Introduction
Gestational diabetes mellitus (GDM) refers to
glucose intolerance that occurs or is first recognized during
pregnancy. It shows a morbidity of 5% among pregnant women, and
obese women face a higher risk of GDM during pregnancy (1). GDM is prone to lead to dystocia,
neonatal hypoglycemia, hyperbilirubinemia, and GDM-related
complications, making a certain impact on the health of pregnant
women and fetuses (2). For example,
women with GDM history face obviously high risks of type 2 diabetes
mellitus and prediabetes after delivery (3). In addition, a study concluded that
compared with pregnant women without gestational diabetes mellitus,
those with this disease showed significantly increased stillbirth
rate and perinatal mortality (4). At
present, the treatment for GDM includes dietary adjustment,
lifestyle changes, and drug therapy such as metformin and insulin
(5). Once the blood sugar control
fails to meet the standard, the incidence of complications such as
premature delivery and neonatal hypoglycemia will greatly increase.
Pregnancy is a special period, so many treatment methods are
limited in different degrees during clinical application. In
addition, there are also some controversies in the diagnosis and
management of this diabetes (6). As
the pathogenesis of GDM is still under investigation, the most
effective treatment method is beyond the reach of clinical practice
at present. However, many studies have revealed that insulin
resistance and pancreatic β cell secretion dysfunction are
important pathological features of gestational diabetes mellitus.
Insulin resistance refers to tissues that do not respond to
insulin. Low-grade chronic inflammation related to obesity is a key
factor of developing insulin resistance (7,8), and
obesity can increase the expression of certain inflammatory
cytokines, activate multiple signal pathways, and participate in
the pathogenesis of insulin resistance by interfering with insulin
signal transmission (9). Tumor
necrosis factor-α (TNF-α) is a pro-inflammatory cytokine, which is
generated by monocytes and macrophages, and participates in the
regulation of many important cellular processes (10). A previous study has proven that the
increase of TNF-α level leads to insulin resistance in adipose
tissues and peripheral tissues (11). In addition, a variety of hormones
secreted by adipocytes, such as adiponectin (ADP), are specifically
expressed in adipose tissue, which directly causes the body
sensitive to insulin. Therefore, ADP may play an important role in
insulin resistance (12). This study
explored the expression of serum ADP and TNF-α in GDM patients to
provide reference for clinical predication and medication guidance
of gestational diabetes mellitus.
Patients and methods
Clinical data
A total of 78 GDM patients admitted to Qingpu Branch
of Zhongshan Hospital Affiliated to Fudan University (Shanghai,
China) from June 2017 to December 2018 were enrolled as an
experimental group, and further 70 healthy pregnant women in
physical examination during the same period were enrolled as a
control group. This study was approved by the Ethics Committee of
Qingpu Branch of Zhongshan Hospital Affiliated to Fudan University,
and signed informed consents were obtained from the patients and/or
guardians.
Inclusion and exclusion criteria
The inclusion criteria of the experimental group
were as follows: Patients first admitted to Qingpu Branch of
Zhongshan Hospital Affiliated to Fudan University, patients with
GDM based on clinical examination, and patients who received
treatment including oral antiglycemics, injection of insulin and
dietary intervention according to the conditions of patients in
Qingpu Branch of Zhongshan Hospital Affiliated to Fudan University
after diagnosis. The blood glucose was controlled between 3.3
mmol/l and 5.3 mmol/l before meal, and between 3.3 mmol/l and 6.7
mmol/l 2 h after meal. When the blood glucose level declined, the
amount of medicine was reduced as appropriate. The exclusion
criteria were as follows: i) Patients with diabetes mellitus before
pregnancy; ii) patients with comorbid cardiovascular diseases,
hepatic or kidney function obstacle; iii) patients with a history
of drug allergy; iv) patients with mental disease and unable to
cooperate; v) patients ending pregnancy in the middle of the
pregnancy course; vi) patients transferred to another hospital
during the study; vii) patients without required pregnancy
examination data.
Methods
Fasting venous blood (2 ml) was sampled from each
subject of the two groups, and the expression of ADP and TNF-α in
the blood samples was determined using the enzyme-linked
immunosorbent assay (ELISA). ADP test kits were purchased from
Shanghai XinYu Biological Technology Co., Ltd. (item no.
xy-A10927), and TNF-α kit was purchased from Shanghai Jingkang
Bioengineering Co., Ltd. (item no. JKSJ-1857). All operations were
carried out strictly in accordance with the kit instructions.
Observation indexes
The expression of ADP and TNF-α in the blood samples
of the experimental group was compared with that in the blood
samples of the control group during pregnancy and after
pregnancy.
Statistical analysis
SPSS 24.0 was employed for statistical analysis.
Enumeration data were expressed as rate, Chi-square test was used
for comparison between groups; measurement data were expressed as
mean ± SD, t-test was used for comparison between groups;
diagnostic value was analyzed by ROC curve. P<0.05 indicates a
significant difference.
