Introduction
The aneurysmal bone cyst (ABC) was first defined by
Jaffe and Lichtenstein, in 1942, as an intra-osseous and osteolytic
lesion (1). ABC is a tumorous lesion
with unknown aetiology, influencing the metaphyseal regions of the
vertebrae and other bones (2). ABC
is usually benign but may be locally aggressive, damaging the
affected bones over time (3). ABC
also exhibits high vascularity and does not often spontaneous heal
(4,5). ABC commonly occurs in adolescents and
children, effecting >70% of patients under 20 years old
worldwide (4). The name ABC refers
to its aneurysmal growth in the bone, where it exhibits a cystic
bulge full of blood (4). Common
locations for ABC are the metaphysis, vertebral body, and iliac and
long tubular bones (4,6).
ABC occurring in the spinal column presents
difficulties during surgical operation (7) due to unclear field of vision, increased
blood loss and the possibility of not fully removing the lesions.
The treatment strategies for ABC are embolization, injection with a
fibrosing agent, intralesional curettage and resection (4,8).
Rigorous imaging evaluations prior to surgery and arterial
embolization can reduce intraoperative bleeding and improve
therapeutic efficacy and treatment compliance (9). In the current study, it was
demonstrated that preoperative embolization is effective and has
practical clinical value for spinal ABC.
Materials and methods
Study participants
A total of 3 males and 2 females were enrolled in
the current study. Inclusive criteria: Diagnosis was confirmed by
imaging and pathology; no other treatment, including drug therapy,
was performed before endovascular embolization. Exclusion criteria:
Secondary aneurysmal bone cyst; non vertebral aneurysmal bone cyst.
These patients were between the ages of 12 and 27 years old and had
been diagnosed with ABC at the Affiliated Hospital of North Sichuan
Medical College and People's Hospital of Nanbu County from January
2015 to April 2018. This study was approved by the Ethical
Committee of the Affiliated Hospital of North Sichuan Medical
College and People's Hospital of Nanbu County (approval no. 2018
ER(A)12-027). Written informed consent was obtained from adult
patients and legal guardian of minor patients. In these cases,
lesions were located in the L1 (n=2), L2 (n=1), T8 (n=1) and T12
(n=1) vertebrae (Table I). The main
symptoms were lumbar back pain and local swelling. Although the
neurological symptoms in this cohort were not obvious, there were
signs of neurological issues, including radiating pain in the upper
limb and chest, little finger abduction and iliopsoas muscle
tenderness.
 | Table IBaseline information of study
participants. |
Table I
Baseline information of study
participants.
| Sex | Age (years) | Region | Symptoms | Signs of physical
examination | Hospital stay
duration (days) | Blood loss (ml) | Treatment
outcome |
|---|
| M | 12 | L1 | Back pain | Radiating right upper
limb pain | 17 | 500 | Symptoms
relieved |
| M | 18 | T8 | Pain and local
swelling | Radiating chest
pain | 18 | 700 | Symptoms
relieved |
| M | 8 | L1 | Local swelling | Flexion of left
pinkie and inability to abduct | 20 | 600 | Symptoms
relieved |
| F | 27 | L2 | Pain | Tenderness of
iliopsoas | 18 | 1000 | Symptoms
relieved |
| F | 8 | T12 | Pain | None | 13 | 700 | Symptoms
relieved |
Arteriography and embolization
therapy
The arteriography and embolization therapy were
conducted as previously reported (10,11) with
a few modifications. Angiography was performed by puncture of the
right femoral artery under local anaesthesia. A pigtail catheter
was used for descending aortography to identify the intercostal
and/or lumbar arteries involved in the lesion's blood supply.
Depending on the supplying artery, an appropriate catheter was used
for selective angiography. The spinal artery may originate from the
posterior intercostal artery, necessitating the dilution contrast
medium during angiography to prevent spinal cord injury. The degree
of embolization was judged by blood flow velocity during
embolization. When the blood flow was visibly slowed, gelatine
sponge particles stopped being inserted and coils were pushed into
the trunk of the supplying artery. After embolization, surgery was
performed to remove the lesion 24-48 h later.
