Introduction
The death of retinal ganglion cell axons and the
alteration of the optic nerve may cause optic neuropathy (1). Chronic neuropathy is termed glaucoma
(2), which may lead to progressive
neuropathy and then blindness (1).
The etiology of blindness varies among different
populations. In developed countries, age-associated macular
degeneration is the primary cause; however, in certain undeveloped
countries, infections (i.e. trachoma) are the leading cause depend
on/vary among ethnicities (3). The
leading cause of blindness among white individuals was reported to
be age-associated macular degeneration (54.4% of cases), while
among black individuals, cataract and glaucoma accounted for
>60% of cases of blindness (4).
The prevalence rates and the clinical burden (e.g. glaucomatous
damage, vision loss, blindness, social withdrawal due to blindness)
of open-angle glaucoma are high in the Chinese population (5).
High intraocular pressure (IOP) is the major risk
parameter used to determine the prevalence and development of
glaucoma. Therefore, lowering the IOP is beneficial in the
development of glaucoma (6).
Several methods are available for reducing IOP, for example, laser
treatment, surgery, and pharmaceutical treatments; however, laser
treatment and surgery are less effective compared with medication
(1).
An evening dose of prostaglandin analogs is
typically used as monotherapy to decrease IOP (7). Latanoprost (LT) is a well-established
monotherapy to treat open-angle glaucoma, initially for 2 years
(8). Travoprost (TV) is a
prostaglandin F2a analog (9) and
has reported efficacy in open-angle glaucoma (10); however, the efficacy and safety of
TV may be different compared with that for LT in treating
open-angle glaucoma (2,11). Certain cross-sectional studies have
reported superiority of TV over LT (7,12);
however, other studies have reported equal efficacy and safety
(13,14) in the management of open-angle
glaucoma. There is also a lack of available comprehensive data on
the effectiveness of TV and associated adverse effects. Thus,
further research is required.
The objectives of the present retrospective study
were to compare the effectiveness and safety of an evening dose of
TV compared with that for LT in the management of open-angle
glaucoma.
Materials and methods
Study population
The records of patients with primary open-angle
glaucoma and an IOP of >21 mmHg were extracted from the
outpatient records from the Huizhou Municipal Central Hospital
(Guangdong, China) from 1st January 2018 to 1st July 2019, and the
