Introduction
The mucinous cystic neoplasms (MCNs) of the pancreas
are rare cystic tumors characterized by mucin production, presence
of ovarian-type stroma, and malignant potential (1). It almost exclusively presents in
middle-aged women and is located at the distal part of the pancreas
(2). Unlike its mucinous producing
counterpart intraductal papillary mucinous neoplasms (IPMNs), MCNs
have no communication with either the main pancreatic duct or
branch duct. Considering the possibility of malignant progression,
surgical resection is usually recommended to MCNs (3,4). The
prognosis of patients with invasive MCNs is much better than that
of patients with invasive IPMNs, with a 10-year disease-specific
survival of 79.6 vs. 27.2%, respectively (1).
Due to the invasive potential of MCNs, an accurate
evaluation of malignant change is needed for appropriate clinical
management (2). Variables including
male sex, pancreatic head and neck location, increased tumor size,
a solid component, and main pancreatic duct dilation have been
reported to be positively associated with malignant change
(5,6). Carbohydrate antigen 125 (CA125),
carbohydrate antigen 19-9 (CA19-9), and carcinoembryonic antigen
(CEA) are commonly used biomarkers for various types of cancers.
Serum CA19-9 and CEA have been recommended to the management of
pancreatic cyst diseases (4,7,8).
However, the value of circulating CA19-9 and CEA in predicting MCN
malignancy is limited. For example, a previous study showed that in
7 patients with pathologically confirmed severe dysplasia of
mucinous cystic pancreatic neoplasms, 3 (42.9%) patients had an
elevated circulating CA19-9 and 2 (28.6%) had an elevated
circulating CEA (9). The study
concluded that serum CA19-9 or CEA is not useful in screening
mucinous cystic pancreatic neoplasm patients with malignancy
(9). Although serum CA125 has been
used in the management of various types of mucinous malignancies,
its role in MCNs has not been identified.
In this study, by including 164 patients with
resected and a histologic diagnosis of MCN, the predictive role of
serum CA125 in assessing malignant change of MCNs was analyzed and
compared with serum CA19-9 and CEA. In addition, the values of
CA125 combined with serum CA19-9 or CEA in evaluating malignant
alteration were also examined.
Patients and methods
Patients and data collection
All patients who underwent surgical resection of
pancreatic MCN from May 2010 to November 2019 were identified from
a prospectively maintained database of Fudan University Shanghai
Cancer Center (Shanghai, China). All patients were pathologically
verified to the diagnosis of MCN of the pancreas. Other
pathological subtypes of pancreatic tumors including
adenocarcinoma, serous cystic neoplasm, solid pseudopapillary
tumor, and IPMN were excluded. Patients with previous or other
concomitant cancer were also excluded. Clinicopathologic
characteristics including age, sex, primary tumor location, cystic
size, serum levels of CA19-9, serum levels of CEA, serum levels of
CA125, and the operation type were collected. The recommended
cutoff points based on the upper limit of the normal range were
used (CA19-9, 37.0 U/ml; CA125, 35.0 U/ml; CEA, 5.2 ng/ml), as used
in previous studies (8,10,11).
This study was based on the ethical guidelines of the World Medical
Association Declaration of Helsinki and was approved by the Ethics
Committee of Fudan University Shanghai Cancer Center. All patients
provided informed consent for the use of their personal data for
research purposes.
Statistics
Variables were presented as median (range) or mean ±
standard deviation (SD), as appropriate. Comparisons of categorical
variables were conducted with ranksum tests or Fisher's exact
tests. Two-tailed t tests or ranksum test were used to compare
parametric data. The ROC curve and the area under the ROC curve
(AUC) were examined to determine the predictive value of
biomarkers. Statistical analyses were conducted using Stata SE12.0
(StataCorp LP) and Prism statistical software (version 8; GraphPad
Software, Inc.). P<0.05 was considered to indicate a
statistically significant difference.
