Introduction
Heart failure (HF) is a clinical syndrome associated
with poor quality of life, substantial health-care resource
utilization and premature mortality (1). Despite the fact that the division of
HF with preserved ejection fraction (HFpEF) varies depending on the
cut-off point of the left ventricular ejection fraction (LVEF)
used, previous studies have reported that HFpEF accounted for ~50%
of patients with HF (2). Unlike HF
with reduced EF (HFrEF), HFpEF is characterized by heterogenetic
pathophysiology processes and various co-morbidities (3).
Hyponatremia, defined as a serum sodium levels of
<135 mmol/l, is one of the major electrolyte disorders in acute
hospitalized patients (4), and its
prevalence in patients with acute HF (AHF) was estimated to be ≤25%
(5-7).
HF involves fluid retention in the body and diuretics are normally
used to induce a negative balance of sodium in patients with HF,
and all of this may lead to hyponatremia. A lower serum sodium
level in AHF may indicate poor water excretion attributed to
cardio-renal insufficiency, which is linked to a worse clinical
outcome. Previous studies have revealed that hyponatremia is an
independent predictor of mortality and re-hospitalization for
patients with HFrEF (7,8) and has been demonstrated in HFpEF
populations (9,10). However, there is limited data on the
burden of hyponatremia and its complications in patients with HFpEF
in China and any other Asian countries.
To the best of our knowledge, the prevalence and
factors associated with hyponatremia among patients with HFpEF have
not been studied in China or other Asian countries. Therefore, the
aim of the present study was to examine the clinical
characteristics of subjects with hyponatremia via a prospective
observational study with a cohort of patients with HFpEF and
examine the prognostic value regarding adverse outcomes.
Materials and methods
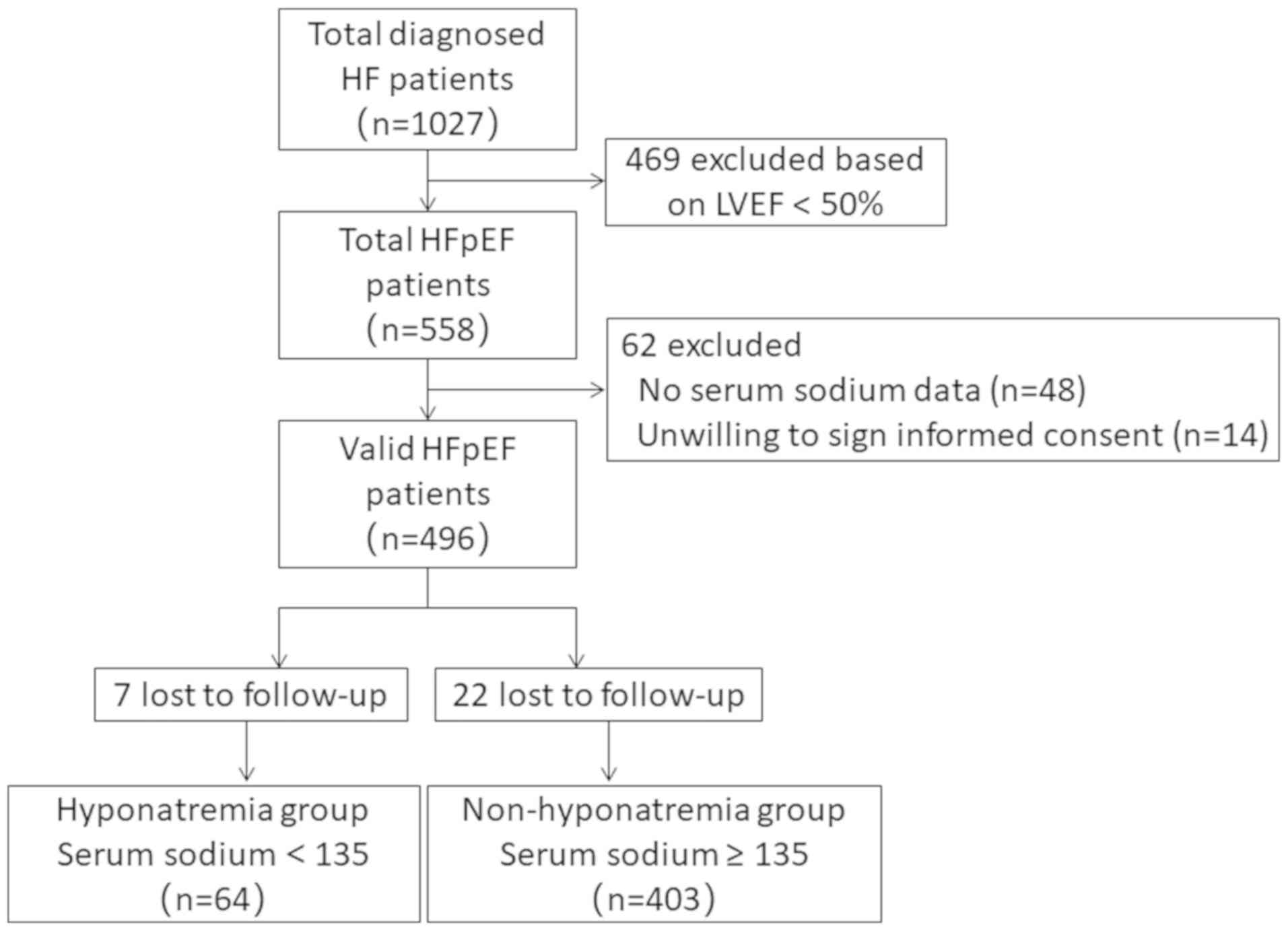
Study population
In the present prospective observational study,
consecutive symptomatic patients with HF hospitalized for the
treatment of decompensated HFpEF from Shanghai 10th People's
Hospital, Tongji University School of Medicine (Shanghai, China)
between July 2017 and December 2018 were enrolled. The study
protocol was approved by the Ethics Committee of Shanghai 10th
People's Hospital (Shanghai, China). Written informed consent for
medical treatment was provided by each patient on admission. The
present study was based on a previously registered clinical trial
(NCT04062500). Symptomatic HFpEF was defined based on the
Framingham criteria (11) and a
left ventricular ejection fraction (LVEF) of >50%. In line with
previous studies, patients were ≥18 years of age and met the
Framingham criteria for the diagnosis of HF (presence of either two
major criteria or combination of one major criterion and two minor
criteria). Patients with severe liver disease, trauma, infection
and recent surgery were excluded. A flow diagram depicting the
movement of the patients throughout the study is presented in
Fig. 1.