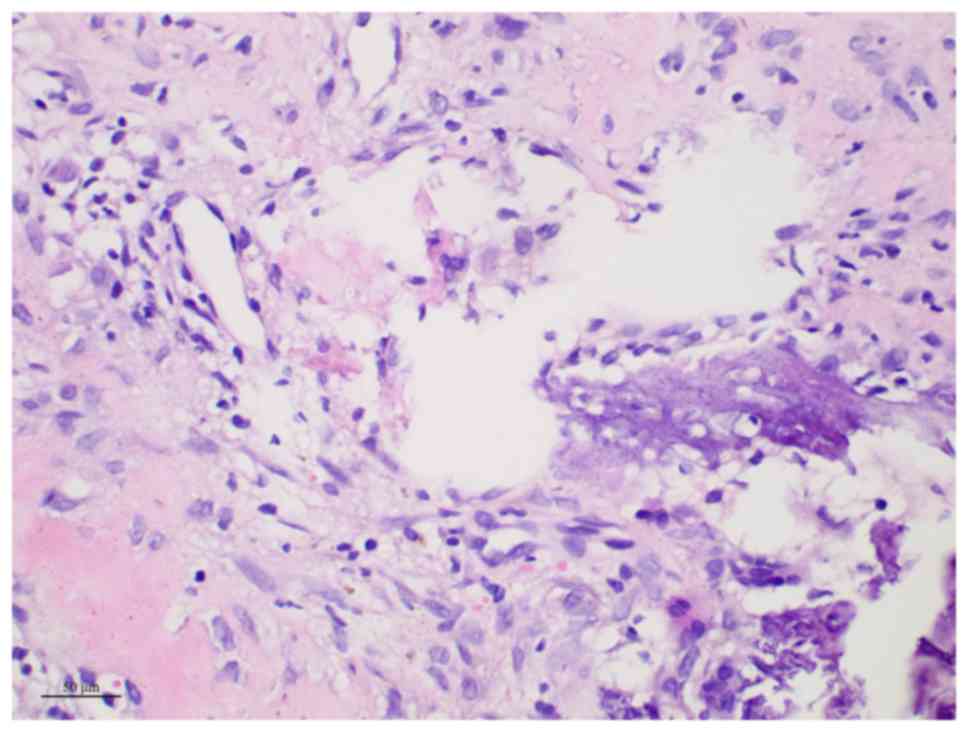
Haematoxylin and eosin staining
The resected bone tissue was fixed with 10% neutral
phosphate buffered formalin (NBF) at 25˚C. After 1-2 days of
fixation, the tissue block was dehydrated with gradient ethanol
solution, washed using xylene, soaked in paraffin (60˚C)
for 2 h, and then embedded into a wax block. A Leica RM 2235 (Leica
Biosystems) slicer was used for slicing. The slice thickness was
0.3 µm. Haematoxylin and eosin [Kilton Biotechnology (Shanghai)
Co., Ltd.] was used to stain the nuclei and cytoplasm for 7-9 and
2-5 min, respectively, both at room temperature. After staining,
gradient ethanol dehydration, washing with xylene and neutral gum
sealing piece were successively carried out. Finally, sections were
observed under a microscope (EM-300; Philips Healthcare) with
magnification, x400.
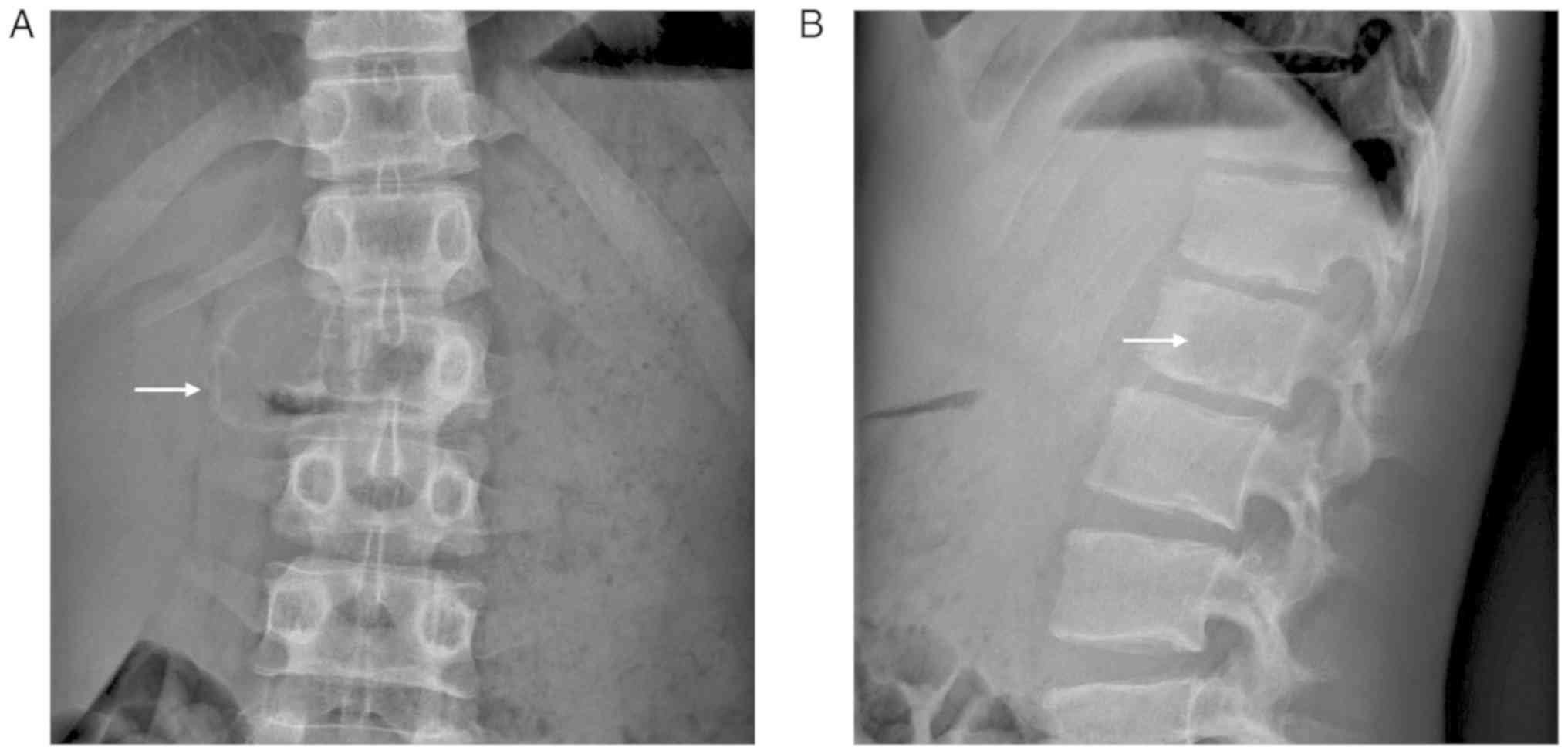
Results
ABC occurred in the extraspinal part of the
