Introduction
Gestational diabetes mellitus (GDM) refers to any
degree of blood glucose intolerance that occurs or being discovered
for the first time during pregnancy, regardless of whether this
condition persists after delivery or whether glucose-control
treatment is needed during pregnancy (1). Gestational diabetes does not include
diabetes occurred before pregnancy. According to statistics
(2), the incidence of GDM is 3-6%,
and it usually occurs after 20-24 weeks of pregnancy. It is a
common high-risk metabolic complication. Gestational diabetes
increases the risk of adverse pregnancy outcomes (3). Studies have found that GDM patients and
their infants also have a significantly increased risk of
developing chronic diseases such as diabetes, metabolic syndrome,
and cardiovascular disease in the future (4,5). In
recent years, with the delay of child-bearing age and changes in
dietary habits and lifestyles, the incidence of GDM has increased
significantly (6). GDM may cause
adverse pregnancy outcomes including miscarriage, premature
delivery, intrauterine distress, fetal malformation, intrauterine
death, intrauterine infection, macrosomia and hypertension during
pregnancy, preeclampsia and polyhydramnios (7). Gestational diabetes may increase the
risk of type 2 diabetes in the mother. Gestational diabetes
patients would meet a peak period to develop diabetes five years
after delivery. The vast majority of gestational diabetes patients
can resume normal glucose metabolism after delivery, but there are
still 40-50% of them who develop type 2 diabetes 5-10 years after
delivery, and long-term treatment is required (8). In view of the short-term and long-term
adverse effects of gestational diabetes on mothers and children, it
is of great significance to analyze the risk factors of GDM, give
early screening and prevention for pregnant women with high-risk
factors, provide intervention guidance to actively control blood
sugar in the normal range in order to reduce the incidence of GDM
and adverse pregnancy outcomes, so as to prevent or delay the
presence of long-term adverse prognosis of mother and child. This
study analyzed the risk factors of 378 GDM patients admitted to the
hospital from January 2017 to December 2018, analyzed the impact on
pregnancy outcomes, and proposed corresponding interventions in
order to provide a basis for comprehensive prevention and treatment
of GDM.
Subjects and methods
Clinical data
From January 2017 to December 2018, 378 GDM patients
awaiting delivery in Weifang People's Hospital (Shandong, China)
were selected as the research subjects. At the same time, 200
pregnant women with normal blood glucose (NGT) during the same
period were randomly selected as controls. Inclusion criteria:
Patients who meet the GDM diagnostic criteria: Fasting blood
glucose (FBG) ≥5.1 mmol/l, 1 h blood glucose ≥10.0 mmol/l, 2 h
blood glucose ≥8.5 mmol/l. GDM was diagnosed when blood glucose
exceeds the diagnostic criteria at any time point; patients who can
independently participate in the study; patients with no history of
mental illness; patients with complete pregnancy examination data
and postpartum follow-up data. Exclusion criteria: Patients with
diabetes combined with pregnancy; patients with severe mental
disorders; patients combined with severe heart, liver, kidney and
autoimmune diseases before pregnancy.
This study was approved by the Ethics Committee of
Weifang People's Hospital (sdlunl:20170116), and all pregnant women
signed informed consent and were included in the study on a
voluntary basis.
Methods Laboratory indicators
According to the time requirements, 3 ml of elbow
vein blood was drawn from each research subject [self-coagulation
was used for blood glucose and blood lipid, EDTA-K2 anticoagulation
was used for glycated hemoglobin (HbA1c)]. Centrifugation was
performed at 2,264 x g for 20 min to separate the upper serum (or
plasma). Lipemia or hemolysis were excluded in all specimen. It is
completed within 2 h from specimen collection to testing.
Blood glucose and blood lipids were measured using
Hitachi 7170S automatic biochemical analyzer (Hitachi, Ltd.);
fasting insulin was detected by electrochemical immunoluminescence
(Roche Diagnostics); HbA1c was analyzed by G8 HbA1c analyzer (Japan
Tosoh Corporation). Oral glucose tolerance test (OGTT): All
pregnant women underwent an OGTT at 24-28 weeks of gestation.
Examine were fasted for 8-12 h before the test, then venous blood
was taken to measure FBG at around 8 am. Patients were asked to
drink 300 ml warm water with 75 g anhydrous glucose powder within 5
min, and blood was taken 1 and 2 h later to measure blood glucose.
Blood lipids and HbA1c were tested when FBG was tested.
