Introduction
Levofloxacin is a third-generation fluoroquinolone
antibiotic with wide-spectrum and potent in vitro
antimicrobial activity against aerobic gram-negative and -positive
microorganisms (1). Levofloxacin
exhibits favorable pharmacokinetic (PK) and pharmacodynamic (PD)
features, including high bactericidal activity, good absorption,
high blood concentration, wide distribution, high tissue
permeability and bioavailability (2-4).
Levofloxacin is one of the major antimicrobial agents for the
treatment of community-acquired lower respiratory tract infections
(LRTIs) (5). The PK/PD parameters of
levofloxacin, including the peak serum concentration
(Cmax)/minimum inhibitory concentration (MIC) and area
under the concentration-time curve from time 0 to 24 h
(AUC0-24 h)/MIC, are closely associated with the
clinical efficacy, bacterial eradication and prevention of the
emergence of resistant bacteria in infectious diseases (6). Levofloxacin is used in clinical
practice worldwide, particularly for the treatment of
community-acquired pneumonia and acute exacerbation of chronic
bronchitis (7-10).
Pulmonary operation is a clean-contaminated surgery
(Altemeier Class II) and this procedure is likely to include
contamination of bacteria colonizing the tracheal or bronchial
mucosa, which is one of the major risk factors for peri-operative
infection (11). Antimicrobial
agents with good pathogen coverage and tissue penetration should be
considered to prevent post-operative infections in clinical
practice (12-20).
Therefore, it is beneficial to perform studies in patients
undergoing pulmonary operation who require antimicrobial agents to
prevent potential infections due to external bacterial infection
from an open airway and/or the colonizing microorganisms in the
respiratory tract.
The present study was designed to examine the PK
profiles and PK/PD of levofloxacin in bronchial mucosa and lung
tissue. Patients undergoing pulmonary operation and those who
required prophylactic antimicrobial therapy were included. All
patients received levofloxacin prophylactically prior to the
operation. The concentration of levofloxacin in the bronchial
mucosa and lung tissues was determined and PK/PD analysis was
performed using Monte Carlo simulation. The results provided
information regarding the levofloxacin concentration in pulmonary
tissues. An optimized dosing regimen allowing for the maximal
bactericidal effect to be achieved in vivo was also
recommended for patients with pulmonary disease.
Materials and methods
Study design
The present study was a randomized, single-center,
open-label clinical trial. The protocol was reviewed and approved
by the Ethics Committee of Huashan Hospital, Fudan University
(Shanghai, China; approval no. 66; 2006). All patients signed an
informed consent form prior to participation in the present study.
The study was performed in compliance with the ethical principles
outlined in the Declaration of Helsinki and all applicable
regulatory requirements. The procedure of the present study is
outlined in Table I. Since the study
was designed as a pharmacokinetic study to explore the penetration
of levofloxacin in tissue, it was not a comparative or controlled
study. According to the Guidance for Industry on Population
Pharmacokinetics released by the US Food and Drug Administration in
July 2019, the data indicating the outcome of patients and the
incidence of post-operative infections were not collected. The aim
of the present study was to investigate the PK of a single drug,
and therefore, no other drug was used for comparison.
 | Table IFlowchart of the study. |
Table I
Flowchart of the study.
| Procedure | Screening | Experiment |
|---|
| D-28 to D-2 | D-1 | D1 | D2 | D3 | D4 |
|---|
| Informed
consent | X | | | | | |
| Medical
history | X | X | | | | |
| Physical
examination | X | X | | | | X |
| Vital sign | X | X | X | | | X |
| Chest X-ray | X | | | | | |
| 12-lead ECG | X | X | | | | X |
| Body weight | X | X | | | | X |
| Inclusion/exclusion
criteria | X | X | | | | |
| Laboratory
tests | | | | | | |
|
Immunology | X | | | | | |
|
Hematology,
biochemistry, urinalysis | X | X | | | | X |
|
Endogenous
creatinine clearance rate | X | X | | | | X |
| Stay in
hospital | | X | X | X | X | X |
| Drug
administration | | | X | | | |
| Clinical
observation | X | X | X | X | X | X |
| Pharmacokinetic
evaluation | | | | | | |
|
Blood
sampling | | | X | X | | |
|
Tissue
sampling | | | X | X | | |
Participants
Recruitment of participants was performed in
Shanghai. Patients who received a pulmonary operation at Huashan
Hospital (Shanghai, China) due to pulmonary disease from June 2006
to June 2007 were enrolled according to the following inclusion
criteria: i) age, at least 18 years; ii) requirement of pulmonary
operation; and iii) voluntary agreement to participate and signing
of informed consent form prior to the study procedure. Patients
were excluded if they had severe pneumonia, moderate or severe
renal impairment, or clinically significant abnormal liver
function, which was defined as alanine aminotransferase or/and
aspartate aminotransferase >3-fold the upper limit of the normal
range (ULN) or total bilirubin >2-fold ULN. Creatinine clearance
(CLcr) was calculated according to the Cockcroft-Gault
formula (21):
Where BW is the body weight and Scr indicates serum
creatinine. Patients were excluded if they had a history of
hypersensitivity to fluoroquinolones or other drugs, or
photosensitivity, a history of epilepsy or other disorders of the
central nervous system, documented QT prolongation or severe
cardiac insufficiency. Pregnant or lactating females and patients
that were treated with levofloxacin or other fluoroquinolones
within 2 weeks prior to screening were also excluded from the
present study.
Study drug
Levofloxacin 500 mg tablets (lot no. 0506G03) were
provided by Daiichi Sankyo Co., Ltd.
Sample collection
The eligible patients were assigned randomly to one
of four groups (8 subjects/group) according to the time of
sampling. All patients received a single dose of 500 mg
levofloxacin orally prior to pulmonary operation. Blood samples
were collected prior to treatment, and at 1.5, 4, 8, 12 or 24 h
following treatment. The samples of lung tissue and bronchial
mucosa were collected at 4, 8, 12 or 24 h following treatment.
Detailed sampling time points for the collection of blood or tissue
samples are presented in Table II.