vertebral body in all 5 cases, showing expansive changes with
varying degrees of bone involvement. Destruction and compression of
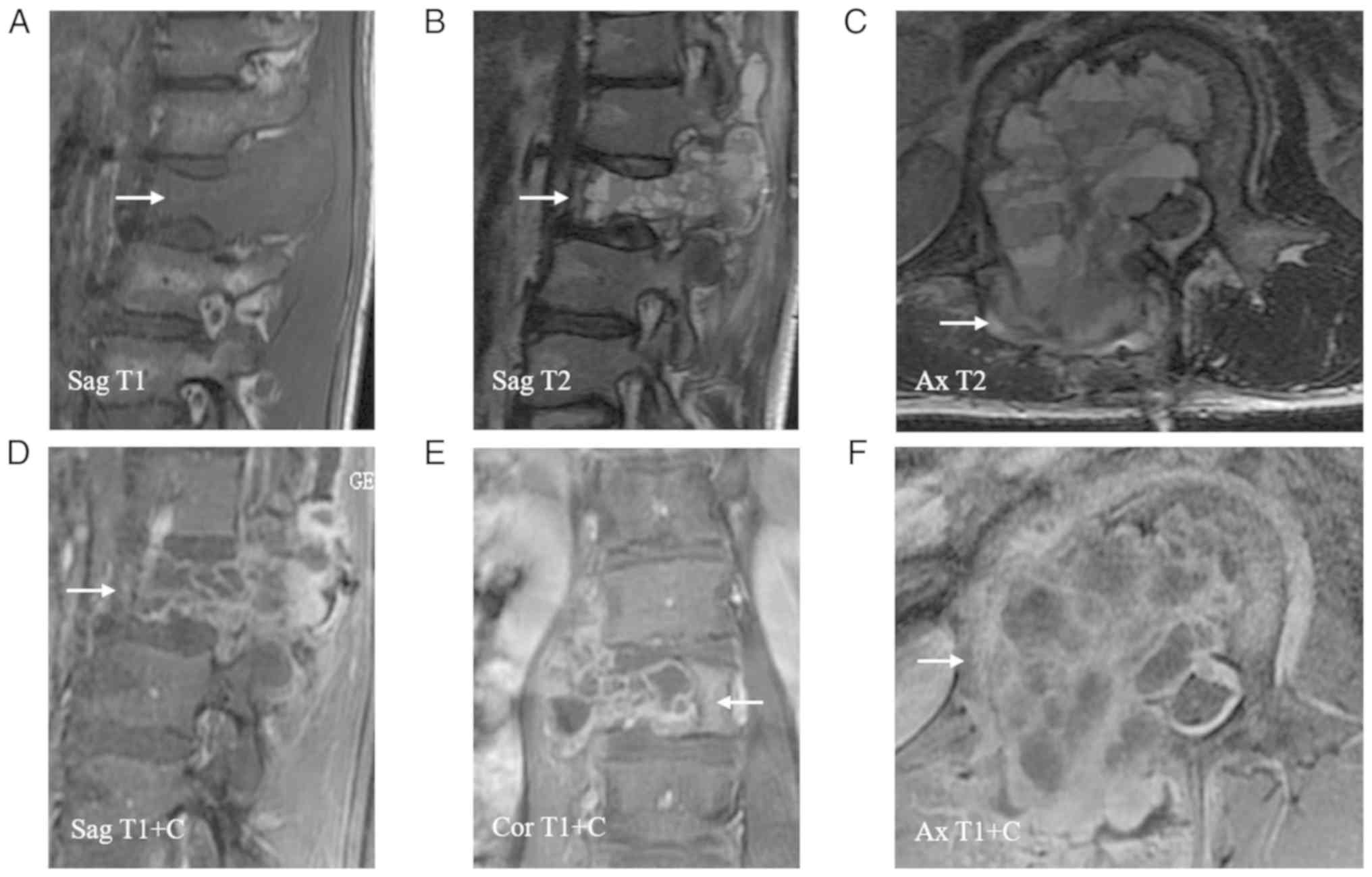
the pedicle and spinous process were present (Fig. 1). The spinal canal at the
corresponding level of the lesion was narrowed and the thecal sac
was compressed with invasion of the right psoas major (Fig. 2).
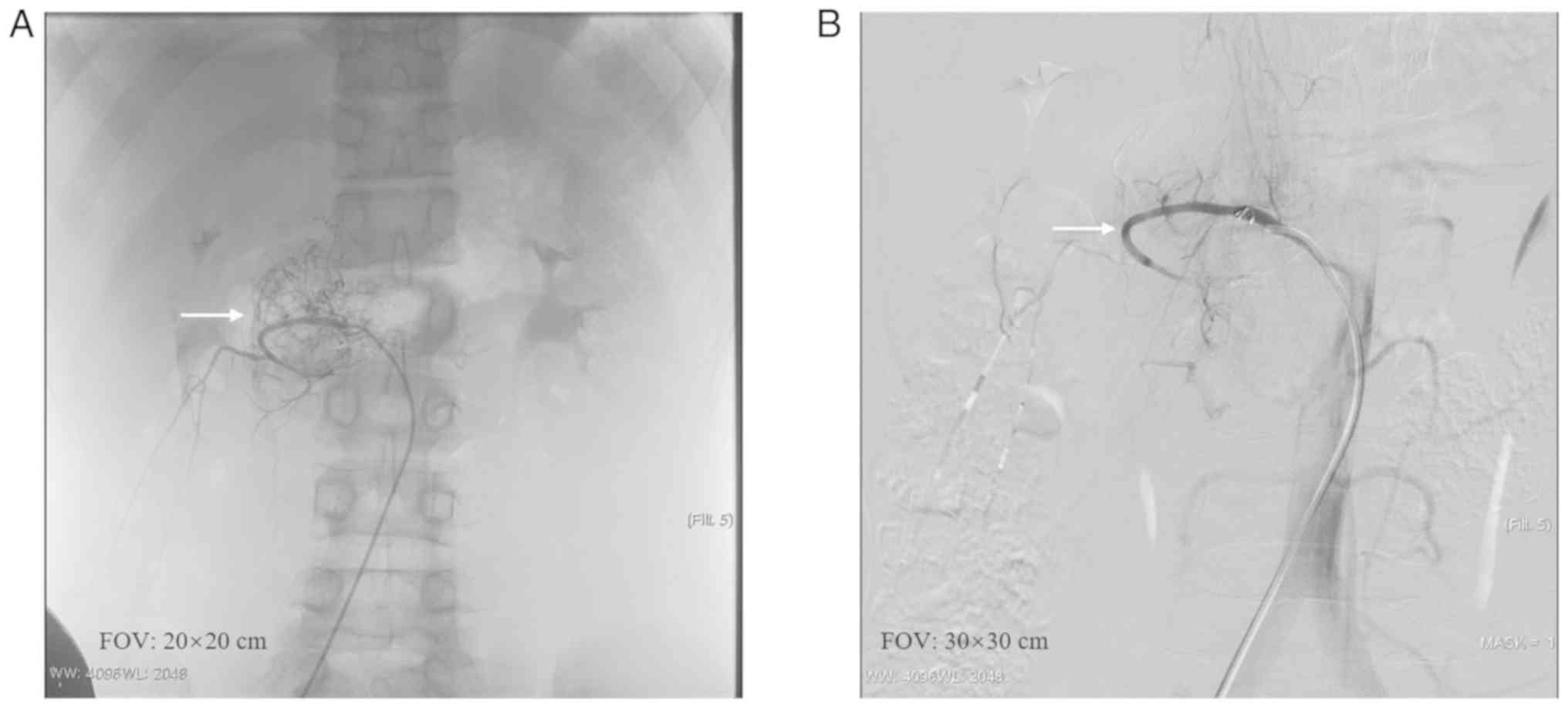
Angiography indicated that the vessels most
frequently supplying the lesions were the intercostal and/or lumbar
artery, which were significantly thickened and showed spiral and
tortuous forms, leading to compression in an arc in some cases
(Fig. 3A). The lesions showed
abnormal mass-like staining. The blood vessels were increased in
number and disordered, displaying multi-vessel tumour-like changes,
and the surrounding soft tissue formed small vessels of different
