Introduction
There are a number of medications which can serve as
catalysts for drug-induced immune thrombocytopenia (DIPT) (1-3).
The majority of DITP cases result in mild symptoms, but there have
been documented instances of dangerous bleeding. A minimum of six
different mechanisms have been put forward as the means by which
drug-induced antibodies can encourage platelet destruction, thus
emphasising the complexity of the pathogenesis of DITP. It is
technically possible to identify the antibodies that react with
platelets when they come in contact with the sensitising drug, but
due to the complexity of the testing and the rarity of the
necessary equipment and expertise, this is often not practical.
Rather, in the vast majority of cases the decision to halt the
suspected medication of subjects who experience DITP is better made
on clinical grounds (4). Acyclovir,
an acyclic purine nucleoside analogue, has been widely used because
of its highly potent prohibitive properties for infections caused
by HSV and VZV (5). Nausea,
diarrhea, dizziness, headaches, and mental changes are the most
common and well-known side effects of this drug. Severe adverse
effects such as neurotoxicity, kidney disorders and psychiatric
effects are not common, mostly related to high dose intravenous
administrations (6-8).
Immune thrombocytopenia induced by acyclovir is unusual.
Case report
A 72-year-old woman was admitted to the Dermatology
Clinic with a moderate clinical form of herpes zoster located on
left thorax area. She was treated with acyclovir in an oral dose of
800 mg five times per day for a proposed period of 10 days with
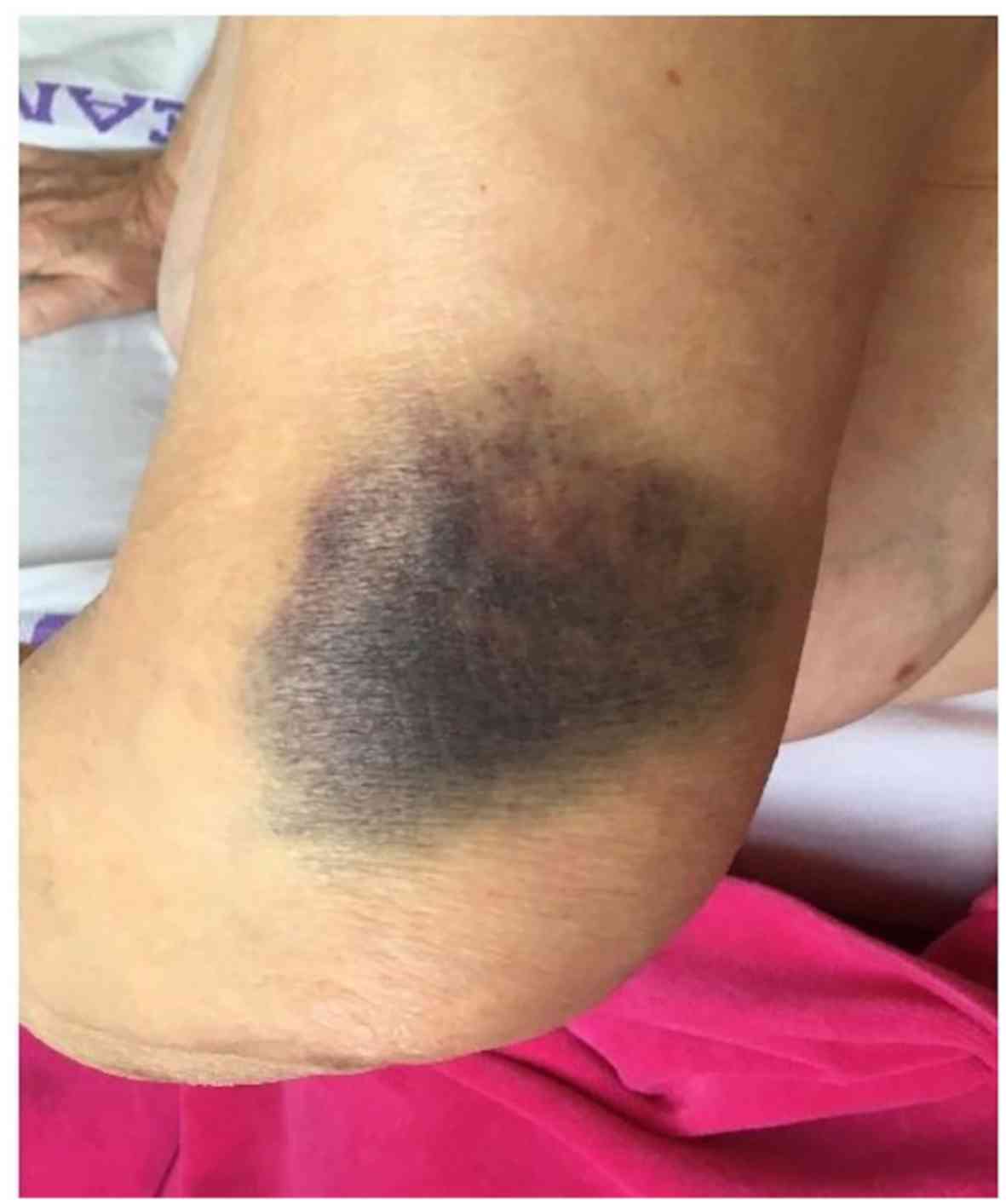
local treatment. On the seventh day of the treatment the patient
presented two round ovalar hematomas. One with 10-cm diameters
located on the left cubital area and another with 7-cm diameter
situated on the right femoral area (Figs. 1 and 2). The patient denied any local trauma to
these areas. She also denied fever, hematochezia, melena,
hemoptysis, hematuria, or any neurologic symptoms. There was no
history of smoking, systemic diseases, or drug allergy. The family
and social history, were unremarkable. No other drugs were taken
before and during the treatment of the herpes zoster virus
infection. Laboratory tests: The performed laboratory tests on the
day of presentation showed normal limits for hemoglobin, white
blood cells and the platelet count was 15x109/l. Also
the liver function, electrolyte profile, renal function and
coagulation studies were in normal limits.
New laboratory tests were performed at the time of
the appearance of the hematomas. The hematologic analysis showed
normal limits except the platelet count which was lower at the
value of 5x109/l. Tests for cytomegalovirus, hepatitis
A, B and C viruses, and Epstein-Barr virus were performed and
yielded negative results. The performed HIV test was also negative.
The hematological consult excluded common known causes of
thrombocytopenia. In order to prove a drug-induced immune
