Introduction
Endometriosis is one of the most common benign
conditions affecting women. The prevalence of the disease is ~10%
in females of reproductive age (15-49 years) and 20-50% in those
diagnosed with infertility (1,2).
Dysmenorrhea, chronic pelvic pain and infertility are commonly
associated with the disorder (3).
Endometriosis can be classified as either superficial or deep.
Peritoneal infiltration of <5 mm is defined as superficial
endometriosis. The presence of endometrial tissue, fibrosis and
hyperplasia with >5 mm peritoneal infiltration is defined as
deep infiltrating endometriosis (DIE) (3). DIE accounts for 15-30% of all diagnosed
endometriosis cases (4,5). While there is no known cure for the
disease, available treatment options include expectant management,
hormonal therapy and surgical management (6). Treatment is usually personalized,
considering the therapeutic goal (subfertility or pain relief) and
the site of disease (6).
Pharmacological therapies for endometriosis include
progestogens, the combined oral contraceptive pill,
gonadotropin-releasing hormone agonists and weak androgens
(7). These drugs alleviate the
symptoms of chronic pelvic pain and dysmenorrhoea; however, they
are associated with adverse events, including irritability, breast
discomfort, bone loss and androgenic symptoms (7). Surgical treatment of endometriosis can
alleviate pain and improve fertility. However, 5-year recurrence
rates following surgery are high (40-50%) (8,9). The
potential success and impact of these strategies is dependent on
early and accurate diagnosis (10).
Laparoscopic observation and biopsy are considered to be the gold
standard for diagnosis of DIE (9).
However, laparoscopy is invasive and does not allow any time for
preoperative planning. Several non-invasive imaging modalities,
such as physical examination, transvaginal ultrasonography (TVUS),
transrectal sonography (TRUS) and MRI, are also available for the
diagnosis of DIE (11). Accuracy of
such non-invasive modalities would ensure their use as standard,
significantly reducing the risk associated with surgery while
facilitating early diagnosis and treatment (11). A number of studies have attempted to
assess the accuracy of such non-invasive diagnostic modalities for
DIE in various settings with different results. However, to the
best of our knowledge, there have been no systematic efforts to
collate evidence comparing these different diagnostic techniques.
Therefore, the purpose of the present study was to systematically
search the literature and perform a meta-analysis of diagnostic
data to compare the accuracy of physical examination, ultrasound
techniques (TVUS & TRUS) and MRI in the diagnosis of DIE.
Materials and methods
Inclusion criteria Studies
All studies examining the diagnostic accuracy of
physical examination, ultrasound techniques (TVUS or TRUS) and MRI
for diagnosis of DIE were included where they reported sensitivity
and specificity values of any of the aforementioned diagnostic
techniques or provided the data required to calculate these rates.
Studies published as full-text manuscripts were included while
abstracts and case reports were excluded.
Participants. Studies conducted on patients
with suspected DIE were included irrespective of the medical
co-morbidities suffered by the participants and the setting in
which the study was conducted.
Index test. Studies utilizing physical
examination, TVUS, TRUS or MRI to diagnose DIE were included.
Reference standards. Studies were included
only if the diagnostic accuracy of physical examination, TVUS, TRUS
or MRI was compared with standard laparoscopic or histopathological
examination. Diagnosis using the reference standard must have been
made by specialist doctors or trained researchers.
Search strategy
An extensive electronic search of the Medline
(PubMed) (https://pubmed.ncbi.nlm.nih.gov/), Scopus (https://www.scopus.com/), Embase (https://www.embase.com/), and Cochrane library
(https://www.cochranelibrary.com/) was
conducted. A combination of medical subject heading (MeSH) and
free-text terms was used to conduct the literature search. The
following MeSH terms and free-text terms were used for the
literature search: ‘Validation studies’, ‘deep infiltrating
endometriosis’, ‘physical examination’, ‘transvaginal
ultrasonography’, ‘transrectal ultrasonography’, ‘magnetic
resonance imaging’, ‘gynaecological disorders’, ‘sensitivity’,
‘specificity’, ‘diagnosis’, ‘endometriosis’ and ‘diagnostic
accuracy studies’. These search terms were used in various
combinations using Boolean operators such as ‘AND’, ‘OR’ or ‘NOT’.
Additional filters related to timeline of search in the database
was between their inception and September 2019. The language of the
studies was restricted to English.
Selection of studies
The literature search was performed by two
investigators independently. Records were screened by their title,
abstract and keywords for possible inclusion in the review. Full
texts of relevant studies were extracted and screened further,
based on the eligibility criteria for final inclusion in the
review. The reference list of all full-text articles was searched
manually to identify any missed studies. Any disagreements between
the two authors during the entire selection process were resolved
either through consensus or consultation with an independent third
investigator.
Data extraction and management
The primary investigator extracted the relevant
study characteristics for the review from all included studies. The
following data were extracted: Author, year of publication, study
design, study setting, index test, reference standards,
comorbidities, number of participants, mean age, inclusion and
exclusion criteria, true positives, true negatives, false positives
and false negatives. Data was transferred to STATA software version
14.2 (StataCorp LLC) by the primary investigator. Data entry was
double-checked for accuracy by the third investigator.
Risk of bias assessment
The risk of bias in all of the included studies was
assessed by two investigators independently using the quality
assessment of diagnostic accuracy studies-2 (QUADAS-2) tool
(12). The following domains were
used for the assessment of the risk of bias: Patient selection,
index test, reference standard and flow and timing of assessments.
Each domain was graded as high, low or unclear risk of bias. Any
discrepancies were resolved by consensus or consultation with the
third investigator.
Statistical analysis
Meta-analysis was performed using STATA software
version 14.2 (StataCorp LLC) to obtain the pooled estimate and 95%
confidence intervals (CI) of sensitivity, specificity, positive
likelihood ratio (LRP), negative likelihood ratio (LRN) and summary
diagnostic odds ratio (DOR) for each of the diagnostic tests.
Summary receiver operator characteristic (sROC) curves were
constructed and the area under the curve (AUC) was obtained. Each
data point in the sROC curve represents a separate study. Test
performance accuracy was classified as follows: AUC 0.5±0.7, low;
AUC 0.7±0.9, medium; and AUC >0.9, high (13).
Forest plots were used to graphically represent the
study-specific and pooled estimates. A Fagan plot was constructed
to estimate how much the result of a diagnostic test changes the
probability that a patient has DIE. Between-study heterogeneity was
assessed using bivariate box plots, χ2 tests and
I2 statistics. I2 values of <25% indicated
mild heterogeneity, 25-75% indicated moderate heterogeneity and
>75% indicated substantial heterogeneity (14). Publication bias was assessed
graphically via funnel plots and the asymmetry of the plot was
evaluated using Deek's test.