Results
General materials
Comparison between the experimental group and the
control group in clinical data revealed that there were no
significant differences in age, pregestational body mass index
(BMI), gestational week, average weekly exercise time, amniotic
fluid volume, medical history (impaired glucose tolerance and
polycystic ovary syndrome), family history of diabetes mellitus,
abortion history, dietary habit, place of residence, and ethnicity
(all P>0.05), which proved the comparability between the two
groups (Table I).
 | Table IComparison between the two groups in
clinical data [mean ± SD, n (%)]. |
Table I
Comparison between the two groups in
clinical data [mean ± SD, n (%)].
| Clinicopathological
characteristics | Experimental group
(n=78) | Control group
(n=70) | t or
χ2 | P-value |
|---|
| Age (years) | 27.13±4.81 | 26.94±4.67 | 0.243 | 0.808 |
| Pregestational BMI
(kg/m2) | 23.52±2.44 | 22.86±3.17 | 1.427 | 0.156 |
| Gestational week | 20.39±3.65 | 20.31±3.96 | 0.128 | 0.898 |
| Average weekly
exercise time (h) | 9.37±2.58 | 9.62±2.74 | 0.572 | 0.569 |
| Amniotic fluid
volume, ml | | | 1.239 | 0.266 |
|
≥2,000 | 14 (17.95) | 8 (11.43) | | |
|
<2,000 | 64 (82.05) | 62 (88.57) | | |
| Medical history | | | 2.161 | 0.142 |
|
Yes | 13 (16.67) | 6 (8.57) | | |
|
No | 65 (83.33) | 64 (91.43) | | |
| Family history of
diabetes mellitus | | | 3.279 | 0.070 |
|
Yes | 31 (39.74) | 18 (25.71) | | |
|
None | 47 (60.26) | 52 (74.29) | | |
| Abortion history | | | 2.351 | 0.125 |
|
Yes | 28 (35.90) | 17 (24.29) | | |
|
None | 50 (64.10) | 53 (75.71) | | |
| Dietary habit | | | 0.440 | 0.507 |
|
Light | 52 (66.67) | 43 (61.43) | | |
|
Spicy | 26 (33.33) | 27 (38.57) | | |
| Place of
residence | | | 0.043 | 0.835 |
|
Rural
area | 31 (39.74) | 29 (41.43) | | |
|
Urban
area | 47 (60.26) | 41 (58.57) | | |
| Ethnicity | | | 1.302 | 0.254 |
|
Han | 62 (79.49) | 50 (71.43) | | |
|
Minority | 16 (20.51) | 20 (28.57) | | |
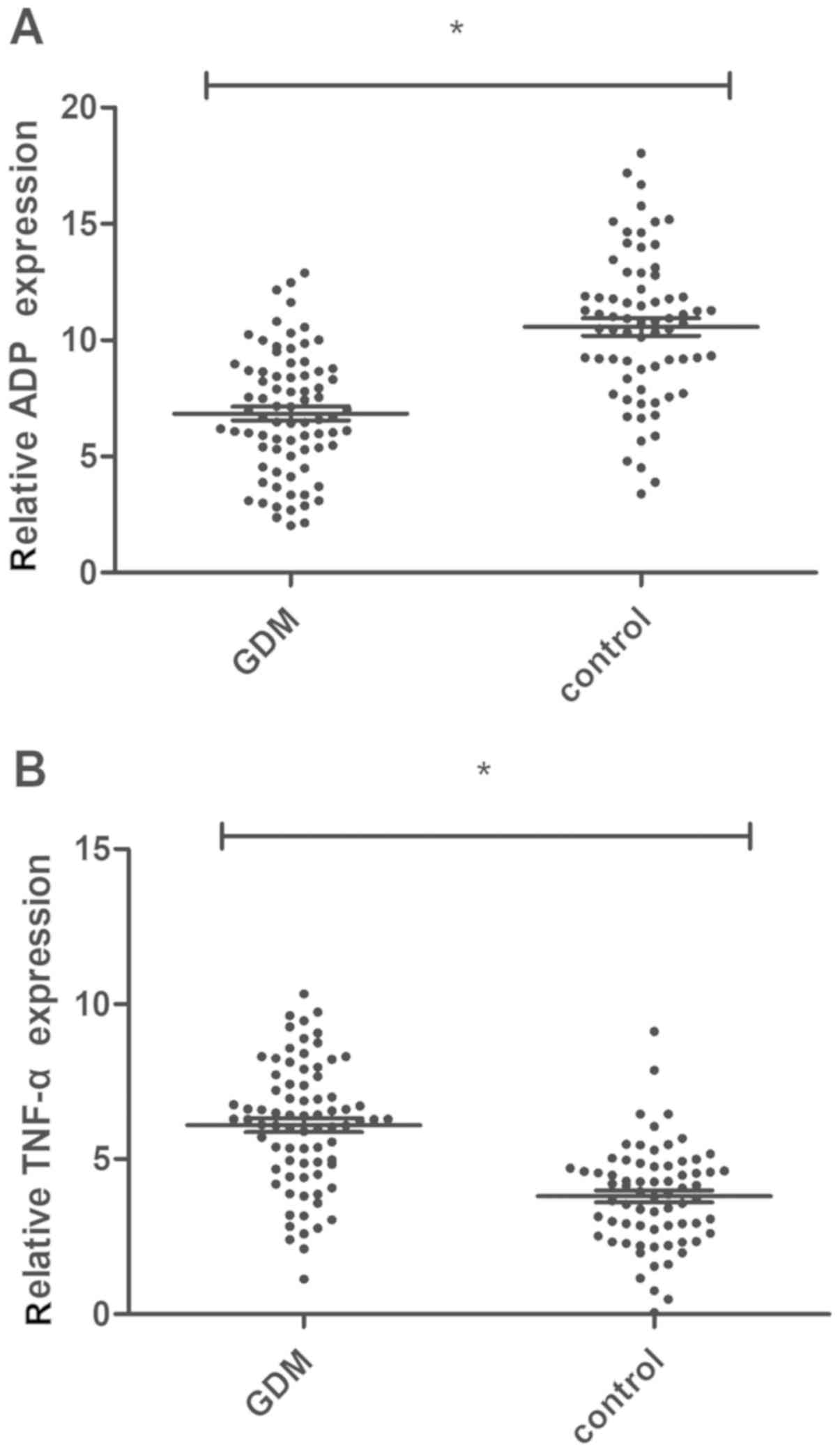
Determination of serum ADP and TNF-α
expression in the experimental group and the control group
Blood was sampled from 78 pregnant women with GDM
and 70 healthy pregnant women before treatment, and the expression
levels of ADP and TNF-α in the blood were determined using the
ELISA. The expression of ADP in pregnant women with GDM was
significantly lower than that in healthy pregnant women (6.84±2.72
vs. 10.21±3.45 mg/l, P<0.01), while the expression of TNF-α in
the pregnant women with GDM was significantly higher than that in
the healthy pregnant women (6.17±2.06 vs. 3.62±1.54 ng/l,
P<0.01) (Fig. 1).
