Introduction
Atmospheric particulate matter with a diameter ≤2.5
µm (PM2.5) has a large surface area, adsorbs toxic
substances and penetrates into the lung alveoli (1-5).
Epidemiological studies have demonstrated that ambient
PM2.5 pollution contributes to lower respiratory tract
infections, cancer of the trachea, bronchus and lungs, ischemic
heart disease, cerebrovascular disease and chronic obstructive
pulmonary disease (6-8).
Therefore, ambient PM2.5 pollution increases the
incidence of premature death (6,7). The
elderly, children and individuals with cardiopulmonary disease are
particularly susceptible to the effects of PM2.5
(6-9).
Certain toxic substances, such as some heavy metals,
adsorbed into PM2.5 are released into the lungs and
adsorb into lung epithelial cells, resulting in penetration to
blood vessels during breathing (10-14).
Therefore, the respiratory and cardiovascular systems are
considered to be the primary biological targets of inhaled
PM2.5 (10-14).
The composition of PM2.5 is complex and varies by source
(2), although it is mainly
comprised of soluble salts, metals, organic compounds, carbon and
biological constituents (15-17).
Organic and inorganic compounds adsorbed into PM2.5 have
been demonstrated to be closely associated with the biologically
toxic effects of the particles (18-20).
While the toxic effects of the water- and fat-soluble components of
PM2.5 have been investigated (21-24),
little research has been conducted on pure PM2.5
particles (PPP2.5), which are primarily comprised of
carbon. Particles of carbon black have been studied (25,26);
however, its toxic effects vary from those of PPP2.5. It
is therefore necessary to characterize the biologically toxic
effects of PPP2.5.
In previous studies (17,27),
atmospheric PM2.5 was sampled from an urban area of
Beijing, China, which tested the original PM2.5
particles (OPP2.5): PPP2.5 (mainly comprised
of insoluble solid components), water-soluble fractions of
PM2.5 and fat-soluble fractions of PM2.5. The
chemical and biological constituents of these four matrices were
characterized and their toxic effects on A549 human alveolar basal
epithelial cells were assessed. OPP2.5 had more complex
constituents than PPP2.5, including large quantities of
water-soluble ions, multiple metals and polycyclic aromatic
hydrocarbons, as well as copies of bacterial and fungal genomes and
endotoxins (0.433 EU/mg). In contrast, PPP2.5 contained
low levels of water-soluble ions and metals, practically
undetectable polycyclic aromatic hydrocarbons, no bacterial or
fungal genomes and endotoxin contents were <1/10 of those of
OPP2.5 (0.0419 EU/mg). The main constituents of the
water-soluble fractions of PM2.5 were ions, while
relatively more polycyclic aromatic hydrocarbons were measured in
fat-soluble fractions of PM2.5. OPP2.5 and
PPP2.5 were more cytotoxic than the water-soluble and
fat-soluble fractions of PM2.5. Therefore, the present
study elected to further evaluate the toxic effects induced by
these two insoluble solid particles in vivo.
The present study investigated the effects of
OPP2.5 and PPP2.5 in male BALB/c mice treated
with instilled aerosols of OPP2.5 or PPP2.5.
Pro-inflammatory cytokines and chemokines and other biochemical
factors were measured in serum. The lungs, the major target organs,
were analyzed histopathologically. Flow cytometry was utilized to
analyze immune status by counting immune cells in the lungs and the
levels of inflammatory cytokines and other biochemical factors in
bronchoalveolar lavage fluid (BALF) were measured. The findings
provided a foundation for future research into the mechanisms of
toxicity induced by inhaled PM2.5.
Materials and methods
Animals
Specific pathogen-free male BALB/c mice (n=36; 6-8
weeks old; weight, 23-29 g pre-treatment and 20-27 g
post-treatment) were obtained from the Laboratory Animal Center of
the Academy of Military and Medical Science. The mice were housed
at 20±1˚C, with 60% humidity and 12/12 h light/dark cycles, 4 mice
per cage, according to the Guideline for Animal Experiments of the
Academy of Military and Medical Sciences. All animals had free
access to water and food and were allowed to acclimatize for 1 week
prior to the experimental procedures. All animal experiments were
approved by the Animal Ethics Committee of the Academy of Military
and Medical Sciences (approval no. AMMS-13-2015-013). No animals
died unexpectedly prior to the end of this experiment. At the end
of the experiment, the mice were euthanized via intraperitoneal
injection of sodium pentobarbital (~150 mg/kg). Death was
determined by cessation of heartbeat or respiratory arrest.
PM sources and processing
PM2.5 sampling and OPP2.5 and
PPP2.5 processing were described previously (17). Briefly, PM was collected during May
and June with a PM10/PM2.5 high-volume air
sampler (Thermo Fisher Scientific, Inc.) equipped with a
PM2.5 pre-separator. Collection was performed in a
typical urban area in Beijing, ~18 m above ground level.
PM2.5 was collected in a quartz filter (Pall
Corporation) that was previously calcinated in a muffle furnace at
600˚C for 2 h to remove organic substances. OPP2.5 was
prepared by resuspending with double-distilled water post-sampled
filters and mixed before use. PPP2.5 was obtained by
removing water- and fat-soluble components using high-temperature
and high-pressure sterilization, including baking at 180˚C for 3 h
to destroy microorganisms and remove endotoxins.
To prepare particle suspensions for the animal
experiments, fractioned OPP2.5 and PPP2.5
particles were immediately suspended in sterile saline (0.9% NaCl)
prior to use and sonicated for 10 min in ice water mixture to
obtain a uniform dispersion and prevent particle aggregation.
Experimental design and execution
OPP2.5 and PPP2.5 were
suspended and sonicated in sterile saline to final concentrations
of 1.6 mg/ml. Mice were randomly divided into 3 groups (n=12/group)
and treated with 50 µl sterile saline (control), OPP2.5
suspension or PPP2.5 suspension. According to a previous
study (28), the instillation dose
in the present study was ~4 times the inhaled dose of mice compared
with the current atmospheric dose at 1 mg/m3 of
PM2.5. Mice were weighed before and after treatment.
Blood, tissues and BALF were collected 24 h post-treatment. Whole
blood was collected for the determination of hematocrit and
preparation of serum.
Prior to the experiment, mice were anesthetized with
pentobarbital sodium (~0.08 g/kg) by intraperitoneal injection.
Once a deep stage of anesthesia was attained (calm and regular
breathing), mice were intratracheally instilled using a
MicroSprayer Aerosolizer system (IA-1C and FMJ-250 High-Pressure
Syringe; Penn-Century, Inc.) with 50 µl isotonic sterile saline
solution containing 80 µg OPP2.5 or PPP2.5.
Saline solution was used for the controls. Each mouse was placed in
a supine position, the mouth was opened and the tongue gently moved
aside using forceps to better cannulate the trachea. The particles
were suspended in the appropriate solution immediately prior to
instillation as aforementioned. Following instillation, the mice
were immediately observed for at least 1 h before being returned to
their cages under the aforementioned controlled environmental
conditions.
Serum preparation and biochemical
analyses
At 24 h post-treatment, ~300 µl blood was collected
from one of the retro orbital sinus into a 1.5 ml centrifuge tube.
Some blood was used for the determination of hematocrit. After
incubating the blood at room temperature for 1-2 h, tubes were
centrifuged at 825 x g for 10 min at 4˚C. The serum supernatants
were collected and divided into aliquots and stored at -80˚C for
the subsequent biochemical analyses on the pro-inflammatory
cytokines and chemokines, and other clinical indicators.