Blood samples and echocardiography were obtained
within 24 h of hospitalization of admission before any treatment
was given. Echocardiographic parameters were measured by
experienced echocardiographic cardiologists according to the
recommendations of the American Society of Echocardiography
(12). The left atrial diameter,
measured as the diameter from the anterior to the posterior side of
the left atrium, the left ventricular end-systolic diameter and the
left ventricular end-diastolic diameter were determined in the
parasternal long-axis view. The left ventricular ejection fraction
was calculated using a biplane methods of disc (modified Simpson's
rule) in four-chamber view (13).
The patients' medical history and current medical
treatment of angiotensin-converting enzyme inhibitors (ACEI),
angiotensin receptor blocker, β-blockers, aldosterone antagonists,
loop diuretics, antiplatelet agents, oral anticoagulants and
calcium channel blockers were collected. Cardiac function was
evaluated using the New York Heart Association (NYHA)
classification (1).
Data preparation and outcome
measures
Patients were categorized depending on their level
of sodium on first admission to the center. Each patient was
assigned to either the hyponatremia group if serum sodium was
<135 mmol/l or the non-hyponatremia group if sodium was ≥135
mmol/l. The follow-up period of the patients was 24 months.
Clinical events, including all-cause mortality, re-hospitalization
for HF and stroke, were recorded via telephone enquiry and
searching of the patients' electronic medical records. The
prognostic value of hyponatremia for the outcomes of patients with
HFpEF was investigated.
Statistical analysis
Continuous, normally distributed variables are
presented as the mean ± standard deviation and non-normally
distributed data as the median (interquartile range). Data were
compared using the independent-samples Student's t-test or by
one-way analysis of variance and the Mann-Whitney U-test, as
appropriate. Categorical data are presented as n (%) and compared
using Pearson's χ2-test.
Univariate logistic regression analysis was used to
assess the influence of relevant variables on hyponatremia that
were derived from a comparison of baseline characteristics and
published literature (14). In
addition, multivariate logistic regression analysis was performed
to determine whether they have a significant influence on the
outcomes. Cumulative survival rates were calculated according to
the Kaplan-Meier method with the log-rank test used for comparison
between hyponatremia and non-hyponatremia groups, setting
statistical power by assuming an event rate of 0.3 for all-cause
mortality, re-hospitalization for HF and stroke.
Cox-proportional hazards models were used to
calculate the hazard ratio (HR) with corresponding 95% CI for
occurrence of the primary study end-points (all-cause mortality,
re-hospitalization for HF and stroke) associated with each pattern
of hyponatremia development. All-cause mortality was adjusted by
age, sex, body mass index (BMI), systolic blood pressure (SBP),
hyponatremia, N-terminal pro B-type natriuretic peptide
(NT-proBNP), NYHA class, atrial fibrillation history, estimated
glomerular filtration rate (eGFR) and hemoglobin.
Re-hospitalization for HF was adjusted by age, sex, BMI, SBP,
hyponatremia, NT-proBNP, NYHA class, atrial fibrillation history,
eGFR and hemoglobin. Furthermore, stroke was adjusted by age, sex,
SBP, hyponatremia, D-dimer, atrial fibrillation history,
anti-platelet use and statin use.
P<0.05 was considered to indicate statistical
significance. All statistical analyses were performed using SPSS
v.25 (IBM Corp.).
Results
Baseline clinical characteristics of
patients with HFpEF
In total, 496 patients with HFpEF (mean age,
72.8±11.6 years; 53.0% males) were included and the mean serum
sodium level was 140.1±4.7 mmol/l. Patients with hyponatremia had a
mean sodium level of 131.1±3.6 mmol/l. Baseline characteristics of
patients with HFpEF are presented in Table I. The hyponatremia group had a
significantly lower blood pressure (SBP, 112.1±13.1 vs. 137.1±22.5
mmHg, P<0.001; diastolic blood pressure (DBP), 67.7±11.6 vs.
76.9±12.4 mmHg, P=0.002) and hemoglobin levels (113.4±14.4 vs.
123.2±22.1 g/l, P<0.001) but higher NT-proBNP [1,168.0
(586.1-3,000.0) vs. 1,046.0 (525.8-2,380.5), P<0.001] and
D-dimer levels [0.78 (0.48-1.43) vs. 0.47 (0.27-0.90), P<0.001].
Furthermore, the hyponatremia group contained a larger proportion
of patients with a history of atrial fibrillation (49.3 vs. 28.9%,
P<0.001). The proportion of patients taking aldosterone
antagonists and loop diuretics was higher in the hyponatremia group
(59.2 vs. 33.4%, P<0.001; 66.2 vs. 40.2%, P<0.001,
respectively). Furthermore, there were no differences in age, sex,
percentage of NYHA III-IV, eGFR, lipid profile, blood glucose,
echocardiographic parameters and other medications that the
patients were taking.
 | Table IBaseline clinical characteristics of
patients with heart failure with preserved ejection fraction based
on serum sodium status. |
Table I
Baseline clinical characteristics of
patients with heart failure with preserved ejection fraction based
on serum sodium status.