Results
Selection of studies
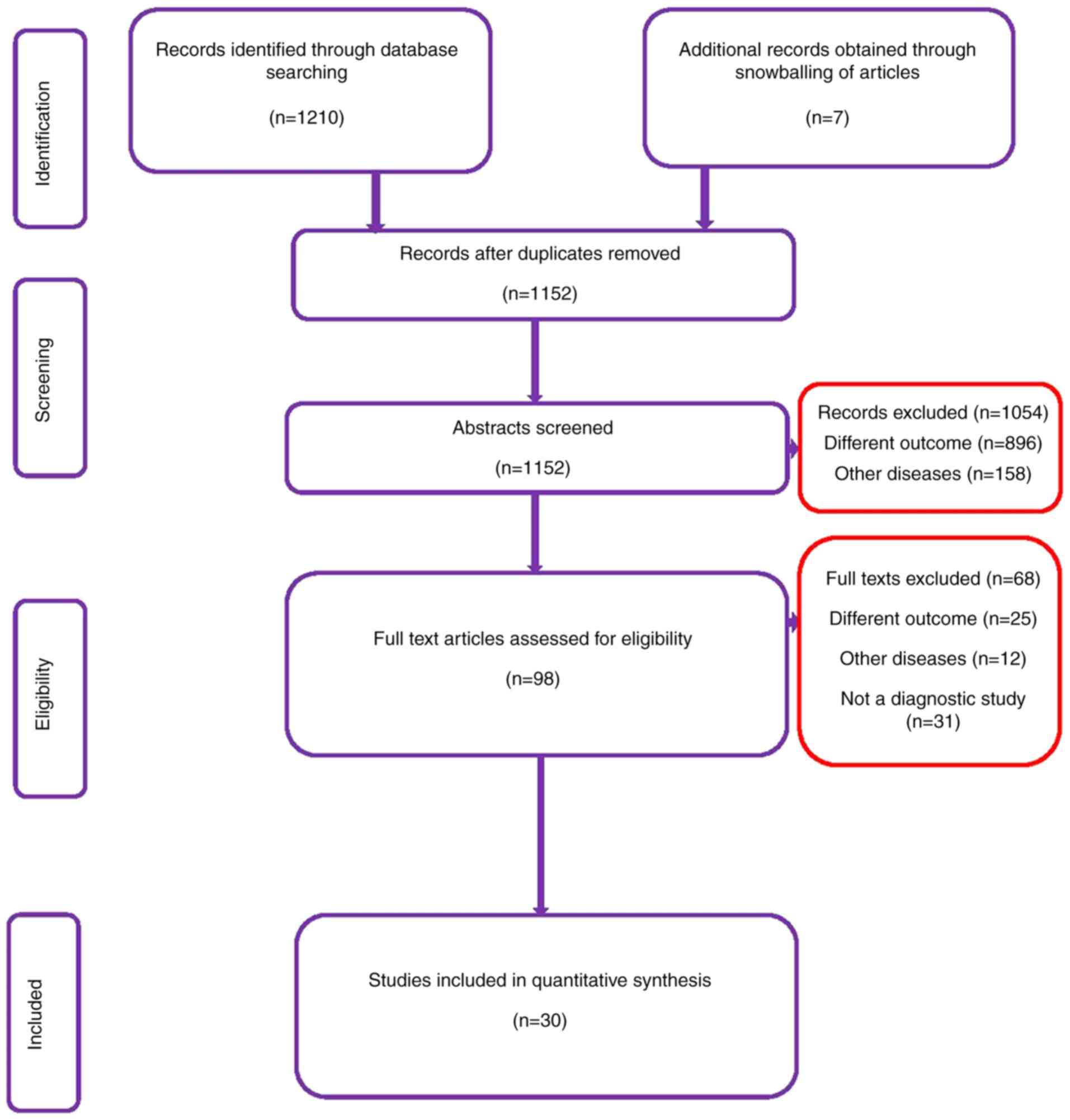
In total, 1,210 citations were found, of which 445
were retrieved from Medline, 411 from Scopus, 302 from Embase and
52 from the Cochrane library. After the first stage of screening
(title, abstract and keywords), 98 relevant studies were retrieved.
The full text of these studies was reviewed based on the
eligibility criteria. Bibliographies of the retrieved articles were
reviewed, and 7 additional studies were identified. In the final
analysis 30 studies with 4,565 participants satisfying the
inclusion criteria were included (Fig.
1) (15-44).
Characteristics of included
studies
Characteristics of the studies are described in
Table I. With the exception of
Chapron et al (19), all
included studies were prospective studies. All the studies were
conducted in high-income countries as per World Bank income group
country classification (45). The
majority of the studies (50%) were conducted in Italy followed by
the United Kingdom, France, the United States of America and
Austria. The mean age of the participants ranged from 28-36 years.
In total, 4,565 participants were assessed in the included studies,
with 469 participants undergoing physical examination, 3,847
undergoing TVUS, 728 undergoing TRUS and 1,298 undergoing MRI. The
total sample size of studies varied from 31-1,440 participants.
Among the 30 studies included, 5 studies reported on the diagnostic
accuracy of physical examination, 21 on TVUS, 6 on TRUS and 13 on
MRI.
 | Table ICharacteristics of the included
studies (n=30). |
Table I
Characteristics of the included
studies (n=30).
| Author, year | Country | Study design | Population
size | Type of diagnostic
modality | Gold standard
comparator | Mean patient age,
years | Time interval
between index test and standards reference | (Refs.) |
|---|
| Abrao et al,
2007 | Brazil | Prospective cross-
sectional study | 104 | Clinical
examination, TVUS, MRI | Laparoscopy +
histopathology | 33.8 | 3 months | (15) |
| Alborzi et
al, 2018 | Iran | Prospective
longitudinal study | 317 | TVUS, TRUS,
MRI | Laparoscopy +
histopathology | 31.0 | Not specified | (16) |
| Bazot et al,
2009 | France | Longitudinal | 92 | Clinical
examination, TVUS, TRUS, MRI | Laparoscopy,
laparotomy + histopathology | 31.8 | <12 months | (17) |
| Bergamini et
al, 2010 | Italy | Prospective | 61 | TRUS | Laparoscopy,
laparotomy + histopathology | 33.1 | Not specified | (18) |
| Chapron et
al, 2004 | France | Retrospective | 81 | TRUS, MRI | Laparoscopy or
laparotomy | 31.9 | Not specified | (19) |
| Charmie et
al, 2009 | Brazil | Prospective | 92 | MRI | Laparoscopy +
histopathology | 33.0 | Not specified | (20) |
| Dessole et
al, 2003 | Italy | Prospective | 46 | TVUS | Laparoscopy,
laparotomy + histopathology | 30.3 | Not specified | (21) |
| Eskenazi et
al, 2001 | Italy | Prospective (study
sample) Retrospective (test sample) | 90 | Clinical
examination, TVUS | Laparoscopy,
laparotomy + histopathology | 35.7 | 34 days | (22) |
| Fedele et
al, 1998 | Italy | Prospective | 140 | TRUS | Laparoscopy,
laparotomy + histopathology | 30.2 | 1 week | (23) |
| Grasso et
al, 2009 | Italy | Prospective | 33 | TVUS, MRI | Laparoscopy +
histopathology | 35.0 | 1-4 weeks | (24) |
| Guerriero et
al, 2007 | Italy | Prospective | 50 | TVUS | Laparoscopy +
histopathology | 33.0 | Within 7 days | (25) |
| Guerriero et
al, 2008 | Italy | Prospective | 88 | TVUS | Laparoscopy +
histopathology | 33.0 | Within 7 days | (26) |
| Guerriero et
al, 2014 | Italy | Prospective | 202 | TVUS | Laparoscopy +
histopathology | 34.0 | Within 1 month | (27) |
| Guerriero et
al, 2017 | Italy | Prospective | 159 | TVUS, MRI | Laparoscopy +
histopathology | 33.0 | Surgery was
performed over 5 years of analysis | (28) |
| Ha et al,
1994 | Korea | Prospective | 186 | MRI | Laparoscopy +
histopathology | 35.0 | Within 2 weeks | (29) |
| Holland et
al, 2010 | London, United
Kingdom | Prospective | 201 | TVUS | Laparoscopy +
histopathology | 34.9 | Mean duration =37.5
days | (30) |
| Holland et
al, 2013 | London, United
Kingdom | Prospective | 198 | TVUS | Laparoscopy +
histopathology | 35.0 | Mean duration =36.8
days | (31) |
| Hudelist et
al, 2011 | United Kingdom | Prospective | 129 | Clinical
examination, TVUS | Laparoscopy +
histopathology | 32.2 | Within 3
months | (32) |
| Hudelist et