Clinical indicators, including the activities of
alanine aminotransferase (ALT), aspartate transaminase (AST),
lactate dehydrogenase (LDH) and alkaline phosphatase (ALP), and the
levels of total protein, albumin (ALB), globulin and creatinine
were measured in serum using an automatic biochemical analyzer
(7080; Hitachi, Ltd.). The concentrations of pro-inflammatory
cytokines/chemokines, including mouse eotaxin, interleukin (IL)1α,
IL-1β, IL-6, leukemia inhibitory factor (LIF), IL-17, monocyte
chemoattractant protein (MCP) 1, macrophage inflammatory protein
(MIP)1α, MIP-2, vascular endothelial growth factor (VEGF) and tumor
necrosis factor (TNF)α were determined in serum using Milliplex MAP
multiplex immunoassay kits (Mouse Cytokine/Chemokine Panel I;
MCYTOMAG-70; MilliporeSigma), according to the manufacturer's
protocol. In addition, the concentration of C-reactive protein
(CRP) in serum was determined using the Mouse CRP ELISA kit (cat.
no. EK0977; Boster Biological Technology), according to the
manufacturer's protocol. Results were normalized to the levels of
hematocrit in blood. All experiments were performed in
octuplicate.
Histopathology
The left lung of each mouse was submerged in 10%
formalin at room temperature (RT) for 48 h and processed for
histology. Paraffin blocks were prepared from dehydrated tissues
(treated with gradient ethanol), and 3-µm-thick sections were
stained with hematoxylin and eosin at RT for ~5 min, followed by
analysis using a light microscope at x40 magnification, and the
levels of inflammatory response were evaluated by assessing the
alveolar structure and alveolar wall thickness in mice. All
experiments were performed in triplicate.
Flow cytometry
Lung single-cell suspensions were prepared at 24 h
post-treatment as described previously (29). Briefly, mice were euthanized via
intraperitoneal injection of pentobarbital sodium (~150 mg/kg)
following treatment with 100 µl of 500 U/ml heparin (Beijing
Solarbio Science & Technology Co., Ltd.) subcutaneously. The
thorax and abdomen were opened, the left atrium excised and the
lungs were perfused through the right ventricle with 15 ml of
phosphate-buffered saline. The trachea was exposed and cannulated,
and the lung was inflated with 1 ml of digestion buffer, containing
1.5 mg/ml collagenase A (cat. no. 10103586001; Roche Diagnostics),
1.5 U/ml of dispase II protease (cat. no. D4693; Sigma-Aldrich;
Merck KGaA), 0.4 mg/ml DNase I (cat. no. D8071; Sangon Biotech Co.,
Ltd.), 10% FBS (Gibco; Thermo Fisher Scientific, Inc.) and 10 mM
HEPES in Hanks' balanced salt solution (cat. no. 14025-092; Gibco;
Thermo Fisher Scientific, Inc.). After the trachea was sealed with
3.0 sutures and the heart and mediastinal tissues were removed, the
lung inflated with digestion buffer was placed in 5 ml of digestion
buffer and incubated at 37˚C for 60 min with shaking. Following
digestion, ~25 ml phosphate-buffered saline, 0.5% bovine serum ALB
and 20 mM EDTA were added. The cell suspensions and lung tissue
were filtered through a 70-µm strainer. After centrifuging the cell
suspensions at 350 g at 4˚C for 5 min, the pellet was treated with
red blood cell lysis solution (Tianjin Haoyang Biological
Manufacture Co., Ltd.) and washed with phosphate-buffered saline in
0.5% bovine serum albumin (Amresco, LLC), then suspended in
phosphate-buffered saline with 2% FBS.
After counting the lung cells using a Countess II FL
automated counter (Thermo Fisher Scientific, Inc.),
~2x106 cells from each mouse were incubated in blocking
solution, consisting of phosphate-buffered saline containing 0.25%
FcBlock (cat. no. 553141; BD Biosciences), for 15 min at 4˚C and
then stained with antibodies (a list of antibodies, clones,
fluorochromes and concentrations are presented in Table SI) for 30 min at 4˚C. Following
staining, cells were washed and fixed with 1% paraformaldehyde in
phosphate-buffered saline for 30 min at 4˚C, then washed and
resuspended in phosphate-buffered saline with 0.5% bovine serum
albumin. Flow cytometry was conducted with a BD FACSymphony A5 flow
cytometer using BD FACSDiva software 8.0 (BD Biosciences), and the
data were analyzed using FlowJo software (version 10; FlowJo LLC).
The present study used a previously published protocol (30) to analyze the immune status in the
lung. Live CD45+ cells were gated, and myeloid cells
were gated based on CD11c vs. CD11b. Total myeloid cells were then
plotted as MerTK vs. CD64, and the MerTK+
CD64+ macrophage gate was plotted as CD11c vs. MHC II to
illustrate the alveolar macrophages and interstitial macrophage
(IM)1, IM2 and IM3. A macrophage-deficient gate was plotted with
CD11c and MHC II to illustrate dendritic cells, which were plotted
as CD11c vs. CD11b to identify Batf3+ and
Irf4+ dendritic cells. A macrophage/dendritic
cell-deficient gate was plotted as Ly6G vs. CD11b to identify
neutrophils (CD11b+ Ly6G+) and a
macrophage/dendritic cell/neutrophil-deficient gate was plotted as
side scatter vs. F4/80 to identify eosinophils and monocytes. All
experiments were performed in quadruplicate.
BALF collection and biochemical
analyses
Following sacrifice 24 h post-treatment, the
tracheas were exposed and cannulated. The lungs were lavaged twice,
each time by instilling a 0.7 ml aliquot of isotonic saline
solution and the two washes were pooled as BALF. The total lavage
fluid from each mouse lung was combined and centrifuged at 400 x g
for 10 min at 4˚C (3-18K; Sigma-Aldrich; Merck KGaA) and the
supernatants were divided into aliquots and stored for subsequent
determination. Levels of clinical indicators and pro-inflammatory
cytokines/chemokines were measured in BALF as aforementioned for
serum analyses. All experiments were performed in octuplicate.
Statistical analysis
SAS software (version 9.3; SAS Institute, Inc.) was
used to analyze data. With the exception of the histopathological
evaluation, all data are expressed as mean ± standard error of the
mean. Statistical differences were assessed by one-way ANOVA
followed by Student-Newman-Keuls comparisons. Non-parametric
Kruskal-Wallis test was performed followed by Dunn's test for data
that did not conform to normality or homogeneity of variance.
P<0.05 was considered to indicate a statistically significant
difference.