| | Serum sodium
concentration (mmol/l) | |
|---|
| Item | Normal range | <135 (n=71) | ≥135 (n=425) | P-value |
|---|
| Age (years) | - | 73.9±11.8 | 72.6±11.6 | 0.381 |
| Male sex | - | 31 (43.7) | 232 (54.6) | 0.104 |
| BMI
(kg/m2) | - | 24.1±3.80 | 23.9±4.16 | 0.342 |
| SBP (mmHg) | - | 112.1±13.1 | 137.1±22.5 | <0.001 |
| DBP (mmHg) | - | 67.7±11.6 | 76.9±12.4 | 0.002 |
| Heart rate
(beats/min) | - | 88.3±17.3 | 89.9±17.5 | 0.490 |
| NYHA class
III-IV | - | 65 (91.5) | 391 (92.0) | 0.761 |
| Medical history | | | | |
|
Diabetes | - | 24 (33.8) | 153 (36.0) | 0.790 |
|
Hypertension | - | 48 (67.6) | 292 (68.7) | 0.893 |
|
Coronary
artery disease | - | 43 (60.6) | 256 (60.2) | 1.000 |
|
Atrial
fibrillation | - | 35 (49.3) | 123 (28.9) | <0.001 |
| Laboratory
data | | | | |
|
Hemoglobin
(g/l) | 110-160 | 113.4±14.4 | 123.2±22.1 | <0.001 |
|
CRP
(mg/l) | 0-10 | 7.65
(3.02-18.0) | 3.23
(3.02-11.9) | 0.079 |
|
Alb
(g/l) | 35-50 | 38.3±5.60 | 39.7±4.81 | 0.082 |
|
UA
(µmol/l) | <420 | 371.6±73.5 | 383.1±62.7 | 0.523 |
|
eGFR
(ml/min/1.73 m2) | >90 | 69.9±23.9 | 67.1±23.5 | 0.357 |
|
TC
(mmol/l) | 2.8-5.2 | 3.75±1.04 | 3.78±1.14 | 0.831 |
|
LDL-C
(mmol/l) | <3.1 | 1.98±0.86 | 2.08±1.00 | 0.442 |
|
HDL-C
(mmol/l) | 0.8-1.8 | 1.09±0.39 | 1.14±0.65 | 0.698 |
|
Sodium
(mmol/l) | 135-145 | 131.1±3.6 | 141.6±2.8 | <0.001 |
|
Potassium
(mmol/l) | 3.5-5.5 | 4.19±0.53 | 3.98±0.54 | 0.980 |
|
HbA1C
(%) | 4-6 | 6.42±1.92 | 6.39±1.60 | 0.195 |
|
NT-proBNP
(ng/l) | 125 (<75 years)
450 (≥75 years) | 1,168.0
(586.1-3,000.0) | 1,046.0
(525.8-2,380.5) | <0.001 |
|
D-dimer
(mg/l) | <0.55 | 0.78
(0.48-1.43) | 0.47
(0.27-0.90) | <0.001 |
| Echocardiographic
parameters | | | | |
|
LVEF
(%) | - | 58.1±4.35 | 58.9±4.45 | 0.104 |
|
LAD
(mm) | - | 41.0±6.12 | 41.1±6.62 | 0.690 |
|
LVeDD
(mm) | - | 45.4±4.88 | 45.9±4.99 | 0.512 |
|
Levs
(mm) | - | 29.7±4.86 | 29.9±4.80 | 0.744 |
| Medications | | | | |
|
ACEI/ARB | - | 29 (40.8) | 170 (40.1) | 0.847 |
|
Beta-blocker | - | 48 (67.7) | 302 (71.1) | 0.059 |
|
Aldosterone
blocker | - | 42 (59.2) | 142 (33.4) | <0.001 |
|
Loop
diuretic | - | 47 (66.2) | 171 (40.2) | <0.001 |
|
Antiplatelet
agent | - | 55 (77.5) | 345 (81.2) | 0.519 |
|
Oral
anticoagulant | - | 26 (36.6) | 189 (44.5) | 0.248 |
|
Calcium
channel blocker | - | 22 (31.0) | 144 (33.9) | 0.692 |
| Cost (Yuan) | - |
31,140.1±30,503.2 |
32,583±64,318.6 | 0.771 |
Serum sodium distribution of patients
with HFpEF and logistic regression analysis for risk factors of
hyponatremia
The distribution of serum sodium levels was analyzed
in patients with HFpEF and the majority of patients was within the
interval of 141.5-142.4 mmol/l (n=56; Fig. S1).
Univariate logistic regression analyses identified
that hyponatremia was positively associated with NT-proBNP
>median [odds ratio (OR)=6.045, 95% CI=3.41-10.72], NYHA
classification III-IV (OR=2.994, 95% CI=1.714-5.057), atrial
fibrillation history (OR=2.100, 95% CI=1.233-3.577), loop diuretics
(OR=1.875, 95% CI=1.094-3.215) and spironolactone (OR=1.799, 95%
CI=1.058-3.058), but it was negatively associated with β-blockers
(OR=0.569, 95% CI=0.331-0.981),SBP (OR=0.946, 95% CI=0.930-0.962)
and DBP (OR=0.965, 95% CI=0.945-0.986). Multivariate logistic
regression analysis demonstrated that in patients with HFpEF, a
higher NT-proBNP (above median, OR=4.521, 95% CI=2.450-9.584) or
worse cardiac function (OR=2.275, 95% CI=1.207-4.338) were
positively associated with hyponatremia. In addition, a higher SBP
(OR=0.942, 95% CI 0.920-0.964) and β-blocker use (OR=0.343, 95%
CI=0.186-0.675) were negatively associated with hyponatremia
(Table II).
| Table IIUnivariate and multivariate logistic
regression analysis for the risk factors of hyponatremia. |
Table II
Univariate and multivariate logistic
regression analysis for the risk factors of hyponatremia.