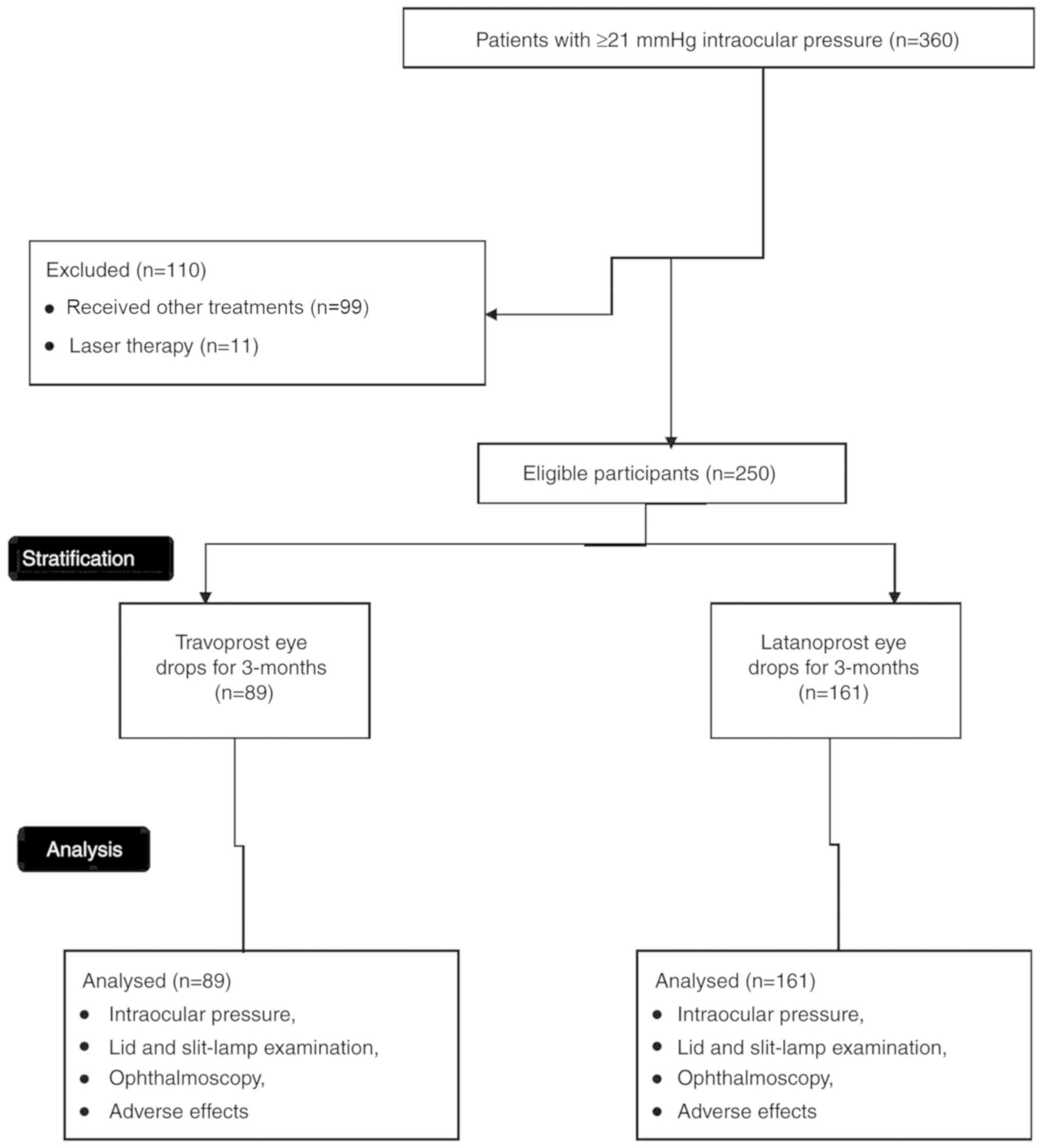
data of 360 affected eyes were retrieved. Patients who were treated
with drugs other than TV or LT (99 affected eyes) and subjected to
laser therapy (11 affected eyes) were excluded from the analysis.
The data on the 250 remaining patients with primary open-angle
glaucoma and treated with either TV or LT [based on the decision of
the ophthalmologist(s)] were retrospectively included in the
analyses (Fig. 1). If patients were
affected bilaterally, the patients were instructed to use drops in
both eyes and the data of both eyes were included in the
analysis.
Cohort
A total of 89 patients with (an) affected eye(s)
were treated with 40 µg/ml TV eye drops (Travatan®;
Alcon Laboratories Inc.) once in the evening (8 pm) (15) for 3-months and 161 patients were
treated with 50 µg/ml LT eye drops (Xalatan; Pfizer Inc.) once in
the evening (8 pm) (16) for
3-months. These two groups were termed the TV and LT group,
respectively.
IOP measurements
A total of 3 different measurements were performed
by ophthalmologists (with a minimum of 3-years of experience) using
the Goldman Applanation Tonometer (Haag-Streit AG) in the morning
(10 am), afternoon (2 pm) and evening (6 pm) and the mean of all
three measurements were used for the analysis of IOP (17).
Lid and slit-lamp examination
The lid and slit-lamp examination was performed by
ophthalmologists (with a minimum of 3-years of experience). The
upper and lower eyelids, the margin between the upper and the lower
eyelids and any abnormal signs within the eyelids, conjunctiva,
cornea, anterior chamber and the lens were examined. The
abnormalities were scored using the following grading system: 0,
Absent; 1, mild; 2, moderate; and 3, severe (maximum possible)
(3). Conjunctival hyperemia was
assessed in the temporal peripheral, nasal peripheral, central
inferonasal, central superonasal, central inferotemporal and
central superotemporal region of the eyes using the following
classification: 0, Absent; 1, mild hyperemia; 2, moderate
hyperemia; and 3, severe hyperemia (maximum possible) (Fig. 2). Conjunctival staining was
evaluated in the same area using Lissamine green dye and scored as
follows: 0, Absent; 1, mild staining; 2, moderate staining; and 3,
severe staining (maximum possible). Corneal staining was assessed
from the superior, inferior, central, temporal and nasal area of
the cornea as follows: 0, Absent; 1, mild staining; 2, moderate
staining; and 3, severe staining (maximum possible; Fig. 3) (13).