Results
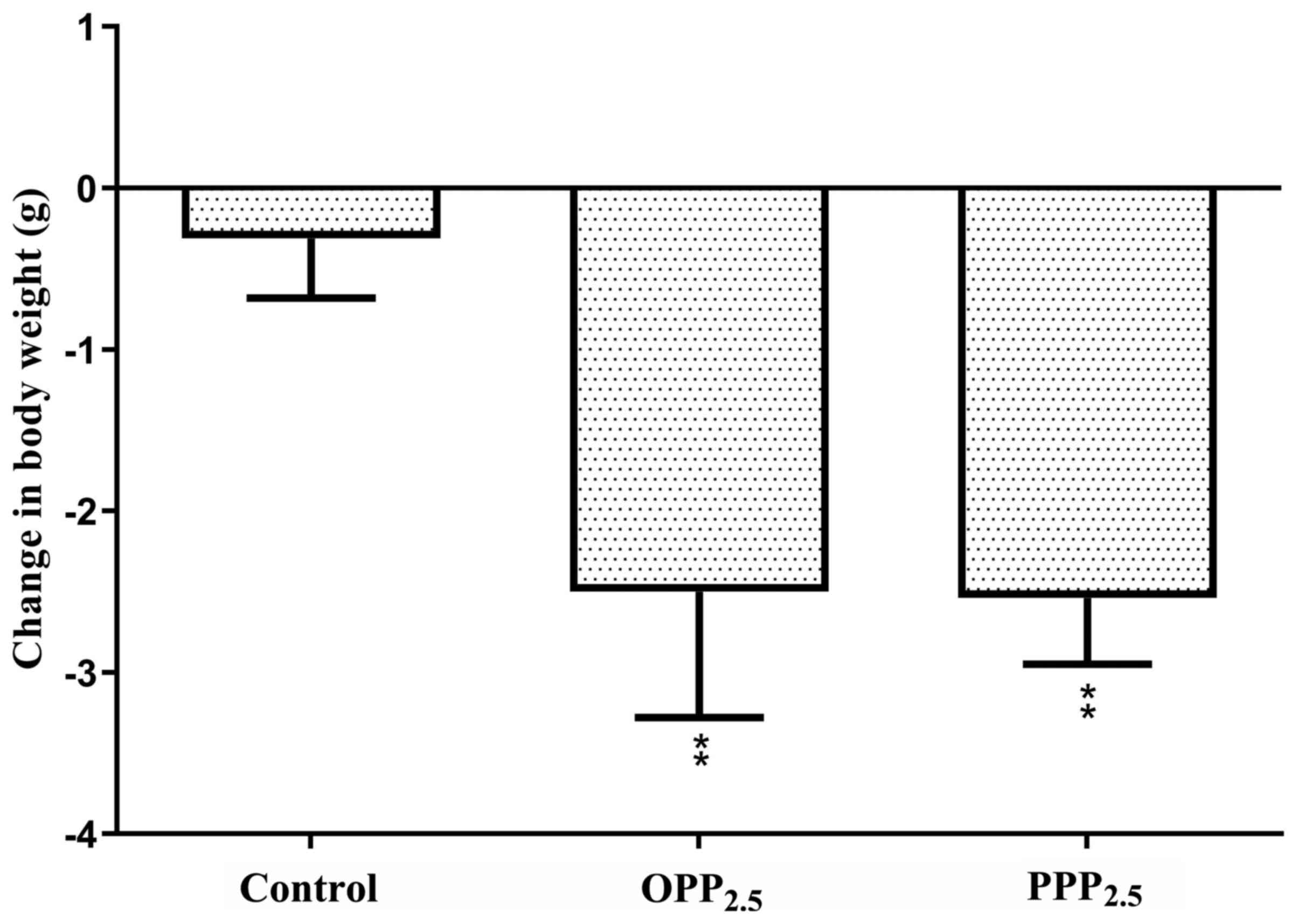
Body weight
Mice were weighed before and after treatment with
OPP2.5 and PPP2.5 (Fig. 1). Body weight decreased in the
treated groups compared with controls. There was no significant
difference between mice treated with OPP2.5 and
PPP2.5.
Serum biochemical analyses
The activities or contents of AST, globulin, total
protein and creatinine in serum did not differ significantly
between the treatment and control groups (data not shown). Compared
with levels in the control group, the blood hematocrit in the
OPP2.5 group was significantly higher compared with
controls (Fig. 2A). Mice treated
with OPP2.5 or PPP2.5 had lower serum ALT,
LDH and ALP activities compared with controls (Fig. 2B, D
and E). Furthermore, serum ALB
levels decreased in the OPP2.5 group compared with
controls (Fig. 2C). With the
exception of ALB and hematocrit, clinical indicator levels did not
differ significantly between the OPP2.5 and
PPP2.5 groups.
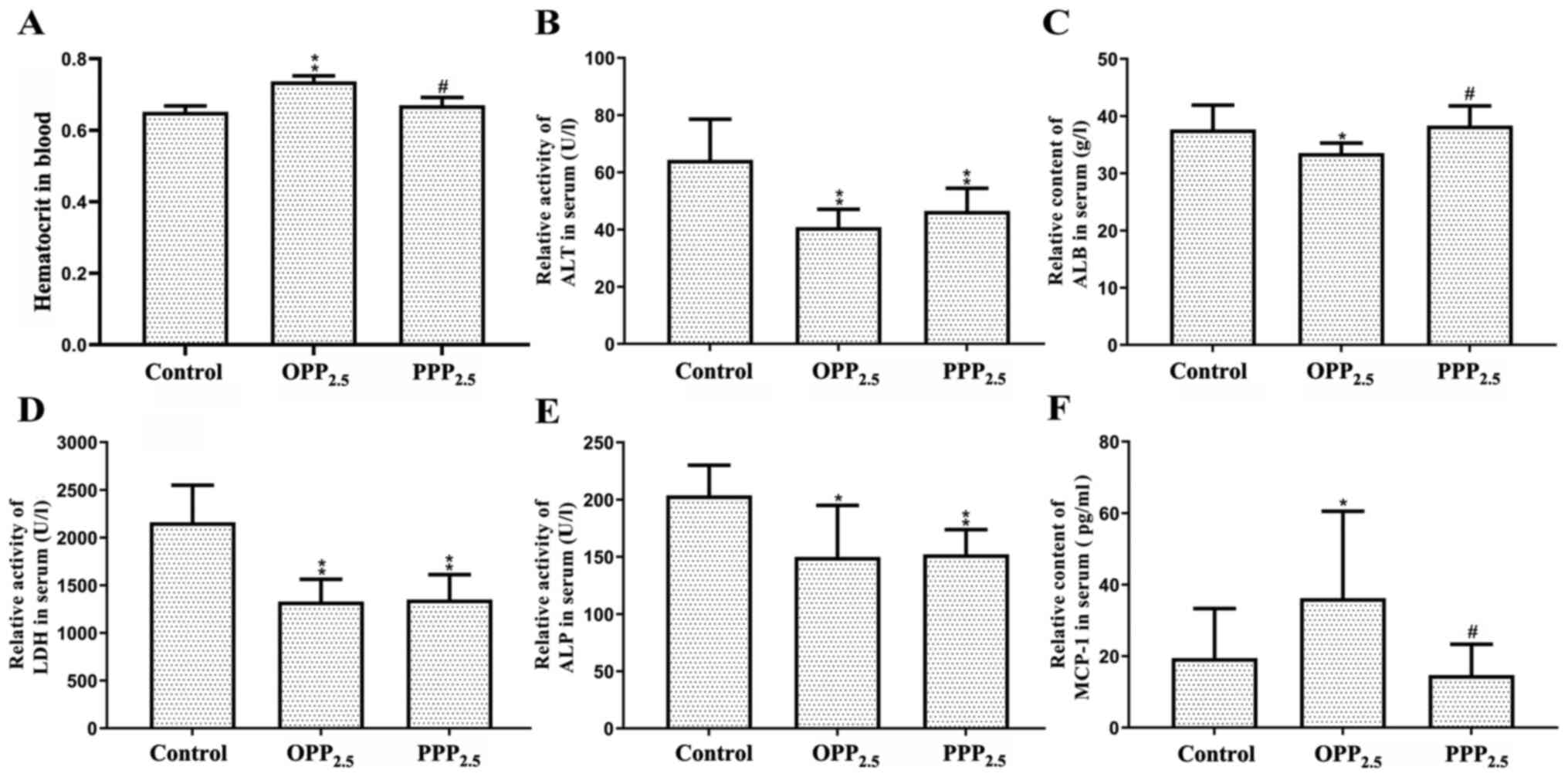 | Figure 2Levels of biochemical factors in
blood and serum following exposure to OPP2.5 particles
(80 µg), PPP2.5 particles (80 µg) or vehicle (50 µl
sterile saline). (A) Hematocrit level. Relative activities of (B)
ALT, (C) ALB, (D) LDH and (E) ALP. (F) Relative content of MCP1.
Results were normalized to hematocrit levels. Data are presented as
mean ± standard error of the mean (n=8/group).
*P<0.05 and **P<0.01 vs. control.
#P<0.05 vs. OPP2.5 group.
OPP2.5, original atmospheric particulate matter with a
diameter ≤2.5 µm; PPP2.5, pure atmospheric particulate
matter with a diameter ≤2.5 µm; ALT, alanine aminotransferase; ALB,
albumin; LDH, lactate dehydrogenase; ALP, alkaline phosphatase;
MCP1, monocyte chemoattractant protein. |
Serum levels of eotaxin, IL-1α, IL-1β, IL-6, LIF,
IL-17, MIP-1α, MIP-2, VEGF, TNF-α and CRP did not differ
significantly between groups (data not shown). Serum MCP-1 levels
increased in the OPP2.5 group compared with the control
and PPP2.5 groups (Fig.
2F).