| | Univariate logistic
regression | Multivariate
logistic regression |
|---|
| Variable | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| SBP | 0.946 | 0.930-0.962 | <0.001 | 0.942 | 0.920-0.964 | <0.001 |
| NYHA III-IV | 2.994 | 1.714-5.057 | <0.001 | 2.275 | 1.207-4.338 | 0.013 |
| Atrial fibrillation
history | 2.100 | 1.233-3.577 | 0.006 | 1.831 | 0.963-3.325 | 0.057 |
| Beta-blocker | 0.569 | 0.331-0.981 | 0.043 | 0.343 | 0.186-0.675 | 0.002 |
| Loop diuretic | 1.875 | 1.094-3.215 | 0.022 | 1.003 | 0.476-2.235 | 0.985 |
| Spironolactone | 1.799 | 1.058-3.058 | 0.030 | 0.907 | 0.422-2.062 | 0.840 |
| NT-proBNP
>mediana | 6.045 | 3.41-10.72 | <0.001 | 4.521 | 2.450-9.584 | 0.001 |
Clinical outcomes of patients with
HFpEF
In total, 29 (6%) patients were lost to follow-up,
mortality occurred in 71 (15.2%) cases in the first 24 months, 129
(27.6%) patients were re-hospitalized for HF and 77 (16.5%)
patients had a stroke. Furthermore, the hyponatremia group had a
worse prognosis compared with the non-hyponatremia group. All-cause
mortality was 39.1% in the hyponatremia group compared with 11.4%
in the non-hyponatremia group (P<0.001). In the hyponatremia
group, 40.6% of patients were re-hospitalized for HF, as compared
with 25.6% in the non-hyponatremia group (P=0.016). Furthermore,
the prevalence of stroke was 28.1% in the hyponatremia group as
compared with 14.6% in the non-hyponatremia group (P=0.011;
Table III).
| Table IIIOutcomes of patients with HF with
preserved ejection fraction based on serum sodium status. |
Table III
Outcomes of patients with HF with
preserved ejection fraction based on serum sodium status.
| | Serum sodium
concentration (mmol/l) | |
|---|
| Variable | All patients | <135 (n=64) | ≥135 (n=403) | P-value |
|---|
| All-cause
mortality | 71 (15.2) | 25 (39.1) | 46 (11.4) | <0.001 |
| Re-hospitalization
for HF | 129 (27.6) | 26 (40.6) | 103 (25.6) | 0.016 |
| Stroke | 77 (16.5) | 18 (28.1) | 59 (14.6) | 0.011 |
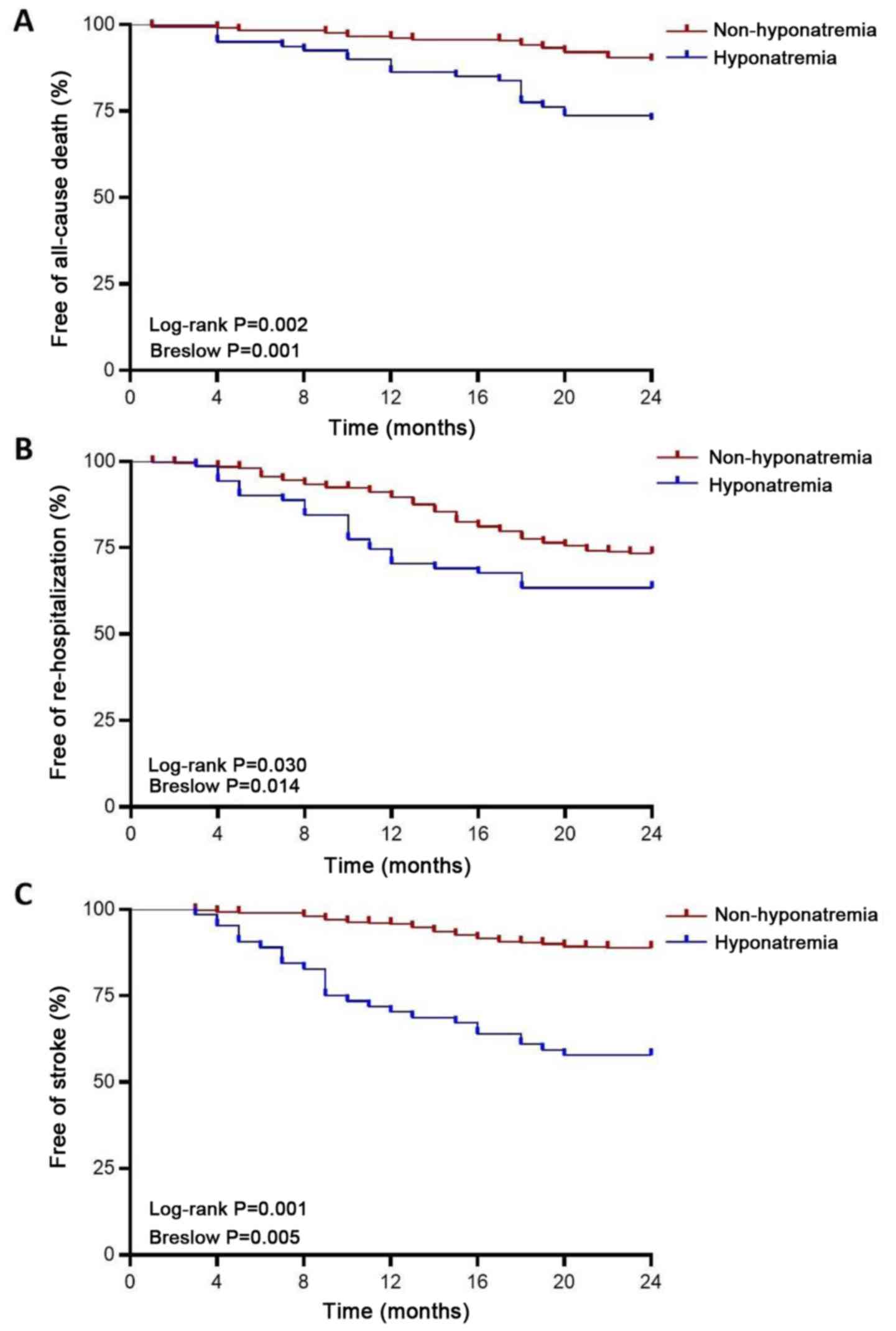
Survival analysis
The median duration of the follow up of the study
participants was 24 months. The number of mortalities in the
hyponatremia group was 25 (39.1% of patients) compared with 46 in
the non-hyponatremia group (11.4% of patients). Kaplan-Meier
survival curves (Fig. 2) indicated
that there were significant differences in survival status,
re-hospitalization and stroke between the two groups of patients
with HFpEF. In addition, patients with sodium levels ≥135 mmol/l
had an improved prognosis compared with patients with
hyponatremia.