Ophthalmoscopy
Ophthalmoscopy was performed by ophthalmologists
(with a minimum of 3-years of experience) to examine the optic
nerve head, the vertical cup to disc ratio and the optic disc
hemorrhages (3). All of the
parameters were evaluated at the start of treatment during a
routine check-up and at the end of treatment. The other adverse
effects occurring were recorded at the end of the 3 months and
analyzed.
Statistical analysis
SPSS statistics version 26 (IBM Corp.) was used for
statistical analysis. Fischer's exact test was performed for
ordinal and continuous data and the Mann-Whitney U test
(between-groups) or the Wilcoxon test (within-group) (3) was performed for continuous variables.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Study population
Patients from 37 to 73 years were included in
analyses. Among 250 patients, 125 patients were male and 125
patients were female (1:1). There was no significant difference in
the demographical characteristics and clinical conditions between
the two cohorts at the time of admission (all P>0.05). The
demographic and clinicopathological characteristics of the patients
enrolled are provided in Table
I.
 | Table IDemographic and clinicopathological
and characteristics of the patients on admission. |
Table I
Demographic and clinicopathological
and characteristics of the patients on admission.
| Characteristic | TV group (n=89) | LT group (n=161) | P-value |
|---|
| Intraocular pressure
(mmHg) | 23.45±1.52 | 23.93±2.11 | 0.060 |
| Age (years) | | | 0.459 |
|
Range | 37-72 | 41-73 | |
|
Mean | 63.12±11.13 | 64.15±10.14 | |
| Sex | | | 0.792 |
|
Male | 43(48) | 82(51) | |
|
Female | 46(52) | 79(49) | |
| History of visual
complications (months) | 40.12±5.45 | 41.23±4.55 | 0.087 |
| Ethnicity | | | 0.910 |
|
Han
Chinese | 80(90) | 147(91) | |
|
Mongolian | 8(9) | 12(8) | |
|
Tibetan | 1(1) | 2(1) | |
|
Diabetes | 11(12) | 18(11) | 0.838 |
|
Dyslipidemia | 8(9) | 18(11) | 0.669 |
|
Hypertension | 8(9) | 13(8) | 0.815 |
|
Migraine | 15(17) | 25(16) | 0.857 |
|
Smoking | 7(19) | 5(9) | 0.122 |
|
Family
history of glaucoma | 5(6) | 11(7) | 0.793 |
Efficacy
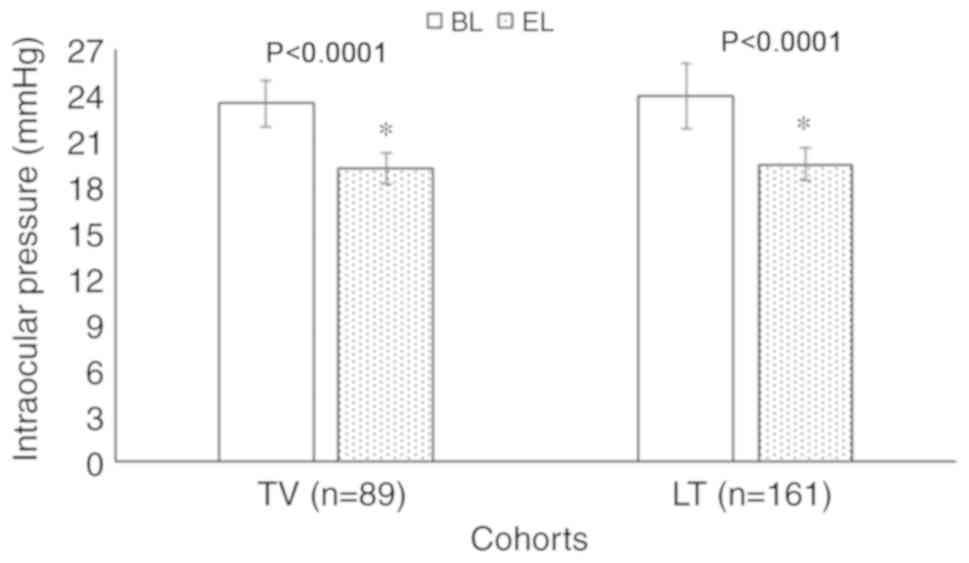
Following 3 months of treatment, a significant
reduction in IOP as compared with that at the start of treatment
was obtained with TV (23.45±1.52 mmHg vs. 19.15±1.01 mmHg;
P<0.0001) and LT (23.93±2.11 mmHg vs. 19.45±1.11 mmHg;
P<0.0001). However, there were no significant differences in IOP
values at the end of treatment between the two groups (19.15±1.01
mmHg vs. 19.45±1.11 mmHg; P=0.120; Fig.