A self-designed questionnaire was used to
investigate the general data of pregnant women and clinical
laboratory data, including age, pre-pregnancy body mass index
(BMI), weight gain during pregnancy, height, family history of
diabetes, women's menstrual period, pregnancy times, history of
polycystic ovary syndrome (PCOS), history of adverse pregnancy and
delivery, history of gestational diabetes, FBG, 1 h postprandial
blood glucose (1hPBG), 2 h postprandial blood glucose (2hPBG),
HbA1c, fasting insulin level (FINS), triglyceride (TG), cholesterol
(TC), high-density lipoprotein cholesterol (HDL-C), low-density
lipoprotein cholesterol (LDL-C), and pregnancy outcomes. The
questionnaires are distributed and collected by trained
investigators. The questionnaire's recovery rate and efficiency are
both 100%. Pre-pregnancy overweight is defined as pre-pregnancy BMI
≥25 kg/m2, for giant baby is defined as body mass ≥4
kg.
Intervention measures
Promote health education: Promote community
pre-pregnancy health education and publicity, pre-pregnancy
counseling and training for women of appropriate age; spread
GDM-related knowledge, including the occurrence, progression and
harmfulness of GDM; enhance pregnant women's self-care awareness;
improve community medical services, including general surveys of
blood sugar and weight; improve the health files of pregnant women
in the community, and do regular follow-up during pregnancy. Diet
intervention: Diet intervention is the primary method of weight
control, vigorously advocate a healthy lifestyle, guide rational
diet before and during pregnancy to actively control weight. GDM
patients are instructed to develop a personalized diet plan. The
diet includes carbohydrates 40%, protein 20%, fat 40%, with more
whole grains, replacing fruits with vegetables like cucumbers and
tomatoes. Foods with a high sugar production index were excluded in
the balanced diet. Exercise intervention: Pregnant women were
guided to do appropriate physical exercise according to their own
situation. Exercise can reduce body weight, reduce insulin
resistance, and reasonable exercise can effectively control weight
gain during pregnancy. Diet intervention and exercise intervention
were implemented in the GDM group, and the levels of blood glucose
2 h after meal (2hPBG) and HbA1c before and after intervention were
compared.
Statistical analysis
Data were statistically processed using SPSS 25.0
(IBM Corp). Measurement data were expressed as mean ± standard
deviation (SD), Student's t-test was used for comparison between
groups; enumeration data were expressed by percentage, and
χ2 test was used for comparison between groups. GDM risk
factors were analyzed using logistic regression. Univariate
analysis was used for general data and clinical data; multivariate
unconditional logistic regression analysis was performed with
statistical parameters (P<0.05) as independent variables and
with GDM as dependent variables. P<0.05 was considered
statistically significant.
Results
Univariate analysis of GDM risk
factors
A univariate analysis of the two groups of data
showed that there were differences between the two groups in age,
family history of diabetes, BMI before pregnancy, GDM history, PCOS
history, FBG level FBG, 1hPBG, 2hPBG, HbA1c, FINS, TG, and HDL-C
(P<0.05) (Table I).
 | Table IUnivariate analysis of risk factors
for GDM [n (%), mean ±SD]. |
Table I
Univariate analysis of risk factors
for GDM [n (%), mean ±SD].
| Variables | GDM (n=378) | NGT (n=200) | χ2/t | P-value |
|---|
| Age n (%), ≥35
years | 124 (32.80) | 32 (16.00) |
χ2=19.378 | <0.001 |
| BMI before pregnancy
(kg/m2) | 28.16±1.38 | 22.78±1.04 | t=6.416 | 0.004 |
| Weight gain during
pregnancy (kg) | 16.82±1.46 | 14.51±1.41 | t=1.247 | 0.259 |
| Height (cm) | 163.57±2.67 | 164.98±2.41 | t=0.174 | 0.868 |
| Family history of
diabetes n (%) | 132 (34.92) | 22 (13.00) |
χ2=31.641 | <0.001 |
| Menstrual period
(d) | 3.62±0.97 | 3.84±0.88 | t=0.235 | 0.786 |
| Gravidity | 2.11±0.63 | 1.91±0.52 | t=0.224 | 0.831 |
| PCOS history n
(%) | 113 (29.89) | 40 (20.00) |
χ2=6.579 | 0.010 |
| History of adverse
pregnancy n (%) | 60 (15.87) | 22 (11.00) |
χ2=2.551 | 0.110 |
| GDM history n
(%) | 162 (42.86) | 10 (5.00) |
χ2=87.679 | <0.001 |
| FBG (mmol/l) | 6.89±1.20 | 4.52±0.48 | t=3.003 | 0.024 |
| 1hPBG (mmol/l) | 12.32±1.65 | 8.29±0.92 | t=3.274 | 0.017 |
| 2hPBG (mmol/l) | 9.33±1.42 | 5.01±0.86 | t=7.851 | <0.001 |
| HbA1c (%) | 8.98±0.42 | 5.56±0.22 | t=7.232 | <0.001 |
| FINS (mmol/l) | 18.43±3.78 | 11.26±1.82 | t=2.697 | 0.035 |
| TG (mmol/l) | 3.08±0.79 | 1.92±0.63 | t=2.612 | 0.042 |
| TC (mmol/l) | 4.97±1.02 | 3.89±0.98 | t=1.015 | 0.349 |
| HDL-C (mmol/l) | 0.92±0.12 | 1.53±0.15 | t=2.967 | 0.028 |
| LDL (mmol/l) | 3.38±0.82 | 3.36±0.77 | t=0.765 | 0.432 |
Multivariate non-conditional logistic
regression analysis of risk factors for GDM
Multivariate non-conditional logistic regression
analysis was performed using statistically significant (P<0.05)
parameter in the single factor analysis as the independent variable
and the presence or absence of GDM as the dependent variable. The
results showed that age, BMI, history of GDM before pregnancy,
family history of diabetes, 2hPBG, and HbA1c were independent risk
factors for GDM (Table II).
