Introduction
Melanoma is a malignant tumor that derives from
melanocytes found in the basal layer of the epidermis but also in
other organs such as oral and nasal mucosa, uvea, vulvar and
anorectal mucosa, brain or gastrointestinal mucosa. Skin is the
commonest site of involvement of melanoma. Cutaneous melanoma is
the most aggressive skin cancer and a major cause of premature
death.
Based on epidemiologic studies, melanoma is the
sixth most common fatal malignancy in USA and the second most
common cancer in women aged between 20 and 29 years. Moreover, it
is considered that, in the future, almost one million of new
melanomas will be diagnosed every year in USA (1-3).
Melanoma risk factors include ultraviolet light
radiation from the sunlight but also from artificial sources of
lights such as tanning beds, history of sunburns in childhood or
adolescence, the number of congenital and acquired nevi and genetic
susceptibility or a family history of melanoma. Regarding
ultraviolet light radiation, melanoma developing risk is associated
with UV level and particularly UV-B, in case of sunlight exposure
or UV-A artificial light (3-6).
Regressive melanoma is a phenomenon characterized by
the partial or complete replacement of cutaneous melanoma by
fibrotic structures as a result of local host immune response
(7).
Cutaneous melanoma can be clinically described as an
asymmetric skin lesion with irregular border and color variation
from brown, dark brown, black or blue while the regression
phenomenon can be initially subtle and even unnoticed evolving from
hyperpigmentation to depigmentation of one or multiple parts of the
lesion resulting in blue, pink, white or gray areas.
Regarding the histologic criteria there is still no
standard definition of histopathologic aspects in regression of
primary melanoma. The histologic findings include variably dense
mononuclear infiltrate, melanophages, dermal fibrosis, epidermal
attenuation and dense vascularity in dermis. These histologic
changes are also seen in the absence of clinical regression
(8,9).
Some authors have classified regression in three
stages: Early stage of regression characterized by mononuclear
inflammatory cell infiltrate with mature lymphocytes and
keratinocyte and disruption of the dermal layer; the intermediate
stage with near complete absence of melanocytes, the presence of
melanophages, lymphohistiocytic infiltrate, fibroblastic
