Introduction
Urinary stones are a significant health problem
affecting ~12% of the population in North America, 5-9% in Europe
and 1-5% in Asia (1). Analysis of
global trends indicates that due to climate change, obesity and
dietary modifications, the worldwide prevalence of urinary stones
is gradually increasing (2). Since
the 1980s, extracorporeal shock wave lithotripsy (ESWL) has been
widely used in the management of urinary tract calculi, due to its
high efficacy and low morbidity (3). After the manufacture of the first ESWL
device in 1984, several modifications have made subsequent devices
smaller and less powerful, allowing the management of urinary
stones without the use of anesthetic (4,5).
Despite technological development, ~30% of patients still complain
of severe pain (6). Pain during
ESWL can affect the patients' tolerance of the procedure as well as
the effectiveness of treatment (7).
Clinicians have reportedly used a number of pain control agents,
including opioids, non-steroidal anti-inflammatory drugs (NSAIDs),
nitrous oxide, local anesthetic infiltration and dermal anesthetics
such as Emla, to manage the analgesic requirements of ESWL
(6).
Nursing personnel play an important role in patient
preparation and management of the patients' pain and anxiety
(8). They are not only responsible
for prescription drug administration but can also support pain
management by a variety of complementary therapies (9,10). In
the world of modern media, audio-visual (AV) or music distraction
has been successfully used to reduce procedural pain for many
non-urological procedures (11-14).
Considering the widespread use of the ESWL procedure, a number of
researchers have also studied the efficacy of such media
distraction techniques for pain management in urinary stone
patients (15,16). A recent meta-analysis from
Kyriakides et al (15)
evaluated the role of music in reducing pain in patients undergoing
urological procedures. Their study, updated to 2017, included only
six trials on patients undergoing ESWL. Their review was focused on
only music therapy and did not present results of studies only on
ESWL. Considering this lacuna in the literature, the purpose of the
present study was to conduct a systematic review and meta-analysis
to assess the effectiveness of any media distraction in reducing
pain and anxiety of ESWL patients.
Materials and methods
Inclusion criteria
The Preferred Reporting Items for Systematic Reviews
and Meta-analyses (PRISMA) guidelines (17) and guidelines from the Cochrane
collaboration (18) were followed
during the conduct of this systematic review. The Population,
Intervention, Comparison, Outcome and Study design (PICOS) model
was used to select studies for inclusion in the review (17). Studies conducted on patients
undergoing ESWL (population) were considered for inclusion. All
randomized controlled trials (RCTs) comparing any type of media
distraction (music/AV media) used during the ESWL procedure
(intervention), with control (comparison) and measuring pain and/or
anxiety (outcomes) were included. Studies were included
irrespective of sample size and language of publication. The
following studies were excluded: i) Studies utilizing a combination
of music/AV media with any other complementary therapy, including
relaxation therapy, acupuncture and guided imagery, in the study
group; ii) studies utilizing music/AV media for any procedures
other than ESWL; iii) studies not reporting pain and/or anxiety as
an outcome measure; iv) non-RCTs; v) studies not comparing music/AV
media with a control and vi) review articles, cases series and case
reports. In the case of duplication of data, the most updated
version of the study was to be included.
Search strategy
An electronic search was performed independently by
two reviewers. The PubMed, Embase, Scopus, BioMed Central, Ovoid,
and Cochrane Central Register of Controlled Trials (CENTRAL)
databases were screened up to 15th February 2020. Both MeSH terms
and free-text keywords were utilized for searching relevant
articles. Search terms and search strategy along with the results
of the PubMed database are presented in Table SI. The reviewers screened the
search results initially by their titles and abstracts for every
database. After identifying potentially pertinent articles, full
texts of the articles were sourced. Both the reviewers assessed
individual articles based on the inclusion and exclusion criteria.
Any disagreements were resolved by discussion. Post-screening, the
bibliography of included studies, as well as review articles on the
subject, were hand searched for any additional references.
Data extraction and risk of bias
assessment
The two reviewers independently extracted data from
the included studies. Data regarding authors, publication year,
study type, inclusion/exclusion criteria, sample size, demographic
details, types of AV media, number of shock waves, ESWL power
settings, use of analgesics and study outcomes were extracted. The
authors were contacted by e-mail for any missing data. The primary
outcome of the analysis was pain scores recorded after the ESWL
procedure using the visual analog scale (VAS). The secondary
outcome of interest was anxiety measured by the State and Trait
Anxiety Inventory-State Anxiety (STAI-SA) test (19).
The Cochrane Collaboration risk assessment tool was
used to assess the quality of included studies (18). Studies were assessed by two
reviewers independently for: Random sequence generation, allocation
concealment, blinding of participants and personnel, blinding of
outcome assessment, incomplete outcome data, selective reporting
and other bias.
Statistical analysis
The software ʻOpen MetaAnalyst (Version 10.10)ʼ was
used for the meta-analysis (20). A
meta-analysis was conducted only if at least three studies reported
data on the same outcome variable. Predicting heterogeneity in the
included studies, a random-effects model was used to calculate the
pooled effect size for all analyses. Heterogeneity was assessed
using the I2 statistic. I2 values of 25-50%
represented low, values of 50-75% medium and >75% represented
substantial heterogeneity. Continuous data were summarized using
the mean difference (MD) with 95% confidence intervals (CI).
Sub-group analysis was performed for the use of music or AV media
and the use of noise-canceling headphones for the primary outcome.
For studies not reporting mean and standard deviation scores of
outcome variables, the same was calculated from median and
interquartile range using methods reported by Wan et al
(21). A sensitivity analysis was
carried out to assess the influence of each study on the pooled
effect size. In this analysis, data from the various included
studies were excluded one at a time and the effect size was
recalculated. Due to the inclusion of fewer than 10 studies in the
review, funnel plots were not used to assess publication bias
(18).