In order to investigate the predictors of adverse
events in patients with HFpEF, a multivariate Cox proportion hazard
regression model was established for all-cause mortality,
re-hospitalization and stroke (Fig.
3). It was indicated that hyponatremia was an independent
predictor for three adverse events in patients with HFpEF
(all-cause mortality: Adjusted HR=1.54, 95% CI=1.07-2.91, P=0.034;
re-hospitalization: Adjusted HR=1.28, 95% CI=1.16-2.47, P=0.013;
stroke: Adjusted HR=1.78, 95% CI=1.04-2.89, P=0.016). Another
independent predictor for all-cause mortality was older age
(adjusted HR=1.07, 95% CI=1.05-1.09, P<0.001). Furthermore,
lower SBP (adjusted HR=0.97, 95% CI=0.97-0.98, P<0.001),
NT-proBNP >median (adjusted HR=1.62, 95% CI=1.05-3.03, P=0.027),
NYHA III-IV (adjusted HR=1.73, 95% CI=1.07-2.81, P=0.021), AF
history (adjusted HR=2.69, 95% CI=1.32-3.58, P<0.001) and
eGFR<60 ml/min/1.73 m2 (adjusted HR=0.51, 95%
CI=0.28-0.91, P=0.024) were significantly associated with all-cause
mortality. Other independent predictors for re-hospitalization were
older age (adjusted HR=1.04, 95% CI=1.02-1.07, P=0.008), lower SBP
(adjusted HR=0.96, 95% CI=0.95-0.99, P=0.001), NT-proBNP >median
(adjusted HR=1.24, 95% CI=1.03-2.08, P=0.042), NYHA III-IV
(adjusted HR=2.15, 95% CI=2.02-2.46, P=0.001) and additional AF
history (adjusted HR=1.48, 95% CI=1.05-2.20, P=0.003). In addition,
other independent predictors for stroke were lower SBP (HR=0.99,
95% CI=0.98-0.99, P=0.042), higher D-dimer levels (HR=1.96, 95%
CI=1.30-2.59, P=0.025) and atrial fibrillation history (HR=1.34,
95% CI=1.15-2.47, P=0.018).
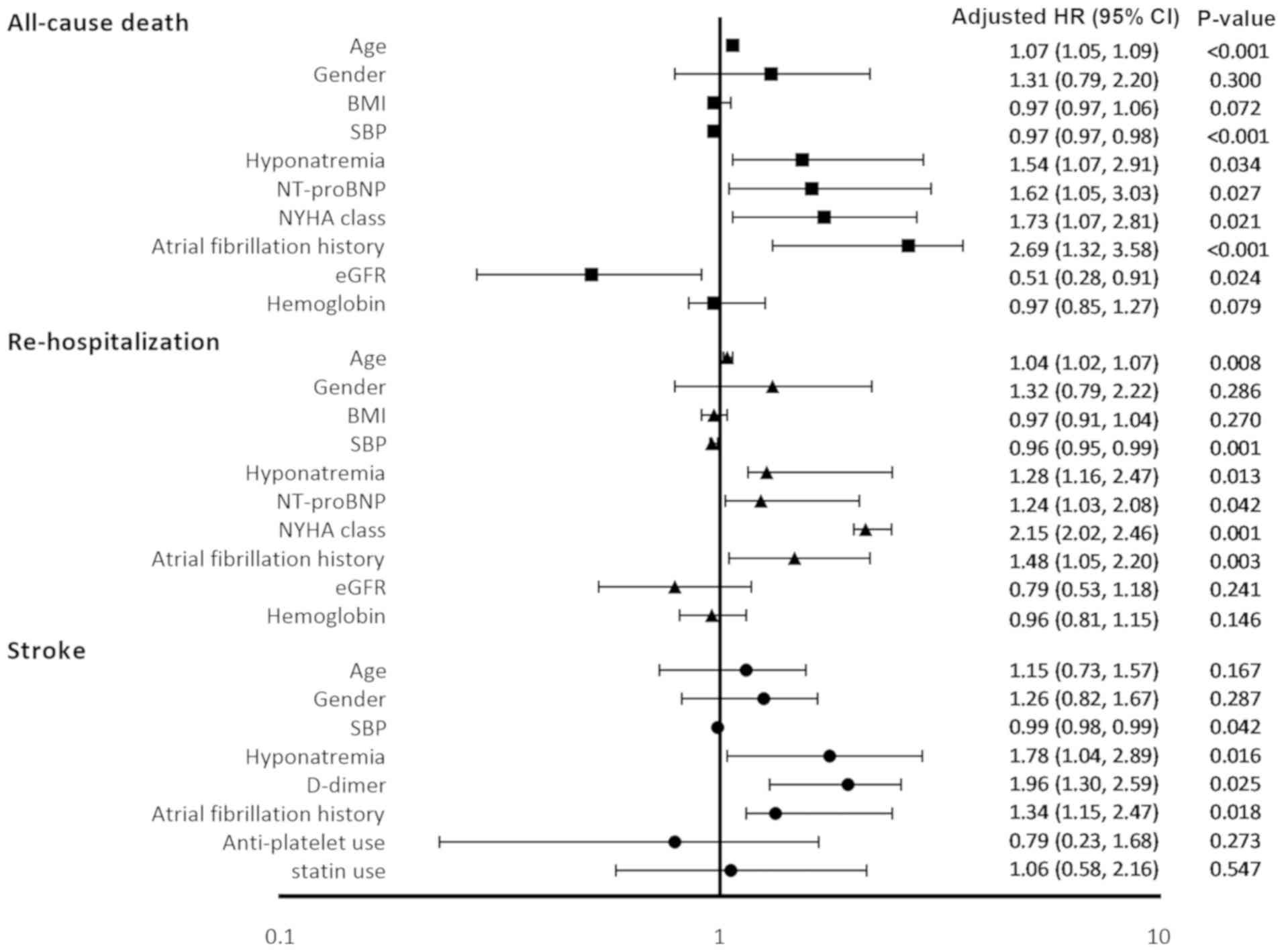 | Figure 3Predictors of all-cause mortality,
re-hospitalization and stroke in patients with HFpEF. Logistic
regression analysis with the Cox proportional hazard model was
performed for the three endpoint events. Univariate analysis was
applied prior to the multivariate analysis (data not shown).