proliferation, mild collagen deposition and increased vascular
pattern in the superficial dermal layer; and the late stage
described as a lesion with complete absence of melanocytes,
fibrosis in the superficial/papillary dermis, ectatic capillaries,
variable numbers of melanophages and a small number of inflammatory
cells (10).
A rare case of regressive melanoma in a 62-year-old
female patient with no other general symptoms before the admission
to our clinic is presented.
Case report
We present the case of a 62-year-old female patient
who was referred to our clinic with a depigmented skin lesion with
areas of brown/black pigment in the middle, located on the left
cheek. The patient could not tell when the lesion first appeared,
but she confirmed the presence of a nodular hyperpigmented lesion
on the left cheek that started to bleed two years ago after a local
trauma. The depigmentation started three months earlier.
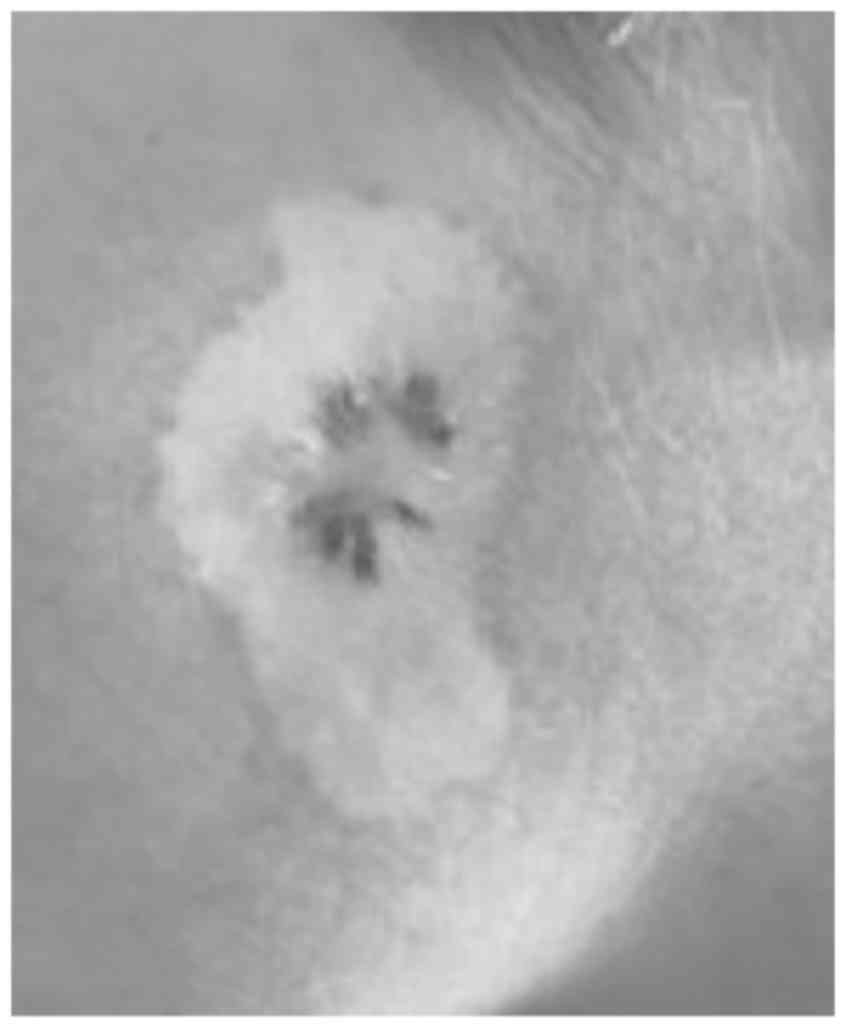
The clinical examination revealed a cutaneous 7/2 cm
asymmetric patch with large pink discolorations and a central
nodular, fibrotic pigmented area (Fig.
1). No ulceration, crusting or active bleeding was seen.
The general examination revealed multiple cervical
lymphadenopathy with the largest one measuring ~3/2 cm. The lymph
nodes were non-tender, firm in consistency, mobile and some were
matted together. Skin in the cervical area was normal, with no sign
of infiltration, inflammation or infection. No other lymph nodes
were detected by clinical examination.
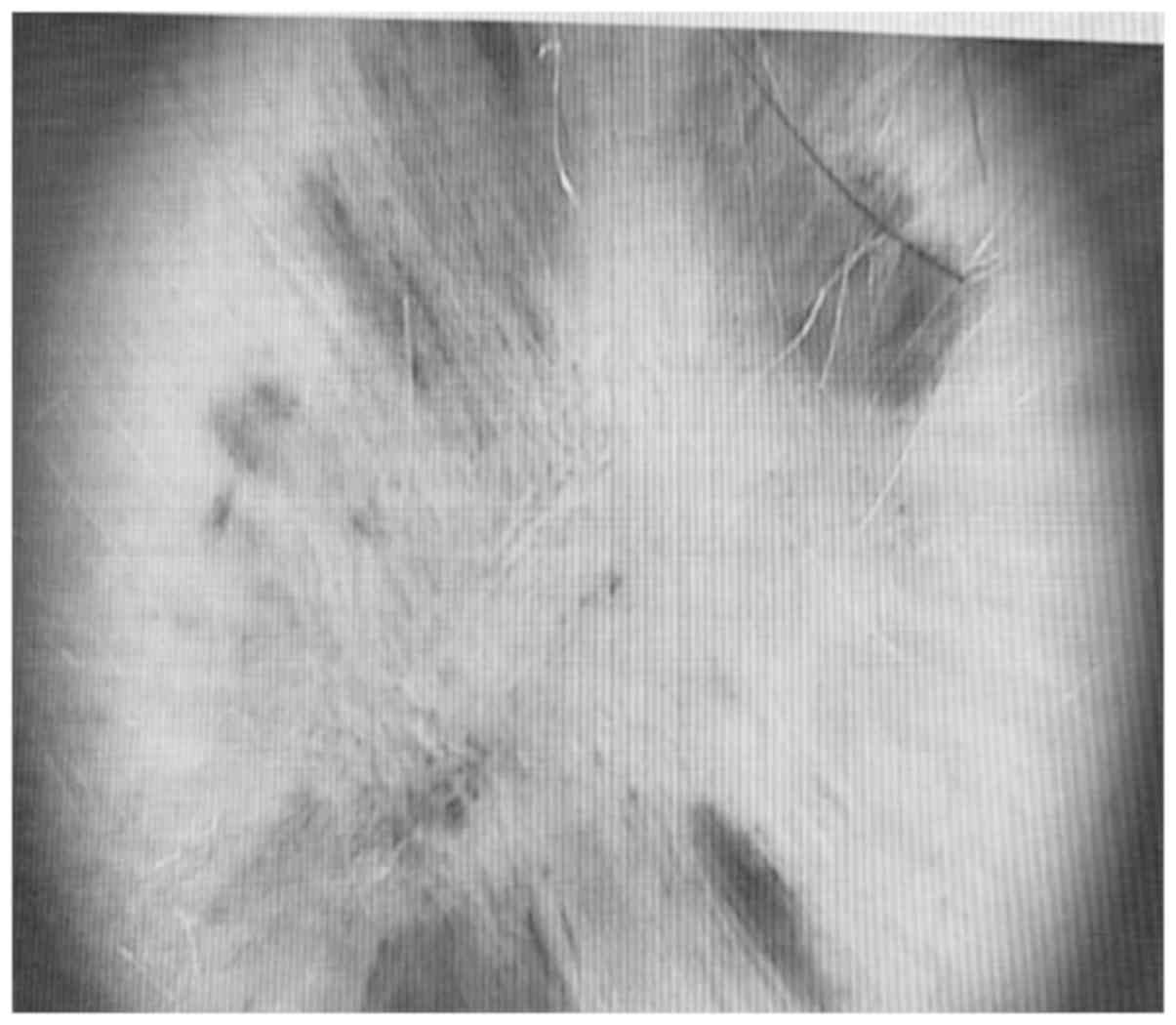
The dermoscopic examination revealed a massive
depigmentation and a central dark black pigmented area with blue
veil and scar-like depigmentation, and multiple dark brown
‘pepper-like’ dots in the middle of this structure (Fig. 2).
Due to its significant extension, it was decided to
perform a skin biopsy from the middle of the lesion in order to
encompass both pink depigmented area and dark-brown pigmented
skin.
The histologic examination revealed infiltrated
nodular dermal tissue with intense pigmented melanophages, dermal
fibrosis, vascular hyperplasia and flat epidermal layer. The
histopathologic changes correspond to the diagnosis of regressive
melanoma. The immunohistochemistry tests with Giemsa counterstain
on formalin fixed, paraffin embedded tissue sections were negative
for Melan A and Tyrosinase presence in dermal cellular infiltrate
and positive for S-100 in dispersed dendritic cells. It was also