| Table IIMultivariate non-conditional logistic
regression analysis of risk factors for GDM. |
Table II
Multivariate non-conditional logistic
regression analysis of risk factors for GDM.
| Items | B | S.E | Wald | P-value | OR | 95% CI |
|---|
| Age ≥35 years | 0.637 | 0.179 | 12.078 | <0.001 | 1.891 | 1.332-2.686 |
| BMI before
pregnancy | 1.117 | 0.307 | 13.261 | <0.001 | 3.045 | 1.657-5.571 |
| Family history of
diabetes | 0.738 | 0.178 | 16.927 | <0.001 | 2.093 | 1.472-2.978 |
| PCOS history | 0.363 | 0.655 | 3.718 | 0.054 | 3.536 | 0.783-6.928 |
| GDM history | 1.005 | 0.728 | 14.002 | <0.001 | 5.326 | 2.315-6.489 |
| FBG | 0.491 | 0.405 | 1.474 | 0.225 | 1.634 | 0.739-3.613 |
| 1hPBG | 0.553 | 0.574 | 0.861 | 0.354 | 0.587 | 0.190-1.809 |
| 2hPBG | 0.452 | 0.188 | 5.801 | 0.016 | 1.572 | 1.008-2.271 |
| HbA1c | 0.678 | 0.312 | 12.309 | <0.001 | 2.989 | 1.621-5.509 |
| FINS | 0.179 | 0.153 | 1.378 | 0.241 | 1.196 | 0.887-1.614 |
| TG | 0.238 | 0.296 | 0.649 | 0.420 | 1.259 | 0.711-2.266 |
| HDL | 0.104 | 0.329 | 0.101 | 0.751 | 1.110 | 0.583-2.115 |
Comparison of pregnancy outcomes
between GDM and control group
GDM has adverse effects on both pregnant and
perinatal infants. This study showed that the incidence of maternal
dystocia, cesarean section, abnormal amniotic fluid, premature
rupture of membranes, and pathological pregnancy in the GDM group
were significantly higher than those in the normal control group,
and the differences were statistically significant (P<0.01); the
probability of fetal distress, macrosomia, small for date children
and premature children in the perinatal infants in the GDM group
were significantly higher than those in the normal control group,
and the difference was statistically significant (P<0.01)
(Table III).
| Table IIIComparison of adverse pregnancy
outcomes between the GDM and the control group, n (%). |
Table III
Comparison of adverse pregnancy
outcomes between the GDM and the control group, n (%).