According to the results of the multivariate analysis,
hyponatremia, older age, lower SBP, NT-proBNP above the median,
NYHA class III-IV, a history of AF and eGFR<60 ml/min/1.73
m2 predicted higher all-cause mortality, after
adjustment for sex, BMI and hemoglobin. Furthermore, hyponatremia
predicted a higher re-hospitalization rate and a higher incidence
of stroke. HR, hazard ratio; HFpEF, heart failure with preserved
ejection fraction; AF, atrial fibrillation; BMI, body mass index;
NT-proBNP, N-terminal pro B-type natriuretic peptide; NYHA, New
York Heart Association; eGFR, estimated glomerular filtration rate;
SBP, systolic blood pressure. |
Discussion
In the present observational study, it was indicated
that hyponatremia was associated with higher all-cause mortality
and re-hospitalization for HF in a cohort of patients with HFpEF;
these results were consistent with those of previous studies
(14-16).
Furthermore, patients with HFpEF with hyponatremia had lower blood
pressure, higher serum levels of NT-proBNP and D-dimer, serious
anemia and atrial fibrillation, as well as higher rate of
medication used, such as spironolactone and loop diuretics, which
suggested that the disease in those patients was more serious and
should be actively treated. To the best of our knowledge, the
present study was the first to demonstrate that hyponatremia was an
independent predictor of the incidence of stroke in a patient
population with HFpEF.
HFpEF is an increasingly prevalent phenotype of HF.
Unlike those for HFrEF, the diagnosis and treatment of HFpEF are
not well-standardized, rendering numerous patients with HFpEF
misdiagnosed or underdiagnosed. In this situation, the disease may
further progress due to poor appetite and low-sodium diet
(insufficient intake), and a high dose of diuretic agents
(excessive loss), leading to electrolyte disorders, particularly
hyponatremia (16).
Hyponatremia is the most common electrolyte disorder
(17) and is frequently encountered
in patients with HF. It may either arise from depletion (excessive
sodium depletion), which is caused by extensive administration of
diuretics as aforementioned, or dilution, which is caused by
impaired glomerular filtration. Therefore, dilutional hyponatremia
in patients with HF with impaired renal function likely results in
volume overload, which deteriorates the condition and subsequently
leads to a worse prognosis (16).
Thus, hyponatremia is an adverse marker of a significant underlying
disease and may enhance the severity and complexity of HF. The
present results suggested a high incidence of hyponatremia of 14.3%
in hospitalized patients with HF, which is comparable to that
reported by other studies on acute decompensated HF (7,18,19).
The causes of hyponatremia are miscellaneous, as the
present results suggested that a higher NYHA class and NT-proBNP
levels increase the risk, while usage of
renin-angiotensin-aldosterone system (RAAS) inhibitor and
β-blockers reduce the risk. On one hand, it has been reported that
NYHA class and NT-proBNP correlate with the severity of HF
(14). While patients with severe
HF require a large dosage of diuretics, this will lead to
disturbance of homeostasis and pose a higher risk for hyponatremia.
The present results support this concept and are consistent with
those of previous studies (20).
One the other hand, dilutional hyponatremia resulting from
concomitant activation of the RAAS and sympathetic nervous system
may be counteracted by the use of RAAS inhibitor or β-blockers
(21,22). This is also in line with the present
results.
Previous studies have reported that hyponatremia was
associated with worse short-term, mid-term and long-term outcomes
(1,19,23).
In the OPTIMIZE-HF (24) and
OPTIME-CHF (19) trials, following
a drop in serum sodium levels (per 3 mmol/l decrease from 140
mmol/l), the OR of in-hospital mortality, 60-day mortality and
60-90 day mortality was 1.25, 1.18 and 1.10, respectively. In the
present study, all-cause mortality was 13.9% in patients with
HFpEF, which is lower than the rates obtained in other trials
(OPTIME-CHF, 27%; ACTIV-in-CHF, 21%) (5,19).
Furthermore, hyponatremia was associated with a 2-fold increased
risk of 24-month all-cause mortality. Hence, hyponatremia is a
valuable predictor of prognosis in patients with HF.
A number of factors contribute to the poor outcomes
in patients with HFpEF with hyponatremia. For instance, HF
progression is closely linked to the activation of the
neuroendocrine system, which is classically represented by the
RAAS. Furthermore, hyponatremia may directly upregulate the
activity of RAAS and arginine vasopressin (AVP), which increase the
heart rate, vessel constriction and renal urine reabsorption.
However, excessive activation of the neuroendocrine system may
result in adverse effects, including increased cardiac afterload
and myocardial oxygen consumption, cardiac cell death and
myocardial fibrosis (25). However,
the amount of BNP secreted into the circulation of patients with
exacerbation inhibits the release of aldosterone to facilitate
natriuresis (26,27).
To the best of our knowledge, the present study was
the first to demonstrate that hyponatremia (OR=1.78, 95% CI=1.04,
2.89, P=0.016) was a stronger predictor of stroke in patients with
HFpEF. Furthermore, a previous study reported that hyponatremia was
associated with stroke (28).
Aberrant serum sodium levels are also considered as a complication
of cerebrovascular disease (29),
and the possible mechanisms are associated with inappropriate
secretion of antidiuretic hormone, frequent use of diuretics, as
well as blood concentration and viscosity (30).
Since hyponatremia is independently associated with
poor outcomes, correcting hyponatremia in a timely and appropriate
manner may improve the prognosis of patients with HFpEF. There are
different treatment options, the first of which includes a daily
fluid allowance of 800-100 ml. As another option, the addition of
furosemide with an ACEI is able to significantly improve the sodium
concentration. In addition, arginine vasopressin (AVP) receptor
antagonists, which have a central role in regulating water
retention via these receptors, may be used. It has been revealed
that anemia, NT-proBNP and NYHA cardiac function not only have an
impact on the risk of mortality, but also on the incidence of
hyponatremia (14,31), which should be corrected as soon as
possible.