The present study did not have a negative control, as the aim of
the study was to observe PK of levofloxacin in the tissue and blood
of patients.
| Table IITime-points for collecting blood or
tissue samples from patients undergoing pulmonary operation. |
Table II
Time-points for collecting blood or
tissue samples from patients undergoing pulmonary operation.
| Group | Number of
subjects | Sampling
time-point |
|---|
| Blood | Lung tissue and
bronchial mucosa |
|---|
| 1 | 8 | Pre-dose, 1.5 h; 4
h post-dose | 4 h post-dose |
| 2 | 8 | Pre-dose, 1.5 h; 8
h post-dose | 8 h post-dose |
| 3 | 8 | Pre-dose, 1.5 h; 12
h post-dose | 12 h post-dose |
| 4 | 8 | Pre-dose, 1.5 h; 24
h post-dose | 24 h post-dose |
All enrolled patients received a pulmonary operation
due to lung cancer (n=23) or other pulmonary diseases, including
old tuberculoma (n=3), pulmonary granuloma (n=3), right lung
angioma, chronic cavity in right lower lobe, and bronchiectasis in
left lung (one each). The patients with peripheral lung cancer
received a lobectomy, and the patients with central type lung
cancer were sampled using a unilateral pneumonectomy. A sample of
lung tissue ~1 cm2 was collected from the external side
of the excised lung lobe and rinsed twice with normal saline. The
moisture on the surface was dried using a clean gauze. Bronchial
rings were excised from the residual end of lung cancer specimen in
patients with peripheral lung cancer, while adequate bronchial
mucosa was collected from the patients with central type lung
cancer to avoid tumor tissue. The bronchial mucosa samples were
rinsed using the same procedures used for lung tissue samples. The
samples of lung tissue and bronchial mucosa were sectioned into
pieces, and a fixed volume of 50 mmol/l
KH2PO4 buffer was added. Homogenate was
extracted using an ultrasonic homogenizer, and tissues were
centrifuged to harvest the supernatant. Blood samples were
heparinized and centrifuged at 4°C, 1,500 x g for 10 min
to separate plasma. All samples were stored in a refrigerator at
-40°C and in dark conditions until subsequent
analysis.
Levofloxacin assay and method
validation
High-performance liquid chromatography was used to
determine the concentration of levofloxacin in blood and tissue
samples. The method used has been reported in a previous study
(22). The analytical system
consisted of a high-performance liquid chromatographer Waters model
2690 equipped with a fluorescent detector (model 474; Waters
Corp.), which measured at wavelengths of 296 mm (excitation) and
504 nm (emission). The stationary phase was a TSK-gel ODS-80™
C18 column (4.6x150 mm; 5 µm; Tosoh Corporation). The
mobile phase consisted of 50 mmol/l KH2PO4
(pH 2.0)-tetrahydrofuran-1 mol/l acetonitrile (92/7/1; v/v/v). The
analysis was performed at a flow rate of 1.0 ml/min, a column
temperature of 35°C and an injection volume of 10 µl.
Compound DL-8493 was used as an internal control, which was
provided by Daiichi Sankyo Co., Ltd. The lower limit of
quantitation was 0.0100 µg/ml and the linear range was 0.01-5
µg/ml. The recovery of levofloxacin was 99.6±1.6%, 101.3±2.2% and
100.8±1.3% from plasma, lung tissue and bronchial mucosa,
respectively. For the plasma and buffer samples, the intra-day
relative standard deviation was ≤4.1 and ≤1.8%, while the inter-day
variability was ≤2.5 and ≤4.2%, respectively. The corresponding
accuracy was 96.1-101.9% and 96.2-103.1%.
PK evaluation
The PK parameters of levofloxacin in plasma, lung
and bronchial mucosa were obtained using non-compartment analysis.
The parameters included Cmax, peak time
(Tmax), AUC0-24, area under the
time-concentration curve from time zero to infinity
(AUC0-∞), half life
(T1/2), mean residence time until
24 h (MRT0-24), total apparent clearance
(CLt/F), apparent volume of distribution
(Vd/F), the ratio of Cmax in tissue vs.
plasma (RCmax), the ratio of levofloxacin
AUC0-24 in tissue vs. plasma (RAUC_0-24) and
the ratio of levofloxacin AUC0-∞ in tissue
vs. plasma (RAUC_0-∞), where the latter three
parameters reflect the permeability of levofloxacin in lung or
bronchial mucosa. Tmax is the time when levofloxacin
concentration reaches Cmax. The area under the
concentration-time curve AUC0-24 was calculated using
the trapezoidal method:
∑ni=1Ci+Ci+1
(ti+1-ti)/2, where
Ci and ti indicate the
concentration and time, respectively. The number of time-points (n)
was 5 for plasma and 4 for lung tissue and bronchial mucosa.
T1/2 is calculated as 0.693/λ,
where λ is the terminal elimination rate. MRT0-24 was
obtained as AUMC0-24/AUC0-24, where
AUMC0-24 is the integration of C x t vs.
time from 0 to 24 h. The CLt/F of levofloxacin is
calculated as Dose/AUC0-∞, while the
Vd/F is obtained as (CLt/F)/λ. Since there
was no single time-concentration curve from 0 to 24 h from the same
subject, the non-parametric bootstrap method was used to obtain the
above parameters (23).
Specifically, a new replication of the dataset (bootstrap sample)
at each time-point was obtained using eight random draws of
individual data (with replacement) from the original dataset. The
non-compartment analysis was performed using average values of each
new dataset and this process was repeated 200 times with different
random draws. All the calculations were performed using Matlab
software (version 7.0.1; Mathworks Inc.).
A pharmacokinetic model was developed to analyze the
time profiles of levofloxacin in plasma, lung tissue and bronchial
mucosa simultaneously (Fig. 1). The
time profiles of the levofloxacin concentration in plasma and
tissues were described using a one-compartment model. The
elimination of levofloxacin from the central, lung and bronchial
compartment, as well as the drug transport from the central to lung
or bronchial compartment, were all consistent with first-order
kinetics. The differential equations are as follows:
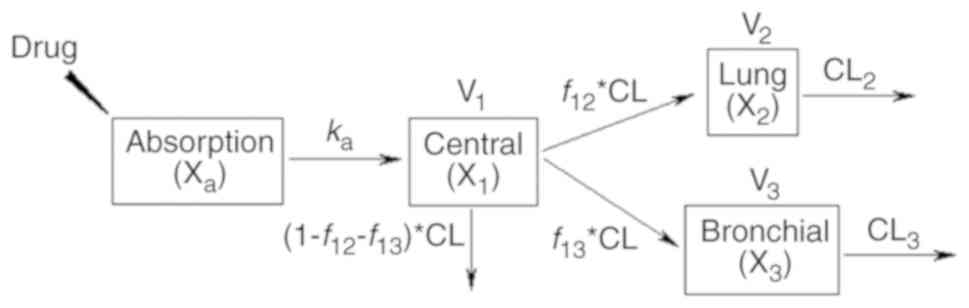 | Figure 1Pharmacokinetic model of levofloxacin
in plasma, lung tissue and bronchial mucosa. Xa,
X1, X2 and X3 denote the amount of
levofloxacin in absorption, central, lung and bronchial
compartment, respectively. ka represents the
absorption rate of levofloxacin. CL is the clearance of
levofloxacin. V1, V2, and V3
indicate the distribution volume in the central, lung, and
bronchial compartment. f12 and
f13 indicate the fraction of levofloxacin
clearance from central to the lung and bronchial compartment,
respectively. CL2 and CL3 are the clearance
of levofloxacin from the lung and bronchial compartment,
respectively. |
Where Xa, X1, X2
and X3 are the amount of levofloxacin in absorption,
central, lung and bronchial compartment, respectively, and
Xa,0, X1,0, X2,0 and
X3,0 are the corresponding initial values.
ka and F represent the absorption rate and
bioavailability of levofloxacin. CL and V1 are the
clearance of levofloxacin and distribution volume in the central
compartment. f12 and f13
indicate the fraction of levofloxacin clearance from the lung and
bronchial compartment, respectively. CL2 and
CL3 are the clearance of levofloxacin from central to
the lung and bronchial compartment. V2 is the weight of
the lung, which was fixed as 1.2 kg according to previous
literature (1/50 of the assumed body weight of 60 kg) (24-26).