Changes of ADP and TNF-α in the
experimental group after treatment
After treatment, the expression levels of ADP and
TNF-α in the experimental group one week after delivery were
9.39±2.15 mg/l and 3.52±1.47 ng/l, respectively, which was
significantly lower than those before treatment (both P<0.01)
(Table II).
| Table IIChanges of ADP and TNF-α in the
experimental group after delivery. |
Table II
Changes of ADP and TNF-α in the
experimental group after delivery.
| Index | ADP (mg/l) | TNF-α (ng/l) |
|---|
| Before
treatment | 6.84±2.72 | 6.17±2.06 |
| One week after
delivery | 9.39±2.15 | 3.52±1.47 |
| t value | 6.496 | 9.248 |
| P-value | <0.001 | <0.001 |
Association of serum ADP and TNF-α
levels and pregnancy outcomes
The serum ADP and TNF-α levels were related to fetal
distress, macrosomia, fetal malformation, and reproductive tract
infection. The experimental group was divided into high ADP
expression group (≥6.84), low ADP expression group (<6.84), high
TNF-α expression group (≥6.17) and low TNF-α expression group
(<6.17) according to the mean ADP concentration and mean TNF-α
concentration. Analysis of Table
III shows that the rate of adverse pregnancy outcomes in the
low ADP expression group was higher than that in the high ADP
expression group, and the rates in both groups were higher than
that in the control group (both P<0.05). Analysis of Table IV shows that the rate of adverse
pregnancy outcomes in the high TNF-α expression group was higher
than that in the low TNF-α expression group, and the rates in both
groups were higher than that in the control group (both
P<0.05).
| Table IIIComparison of pregnancy outcomes
between two groups with different ADP expression [mean ± SD, n
(%)]. |
Table III
Comparison of pregnancy outcomes
between two groups with different ADP expression [mean ± SD, n
(%)].
| Group | Concentration
(mg/l) | No. of
patients | Fetal distress | Macrosomia | Fetal
malformation | Reproductive tract
infection | Adverse pregnancy
outcomes |
|---|
| High expression
group | 9.51±2.17 | 36 | 4 (11.11) | 3 (8.33) | 2 (5.56) | 5 (13.89) | 14
(38.89)b |
| Low expression
group | 8.43±2.44 | 42 | 7 (16.67) | 9 (21.43) | 4 (9.52) | 10 (23.81) | 30
(71.43)a,b |
| Control group | | 70 | 2 (2.86) | 2 (2.86) | 0 (0.00) | 5 (7.14) | 9 (12.86) |
| χ2
value | | | | | | | 39.370 |
| P-value | | | | | | | <0.01 |
| Table IVComparison of pregnancy outcomes
between two groups with different TNF-α expression [mean ± SD, n
(%)]. |
Table IV
Comparison of pregnancy outcomes
between two groups with different TNF-α expression [mean ± SD, n
(%)].