| Groups | Dystocia and
cesarean section | Abnormal amniotic
fluid | Premature rupture
of membranes | Pathological
pregnancy | Fetal distress | Macrosomia | Small for date
children | Preterm
children |
|---|
| GDM (n=378) | 170
(44.97)a | 51
(13.49)a | 65
(17.20)a | 105
(27.78)a | 55
(14.55)a | 78
(20.63)a | 34
(8.99)a | 64
(16.93)a |
| Control
(n=200) | 58 (29.00) | 9 (4.50) | 11 (5.50) | 12 (6.00) | 6 (3.00) | 8 (4.00) | 5 (2.50) | 8 (4.00) |
| χ2 | 13.972 | 11.368 | 15.667 | 38.423 | 18.485 | 28.578 | 8.763 | 20.056 |
| P-value | <0.001 | 0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.003 | <0.001 |
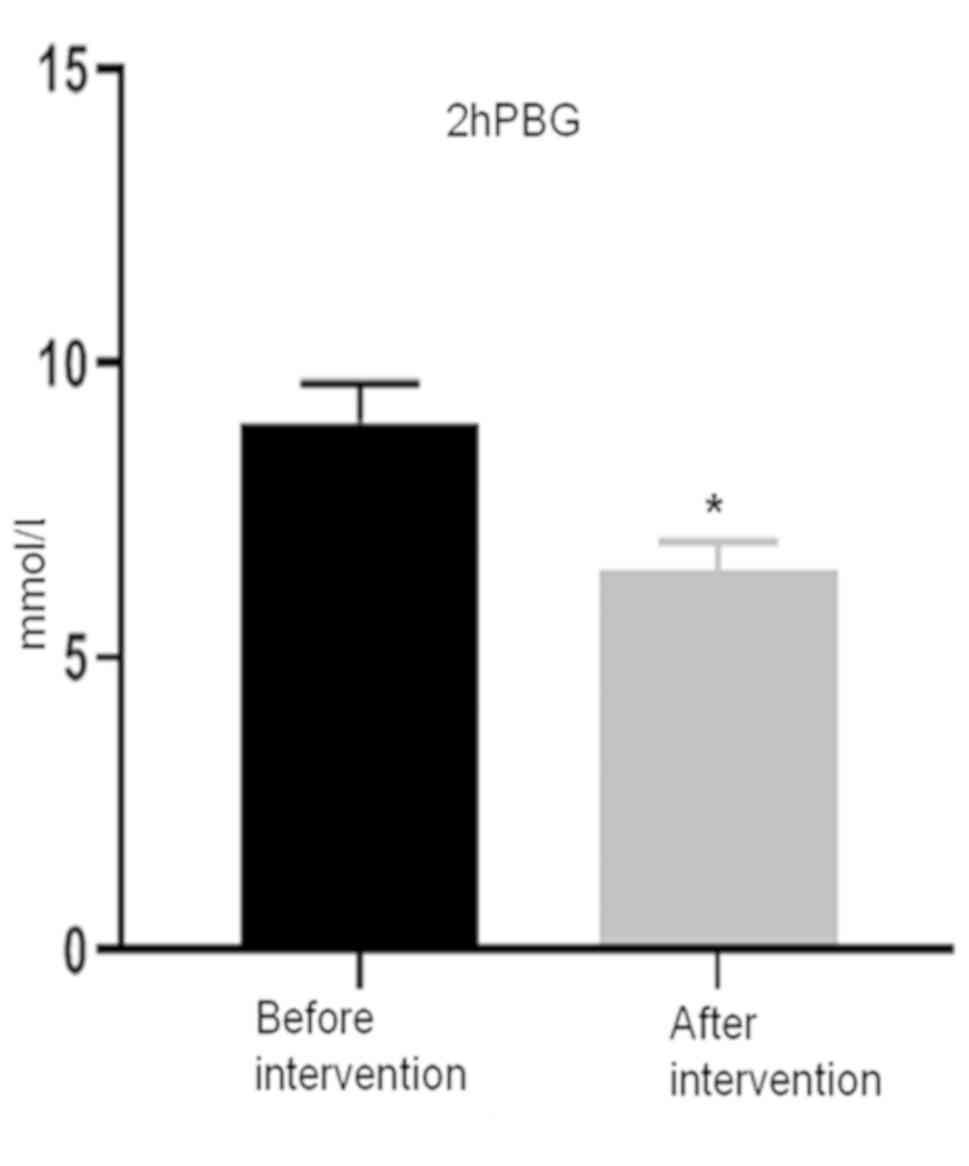
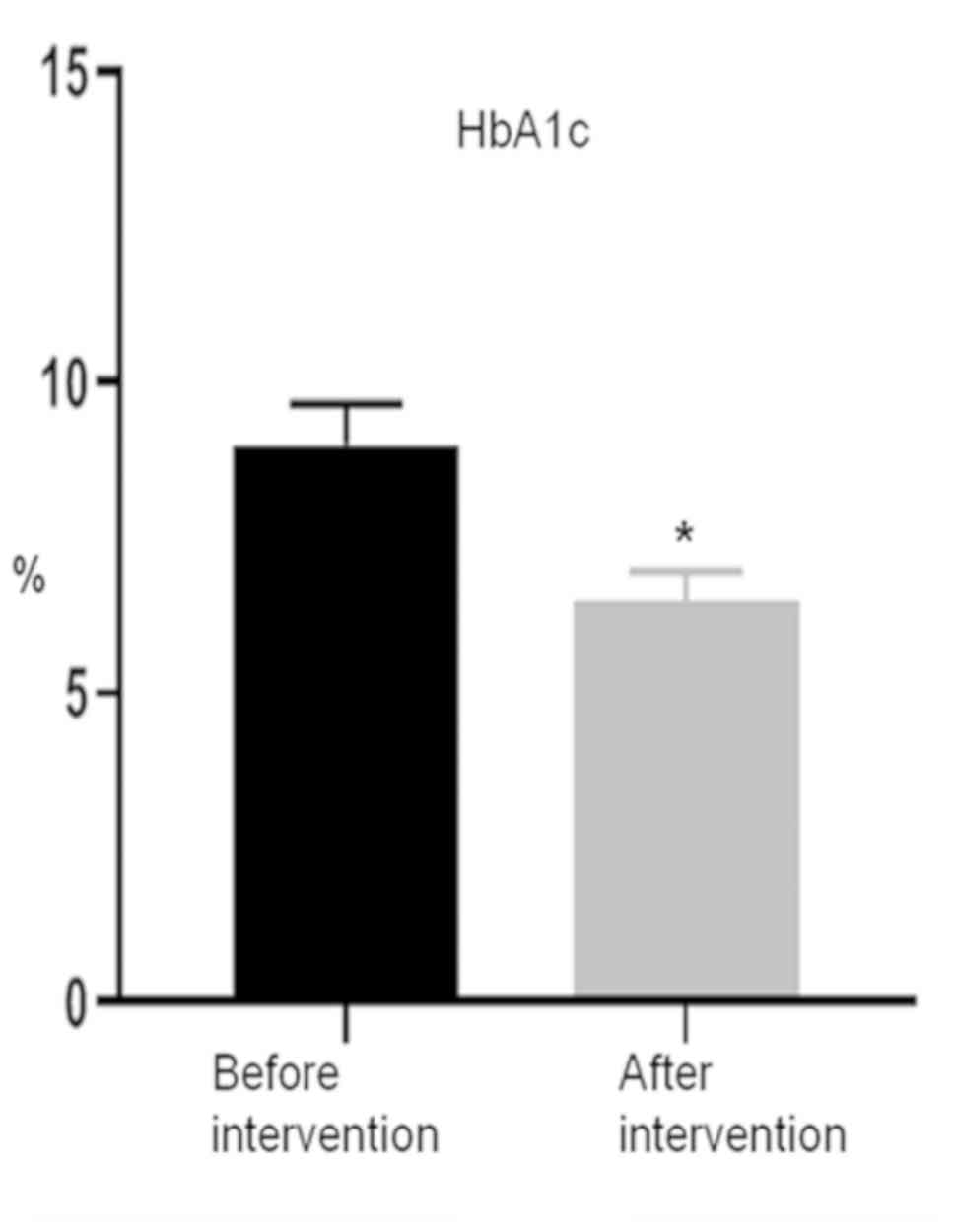
Comparison of 2hPBG and HbA1c levels
in the GDM group before and after the intervention
The 2hPBG and HbA1c levels in the GDM group after
intervention were significantly lower than those before
intervention (t=2.842, 2.986, P=0.029, 0.020). The comparison of
2hPBG post-intervention and pre-intervention is shown in Fig. 1. The comparison of HbA1c post- and
pre-intervention is shown in Fig.
2.
Discussion
GDM is a hyperglycemia in pregnant women. In recent
years, the incidence of GDM has been increasing year by year. The
early clinical symptoms of GDM are not typical. Without being
promptly screened and early intervention, it will affect not only
the health of the mother, but also the health of the infant for a
long period of time. Exploring the risk factors of GDM, analyzing
the adverse effects on pregnancy outcomes, and proposing
corresponding preventive measures are of great significance for
reducing the presence and progression of GDM and ensuring the
safety of mothers and infants.
Previous studies have shown (9,10) that
pre-pregnancy obesity and advanced age are closely related to GDM.
The higher the BMI before pregnancy and the older the age of
pregnancy, the higher the incidence of GDM. As pregnancy
progresses, hormones such as prolactin (HPL) and prolactin (PRL)
secreted by the placenta gradually increase, resulting in insulin
resistance; in addition, obesity is prone to insulin resistance,
and insulin resistance produces and exacerbates obesity, so
overweight and obese pregnant women are more likely to develop GDM.