V3 is the weight of the bronchial mucosa, which was
fixed as a value of 1, since the data were not identifiable.
C1, C2 and C3 indicate the
levofloxacin concentration in the plasma (mg/l), lung (mg/kg) and
bronchial mucosa (mg/kg), respectively.
The PK model was developed in three steps: i) The
mean C1 data were fit to obtain CL, volume of
distribution in central department (V1/F) and
ka; ii) the mean C2 data were fit to
obtain f12 and CL2; iii) the mean
C3 data were fit to obtain f13 and
CL3. Non-compartment analysis was used to provide
initial estimates of the parameters. Model fittings were performed
by non-linear regression analysis using a maximum likelihood
algorithm in Matlab software. The ordinary differential equation
functions were used to solve differential equations. Goodness of
fit was evaluated by the objective function (mean residual fraction
ratio) and by visual inspection of diagnostic plots. Non-parametric
bootstrap analysis was performed in order to obtain more accurate
parameter estimates. This process was similar to that in the
non-compartment analysis. The stability of the final model was
evaluated by inspection of the distribution of parameter estimates
from the new datasets and comparing these with values obtained from
the fit of the original dataset.
Statistical analysis
The demographic and baseline characteristics of
patients were summarized and compared between groups. Values are
expressed as n or the mean ± standard deviation. Continuous data
were assessed using analysis of variance and the least-significant
difference test. The categorical data, including sex, history of
smoking and concomitant medications, were compared using Fisher's
exact test. All statistical analyses were performed using SPSS
software (version 19.0; IBM Corp.). P<0.05 was considered to
indicate a statistically significant difference.
PK/PD analysis
Levofloxacin is a concentration-dependent quinolone
antibiotic. The major PK/PD parameters are AUC/MIC and
Cmax/MIC (26-28).
The MIC data of levofloxacin were obtained from a previous study
(29). The
fAUC0-24/MIC90 and
fCmax/MIC90 of levofloxacin were
calculated using the PK parameters obtained from a non-compartment
analysis, where f is the free fraction of levofloxacin (0.7)
(30). PK/PD analysis of
levofloxacin was performed using Monte Carlo simulation. The
simulated data of AUC0-24 and Cmax were
obtained based on a logarithmic normal distribution. The simulated
MIC values were generated based on a discrete distribution
according to specified probability at each MIC level. The PK/PD
targets of levofloxacin (fAUC0-24/MIC ≥30;
fCmax/MIC ≥5) were used to predict the
bacteriological efficacy of the drug against Streptococcus
pneumonia (4,31-34).
The probability of target attainment (PTA) of levofloxacin was
calculated as the percentage of PK/PD parameter reaching the target
at each specified MIC level, while the cumulative fraction of
response (CFR) of levofloxacin was obtained as the percentage of
PK/PD parameters attaining the target values (35). The simulation was performed in 5,000
patients using Matlab software.
Results
Baseline characteristics of
patients
A total of 32 patients were enrolled in the present
study. The underlying diseases of the patients included lung cancer
(n=23), old tuberculosis (n=3), lung inflammatory granuloma (n=3),
right lung angioma (n=1), chronic cavitation in the right lower
lobe (n=1) and bronchiectasis in the left lower lobe (n=1). A total
of 20 (62.5%) male and 12 (37.5%) female patients were enrolled,
with an average age of 56±12 (range 23-80) years and an average
CLcr of 92.2±20.9 ml/min. The baseline characteristics
of sex, age, body weight, CLcr and alanine
aminotransferase were well-balanced among the 4 patient groups
(P>0.05; Table III). No
significant difference between history of smoking or use of
concomitant drugs was present among the 4 groups.
| Table IIIBaseline characteristics of patients
undergoing pulmonary operation (8 patients/group). |
Table III
Baseline characteristics of patients
undergoing pulmonary operation (8 patients/group).
| Group | Sex
(male/female) | Age (years) | Body weight
(kg) |
CLcr(ml/min) | ALT (U/l) | Smoking
(yes/no) | Concomitant drugs
(yes/no) |
|---|
| 1 | 7/1 | 48±13 | 65±10 | 105±17 | 23.9±13.8 | 6/2 | 0/8 |
| 2 | 6/2 | 61±10 | 64±7 | 80±14 | 18.8±7.21 | 4/4 | 0/8 |
| 3 | 3/5 | 58±13 | 65±10 | 94±23 | 22.3±8.43 | 2/6 | 1/7 |
| 4 | 4/4 | 58±12 | 61±12 | 90±23 | 21.6±14.8 | 2/6 | 3/5 |
| Total | 20/12 | 56.0±12.0 | 63.8±9.5 | 92.2±20.9 | 21.6±11.1 | 14/18 | 4/28 |
Permeability of levofloxacin in lung
tissue and bronchial mucosa
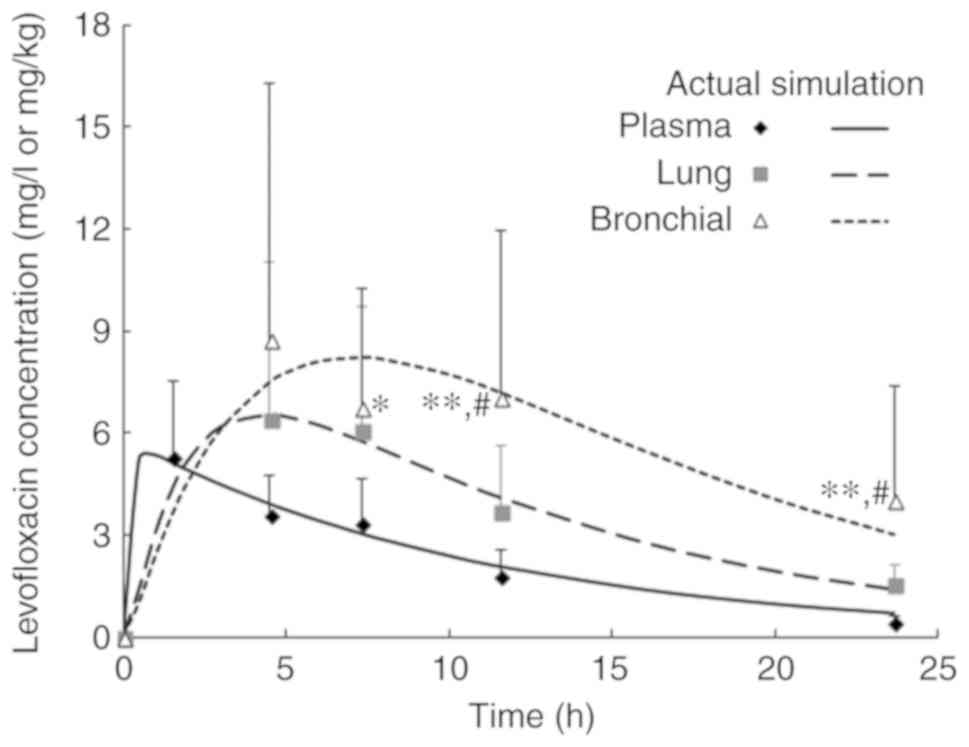
The mean concentration-time curves of levofloxacin
in lung tissue, bronchial mucosa and plasma of the patients are
presented in Fig. 1. Table IV presents the concentration ratio
of levofloxacin in lung tissue and bronchial mucosa at each
time-point. The RCmax in lung tissue and bronchial
mucosa was 1.7±1.0 and 2.2±1.1 at 4 h post-dose. These ratios
increased to 3.8±2.0 and 9.0±8.0 at 24 h, respectively. Statistical
analysis demonstrated that the concentration ratio of levofloxacin
at 24 h was significantly higher compared with that at other
sampling times in lung tissue and bronchial mucosa (Table IV). The results also indicated that
the mean concentration ratio of levofloxacin in bronchial mucosa
was significantly higher compared with that in lung tissue at 24 h
post-dose.