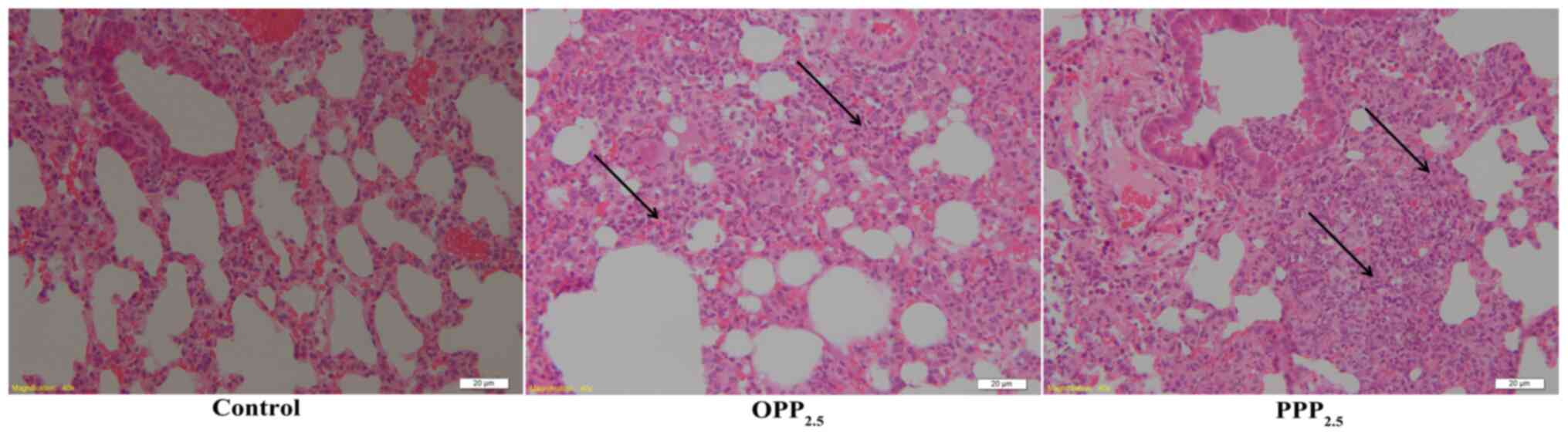
Histopathology
Lung tissue structure in the control group was
normal, with almost all alveolar walls intact. There were
interstitial inflammatory changes in the lungs of mice treated with
OPP2.5 or PPP2.5 (Fig. 3). These included a widening of the
alveolar septa and inflammatory cell infiltration. Inflammatory
responses did not differ between the OPP2.5 and
PPP2.5 groups.
Immune status
The flow cytometry gating scheme of the present
study is shown in Fig. 4A. The
number of CD45+ cells in the lungs from the treated
groups was higher compared with that from the control group
(Fig. 4B). Among these, the numbers
of interstitial macrophages (Fig.
4D) and neutrophils (Fig. 4E)
increased significantly in the treated groups compared with in the
control group. Additionally, the numbers of alveolar macrophages
(Fig. 4C), dendritic cells
(Fig. 4F) and monocytes (Fig. 4I) increased significantly in the
OPP2.5 group but not in the PPP2.5 group
compared with in the control group. The most accumulated dendritic
cells in the OPP2.5 group were Irf4+ cells
(Fig. 4H), not Batf3+
cells (Fig. 4G). The numbers of IM2
and 3 cells and eosinophils did not differ between the treated and
control groups (Fig. S1).
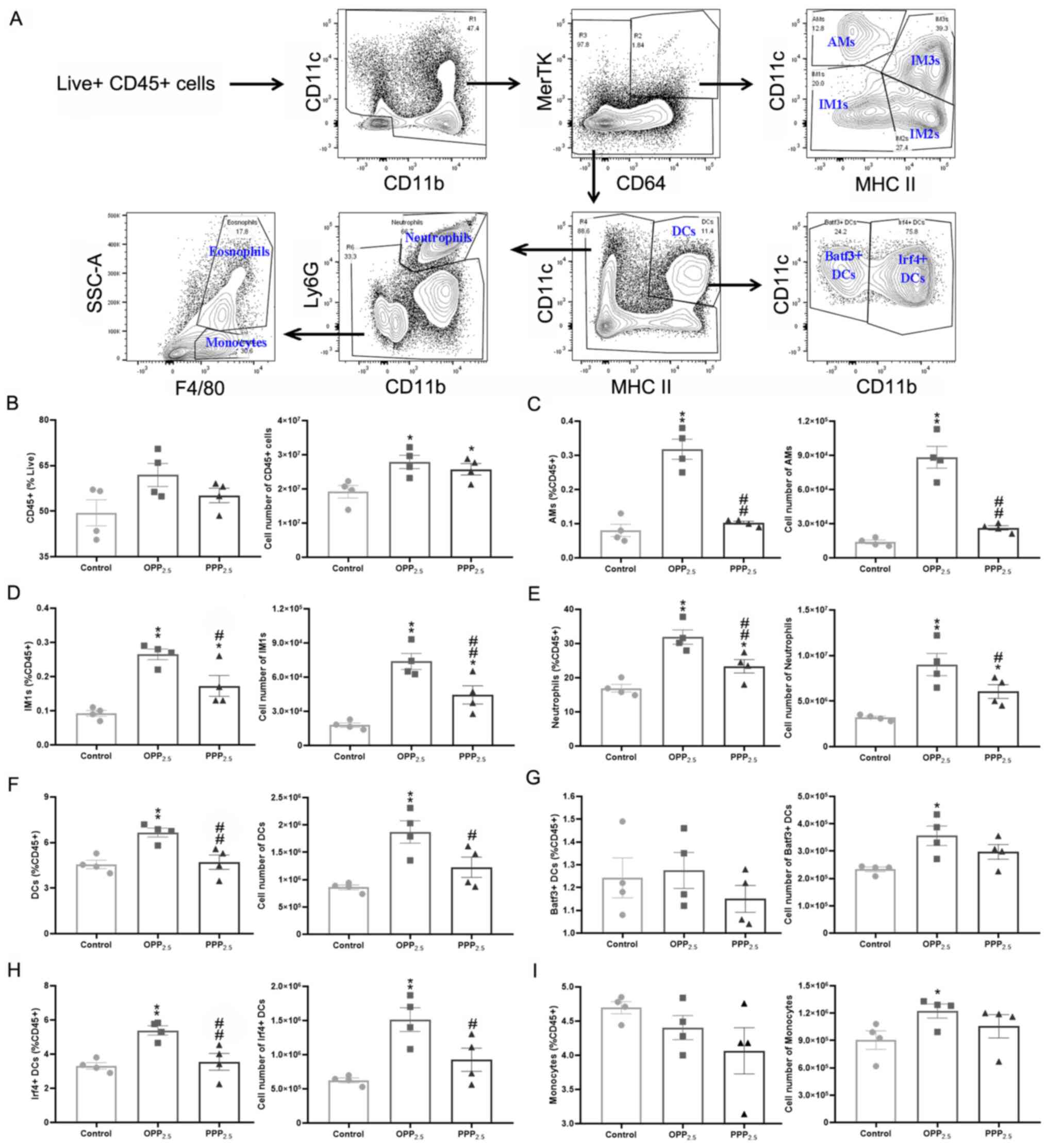 | Figure 4Comparison of pulmonary immune cell
numbers obtained by flow cytometry following exposure to
OPP2.5 particles (80 µg), PPP2.5 particles
(80 µg) or vehicle (50 µl sterile saline). (A)
Fluorescence-activated cell sorting gating strategy used to
identify pulmonary major immune cells. Live CD45+ cells
were gated and myeloid cells were gated on CD11c vs. CD11b. Total
myeloid cells were then plotted as MerTK vs. CD64 and the
MerTK+ CD64+ macrophage gate was plotted as
CD11c vs. MHC II to illustrate the AMs and IM1, IM2 and IM3. A
macrophage-deficient gate was plotted with CD11c and MHC II to
illustrate DCs, which were plotted as CD11c vs. CD11b to identify
Batf3+ and Irf4+ DCs. A
macrophage/DC-deficient gate was plotted as Ly6G vs. CD11b to
identify neutrophils (CD11b+ Ly6G+) and a
macrophage/DC/neutrophil-deficient gate was plotted as SSC vs.