The present study had several limitations. First, it
was designed as an observational study and was potentially open to
selection bias, as patients with severe liver disease, trauma,
infection and recent surgery were excluded. Furthermore, the
etiology of hyponatremia was not surveyed in the patients. The
present study did not differentiate true hyponatremia from
pseudo-hyponatremia and did not analyze depletion and dilution
hyponatremia, but the prognosis and treatment were different
between them (32). In addition,
tolvaptan and AVP receptor antagonists were not widely used in the
current cohort and these should be further examined to assess their
effect on patients with HFpEF. Due to potential recall bias when
performing the subgroup analysis, the present study did not avoid
the influence of the history of atrial fibrillation on the
incidence of stroke.
In conclusion, the present results indicated that
hyponatremia on admission may be a useful prognostic marker for
patients with HFpEF. However, larger studies are required to be
performed to confirm these results, as well as to elucidate the
mechanisms of mortality and stroke associated with hyponatremia and
identify the potential benefit of correction of hyponatremia in
patients with HFpEF.
Supplementary Material
Frequency distribution of serum sodium
levels within the cohort.
Acknowledgements
Not applicable.
Funding
This work was supported by a grant from the National
Nature Science Foundation of China (grant no. 81270194).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
Conception and design: YS, YL, CY. Clinical support
and acquisition of data: YS, YL, CY. Provision of study materials
or patients: YS, YL. Collection and collation of data: YS, MM, HZ,
XP, XZ and FZ. Data analysis and interpretation: YS, YL. Manuscript
writing: YS, MM, HZ, YL, CY. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The study protocol was approved by the Research
Ethical Committee of Shanghai 10th People's Hospital of Tongji
University School of Medicine (Shanghai, China) and conducted
according to the principles expressed in the Declaration of
Helsinki. The data were retrieved from the hospital's medical
record system and therefore, no additional informed consent was
required. The institutional review board also waived the need for
written informed consent from the participants. The privacy of
patients' personal data was protected.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ponikowski P, Voors AA, Anker SD, Bueno H,
Cleland JG, Coats AJ, Falk V, González-Juanatey JR, Harjola VP,
Jankowska EA, et al: 2016 ESC guidelines for the diagnosis and
treatment of acute and chronic heart failure: The task force for
the diagnosis and treatment of acute and chronic heart failure of
the European society of cardiology (ESC). Developed with the
special contribution of the heart failure association (HFA) of the
ESC. Eur J Heart Fail. 18:891–975. 2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Dunlay SM, Roger VL and Redfield MM:
Epidemiology of heart failure with preserved ejection fraction. Nat
Rev Cardiol. 14:591–602. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ge J: Coding proposal on phenotyping heart
failure with preserved ejection fraction: A practical tool for
facilitating etiology-oriented therapy. Cardiol J. 27:97–98.
2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mohan S, Gu S, Parikh A and Radhakrishnan
J: Prevalence of hyponatremia and association with mortality:
Results from NHANES. Am J Med. 126:1127–1137.e1. 2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Rossi J, Bayram M, Udelson JE, Lloyd-Jones
D, Adams KF, Oconnor CM, Stough WG, Ouyang J, Shin DD, Orlandi C
and Gheorghiade M: Improvement in hyponatremia during
hospitalization for worsening heart failure is associated with
improved outcomes: Insights from the acute and chronic therapeutic
impact of a vasopressin antagonist in chronic heart failure (ACTIV
in CHF) trial. Acute Card Care. 9:82–86. 2007.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Gheorghiade M, Abraham WT, Albert NM,
Gattis Stough W, Greenberg BH, O'Connor CM, She L, Yancy CW, Young
J and Fonarow GC: OPTIMIZE-HF Investigators and Coordinators.
Relationship between admission serum sodium concentration and
clinical outcomes in patients hospitalized for heart failure: An
analysis from the OPTIMIZE-HF registry. Eur Heart J. 28:980–988.
2007.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Gheorghiade M, Rossi JS, Cotts W, Shin DD,
Hellkamp AS, Piña IL, Fonarow GC, DeMarco T, Pauly DF, Rogers J, et
al: Characterization and prognostic value of persistent
hyponatremia in patients with severe heart failure in the ESCAPE
Trial. Arch Intern Med. 167:1998–2005. 2007.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Lu DY, Cheng HM, Cheng YL, Hsu PF, Huang
WM, Guo CY, Yu WC, Chen CH and Sung SH: Hyponatremia and worsening
sodium levels are associated with long-term outcome in patients
hospitalized for acute heart failure. J Am Heart Assoc.
5(e002668)2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Patel YR, Kurgansky KE, Imran TF, Orkaby
AR, McLean RR, Ho YL, Cho K, Gaziano JM, Djousse L, Gagnon DR and
Joseph J: Prognostic significance of baseline serum sodium in heart
failure with preserved ejection fraction. J Am Heart Assoc.
7(e007529)2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Park JJ, Cho YJ, Oh IY, Park HA, Lee HY,
Kim KH, Yoo BS, Kang SM, Baek SH, Jeon ES, et al: Short and
long-term prognostic value of hyponatremia in heart failure with
preserved ejection fraction versus reduced ejection fraction: An
analysis of the Korean acute heart failure registry. Int J Cardiol.
248:239–245. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
McKee PA, Castelli WP, McNamara PM and
Kannel WB: The natural history of congestive heart failure: The
Framingham study. N Engl J Med. 285:1441–1446. 1971.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Lang RM, Badano LP, Mor-Avi V, Afilalo J,
Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA,
Kuznetsova T, et al: Recommendations for cardiac chamber
quantification by echocardiography in adults: An update from the
American society of echocardiography and the European association
of cardiovascular imaging. J Am Soc Echocardiogr. 28:1–39.e14.
2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Cabuk AK, Cabuk G, Sayin A, Karamanlioglu
M, Kilicaslan B, Ekmekci C, Solmaz H, Aslanturk OF and Ozdogan O:
Do we overestimate left ventricular ejection fraction by
two-dimensional echocardiography in patients with left bundle
branch block? Echocardiography. 35:148–152. 2018.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Bavishi C, Ather S, Bambhroliya A, Jneid
H, Virani SS, Bozkurt B and Deswal A: Prognostic significance of
hyponatremia among ambulatory patients with heart failure and
preserved and reduced ejection fractions. Am J Cardiol.