Results
Study characteristics
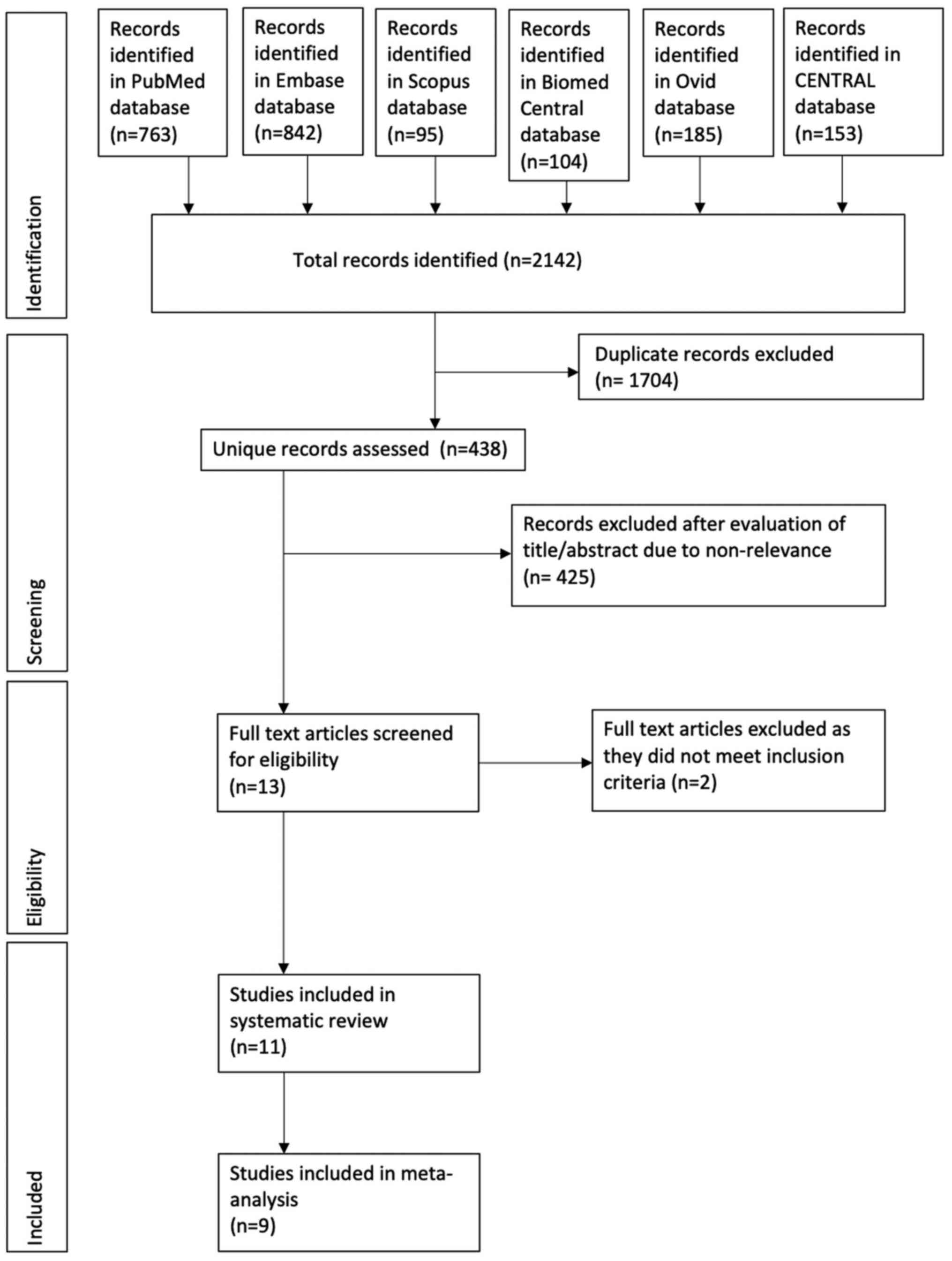
A total of 438 unique records were screened and 13
articles were selected for full-text review (Fig. 1). Finally, 11 articles were included
in this systematic review and meta-analysis (22-32).
Details of the included studies are presented in Table I. Amongst all RCTs, only one was a
cross-over trial (27). The sample
size per arm in the included studies varied from 21-200 patients.
In the study of Karalar et al (28), the study sample was further
subdivided into two groups, based on the use of noise cancellation
headphones. Details of these sub-groups were pooled separately.
El-Khoury et al (32)
conducted a three-arm trial comparing AV media and music with
control. The data of these study groups were pooled separately for
the meta-analysis. Çift and Benlioglu (24) in a five-arm study, compared three
different types of music with two control groups of which one was
provided with headphones while the other was not. The results of
the study and control groups were pooled using a random-effects
meta-analysis model into a single group (18). While different types of music were
used in the included studies, two studies used AV media during
ESWL. In the study of Marsdin et al (22), patients were provided with DVDs and
television sets, while in the trial of El-Khoury et al
(32) an iPad with music videos was
used. Media distraction was delivered via headphones in all trials.
A total of three studies reported the use of noise-cancellation
headphones (28,30,32).
In studies reporting adequate data, there was no statistically
significant difference in the number of shock waves and the power
setting of ESWL between the study and control groups. Seven studies
reported the use of analgesic/anxiolytics during the trial
(22,23,25,26,28,30,32).
In the trial of Yilmaz et al (26), midazolam was used only in the
control group whereas in all remaining studies drugs were not
restricted to any specific group.
 | Table ICharacteristics of included
studies. |
Table I
Characteristics of included
studies.
| | Sample size | Mean age | Male sex (%) | | Number of shock
waves | ESWL power
settings | |
|---|
| Author/Year | Inclusion
criteria | Exclusion
criteria | Study | Control | Study | Control | Study | Control | Media
distraction | Study | Control | Study | Control | Analgesia during
procedure |
|---|
| Cepeda et al
(25), 1998 | Age: 15-65 years
First ESWL | Serum creatinine
>1.5 mg/dl History of opioid use | 97 | 96 | 40.7 | 41 | 49.4 | 48.9 | Patient selected
classical, Caribbean, soft rock, and jazz music via headphones
started 10 mins before procedure and continued up to 10 mins post-
procedure | NR | NR | All patients
reached 17 V | Morphine 10 mg SC
with ketor olac 30 mg IV + alfentanil PCA (0.25 mg dose with 1 min
lockout interval) |
| Koch et al
(23), 1998 | NR | NR | 21 | 22 | 54 | 53 | 80 | 44 | Any music pf
patients choice via headphone during procedure | NR | NR | NR | NR | Midazolam and
Alfentanil 10 µg/kg PCA |
| Yilmaz et al
(26), 2003 | Age: 19-68
years | NR | 48 | 50 | 40.8 | 39.3 | 60.4 | 64 | Relaxing, slow
rhythm sedative music via headphones during procedure | 3043± 110.42 | 3016± 64.22 | 21.96± 0.54 kV | 21.03± 0.48 kV | 15 g emla cream
over flank, 25 mg fentanyl IV given to patients reporting pain.