al, 2013 | Austria | Prospective | 117 | TVUS | Laparoscopy +
histopathology | 31.6 | Within 2
months | (33) |
| Manganaro et
al, 2013 | Italy | Prospective | 42 | MRI | Laparoscopy +
histopathology | 28.0 | Within 3
months | (34) |
| Piessens et
al, 2014 | Australia | Prospective | 85 | TVUS | Laparoscopy +
histopathology | Age range given
(18-48) | Within 12
months | (35) |
| Ribeiro et
al, 2008 | United Kingdom | Prospective | 37 | TRUS | Laparoscopy +
histopathology | 35.8 | 1-3 months | (36) |
| Saba et al,
2011 | Italy | Prospective | 59 | TVUS, MRI | Laparoscopy,
laparotomy + histopathology | Not given | Not specified | (37) |
| Saccardi et
al, 2012 | Italy | Prospective | 54 | Clinical
examination, TVUS, MRI | Laparoscopy +
histopathology | 32.3 | Not specified | (38) |
| Savelli et
al, 2011 | Italy | Prospective | 69 | TVUS | Laparoscopy +
histopathology | 33.6 | Within 1 month | (39) |
| Stratton et
al, 2003 | USA | Prospective | 48 | MRI | Laparoscopy +
histopathology | Age range
(20-44) | Within 1 month | (40) |
| Takeuchi et
al, 2005 | Japan | Prospective | 31 | MRI | Laparoscopy +
histopathology | 32.1 | Not specified | (41) |
| Ubaldi et
al, 1998 | Belgium | Prospective | 133 | TVUS | Laparoscopy +
histopathology | Age range
(21-41) | 1 day | (42) |
| Valenzeno Menada
et al, 2008 | Italy | Prospective | 181 | TVUS | Laparoscopy +
histopathology | 32.0 | Not specified | (43) |
| Vimercati et
al, 2012 | Italy | Prospective | 1440 | TVUS | Laparoscopy +
histopathology | 34.0 | 4-8 weeks | (44) |
Methodological quality of the included
studies
The risk of bias assessment of the included studies
is presented in Table II and
Fig. S1. A total of 13 studies had
a high risk of bias for patient selection, while 5 studies had a
high risk of bias for the conduct and interpretation of the index
test domain. A total of 12 studies had a high risk of bias due to
the conduct and interpretation of reference standards and 12
studies had a high risk of bias for the flow of patients and the
time interval between index test and reference standard.
| Table IIRisk of bias assessment for the
included studies (n=30). |
Table II
Risk of bias assessment for the
included studies (n=30).
| Author, year | Selection bias | Index test
standards | Reference test
standards | Flow and timing of
Index and Reference standard | (Refs.) |
|---|
| Abrao et al,
2007 | Low | Low | Low | Low | (15) |
| Alborzi et
al, 2018 | Low | Low | High | Low | (16) |
| Bazot et al,
2009 | Low | Low | Low | Low | (17) |
| Bergamini et
al, 2010 | Low | High | High | High | (18) |
| Chapron et
al, 2004 | High | High | High | High | (19) |
| Charmie et
al, 2009 | High | Low | High | High | (20) |
| Dessole et
al, 2003 | Low | High | High | High | (21) |
| Eskenazi et
al, 2001 | High | Low | Low | Low | (22) |
| Fedele et
al, 1998 | Low | Low | Low | High | (23) |
| Grasso et
al, 2009 | High | Low | Low | Low | (24) |
| Guerriero et
al, 2007 | Low | Low | Low | Low | (25) |
| Guerriero et
al, 2008 | Low | Low | Low | Low | (26) |
| Guerriero et
al, 2014 | Low | Low | Low | Low | (27) |
| Guerriero et
al, 2017 | Low | Low | Low | Low | (28) |
| Ha et al,
1994 | High | Low | High | Low | (29) |
| Holland et
al, 2010 | Low | Low | Low | Low | (30) |
| Holland et
al, 2013 | Low | Low | Low | Low | (31) |
| Hudelist et
al, 2011 | Low | Low | Low | Low | (32) |
| Hudelist et
al, 2013 | Low | Low | Low | Low | (33) |
| Manganaro et
al, 2013 | High | Low | Low | Low | (34) |
| Piessens et
al, 2014 | Low | Low | High | Low | (35) |
| Ribeiro et
al, 2008 | Low | Low | High | Low | (36) |
| Saba et al,
2011 | Low | Low | Low | High | (37) |
| Saccardi et
al, 2012 | Low | Low | Low | High | (38) |
| Savelli et
al, 2011 | Low | High | Low | Low | (39) |
| Stratton et
al, 2003 | High | Low | Low | Low | (40) |
| Takeuchi et
al, 2005 | High | Low | Low | Low | (41) |
| Ubaldi et
al, 1998 | Low | Low | Low | Low | (42) |
| Valenzeno Menada
et al, 2008 | High | Low | Low | High | (43) |
| Vimercati et
al, 2012 | Low | Low | Low | Low | (44) |
Diagnostic performance of physical
examination
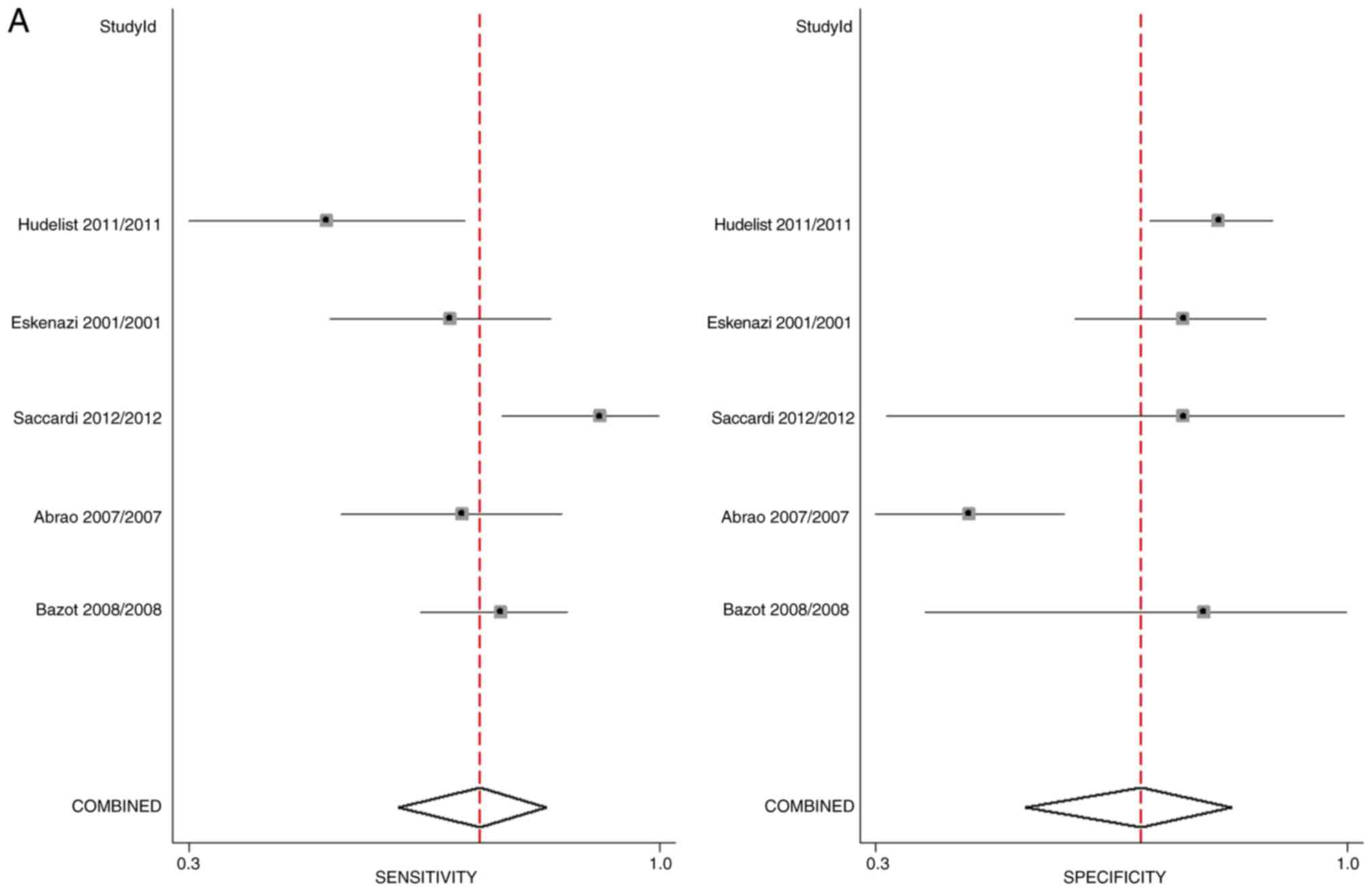
In total, five studies assessed the diagnostic
accuracy of physical examination for DIE. The pooled sensitivity
and specificity of physical examination for the diagnosis of DIE
were 71% (95% CI, 60-80%) and 69% (95% CI, 54-82%), respectively.