113:1834–1838. 2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kusaka H, Sugiyama S, Yamamoto E, Akiyama
E, Matsuzawa Y, Hirata Y, Fujisue K, Kurokawa H, Matsubara J,
Sugamura K, et al: Low-normal serum sodium and heart
failure-related events in patients with heart failure with
preserved left ventricular ejection fraction. Circ J. 80:411–417.
2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Rusinaru D, Buiciuc O, Leborgne L, Slama
M, Massy Z and Tribouilloy C: Relation of serum sodium level to
long-term outcome after a first hospitalization for heart failure
with preserved ejection fraction. Am J Cardiol. 103:405–410.
2009.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Upadhyay A, Jaber BL and Madias NE:
Incidence and prevalence of hyponatremia. Am J Med. 119 (7 Suppl
1):S30–S35. 2006.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Gheorghiade M, Gattis WA, O'Connor CM,
Adams KF Jr, Elkayam U, Barbagelata A, Ghali JK, Benza RL, McGrew
FA, Klapholz M, et al: Effects of tolvaptan, a vasopressin
antagonist, in patients hospitalized with worsening heart failure:
A randomized controlled trial. JAMA. 291:1963–1971. 2004.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Klein L, O'Connor CM, Leimberger JD,
Gattis-Stough W, Piña IL, Felker GM, Adams KF Jr, Califf RM and
Gheorghiade M: OPTIME-CHF Investigators. Lower serum sodium is
associated with increased short-term mortality in hospitalized
patients with worsening heart failure: Results from the outcomes of
a prospective trial of intravenous milrinone for exacerbations of
chronic heart failure (OPTIME-CHF) study. Circulation.
111:2454–2460. 2005.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Stolfo D, Uijl A, Vedin O, Strömberg A,
Faxén UL, Rosano GMC, Sinagra G, Dahlström U and Savarese G:
Sex-based differences in heart failure across the ejection fraction
spectrum: Phenotyping, and prognostic and therapeutic implications.
JACC Heart Fail. 7:505–515. 2019.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Baldasseroni S, Urso R, Orso F, Bianchini
BP, Carbonieri E, Cirò A, Gonzini L, Leonardi G, Marchionni N and
Maggioni AP: IN-CHF Investigators. Relation between serum sodium
levels and prognosis in outpatients with chronic heart failure:
Neutral effect of treatment with beta-blockers and
angiotensin-converting enzyme inhibitors: Data from the Italian
network on congestive heart failure (IN-CHF database). J Cardiovasc
Med (Hagerstown). 12:723–731. 2011.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Lee WH and Packer M: Prognostic importance
of serum sodium concentration and its modification by
converting-enzyme inhibition in patients with severe chronic heart
failure. Circulation. 73:257–267. 1986.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Yoo BS, Park JJ, Choi DJ, Kang SM, Hwang
JJ, Lin SJ, Wen MS, Zhang J and Ge J: COAST investigators.
Prognostic value of hyponatremia in heart failure patients: An
analysis of the clinical characteristics and outcomes in the
relation with serum sodium level in asian patients hospitalized for
heart failure (COAST) study. Korean J Intern Med. 30:460–470.
2015.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Abraham WT, Fonarow GC, Albert NM, Stough
WG, Gheorghiade M, Greenberg BH, O'Connor CM, Sun JL, Yancy CW and
Young JB: OPTIMIZE-HF Investigators and Coordinators. Predictors of
in-hospital mortality in patients hospitalized for heart failure:
Insights from the organized program to initiate lifesaving
treatment in hospitalized patients with heart failure
(OPTIMIZE-HF). J Am Coll Cardiol. 52:347–356. 2008.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Vergaro G, Aimo A, Prontera C, Ghionzoli
N, Arzilli C, Zyw L, Taddei C, Gabutti A, Poletti R, Giannoni A, et
al: Sympathetic and renin-angiotensin-aldosterone system activation
in heart failure with preserved, mid-range and reduced ejection
fraction. Int J Cardiol. 296:91–97. 2019.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Azim A and Jena S: BNP: Is it an ideal
marker to assess volume status in patients with hyponatremia and
natriuresis? Neurol India. 66:1392–1393. 2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Tobin G, Chacko AG and Simon R: Evaluation
of NT-ProBNP as a marker of the volume status of neurosurgical
patients developing hyponatremia and natriuresis: A pilot study.
Neurol India. 66:1383–1388. 2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Wannamethee G, Whincup PH, Shaper AG and
Lever AF: Serum sodium concentration and risk of stroke in
middle-aged males. J Hypertens. 12:971–979. 1994.PubMed/NCBI
|
|
29
|
Zheng B, Qiu Y, Jin H, Wang L, Chen X, Shi
C and Zhao S: A predictive value of hyponatremia for poor outcome
and cerebral infarction in high-grade aneurysmal subarachnoid
haemorrhage patients. J Neurol Neurosurg Psychiatry. 82:213–217.
2011.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Writing Group Members. Mozaffarian D,
Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de
Ferranti S, Després JP, et alHeart disease and stroke
statistics-2016 update: A report from the American heart
association. Circulation. 133:e38–e360. 2016.PubMed/NCBI View Article : Google Scholar
|
|
31
|
McGirt MJ, Blessing R, Nimjee SM, Friedman
AH, Alexander MJ, Laskowitz DT and Lynch JR: Correlation of serum
brain natriuretic peptide with hyponatremia and delayed ischemic
neurological deficits after subarachnoid hemorrhage. Neurosurgery.
54:1369–1373; discussion 1373-1364. 2004.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Verbrugge FH, Steels P, Grieten L, Nijst
P, Tang WH and Mullens W: Hyponatremia in acute decompensated heart
failure: Depletion versus dilution. J Am Coll Cardiol. 65:480–492.
2015.PubMed/NCBI View Article : Google Scholar
|