Riskin-Mashiah et al (11)
conducted a statistical analysis of BMI in early pregnancy and
found that for every 3.5 kg/m2 increase in BMI in early
pregnancy, the risk of GDM increased by 1.5 times. Kim et al
(12) analyzed the association
between BMI and GDM and found that the incidence of GDM in normal
body weight pregnant women, overweight pregnant women, obese
pregnant women, and severely obese pregnant women increased 2.3,
4.8, 5.5, and 11.5%, respectively, suggesting the association
between BMI and GDM before pregnancy. Ogonowski et al
(13) found through case-control
studies that the risk of GDM increases with the increase in BMI
before pregnancy. In addition, advanced pregnancy is currently
recognized as one of the major risk factors for gestational
diabetes. Lao et al (14)
retrospectively analyzed 15,827 pregnant women from 1998 to 2001 in
Hong Kong, China, and concluded that the incidence risk of GDM
significantly increases with the age of pregnant women. The results
of this study showed that pregnant women aged ≥35 years and being
overweight before pregnancy are independent risk factors for the
progression of GDM, which is consistent with the above-mentioned
report, and their OR values for GDM were 1.891 and 3.045,
respectively.
Family history of diabetes plays a very important
role in the presence of gestational diabetes. Genetics may be
related to susceptibility genes and intrauterine high glucose
environment. The incidence of type 2 diabetes in maternal lines of
women with gestational diabetes is high. It can be speculated that
their mothers have also suffered from gestational diabetes, and
their children were in intrauterine high glucose environment when
they were embryo. In addition, fetal pancreatic islet β cells and
adipocytes are stimulated by hyperglycemia and abnormally
proliferate, so it is prone to produce large infant. Those infants
are prone to obesity and insulin resistance in adulthood, and prone
to GDM after pregnancy (15).
Retnakaran et al (16) has
shown that 38.1% of GDM have a family history of diabetes, which is
a 2.9-fold increase in the risk of GDM compared with those without
a family history of diabetes. According to a previous study
(17), the risk of GDM in people
with a previous history of GDM during multiple pregnancies is 13.2
times that of those without a history of GDM, and the risk of GDM
in those who have twice previous histories of GDM is 25.9 times
that of those without a history of GDM. In addition, the risk of
GDM is closely related to the postprandial hyperglycemia and high
HbAIc of pregnant women (18). The
2hPBG does not meet the standard, indicating impaired glucose
tolerance. HbAIc reflects the level of blood glucose control in the
past 2-3 months, and can better reflect the situation of blood
glucose control than FBG. There might be insulin resistance in the
indirect reaction of long-term OGTT 2 h blood glucose and HbAIc
control failure. The results of this study showed that family
history of diabetes, GDM, 2hPBG, and HbA1c were independent risk
factors for gestational diabetes. The OR values of multi-factor
unconditional logistic regression analysis were 2.903, 5.326,
1.527, and 2.989, respectively, indicating that family history of
diabetes, GDM, 2hPBG, HbA1c are risk factors for GDM.
The short-term adverse effects of GDM on pregnant
women may mainly cause pregnancy-induced hypertension,
pre-eclampsia, postpartum hemorrhage, amniotic fluid pollution,
premature rupture of membranes; meanwhile, there would be an
increase in dystocia, birth injury and cesarean section (19). The long-term impact is mainly a
significant increase in the risk of post-natal diabetes. The
short-term impact on the fetus is that the continuous high glucose
environment in the uterus stimulates the pancreatic β cells of the
fetus to secrete insulin, which brings the fetus persistent
hyperinsulinemia. Hyperinsulin promotes the increase of fat and
protein synthesis, causing excessive growth of the fetus (20), which in turn leads to increased risk
of brachial plexus nerve injury and shoulder dystocia (21). At the same time, the incidence of
full-term infants, gestational age and premature infants increased,
and the perinatal fetal mortality rate increased; the long-term
impact is mainly due to the increased risk of obesity and diabetes
in adults (22). Women with a
history of childbirth have a 2.25 times incidence of GDM when they
become pregnant again (23). Obesity
can reduce the sensitivity of insulin target organs to insulin and
produce insulin resistance. Therefore, women with larger BMI have a
higher risk of GDM than healthy women, and the risk of adverse
pregnancy outcomes also increases (24,25). The
results of this study showed that the incidence of maternal
dystocia, cesarean section, abnormal amniotic fluid, premature
rupture of membranes, and pathological pregnancy in the GDM group
were significantly higher than those in the control group. The
probability of fetal distress, huge infants, full-term infants and
premature infants in perinatal infants is significantly higher than
that in the normal control group, the difference is statistically
significant (all P<0.01).
