to support the conclusion
that tantalum rod implantation is more effective than bone
transplant or core decompression and to assess the risks, benefits
and financial issues for patients.
In conclusion, when compared with non-surgical
treatment, core decompression and porous tantalum rod implantation
are suitable treatment methods for AVN of the femoral head with
beneficial short- and mid-term results.
Acknowledgements
Not applicable.
Funding
The current study was supported by the National
Natural Science Foundation of China (grant no. 81672197).
Availability of data and materials
The data sets used and/or analysed during the
current study are available from the corresponding author on
reasonable request.
Authors' contributions
HZ and YW designed the study. YF, CD and YW
participated in the acquisition of samples and clinical data. CD
and YF performed statistical analysis. YF drafted the manuscript.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the Institutional Review Board of the Affiliated
Hospital of Qingdao University (approval no. QYFYKYLL 2010-09;
Qingdao, China). Written informed consent was obtained from all
patients whose specimens and clinical information were used for the
current study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Babis GC, Sakellariou V, Parvizi J and
Soucacos P: Osteonecrosis of the femoral head. Orthopedics.
34(39)2011.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mont MA, Jones LC and Hungerford DS:
Nontraumatic osteonecrosis of the femoral head: Ten years later. J
Bone Joint Surg Am. 88:1117–1132. 2006.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Amanatullah DF, Strauss EJ and Di Cesare
PE: Current management options for osteonecrosis of the femoral
head: Part II, operative management. Am J Orthop (Belle Mead NJ).
40:E216–E225. 2011.PubMed/NCBI
|
|
4
|
Rajpura A, Wright AC and Board TN: Medical
management of osteonecrosis of the hip: A review. Hip Int.
21:385–392. 2011.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Malizos KN, Karantanas AH, Varitimidis SE,
Dailiana ZH, Bargiotas K and Maris T: Osteonecrosis of the femoral
head: Etiology, imaging and treatment. Eur J Radiol. 63:16–28.
2007.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Tripathy SK, Goyal T and Sen RK:
Management of femoral head osteonecrosis: Current concepts. Indian
J Orthop. 49:28–45. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Jones CA and Pohar S: Health-Related
quality of life after total joint arthroplasty: A scoping review.
Clin Geriatr Med. 28:395–429. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Lee GW, Park KS, Kim DY, Lee YM,
Eshnazarov KE and Yoon TR: Results of total hip arthroplasty after
core decompression with tantalum rod for osteonecrosis of the
femoral head. Clin Orthop Surg. 8:38–44. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Zhang X, Wang J, Xiao J and Shi Z: Early
failures of porous tantalum osteonecrosis implants: A case series
with retrieval analysis. Int Orthop. 40:1827–1834. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Fernandez-Fairen M, Murcia A, Iglesias R,
Sevilla P, Manero JM and Gil FJ: Analysis of tantalum implants used
for avascular necrosis of the femoral head: A review of five
retrieved specimens. J Appl Biomater Funct Mater. 10:29–36.
2012.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Floerkemeier T, Thorey F, Daentzer D,
Lerch M, Klages P, Windhagen H and von Lewinski G: Clinical and
radiological outcome of the treatment of osteonecrosis of the
femoral head using the osteonecrosis intervention implant. Int
Orthop. 35:489–495. 2011.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Liu G, Wang J, Yang S, Xu W, Ye S and Xia
T: Effect of a porous tantalum rod on early and intermediate stages
of necrosis of the femoral head. Biomed Mater.
5(065003)2010.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Nadeau M, Seguin C, Theodoropoulos JS and
Harvey EJ: Short term clinical outcome of a porous tantalum implant
for the treatment of advanced osteonecrosis of the femoral head.
Mcgill J Med. 10:4–10. 2007.PubMed/NCBI
|
|
14
|
Schmitt-Sody M, Kirchhoff C, Mayer W,
Goebel M and Jansson V: Avascular necrosis of the femoral head:
Inter- and intraobserver variations of ficat and ARCO
classifications. Int Orthop. 32:283–287. 2008.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Jawad MU, Haleem AA and Scully SP: In
brief: Ficat classification: Avascular necrosis of the femoral
head. Clin Orthop Relat Res. 470:2636–2639. 2012.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ovre S, Sandvik L, Madsen JE and Roise O:
Comparison of distribution, agreement and correlation between the
original and modified merle d'Aubigne-Postel score and the harris
hip score after acetabular fracture treatment: Moderate agreement,
high ceiling effect and excellent correlation in 450 patients. Acta
Orthop. 76:796–802. 2005.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Lieberman JR, Engstrom SM, Meneghini RM
and SooHoo NF: Which factors influence preservation of the
osteonecrotic femoral head? Clin Orthop Relat Res. 470:525–534.