The DOR was 5 (95% CI, 3-12) as indicated by the Forest plot
(Fig. 2A). LRP was 2.3 (95% CI,
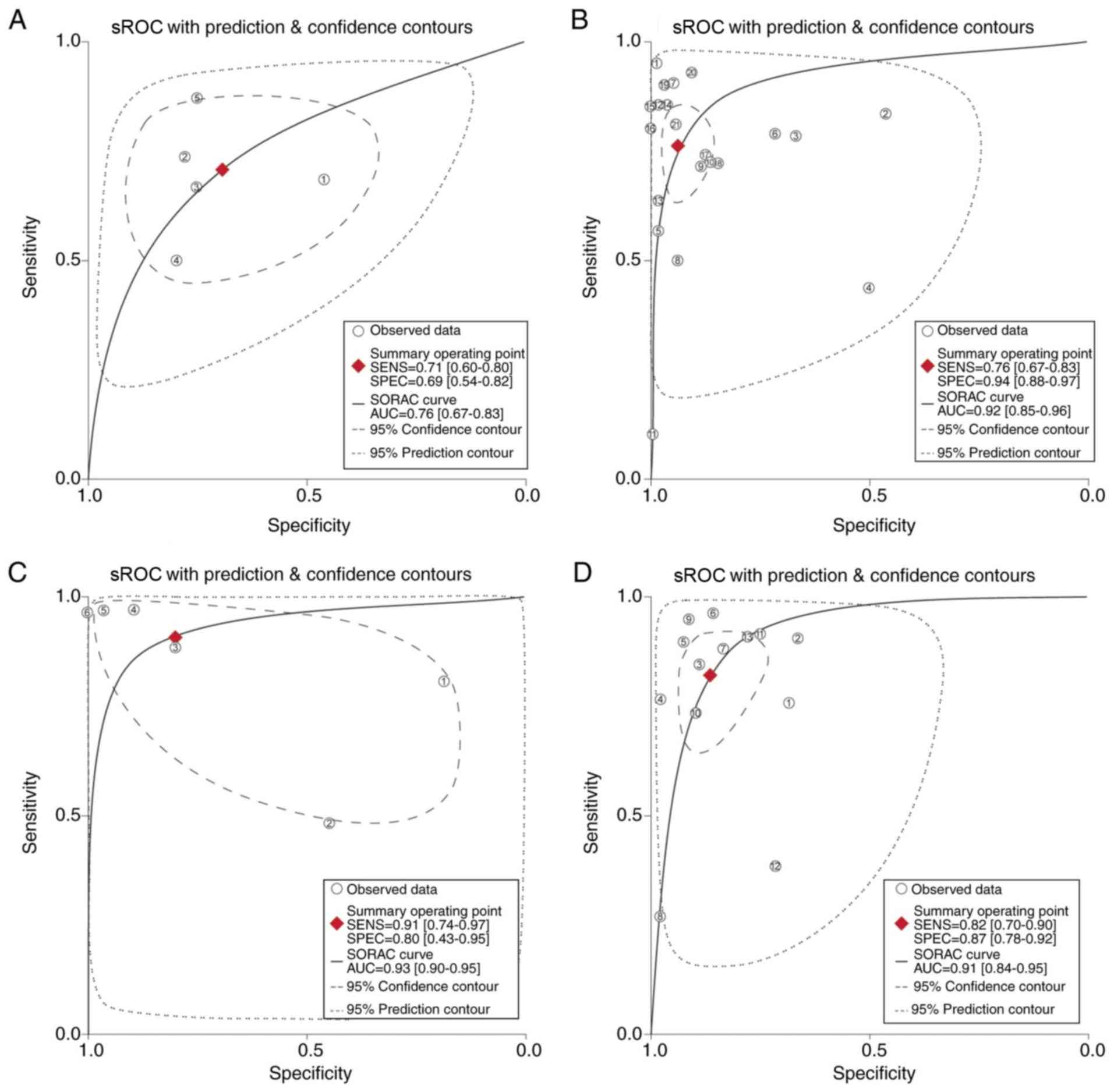
1.5-3.6) and LRN was 0.42 (95% CI, 0.29-0.61). Fig. 3A depicts the sROC curve for physical
examination. The AUC was 0.76 (95% CI, 0.66-0.83), which indicates
that physical examination has an intermediate level of diagnostic
value.