4).
Safety
Corrected visual acuity (P=0.936), visual field
defect (P=0.367), and vertical cup to disc ratio (P=0.086) had no
differences between the two groups at baseline. Following treatment
for 3 months and a comparison between 3 months and the baseline, no
adverse effects on visual acuity, visual field and the vertical cup
to disc ratio were observed for TV and LT and the data were very
similar between the two cohorts at 3 months (all P>0.05;
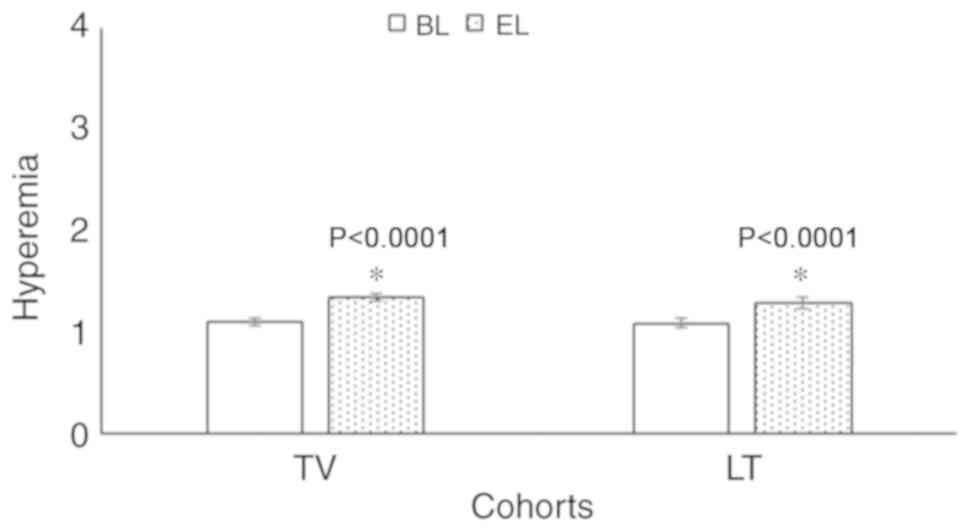
Table II). There was also no
significant difference in the qualitative slit-lamp characteristics
(all P>0.05; Table III), but
non-slit-lamp characteristics, for example hyperemia, were
significantly increased in each group after treatment (P<0.0001
for both drugs; Fig. 5) but that
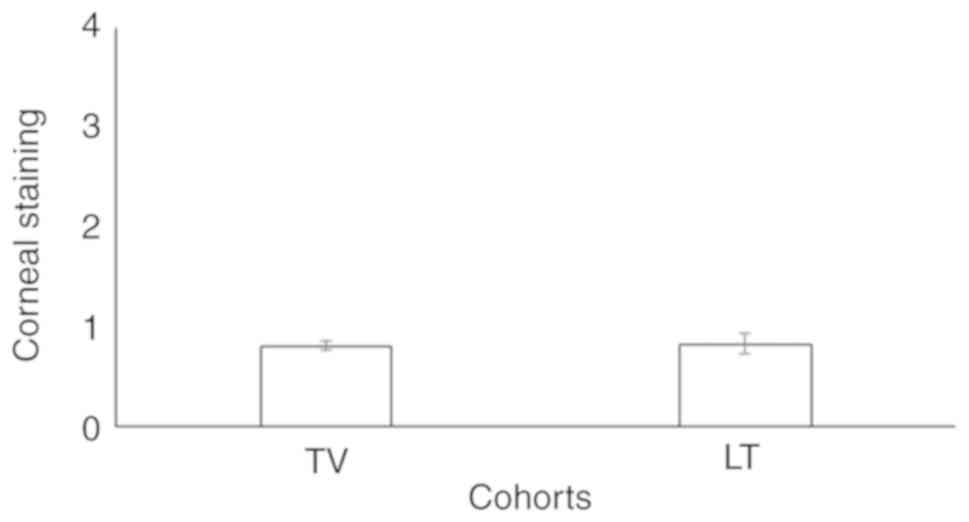
there was no significant inter-group difference. In addition, there
was no significant difference in corneal staining (0.81±0.05 vs.