observed that D2-40 was positive in the lymphatic endothelium and
did not show the presence of lymphatic tumor emboli while CD68 was
positive in dermal cellular infiltrate. The data supported the
diagnosis of regressive melanoma.
CT examination was performed revealing multiple
lymph node metastases together with lung and brain metastases. The
brain metastases were located supratentorial in both cerebral
hemispheres with axial diameter of 46/37 mm in right
fronto-parietal area and 36/35 mm in left frontal area, being
spontaneous and hyperdense (probably a bleeding process). No bones
metastases were seen.
Due to the advance stage of the disease, the patient
was admitted to the oncological department for palliative
treatment.
Discussion
Regression is a phenomenon that occurs as a result
of host immune response that attacks the primary melanocytic tumor
cells through lymphocytes determining a fibrotic process. The
mechanism of regression occurs in 35% of skin melanomas. Few cases
of fully regressive melanomas are described in the literature.
Regarding the metastatic sites, brain is the commonest with an
incidence of 91% in cutaneous melanoma due to the capacity of
tumoral cells to migrate along the external surfaces of vascular
channels without extravasation (11). The majority of regressive melanomas
were described after the occurrence of metastases, being one of the
reasons that regression is considered to be a negative prognostic
factor in melanoma (12).
There are some clinical studies that observed the
immunological mechanism implied in regressive phenomenon. It is
well known that cytotoxic T-cell response has an integral role in
the regression process of melanomas. Other molecules were also
identified in this process. A study outlined the high expression of
MxA which was found in inflamed melanoma. MxA is an antiviral
protein induced by type I interferon. Interferon also induces
chemokine IP10/CXCL10, CXCR3+ lymphocyte and granzyme
B+ lymphocytes. Collectively this evidence demonstrated
that cytotoxic immune response is implied in spontaneous regression
of melanoma (13). Another study
showed the involvement of cytotoxic immune response through the
correlation between expression of ICAM-1 and CD8+ cells
near tumor cells (14). The role of
interferon is sustained by the studies that confirmed the
appearance of regressive changes of melanomas after the treatment
with α interferon (15-18).