Midazolam 2 mg in control group only |
| Marsdin et
al (22), 2012 | Elective outpatient
ESWL patients | Ureteric stents
Emergency patients | 61 | 57 | 51.7 | 53.5 | 54 | 56 | 32-inch television
with 30 different DVDs of 30-min programs provided with wireless
headphones | 3948± NR | 3764± NR | NR | NR | Pethidine 100 mg IM
and diclofenac 75 mg IM |
| Akbas et al
(27), 2016 | Age: >18 y No
preoperative pain No analgesic use before the procedure No ureteral
stent inserted Radio-opaque stone | Not completed
procedure Development of complications Refusing to listen to music
Not completing the second session | 200 | 200 | - | - | - | - | Turkish folk,
classical, popular music during procedure | 2724± 492 | 2710± 551 | 17.71± 2.59 J | 17.04± 2.07 J | None |
| Karalar et
al (28), 2016 | Radio- opaque renal
stone | Prior ESWL Ureteric
stents Renal colic | S1: 28 S2: 29 | 32 | S1: 47.8 S2:
47.7 | 48.2 | S1: 61 S2: 62 | 59 | S1: Turkish
classical music by noise cancellation headphones during procedure
S2: Turkish classical music via non noise cancellation headphones
during procedure | 2913± 444 | 2828± 272 | 20.1± 1.1 kV | 19.9± 1.3 kV | Diclofenac 75 mg
IM |
| Cakmak et al
(29), 2017 | Age: >18 y
Radio-opaque renal stone Located in upper/middle calices, renal
pelvis: <20 mm in diameter Proximal ureter: <10 mm in
diameter | Prior ESWL Ureteric
stents Hearing disorders Uncontrolled hypertension History of
psychiatric disease and antidepressant drug use | 95 | 105 | NR | NR | NR | NR | Turkish folk,
classical, popular, relaxing or slow rhythm music via headphones
during procedure | 2764.5± 699.1 | 2777.9± 724.9 | 17.4± 5.3 kV | 17.5± 5.5 kV | NR |
| Jurado et al
(30), 2017 | Age: 18-80 y | Prior ESWL Hearing
loss Analgesia prior to procedure Regularly taking painkillers | 42 | 53 | 52.6 | 52 | 54.8 | 69.8 | Patient selected
classical, chill out, pop, jazz music via by noise cancellation
headphones during procedure | NRa | NR | NRa | NR | Pethidine 20 mg IV
and paracetamol 1 g IV. 10 cc (max 50 cc) of pethidine given to
patients reporting pain. |
| Gezginci et
al (31), 2018 | Age: >18 y First
ESWL BMI: <30 kg/m2 No contradiction for ESWL | Analgesic before
procedure Renal colic before procedure Ureteric stents | 40 | 40 | NRa | NR | 33.3 | 35.2 | Patient selected
Turkish (folk, art, arabesque, pop) music, foreign pop music, rock
and classical music via headphones during procedure | Targeted 3,000 per
session | | NR | NR | None |
| El-Khoury et
al (32), 2020 | Adult patients | NR | AV media: 33 Music:
30 | 31 | AV media: 52.4
Music: 51.5 | 52.6 | AV media: 70 Music:
90 | 71 | AV media: music
videos using Apple iPad Music: Any music/local radio Both delivered
by noise cancellation headphones during procedure | AV media: 3205.9±
545.3 Music: 3175.1± 434.1 | 3150.4± 424.5 | AV media: 74.3± 10
kV Music: 74.3± 9.1 kV | 70.4±16 kV | NSAID suppository
offered to all patients. Breakthrough pain treated by Fentanyl
IM |
| Çift et al
(24), 2020 | Age: >18 years
Radiopaque stone 10-20 mm in diameter localized in the renal pelvis
or ureteropelvic junction Absence of renal colic before the
procedure | Previous ESWL