F4/80 to identify eosinophils and monocytes. (B) The proportion of
CD45+ cells in living cells and the absolute number of
CD45+ cells in each sample from treated and control
groups. The proportion of (C) AMs, (D) IM1s, (E) neutrophils, (F)
DCs, (G) Batf3+, (H) Irf4+ and (I) monocytes
in CD45+ cells and their absolute number. The circles
represent the corresponding data of each mouse in the control
group, the squares represent the corresponding data of each mouse
in the OPP2.5 group, and the triangles represent the
corresponding data of each mouse in the PPP2.5 group.
Data are presented as mean ± standard error of the mean
(n=4/group). *P<0.05 and **P<0.01 vs.
control. #P<0.05 and ##P<0.01 vs.
OPP2.5 group. OPP2.5, original atmospheric
particulate matter with a diameter ≤2.5 µm; PPP2.5, pure
atmospheric particulate matter with a diameter ≤2.5 µm; CD, cluster
of differentiation; MHC, major histocompatibility complex; AMs,
alveolar macrophages; IM, interstitial macrophage; DC, dendritic
cell; SSC, side scatter. |
BALF biochemical analyses
BALF levels of ALT, ALB, creatinine, globulin, total
protein and ALP did not differ significantly between the treated
and control groups (data not shown). The activity of AST (Fig. 5A) and LDH (Fig. 5B) were significantly higher in BALF
from the treated groups compared with controls; however, there was
no significant difference between the OPP2.5 and
PPP2.5 groups. These results indicated that acute
inhalation of OPP2.5 or PPP2.5 damages
alveolar-capillary barriers and cell membranes in the lung.
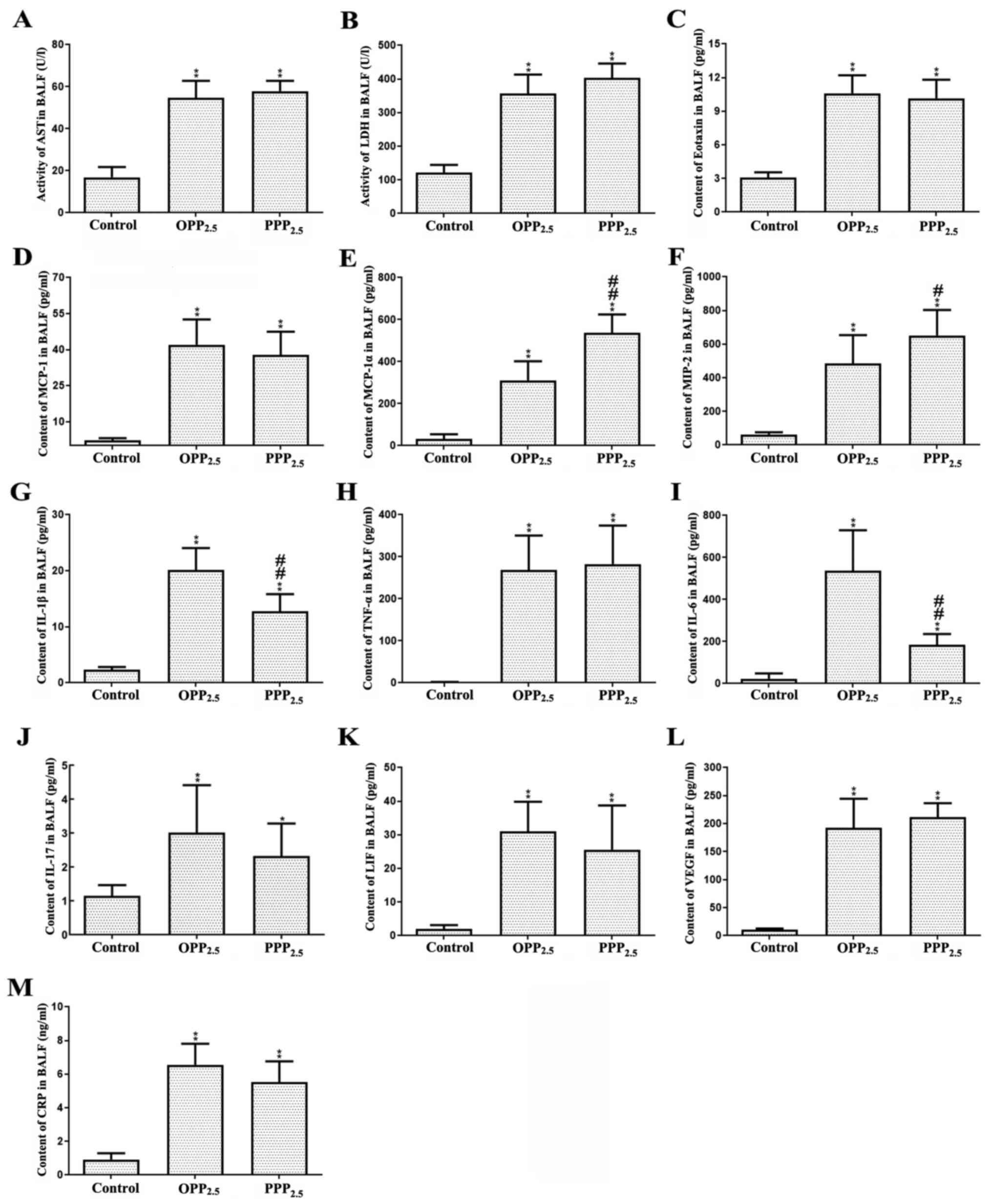 | Figure 5Levels of biochemical factors (A)
AST, (B) LDH, (C) eotaxin, (D) MCP-1, (E) MIP-1α, (F) MIP-2, (G)
IL-1β, (H) TNF- α, (I) IL-6, (J) IL-17, (K) LIF, (L) VEGF and (M)
CRP in BALF from mice treated with OPP2.5 particles (80
µg), PPP2.5 particles (80 µg) or vehicle (50 µl sterile
saline). Data are presented as mean ± standard error of mean
(n=8/group). *P<0.05 and **P<0.01 vs.
control. #P<0.05 and ##P<0.01 vs.
OPP2.5 group. AST, aspartate transaminase; LDH, lactate
dehydrogenase; MCP, monocyte chemoattractant protein; MIP,
macrophage inflammatory protein; IL, interleukin, TNF, tumor
necrosis factor; LIF, leukemia inhibitory factor; VEGF, vascular
endothelial growth factor; CRP, C-reactive protein; BALF,
bronchoalveolar lavage fluid; OPP2.5, original
atmospheric particulate matter with a diameter ≤2.5 µm;
PPP2.5, pure atmospheric particulate matter with a
diameter ≤2.5 µm. |
IL-1α levels in BALF did not differ between groups
(data not shown). Levels of eotaxin, MCP-1, MIP-1α, MIP-2, IL-1β,
TNF-α, IL-6, IL-17, LIF, VEGF and CRP were significantly higher in
the treated groups compared with controls (Fig. 5C-M). Levels of MIP-1α and MIP-2 were
higher in the PPP2.5 group compared with the
OPP2.5 group. Levels of IL-1β and IL-6 were higher in
the OPP2.5 group compared with the PPP2.5
group.
Discussion
OPP2.5 has more complex constituents than
PPP2.5 (27). The
composition of PPP2.5 is simple for relatively pure
solid particles, having almost no complex constituents adsorbed
into particle surfaces. The aim of the present study was to
determine whether pure solid PM2.5 exerts toxic effects
similar to those of original PM2.5 with its complex
constituents. The results demonstrated that mouse body weight
decreased to varying degrees following acute exposure, perhaps due
to the influence of anesthesia. However, treatment still decreased
body weight. Hematocrit levels in mice treated with
OPP2.5 were slightly elevated, suggesting minor
dehydration. Decreased activity of ALT, LDH and ALP in mice treated
with OPP2.5 and PPP2.5 and decreased ALB in
mice treated with OPP2.5 indicated that the treatment
may have induced mild malnutrition, which may explain the observed
weight loss.