Intervention countermeasures: With the increase of
gestational age in pregnant women, the hormones that antagonize
insulin in the body continue to increase, and the sensitivity to
insulin decreases. In order to maintain normal glucose metabolism
levels, more insulin secretion is required, and the characteristic
of blood sugar metabolism is that blood sugar is more likely to
rise after a meal or after a sugar load stimulation. Therefore, it
is more difficult to meet the standard for blood glucose after
meals. At the same time, long-term hyperglycemia, HbA1c also
increases, and the incidence of adverse pregnancy outcomes
increases (26), so it is important
to actively control postprandial blood glucose. The results of the
present study show that after diet intervention and exercise
intervention, the blood glucose and HbA1c levels of pregnant women
2 hours after meal were significantly lower than before
intervention, which is consistent with literature reports (27). It is necessary for pregnant women who
do not meet the blood glucose standards for diet and exercise
intervention to receive adjuvant insulin therapy (28). Planned marriage and childbirth age
could avoid pregnancy GDM. The government, society and families
should encourage early childbirth to minimize the risk of GDM.
Family history of diabetes and previous GDM history are
non-interventional factors. Patients with such history should take
blood sugar screening as soon as possible. Even if the OGTT
screening is negative in the early pregnancy, it cannot completely
rule out the risk of GDM in the later stage of pregnancy. It is
appropriate to select several important GDM high-risk factors for a
comprehensive evaluation of pregnant women to assess whether there
is a risk of GDM, and then decide whether to conduct repeated OGTT
screening of pregnant women, to reduce missed detection rates of
GDM (29). The OGTT screening for
pregnant women with 24-28 weeks of pregnancy should be paid more
attention to, because during the 24-28 weeks of pregnancy, the
levels of hormones (HPL, PRL) secreted by placenta are
significantly increased, which can produce insulin resistance
against insulin and increase blood sugar. At this time, screening
OGTT is conducive to the detection of GDM (21). The early symptoms of GDM are not
obvious, and the principle of prevention and treatment is early
screening, early diagnosis, and early treatment to improve the
prognosis of mothers and infants and avoid the presence of adverse
pregnancy outcomes.
In conclusion, the present study comprehensively
analyzed the risk factors of gestational diabetes, which is more
comprehensive than previous studies, and proposed corresponding
intervention countermeasures. In the study, the impact of BMI or
age on GDM was reported, and the effects of the family history of
diabetes, GDM history, 2hPBG and HbA1c on GDM were discussed.
In the present study, the risk factors of GDM were
analyzed. Early screening, early prevention and early intervention
can improve the prognosis and outcome of mother and infant,
however, long-term follow-up of postpartum mothers and infants is
required.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Author's contributions
WZ conceived the study and drafted the manuscript.
JL collected and analyzed the clinical data. QL and WC were
responsible for the laboratory indicators. SZ and XS were
responsible for the intervention measures. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
the Weifang People's hospital (Shandong, China) (sdlunl:20170116),
and all pregnant women signed informed consent and were included in
the study on a voluntary basis.
Patient consent for publication
Not applicable
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
American Diabetes Association. Diagnosis
and classification of diabetes mellitus. Diabetes Care. 32 (Suppl
1):S62–S67. 2009.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Halbritter S, Fedrigo M, Höllriegl V,
Szymczak W, Maier JM, Ziegler AG and Hummel M: Human breath gas
analysis in the screening of gestational diabetes mellitus.
Diabetes Technol Ther. 14:917–925. 2012.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Crowther CA, Hiller JE, Moss JR, McPhee
AJ, Jeffries WS and Robinson JS: Australian Carbohydrate
Intolerance Study in Pregnant Women (ACHOIS) Trial Group. Effect of
treatment of gestational diabetes mellitus on pregnancy outcomes. N
Engl J Med. 352:2477–2486. 2005.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Nilofer AR, Raju VS, Dakshayini BR and
Zaki SA: Screening in high-risk group of gestational diabetes
mellitus with its maternal and fetal outcomes. Indian J Endocrinol
Metab. 16 (Suppl 1):S74–S78. 2012.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Fall CH: Evidence for the intra-uterine
programming of adiposity in later life. Ann Hum Biol. 38:410–428.
2011.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ostadrahimi A, Mohammad-Alizadeh S,
Mirgafourvand M, Yaghoubi S, Shahrisa E and Farshbaf-Khalili A:
Effects of fish oil supplementation on gestational diabetes
mellitus (GDM): A systematic review. Iran Red Crescent Med J.
18(e24690)2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Buchanan TA, Xiang AH and Page KA:
Gestational diabetes mellitus: Risks and management during and
after pregnancy. Nat Rev Endocrinol. 8:639–649. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Moses RG: Gestational diabetes mellitus:
Implications of an increased frequency with IADPSG criteria.
Diabetes Care. 35:461–462. 2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Sorbye LM, Skjaerven R, Klungsoyr K and
Morken NH: Gestational diabetes mellitus and interpregnancy weight
change: A population-based cohort study. PLoS Med.