history Ureteral stent Hearing deficit, Uncontrolled hypertension
Antidepressant drug usage | S1: 30 S2: 30 S3:
30 | C1: 30 C2: 30 | S1: 37.7 S2: 36.3
S3: 36.4 | C1: 38.4 C2:
39.2 | S1: 83.3 S2: 70 S3:
73.3 | C1: 53.3 C2:
56.7 | S1: Turkish art
music S2: Western classical music S3: Patient selected any type of
music. All delivered via headphones during procedure C1: No
headphones, no music C2: Headphones on, no music | S1: 2851.5
(2685.7-3000) S2: 2842.5 (2437.2-2958.7) S3: 2800 (2500-2925) | C1: 2700
(2500-2900) C2: 2725 (2500-2900) | S1: 92 (82-101.25)
S2: 90 (64.25-103.5) S3: 94 (79.75-96.25) | C1: 80 (74.75-92.5)
C2: 85 (65.0-93.25) | None |
The authors' assessment of the quality of included
studies is presented in Table II.
Appropriate methods of randomization were not used in majority
studies. Due to the nature of the intervention, blinding of
patients was not possible. The use of analgesics, which could have
introduced bias in pain outcomes, was taken into consideration for
‘other bias’.
| Table IIRisk of bias in included studies. |
Table II
Risk of bias in included studies.
| Study | Random sequence
generation | Allocation
concealment | Blinding of
participants and personnel | Blinding of outcome
assessment | Incomplete outcome
data | Selective
reporting | Other bias |
|---|
| Cepeda et al
(25) | Unclear risk | Unclear risk | High risk | High risk | Low risk | Unclear risk | Unclear risk |
| Koch et al
(23) | Unclear risk | Unclear risk | High risk | High risk | Low risk | Unclear risk | Unclear risk |
| Yilmaz et al
(26) | Unclear risk | Unclear risk | High risk | High risk | Low risk | Unclear risk | High risk |
| Marsdin et
al (22) | Unclear risk | Unclear risk | High risk | High risk | Low risk | Unclear risk | Unclear risk |
| Akbas et al
(27) | Unclear risk | Unclear risk | High risk | High risk | Low risk | Unclear risk | Low risk |
| Karalar et
al (28) | High risk | Unclear risk | High risk | High risk | Low risk | Unclear risk | Unclear risk |
| Cakmak et al
(29) | Unclear risk | Unclear risk | High risk | High risk | Low risk | Unclear risk | Low risk |
| Jurado et al
(30) | Low risk | Unclear risk | High risk | Low risk | Low risk | Unclear risk | Unclear risk |
| Gezginci et
al (31) | Low risk | Unclear risk | High risk | High risk | Low risk | Low risk | Low risk |
| El-Khoury et
al (32) | Low risk | Unclear risk | High risk | High risk | Low risk | Unclear risk | Unclear risk |
| Çift et al
(24) | Low risk | Low risk | High risk | Low risk | Low risk | Unclear risk | Low risk |
Outcomes
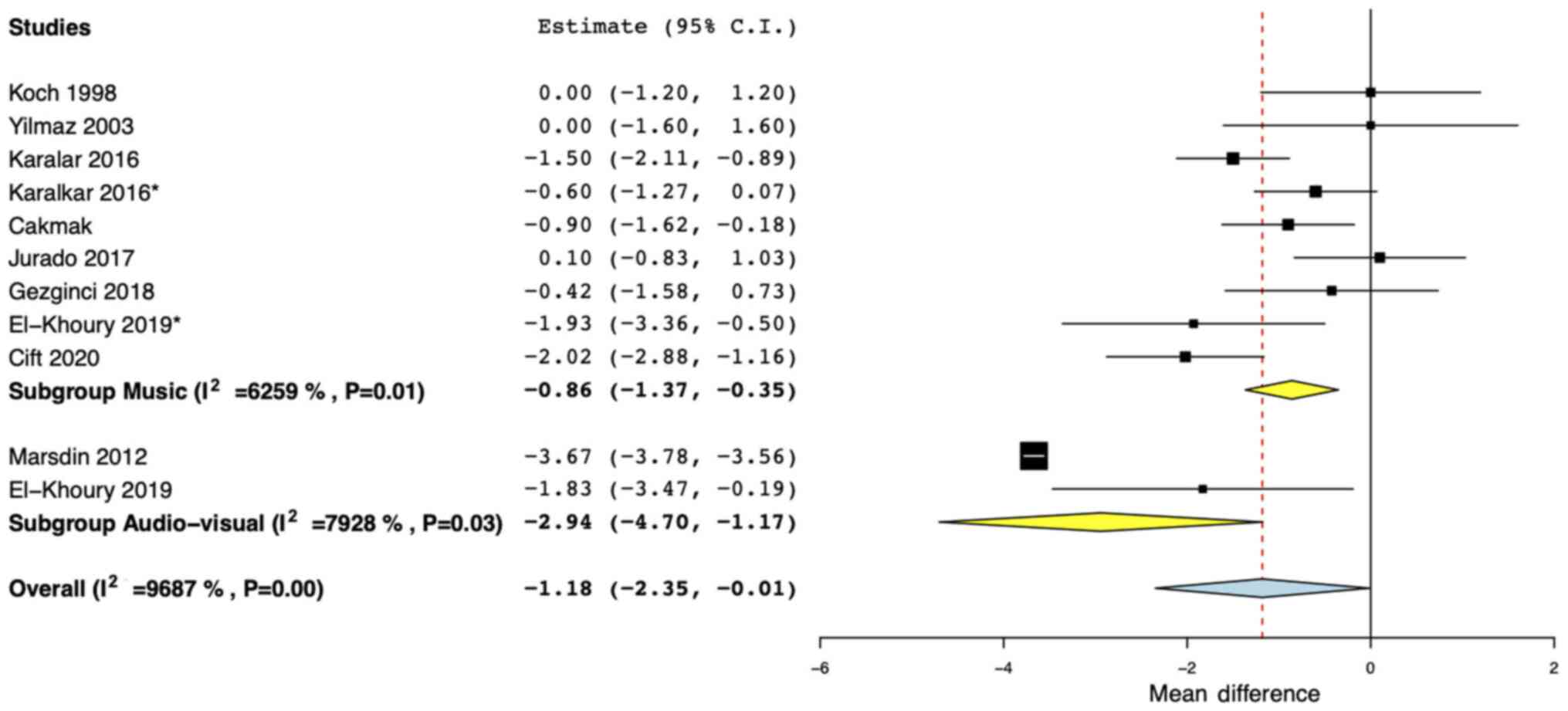
A total of nine studies reported pain outcomes on
the VAS scale (22-24,26,28-32).
Pooled analysis indicated a statistically significant difference in
pain outcomes in favor of media distraction (MD: -1.18; 95% CI:
-2.35, -0.01; I2=96.8%; Fig.
2). On subgroup analysis based on the type of media
distraction, the use of both, AV media (MD: -2.94; 95% CI: -4.70,
-1.17; I2=79.2%) and music (MD: -0.86; 95% CI: -1.37,
-0.35; I2=62.5%), was indicated to lead to a significant
reduction in pain outcomes (Fig.
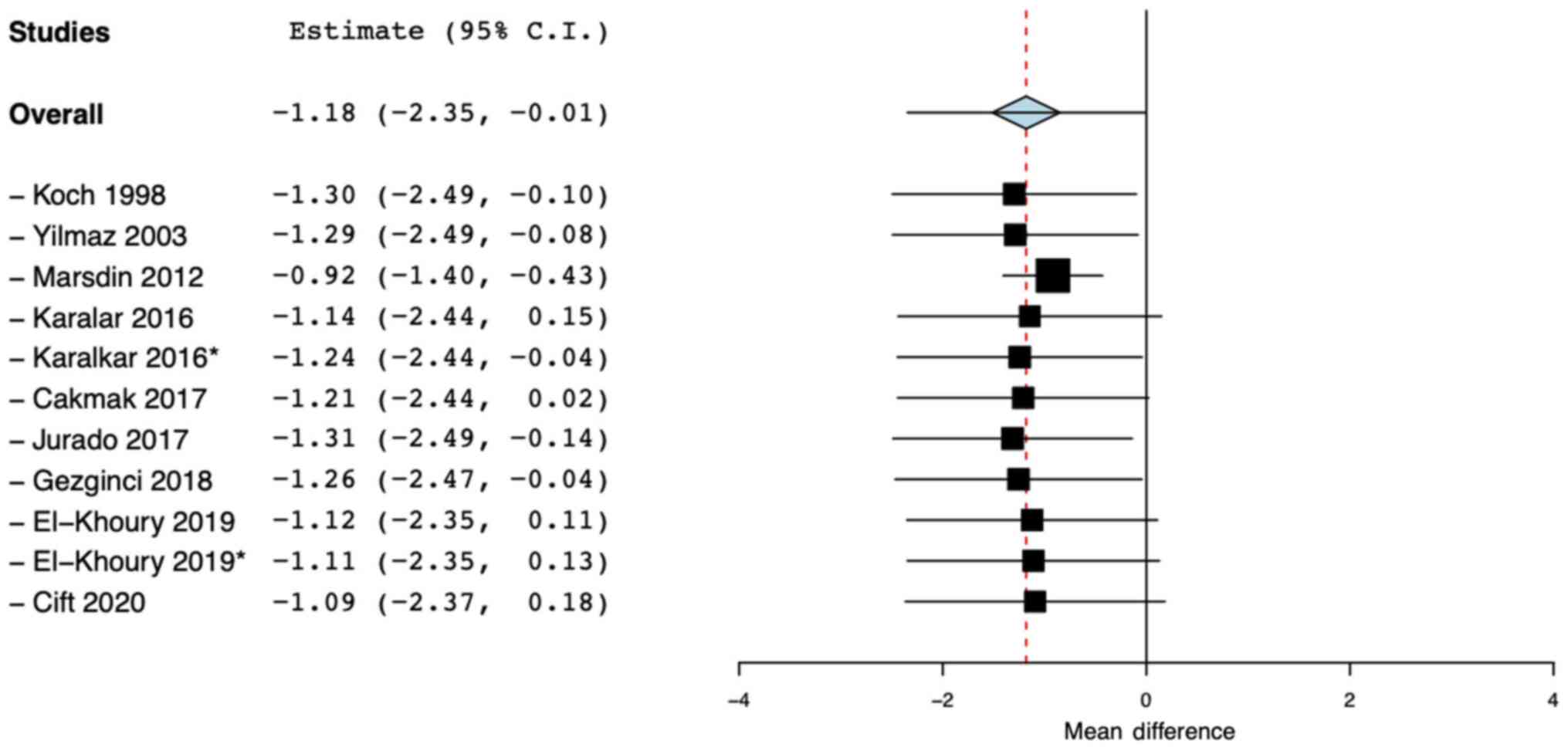
2). Results were, however, not stable on sensitivity analysis.