Regarding the dermoscopic changes in regressive
melanoma, Bories et al (19)
proposed seven criteria: ‘Scar-like’ depigmentation that can be
described as hypopigmented to pigmented macules, pink macules,
linear-irregular vessels, globular vessel pattern, hyperpigmented
macular remnants, blue-gray ‘peppered’ papular remnants and white
transverse bands.
The diagnosis of regressive melanoma is the same as
for primary cutaneous melanoma and set after histologic examination
on hematoxylin and eosin staining (20). Immunohistochemical test can also help
differentiate between benign and malignant tumor.
The management of regressive melanoma depends on
Breslow's thickness (the length from the granulosum stratum of
epidermis to the deepest margin of the tumor), number of mitosis
per square millimeter and ulceration, all helping to establish the
tumor stage and appropriate therapeutic management.
The authors consider that patient with fully or
partially regressive cutaneous melanoma should have the same
diagnosis and treatment management as primary cutaneous melanoma
(21-25).
In conclusion, regressive process of melanoma is a
rare phenomenon that is usually noticed after the onset of visceral
metastases. The immune mechanism is unclear but is considered that
cytotoxic T-cell response is part of the regressive process. The
prognosis of regressive melanomas is poor, mainly because most of
them are associated with lymph nodes or organ metastases. We
outlined this case because the patient was referred to dermatology
unit due to the pink macule and not for general symptoms. The
general examination showed the advance stage of the disease due to
numerous cervical adenopathy and their tendency towards confluence.
The brain CT showed cerebral metastases, so no curative treatment
could be offered.
Acknowledgements
Not applicable.
Funding
Not funding was received.
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors's contributions
AP contributed to the design of the case study. FS
was involved in the writing of the manuscript and was responsible
for the patient’s follow up based on clinical and imaging
examinations. CCD was responsible for the figures and was also
involved in the conception of the study. TC analyzed the data from
the literature research regarding regressive melanoma, and
contributed in the writing of the manuscript. TP examined the
patient and contributed in the writing of the manuscript regarding
the clinical and dermoscopic examination of the lesion. MMC
analyzed the histologic characteristics of regression and was
responsible for the writing of the relevant section. RCP analyzed
the melanoma risk factors and wrote the relevant section of the
manuscript. MCD was also involved in the conception and design of
the study, and contributed in the writing of the manuscript. All
authors critically revised the manuscript and approved the final
version of the manuscript to be published.
Ethics approval and consent to
participate
Written informed consent was provided by the
patient.
Patient consent for publication
The patient provided written informed consent for
the publication of the data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Losina E, Walensky RP, Geller A,
Beddingfield FC III, Wolf LL, Gilchrest BA and Freedberg KA: Visual
screening for malignant melanoma: A cost-effectiveness analysis.
Arch Dermatol. 143:21–28. 2007.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Rigel D: Cutaneous ultraviolet exposure
and its relationship to the development of skin cancer. J Am Acad
Dermatol. 58 (Suppl 2)(S129-S132)2008.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Food and Drug Administration: Consumer
health information November 2009. Available at: uriwww.fda.gov/consumer.https://www.fda.gov/consumer.
Accessed Feb 18, 2010.
|
|
4
|
Candido S, Rapisarda V, Marconi A,
Malaponte G, Bevelacqua V, Gangemi P, Scalisi A, McCubrey JA,
Maestro R, Spandidos DA, et al: Analysis of the B-RafV600E mutation
in cutaneous melanoma patients with occupational sun exposure.
Oncol Rep. 31:1079–1082. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Gandini S, Sera F, Cattaruzza MS, Pasquini
P, Picconi O, Boyle P and Melchi CF: Meta-analysis of risk factors
for cutaneous melanoma: II, Sun exposure. Eur J Cancer. 41:45–60.
2005.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Elwood JM and Jopson J: Melanoma and sun
exposure: An overview of published studies. Int J Cancer.
73:198–203. 1997.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ehrsam E, Kallini JR, Lebas D, Khachemoune
A, Modiano P and Cotten H: Fully regressive melanoma - a case
without metastasis. J Clin Aesthet Dermatol. 9:42–46.