| Table IVConcentration ratio of levofloxacin
in patients undergoing pulmonary operation after oral
administration of a single 500-mg tablet (n=8 per group). |
Table IV
Concentration ratio of levofloxacin
in patients undergoing pulmonary operation after oral
administration of a single 500-mg tablet (n=8 per group).
| Group | Actual sampling
time (h) | Concentration
ratioa |
|---|
| Lung/plasma | Bronchial
mucosa/plasma |
|---|
| 1 | 4.5±0.2 |
1.7±1.0b |
2.2±1.1b |
| 2 | 7.3±1.3 |
1.8±0.9b |
2.1±0.8b |
| 3 | 11.6±0.8 |
2.3±1.5c |
4.2±2.5a,c |
| 4 | 23.6±0.9 | 3.8±2.0 | 9.0±8.0 |
| Overall | | 2.4±1.6 | 4.4±5.0 |
PK of levofloxacin
Non-compartment parameters of levofloxacin in
plasma, lung tissue and bronchial mucosa are presented in Table V. For the majority of parameters, the
values were ranked as plasma < lung tissue < bronchial
mucosa. The AUC0-24 of levofloxacin in the plasma, lung
tissue and bronchial mucosa was 65.2±4.0, 85.7±8.5 and 137.3±19.4
mg h/l, respectively. RAUC_0-24 was 1.3±0.2 in the lung
and 2.1±0.3 in the bronchial mucosa. The levofloxacin concentration
reached Cmax in plasma at 1.5 h, while the concentration
in lung tissue and bronchial mucosa reached Cmax at 4 h
post-dose. The Cmax in lung tissue and bronchial mucosa
was increased by 32 and 77% compared with that in plasma. The
T1/2 of levofloxacin was increased
by 46% in lung tissue and 254% in bronchial mucosa compared with
that in plasma. The MRT0-24 of levofloxacin exhibited a
similar pattern of change to that of
T1/2.
| Table VNon-compartment parameters of
levofloxacin following single oral administration of 500 mg tablet
in patients undergoing pulmonary operation. |
Table V
Non-compartment parameters of
levofloxacin following single oral administration of 500 mg tablet
in patients undergoing pulmonary operation.
| Parameter | Plasma | Lung tissue | Bronchial
mucosa |
|---|
| Cmax
(mg/l or mg/kg) | 5.4±0.7 | 7.0±1.2 | 9.4±2.1 |
| Tmax
(h) | 1.7±0.9 | 5.9±1.4 | 6.4±2.8 |
| AUC0-24
(mg h/l or mg h/kg) | 65.2±4.0 | 85.7±8.5 | 137.3±19.4 |
|
AUC0-∞ (mg h/l or mg
h/kg) | 69.4±4.1 | 106.6±8.1 | 273.7±129.7 |
|
T1/2
(h) | 6.1±0.7 | 8.9±1.5 | 21.6±14.2 |
| MRT0-24
(h) | 8.3±0.3 | 9.9±0.4 | 11.2±0.7 |
| CLt/F
(l/h) | 7.2± 0.4 | | |
| Vd/F
(l) | 63.7±8.1 | | |
| RCmax
(l/kg) | | 1.3±0.3 | 1.8±0.5 |
|
RAUC_0-24 (l/kg) | | 1.3±0.2 | 2.1±0.3 |
|
RAUC_0-∞ (l/kg) | | 1.5±0.1 | 4.0±1.9 |
The time profiles of levofloxacin in plasma, lung
tissue and bronchial mucosa were well-described by the PK model
(Fig. 2). The absorption rate of
levofloxacin was 5.6 1/h, while the CLt/F was 7.8 l/h
(Table VI). Bootstrapping for PK
model showed that f12 and f13
were 0.128 and 0.074, which indicate that the percentage sof the
levofloxacin dose distributed to the lung and bronchial compartment
was 12.8 and 7.4%, respectively (Table
VI). The parameter values obtained from the bootstrap dataset
had almost the same order of magnitude as those from the original
dataset. The coefficient of variation of parameters in tissue
(f12, CL2, f13 and
CL3) obtained from the bootstrap dataset was relatively
high (Table VI). This is consistent
with the high standard deviation of the levofloxacin concentration
in lung tissue and bronchial mucosa (Fig. 2).
| Table VIPharmacokinetic parameters of
levofloxacin in patients undergoing pulmonary operation. |
Table VI
Pharmacokinetic parameters of
levofloxacin in patients undergoing pulmonary operation.
| Parameter
(Unit) | Original
dataset | Bootstrap
dataset |
|---|
| Mean ±
SDa | CV (%) |
|---|
|
ka (l/h) | 5.6 | 6.2±2.0 | 32.6 |
| CL (l/h) | 7.8 | 8.2±0.8 | 9.8 |
| V1/F
(l) | 86.4 | 85.6±11.9 | 13.9 |
|
f12 | 0.128 | 0.2±0.1 | 77.7 |
| CL2
(l/h) | 0.6 | 0.8±0.6 | 72.3 |
|
f13 | 0.074 | 0.1±0.08 | 69.3 |
| CL3
(l/h) | 0.2 | 0.3±0.3 | 75.9 |
Therapeutic implication of
levofloxacin PK/PD
The PK/PD parameters of levofloxacin against common
pathogens of community-acquired LRTIs are presented in Table VII. The
fAUC0-24/MIC and fCmax/MIC of
levofloxacin in lung tissue and bronchial mucosa were higher
compared with those in plasma. The fAUC0-24/MIC
was 45.6-182.5, 60.0-239.8 and 96.1-384.5 in plasma, lung tissue
and bronchial mucosa, respectively, against gram-positive bacteria.