| Group | Concentration
(ng/l) | No. of cases | Fetal distress | Macrosomia | Fetal
malformation | Reproductive tract
infection | Adverse pregnancy
outcomes |
|---|
| High expression
group | 5.97±1.61 | 43 | 8 (18.60) | 8 (18.60) | 4 (9.30) | 12 (27.91) | 32
(74.41)a,b |
| Low expression
group | 4.36±1.52 | 35 | 4 (11.43) | 5 (14.29) | 2 (5.71) | 7 (20.00) | 18
(51.43)b |
| Control group | | 70 | 2 (2.86) | 2 (2.86) | 0 (0.00) | 5 (7.14) | 9 (12.86) |
| χ2
value | | | | | | | 44.670 |
| P-value | | | | | | | <0.01 |
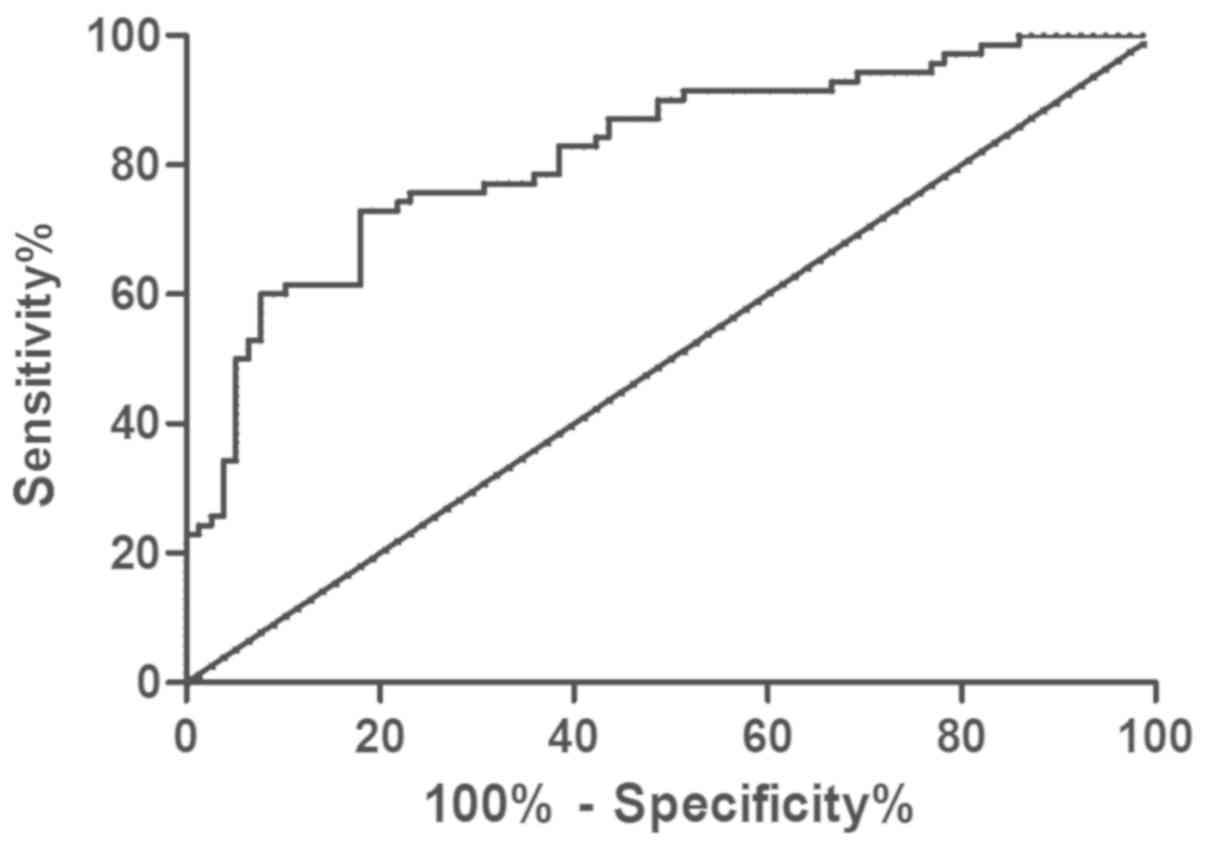
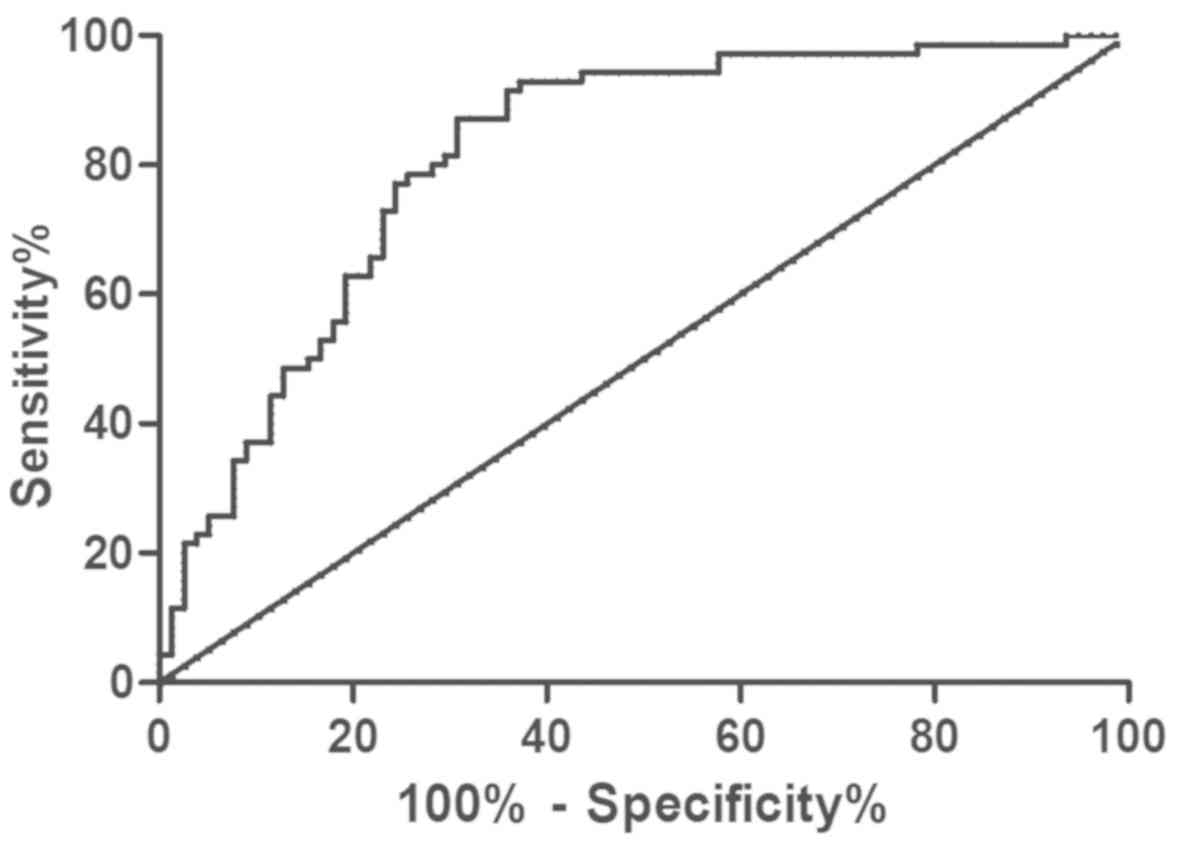
Prediction of GDM by ADP and
TNF-α
The expression levels of serum ADP and TNF-α in the
GDM patients were determined using ELISA, and ROC curves were
drawn. Analysis of the curves showed that the area under the curve
(AUC) of ADP was 0.821, and the sensitivity, specificity, critical
value, and 95% CI were 72.86, 82.05, 9.09, and 71.72-89.83%,
respectively; the AUC of TNF-α was 0.815, and the sensitivity,
specificity, critical value, and 95% CI were 87.14, 69.23, 5.32 and
57.76-79.19%, respectively (Figs. 2
and 3).
Association of ADP and TNF-α
concentrations with clinical pathology in the experimental
group
Analysis revealed that in the experimental group,
ADP was not significantly correlated with amniotic fluid volume,
abortion history, ethnicity, or dietary habit (all P>0.05), but
significantly and negatively correlated with age, pregestational
BMI, gestational week, medical history, and family history of
diabetes mellitus (all P<0.05). In addition, TNF-α was not
significantly correlated with ethnicity or dietary habit (both