sizes (Fig. 3A). Contrast media was
patchy and irregular and no manifestations of arteriovenous fistula
were identified. Following embolization, the vessels and lesions
were not stained by the contrast media, indicating an adequate
reduction in perfusion (Fig. 3B).
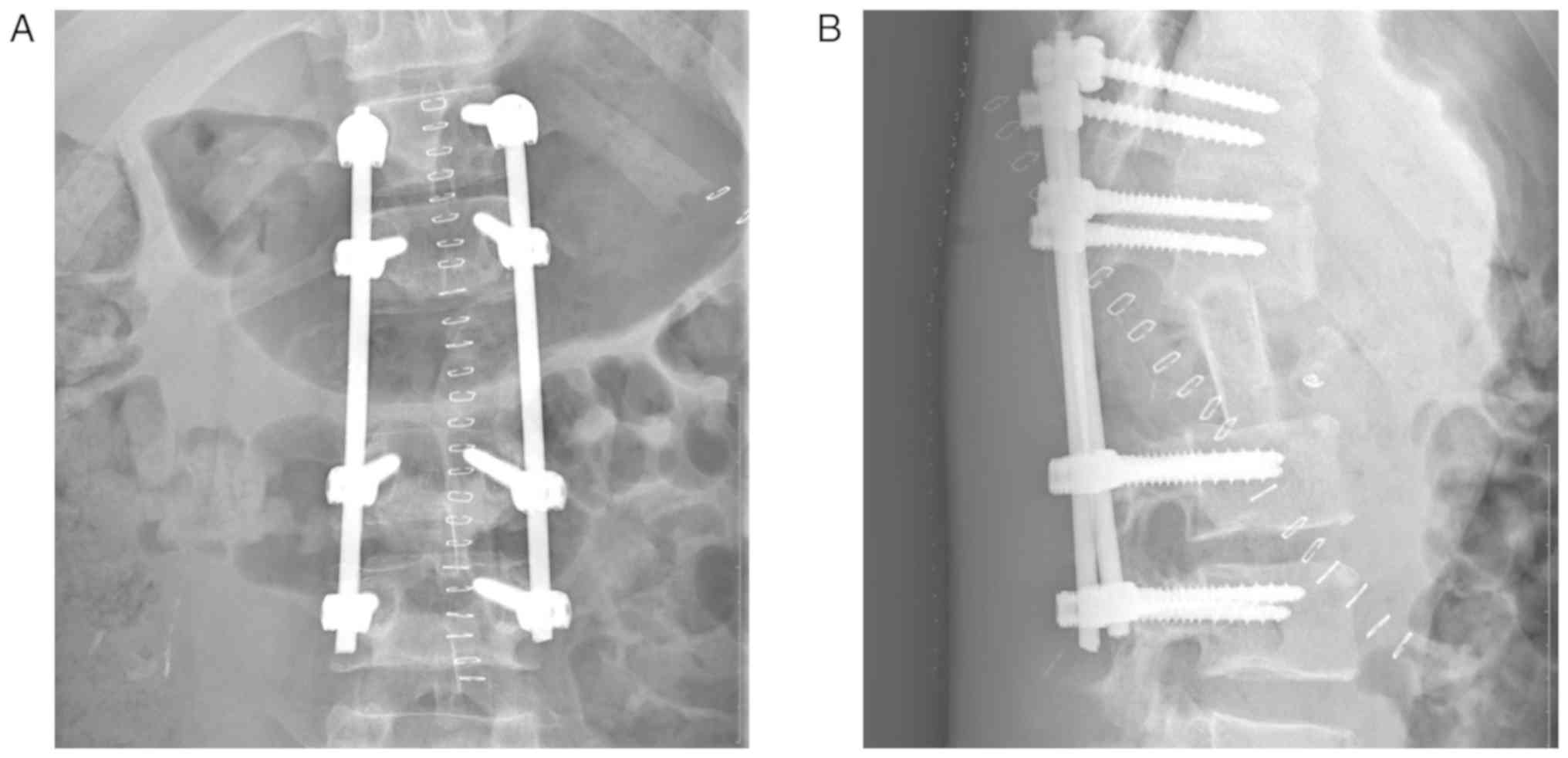
Laminectomy and posterior fixation were performed 1-2 days after
embolization (Fig. 4) and blood loss
during surgery was between 500-1,000 ml. Images of haematoxylin and
eosin staining were consistent with ABC, and no obvious
inflammatory or pathological changes were observed in the samples
(Fig. 5). The figures presented
represent the imaging manifestations and endovascular treatment of
all 5 patients.
Discussion
ABC may occur at any segment of the spine and has
different imaging characteristics at different stages and
locations. Radiographic manifestations such as lytic bone
destruction, thin layer ossification, bone surface roughness, bone