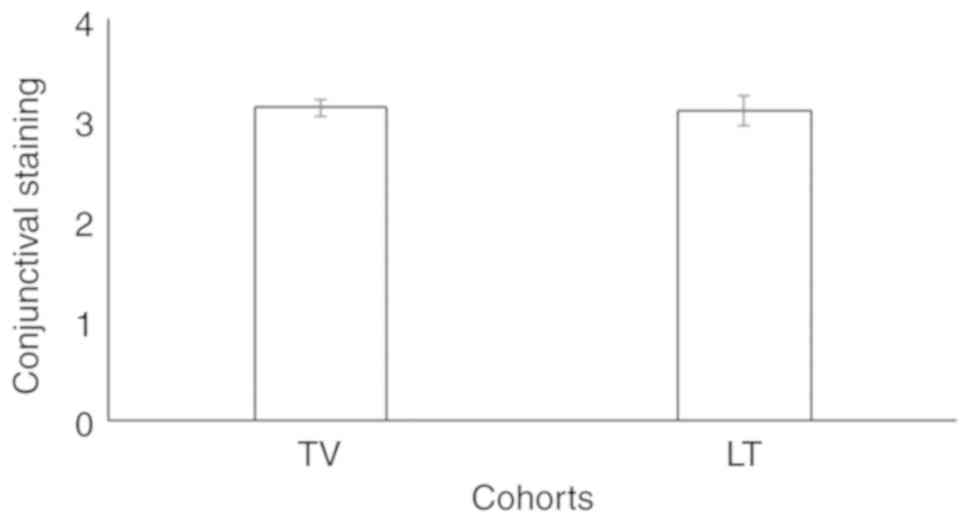
0.83±0.10; P=0.078; Fig. 6) and
conjunctival staining (3.11±0.08 vs. 3.08±0.15; P=0.081; Fig. 7) between the two groups at the end
of treatment.
| Table IISafety assessment. |
Table II
Safety assessment.
| | TV group | LT group |
|---|
| Item | BL (n=89) | EL (n=89) | P-value | BL (n=161) | EL (n=161) | P-value |
|---|
| Best-corrected
visual acuity | 9.25±1.88 | 9.24±1.81 | 0.971 | 9.27±1.89 | 9.26±1.88 | 0.962 |
| Visual field
defect | -0.66±0.09 | -0.67±0.10 | 0.484 | -0.65±0.08 | -0.66±0.09 | 0.293 |
| Vertical cup to
disc ratio | 0.61±0.03 | 0.62±0.04 | 0.061 | 0.62±0.05 | 0.63±0.06 | 0.105 |
| Table IIIQualitative results of the slit-lamp
examination. |
Table III
Qualitative results of the slit-lamp
examination.
| | TV group | LT group |
|---|
| Location | BL (n=89) | EL (n=89) | P-value | BL (n=161) | EL (n=161) | P-value |
|---|
| Eyelids | 1.03±0.02 | 1.04±0.05 | 0.082 | 1.04±0.04 | 1.05±0.06 | 0.079 |
| Cornea | 1.02±0.03 | 1.03±0.05 | 0.108 | 1.01±0.03 | 1.02±0.06 | 0.060 |
| Conjunctiva | 1.03±0.03 | 1.04±0.04 | 0.061 | 1.04±0.05 | 1.05±0.09 | 0.219 |
| Iris | 1.09±0.05 | 1.10±0.05 | 0.184 | 1.08±0.04 | 1.09±0.06 | 0.079 |
| Anterior
chamber | 1.02±0.04 | 1.03±0.05 | 0.142 | 1.06±0.06 | 1.07±0.07 | 0.170 |
| Lens | 1.60±0.05 | 1.61±0.06 | 0.229 | 1.58±0.09 | 1.59±0.10 | 0.346 |
Treatment-emergent adverse
effects
Discomfort and irritation in the eyes were commonly
reported by patients during the 3 months of treatment. There were
significantly more patients with dry eyes (P=0.020) who received TV
treatment, while patients treated with LT had significantly more
frequent eyelid swelling (P=0.036) and complaints of headache
(P=0.037) following 3 months of treatment (Table IV).