P>0.05), but was significantly correlated with age,
pregestational BMI, gestational week amniotic fluid volume, medical
history, abortion history, and family history of diabetes mellitus
(all P<0.05). Details are shown in Tables V and VI.
| Table VAssociation of ADP with clinical
pathology in the experimental group . |
Table V
Association of ADP with clinical
pathology in the experimental group .
| Clinicopathological
characteristics | No. | Concentration
(mg/l) | t | P-value |
|---|
| Age, weeks | | | 2.243 | 0.029 |
|
>28 | 43 | 5.46±2.34 | | |
|
≤28 | 35 | 6.77±2.82 | | |
| Pregestational BMI,
kg/m2 | | | 2.558 | 0.013 |
|
≤22.15 | 49 | 6.42±2.05 | | |
|
>22.15 | 29 | 5.23±1.87 | | |
| Gestational
week | | | 2.111 | 0.038 |
|
≤20.23 | 30 | 6.19±1.87 | | |
|
>20.23 | 48 | 5.31±1.74 | | |
| Amniotic fluid
volume, ml | | | 0.204 | 0.839 |
|
≥2,000 | 14 | 6.28±2.56 | | |
|
<2,000 | 64 | 6.41±2.07 | | |
| Abortion
history | | | 0.444 | 0.658 |
|
Yes | 28 | 6.27±2.08 | | |
|
None | 50 | 6.49±2.11 | | |
| Medical
history | | | 2.412 | 0.018 |
|
Yes | 13 | 5.67±1.33 | | |
|
No | 65 | 6.89±1.72 | | |
| Family history of
diabetes mellitus | | | 2.120 | 0.037 |
|
Yes | 31 | 5.73±1.47 | | |
|
None | 47 | 6.54±1.76 | | |
| Ethnicity | | | 0.363 | 0.718 |
|
Han | 62 | 6.28±2.31 | | |
|
Minority | 16 | 6.52±2.54 | | |
| Dietary habit | | | 0.272 | 0.787 |
|
Light | 52 | 6.32±2.13 | | |
|
Spicy | 26 | 6.47±2.61 | | |
| Table VIAssociation of TNF-α with clinical
pathology in the experimental group. |
Table VI
Association of TNF-α with clinical
pathology in the experimental group.