ridge and bone separation can be detected by X-ray (12,13). As
the lesion progresses, vertebral segments, including the vertebral
arch and transverse process are damaged and become thinner,
compressed and displaced, which may easily lead to pathological
fracture (14). Computed tomography
(CT) aids in the assessment of pedicle and vertebral body integrity
prior to surgery. The presence of a multilocular cyst with a
liquid-liquid interface on T2WI is highly suggestive of
ABC (6,15). Inside the tumour, multiple cysts with
fluid matter are present, revealing a different signal intensity in
T1WI and T2WI. These liquid-liquid
manifestations are due to the varying degrees of blood oxidation
and breakdown products in the cyst fluid (16,17).
Treatment for some ABCs is difficult, especially in
the spine and sacrum. For large frontal lesions, local excision or
scraping is not easy and disease tissue may remain after surgery.
Simultaneously, massive intraoperative bleeding is a significant
problem (18). Current surgical
treatments are not satisfactory in the balance of trauma and
therapeutic effect and the occurrence of relapse is high (19). Radiotherapy and hormone therapy are
also ineffective treatment and can lead to recurrence (6,20). In
addition, radiotherapy carries other risks such as myelopathy and
radiation-induced spinal deformity. Interventional embolization can
affect the lesion's hemodynamic features, thus promoting the repair
process (21,22). Identification of the blood vessels
responsible for the tumour's blood supply is critical for
preoperative embolization. The purpose of angiography is to
understand the extent of the lesion, the relationship between
multiple supply arteries and to identify the relationship between
the spinal cord feeding arteries and the arteries supplying the
lesion (23).