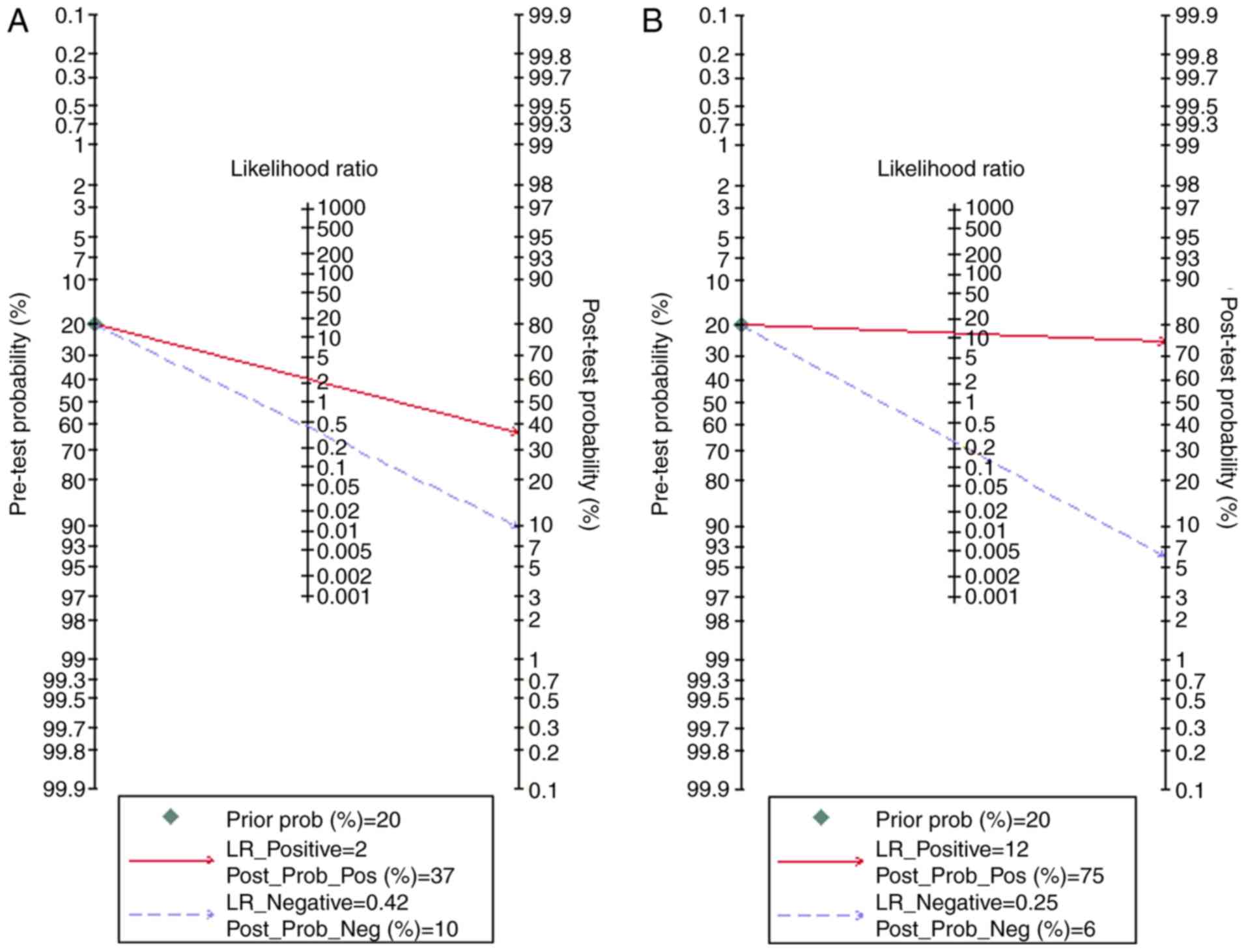
The clinical utility of physical examination for DIE
was average and Fagan's nomogram (Fig.
4A) indicated that post-test probability (positive, 37%;
negative, 10%) differed significantly from pre-test probability
(20%). There was substantial heterogeneity, with an I2
value of 75%, and χ2 test for heterogeneity was
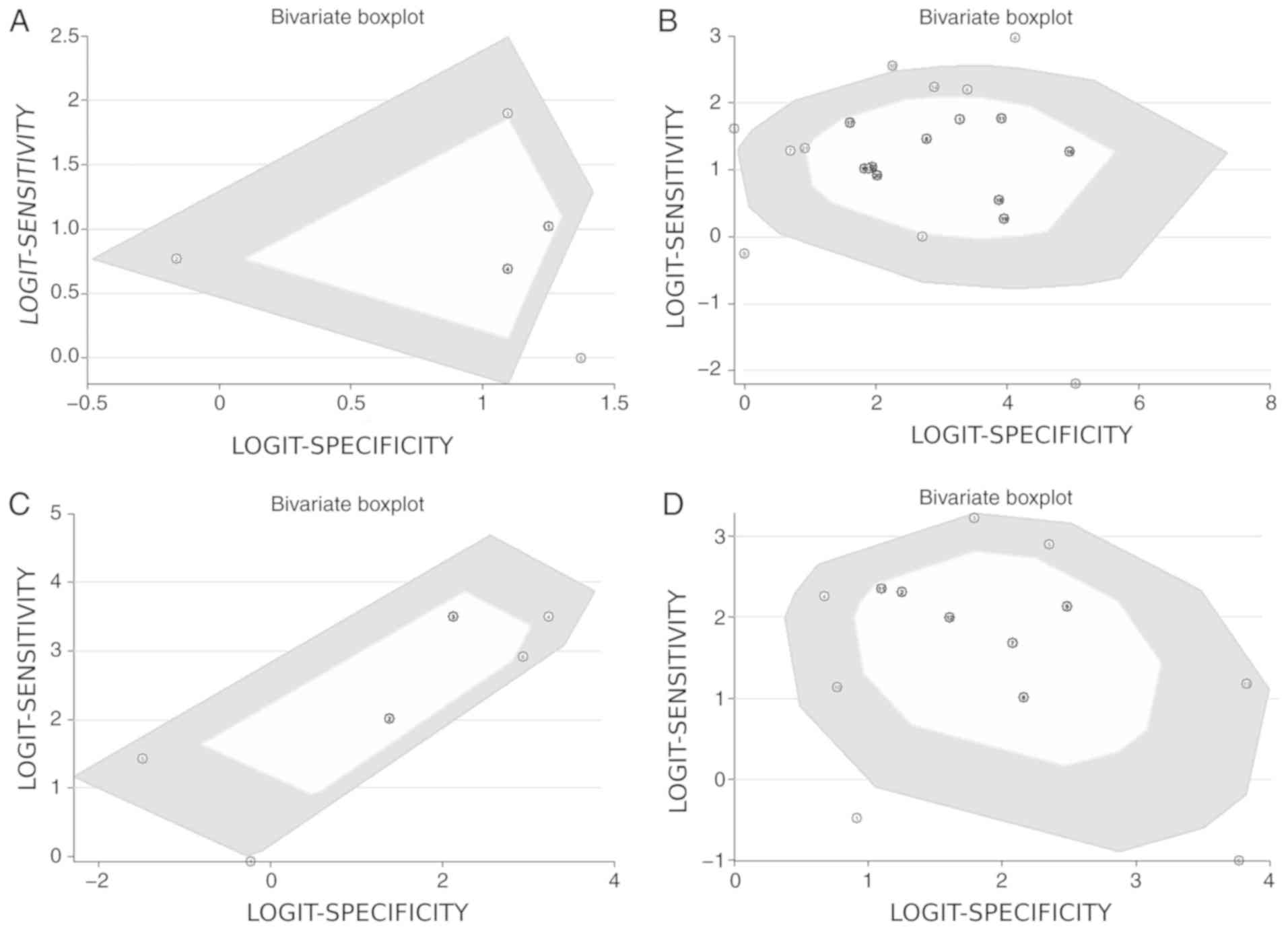
statistically significant (P=0.009). A bivariate box plot (Fig. 5A) indicated that there was a study
out of the circle, illustrating the heterogeneity between the
included studies. As there were <10 studies, publication bias
was not tested.
Diagnostic performance of TVUS
In total, 21 studies assessed the diagnostic
accuracy of TVUS. The pooled sensitivity and specificity of TVUS
for diagnosis of DIE were 76% (95% CI, 67-83%) and 94% (95% CI,
88-97%), respectively. The DOR was 47 (95% CI, 21-104) as displayed
in the Forest plot (Fig. 2B). LRP
was 12.0 (95% CI, 6.3-22.7) and LRN was 0.25 (95% CI, 0.18-0.36).
Fig. 3B depicts the sROC curve for
TVUS. The AUC was 0.92 (95% CI, 0.86-0.96), which indicates the
high diagnostic value of TVUS.
The clinical utility of TVUS for DIE was good and
Fagan's nomogram (Fig. 4B) revealed
that post-test probability (positive, 75%; negative, 6%) differed
significantly from pre-test probability (20%). There was
substantial heterogeneity, with an I2 value of 99%, and
χ2 test for heterogeneity was statistically significant
(P<0.001). A bivariate box plot (Fig.