Results
Baseline characteristics
The clinicopathologic characteristics of 164
patients with MCN are summarized in Table I. The female-to-male ratio was
11.6:1 and the median age was 48 years (range 18-82 years). Most of
(91.5%) the primary tumors were located at the body and tail of the
pancreas. All the patients underwent tumor resection and 86.6% of
patients received distal pancreatectomy. The mean cyst size in
diameter was 4.6 cm.
 | Table IBaseline characteristics. |
Table I
Baseline characteristics.
| Characteristics | Total (n=164) | Low/moderate grade
(n=153) | High grade and
invasive (n=11) | P-value |
|---|
| Age [median (range),
years] | 48 (18-82) | 48 (18-75) | 58 (28-82) | 0.384a |
| Sex | | | | 0.192 |
|
Female
(%) | 151 (92.1) | 142 (92.8) | 9 (81.8) | |
|
Male
(%) | 13 (7.9) | 11 (7.2) | 2 (18.2) | |
| Location | | | | 0.294 |
|
Head
(%) | 14 (8.5) | 14 (9.2) | 0 (0.0) | |
|
Body and
tail (%) | 150 (91.5) | 139 (90.8) | 11 (100.0) | |
| Operation type | | | | |
|
Distal
pancreatectomy | 142 (86.6) | 131 (85.6) | 11 (100.0) | 0.609b |
|
Enucleation | 9 (5.5) | 9 (5.9) | 0 (0.0) | |
|
Middle
segmental pancreatectomy | 2 (1.2) | 2 (1.3) | 0 (0.0) | |
|
Pancreatoduodenectomy | 11 (6.7) | 11 (7.2) | 0 (0.0) | |
| Cyst size (mean ± SD,
cm) | 4.6±2.9 | 4.5±2.8 | 6.5±3.0 | 0.017a |
Characteristics according to
malignancy