The fCmax/MIC of levofloxacin was 3.8-15.1,
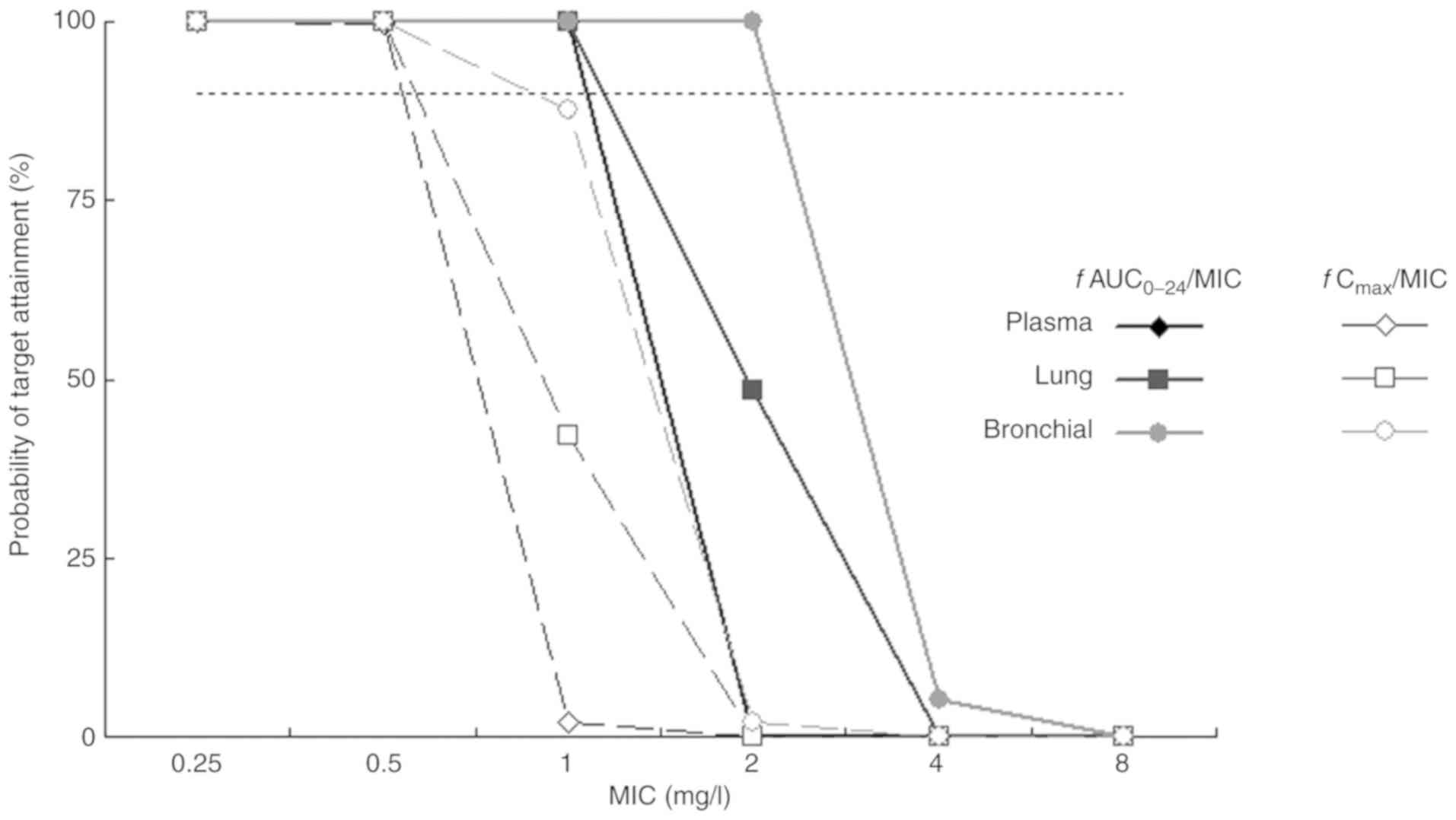
4.9-19.7 and 6.6-26.3 in the corresponding tissue. The PTA of PK/PD
parameters of levofloxacin against S. pneumoniae are
indicated in Fig. 3. The PTA of
levofloxacin fAUC0-24/MIC was maintained at 100%
in plasma and lung tissue when MIC ≤1 mg/l. The PTA of
fAUC0-24/MIC was >90% in bronchial mucosa when
the MIC was ≤2 mg/l. The CFR of levofloxacin for S.
pneumoniae was 90.6, 94.4 and 98.1% in plasma, lung tissue and
bronchial mucosa, respectively, when
fAUC0-24/MIC=30. The CFR of levofloxacin
fCmax/MIC was 44.7, 64.8 and 85.4% in the
corresponding tissues.
| Table VIIPharmacokinetic/pharmacodynamic
parameters of levofloxacin in patients undergoing pulmonary
operation following single oral administration of a 500-mg
levofloxacin tablet. |
Table VII
Pharmacokinetic/pharmacodynamic
parameters of levofloxacin in patients undergoing pulmonary
operation following single oral administration of a 500-mg
levofloxacin tablet.
| Bacteria (no. of
strains) | MIC90
(mg/l) |
fAUC0-24/MIC90 |
fCmax/MIC90 |
|---|
| Plasma | Lung tissue | Bronchial
mucosa | Plasma | Lung tissue | Bronchial
mucosa |
|---|
| MSSA (21) | 0.25 | 182.5 | 239.8 | 384.5 | 15.1 | 19.7 | 26.3 |
| S.
pneumoniae (28) | 1 | 45.6 | 60.0 | 96.1 | 3.8 | 4.9 | 6.6 |
| H.
influenzae (45) | 0.5 | 91.3 | 119.9 | 192.3 | 7.6 | 9.8 | 13.2 |
| K.
pneumoniae (87) | 1 | 45.6 | 60.0 | 96.1 | 3.8 | 4.9 | 6.6 |
| P.
aeruginosa (18) | 16 | 2.9 | 3.7 | 6.0 | 0.2 | 0.3 | 0.4 |
|
Acinetobacter spp. (22) | 0.25 | 182.5 | 239.8 | 384.5 | 15.1 | 19.7 | 26.3 |
Discussion
The results of the present study indicated that
levofloxacin is able to rapidly penetrate into the lung tissue and
bronchial mucosa. Following a single oral dose of 500 mg
levofloxacin, the average concentration of levofloxacin in plasma,
lung tissue and bronchial mucosa was 3.6 µg/ml, 6.4 and 8.7 µg/g at
4 h post-dose, and this was reduced to 0.5 µg/ml, 1.6 and 4.1 µg/g
at 24 h. Compared with the plasma concentration, the levofloxacin
concentration was higher in lung tissue and bronchial mucosa at
4-24 h post-dose. The average concentration ratio of the
levofloxacin penetration into lung tissue was 2.4 (0.7-7.8) and the
maximal concentration ratio value was observed at 24 h post-dose.
The permeability of levofloxacin in lung tissue increased with
time, demonstrating the high permeability of levofloxacin in lung
tissue. Other studies have reported that the mean tissue
permeability of levofloxacin was 4.0 within 24 h and 5.1 at 12 h
following a single oral dose of 500 mg levofloxacin in patients
receiving pulmonary biopsy or pneumonectomy (36). These data are inconsistent with the
results of the present study and may be due to the patients in the
aforementioned studies being from different ethnic groups and
exhibiting high inter-subject variability due to the smaller
patient sample size. In the present study, a total of 8 Chinese
patients were enrolled in each group.