2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Zalavras CG and Lieberman JR:
Osteonecrosis of the femoral head: Evaluation and treatment. J Am
Acad Orthop Surg. 22:455–464. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Microsurgery Department of the Orthopedics
Branch of the Chinese Medical Doctor Association, Group from the
Osteonecrosis, Bone Defect Branch of the Chinese Association of
Reparative, Reconstructive Surgery, Microsurgery and Reconstructive
Surgery Group of the Orthopedics Branch of the Chinese Medical
Association: Chinese guideline for the diagnosis and treatment of
osteonecrosis of the femoral head in adults. Orthop Surg 9: 3-12,
2017.
|
|
20
|
Lavernia CJ and Sierra RJ: Core
decompression in atraumatic osteonecrosis of the hip. J
Arthroplasty. 15:171–178. 2000.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Lv H, Zhang L, Yang F, Zhao Z, Yao Q,
Zhang L and Tang P: Comparison of microstructural and mechanical
properties of trabeculae in femoral head from osteoporosis patients
with and without cartilage lesions: A case-control study. BMC
Musculoskelet Disord. 16(72)2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Aldridge JM III, Berend KR, Gunneson EE
and Urbaniak JR: Free vascularized fibular grafting for the
treatment of postcollapse osteonecrosis of the femoral head.
Surgical technique. J Bone Joint Surg Am. 86:87–101.
2004.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Wang BL, Sun W, Shi ZC, Zhang NF, Yue DB,
Guo WS, Shi SH and Li ZR: Treatment of nontraumatic osteonecrosis
of the femoral head using bone impaction grafting through a femoral
neck window. Int Orthopaedics. 34:635–639. 2010.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Tsao AK, Roberson JR, Christie MJ, Dore
DD, Heck DA, Robertson DD and Poggie RA: Biomechanical and clinical
evaluations of a porous tantalum implant for the treatment of
early-stage osteonecrosis. J Bone Joint Surg Am. 87:22–27.
2005.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Veillette CJ, Mehdian H, Schemitsch EH and
McKee MD: Survivorship analysis and radiographic outcome following
tantalum rod insertion for osteonecrosis of the femoral head. J
Bone Joint Surg Am. 88:48–55. 2006.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Plakseychuk AY, Shah M, Varitimidis SE,
Rubash HE and Sotereanos D: Classification of osteonecrosis of the
femoral head. Reliability, reproducibility, and prognostic value.
Clin Orthop Relat Res. 386:34–41. 2001.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Shuler MS, Rooks MD and Roberson JR:
Porous tantalum implant in early osteonecrosis of the hip:
Preliminary report on operative, survival, and outcomes results. J
Arthroplasty. 22:26–31. 2007.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Zhao D, Liu B, Wang B, Yang L, Xie H,
Huang S, Zhang Y and Wei X: Autologous bone marrow mesenchymal stem
cells associated with tantalum rod implantation and vascularized
iliac grafting for the treatment of end-stage osteonecrosis of the
femoral head. Biomed Res Int. 2015(240506)2015.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Shi J, Chen J, Wu J, Chen F, Huang G, Wang
Z, Zhao G, Wei Y and Wang S: Evaluation of the 3D finite element
method using a tantalum rod for osteonecrosis of the femoral head.