In this cohort, 6.7% (11/164) of patents were
diagnosed with malignant MCNs (high grade and invasive). The cystic
size in the high grade and invasive group (6.5±3.0 cm) was larger
than that in the low/moderate grade group (4.5±2.8 cm, P=0.017).
There was no statistical difference between the low/moderate grade
group and the high grade and invasive group in age (P=0.384), sex
(P=0.192), primary tumor location (P=0.294), and operation type
(P=0.609).
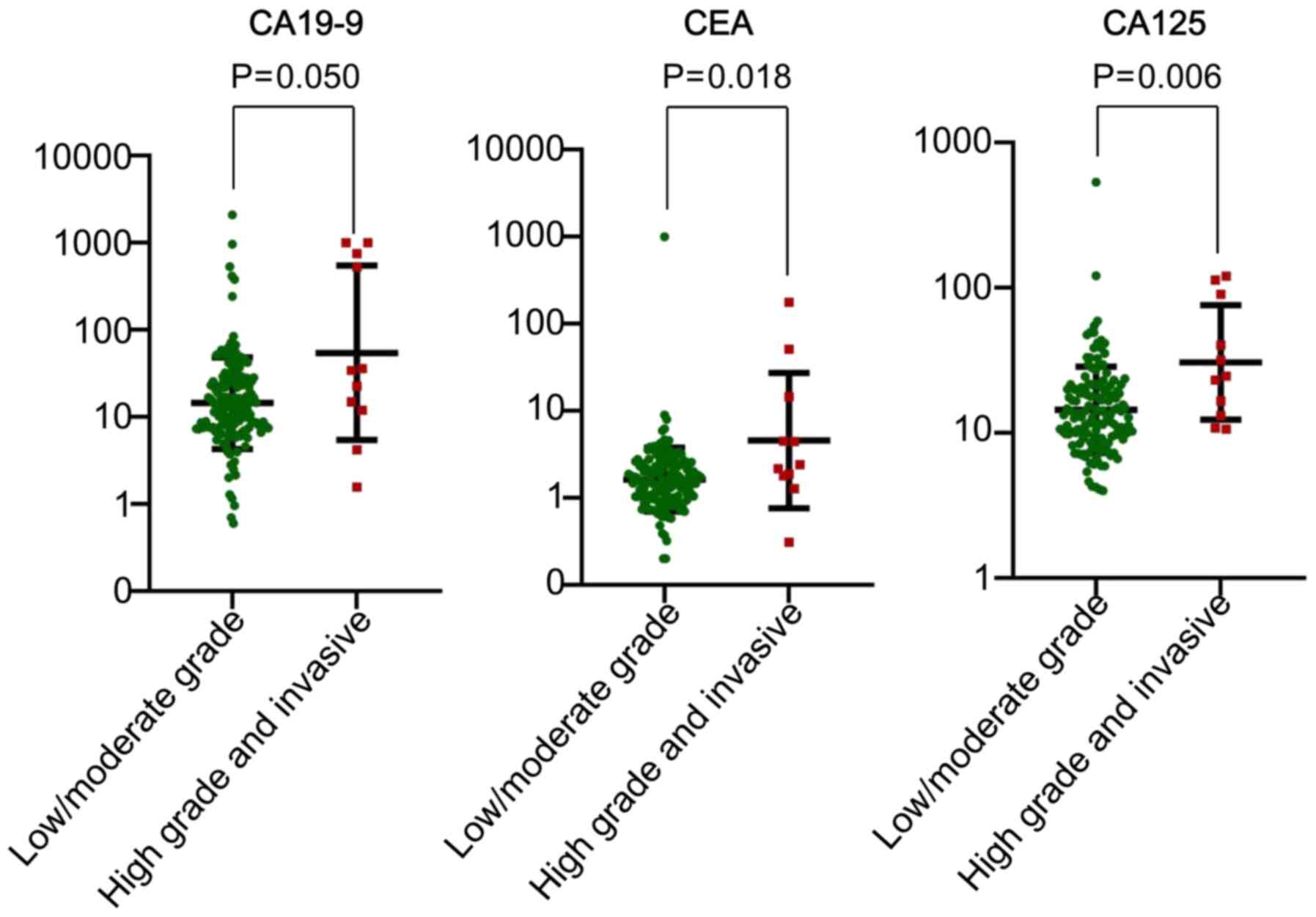
Tumor biomarker levels according to
histological grade of dysplasia
Serum levels of CA19-9, CEA, and CA125 in the
low/moderate grade group and the high grade and invasive group are
shown in Table II and Fig. 1. The serum levels of CA19-9
(309.2±423.2 vs. 49.0±198.3 U/ml, P=0.050), CEA (23.7±52.9 vs.
8.7±82.6 ng/ml, P=0.018), and CA125 (45.1±42.1 vs. 21.0±46.2 U/ml,
P=0.006) in the high grade and invasive group was significantly
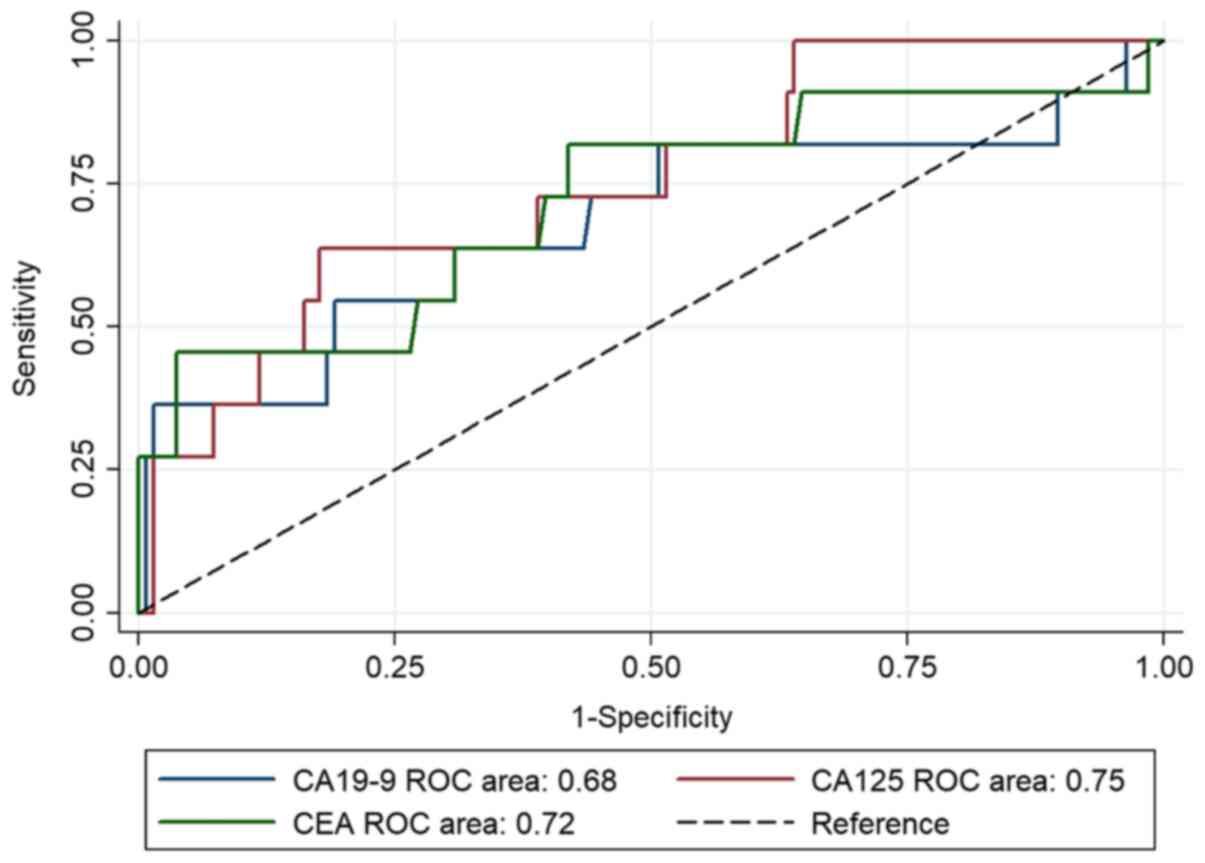
higher than those in the low/moderate grade group. The area under
the ROC curve of CA125 (0.75) for predicting malignancy of MCNs was
higher than that of CA19-9 (0.68) or CEA (0.72, Fig. 2).
| Table IITumor biomarker levels according to
the histological grade of dysplasia. |
Table II
Tumor biomarker levels according to
the histological grade of dysplasia.
| Biomarker | Total (n=164) | Low/moderate grade