| Clinicopathological
characteristics | n | Concentration
(ng/l) | t value | P-value |
|---|
| Age, weeks | | | 2.004 | 0.049 |
|
>28 | 43 | 6.88±1.72 | | |
|
≤28 | 35 | 6.04±1.98 | | |
| Pregestational BMI,
kg/m2 | | | 2.074 | 0.041 |
|
≤22.15 | 49 | 6.24±1.85 | | |
|
>22.15 | 29 | 7.25±2.42 | | |
| Gestational
week | | | 2.411 | 0.018 |
|
≤20.23 | 30 | 5.54±1.61 | | |
|
>20.23 | 48 | 6.71±2.33 | | |
| Amniotic fluid
volume, ml | | | 2.083 | 0.041 |
|
≥2,000 | 14 | 7.39±2.36 | | |
|
<2,000 | 64 | 6.14±1.96 | | |
| Abortion
history | | | 2.460 | 0.016 |
|
Yes | 28 | 6.24±1.72 | | |
|
None | 50 | 5.36±1.39 | | |
| Medical
history | | | 2.336 | 0.022 |
|
Yes | 13 | 6.73±2.31 | | |
|
No | 65 | 5.44±1.71 | | |
| Family history of
diabetes mellitus | | | 2.221 | 0.029 |
|
Yes | 31 | 6.47±2.27 | | |
|
None | 47 | 5.42±1.88 | | |
| Ethnicity | | | 1.375 | 0.173 |
|
Han | 62 | 6.48±2.11 | | |
|
Minority | 16 | 5.72±1.26 | | |
| Dietary habit | | | 0.963 | 0.338 |
|
Light | 52 | 5.48±1.91 | | |
|
Spicy | 26 | 5.89±1.45 | | |
Discussion
GDM refers to glucose intolerance that occurs or is
first recognized during pregnancy (13). It can be diagnosed when the patient
has no diabetes before pregnancy and fasting blood glucose ≥5.1
mmol/l, and occur in second and third trimester. Overweight and
obesity increase the risk of disease (14). GDM is a risk factor for type 2
diabetes mellitus. A study has shown that women with GDM history
face a higher risk of suffering from type 2 diabetes mellitus than
healthy pregnancy women (15).
Moreover, women with GDM face a higher risk of adverse pregnancy
outcomes such as macrosomia, dystocia, and abortion, of which
macrosomia is the result of maternal hyperglycemia accelerating
fetal growth (16). Moreover, women
with GDM also face a higher risk of suffering from cardiovascular
diseases after delivery (17,18).
Therefore, GDM is seriously endangering the health of pregnant
women and infants, and is likely to play an important role in the
global diabetes epidemic (19). At
present, GDM is mainly treated by lifestyle intervention, oral
hypoglycemic agents, and insulin injection (20,21), but
there are still adverse reactions such as neonatal hypoglycemia and
preeclampsia due to diseases (22).
A study concluded that insulin resistance is an
important pathophysiological factor of GDM (23). With the deepening of research,
increasing number of researchers have pointed out that many factors
including interleukin and adipocyte factors are involved in the
occurrence and progression of GDM (7). ADP is an endogenous bioactive
polypeptide or protein secreted by adipocytes, and an
insulin-sensitizing hormone, which is closely related to insulin
resistance, obesity, and cardiovascular diseases (24). TNF includes TNF-β secreted by
activated T lymphocytes and TNF-α secreted by monocyte-macrophage
cells, of which TNF-α is a pro-inflammatory cell and is considered
to be one of the important factors of insulin resistance in
diabetes mellitus (25). A previous
study revealed that the overall risk of type 2 diabetes mellitus
was closely related to TNF-α and low adiponectin concentration, and
they were predictive indexes of type 2 diabetes mellitus (26). However, the roles of ADP and TNF-α in
GDM remain unclear. Some studies considered that dysregulation of
various adipocyte factors in GDM may have pathophysiological and
prognostic significance in pregnancy complications (27). Inflammation is characterized by an
increase in the activity of inflammatory circulating biomarkers and
monocytes. The association of inflammation and hyperglycemia with
insulin resistance has been extensively studied in diabetic
patients (28). This investigation
was to provide relevant basis for screening and prediction of GDM
by studying the changes of ADP and TNF-α concentrations in the
blood of GDM patients, and their relationship with pregnancy
outcome. In this study, the controls were all healthy pregnant
women without gestational diabetes during pregnancy. The results
revealed that compared with healthy pregnant women, GDM patients
showed higher blood TNF-α expression and lower blood ADP
expression, which was consistent with previous research results
(29,30). The low expression of ADP was related
to age, pregestational BMI, gestational week, medical history, and
family history of diabetes mellitus (all P<0.05), and the high
expression of TNF-α was related to age, pregestational BMI,
gestational week, amniotic fluid volume, medical history, abortion
history, and family history of diabetes mellitus (all P<0.05).