Med Sci Monit. 20:2556–2564. 2014.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Zhang Y, Li L, Shi ZJ, Wang J and Li ZH:
Porous tantalum rod implant is an effective and safe choice for
early-stage femoral head necrosis: A meta-analysis of clinical
trials. Eur J Orthop Surg Traumatol. 23:211–217. 2013.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Wang C, Meng H, Wang Y, Zhao B, Zhao C,
Sun W, Zhu Y, Han B, Yuan X, Liu R, et al: Analysis of early stage
osteonecrosis of the human femoral head and the mechanism of
femoral head collapse. Int J Biol Sci. 14:156–164. 2018.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Liu Y, Zhao D, Wang W, Zhang Y, Wang B and
Li Z: Efficacy of core decompression for treatment of canine
femoral head osteonecrosis induced by arterial ischaemia and venous
congestion. Hip Int. 27:406–411. 2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Castro FP Jr and Barrack RL: Core
decompression and conservative treatment for avascular necrosis of
the femoral head: A meta-analysis. Am J Orthop (Belle Mead NJ).
29:187–194. 2000.PubMed/NCBI
|
|
34
|
Arbab D and Konig DP: Atraumatic femoral
head necrosis in adults. Dtsch Arztebl Int. 113:31–38.
2016.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Miao H, Ye D, Liang W and Yao Y: Effect of
osteonecrosis intervention rod versus core decompression using
multiple small drill holes on early stages of necrosis of the
femoral head: A prospective study on a series of 60 patients with a
minimum 1 year-follow-up. Open Orthop J. 9:179–184. 2015.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Liu Y, Su X, Zhou S, Wang L, Wang C and
Liu S: A modified porous tantalum implant technique for
osteonecrosis of the femoral head: Survivorship analysis and
prognostic factors for radiographic progression and conversion to
total hip arthroplasty. Int J Clin Exp Med. 8:1918–1930.
2015.PubMed/NCBI
|
|
37
|
Mao Q, Wang W, Xu T, Zhang S, Xiao L, Chen
D, Jin H and Tong P: Combination treatment of biomechanical support
and targeted intra-arterial infusion of peripheral blood stem cells
mobilized by granulocyte-colony stimulating factor for the
osteonecrosis of the femoral head: A randomized controlled clinical
trial. J Bone Miner Res. 30:647–656. 2015.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Huang X, Jiang H, Liu D, Zhou Z and Wang
L: Implantation of calcium phosphate cement/danshen drug delivery
system for avascular necrosis of femoral head. Zhongguo Xiu Fu
Chong Jian Wai Ke Za Zhi. 22:307–310. 2008.PubMed/NCBI(In Chinese).
|
|
39
|
Jiang HJ, Huang XJ, Tan YC, Liu DZ and
Wang L: Core decompression and implantation of calcium phosphate
cement/danshen drug delivery system for treating ischemic necrosis
of femoral head at Stages I, II and III of antigen reactive cell
opsonization. Chin J Traumatol. 12:285–290. 2009.PubMed/NCBI
|
|
40
|
Fan Y, Tang L and He W: Clinical study on
the interventional treatment of non-traumatic femoral head mecrosis
by integrated traditional Chinese and western medicine. Zhongguo
Zhong Xi Yi Jie He Za Zhi. 19:605–606. 1999.PubMed/NCBI(In Chinese).
|
|
41
|
Jiang Y, Liu C, Chen W, Wang H, Wang C and
Lin N: Tetramethylpyrazine enhances vascularization and prevents
osteonecrosis in steroid-treated rats. Biomed Res Int.
2015(315850)2015.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Zheng SD and Wu HJ: Progress of studies on
effects of ligustrazine on blood vessel endothelium protection.
Zhongguo Zhong Xi Yi Jie He Za Zhi. 31:1004–1008. 2011.PubMed/NCBI(In Chinese).
|
|
43
|
Liu Y, Yan L, Zhou S, Su X, Cao Y, Wang C
and Liu S: Tantalum rod implantation for femoral head
osteonecrosis: Survivorship analysis and determination of
prognostic factors for total hip arthroplasty. Int Orthop.
40:1397–1407. 2016.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Olsen M, Lewis PM, Morrison Z, McKee MD,
Waddell JP and Schemitsch EH: Total hip arthroplasty following
failure of core decompression and tantalum rod implantation. Bone
Joint J. 98:1175–1179. 2016.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Cheng Q, Tang JL, Gu JJ, Guo KJ, Guo WS,
Wang BL and Zhao FC: Total hip arthroplasty following failure of
tantalum rod implantation for osteonecrosis of the femoral head
with 5- to 10 year follow-up. BMC Musculoskelet Disord.
19(289)2018.PubMed/NCBI View Article : Google Scholar
|