5B) indicated 4 studies out of the circle illustrating
heterogeneity between the included studies. The Funnel plot
(Fig. S2) for publication bias was
symmetrical with non-significant Deek's test (P=0.60).
Diagnostic performance of TRUS
In total, six studies assessed the diagnostic
accuracy of TRUS. The pooled sensitivity and specificity of TRUS
for diagnosis of DIE were 91% (95% CI, 74-97%) and 80% (95% CI,
43-95%), respectively. The DOR was 39 (95% CI, 35-43) as shown in
the Forest plot (Fig. 2C). LRP was
4.5 (95% CI, 1.1-18.4) and LRN was 0.12 (95% CI, 0.03-0.45).
Fig. 3C depicts the sROC curve for
TRUS. The AUC was found to be 0.93 (95% CI, 0.86-0.97), which
indicates the high diagnostic value of TRUS.
The clinical utility of TRUS for DIE was good and
Fagan's nomogram (Fig. 4C) showed
that post-test probability (positive, 53%; negative, 3%) differed
significantly from pre-test probability (20%). There was
substantial heterogeneity, with an I2 value of 83%, and
the χ2 test for heterogeneity was statistically
significant (P=0.001). A bivariate box plot (Fig. 5C) indicated that there was a study
out of the circle, illustrating the heterogeneity between the
included studies. As there were <10 studies, publication bias
was not tested.
Diagnostic performance of MRI
In total, 13 studies assessed the diagnostic
accuracy of MRI. The pooled sensitivity and specificity of MRI for
diagnosis of DIE were 82% (95% CI, 70-90%) and 87% (95% CI,
78-92%), respectively. The DOR was 30 (95% CI, 14-62) as shown in
the Forest plot (Fig. 2D). LRP was
6.1 (95% CI, 3.7-9.9) and LRN was 0.21 (95% CI, 0.12-0.35).
Fig. 3D depicts the sROC curve for
MRI. The AUC was found to be 0.91 (95% CI, 0.80-0.97), which
indicates a high diagnostic value of MRI.
The clinical utility of MRI for DIE was good and
Fagan's nomogram (Fig. 4D) showed
that post-test probability (positive, 60%; negative, 5%) differed
significantly from pre-test probability (20%). There was
substantial heterogeneity, with an I2 value of 98%, and
χ2 test for heterogeneity was statistically significant
(P<0.001). A bivariate box plot (Fig.
5D) indicated 2 studies out of the circle, showing the
heterogeneity between the included studies. The Funnel plot
(Fig. S3) for publication bias was
symmetrical with non-significant Deek's test (P=0.41).
Discussion
Various imaging modalities are available for
diagnosis of DIE. Clinical history and physical examination of the
pelvis may suggest endometriosis; however, the heterogeneity of
clinical presentation, the prevalence of asymptomatic endometriosis
(2-50%), and a lack of association between disease severity and
presenting symptoms results in significant difficulty in obtaining
an accurate diagnosis based solely on patient history and physical
examination (4,5,8,9). Several advanced ultrasonographic
techniques have been described to identify endometriosis, such as
pelvic organ mobility, sliding sign, rectal water contrast,
tenderness-guided ultrasound and bowel preparation (25,33,43).
These techniques can significantly improve the diagnostic
performance of TVUS for endometriosis. Furthermore, the MRI ‘jelly
method’ appears to have improved diagnostic accuracy compared to
older MRI modalities (41). Although
these modalities cannot replace histopathology or biopsy as the
gold standard for diagnosis, a high diagnostic accuracy of such
non-invasive methods may reduce the diagnostic delay and
complications associated with invasive diagnostic methods. Hence,
it is important to precisely determine the diagnostic accuracy of
each of these modalities. In the present review of 30 studies with
4,565 participants, the results suggested that while physical
examination has intermediate diagnostic accuracy, TRUS, TVUS and
MRI have high diagnostic accuracy for DIE.
To the best of our knowledge, diagnostic accuracy of
physical examination for DIE has not been assessed in any previous
reviews. The present study results indicated the pooled sensitivity
and specificity of physical examination to be 71 and 69%,
respectively, with average diagnostic accuracy (AUC =0.76). TVUS
had a pooled sensitivity and specificity of 76 and 94% with high
diagnostic accuracy (AUC =0.92). These findings are in agreement
with earlier reviews on the diagnostic accuracy of TVUS, which also
indicated the high specificity and high diagnostic accuracy of this
technique (AUC >0.90) (11,46-48).
However, compared with the previous reviews, a greater number of
studies were included in the present analysis.
In the present analysis, TRUS had a pooled
sensitivity of 91% and a specificity of 80% with an AUC of 0.93,
which is similar to the diagnostic accuracy of TVUS. To the best of
our knowledge, no previous reviews have compared the accuracy of
TRUS and TVUS for the diagnosis of DIE. The present study revealed
MRI to have lower sensitivity (82%) and specificity (87%) for
diagnosis of DIE when compared with the previous reviews of Moura
et al (46) and Nisenblat
et al (11). Their studies
demonstrated ~90% sensitivity and specificity of MRI for diagnosis
of DIE. However, compared to these previous reviews, a greater
number of studies were included in the present analysis. The
results of the present study also suggested that TVUS may be used
to exclude the diagnosis of endometriosis with certainty, which was
not seen in the previous reviews.
The results of the present study should be
interpreted cautiously, considering the inter-study heterogeneity
and quality of the included studies. The high heterogeneity limits
any strong conclusions on the diagnostic accuracy of the
non-invasive modalities for DIE. There was no significant
publication bias among studies reporting diagnostic accuracy of
TVUS and MRI. However, publication bias for studies reporting TRUS
and physical examination could not be assessed due to the limited
number of studies included. The overall quality of studies was
good, as most of the studies had a low risk of bias with respect to
all the four domains measured using the QUADAS tool.
The present study had certain strengths. A
comprehensive review including 30 studies with 4,565 participants
to evaluate the accuracy of various imaging modalities and clinical
examination in diagnosing DIE was conducted. To the best of our
knowledge, this is the first review to provide pooled estimates for
four different diagnostic methods of DIE. The lack of any
significant publication bias adds credibility to the current
results. Nonetheless, the present study has certain limitations.
First, some studies included in the review had a high risk of bias
in certain domains, which may have influenced individual study
results. Secondly, significant heterogeneity was revealed between
the studies included in the review, which limited the
interpretation of the pooled outcomes.
Despite these limitations, the present study
provided valuable insights regarding the diagnostic accuracy of
various non-invasive techniques for DIE. Though all the imaging
modalities had good sensitivity and specificity, only TVUS was
close to fulfilling the SpPin i.e., specific positive in triage
test criteria (95% specificity). None of the modalities met the
SnNout criteria i.e. sensitive negative for 95% sensitivity of a
diagnostic test (11,49). This suggests that TVUS may be used to
diagnose DIE, but cannot confirm a woman to be disease-free based
on radiological evidence. These findings are in line with the
international guidelines for the diagnosis of DIE, which suggests
TVUS as a first-line imaging modality following history and
physical examination (50,51). However, TVUS does not replace
laparoscopic surgery and biopsy, which is still the gold standard
for diagnosing DIE.
To summarize, the present study demonstrated that
TRUS, TVUS and MRI have good diagnostic accuracy for DIE and have a
high sensitivity and specificity. The diagnostic accuracy was most
similar for TVUS, TRUS and MRI, with all the modalities having AUC
>0.9. Physical examination was also indicated to have reasonable
diagnostic accuracy. TVUS was the most specific imaging modality
while TRUS was the most sensitive modality for diagnosis of DIE.