(n=153) | High grade and
invasive (n=11) | P-value |
|---|
| CA19-9 (mean ± SD,
U/ml) | 67.0±228.7 | 49.0±198.3 | 309.2±423.2 | 0.050a |
|
<37
(%) | 128 (80.5) | 121 (81.8) | 7 (63.6) | |
|
≥37 (%) | 31 (19.5) | 27 (18.2) | 4 (36.4) | |
| CEA (mean ± SD,
ng/ml) | 9.8±80.9 | 8.7±82.6 | 23.7±52.9 | 0.018a |
|
<5.2
(%) | 149 (94.9) | 141 (96.6) | 8 (72.7) | |
|
≥5.2
(%) | 8 (5.1) | 5 (3.4) | 3 (27.3) | |
| CA125 (mean ± SD,
U/ml) | 22.8±46.2 | 21.0±46.2 | 45.1±42.1 | 0.006a |
|
<35
(%) | 132 (88.6) | 125 (90.6) | 7 (63.6) | |
|
≥35 (%) | 17 (11.4) | 13 (9.4) | 4 (36.4) | |
Combining serum biomarkers in
predicting malignancy of MCNs
The sensitivity and specificity of CA125 as a
biomarker in predicting malignancy of MCNs was 36.4% and 90.6%,
respectively, with an accuracy of 86.6% when using 35 U/ml as the
cut-off value (Table III). The
accuracy of CA125 in predicting malignancy of MCNs was higher than
CA19-9 (78.6%) and was comparable to CEA (91.7%) when using the
recommended cut-off values. The prediction value was improved when
combining CA125 with CEA (sensitivity 45.5%, specificity 88.2%,
accuracy 85.0%).
| Table IIIDiagnostic indices for CA19-9, CEA,
and CA125 in predicting the malignant alteration of MCN. |
Table III
Diagnostic indices for CA19-9, CEA,
and CA125 in predicting the malignant alteration of MCN.