After treatment, the GDM patients showed increased ADP
concentration and decreased TNF-α concentration. The study also
found that the rate of adverse pregnancy outcomes in the low ADP
expression group was higher than that in the high ADP expression
group (P<0.05), and the rate in the high TNF-α expression group
was higher than that in the low TNF-α expression group (P<0.05).
In addition, the risk of adverse pregnancy outcomes in the
experimental group was higher than that in the control group. In
the present study, GDM patients showed decreased ADP concentration
and increased TNF-α concentration, and indexes of delivery were
improved after treatment, suggesting that ADP and TNF-α were bound
up with GDM. However, whether the pregnancy outcomes can be
improved by interfering with ADP and TNF-α expression, and whether
there are the same inflammatory factors or adipocyte factors
involved in the occurrence of the disease need further study.
However, no basic research was carried out, so it
was impossible to assess how ADP and TNF-α participate in the
occurrence of diseases or to judge which treatment method can
better affect the expression of ADP and TNF-α. These aspects
require further research, together with the long-term effects of
ADP and TNF-α on puerperae and infants.
In conclusion, both ADP and TNF-α are abnormally
expressed in the GDM patients, and TNF-α is affected by more of the
factors. The concentrations of both ADP and TNF-α affect the
pregnancy outcomes. It suggests that ADP and TNF-α can be used as
indexes for predicating pregnancy outcomes, and for judging the
disease conditions and treatment situation of patients.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WW wrote the manuscript. WW and XZ conceived and
designed the study. WW and XZ were responsible for the collection
and analysis of the experimental data. XZ revised the manuscript
critically for important intellectual content. Both authors read
and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Qingpu Branch of Zhongshan Hospital Affiliated to Fudan University
(Shanghai,China). Patients who participated in this research had
complete clinical data. Signed informed consents were obtained from
the patients and/or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Pantham P, Aye IL and Powell TL:
Inflammation in maternal obesity and gestational diabetes mellitus.
Placenta. 36:709–715. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kampmann U, Madsen LR, Skajaa GO, Iversen
DS, Moeller N and Ovesen P: Gestational diabetes: A clinical
update. World J Diabetes. 6:1065–1072. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Zhu Y and Zhang C: Prevalence of
gestational diabetes and risk of progression to type 2 diabetes: A
Global Perspective. Curr Diab Rep. 16(7)2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Yu L, Zeng XL, Cheng ML, Yang GZ, Wang B,
Xiao ZW, Luo X, Zhang BF, Xiao DW, Zhang S, et al: Quantitative
assessment of the effect of pre-gestational diabetes and risk of
adverse maternal, perinatal and neonatal outcomes. Oncotarget.
8:61048–61056. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ainuddin J, Karim N, Hasan AA and Naqvi
SA: Metformin versus insulin treatment in gestational diabetes in
pregnancy in a developing country: A randomized control trial.
Diabetes Res Clin Pract. 107:290–299. 2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Chiefari E, Arcidiacono B, Foti D and
Brunetti A: Gestational diabetes mellitus: An updated overview. J
Endocrinol Invest. 40:899–909. 2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Zhang J, Chi H, Xiao H, Tian X, Wang Y,
Yun X and Xu Y: Interleukin-6 (IL-6) and tumor necrosis factor-α
(TNF-α) single nucleotide polymorphisms (SNPs), inflammation and
metabolism in gestational diabetes mellitus in Inner Mongolia. Med
Sci Monit. 23:4149–4157. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
da Costa RM, Neves KB, Mestriner FL,
Louzada-Junior P, Bruder-Nascimento T and Tostes RC: TNF-α induces
vascular insulin resistance via positive modulation of PTEN and
decreased Akt/eNOS/NO signaling in high fat diet-fed mice.
Cardiovasc Diabetol. 15(119)2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Chen L, Chen R, Wang H and Liang F:
Mechanisms linking inflammation to insulin resistance. Int J
Endocrinol. 2015(508409)2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
El-Tahan RR, Ghoneim AM and El-Mashad N:
TNF-α gene polymorphisms and expression. Springerplus.