| Table IVTreatment-emergent adverse effects
after 3 months. |
Table IV
Treatment-emergent adverse effects
after 3 months.
| Adverse effect | TV (n=89) | LT (n=161) | P-value |
|---|
| Eye pain | 8(9) | 7(4) | 0.167 |
| Change in color of
the iris | 4(4) | 11(7) | 0.583 |
| Eye discomfort | 12(13) | 15(9) | 0.192 |
| Dry eye | 11(12) | 8(5) | 0.020a |
| Itching in eye | 4(4) | 7(4) | 0.999 |
| Irritation in
eye | 5(6) | 16(10) | 0.341 |
| Eyelid
swelling | 1(1) | 12(7) | 0.036b |
| Skin rash | 1(1) | 5(3) | 0.426 |
| Headache | 2(2) | 15(9) | 0.037b |
Discussion
The present retrospective study indicated that the
evening doses of TV and LT controlled IOP at a similar level with
no significant inter-group difference (P=0.120) following 3 months
of treatment in patients with glaucoma. The results of IOP of the
present study were consistent with those of previous open-label,
prospective, non-randomized cohort studies (13,18),
prospective randomized clinical trials (19), a single-center, open-label trial
(14), a randomized crossover study
(20) and a prospective
observational study (21); however,
they were not in agreement with those of prospective,
cross-sectional studies (7,17). Comparisons over time are difficult
to evaluate in a cross-sectional study (22), as carry-over effects maybe reported
in a cross-sectional study (3,17),
which may be a possible reason for this discrepancy. The results of
the present study are also in contrast to those of a cross-over
randomized trial using morning doses of TV, as the IOP is higher in
the morning compared with that in the evening (higher baseline
untreated IOP) (23). The present
study identified that TV efficiently reduced IOP, and the efficacy
was similar to that of LT.
The IOP is higher in the morning (23) and a previous cross-sectional study
reported that TV was more effective in the management of IOP alone
compared with LT (7) and with
timolol (12); however, the present
study was performed using an evening dose, as the higher IOP values
in the morning may cause a type I error in the analysis (23). In addition, the manufacturers of TV
(15) and LT (16) advise that the drops should be used
in the evening in the management of glaucoma. The evening dose of
prostaglandin analogues may provide exact effects to reduce the
IOP.
The present study suggested that an evening dose of
TV was as safe as LT during the 3-months of treatment for patients
with glaucoma, which was consistent with the results of a previous
prospective nonrandomized study (1)
and a retrospective multicenter review (24). This indicates that the prostaglandin
analogs TV and LT may have a similar safety profile.
In the present study, a comparatively larger
proportion of patients receiving TV treatment experienced dry eyes,
while patients with LT treatment had more eyelid swelling and
headache following 3-months of treatment, while there was no
difference in the frequency of discomfort, irritation and hyperemia
between the groups. The results were consistent with those of a
previous randomized controlled trial (8), an open-label, prospective,
non-randomized cohort study (13),
a double-blinded randomized trial (9), a single-center, open-label trial
(14), and several randomized
crossover studies (12,17,20)
and prospective observational studies (18,21).
Of note, different prostaglandin analogs act on different
inflammatory pathways (1).
Long-term follow-up is required to evaluate the adverse effects of
treatment with prostaglandin analogs in the management of
glaucoma.
According to the manufacturer, Icare® PRO
is a high-precision tonometer; however, the present study used the
Goldman Applanation Tonometer for measuring IOP. There is a lack of
agreement regarding the accuracy of the Icare® PRO
tonometer, while the reports for the Goldman Applanation Tonometer
are consistent and provide an improved interpretation of the
IOP-lowering effect of anti-glaucoma medication (25). Clinicians should be aware of the
limitations of their labeled devices used in experimental
studies.
The present study is novel, as it provided a
justification for the use of the Goldman Applanation Tonometer; the
results are in contrast to those of a previous study (as discussed
above regarding the evening dose) and the present study provides
evidence for the preferred use of an evening dose. However, there
are several limitations. For instance, the present study was a
retrospective study with a relatively short duration and lacking a
control group. A longitudinal study is required, as different
prostaglandin analogs have a different time-span for peak action
(1). The follow-up period was
relatively short and did not include the result of the visual field
test of the patients. The interpretation of the IOP may be affected
by the central corneal thickness; however, this was not considered
in the present study.