Pulmonary lobectomy is an effective treatment for
intrapulmonary and bronchial diseases (37). However, this procedure to remove the
source of contamination in bronchi may cause infection (38), and is a critical occasion for the
prophylactic use of antimicrobial agents. Following oral
administration of a single dose of 500 mg levofloxacin, the average
concentration ratio of levofloxacin was 4.4 in bronchial mucosa
within 24 h, which was significantly higher compared with that in
lung tissue (2.4). Compared with water-soluble drugs, lipid-soluble
antimicrobial agents, including fluoroquinolones, are more readily
absorbed through the cell membrane and exhibit increased tissue
permeability (39). Antimicrobial
agents have been extensively studied in sputum (40). However, sputum is non-homogeneous
sample and may be easily diluted by saliva (41). Therefore, bronchial mucosa is more
reliable than sputum in the evaluation of antimicrobial agent
permeability in lung tissues (42);
however, it is more difficult to collect samples of bronchial
mucosa and lung tissue than sputum. The present study provided
direct evidence for the tissue permeability of levofloxacin.
Zhang et al (2) indicated that the
Cmax/MIC90 ratio was 3-57 in epithelial
lining fluid (ELF), and 1-6 in sputum following a single oral dose
of 500 mg levofloxacin at the fasting state in patients with LRTI
undergoing bronchoalveolar lavage (2). The AUC0-24
h/MIC90 of levofloxacin reached 35-138 and 9-38,
respectively. Compared with the plasma concentration at the same
time-point, the concentration ratio of levofloxacin in ELF was high
(~1.04 at 24 h after dosing), but the concentration ratio in sputum
was low (0.09) (2). The results of
the present study demonstrated that the permeability of
levofloxacin is more prominent in lung tissue and bronchial mucosa
following an oral dose of 500 mg, and is higher compared with that
in ELF and sputum.
The Vd of levofloxacin decreased
significantly by 47.8% in patients undergoing pulmonary operation
(1.0 vs. 1.9 l/kg), T1/2 decreased
by 34.8% (6.1 vs. 9.4 h) and Cmax decreased by 23.1%
(5.4 vs. 7.0 mg/l), while the AUC0-24 and
AUC0-∞ of levofloxacin increased by 35.3%
(65.2 mg h/l vs. 48.2 mg h/l) and 26.7% (69.4 mg h/l vs. 54.8 mg
h/l), respectively, compared with that in healthy subjects
(43). These results indicated that
a decreased distribution volume of levofloxacin may be the reason
for the higher drug exposure in patients undergoing pulmonary
operation.
During the development of the compartment model,
the levofloxacin concentration data in plasma and lung tissue was
fit using a two-compartment model, where the peripheral compartment
represents lung tissue. The results indicated that the
inter-compartment clearance of levofloxacin was close to zero.
Subsequently, a model was developed where drug elimination from the
peripheral compartment was introduced. Although the model fittings
improved, the simulated concentration of levofloxacin in plasma was
higher than the actual values at all time-points. A
three-compartment model was also used to analyze the PK data of
levofloxacin, where the two peripheral compartments represented
lung tissue and bronchial mucosa and the simulation results were
not satisfactory. The final PK model was obtained by simplification
of this model and by introducing an elimination pathway from
peripheral compartments (Fig. 1).
For instance, the elimination of levofloxacin from the lung
compartment represented the process of drug efflux from lung tissue
to blood. The structure of the final PK model was similar to that
of the PK model of moxifloxacin in patients with bronchopneumonia
(44). The CL of levofloxacin was
close to the non-compartment parameter CLt/F and the
distribution volume in the central compartment V1/F was
similar to Vd/F. The results of most PK parameters
derived from the bootstrap method were close to the results
calculated from original dataset, and this was supported by the
standard deviation for PK parameters. This suggested that the
estimation of the results of the final PK model were reliable.
The PK/PD parameters of levofloxacin determined in
the present study were similar to the literature reports following
the adjustment by dose and drug unbound fraction. For S.
pneumoniae, the Cmax/MIC90 and
AUC/MIC90 of levofloxacin in plasma were similar to
those in patients with bronchitis or obstructive pulmonary disease
(32). The results of the present
study were also similar to a PK study of levofloxacin in elderly
adults receiving diagnostic bronchoscopy (45). The Cmax/MIC90
and AUC/MIC90 of levofloxacin in lung tissue against
P. aeruginosa and K. pneumoniae exhibited the same
orders of magnitude to the parameter values in patients undergoing
off-pump coronary artery bypass grafting (46).
The results indicated that the
fAUC0-24/MIC90 of levofloxacin was
only 3.7 in lung tissue against P. aeruginosa. This result
indicated that levofloxacin cannot be recommended as a first-line
therapy of LRTIs where P. aeruginosa is isolated or is
suspected to be the causative pathogen. This result is similar to a
PK/PD report of levofloxacin in acutely hospitalized elderly
patients (27). A previous study
demonstrated that a PK/PD model predicted that 500 mg levofloxacin
was not effective for treating multidrug- and drug-resistant
tuberculosis (47-49).
By contrast, the fAUC0-24/MIC of levofloxacin
reached 60 in lung tissue against S. pneumoniae. The Monte
Carlo simulation revealed that the PTA of levofloxacin
fAUC0-24/MIC in lung tissue and bronchial mucosa
was maintained at 100% when MIC ≤1 mg/l and the CFR of
fAUC0-24/MIC was also >90% in these two
tissues. These results are supported by a population PK (PPK) study
of levofloxacin (26), which
indicated an AUC0-24 of 66.19±1.30 mg h/l and the
predicted CFR for a target AUC0-24/MIC ratio of 30 was
83.12% for S. aureus and 92.63% for S. pneumoniae.
Due to the MIC90 of levofloxacin against S.
pneumoniae being 1 mg/l, it may be suggested that a
levofloxacin 500 mg dosing regimen has good clinical and
microbiological efficacy in the treatment of pulmonary infections
that are caused by S. pneumoniae.
In the present study, it was not possible to
develop a PPK model of levofloxacin due to the small number of lung
tissue and bronchial mucosa samples. It was impossible to estimate
inter-subject variation due to there only being one data-point for
each tissue sample type that was collected in one subject.
Therefore, a compartment model was developed to analyze the PK data
of levofloxacin in plasma, lung tissue and bronchial mucosa
simultaneously. This provides more details about drug ADME compared
with general non-compartment PK parameters. Treatment-emergent
adverse events were not monitored, but the record of data did not
indicate any significant or outstanding adverse events in the
present study. The body mass index was also not calculated as
patient height was not recorded. The standard error is particularly
high for levofloxacin concentration in bronchial samples as
compared with that in the other types of samples. This may be due
to fewer number of samples at the time point of sampling and
inter-individual variation. The bootstrap simulation in this study
may offset this limitation to some extent.