5(1508)2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Akash MSH, Rehman K and Liaqat A: Tumor
necrosis factor-alpha: Role in development of insulin resistance
and pathogenesis of type 2 diabetes mellitus. J Cell Biochem.
119:105–110. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Kadowaki T, Yamauchi T, Kubota N, Hara K,
Ueki K and Tobe K: Adiponectin and adiponectin receptors in insulin
resistance, diabetes, and the metabolic syndrome. J Clin Invest.
116:1784–1792. 2006.PubMed/NCBI View
Article : Google Scholar
|
|
13
|
Kc K, Shakya S and Zhang H: Gestational
diabetes mellitus and macrosomia: A literature review. Ann Nutr
Metab. 66 (Suppl 2):14–20. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Billionnet C, Mitanchez D, Weill A, Nizard
J, Alla F, Hartemann A and Jacqueminet S: Gestational diabetes and
adverse perinatal outcomes from 716,152 births in France in 2012.
Diabetologia. 60:636–644. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lowe WL Jr, Scholtens DM, Lowe LP, Kuang
A, Nodzenski M, Talbot O, Catalano PM, Linder B, Brickman WJ,
Clayton P, et al: HAPO Follow-up Study Cooperative Research Group:
Association of gestational diabetes with maternal disorders of
glucose metabolism and childhood adiposity. JAMA. 320:1005–1016.
2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Macaulay S, Dunger DB and Norris SA:
Gestational diabetes mellitus in Africa: A systematic review. PLoS
One. 9(e97871)2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kessous R, Shoham-Vardi I, Pariente G,
Sherf M and Sheiner E: An association between gestational diabetes
mellitus and long-term maternal cardiovascular morbidity. Heart.
99:1118–1121. 2013.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Gabbe SG, Landon MB, Warren-Boulton E and
Fradkin J: Promoting health after gestational diabetes: A National
Diabetes Education Program call to action. Obstet Gynecol.
119:171–176. 2012.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Damm P, Houshmand-Oeregaard A, Kelstrup L,
Lauenborg J, Mathiesen ER and Clausen TD: Gestational diabetes
mellitus and long-term consequences for mother and offspring: A
view from Denmark. Diabetologia. 59:1396–1399. 2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Brown J, Alwan NA, West J, Brown S,
McKinlay CJ, Farrar D and Crowther CA: Lifestyle interventions for
the treatment of women with gestational diabetes. Cochrane Database
Syst Rev. 5(CD011970)2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Nachum Z, Zafran N, Salim R, Hissin N,
Hasanein J, Gam ZE, Letova Y, Suleiman A and Yefet E: Glyburide
versus metformin and their combination for the treatment of
gestational diabetes mellitus: A randomized controlled study.
Diabetes Care. 40:332–337. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Brown J, Grzeskowiak L, Williamson K,
Downie MR and Crowther CA: Insulin for the treatment of women with
gestational diabetes. Cochrane Database Syst Rev.
11(CD012037)2017.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Feng H, Su R, Song Y, Wang C, Lin L, Ma J
and Yang H: Positive correlation between enhanced expression of
TLR4/MyD88/NF-κB with insulin resistance in placentae of
gestational diabetes mellitus. PLoS One.
11(e0157185)2016.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Lekva T, Michelsen AE, Aukrust P,
Henriksen T, Bollerslev J and Ueland T: Leptin and adiponectin as
predictors of cardiovascular risk after gestational diabetes
mellitus. Cardiovasc Diabetol. 16(5)2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Li W, Yang X, Zheng T, Xing S, Wu Y, Bian
F, Wu G, Li Y, Li J, Bai X, et al: TNF-α stimulates endothelial
palmitic acid transcytosis and promotes insulin resistance. Sci
Rep. 7(44659)2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Liu C, Feng X, Li Q, Wang Y, Li Q and Hua
M: Adiponectin, TNF-α and inflammatory cytokines and risk of type 2
diabetes: A systematic review and meta-analysis. Cytokine.
86:100–109. 2016.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Miehle K, Stepan H and Fasshauer M:
Leptin, adiponectin and other adipokines in gestational diabetes
mellitus and pre-eclampsia. Clin Endocrinol (Oxf). 76:2–11.
2012.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Xie BG, Jin S and Zhu WJ: Expression of
toll-like receptor 4 in maternal monocytes of patients with
gestational diabetes mellitus. Exp Ther Med. 7:236–240.
2014.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Sudharshana Murthy KA, Bhandiwada A,
Chandan SL, Gowda SL and Sindhusree G: Evaluation of oxidative
stress and proinflammatory cytokines in gestational diabetes
mellitus and their correlation with pregnancy outcome. Indian J
Endocrinol Metab. 22:79–84. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Çetin C, Baş F, Uçar A, Poyrazoğlu S, Saka
N, Bundak R and Darendeliler F: Comparative analysis of
glucoinsulinemic markers and proinflammatory cytokines in
prepubertal children born large-versus appropriate-for gestational
age. Endocrine. 47:816–824. 2014.PubMed/NCBI View Article : Google Scholar
|