| Valuea | CA19-9 | CEA | CA125 | CA19-9 and/or
CEA | CA19-9 and/or
CA125 | CA125 and/or
CEA |
|---|
| Sensitivity
(%) | 36.4 | 27.3 | 36.4 | 54.5 | 54.5 | 45.5 |
| Specificity
(%) | 81.8 | 96.6 | 90.6 | 78.8 | 75.2 | 88.2 |
| PPV (%) | 12.9 | 37.5 | 23.5 | 16.2 | 15.0 | 23.8 |
| NPV (%) | 94.5 | 94.6 | 94.7 | 95.8 | 95.4 | 95.2 |
| Accuracy (%) | 78.6 | 91.7 | 86.6 | 77.1 | 73.6 | 85.0 |
Discussion
The role of CA125 in predicting the malignant change
of MCNs is currently unknown. In this study, by including 164
patients with MCN (low/moderate grade, 153 cases; high grade and
invasive, 11 cases), the serum levels of CA125 in the high grade
and invasive group (45.1±42.1 U/ml) was significantly higher than
those in the low/moderate grade group (21.0±46.2 U/ml, P=0.006).
The area under the ROC curve of CA125 (0.75) for predicting
malignancy of MCNs was higher than that of CA19-9 (0.68) or CEA
(0.72). The predicting value of CA125 was improved when combined
with CEA (CA125 alone, sensitivity 36.4%, specificity 90.6%,
accuracy 86.6%; combined with CEA, sensitivity 45.5%, specificity
88.2%, accuracy 85.0%). These results indicate that CA125 could be
used to predict the malignant change of MCNs and the predictive
value is improved when combined with CEA.
CA125, also called MUC16, is a commonly used
biomarker for various types of malignancy, especially ovarian
tumors (12). The role of CA125 in
MCNs has been largely unconfirmed. Nagashio et al (13) collected cyst fluid from 68 patients
with pancreatic cystic diseases to determine the application of
cyst fluid analysis (CA125, CEA, CA19-9, amylase, and cytology) in
differentiating pancreatic cystic lesions. They showed that cyst
fluid CA125 concentrations may help to segregate MCNs (median,
1135.5 U/ml) from IPMNs (2 U/ml), serous cystic neoplasms (68.5
U/ml), and pseudocysts (6.5 U/ml), indicating the aberrant
secretion of CA125 in MCNs (13). A
multicentric retrospective study collected 347 patients with
pancreatic MCN and found that CEA, CA19-9, and CA125 were
remarkably different between the benign lesion group and the
malignant lesion group (P<0.05) (14). However, none of these studies
compared CA125 with CA19-9 or CEA. In this study, the area under
the ROC curve of CA125 (0.75) for predicting malignancy of MCNs was
higher than that of CA19-9 (0.68) or CEA (0.72), suggesting CA125
could be used to predict the malignant change of MCNs. Moreover,
the predicting value of CA125 was improved when combined with
CEA.
CA19-9, also termed as sialyl Lewis antigen a, is
the best-validated biomarker for pancreatic adenocarcinoma
(10,15). The biosynthesis of CA19-9 is
affected by the Lewis antigen status (15). Lewis antigen negative individuals,
accounting for 5-10% of the population, have no or low secretion of
CA19-9(15). CA19-9 has been
recommended to assess the malignant change of pancreatic cyst
tumors, including IPMNs and MCNs (3,5,7,16).
Postlewait et al retrospectively identified 349 patients
with MCN and demonstrated that patients with malignant neoplasms
had a higher serum CA19-9 level than those without (median, 210 vs.
15 U/ml, P=0.001) (5). Zhao et
al (17) showed that serum
CA19-9 levels were significantly higher in malignant MCNs than in
benign MCNs patients (P=0.026) for resected MCNs. Our study is
consistent with previous findings, which finds that the serum
levels of CA19-9 in the high grade and invasive group (309.2±423.2
U/ml) was significantly higher than those in the low/moderate grade
group (49.0±198.3 U/ml, P=0.050), with an area under the ROC curve
of 0.68.
CEA is a glycosylation biomarker which has been
widely applied in the management of gastrointestinal malignancies
(10). For pancreatic cyst tumors,
cyst fluid CEA have been used to differentiate mucinous tumors
(>192 ng/ml) from non-mucinous tumors (<5 ng/ml) (4,18).