On the exclusion of the studies of Karalar et al (28) and El-Khoury et al (32), no significant effect of media
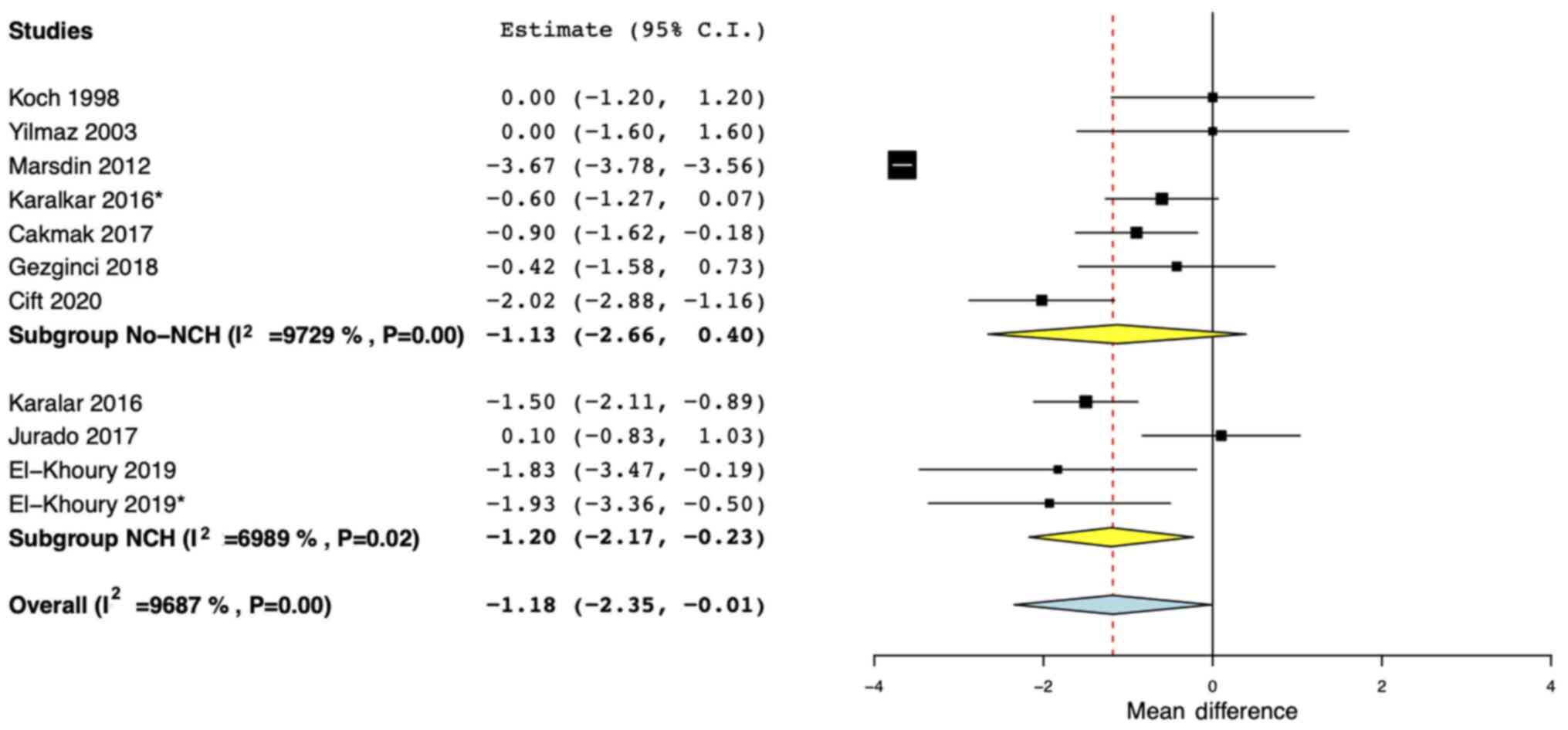
distraction on pain outcomes was identified (Fig. 3). Data from study groups using
noise-cancellation headphones were pooled separately in a sub-group
analysis. The results indicated that there was a statistically
significant reduction in pain scores with the use of
noise-cancellation headphones (MD: -1.20; 95% CI: -2.17, -0.23;
I2=69.8) but no such effect was seen with regular
headphones (MD: -1.13; 95% CI: -2.66, 0.40; I2=97.2%)
(Fig. 4).
There were two studies that did not report pain
outcomes as mean ± standard deviation. E-mail to the corresponding
author for these missing data did not elicit a response. In the
trial of Cepeda et al (25),
alfentanil consumption was compared in the study and control
groups. The authors reported no statistically significant
difference in analgesic use and pain intensity during ESWL in the
two groups. Akbas et al (27), on the other hand, in a cross-over
RCT, reported a statistically significant reduction of pain with
the use of music after both treatment sessions.
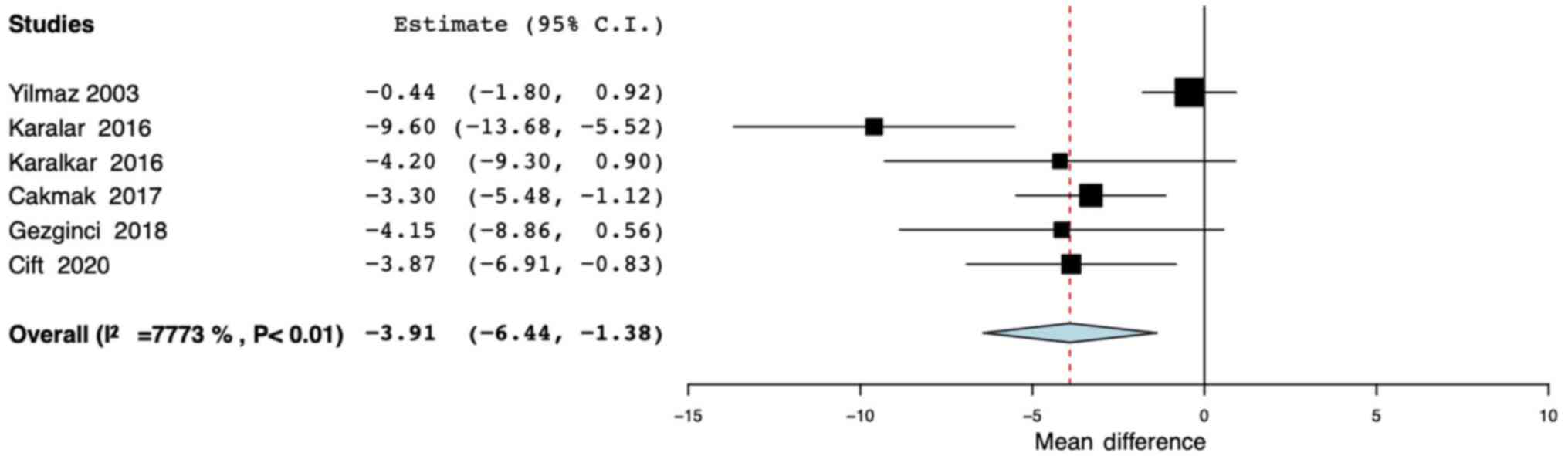
Anxiety outcomes using STAI-SA were reported by five
studies (24,26,28,29,31).
All studies had used only music in the study groups. Pooled
analysis indicated a statistically significant reduction of anxiety
scores with the use of media distraction (MD: -3.91; 95% CI: -6.44,
-1.38; I2=77.7%; Fig.