In conclusion, the evening dose of TV and LT had the
same efficacy and safety in the management of primary open-angle
glaucoma with hyperemia (was significantly increased at 3 months
vs. baseline, but there was no significant difference between the
two drugs) and a relatively low frequency of manageable adverse
effects following treatment. However, a large randomized trial is
recommended to further support the present results.
Acknowledgements
Not applicable.
Funding
No funding received.
Availability of data and materials
The datasets used and analyzed during the current
study available from the corresponding author on reasonable
request.
Authors' contributions
All authors read and approved the study prior to
submission for publication. JL, as the project administrator,
contributed measurement of data and their evaluation and resources,
and performed checking of the results or internal/external
data/analysis and literature review of the study. XW contributed to
the methodology, supervision, software and literature review of the
study. GX contributed to the investigation, resources, formal
analysis and literature review of the study. RD contributed to
formal analysis, data curation, resources and literature review of
the study. LW contributed to supervision, data curation, validation
and literature review of the study. LZ contributed to validation,
supervision, software and literature review of the study. ZC
contributed to software, formal analysis, data curation and
literature review of the study and drafted, reviewed and edited the
manuscript for intellectual content. The author agrees to be
accountable for all aspects of work ensuring integrity and
accuracy.
Ethics approval and consent to
participate
The designed protocol (HMC/CL/14/19 dated 9 October
2019) of the present study was approved by the review board of
Huizhou Municipal Central Hospital (Huizhou, China). The study
adheres to the Law of China. Data of patients were collected from
institute following written approval from Huizhou Municipal Central
Hospital, China. The patients included provided written informed
consent for treatment during hospitalization.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ayala M and Chen E: The influence of
topical prostaglandin analogues in inflammation after selective
laser trabeculoplasty treatment. J Ocul Pharmacol Ther. 28:118–122.
2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Zhang XL and Qin L: Efficacy of travoprost
for the treatment of patients with glaucoma. Medicine (Baltimore).
98(e16526)2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Stalmans I, Oddone F, Cordeiro MF, Hommer
A, Montesano G, Ribeiro L, Sunaric-Mégevand G and Rossetti L:
Comparison of preservative-free latanoprost and preservative-free
bimatoprost in a multicenter, randomized, investigator-masked
cross-over clinical trial, the SPORT trial. Graefes Arch Clin Exp
Ophthalmol. 254:1151–1158. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Congdon N, O'Colmain B, Klaver CC, Klein
R, Muñoz B, Friedman DS, Kempen J, Taylor HR and Mitchell P: Eye
Diseases Prevalence Research Group. Causes and prevalence of visual
impairment among adults in the United States. Arch Ophthalmol.
122:477–485. 2004.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Song P, Wang J, Bucan K, Theodoratou E,
Rudan I and Chan KY: National and subnational prevalence and burden
of glaucoma in China: A systematic analysis. J Glob Health.
7(020705)2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ernest PJ, Schouten JS, Beckers HJ,
Hendrikse F, Prins MH and Webers CA: An evidence-based review of
prognostic factors for glaucomatous visual field progression.
Ophthalmology. 120:512–519. 2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Denis P, Launois R, Devaux M and Berdeaux
G: Comparison of diurnal intraocular pressure control by
latanoprost versus travoprost: Results of an observational survey.
Clin Drug Investig. 26:703–714. 2006.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Garway-Heath DF, Crabb DP, Bunce C,
Lascaratos G, Amalfitano F, Anand N, Azuara-Blanco A, Bourne RR,
Broadway DC, Cunliffe IA, et al: Latanoprost for open-angle
glaucoma (UKGTS): A randomised, multicentre, placebo-controlled
trial. Lancet. 385:1295–1304. 2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Peace JH, Ahlberg P, Wagner M, Lim JM,
Wirta D and Branch JD: Polyquaternium-1-preserved travoprost 0.003%
or benzalkonium chloride-preserved travoprost 0.004% for glaucoma
and ocular hypertension. Am J Ophthalmol. 160:266–274.
2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Chander A, Kapoor H and Thomas S:
Comparison of the efficacy and safety of bimatoprost (0.03%) and
travoprost (0.004%) in patients with primary open angle glaucoma.