However, these findings should be interpreted with caution owing to
the significant heterogeneity between the included studies. These
results suggest that these imaging modalities can be utilized as
efficient and time-saving screening tools for DIE.
Supplementary Material
Quality assessment among the included
studies using the quality assessment of diagnostic accuracy
studies-2 tool (n=30).
Funnel plot assessing publication bias
among studies reporting the diagnostic accuracy of transvaginal
ultrasound. ESS, Effective Sample Size.
Funnel plot assessing publication bias
among studies reporting the diagnostic accuracy of magnetic
resonance imaging. ESS, Effective Sample Size.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request. The relevant data is also available in the referenced
studies.
Authors' contributions
XZ conceived and designed the study. XZ, TH and WS
collected the data, performed the literature search and analyzed
the data. XZ was involved in the writing of the manuscript. All
authors have read and approved the final manuscript.
Ethical approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Irving JA and Clement PB: Diseases of the
Peritoneum. In: Blaustein's Pathology of the Female Genital Tract.
Kurman RJ, Ellenson LH and Ronnett BM (eds) Springer US, Boston,
MA, pp625-678, 2011.
|
|
2
|
Wheeler JM: Epidemiology of
endometriosis-associated infertility. J Reprod Med. 34:41–46.
1989.PubMed/NCBI
|
|
3
|
Foti PV, Farina R, Palmucci S, Vizzini
IAA, Libertini N, Coronella M, Spadola S, Caltabiano R, Iraci M,
Basile A, et al: Endometriosis: Clinical features, MR imaging
findings and pathologic correlation. Insights Imaging. 9:149–172.
2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Nisolle M and Donnez J: Peritoneal
endometriosis, ovarian endometriosis, and adenomyotic nodules of
the rectovaginal septum are three different entities. Fertil
Steril. 68:585–596. 1997.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Cornillie FJ, Oosterlynck D, Lauweryns JM
and Koninckx PR: Deeply infiltrating pelvic endometriosis:
Histology and clinical significance. Fertil Steril. 53:978–983.
1990.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Johnson NP and Hummelshoj L: World
Endometriosis Society Montpellier Consortium. Consensus on current
management of endometriosis. Hum Reprod. 28:1552–1568.
2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Rafique S and Decherney AH: Medical
management of endometriosis. Clin Obstet Gynecol. 60:485–496.
2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Guo SW: Recurrence of endometriosis and
its control. Hum Reprod Update. 15:441–461. 2009.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Duffy JMN, Arambage K, Correa FJS, Olive
D, Farquhar C, Garry R, Barlow DH and Jacobson TZ: Laparoscopic
surgery for endometriosis. Cochrane Database Syst Rev.
3(CD011031)2014.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Dmowski WP, Lesniewicz R, Rana N, Pepping
P and Noursalehi M: Changing trends in the diagnosis of
endometriosis: A comparative study of women with pelvic
endometriosis presenting with chronic pelvic pain or infertility.
Fertil Steril. 67:238–243. 1997.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Nisenblat V, Bossuyt PMM, Farquhar C,
Johnson N and Hull ML: Imaging modalities for the non-invasive
diagnosis of endometriosis. Cochrane Database Syst Rev.
2(CD009591)2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Whiting PF, Rutjes AWS, Westwood ME,
Mallett S, Deeks JJ, Reitsma JBR, Leeflang MMG, Sterne JAC and
Bossuyt PMM: QUADAS-2 Group. QUADAS-2: A revised tool for the
quality assessment of diagnostic accuracy studies. Ann Intern Med.
155:529–536. 2011.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Pan B, Zhang X and Liu S: Evaluation of
the ROC analysis in SPSS in the test/diagnosis. Strait J Prev Med.
9(5)2003.
|
|
14
|
Higgins JPT, Altman DG and Sterne JAC
(eds): Chapter 8: Assessing risk of bias in included studies. In:
Higgins JPT, Churchill R, Chandler J, Cumpston MS (eds), Cochrane
Handbook for Systematic Reviews of Interventions version 5.2.0
(updated June 2017), Cochrane, 2017.
|
|
15
|
Abrao MS, Gonçalves MO, Dias JA Jr,
Podgaec S, Chamie LP and Blasbalg R: Comparison between clinical
examination, transvaginal sonography and magnetic resonance imaging
for the diagnosis of deep endometriosis. Hum Reprod. 22:3092–3097.
2007.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Alborzi S, Rasekhi A, Shomali Z, Madadi G,
Alborzi M, Kazemi M and Hosseini Nohandani A: Diagnostic accuracy
of magnetic resonance imaging, transvaginal, and transrectal
ultrasonography in deep infiltrating endometriosis. Medicine
(Baltimore). 97(e9536)2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Bazot M, Lafont C, Rouzier R, Roseau G,
Thomassin-Naggara I and Daraï E: Diagnostic accuracy of physical
examination, transvaginal sonography, rectal endoscopic sonography,
and magnetic resonance imaging to diagnose deep infiltrating
endometriosis. Fertil Steril. 92:1825–1833. 2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Bergamini V, Ghezzi F, Scarperi S,
Raffaelli R, Cromi A and Franchi M: Preoperative assessment of
intestinal endometriosis: A comparison of transvaginal sonography
with water-contrast in the rectum, transrectal sonography, and
barium enema. Abdom Imaging. 35:732–736. 2010.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Chapron C, Vieira M, Chopin N, Balleyguier
C, Barakat H, Dumontier I, Roseau G, Fauconnier A, Foulot H and
Dousset B: Accuracy of rectal endoscopic ultrasonography and
magnetic resonance imaging in the diagnosis of rectal involvement
for patients presenting with deeply infiltrating endometriosis.
Ultrasound Obstet Gynecol. 24:175–179. 2004.PubMed/NCBI View
Article : Google Scholar
|
|
20
|
Chamié LP, Blasbalg R, Gonçalves MOC,
Carvalho FM, Abrão MS and de Oliveira IS: Accuracy of magnetic
resonance imaging for diagnosis and preoperative assessment of
deeply infiltrating endometriosis. Int J Gynaecol Obstet.
106:198–201. 2009.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Dessole S, Farina M, Rubattu G, Cosmi E,
Ambrosini G and Nardelli GB: Sonovaginography is a new technique
for assessing rectovaginal endometriosis. Fertil Steril.
79:1023–1027. 2003.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Eskenazi B, Warner M, Bonsignore L, Olive
D, Samuels S and Vercellini P: Validation study of nonsurgical
diagnosis of endometriosis. Fertil Steril. 76:929–935.
2001.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Fedele L, Bianchi S, Portuese A, Borruto F
and Dorta M: Transrectal ultrasonography in the assessment of
rectovaginal endometriosis. Obstet Gynecol. 91:444–448.
1998.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Grasso RF, Di Giacomo V, Sedati P, Sizzi
O, Florio G, Faiella E, Rossetti A, Vescovo RD and Zobel BB:
Diagnosis of deep infiltrating endometriosis: accuracy of magnetic
resonance imaging and transvaginal 3D ultrasonography. Abdom
Imaging. 35:716–725. 2010.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Guerriero S, Ajossa S, Gerada M, D'Aquila
M, Piras B and Melis GB: ‘Tenderness-guided’ transvaginal
ultrasonography: A new method for the detection of deep
endometriosis in patients with chronic pelvic pain. Fertil Steril.