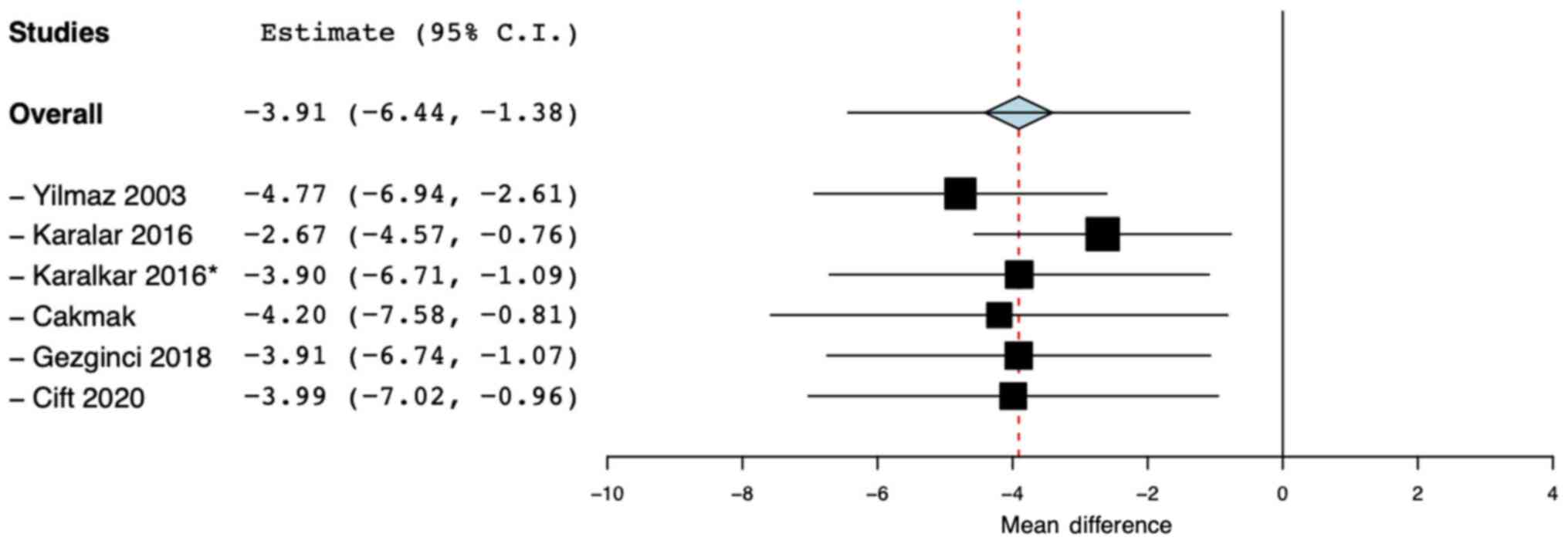
5). The results were stable on sensitivity analysis as there
was no change in significance of the results on exclusion of one
study at a time (Fig. 6). Exclusion
of the study of Yilmaz et al (26) used midazolam in the control group
and the ‘noise cancellation headphone’ group of Karalar et
al (28) did not change the
significance of results. Ordaz Jurado et al (30) compared anxiety in the two groups
using a 10-point VAS scale and reported no statistically
significant difference between the two groups.
Discussion
After a comprehensive review of the literature, the
results of the present study indicated that media distraction in
the form of AV media or music may lead to a statistically
significant reduction of pain and anxiety in patients undergoing
ESWL. Data from a limited number of studies also indicate that the
use of noise-canceling headphones may lead to a significant
reduction in pain and that such an effect may not be seen with
regular headphones.
Several non-pharmacological methods of pain
management, including massage, relaxation therapy, acupuncture,
hypnosis, aromatherapy, music and AV distraction, have been used
for a variety of healthcare-procedures worldwide (33,34).
Music interventions for pain management can be in the form of music
therapy, where a trained professional selects tempo-controlled
melodies to have a calming effect, or in the form of random music
listening which acts as a distraction tool similar to AV aids
(35,36). Owing to its ease of application, a
number of studies have assessed the efficacy of such music and/or
AV distraction for different medical and surgical procedures. In a
recent systematic review and meta-analysis of nine RCTs, Song et
al (11) have demonstrated
significantly reduced pain and anxiety with the use of music in
patients undergoing biopsy. Another RCT has demonstrated that
listening to music during labor significantly reduces pain and
anxiety of mothers during all stages of labor (37). Similarly, AV aids are effective to
reduce pain in patients with sickle cell disease (38), those undergoing colonoscopy
(12), as well as those undergoing
minor surgeries (39).
The application of media distraction, specifically
music, during urological procedures has been evaluated by several
trials with conflicting results. Chang et al (40) in a pilot RCT found music to be
effective in reducing pain, discomfort, and dissatisfaction in
patients undergoing transrectal ultrasound (TRUS)-guided prostate
biopsy, however, no such effect was noted in a similar trial by
Packiam et al (41). Music
has also been used to reduce patient-reported pain and anxiety for
other urological procedures, including percutaneous nephrostomy
tube placement and urodynamic studies (42,43).
As different urological procedures entail different degrees of
pain, the current review was focused solely on ESWL to ensure
reduced bias owing to non-homogenous procedures. Pain during ESWL
can be attributed to several reasons, including trauma caused by
shock waves passing through skin and muscles, stretching of the
renal capsule where therapy is delivered, or due to an increase in
the internal pressure of the kidney (7). Many factors can influence the degree
of pain, including the dimensions and position of the urinary
stone, frequency of shock waves, power settings, sex and the pain
threshold of the patient and use of pre-procedural analgesic
(44). As all included studies were
RCTs, it is hypothesized that the effect of such baseline variables
on outcomes is negated.
The results of the present analysis indicate that
media distraction may significantly reduce pain and anxiety scores
in patients undergoing ESWL. Similar results were obtained by
Kyriakides et al (15) in
their meta-analysis of the role of music in reducing pain and
anxiety for any urological procedure. Compared to the present
review, they focused only on music and were able to include only
six studies for ESWL. The present results also concur with a very
recent systematic review of Saraogi et al (45), which indicates that complementary
medicine strategies including music, acupressure, acupuncture,
transcutaneous electrical nerve stimulation and audiovisual
distractions can reduce pain and anxiety in patients undergoing
ESWL.
In a sub-group analysis based on the type of media,
both AV-media and music were found to significantly reduce pain.
However, results should be interpreted with caution, as only two
studies were available for the sub-group analysis of AV media.
Also, relevant data on anxiety were reported by only five studies.
While assessing the results of patient-reported outcomes, it is
important to bear in mind the concept of minimal clinically
important difference (MCID). The MCID is defined as the smallest
change in a measurement that signifies an important improvement in
a symptom (46). Data from
non-urological studies indicates that the MCID for the VAS scale is
1.4 while for STAI-SA is 10 (47,48).