Serum levels of cytokine MCP-1 were higher in the
OPP2.5 group compared with the control and
PPP2.5 groups. MCP-1 promotes monocyte adhesion to
vascular endothelial cells, which enables mononuclear cells to
mediate immune phagocytosis and scavenging (31). The results indicated that
OPP2.5 and PPP2.5 cause acute toxic effects
at the whole-body level, such as weight loss and mild malnutrition.
Furthermore, OPP2.5 causes minor dehydration and
systemic inflammation.
To assess lung toxicity, lung damage was evaluated
using histopathology, localized counts of major immune cells and
cytokines, and clinical parameters. Lung histopathology reported
inflammatory changes in the treated groups, with inflammatory cell
infiltration into the alveolar interstitial space. This was
confirmed by flow cytometry, which recorded numerous immune cells
(cluster of differentiation 45+ cells) in the lungs of
treated mice, particularly IM1 and neutrophils in both treated
groups and alveolar macrophages, dendritic cells and monocytes in
the OPP2.5 group. Neutrophils have been proposed to
mediate acute lung injury (32) and
IM1 form the branch of interstitial macrophages that influence
pulmonary fibrotic processes (33);
however, its function in PM-treated mice requires further study.
Alveolar macrophages usually inhabit the position of interface
between pulmonary mucosa and the external environment, sense
immunostimulation directly and maintain immune tolerance (33). Dendritic cells are important
regulators in the innate and adaptive immune responses (34). The results demonstrated that PM,
particularly OPP2.5, stimulate the innate immune
response in mice, leading to the accumulation of numerous immune
cells in the lung 24 h post-treatment.
Treatment with PM increased AST and LDH in BALF in
the present study. AST was primarily derived from plasma exudation
and reflects damage to the alveolar-capillary barrier. LDH, an
enzyme located in the cytoplasm, is released when cell membranes
are damaged or disintegrate following cell death (35). The results indicated that, to a
certain degree, cell membranes and parenchymal cells in the lung
were damaged by OPP2.5 and PPP2.5.
The levels of multiple pro-inflammatory
cytokines/chemokines increased in BALF following treatment in the
present study. Eotaxin is a chemoattractant that recruits
eosinophils (36) and MIP-1α
attracts lymphocytes, monocytes and neutrophils to an inflammatory
infection site and mediate immune cell infiltration, positioning
and activation in tissues (37).
MIP-2 specifically recruits neutrophils, macrophages and
lymphocytes to sites of inflammation following particle exposure
(38) and enhances neutrophil
participation in immune responses (16). This explains the observed
inflammatory cell infiltration via histopathology and flow
cytometry, which demonstrated the accumulation of macrophages and
neutrophils in both treated groups and monocytes in the
OPP2.5 group. Numerous eosinophils in the lung were not
reported and the higher levels of MIP-1α and MIP-2 in the
PPP2.5 group did not correspond to the expected
accumulation of macrophages, neutrophils and monocytes. This may be
due to eotaxin measured in BALF not being effectively released into
the bloodstream in the PPP2.5 group or that other
cytokines are involved in the chemotaxis of macrophages,
neutrophils and monocytes to the lung.
IL-6 is an important mediator of fever and of
acute-phase responses. It is also an anti-inflammatory factor that
inhibits pulmonary inflammation and fibrosis (39). TNF-α is involved in apoptosis, cell
differentiation and cell recruitment (40). As early biochemical mediators of
pulmonary inflammation (41), TNF-α
and IL-1 are involved in the initial stage of inflammation
(42) and are released by resident
macrophages to promote adhesion of circulating inflammatory cells
to the endothelium (42). These two
cytokines also induce the release of chemoattractant factors,
including IL-6, MIP-2 and MCP-1, all of which attract inflammatory
cells into the alveoli (16,41,43)
and enhance inflammatory and immune responses. IL-1α, IL-1β and
TNF-α increase mRNA expression of LIF (44), an anti-inflammatory factor that is
upregulated during peripheral inflammation (45). VEGF can bind to the VEGF receptor on
the surface of vessel endothelial cells, enhancing vascular
permeability and promoting the formation of blood vessels (46,47).
Upregulation of VEGF is often interpreted as a protective attempt
to restore tissue homeostasis (48,49).
Analyses of pro-inflammatory cytokines in BALF indicated extensive
inflammation in the lungs of mice treated with OPP2.5 or
PPP2.5 24 h post-treatment, with higher levels of IL-1β
and IL-6 in the OPP2.5 group. These findings were
consistent with the flow cytometry analysis, which recorded
numerous immune cells, including neutrophils and macrophages, in
the lungs of treated mice, particularly in the OPP2.5
group. However, due to precise regulatory networks, increased
levels of cytokines promoting inflammatory and immune responses
triggered a concomitant increase in the levels of LIF, which can
limit excessive responses (50).
Overall, the results of the current study for
OPP2.5 were consistent with those of previous reports,
suggesting that intratracheal instillation of PM in rodents induced
pulmonary and systemic inflammation (16,51-54).
Previous studies have demonstrated that water-soluble components
and metals such as manganese, chromium, titanium, iron, copper,
zinc, nickel and molybdenum in particulate matter may be associated
with the generation of reactive oxygen species (55,56).
Oxidative stress is considered to be positively associated with
induction of inflammation (57). In
the present study, PPP2.5, which is comprised of pure
solid particles without complex constituents adsorbed into the
surface, caused pulmonary inflammation in mice. However, the
systemic and pulmonary inflammatory responses were weaker than
those induced by OPP2.5. The reason may be that less
water-soluble components and metals were absorbed onto the surface
of PPP2.5, as demonstrated by a previous study (27). These results provide a new
perspective on the acute toxicity of PM and a reference for
evaluating other pollutants. The acute toxicity of pure solid
particles should be considered in tandem with that of the
constituents that adsorb onto the particle surface.
Additionally, the toxicities and constituents of
particles may be associated with wind direction, region or/and
season (58,59). These factors were not considered in
the present study; however, they have little effect on the
conclusion. However, one limitation of the present study was that
the normal daily inhaled dose of the mice at the beginning of the
study was not considered and should be investigated by future
studies. Another limitation was that the local expression level of
cytokines in the lungs was not assessed, and histological score was
not performed, which could be investigated in future studies.
Furthermore, the small number of mice in each group for flow
cytometry may also be a limitation, which can be improved in future
studies, and the toxicity of chronic exposure to pure solid
particles should be assessed in the future.
Supplementary Material
Pulmonary immune cell numbers counted
by flow cytometry following exposure to OPP2.5 particles
(80 μg), PPP2.5 particles (80 μg) or vehicle (50 μl
sterile saline). Percentage and absolute number of (A) IM2, (B) IM3
and (C) eosinophil cells in CD45+ cells. The circles
represent the corresponding data of each mouse in the control
group, the squares represent the corresponding data of each mouse
in the OPP2.5 group, and the triangles represent the
corresponding data of each mouse in the PPP2.5 group.
Data are presented as mean ± standard error of the mean
(n=4/group). **P<0.01 vs. control. OPP2.5,
original atmospheric particulate matter with a diameter ≤2.5 μm;
PPP2.5, pure atmospheric particulate matter with a
diameter ≤2.5 μm; IM, interstitial macrophage; CD, cluster of
differentiation.
Immunophenotyping antibodies.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the National Science
Foundation of China (grant no. 41205102).
Availability of data and materials
All data generated and/or analyzed during the
present study are included in this published article.