14(e1002367)2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Torloni MR, Betrán AP, Horta BL, Nakamura
MU, Atallah AN, Moron AF and Valente O: Prepregnancy BMI and the
risk of gestational diabetes: A systematic review of the literature
with meta-analysis. Obes Rev. 10:194–203. 2009.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Riskin-Mashiah S, Damti A, Younes G and
Auslender R: First trimester fasting hyperglycemia as a predictor
for the development of gestational diabetes mellitus. Eur J Obstet
Gynecol Reprod Biol. 152:163–167. 2010.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Kim SY, England L, Wilson HG, Bish C,
Satten GA and Dietz P: Percentage of gestational diabetes mellitus
attributable to overweight and obesity. Am J Public Health.
100:1047–1052. 2010.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ogonowski J, Miazgowski T, Kuczyńska M,
Krzyzanowska-Swiniarska B and Celewicz Z: Pregravid body mass index
as a predictor of gestational diabetes mellitus. Diabet Med.
26:334–338. 2009.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Lao TT, Ho LF, Chan BC and Leung WC:
Maternal age and prevalence of gestational diabetes mellitus.
Diabetes Care. 29:948–949. 2006.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Sewell MF, Presley LH, Holland SH and
Catalano PM: Genetic causes of maturity onset diabetes of the young
may be less prevalent in American pregnant women recently diagnosed
with diabetes mellitus than in previously studied European
populations. J Matern Fetal Neonatal Med. 28:1113–1115.
2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Retnakaran R, Connelly PW, Sermer M,
Zinman B and Hanley AJG: The impact of family history of diabetes
on risk factors for gestational diabetes. Clin Endocrinol (Oxf).
67:754–760. 2007.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Metzger BE, Lowe LP, Dyer AR, Trimble ER,
Chaovarindr U, Coustan DR, Hadden DR, McCance DR, Hod M, McIntyre
HD, et al: HAPO Study Cooperative Research Group. Hyperglycemia and
adverse pregnancy outcomes. N Engl J Med. 358:1991–2002.
2008.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Ares J, Martín-Nieto A, Díaz-Naya L,
Tartón T, Menéndez-Prada T, Ragnarsson CS, Delgado-Álvarez E and
Menéndez-Torre E: Gestational diabetes mellitus (GDM): Relationship
between higher cutoff values for 100 g oral glucose tolerance test
(OGTT) and insulin requirement during pregnancy. Matern Child
Health J. 21:1488–1492. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Ekelund M, Shaat N, Almgren P, Groop L and
Berntorp K: Prediction of pospartum diabetes in women with
gestational diabetes mellitus. Diabetologia. 53:452–457.
2010.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kc K, Shakya S and Zhang H: Gestational
diabetes mellitus and macrosomia: A literature review. Ann Nutr
Metab. 66 (Suppl 2):14–20. 2015.PubMed/NCBI View Article : Google Scholar
|
|
21
|
McFarland MB, Trylovich CG and Langer O:
Anthropometric differences in macrosomic infants of diabetic and
nondiabetic mothers. J Matern Fetal Med. 7:292–295. 1998.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Getahun D, Fassett MJ and Jacobsen SJ:
Gestational diabetes: Risk of recurrence in subsequent pregnancies.
Am J Obstet Gynecol. 203:467.e1–467.e6. 2010.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Liu B, Chen H, Xu Y, An C, Zhong L, Wang
X, Zhang Y, Chen H, Zhang J and Wang Z: Fetal growth is associated
with maternal fasting plasma glucose at first prenatal visit. PLoS
One. 9(e116352)2014.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Martin KE, Grivell RM, Yelland LN and Dodd
JM: The influence of maternal BMI and gestational diabetes on
pregnancy outcome. Diabetes Res Clin Pract. 108:508–513.
2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Young C, Kuehl TJ, Sulak PJ and Allen SR:
Gestational diabetes screening in subsequent pregnancies of
previously healthy patients. Am J Obstet Gynecol. 182:1024–1026.
2000.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Bianco ME and Josefson JL: Hyperglycemia
during pregnancy and long-term offspring outcomes. Curr Diab Rep.
19(143)2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
American Diabetes Association: 13.
Management of diabetes in pregnancy. Standards of medical care in
diabetes-2018. Diabetes Care. 41 (Suppl 1):S137–S143.
2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Mirghani HM and Hamud OA: The effect of
maternal diet restriction on pregnancy outcome. Am J Perinatol.
23:21–24. 2006.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Kösüs N, Kösüs A, Duran M and Turhan NO:
Effect of number of abnormal oral glucose tolerance test (OGTT)
values on birthweight in women with gestational diabetes. Indian J
Med Res. 137:95–101. 2013.PubMed/NCBI
|