The pooled MD of VAS scores of all studies in the present analysis
was -1.18 (95% CI: -2.35, -0.01), for studies on music was -0.86
(95% CI: -1.37, -0.35) and for STAI-SA scores was -3.91 (95% CI:
-6.44, -1.38). Interpreted in the context of the reported MCID, it
can be noted that the effect size of the intervention was small and
the upper limits of 95% CI were close to zero for both pain and
anxiety outcomes. This can have important clinical implications as,
even though studies suggest a significant difference in pain and
anxiety outcomes with media distraction, the resultant effect may
not produce a clinically significant improvement in symptoms.
In another sub-group analysis, the present results
indicated a significant reduction in pain scores with the use of
noise cancellation headphones, but no such effect was noted with
regular headphones. Since ESWL is a noisy procedure, the continuous
unpleasant sound of shockwaves may affect patient comfort and
anxiety (28). Therefore, active
noise control employed by such noise-cancellation headphones may
lend a more comfortable environment for ESWL thereby influencing
pain outcomes. However, since only three studies utilized this
technology, results should be interpreted with caution.
The limitations of the present review should be
mentioned. Firstly, the quality of the included studies in the
present review was not high. The absence of adequate methods of
randomization and lack of blinding, due to the nature of the
intervention, may have influenced outcomes. Secondly, there were
methodological variations amongst included studies for the type of
music/AV media, choice of music, use of pre-procedural analgesics
and patient-controlled analgesia. This may have contributed to the
high heterogeneity in the present meta-analyses. Thirdly, data from
two studies were not available for the primary outcome and only
five studies were pooled for the secondary outcome, which has
limited the power of the present analyses. Further, all studies
assessing the role of media distraction on anxiety utilized only
music as the intervention. The role of AV media on anxiety scores
could not be assesses. Fourthly, due to a limited number of studies
in the analysis and limitations of the meta-analysis software,
publication bias could not be assessed in the present review.
Lastly, the results for pain were not stable on sensitivity
analysis, as the exclusion of two studies resulted in
non-significant results.
The present study has its strengths in being the
first meta-analysis focused on the role of media distraction during
ESWL. Only RCTs were analyzed to provide level-1 evidence.
Sensitivity and subgroup analysis were performed to assess the
influence of each study on the effect size and to account for
inter-study variations.
To conclude, the present study indicates that media
distraction in the form of AV media or music may be beneficial in
reducing the pain and anxiety of patients undergoing ESWL. The use
of noise-canceling headphones to deliver the intervention may have
some benefit over regular headphones. Evidence is, however, weak
considering the small effect size, confidence intervals being close
to zero and instability of the results on sensitivity analysis. In
clinical practice, media distraction may be used during ESWL as a
nursing intervention, but a clinically important reduction of pain
and anxiety may not be expected.
Supplementary Material
Search strategy and PubMed search
results.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WH conceived and designed the study. KY, LZ and XL
collected the data, performed the literature search and were
responsible for confirming the authenticity of all the raw data. WH
was involved in the writing of the manuscript. All authors have
read and approved the final manuscript.
Ethical approval
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Amato M, Lusini ML and Nelli F:
Epidemiology of nephrolithiasis today. Urol Int. 72 (Suppl
1):S1–S5. 2004.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Raheem OA, Khandwala YS, Sur RL, Ghani KR
and Denstedt JD: Burden of urolithiasis: Trends in prevalence,
treatments, and costs. Eur Urol Focus. 3:18–26. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kim CH, Shin DS, Kim TB and Jung H: The
efficacy of early extracorporeal shockwave lithotripsy for the
treatment of ureteral stones. Urol J. 16:331–336. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Gupta NP and Kumar A: Analgesia for pain
control during extracorporeal shock wave lithotripsy: Current
status. Indian J Urol. 24:155–158. 2008.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Chaussy C, Schmiedt E, Jocham D, Brendel
W, Forssmann B and Walther V: First clinical experience with
extracorporeally induced destruction of kidney stones by shock
waves. J Urol. 127:417–420. 1982.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Bach C, Zaman F, Kachrilas S, Kumar P,
Buchholz N and Masood J: Drugs for pain management in shock wave
lithotripsy. Pain Res Treat. 2011(259426)2011.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ozsaker E and Diramali A: The effect of
transcutaneous electrical nerve stimulation for pain relief during
extracorporeal shock-wave lithotripsy procedure. Pain Manag Nurs.
15:59–68. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Brown MA: The role of nurses in pain and
palliative care. J Pain Palliat Care Pharmacother. 27:300–302.
2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Zins S, Gross C and Hooke MC:
Complementary therapies for pain among individuals receiving
hemodialysis: A systematic review. Nephrol Nurs J. 45:13–23.
2018.PubMed/NCBI
|
|
10
|
Aydin D, Sahiner NC and Ciftci EK:
Non-pharmacological strategies used to reduce procedural pain in
infants by nurses at family health centres. J Pak Med Assoc.
67:889–894. 2017.PubMed/NCBI
|
|
11
|
Song M, Li N, Zhang X, Shang Y, Yan L, Chu
J, Sun R and Xu Y: Music for reducing the anxiety and pain of
patients undergoing a biopsy: A meta-analysis. J Adv Nurs.
74:1016–1029. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Xiaolian J, Xiaolin L and Lan ZH: Effects
of visual and audiovisual distraction on pain and anxiety among
patients undergoing colonoscopy. Gastroenterol Nurs. 38:55–61.
2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Drahota A, Galloway E, Stores R, Ward D,
Severs M and Dean T: Audiovisual distraction as an adjunct to pain
and anxiety relief during minor surgery. Foot (Edinb). 18:211–219.
2008.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Sahiner NC and Bal MD: The effects of
three different distraction methods on pain and anxiety in
children. J Child Health Care. 20:277–285. 2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kyriakides R, Jones P, Geraghty R,
Skolarikos A, Liatsikos E, Traxer O, Pietropaolo A and Somani BK:
Effect of music on outpatient urological procedures: A systematic
review and meta-analysis from the european association of urology
section of uro-technology. J Urol. 199:1319–1327. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Goh NM, Drake T, Rai BP and Somani BK:
Complementary approaches to decreasing discomfort during shockwave
lithotripsy (SWL). Urolithiasis. 42:189–193. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Moher D, Liberati A, Tetzlaff J and Altman
DG: PRISMA Group. Preferred reporting items for systematic reviews
and meta-analyses: The PRISMA statement. PLoS Med.
6(e1000097)2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Higgins J, Thomas J, Chandler J, Cumpston
M, Li T, Page M and Welch V (eds): Cochrane handbook for systematic
reviews of interventions. Version 6. Cochrane, 2019.
|
|
19
|
Elwood LS, Wolitzky-Taylor K and Olatunji
BO: Measurement of anxious traits: A contemporary review and
synthesis. Anxiety Stress Coping. 25:647–666. 2012.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wallace BC, Schmid CH, Lau J and
Trikalinos TA: Meta-analyst: Software for meta-analysis of binary,
continuous and diagnostic data. BMC Med Res Methodol.
9(80)2009.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Wan X, Wang W, Liu J and Tong T:
Estimating the sample mean and standard deviation from the sample
size, median, range and/or interquartile range. BMC Med Res
Methodol. 14(135)2014.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Marsdin E, Noble JG, Reynard JM and Turney
BW: Audiovisual distraction reduces pain perception during
shockwave lithotripsy. J Endourol. 26:531–534. 2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Koch ME, Kain ZN, Ayoub C and Rosenbaum
SH: The sedative and analgesic sparing effect of music.