Brugge et al (19) showed
cyst fluid CEA (optimal cut-off of 192 ng/ml, accuracy 79%) to be
more useful than endoscopic ultrasound morphology (accuracy 51%) or
cyst fluid cytology (accuracy 59%) for differentiating mucinous
from nonmucinous cystic lesions. However, cyst fluid CEA has
limited role in predicting malignancy or radiographic progression
mucinous cysts of the pancreas (18). Several studies have also determined
circulating CEA in predicting malignant MCNs (14,16,17).
For example, Zhao et al (17) demonstrated that serum CEA levels
were significantly higher in malignant MCNs than in benign MCNs
patients (P=0.005) for 82 patients with resected MCNs. In this
study, the serum levels of CEA in the high grade and invasive group
(23.7±52.9 ng/ml) was significantly higher than those in the
low/moderate grade group (8.7±82.6 ng/ml, P=0.018), with an area
under the ROC curve of 0.72. Our study confirms previous findings
that CEA could be used to predict malignant MCNs.
In summary, CA125 shows promising value in
predicting malignant MCNs. Its predictive value may be strengthened
by combining with CEA. However, further evidence, especially
evidence from multicentric, large sample size, and/or prospective
studies is needed to confirm the findings.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural
Science Foundation of China (grant nos. 81625016, 81871940 and
81902417), the Scientific Innovation Project of Shanghai Education
Committee (grant no. 2019-01-07-00-07-E00057), Clinical and
Scientific Innovation Project of Shanghai Hospital Development
Center (SHDC12018109), the Shanghai Natural Science Foundation
(grant no. 17ZR1406300), the Shanghai Cancer Center Foundation for
Distinguished Young Scholars (grant no. YJJQ201803), and the Fudan
University Personalized Project for ‘Double Top’ Original Research
(grant no. XM03190633).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
GL, CL, XY designed the study. SD, ZF, YG, HC, KJ,
YQ, ZX, YL, RW, YZ, QN, XY, CL and GL collected and analyzed data.
GL wrote the draft. XY and CL revised it critically. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The study protocol was approved by the ethics
committee of Fudan University Shanghai Cancer Center.
Patient consent for publication
Written informed consent was acquired from all of
the subjects enrolled.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Griffin JF, Page AJ, Samaha GJ,
Christopher A, Bhaijee F, Pezhouh MK, Peters NA, Hruban RH, He J,
Makary MA, et al: Patients with a resected pancreatic mucinous
cystic neoplasm have a better prognosis than patients with an
intraductal papillary mucinous neoplasm: A large single institution
series. Pancreatology. 17:490–496. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Nilsson LN, Keane MG, Shamali A, Millastre
Bocos J, Marijinissen van Zanten M, Antila A, Verdejo Gil C, Del
Chiaro M and Laukkarinen J: Nature and management of pancreatic
mucinous cystic neoplasm (MCN): A systematic review of the
literature. Pancreatology. 16:1028–1036. 2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tanaka M, Fernández-Del Castillo C,
Kamisawa T, Jang JY, Levy P, Ohtsuka T, Salvia R, Shimizu Y, Tada M
and Wolfgang CL: Revisions of international consensus Fukuoka
guidelines for the management of IPMN of the pancreas.
Pancreatology. 17:738–753. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Stark A, Donahue TR, Reber HA and Hines
OJ: Pancreatic cyst disease: A Review. JAMA. 315:1882–1893.
2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Postlewait LM, Ethun CG, McInnis MR,
Merchant N, Parikh A, Idrees K, Isom CA, Hawkins W, Fields RC,
Strand M, et al: Association of preoperative risk factors with
malignancy in pancreatic mucinous cystic neoplasms: a multicenter
study. JAMA Surg. 152:19–25. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Le Baleur Y, Couvelard A, Vullierme MP,
Sauvanet A, Hammel P, Rebours V, Maire F, Hentic O, Aubert A,
Ruszniewski P, et al: Mucinous cystic neoplasms of the pancreas:
Definition of preoperative imaging criteria for high-risk lesions.