thrombocytopenia, detection of acyclovir-dependent platelet
antibodies was performed using enzyme-linked immunoassay (ELISA)
which was positive. The clinical and laboratory findings, taken
together with the transitory relationship between acyclovir and the
start of thrombocytopenia, combined with the elimination of the
other know sources of thrombocytopenia, allowed us to reach the
diagnosis of acyclovir-induced immune thrombocytopenia. The
administration of acyclovir was discontinued and oral prednisone
treatment was introduced at 1 mg/kg body weight dose. The platelet
count was checked every second day and began to rise 10 days after
discontinuation of acyclovir and returned to normal values over a
period of 15 days. After this period the dose of prednisone was
decreased with 5 mg, every 3 days. The patient left the hospital
clinically healed with normal levels of hematological laboratory
findings including a normal platelet count level.
Discussion
Epidemiologic studies performed in the US and Europe
suggest that ~10 persons per million are affected by DITP each year
(9). The real incidence is unknown,
but could be higher in elderly especially with associated severe
co-morbidities and hospitalized persons, who are more likely to be
exposed to different medications. The first report of DITP was
published in 1865(10). Despite the
low frequency, DITP is important to recognize because >200
drugs, including some herbal medicines, that have been reported to
be causative (11). A minimum of six
different mechanisms have been put forward as the means by which
drug-induced antibodies can encourage platelet destruction, thus
emphasising the complexity of the pathogenesis of DITP. The
majority of DITPs are believed to have a drug-dependent immune
mechanism as their source. How drugs induce platelet antibodies and
how platelets are destroyed by these antibodies are still unclear
(4). The clinical diagnosis of DITP
is based on a few key features like: a) extensive petechiae,
ecchymosis or hematomas appeared a few days after taking the
putative drug, b) markedly low blood platelet levels appeared ~3-10
days after starting a putative medication, c) platelet counts
return to normal at ~7 days after stopping the putative drug
(usually in 1-10 days) and d) exclusion of common known causes of
thrombocytopenia (12,13). In laboratory findings the presence of
the specific drug-dependent platelet antibodies are crucial for the
diagnosis. Also a careful, detailed personal and family history is
important to patient evaluation. After examining methodologically
and in detail the instances of drug-induced thrombocytopenia
through 2008, George et al (14) constructed a database which catalogued
the suspected drugs. The database is updated at regular intervals
and can be accessed online at http://www.ouhsc.edu/platelets. They also devised a
set of four clinical criteria and four levels of evidence to assess
the likelihood that individual drugs are capable of causing DITP.