Authors' contributions
ZJ, ZW, LH and JL designed the present study. ZJ, LH
and WY performed the experiments. ZJ analyzed data and wrote the
manuscript draft. JL and ZW revised the final manuscript. ZW and LH
confirm the authenticity of all the raw data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
All animal experiments in the present study were
approved by the Animal Ethics Committee of the Academy of Military
and Medical Sciences (approval no. AMMS-13-2015-013).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Nemmar A, Hoet PHM, Vanquickenborne B,
Dinsdale D, Thomeer M, Hoylaerts MF, Vanbilloen H, Mortelmans L and
Nemery B: Passage of inhaled particles into the blood circulation
in humans. Circulation. 105:411–414. 2002.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Yoon S, Han S, Jeon KJ and Kwon S: Effects
of collected road dusts on cell viability, inflammatory response,
and oxidative stress in cultured human corneal epithelial cells.
Toxicol Lett. 284:152–160. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Jerrett M: Atmospheric science: The death
toll from air-pollution sources. Nature. 525:330–331.
2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Oberdorster G: Pulmonary effects of
inhaled ultrafine particles. Int Arch Occup Environ Health. 74:1–8.
2001.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Donaldson K, Stone V, Seaton A and MacNee
W: Ambient particle inhalation and the cardiovascular system:
Potential mechanisms. Environ Health Perspect. 109 (Suppl
4):S523–S527. 2001.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Lim SS, Vos T, Flaxman AD, Danaei G,
Shibuya K, Adair-Rohani H, Amann M, Anderson HR, Andrews KG, Aryee
M, et al: A comparative risk assessment of burden of disease and
injury attributable to 67 risk factors and risk factor clusters in
21 regions, 1990-2010: A systematic analysis for the global burden
of disease study 2010. Lancet. 380:2224–2260. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Pope CA III, Burnett RT, Thun MJ, Calle
EE, Krewski D, Ito K and Thurston GD: Lung cancer, cardiopulmonary
mortality, and long-term exposure to fine particulate air
pollution. JAMA. 287:1132–1141. 2002.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Hart JE, Spiegelman D, Beelen R, Hoek G,
Brunekreef B, Schouten LJ and van den Brandt P: Long-term ambient
residential traffic-related exposures and measurement
error-adjusted risk of incident lung cancer in the netherlands
cohort study on diet and cancer. Environ Health Perspect.
123:860–866. 2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Chen C, Zhu P, Lan L, Zhou L, Liu R, Sun
Q, Ban J, Wang W, Xu D and Li T: Short-term exposures to PM2.5 and
cause-specific mortality of cardiovascular health in China. Environ
Res. 161:188–194. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Ulrich MM, Alink GM, Kumarathasan P,
Vincent R, Boere AJ and Cassee FR: Health effects and time course
of particulate matter on the cardiopulmonary system in rats with
lung inflammation. J Toxicol Environ Health A. 65:1571–1595.
2002.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Muller B, Seifart C and Barth PJ: Effect
of air pollutants on the pulmonary surfactant system. Eur J Clin
Invest. 28:762–777. 1998.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Burch WM: Passage of inhaled particles
into the blood circulation in humans. Circulation. 106:e141–142;
author reply e141-142. 2002.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Du Y, Xu X, Chu M, Guo Y and Wang J: Air
particulate matter and cardiovascular disease: The epidemiological,
biomedical and clinical evidence. J Thorac Dis. 8:E8–E19.
2016.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Lee BJ, Kim B and Lee K: Air pollution
exposure and cardiovascular disease. Toxicol Res. 30:71–75.
2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Obot CJ, Morandi MT, Beebe TP, Hamilton RF
and Holian A: Surface components of airborne particulate matter
induce macrophage apoptosis through scavenger receptors. Toxicol
Appl Pharmacol. 184:98–106. 2002.PubMed/NCBI
|
|
16
|
Mantecca P, Farina F, Moschini E,
Gallinotti D, Gualtieri M, Rohr A, Sancini G, Palestini P and
Camatini M: Comparative acute lung inflammation induced by
atmospheric PM and size-fractionated tire particles. Toxicol Lett.
198:244–254. 2010.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Jiao ZG, Fu XL, Wen ZB, Li JS, Li N, Zhang
K, Wang J and Hu LF: Toxicological study at imflammatory factors
and DNA damages effects of Beijing atmospheric PM2.5 and
its different fractions to pulmonary epithelial cells A549 of
human. China Environ Sci. 1579–1588. 2016.(In Chinese).
|
|
18
|
Hiura TS, Kaszubowski MP, Li N and Nel AE:
Chemicals in diesel exhaust particles generate reactive oxygen
radicals and induce apoptosis in macrophages. J Immunol.
163:5582–5591. 1999.PubMed/NCBI
|
|
19
|
Ghio AJ, Stonehuerner J, Dailey LA and
Carter JD: Metals associated with both the water-soluble and
insoluble fractions of an ambient air pollution particle catalyze
an oxidative stress. Inhal Toxicol. 11:37–49. 1999.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Prahalad AK, Soukup JM, Inmon J, Willis R,
Ghio AJ, Becker S and Gallagher JE: Ambient air particles: Effects
on cellular oxidant radical generation in relation to particulate
elemental chemistry. Toxicol Appl Pharmacol. 158:81–91.
1999.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Rumelhard M, Ramgolam K, Auger F, Dazy AC,
Blanchet S, Marano F and Baeza-Squiban A: Effects of PM2.5
components in the release of amphiregulin by human airway
epithelial cells. Toxicol Lett. 168:155–164. 2007.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Xu H, Wang X, Pöschl U, Feng S, Wu D, Yang
L, Li S, Song W, Sheng G and Fu J: Genotoxicity of total and
fractionated extractable organic matter in fine air particulate
matter from urban Guangzhou: Comparison between haze and nonhaze
episodes. Environ Toxicol Chem. 27:206–212. 2008.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Liu FY, Ding MY, Wang FF and Li J:
Cytotoxicity of different compositions of coal-fired
PM2.5 on vascular endothelial cells. Res Environ Sci.
24:684–690. 2011.(In Chinese).
|
|
24
|
Cao Q, Qian XL, Zhang S and Song WM:
Cytotoxicity of soluble and insoluble components of atmospheric
fine particles. Acta Scientiae Circumstantiae. 28:1167–1172.
2008.(In Chinese).
|
|
25
|
Pozzi R, De Berardis B, Paoletti L and
Guastadisegni C: Inflammatory mediators induced by coarse
(PM2.5-10) and fine (PM2.5) urban air particles in RAW 264.7 cells.
Toxicology. 183:243–254. 2003.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Qian XL, Song WM and Cao Q: Oxidative
injury of alveolar epithelium cell ll rs induced by coaine carbon
black. J Toxicol. 22:14–16. 2008.
|
|
27
|
Jiao ZG, Li JY, Wen ZB, Li J, Gao J, Li N
and Wang H: Chemical and biological components analysis of
PM2.5 and its different fractions in summer atmosphere
in Beijing urban areas. Chin J Environ Engineering. 5009–5015.
2016.(In Chinese).
|
|
28
|
He M, Ichinose T, Yoshida S, et al: PM2.
5. 5re in Beijing urban areas. Chinese journal of f inflammatory
response in macrophages and type II alveolar cells. J Appl Toxicol.
37:1203–1218. 2017.
|
|
29
|
Yu YR, O'Koren EG, Hotten DF, Kan MJ,
Kopin D, Nelson ER, Que L and Gunn MD: A protocol for the
comprehensive flow cytometric analysis of immune cells in normal
and inflamed murine non-lymphoid tissues. PLoS One.
11(e0150606)2016.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Gibbings SL, Thomas SM, Atif SM, McCubbrey
AL, Desch AN, Danhorn T, Leach SM, Bratton DL, Henson PM, Janssen
WJ and Jakubzick CV: Three unique interstitial macrophages in the
murine lung at steady state. Am J Respir Cell Mol Biol. 57:66–76.
2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Gerszten RE, Garcia-Zepeda EA, Lim YC,
Yoshida M, Ding HA, Gimbrone MA Jr, Luster AD, Luscinskas FW and
Rosenzweig A: MCP-1 and IL-8 trigger firm adhesion of monocytes to
vascular endothelium under flow conditions. Nature. 398:718–723.