Anesthesiology. 89:300–306. 1998.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Çift A and Benlioglu C: Effect of
different musical types on patient's relaxation, anxiety and pain
perception during shock wave lithotripsy: A randomized controlled
study. Urol J. 17:19–23. 2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Cepeda MS, Diaz JE, Hernandez V, Daza E
and Carr DB: Music does not reduce alfentanil requirement during
patient-controlled analgesia (PCA) use in extracorporeal shock wave
lithotripsy for renal stones. J Pain Symptom Manage. 16:382–387.
1998.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Yilmaz E, Ozcan S, Basar M, Basar H,
Batislam E and Ferhat M: Music decreases anxiety and provides
sedation in extracorporeal shock wave lithotripsy. Urology.
61:282–286. 2003.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Akbas A, Gulpinar MT, Sancak EB, Karakan
T, Demirbas A, Utangac MM, Dede O, Sancaktutar AA, Simsek T, Sahin
B and Resorlu B: The effect of music therapy during shockwave
lithotripsy on patient relaxation, anxiety, and pain perception.
Ren Fail. 38:46–49. 2016.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Karalar M, Keles I, Doğantekin E, Kahveci
OK and Sarici H: Reduced pain and anxiety with music and
noise-canceling headphones during shockwave lithotripsy. J
Endourol. 30:674–677. 2016.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Cakmak O, Cimen S, Tarhan H, Ekin RG,
Akarken I, Ulker V, Celik O, Yucel C, Kisa E, Ergani B, et al:
Listening to music during shock wave lithotripsy decreases anxiety,
pain, and dissatisfaction: A randomized controlled study. Wien Klin
Wochenschr. 129:687–691. 2017.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Ordaz Jurado DG, Budia Alba A, Bahilo
Mateu P, Trassierra Villa M, López-Acón D and Boronat Tormo F:
Litotricia por ondas de choque con música: Un tratamiento menos
doloroso y más satisfactorio/Shockwave lithotripsy with music: Less
painful and more satisfactory treatment. Actas Urol Esp.
41:584–589. 2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Gezginci E, Iyigun E, Yalcin S, Bedir S
and Ozgok IY: Comparison of two different distraction methods
affecting the level of pain and anxiety during extracorporeal shock
wave lithotripsy: A randomized controlled trial. Pain Manag Nurs.
19:295–302. 2018.PubMed/NCBI View Article : Google Scholar
|
|
32
|
El-Khoury HJ, Brookes JDL, Tan B, Shahbaz
S and McCahy PJ: Impact of modern media on analgesic requirements
during extracorporeal shockwave lithotripsy. ANZ J Surg. 90:53–56.
2020.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Smith CA, Levett KM, Collins CT, Armour M,
Dahlen HG and Suganuma M: Relaxation techniques for pain management
in labour. Cochrane Database Syst Rev. 3(CD009514)2018.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Lin YC, Wan L and Jamison RN: Using
integrative medicine in pain management: An evaluation of current
evidence. Anesth Analg. 125:2081–2093. 2017.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Bradt J, Potvin N, Kesslick A, Shim M,
Radl D, Schriver E, Gracely EJ and Komarnicky-Kocher LT: The impact
of music therapy versus music medicine on psychological outcomes
and pain in cancer patients: A mixed methods study. Support Care
Cancer. 23:1261–1271. 2015.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Gold C, Erkkilä J, Bonde LO, Trondalen G,
Maratos A and Crawford MJ: Music therapy or music medicine?
Psychother Psychosom. 80:304–305. 2011.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Simavli S, Gumus I, Kaygusuz I, Yildirim
M, Usluogullari B and Kafali H: Effect of music on labor pain
relief, anxiety level and postpartum analgesic requirement: A
randomized controlled clinical trial. Gynecol Obstet Invest.
78:244–250. 2014.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Ezenwa MO, Yao Y, Engeland CG, Molokie RE,
Wang ZJ, Suarez ML and Wilkie DJ: A randomized controlled pilot
study feasibility of a tablet-based guided audio-visual relaxation
intervention for reducing stress and pain in adults with sickle
cell disease. J Adv Nurs. 72:1452–1463. 2016.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Hudson BF and Ogden J: Exploring the
impact of intraoperative interventions for pain and anxiety
management during local anesthetic surgery-a systematic review and
meta-analysis. J Perianesth Nurs. 31:118–133. 2016.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Chang YH, Oh TH, Lee JW, Park SC, Seo IY,
Jeong HJ and Kwon WA: Listening to music during transrectal
ultrasound-guided prostate biopsy decreases anxiety, pain and
dissatisfaction in patients: A pilot randomized controlled trial.
Urol Int. 94:337–341. 2015.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Packiam VT, Nottingham CU, Cohen AJ,
Eggener SE and Gerber GS: No effect of music on anxiety and pain
during transrectal prostate biopsies: A randomized trial. Urology.
117:31–35. 2018.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Hamidi N and Ozturk E: The effect of
listening to music during percutaneous nephrostomy tube placement
on pain, anxiety, and success rate of procedure: A randomized
prospective study. J Endourol. 31:457–460. 2017.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Diri MA, Çetinkaya F and Gül M: The
effects of listening to music on anxiety, pain, and satisfaction
during urodynamic study: A randomized controlled trial. Urol Int.
103:444–449. 2019.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Kumar A, Gupta NP, Hemal AK and Wadhwa P:
Comparison of three analgesic regimens for pain control during
shockwave lithotripsy using dornier delta compact lithotripter: A
randomized clinical trial. J Endourol. 21:578–582. 2007.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Saraogi M, Geraghty RM, Hameed B, Rob S,
Pietropaolo A, Sarica K, Gozen A, Liatsikos E and Somani BK: Role
of complementary medicine (music, acupuncture, acupressure, TENS
and audio-visual distraction) in shockwave lithotripsy (SWL): A
systematic review from EAU sections of urolithiasis (EULIS) and
uro-technology (ESUT). Urology. 145:38–51. 2020.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Tashjian RZ, Deloach J, Porucznik CA and
Powell AP: Minimal clinically important differences (MCID) and
patient acceptable symptomatic state (PASS) for visual analog
scales (VAS) measuring pain in patients treated for rotator cuff
disease. J Shoulder Elbow Surg. 18:927–932. 2009.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Delgado DA, Lambert BS, Boutris N,
McCulloch PC, Robbins AB, Moreno MR and Harris JD: Validation of
digital visual analog scale pain scoring with a traditional
paper-based visual analog scale in adults. J Am Acad Orthop Surg
Glob Res Rev. 2(e088)2018.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Corsaletti BF, Proença M-DGL, Bisca GKW,
Leite JC, Bellinetti LM and Pitta F: Minimal important difference
for anxiety and depression surveys after intervention to increase
daily physical activity in smokers. Fisioter E Pesqui. 21:359–364.
2014.
|