In our case, the clinical aspect, the exclusion of other etiologies
of thrombocytopenia, platelet count fluctuation, and the positive
anti-platelet antibodies, and with the temporal relationship
between the acyclovir and the start of thrombocytopenia allowed us
to reach the diagnosis of acyclovir-induced immune
thrombocytopenia. Based on the published clinical criteria we
ranked the relationship between the drug and the disease on level 2
of evidence meeting three criteria of the four. The first step in
the treatment is to discontinue medication in a patient with
possible DITP. In many cases platelet levels start to increase
without any medication. It is recommended as a common practice to
administer corticosteroids, but whether they are beneficial in
patients with DITP is not established. Other treatment options are
mentioned in the literature i.e. platelet transfusion, intravenous
IgG, or even plasma exchange with different results (15-17).
Our patient was treated with oral corticosteroid with a good
result. An international database search was employed to complete
an extensive review of the current literature. Contemporary
information on acyclovir-induced immune thrombocytopenia was
further informed by the analysis of present day review articles and
accessible case reports. Search of PubMed/MEDLINE, Google Scholar,
and Web of Science databases found five published cases of
acyclovir-induced immune thrombocytopenia (18-22).
Acyclovir treatment was indicated for herpes simplex infection in
three cases (18,20,22) and
for zoster in two cases, similarly to our case (19,21). For
the herpes simplex infections the treatment was oral, like in our
case, in the other cases the administration of the drug was
parenteral. All the cases were males aged between 20 and 81 years,
except our presented case. The evolution in all the cases was
similar, the clinical findings and the lower level of platelet
count appeared after 4-8 days after starting the acyclovir
treatment. In all the cases the specific drug-dependent platelet
antibodies were done, with positive results. In all cases the
treatment was stopped and different treatment options were used.
Oral prednisone in one case, as in our case, intravenous IgG in one
case, platelet mass transfusion in one case and in the others
supportive treatment was used. In two cases the patients were
without remarkable co-morbidities, similarly to our presented case
(19,21). The other patients had severe
co-morbidities such as systemic lupus, AIDS and chronic obstructive
pulmonary disease, and were also treated for these diseases
(18,20,22). In
every case the evolution was good, platelet count levels became
normal in 10-15 days (18-22).
The immune thrombocytopenia induced by acyclovir is rare and an
unusual side effect of a commonly used drug. Most DITPs are thought
to be caused by, still unclear, drug-dependent immune mechanism. In
elderly patients, and especially those with associated severe
co-morbidities, who need to be treated with acyclovir, regular
platelet count measurement should be considered. Prompt diagnosis
is vital to appropriate management, therefore clinicians need to be
cognisant of this rare potential adverse reaction (23,24).
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
GLF was responsible for the clinical management of
the patient, the evaluation and analysis of the data, and the
writing of the manuscript. LF was involved in the conception of the
study and was responsible for the preparation and revisions of the
manuscript. RA, SLI, and MD were responsible for the literature
research and the revisions of the manuscript. IB was involved in
the conception of the study and contributed to the writing of the
manuscript. The final version of the article was read and approved
by all the authors.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
the Romanian College of Physicians of Mures County (Târgu Mureș,
Romania).
Patient consent for publication
Written informed consent was obtained from the
patient.
Competing interests
The authors declare that they have no competing
interests.
Authors' information
GLF: Associate Professor of Dermatology, Department
of Dermatology, Dermatology Clinic, ‘George Emil Palade’ University
of Medicine, Pharmacy, Science and Technology (Târgu Mureş,
Romania).
References
|
1
|
Tatu AL, Elisei AM, Chioncel V, Miulescu M
and Nwabudike LC: Immunologic adverse reactions of β-blockers and
the skin (Review). Exp Ther Med. 18:955–959. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Fekete GL and Fekete L: Cutaneous
leukocytoclastic vasculitis associated with erlotinib treatment: A
case report and review of the literature. Exp Ther Med.
17:1128–1131. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tatu AL, Ciobotaru OR, Miulescu M, Buzia
OD, Elisei AM, Mardare N, Diaconu C, Robu S and Nwabudike LC:
Hydrochlorothiazide: Chemical structure, therapeutic, phototoxic
and carcinogenetic effects in dermatology. Rev Chim (Bucharest).