The blood supply in the spinal ABC is complex and
involves multiple blood vessels (13). In general, the lesion is supplied by
the intercostal artery and lumbar artery at the same level as the
vertebra, but adjacent arteries may also be involved. Therefore,
preoperative abdominal aortography is of great significance in
assessing the number supplying arteries. This technique can also
determine whether there are vascular co-trunks in the vessels
supplying the spinal cord, providing visual confirmation for
vascular selection and embolization.
It is crucial to select the appropriate size of the
materials used for embolization because of the potential of
breaking off during the procedure, leading to ectopic embolization
(24). Therefore, the embolization
process should be hyper-selective, target the vessel furthest from
the lesion to avoid the remaining small co-trunk vessels, and be
performed slowly under fluoroscopy. When the blood flow velocity is
visibly slowed, the main trunk of the supply artery is adequately
embolized with appropriately-sized micro-coils. After embolization
of the supply artery, the demarcation between the tumour-like
tissue and the surrounding normal tissue becomes more clear, which
is beneficial for reducing bleeding, separating the tissue during
surgery and improving the therapeutic effect of the treatment. In
the present study, surgical operations, including curettage and
resection, were performed 1-2 days after interventional
embolization and it was demonstrated that preoperative embolization
was effective and is a valuable treatment method for this
condition. Some studies have previously reported that zoledronic
acid and other materials can be used to treat ABCs (25-27).
In the cohort enrolled in the current study, preoperative
embolization was only used as an adjuvant treatment in combination
with other treatment methods, rather than a standalone treatment
strategy.
The present study was a retrospective analysis, and
no comparative analysis and case-control cohort were conducted.
Additionally, the small sample size was also a limitation of the
current study. In conclusion, interventional embolization can be
used before surgery to optimise conditions for ABCs in challenging
locations.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analysed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
QZ and HX made substantial contributions to the
conception and design of the study and wrote the original draft of
the manuscript. XLM, LY and YJR were responsible for data
acquisition and conducted data analysis and interpretation. HX
revised the manuscript critically for important intellectual
content. All authors read and approved the final version of the
manuscript.
Ethical approval and consent to
participate
This study was approved by the Ethical Committee of
the Affiliated Hospital of North Sichuan Medical College and
People's Hospital of Nanbu County (approval no. 2018 ER(A)12-027).
Written informed consent was obtained from adult patients and legal
guardian of minor patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jaffe HL: Aneurysmal bone cyst. Bull Hosp
Joint Dis. 11:3–13. 1950.PubMed/NCBI
|
|
2
|
Hetaimish BM and Alshaya OS: Pediatric
aneurysmal bone cyst in the ischial region. Saudi Med J.
37:799–803. 2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Mankin KP, Bischoff RJ, Gelberman RH and
Rosenberg AE: Aneurysmal bone cyst in involving the lunate. J Hand
Surg Br. 20:12–15. 1995.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Cottalorda J, Kohler R, Sales de Gauzy J,
Chotel F, Mazda K, Lefort G, Louahem D, Bourelle S and Dimeglio A:
Epidemiology of aneurysmal bone cyst in children: A multicenter
study and literature review. J Pediatr Orthop B. 13:389–394.
2004.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Malghem J, Maldague B, Esselinckx W, Noel
H, De Nayer P and Vincent A: Spontaneous healing of aneurysmal bone
cysts. A report of three cases. J Bone Joint Surg Br. 71:645–650.
1989.PubMed/NCBI
|
|
6
|
Parker J, Soltani S, Boissiere L, Obeid I,
Gille O and Kieser DC: Spinal Aneurysmal bone cysts (ABCs): Optimal
management. Orthop Res Rev. 11:159–166. 2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Mascard E, Gomez-Brouchet A and Lambot K:
Bone cysts: Unicameral and aneurysmal bone cyst. Orthop Traumatol
Surg Res. 101 (Suppl 1):S119–S127. 2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Dormans JP, Hanna BG, Johnston DR and
Khurana JS: Surgical treatment and recurrence rate of aneurysmal
bone cysts in children. Clin Orthop Relat Res. 421:205–211.
2004.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Liu Y, Wang J, Lin L, Sang C, Lin Z, Pan Y
and Fu X: Clinical study on complications of intracranial reptured
aneurysm embolization by stent-assisted coil. Med Sci Monit.