1999.PubMed/NCBI View
Article : Google Scholar
|
|
32
|
Sapoznikov A, Gal Y, Falach R, Sagi I,
Ehrlich S, Lerer E, Makovitzki A, Aloshin A, Kronman C and Sabo T:
Early disruption of the alveolar-capillary barrier in a
ricin-induced ARDS mouse model: Neutrophil-dependent and
-independent impairment of junction proteins. Am J Physiol Lung
Cell Mol Physiol. 316:L255–L268. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Byrne AJ, Maher TM and Lloyd CM: Pulmonary
macrophages: A new therapeutic pathway in fibrosing lung disease?
Trends Mol Med. 22:303–316. 2016.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Greter M, Helft J, Chow A, Hashimoto D,
Mortha A, Agudo-Cantero J, Bogunovic M, Gautier EL, Miller J,
Leboeuf M, et al: GM-CSF controls nonlymphoid tissue dendritic cell
homeostasis but is dispensable for the differentiation of
inflammatory dendritic cells. Immunity. 36:1031–1046.
2012.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Drent M, Cobben NA, Henderson RF, Wouters
EF and van Dieijen-Visser M: Usefulness of lactate dehydrogenase
and its isoenzymes as indicators of lung damage or inflammation.
Eur Respir J. 9:1736–1742. 1996.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Kim GH, Park YS, Jung KW, Kim M, Na HK,
Ahn JY, Lee JH, Kim DH, Choi KD, Song HJ, et al: An increasing
trend of eosinophilic esophagitis in korea and the clinical
implication of the biomarkers to determine disease activity and
treatment response in eosinophilic esophagitis. J
Neurogastroenterol Motil. 25:525–533. 2019.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Pi XM, Li ZZ, Ma YR and Li DW: MIP-1α
enhances trans-endothelial migration of CIK cells in lung cancer
patients with brain metastasis. J China Med University. 45:141–144.
2016.(In Chinese).
|
|
38
|
Driscoll KE, Hassenbein DG, Carter JM,
Kunkel SL, Quinlan TR and Mossman BT: TNF alpha and increased
chemokine expression in rat lung after particle exposure. Toxicol
Lett. 82-83:483–489. 1995.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Xu DQ, Huang NH, Wang Q and Liu HG: Study
of ambient PM2.5 on the influence of the inflammation
injury and the immune function of subchronic exposure rats. Wei
Sheng Yan Jiu. 37:423–428. 2008.PubMed/NCBI(In Chinese).
|
|
40
|
Akash MSH, Rehman K and Liaqat A: Tumor
necrosis factor-alpha: Role in development of insulin resistance
and pathogenesis of type 2 diabetes mellitus. J Cell Biochem.
119:105–110. 2018.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Henderson RF: Use of bronchoalveolar
lavage to detect respiratory tract toxicity of inhaled material.
Exp Toxicol Pathol. 57 (Suppl 1):S155–S159. 2005.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Finkelstein JN, Johnston C, Barrett T and
Oberdorster G: Particulate-cell interactions and pulmonary cytokine
expression. Environ Health Perspect. 105 (Suppl 5):S1179–S1182.
1997.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Tessier PA, Naccache PH, Clark-Lewis I,
Gladue RP, Neote KS and McColl SR: Chemokine networks in vivo:
Involvement of C-X-C and C-C chemokines in neutrophil extravasation
in vivo in response to TNF-alpha. J Immunol. 159:3595–3602.
1997.PubMed/NCBI
|
|
44
|
Wetzler M, Talpaz M, Lowe DG, Baiocchi G,
Gutterman JU and Kurzrock R: Constitutive expression of leukemia
inhibitory factor RNA by human bone marrow stromal cells and
modulation by IL-1, TNF-alpha, and TGF-beta. Exp Hematol.
19:347–351. 1991.PubMed/NCBI
|
|
45
|
Liu J, Yu H and Hu W: LIF is a new p53
negative regulator. J Nat Sci. 1(e131)2015.PubMed/NCBI
|
|
46
|
Wakabayashi Y, Iwaya M, Akita M, Takeuchi
W, Yamazaki K and Iijima A: Pulmonary tumor thrombotic
microangiopathy caused by urothelial carcinoma expressing vascular
endothelial growth factor, platelet-derived growth factor, and
osteopontin. Intern Med. 55:651–656. 2016.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Zhang RP and Guo PF: Study progress of
vascular endothelial growth factor. Med Recapitulate. 14:2258–2260.
2008.(In Chinese).
|
|
48
|
Lahm T, Crisostomo PR, Markel TA, Wang M,
Lillemoe KD and Meldrum DR: The critical role of vascular
endothelial growth factor in pulmonary vascular remodeling after
lung injury. Shock. 28:4–14. 2007.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Campbell AI, Zhao Y, Sandhu R and Stewart
DJ: Cell-based gene transfer of vascular endothelial growth factor
attenuates monocrotaline-induced pulmonary hypertension.
Circulation. 104:2242–2248. 2001.PubMed/NCBI View Article : Google Scholar
|
|
50
|
West NR: Coordination of immune-stroma
crosstalk by il-6 family cytokines. Front Immunol.
10(1093)2019.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Kodavanti UP, Schladweiler MC, Ledbetter
AD, Hauser R, Christiani DC, McGee J, Richards JR and Costa DL:
Temporal association between pulmonary and systemic effects of
particulate matter in healthy and cardiovascular compromised rats.
J Toxicol Environ Health A. 65:1545–1569. 2002.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Stoeger T, Reinhard C, Takenaka S,
Schroeppel A, Karg E, Ritter B, Heyder J and Schulz H: Instillation
of six different ultrafine carbon particles indicates a surface
area threshold dose for acute lung inflammation in mice. Environ
Health Perspect. 114:328–333. 2006.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Upadhyay S, Ganguly K, Stoeger T,
Semmler-Bhenke M, Takenaka S, Kreyling WG, Pitz M, Reitmeir P,
Peters A, Eickelberg O, et al: Cardiovascular and inflammatory
effects of intratracheally instilled ambient dust from Augsburg,
Germany, in spontaneously hypertensive rats (SHRs). Part Fibre
Toxicol. 7(27)2010.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Sun X, Wei H, Young DE, Bein KJ,
Smiley-Jewell SM, Zhang Q, Fulgar CCB, Castañeda AR, Pham AK, Li W
and Pinkerton KE: Differential pulmonary effects of wintertime
California and China particulate matter in healthy young mice.
Toxicol Lett. 278:1–8. 2017.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Shuster-Meiseles T, Shafer MM, Heo J,
Pardo M, Antkiewicz DS, Schauer JJ, Rudich A and Rudich Y:
ROS-generating/ARE-activating capacity of metals in roadway
particulate matter deposited in urban environment. Environ Res.
146:252–262. 2016.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Spagnolo AM, Ottria G, Perdelli F and
Cristina ML: Chemical characterisation of the coarse and fine
particulate matter in the environment of an underground railway
system: Cytotoxic effects and oxidative stress-a preliminary study.
Int J Environ Res Public Health. 12:4031–4046. 2015.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Zeng L, Lin L, Peng Y, Yuan D, Zhang S,
Gong Z and Xiao W: l-Theanine attenuates liver aging by inhibiting
advanced glycation end products in d-galactose-induced rats and
reversing an imbalance of oxidative stress and inflammation. Exp
Gerontol. 131(110823)2019.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Kamal AS, Rohr AC, Mukherjee B, Morishita
M, Keeler GJ, Harkema JR and Wagner JG: PM2. 5-induced changes in
cardiac function of hypertensive rats depend on wind direction and
specific sources in Steubenville, Ohio. Inhal Toxicol. 23:417–430.
2011.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Cho CC, Hsieh WY, Tsai CH, Chen CY, Chang
HF and Lin CS: In vitro and in vivo experimental studies of PM2. 5
on disease progression. Int J Environ Res Public Health.
15(1380)2018.PubMed/NCBI View Article : Google Scholar
|