69:2110–2114. 2018.
|
|
4
|
Aster RH, Curtis BR, McFarland JG and
Bougie DW: Drug-induced immune thrombocytopenia: Pathogenesis,
diagnosis, and management. J Thromb Haemost. 7:911–918.
2009.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Dworkin RH, Johnson RW, Breuer J, Gnann
JW, Levin MJ, Backonja M, Betts RF, Gershon AA, Haanpaa ML,
McKendrick MW, et al: Recommendations for the management of herpes
zoster. Clin Infect Dis. 44 (Suppl 1):S1–S26. 2007.PubMed/NCBI View
Article : Google Scholar
|
|
6
|
Busso M and Berman B: Antivirals in
dermatology. J Am Acad Dermatol. 32:1031–1040. 1995.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Adair JC, Gold M and Bond RE: Acyclovir
neurotoxicity: Clinical experience and review of the literature.
South Med J. 87:1227–1231. 1994.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Haefeli WE, Schoenenberger RA, Weiss P and
Ritz RF: Acyclovir-induced neurotoxicity: Concentration - side
effect relationship in acyclovir overdose. Am J Med. 94:212–215.
1993.PubMed/NCBI View Article : Google Scholar
|
|
9
|
van den Bemt PM, Meyboom RH and Egberts
AC: Drug-induced immune thrombocytopenia. Drug Saf. 27:1243–1252.
2004.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Vipan W: Quinine as a cause of purpura.
Lancet. 86(37)1865.
|
|
11
|
Aster RH and Bougie DW: Drug-induced
immune thrombocytopenia. N Engl J Med. 357:580–587. 2007.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Chong BH: Drug-induced immune
thrombocytopenia. Platelets. 2:173–181. 1991.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Visentin GP and Liu CY: Drug-induced
thrombocytopenia. Hematol Oncol Clin North Am. 21:685–696.
vi:2007.PubMed/NCBI View Article : Google Scholar
|
|
14
|
George JN, Raskob GE, Shah SR, Rizvi MA,
Hamilton SA, Osborne S and Vondracek T: Drug-induced
thrombocytopenia: A systematic review of published case reports.
Ann Intern Med. 129:886–890. 1998.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Crosby WH: Editorial: Wet purpura, dry
purpura. JAMA. 232:744–745. 1975.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ray JB, Brereton WF and Nullet FR:
Intravenous immune globulin for the treatment of presumed
quinidine-induced thrombocytopenia. DICP. 24:693–695.
1990.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Pourrat O: Treatment of drug-related
diseases by plasma exchanges. Ann Med Interne (Paris). 145:357–360.
1994.PubMed/NCBI
|
|
18
|
Tsappa I, Missouris C and Psarellis S:
Acyclovir-induced thrombocytopenia in a patient with SLE. BMJ Case
Rep. 2018(pii: bcr-2018-225118)2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Hong X, Wang X and Wang Z: A rare case
report of acyclovir- induced immune thrombocytopenia with tongue
hematomas as the first sign, and a literature review. BMC Pharmacol
Toxicol. 18(12)2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kamboj J, Wu F, Kamboj R, Suzue K and
Khosla P: A rare case of acyclovir-induced thrombocytopenia. Am J
Ther. 21:e159–162. 2014.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Katsenos S, Gkolias D and Nikolopoulou M:
Acyclovir-induced immune thrombocytopenia in a patient with herpes
zoster of the trigeminal nerve. Pharmacotherapy. 30:1085–1086.
2010.
|
|
22
|
Cersosimo RJ, Hankins MA and Hamrah SD: An
unusual case of thrombocytopenia and leukopenia associated with
diltiazem and acyclovir. J Pharm Technol. 19:154–158. 2003.
|
|
23
|
Fekete GL, Cotoi OS and Fekete JE:
Multiple nodular cutaneous metastasis as first clinical sign of
signet ring cell gastric carcinoma - case report. Acta
Dermatovenerol Croat. 20:34–37. 2012.PubMed/NCBI
|
|
24
|
Brănişteanu DE, Pintilie A, Andreş LE,
Dimitriu A, Oanţă A, Stoleriu G and Brănişteanu DC: Ethiopatogenic
hypotheses in lichen planus. Rev Med Chir Soc Med Nat Iasi.
120:760–767. 2016.PubMed/NCBI
|