Pancreatology. 11:495–499. 2011.PubMed/NCBI View Article : Google Scholar
|
|
7
|
European Study Group on Cystic Tumours of
the Pancreas. European evidence-based guidelines on pancreatic
cystic neoplasms. Gut. 67:789–804. 2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Fritz S, Hackert T, Hinz U, Hartwig W,
Büchler MW and Werner J: Role of serum carbohydrate antigen 19-9
and carcinoembryonic antigen in distinguishing between benign and
invasive intraductal papillary mucinous neoplasm of the pancreas.
Br J Surg. 98:104–110. 2011.PubMed/NCBI View
Article : Google Scholar
|
|
9
|
Pezzilli R, Calculli L, Melzi d'Eril G and
Barassi A: Serum tumor markers not useful in screening patients
with pancreatic mucinous cystic lesions associated with malignant
changes. Hepatobiliary Pancreat Dis Int. 15:553–557.
2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Luo G, Liu C, Guo M, Cheng H, Lu Y, Jin K,
Liu L, Long J, Xu J, Lu R, et al: Potential biomarkers in lewis
negative patients with pancreatic cancer. Ann Surg. 265:800–805.
2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Liu L, Xu H, Wang W, Wu C, Chen Y, Yang J,
Cen P, Xu J, Liu C, Long J, et al: A preoperative serum signature
of CEA+/CA125+/CA19-9 ≥1000 U/ml indicates poor outcome to
pancreatectomy for pancreatic cancer. Int J Cancer. 136:2216–2227.
2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Felder M, Kapur A, Gonzalez-Bosquet J,
Horibata S, Heintz J, Albrecht R, Fass L, Kaur J, Hu K, Shojaei H,
et al: MUC16 (CA125): Tumor biomarker to cancer therapy, a work in
progress. Mol Cancer. 13(129)2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Nagashio Y, Hijioka S, Mizuno N, Hara K,
Imaoka H, Bhatia V, Niwa Y, Tajika M, Tanaka T, Ishihara M, et al:
Combination of cyst fluid CEA and CA 125 is an accurate diagnostic
tool for differentiating mucinous cystic neoplasms from intraductal
papillary mucinous neoplasms. Pancreatology. 14:503–509.
2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Li WL, Xu YD, Han X, Wu WC and Lou WH:
Pancreatic Surgery of Chinese Academic Society of Young Surgeons.
Clinical analysis and prognosis factors of malignancy in the
patients with mucinous cystic neoplasms of the pancreas. Zhonghua
Wai Ke Za Zhi. 58:225–229. 2020.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
15
|
Luo G, Fan Z, Cheng H, Jin K, Guo M, Lu Y,
Yang C, Fan K, Huang Q, Long J, et al: New observations on the
utility of CA19-9 as a biomarker in Lewis negative patients with
pancreatic cancer. Pancreatology. 18:971–976. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Goh BK, Tan DM, Thng CH, Lee SY, Low AS,
Chan CY, Wong JS, Lee VT, Cheow PC, Chow PK, et al: Are the Sendai
and Fukuoka consensus guidelines for cystic mucinous neoplasms of
the pancreas useful in the initial triage of all suspected
pancreatic cystic neoplasms? A single-institution experience with
317 surgically-treated patients. Ann Surg Oncol. 21:1919–1926.
2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Zhao ZM, Jiang N, Gao YX, Yin ZZ, Zhao GD,
Tan XL, Xu Y and Liu R: Clinical diagnosis and management of
pancreatic mucinous cystadenoma and cystadenocarcinoma:
Single-center experience with 82 patients. World J Gastrointest
Oncol. 12:642–650. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Nagula S, Kennedy T, Schattner MA, Brennan
MF, Gerdes H, Markowitz AJ, Tang L and Allen PJ: Evaluation of cyst
fluid CEA analysis in the diagnosis of mucinous cysts of the
pancreas. J Gastrointest Surg. 14:1997–2003. 2010.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Brugge WR, Lewandrowski K,
Lee-Lewandrowski E, Centeno BA, Szydlo T, Regan S, del Castillo CF
and Warshaw AL: Diagnosis of pancreatic cystic neoplasms: A report
of the cooperative pancreatic cyst study. Gastroenterology.
126:1330–1336. 2004.PubMed/NCBI View Article : Google Scholar
|