24:8115–8124. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
You Y, Choi SH, Choi DW, Heo JS, Han IW,
Han S, Shin SW, Park KB, Park HS, Cho SK and Han SH: Long-term
clinical outcomes after endovascular management of ruptured
pseudoaneurysm in patients undergoing pancreaticoduodenectomy. Ann
Surg Treat Res. 96:237–247. 2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Meyers PM, Shcumacher HC, Higashida RT,
Derdeyn CP, Nesbit GM, Sacks D, Wechsler LR, Bederson JB, Lavine SD
and Rasmussen P: Reporting standards for endovascular repair of
saccular intracranial cerebral aneurysms. AJNR Am J Neuroradiol.
31:E12–E24. 2010.PubMed/NCBI
|
|
12
|
Hermann AL, Polivka M, Loit MP, Guichard
JP and Bousson V: Aneurysmal bone cyst of the frontal bone-A
radiologic-pathologic correlation. J Radiol Case Rep. 12:16–24.
2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Afnan J, Snuderl M and Small J:
Intracranial, intradural aneurysmal bone cyst. Clin Imaging.
39:297–299. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ghermandi R, Terzi S, Gasbarrini A and
Boriani S: Denosumab: Non-surgical treatment option for selective
arterial embolization resistant aneurysmal bone cyst of the spine
and sacrum. Case report. Eur Rev Med Pharmacol Sci. 20:3692–3695.
2016.PubMed/NCBI
|
|
15
|
Bazzocchi A, Spinnato P, Mercatelli D and
Aparisi Gómez MP: Fluid-fluid levels in aneurysmal bone cysts. J
Pediatr. 204(317)2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Lopez LV, Roduriguez MG, Siegal GP and Wei
S: Extraskeletal aneurysmal bone cyst: Report of a case and review
of the literature. Pathol Res Pract. 213:1445–1449. 2017.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Baker KS, Gould ES, Patel HB and Hwang SJ:
Soft tissue aneurysmal bone cyst: A rare case in a middle aged
patient. J Radiol Case Rep. 9:26–35. 2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Mankin HJ, Homicek FJ, Ortiz-Cruz E,
Villafuerte J and Gebhardt MC: Aneurysmal bone cyst: A review of
150 patients. J Clin Oncol. 23:6756–6762. 2015.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Steffner RJ, Liao C, Stacy G, Atanda A,
Attar S, Avedian R and Peabody TD: Factors associated with
recurrence of primary aneurysmal bone cysts: Is argon beam
coagulation an effective adjuvant treatment? J Bone Joint Surg Am.
93:e1221–e1229. 2011.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Patel RS, Dhamne CA, Gopinathan A and
Kumar N and Kumar N: Denosumab: A potential treatment option for
aneurysmal bone cyst of the atlas. Eur Spine J. 27 (Suppl
3):S494–S500. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Rajput D, Tungaria A, Jaiswal A and Jain
V: Aneurysmal bone cyst of clivus and C1 C2: Case report and review
of literature. Turk Neurosurg. 22:105–108. 2012.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Doss VT, Weaver J, Didier S and Arthur AS:
Serial endovascular embolization as stand-alone treatment of a
sacral aneurysmal bone cyst. J Neurosurg Spine. 20:234–238.
2014.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Patsalides A, Leng LZ, Kimball D, Marcus
J, Knopman J, Laufer I, Bilsky M and Gobin YP: Preoperative
catheter spinal angiography and embolization of cervical spinal
tumors: Outcomes from a single Center. Interv Neuroradiol.
22:457–465. 2016.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Guo J, Yu J, Zhang Q and Song X: Clinical
efficacy and safety of Utrine artery embolization (UAE) versus
laparoscopic Cesarean scar pregnancy debridement surgery (LCSPDS)
in treatment of Cesarean scar pregnancy. Med Sci Monit.
24:4659–4666. 2018.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Simm PJ, O'Sullivan M and Zacharin MR:
Successful treatment of a sacral aneurysmal bone cyst with
Zoledronic acid. J Pediatr Orthop. 33:e61–e64. 2013.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Topouchian V, Mazda K, Hamze B, Laredo JD
and Penneçot GF: Aneurysmal bone cysts in children: Complications
of fibrosing agent injection. Radiology. 232:522–526.
2004.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Peraud A, Drake JM, Armstrong D, Hedden D,
Babyn P and Wilson G: Fatal ethibloc embolization of
vertebrobasilar system following percutaneous injection into
aneurysmal bone cyst of the second cervical vertebra. AJNR Am J
Neuroradiol. 25:1116–1120. 2004.PubMed/NCBI
|