To the best of our knowledge, the present study was
the first to characterize the penetration of levofloxacin in
bronchial mucosa. An integrated model was developed describing
disposition and elimination of levofloxacin in plasma, lung tissue
and bronchial mucosa, and PK/PD indices of levofloxacin in
patients' bronchial mucosa were provided. The results indicated
that levofloxacin is able to distribute to bronchi and lung tissues
to reach an effective antimicrobial concentration after a single
oral dose of 500 mg. The permeability of levofloxacin was
demonstrated to be higher in bronchial mucosa compared with that in
lung tissue. The PK/PD profiles of levofloxacin in lung tissues
support the favorable efficacy of levofloxacin 500 mg regimen for
managing the community-acquired LRTIs that are caused by S.
pneumoniae.
Acknowledgements
Not applicable.
Funding
The current study was supported by grants from the
Ministry of Science and Technology of China (grant nos.
2012ZX09303004-001 and 2017ZX09304005) and the Natural Science
Foundation of China (grant no. 81202582). Japan Daiichi
Pharmaceutical Co. also sponsored this study.
Availability of data and materials
The datasets used and/or analyzed during the
current study are available from the corresponding author on
reasonable request.
Authors' contributions
GC, JZ and ZC conceived and designed the
experiments, and wrote and modified the manuscript. YoZ and LP
performed surgery and collected tissue samples. XX, YC and JY
performed the PK/PD analysis. YiZ, JZ and YS critically interpreted
the data and reviewed the manuscript. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
All study procedures in this study were approved by
the Ethics Committee of Huashan Hospital, Fudan University
(Shanghai, China). All patients provided written informed consent
form prior to participation in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Torres A and Liapikou A: Levofloxacin for
the treatment of respiratory tract infections. Expert Opin
Pharmacother. 13:1203–1212. 2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Zhang J, Xie X, Zhou X, Chen YQ, Yu JC,
Cao GY, Wu XJ, Shi YG and Zhang YY: Permeability and concentration
of levofloxacin in epithelial lining fluid in patients with lower
respiratory tract infections. J Clin Pharmacol. 50:922–928.
2010.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Nakajima T, Kaji Y and Miyawaki M:
Penetration of single-dose levofloxacin into intestinal tissue. J
Gastroen Hepatol Res. 2:399–402. 2013.
|
|
4
|
Hutschala D, Skhirtladze K, Zuckermann A,
Wisser W, Jaksch P, Mayer-Helm BX, Burgmann H, Wolner E, Müller M
and Tschernko EM: In vivo measurement of levofloxacin penetration
into lung tissue after cardiac surgery. Antimicrob Agents
Chemother. 49:5107–5111. 2005.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Grossman RF, Rotschafer JC and Tan JS:
Antimicrobial treatment of lower respiratory tract infections in
the hospital setting. Am J Med. 118 (Suppl)(29S-38S)2005.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Andes D and Craig WA: Animal model
pharmacokinetics and pharmacodynamics: A critical review. Int J
Antimicrob Agents. 19:261–268. 2002.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Friedman H, Song X, Crespi S and
Navaratnam P: Comparative analysis of length of stay, total costs,
and treatment success between intravenous moxifloxacin 400 mg and
levofloxacin 750 mg among hospitalized patients with
community-acquired pneumonia. Value Health. 12:1135–1143.
2009.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Frei CR, Jaso TC, Mortensen EM, Restrepo
MI, Raut MK, Oramasionwu CU, Ruiz AD, Makos BR, Ruiz JL, Attridge
RT, et al: Medical resource utilization among community-acquired
pneumonia patients initially treated with levofloxacin 750 mg daily
versus ceftriaxone 1000 mg plus azithromycin 500 mg daily: A
US-based study. Curr Med Res Opin. 25:859–868. 2009.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Schein J, Janagap-Benson C, Grant R,
Sikirica V, Doshi D and Olson W: A comparison of levofloxacin and
moxifloxacin use in hospitalized community-acquired pneumonia (CAP)
patients in the US: Focus on length of stay. Curr Med Res Opin.
24:895–906. 2008.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Lynch-JP III, File-TM Jr and Zhanel GG:
Levofloxacin for the treatment of community-acquired pneumonia.
Expert Rev Anti Infect Ther. 4:725–742. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
DiPiro JT: Short-term prophylaxis in
clean-contaminated surgery. J Chemother. 11:551–555.
1999.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Radu DM, Jauréguy F, Seguin A, Foulon C,
Destable MD, Azorin J and Martinod E: Postoperative pneumonia after
major pulmonary resections: An unsolved problem in thoracic
surgery. Ann Thorac Surg. 84:1669–1673. 2007.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Schussler O, Alifano M, Dermine H, Strano
S, Casetta A, Sepulveda S, Chafik A, Coignard S, Rabbat A and
Regnard JF: Postoperative pneumonia after major lung resection. Am
J Respir Crit Care Med. 173:1161–1169. 2006.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Belda J, Cavalcanti M, Ferrer M, Serra M,
Puig de la Bellacasa J, Canalis E and Torres A: Bronchial
colonization and postoperative respiratory infections in patients
undergoing lung cancer surgery. Chest. 128:1571–1579.
2005.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Bratzler DW and Houck PM: Antimicrobial
prophylaxis for surgery: An advisory statement from the National
Surgical infection prevention project. Am J Surg. 189:395–404.
2005.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Gupta R, Sinnett D, Carpenter R, Preece PE
and Royle GT: Antibiotic prophylaxis for post-operative wound
infection in clean elective breast surgery. Eur J Surg Oncol.
26:363–366. 2000.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Bratzler DW, Houck PM, Richards C, Steele
L, Dellinger EP, Fry DE, Wright C, Ma A, Carr K and Red L: Use of
antimicrobial prophylaxis for major surgery: Baseline results from
the National Surgical Infection Prevention Project. Arch Surg.
140:174–182. 2005.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Malone DL, Genuit T, Tracy JK, Gannon C
and Napolitano LM: Surgical site infections: Reanalysis of risk
factors. J Surg Res. 103:89–95. 2002.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Von Baum H, Böttcher S, Hoffmann H and
Sonntag HG: Tissue penetration of a single dose of levofloxacin
intravenously for antibiotic prophylaxis in lung surgery. J
Antimicrob Chemother. 47:729–730. 2001.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Swoboda S, Oberdorfer K, Klee F,
Hoppe-Tichy T, von Baum H and Geiss HK: Tissue and serum
concentrations of levofloxacin 500 mg administered intravenously or
orally for antibiotic prophylaxis in biliary surgery. J Antimicrob
Chemother. 51:459–462. 2003.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Cockcroft DW and Gault MH: Prediction of
creatinine clearance from serum creatinine. Nephron. 16:31–41.
1976.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Xie X, Zhang J, Yu JC, Shi YG and Zhang
YY: HPLC assay of levofloxacin concentration in plasma, lung
tissue, and body fluids. Chin J Clin Pharmacol Ther. 17:158–162.
2008.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Chen Y, Cao Y, Zhou J and Liu X:
Mechanism-based pharmacokinetic-pharmacodynamic modeling of
bidirectional effect of danshensu on plasma homocysteine in rats.