Nepal J Ophthalmol. 5:75–80. 2013.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Tang W, Zhang F, Liu K and Duan X:
Efficacy and safety of prostaglandin analogues in primary
open-angle glaucoma or ocular hypertension patients: A
meta-analysis. Medicine (Baltimore). 90(e16597)2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Shoji T, Sato H, Mizukawa A, Hirota N,
Enoki T, Kojima T, Kanda T and Takeuchi M: Hypotensive effect of
latanoprost/timolol versus travoprost/timolol fixed combinations in
NTG patients: A randomized, multicenter, crossover clinical trial.
Invest Ophthalmol Vis Sci. 54:6242–6247. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Rahmatnejad K, Rapuano CJ, Ichhpujani P,
Wizov SS, Moster MR, Hark LA and Katz LJ: The effects of
latanoprost with benzalkonium chloride versus travoprost with
SofZia on the ocular surface. Eye Contact Lens. 44 (Suppl
2):S93–S98. 2018.PubMed/NCBI View Article : Google Scholar
|
|
14
|
El Hajj Moussa WG, Farhat RG, Nehme JC,
Sahyoun MA, Schakal AR, Jalkh AE, Abi Karam MP and Azar GG:
Comparison of efficacy and ocular surface disease index score
between bimatoprost, latanoprost, travoprost, and tafluprost in
glaucoma patients. J Ophthalmol. 2018(1319628)2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Alcon Laboratories Inc.: Package leaflet:
Information for the user TRAVATAN® 40 micrograms/ml eye
drops, solution travoprost. Available from: https://www.medicines.org.uk/emc/files/pil.1556.pdf.
Accessed October 1, 2019.
|
|
16
|
Pfizer Inc.. Package leaflet: Information
for the user Xalatan® 50 micrograms/ml eye drops,
solution latanoprost. Available from: https://www.medicines.org.uk/emc/files/pil.1616.pdf.
Accessed October 1, 2019.
|
|
17
|
Konstas AG, Kozobolis VP, Katsimpris IE,
Boboridis K, Koukoula S, Jenkins JN and Stewart WC: Efficacy and
safety of latanoprost versus travoprost in exfoliative glaucoma
patients. Ophthalmology. 114:653–657. 2007.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Parmaksiz S, Yüksel N, Karabas VL, Ozkan
B, Demirci G and Caglar Y: A comparison of travoprost, latanoprost,
and the fixed combination of dorzolamide and timolol in patients
with pseudoexfoliation glaucoma. Eur J Ophthalmol. 16:73–80.
2006.PubMed/NCBI
|
|
19
|
Blondeau P, Hamid M and Ghalie Z:
Prospective randomized clinical trial on the effects of
latanoprost, travoprost and bimatoprost on latanoprost
non-responders. J Fr Ophtalmol. 42:894–899. 2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Sawada A, Yamamoto T and Takatsuka N:
Randomized crossover study of latanoprost and travoprost in eyes
with open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol.
250:123–129. 2012.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Mishra D, Sinha BP and Kumar MS: Comparing
the efficacy of latanoprost (0.005%), bimatoprost (0.03%),
travoprost (0.004%), and timolol (0.5%) in the treatment of primary
open angle glaucoma. Korean J Ophthalmol. 28:399–407.
2014.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Setia MS: Methodology series module 3:
Cross-sectional studies. Indian J Dermatol. 61:261–264.
2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Yan DB, Battista RA, Haidich AB and
Konstas AG: Comparison of morning versus evening dosing and 24-h
post-dose efficacy of travoprost compared with latanoprost in
patients with open-angle glaucoma. Curr Med Res Opin. 24:3023–3027.
2008.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Fain JM, Kotak S, Mardekian J, Bacharach
J, Edward DP, Rauchman S, Brevetti T, Fox JL and Lovelace C: A
multicenter, retrospective chart review study comparing index
therapy change rates in open-angle glaucoma or ocular hypertension
patients newly treated with latanoprost or travoprost-Z
monotherapy. BMC Ophthalmol. 11(13)2011.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Rödter TH, Knippschild S, Baulig C and
Krummenauer F: Meta-analysis of the concordance of
Icare® PRO-based rebound and Goldmann applanation
tonometry in glaucoma patients. Eur J Ophthalmol. 30:245–252.
2020.PubMed/NCBI View Article : Google Scholar
|