2016.PubMed/NCBI
|
|
8
|
Smoller BR: Histologic criteria for
diagnosing primary cutaneous malignant melanoma. Mod Pathol. 19
(Suppl 2)(S34-S40)2006.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Zurac S, Negroiu G, Petrescu S, Andrei R,
Tebeica T, Popp C, Musţată R, Neagu M, Constantin C, Solovan C, et
al: Spectrum of morphologic alterations of regression in cutaneous
melanoma - potential for improving disease prognosis. Rom J Intern
Med. 50:145–153. 2012.PubMed/NCBI
|
|
10
|
Aung PP, Nagarajan P and Prieto VG:
Regression in primary cutaneous melanoma: Etiopathogenesis and
clinical significance. Lab Invest. 97:657–668. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Gugger A, Barnhill RL, Seifert B, Dehler
S, Moch H, Lugassy C, Marques-Maggio E, Rushing EJ and Mihic-Probst
D: Cutaneous melanoma with brain metastasis: Report of 193 patients
with new observations. PLoS One. 11(e0156115)2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Printz C: Spontaneous regression of
melanoma may offer insight into cancer immunology. J Natl Cancer
Inst. 93:1047–1048. 2001.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Wenzel J, Bekisch B, Uerlich M, Haller O,
Bieber T and Tüting T: Type I interferon-associated recruitment of
cytotoxic lymphocytes: A common mechanism in regressive melanocytic
lesions. Am J Clin Pathol. 124:37–48. 2005.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Håkansson A, Gustafsson B, Krysander L,
Hjelmqvist B, Rettrup B and Håkansson L: Expression of ICAM-1
during IFN-alpha-based treatment of metastatic malignant melanoma:
Relation to tumor-infiltrating mononuclear cells and regressive
tumor changes. J Interferon Cytokine Res. 19:171–177.
1999.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lupu M, Caruntu A, Caruntu C, Papagheorghe
LML, Ilie MA, Voiculescu V, Boda D, Constantin C, Tanase C, Sifaki
M, et al: Neuroendocrine factors: The missing link in non melanoma
skin cancer (Review). Oncol Rep. 38:1327–1340. 2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Sandru F, Popa A and Dumitrascu MC:
Dermoscopic view of vertical growth phase nodular malignant
melanoma. Med Image Database. 2:35–36. 2019. View Article : Google Scholar
|
|
17
|
Caruntu C, Boda D, Constantin C, Caruntu A
and Neagu M: Catecholamines increase in vitro proliferation of
murine B16F10 melanoma cells. Acta Endocrinol (Copenh). 10:545–558.
2014. View Article : Google Scholar
|
|
18
|
Boda D: Cellomics as integrative omics for
cancer. Curr Proteomics. 10:237–245. 2013. View Article : Google Scholar
|
|
19
|
Bories N, Dalle S, Debarbieux S, Balme B,
Ronger-Savlé S and Thomas L: Dermoscopy of fully regressive
cutaneous melanoma. Br J Dermatol. 158:1224–1229. 2008.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Prodea MC, Sandru F, Carpenco E, Gaje PN,
Horhat ID, Ceausu AR, Mederle N and Mederle OA: A rare sweat gland
tumour-immunohistochemical features. Rev Chim (Bucharest).
70:1863–1865. 2019. View Article : Google Scholar
|
|
21
|
Ilie MA, Caruntu C, Lupu M, Lixandru D,
Tampa M, Georgescu SR, Bastian A, Constantin C, Neagu M, Zurac SA,
et al: Current and future applications of confocal laser scanning
microscopy imaging in skin oncology. Oncol Lett. 17:4102–4111.
2019.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Stefan O, Tudor G, Constantinescu C, Luca
C, Boda D, Caruntu C, Cioplea M, Nichita L and Zurac SA: E-cadherin
and N-cadherin expression pattern in common melanocytic nevi.
Virchows Arch. 475(S28-S28)2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Neagu M, Constantin C, Tanase C and Boda
D: Patented biomarker panels in early detection of cancer. Recent
Pat Biomark. 1:10–24. 2011. View Article : Google Scholar
|
|
24
|
Zurac S, Neagu M, Constantin C, Cioplea M,
Nedelcu R, Bastian A, Popp C, Nichita L, Andrei R, Tebeica T, et
al: Variations in the expression of TIMP1, TIMP2 and TIMP3 in
cutaneous melanoma with regression and their possible function as
prognostic predictors. Oncol Lett. 11:3354–3360. 2016.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Diaconeasa A, Boda D, Solovan C, Enescu
DM, Vîlcea AM and Zurac S: Histopathologic features of Spitzoid
lesions in different age groups. Rom J Morphol Embryol. 54:51–62.
2013.PubMed/NCBI
|