Pharm Res. 26:1863–1673. 2009.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Askenazi SS and Perlman M: Pulmonary
hypoplasia: Lung weight and radial alveolar count as criteria of
diagnosis. Arch Dis Child. 54:614–618. 1979.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Qi XL, Bo AH and Xia L: Determination of
cerebral and lung weight of fetus. Chin J Birth Health Heredity.
65(65)1993.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Jaruratanasirikul S, Jaspattananon A,
Wongpoowarak W, Nawakitrangsan M, Thengyai S and Samaeng M:
Population pharmacokinetics and pharmacodynamics modeling of oral
levofloxacin. J Med Assoc Thai. 99:886–892. 2018.PubMed/NCBI
|
|
27
|
Cojutti PG, Ramos-Martin V, Schiavon I,
Rossi P, Baraldo M, Hope W and Pea F: Population pharmacokinetics
and pharmacodynamics of levofloxacin in acutely hospitalized older
patients with various degrees of renal function. Antimicrob Agents
Chemothe. 61(e02134-16)2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Scaglione F, Mouton JW, Mattina R and
Fraschini F: Pharmacodynamics of levofloxacin and ciprofloxacin in
a murine pneumonia model: Peak concentration/MIC versus area under
the curve/MIC ratios. Antimicrob Agents Chemother. 47:2749–2755.
2003.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Zhang YY, Huang HH and Ren ZY: Clinical
evaluation of oral levofloxacin 500 mg once-daily dosage for
treatment of lower respiratory tract infections and urinary tract
infections: A prospective multicenter study in China. J Infect
Chemother. 15:301–311. 2009.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Cao G, Zhang J, Wu X, Yu J, Chen Y, Ye X,
Zhu D, Zhang Y, Guo B and Shi Y: Pharmacokinetics and
pharmacodynamics of levofloxacin injection in healthy Chinese
volunteers and dosing regimen optimization. J Clin Pharm Ther.
38:394–400. 2013.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Rodvold KA, Danziger LH and Gotfried MH:
Steady-state plasma and bronchopulmonary concentrations of
intravenous levofloxacin and Azithromycin in healthy adults.
Antimicrob Agents Chemother. 47:2450–2457. 2003.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Conte JE Jr, Golden JA, McIver M, Little E
and Zurlinden E: Intrapulmonary pharmacodynamics of high-dose
levofloxacin in subjects with chronic bronchitis or chronic
obstructive pulmonary disease. Int J Antimicrob Agents. 30:422–427.
2007.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Preston SL, Drusano GL, Berman AL, Fowler
CL, Chow AT, Dornseif B, Reichl V, Natarajan J and Corrado M:
Pharmacodynamics of levofloxac in: A new paradigm for early
clinical trials. JAMA. 279:125–129. 1998.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Zhang J, Yu JC, Shi YG, Zhou L, Ye XY, Zhu
DM and Zhang YY: Study of pharmacokinetics/pharmacodynamics of
levofloxacin. Zhonghua Yi Xue Za Zhi. 85:1926–1932. 2005.(In
Chinese). PubMed/NCBI
|
|
35
|
Wu XJ, Zhang J, Guo BN, Zhang YY, Yu JC,
Cao GY, Chen YC, Zhu DM, Ye XY, Wu JF, et al: Pharmacokinetics and
pharmacodynamics of multiple-dose intravenous nemonoxacin in
healthy Chinese volunteers. Antimicrob Agents Chemother.
59:1446–1454. 2015.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Lee LJ, Sha X, Gotfried MH, Howard JR, Dix
RK and Fish DN: Penetration of levofloxacin into lung tissue after
oral administration to subjects undergoing lung biopsy or
lobectomy. Pharmacotherapy. 18:35–41. 1998.PubMed/NCBI
|
|
37
|
Wang CQ, Wang W, Jin MH, Huang Q and Guan
Q: Pulmonary resections in surgical treatment of lung tuberculosis.
J Clin Pulmonary Med. 14:906–908. 2009.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Li P, Mao YB and Liu CT: Risk factors for
surgical site infections in patients undergoing pneumonectomy. Chin
J Nosocomiol. 23(5198-5199-5202)2013.
|
|
39
|
Pea F: Intracellular pharmacokinetics of
antibacterials and their clinical implications. Clin Pharmacokinet.
57:177–189. 2018.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Moriarty TF, McElnay JC, Elborn JS and
Tunney MM: Sputum antibiotic concentrations: Implications for
treatment of cystic fibrosis lung infection. Pediatr Pulmonol.
42:1008–1017. 2007.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Kelly MM, Efthimiadis A and Hargreave FE:
Induced sputum: Selection method. Methods Mol Med. 56:77–91.
2001.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Cazzola M, Blasi F, Terzano C, Matera MG
and Marsico SA: Delivering antibacterials to the lungs:
Considerations for optimizing outcomes. Am J Respir Med. 1:261–272.
2002.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Yu JC, Zhang J and Cao GY: Single-dose and
multiple-dose pharmacokinetics of levofloxacin in Chinese healthy
subjects. J Third Mil Med Univ. 35:2516–2520. 2013.
|
|
44
|
Simon N, Sampol E, Albanese J, Martin C,
Arvis P, Urien S, Lacarelle B and Bruguerolle B: Population
pharmacokinetics of moxifloxacin in plasma and bronchial secretions
in patients with severe bronchopneumonia. Clin Pharmacol Ther.
74:353–363. 2003.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Capitano B, Mattoes HM, Shore E, O'Brien
A, Braman S, Sutherland C and Nicolau DP: Steady-state
intrapulmonary concentrations of moxifloxacin, levofloxacin, and
azithromycin in older adults. Chest. 125:965–973. 2004.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Hutschala D, Kinstner C, Skhirtladze K,
Mayer-Helm BX, Zeitlinger M, Wisser W, Müller M and Tschernko E:
The impact of perioperative atelectasis on antibiotic penetration
into lung tissue: An in vivo microdialysis study. Intensive Care
Med. 34:1827–1834. 2008.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Van't Boveneind-Vrubleuskaya N, Seuruk T,
van Hateren K, van der Laan T, Kosterink JGW, van der Werf TS, van
Soolingen D, van den Hof S, Skrahina A and Alffenaar JC:
Pharmacokinetics of levofloxacin in multidrug- and extensively
drug-resistant tuberculosis patients. Antimicrob Agents Chemother.
61(pii: e00343-17)2017.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Al-Shaer MH, Alghamdi WA, Alsultan A, An
G, Ahmed S, Alkabab Y, Banu S, Barbakadze K, Houpt E, Kipiani M, et
al: Fluoroquinolones in drug-resistant tuberculosis: Culture
conversion and pharmacokinetic/pharmacodynamic target attainment to
guide dose selection. Antimicrob Agents Chemother. 63(pii:
e00279-19)2019.PubMed/NCBI View Article : Google Scholar
|
|
49
|
U.S. Department of Health and Human
Services. FDA guidance for industry: Population Pharmacokinetics,
July 2019. https://www.fda.gov/media/128793/download.
Accessed October 2019.
|