88:1293–1297. 2007.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Guerriero S, Ajossa S, Gerada M, Virgilio
B, Angioni S and Melis GB: Diagnostic value of transvaginal
‘tenderness-guided’ ultrasonography for the prediction of location
of deep endometriosis. Hum Reprod. 23:2452–2457. 2008.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Guerriero S, Saba L, Ajossa S, Peddes C,
Angiolucci M, Perniciano M, Melis GB and Alcázar JL:
Three-dimensional ultrasonography in the diagnosis of deep
endometriosis. Hum Reprod. 29:1189–1198. 2014.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Guerriero S, Alcázar JL, Pascual MA,
Ajossa S, Perniciano M, Piras A, Mais V, Piras B, Schirru F,
Benedetto MG and Saba L: Deep infiltrating endometriosis:
Comparison between 2-dimensional ultrasonography (US),
3-dimensional US, and magnetic resonance imaging. J Ultrasound Med.
37:1511–1521. 2018.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Ha HK, Lim YT, Kim HS, Suh TS, Song HH and
Kim SJ: Diagnosis of pelvic endometriosis: fat-suppressed
T1-weighted vs conventional MR images. AJR Am J Roentgenol.
163:127–131. 1994.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Holland TK, Yazbek J, Cutner A, Saridogan
E, Hoo WL and Jurkovic D: Value of transvaginal ultrasound in
assessing severity of pelvic endometriosis. Ultrasound Obstet
Gynecol. 36:241–248. 2010.PubMed/NCBI View
Article : Google Scholar
|
|
31
|
Holland TK, Cutner A, Saridogan E,
Mavrelos D, Pateman K and Jurkovic D: Ultrasound mapping of pelvic
endometriosis: Does the location and number of lesions affect the
diagnostic accuracy? A multicentre diagnostic accuracy study. BMC
Womens Health. 13(43)2013.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Hudelist G, Ballard K, English J, Wright
J, Banerjee S, Mastoroudes H, Thomas A, Singer CF and Keckstein J:
Transvaginal sonography vs. clinical examination in the
preoperative diagnosis of deep infiltrating endometriosis.
Ultrasound Obstet Gynecol. 37:480–487. 2011.PubMed/NCBI View
Article : Google Scholar
|
|
33
|
Hudelist G, Fritzer N, Staettner S, Tammaa
A, Tinelli A, Sparic R and Keckstein J: Uterine sliding sign: A
simple sonographic predictor for presence of deep infiltrating
endometriosis of the rectum. Ultrasound Obstet Gynecol. 41:692–695.
2013.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Manganaro L, Vinci V, Bernardo S and
Storelli P: The role of 3.0T MRI in the assessment of deep
endometriosis located on the uterosacral ligaments. J Endo.
5:10–16. 2013.
|
|
35
|
Piessens S, Healey M, Maher P, Tsaltas J
and Rombauts L: Can anyone screen for deep infiltrating
endometriosis with transvaginal ultrasound? Aust N Z J Obstet
Gynaecol. 54:462–468. 2014.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Ribeiro HSAA, Ribeiro PA, Rossini L,
Rodrigues FC, Donadio N and Aoki T: Double-contrast barium enema
and transrectal endoscopic ultrasonography in the diagnosis of
intestinal deeply infiltrating endometriosis. J Minim Invasive
Gynecol. 15:315–320. 2008.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Saba L, Guerriero S, Sulis R, Pilloni M,
Ajossa S, Melis G and Mallarini G: Learning curve in the detection
of ovarian and deep endometriosis by using magnetic resonance:
Comparison with surgical results. Eur J Radiol. 79:237–244.
2011.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Saccardi C, Cosmi E, Borghero A, Tregnaghi
A, Dessole S and Litta P: Comparison between transvaginal
sonography, saline contrast sonovaginography and magnetic resonance
imaging in the diagnosis of posterior deep infiltrating
endometriosis. Ultrasound Obstet Gynecol. 40:464–469.
2012.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Savelli L, Manuzzi L, Coe M, Mabrouk M, Di
Donato N, Venturoli S and Seracchioli R: Comparison of transvaginal
sonography and double-contrast barium enema for diagnosing deep
infiltrating endometriosis of the posterior compartment. Ultrasound
Obstet Gynecol. 38:466–471. 2011.PubMed/NCBI View
Article : Google Scholar
|
|
40
|
Stratton P, Winkel C, Premkumar A, Chow C,
Wilson J, Hearns-Stokes R, Heo S, Merino M and Nieman LK:
Diagnostic accuracy of laparoscopy, magnetic resonance imaging, and
histopathologic examination for the detection of endometriosis.
Fertil Steril. 79:1078–1085. 2003.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Takeuchi H, Kuwatsuru R, Kitade M, Sakurai
A, Kikuchi I, Shimanuki H and Kinoshita K: A novel technique using
magnetic resonance imaging jelly for evaluation of rectovaginal
endometriosis. Fertil Steril. 83:442–447. 2005.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Ubaldi F, Wisanto A, Camus M, Tournaye H,
Clasen K and Devroey P: The role of transvaginal ultrasonography in
the detection of pelvic pathologies in the infertility workup. Hum
Reprod. 13:330–333. 1998.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Valenzano Menada M, Remorgida V, Abbamonte
LH, Nicoletti A, Ragni N and Ferrero S: Does transvaginal
ultrasonography combined with water-contrast in the rectum aid in
the diagnosis of rectovaginal endometriosis infiltrating the bowel?
Hum Reprod. 23:1069–1075. 2008.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Vimercati A, Achilarre MT, Scardapane A,
Lorusso F, Ceci O, Mangiatordi G, Angelelli G, Van Herendael B,
Selvaggi L and Bettocchi S: Accuracy of transvaginal sonography and
contrast-enhanced magnetic resonance-colonography for the
presurgical staging of deep infiltrating endometriosis. Ultrasound
Obstet Gynecol. 40:592–603. 2012.PubMed/NCBI View Article : Google Scholar
|
|
45
|
James FN and Umar S: 2016. The World
Bank's classification of countries by income (English). Policy
Research working paper; no. WPS 7528. Washington, DC: World Bank
Group. Available from: http://documents.worldbank.org/curated/en/408581467988942234/The-World-Banks-classification-of-countries-by-income.
|
|
46
|
Moura APC, Ribeiro HSAA, Bernardo WM,
Simões R, Torres US, D'Ippolito G, Bazot M and Ribeiro PA: Accuracy
of transvaginal sonography versus magnetic resonance imaging in the
diagnosis of rectosigmoid endometriosis: Systematic review and
meta-analysis. PLoS One. 14(e0214842)2019.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Guerriero S, Saba L, Pascual MA, Ajossa S,
Rodriguez I, Mais V and Alcazar JL: Transvaginal ultrasound vs
magnetic resonance imaging for diagnosing deep infiltrating
endometriosis: Systematic review and meta-analysis. Ultrasound
Obstet Gynecol. 51:586–595. 2018.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Guerriero S, Ajossa S, Orozco R,
Perniciano M, Jurado M, Melis GB and Alcazar JL: Accuracy of
transvaginal ultrasound for diagnosis of deep endometriosis in the
rectosigmoid: Systematic review and meta-analysis. Ultrasound
Obstet Gynecol. 47:281–289. 2016.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Šikic Z: Rules of thumb for positive and
negative test results. J Eval Clin Pract. 28(1111)2020.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Practice Bulletin no. 114: Management of
endometriosis. Obstet Gynecol. 116:223–236. 2010.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Dunselman GAJ, Vermeulen N, Becker C,
Calhaz-Jorge C, D'Hooghe T, Bie BD, Heikinheimo O, Horne AW, Kiesel
L, Nap A, et al: ESHRE guideline: Management of women with
endometriosis. Hum Reprod. 29:400–412. 2014.PubMed/NCBI View Article : Google Scholar
|