Introduction
Cushing's syndrome (CS) is considered a rare and
challenging disorder (1,2). It can be classified by the level of
adrenocorticotropic hormone (ACTH) in two major subtypes:
ACTH-independent with autonomous production of corticoid hormones,
and ACTH-dependent with peripheral hyperproduction of corticoid
hormones which is dictated by the pituitary gland through
hypersecretion of ACTH (3). It is
highly important to exclude exogenous causes, more specifically the
administration of steroid hormones. There are three major
situations which lead to CS: Adrenal adenomas, adrenal carcinomas,
and adrenal hyperplasia, excluding a pituitary origin of the
syndrome (4,5).
In all these situations, the standard treatment is
surgical resection of the adenomatous gland when there is
unilateral involvement or bilateral suprarenalectomy, when both
glands have functional active adenomas (6). Bilateral adrenalectomy is associated
with a decrease in the patient's quality of life, requiring
mineralocorticoid and glucocorticoid replacement therapy.
Therefore, effective investigations are crucial to diagnose
preoperatively the origin of hyperproduction of the adrenal gland.
The computed tomography scan can identify bilateral adrenal
adenomas, with three possible scenarios: Hyperproductive bilateral
cortisol tumors, adrenal macronodular hyperplasia or
hyperproductive unilateral cortisol tumor, and a non-functional
contralateral tumor (6). In the
case that primary hyperaldosteronism adenoma is suspected, adrenal
scintigraphy is considered a safe and effective diagnostic solution
(7).
Currently, the gold standard diagnostic tool for
patients with bilateral adrenal adenoma and ACTH-independent CS is
bilateral adrenal venous sampling and the dosage of cortisol
levels. Value comparison provides definitive results in 99.9% of
cases (8). This diagnostic
procedure is an invasive one that involves a number of risks for
the patient and limitations for the physician. The method is based
on left adrenal vein cannulation which is difficult intervention
due to the fact that the vein is often narrow with a sinuous route
being difficult to locate.
Research methods
This paper exemplifies the importance of this
diagnostic procedure through a clinical case described in the next
paragraph. To perform a pertinent review of the literature on the
described topic, successive searches were obtained from the PubMed
database between 1 January, 1995 and 1 October, 2020 using the
keywords: ‘Adrenal vein sampling’ AND ‘adrenal mass imaging’ AND
‘ACTH non-dependent Cushing syndrome’. The search was refined for
original articles and rare clinical cases written only in English.
A total of 43 articles were identified. After manual selection that
met the PICO criteria, 13 articles were eliminated as such:
Incomplete data (4 articles), 7 articles did not have the full text
available and 2 articles did not incorporate a study on bilateral
suprarenal adenomas and as such were not introduced in the
analysis. A total of 30 articles were selected and 22 were selected
for discussion, which will be described in detail subsequently in
the study.
The study was conducted according to the World
Medical Association Declaration of Helsinki, using a protocol
approved by the local Bioethics Committee from ‘Prof. Dr. Agrippa
Ionescu’ Clinical Emergency Hospital (Bucharest, Romania). The
patient previously signed informed written consent about
hospitalization, treatment and a future publication of data.
Case presentation
This is the case of a 32-year-old female patient who
presented to the hospital for progressive weight gain over the
previous 6 months. The clinical examination identified an abdominal
distribution of adipose tissue, cutaneous fragility, stretch marks
on the abdomen and lower limbs, hirsutism, and oligomenorrhea.
Common laboratory tests confirmed the presence of
leukocytosis with neutrophilia and hypoglycemia (unusual),
hypercholesterolemia and D-vitamin insufficiency, which are
characteristic (9).
The hormonal profile was obtained: Blood cortisol
values, 23.05 µg/dl (6.7-22.6); cortisol values at 24:00 h, 4.56
µg/dl. The circadian rate of cortisol hormone secretion was
maintained. ACTH value was 1.21 pg/ml and urinary free cortisol
(UFC) value was 1,448 nmol/24 h [52.48 µg/dl]. The values obtained
after the 1 mg overnight dexamethasone test were: Cortisol, 10.47
µg/dl [288.9 nmol/l]; follicle-stimulating hormone (FSH), 5.72
mUI/ml; luteinizing hormone (LH), 6.04 mUI/ml; estradiol, 28.6
pg/ml and prolactin (PRL), 13.16 ng/ml, indicating intact
hypophyseal ovarian axis. Osteopenia was also confirmed.
After the 24-h blood pressure monitoring was
performed, the presence of a dipper profile was confirmed: The
average diurnal value was 126/80 mmHg and nocturnal value of 100/71
mmHg.
A glucose tolerance test was performed which
revealed glycemia value of 75 mg/dl at 2 h. Echocardiography
excluded the presence of atrial myxoma or other cardiovascular
abnormalities.
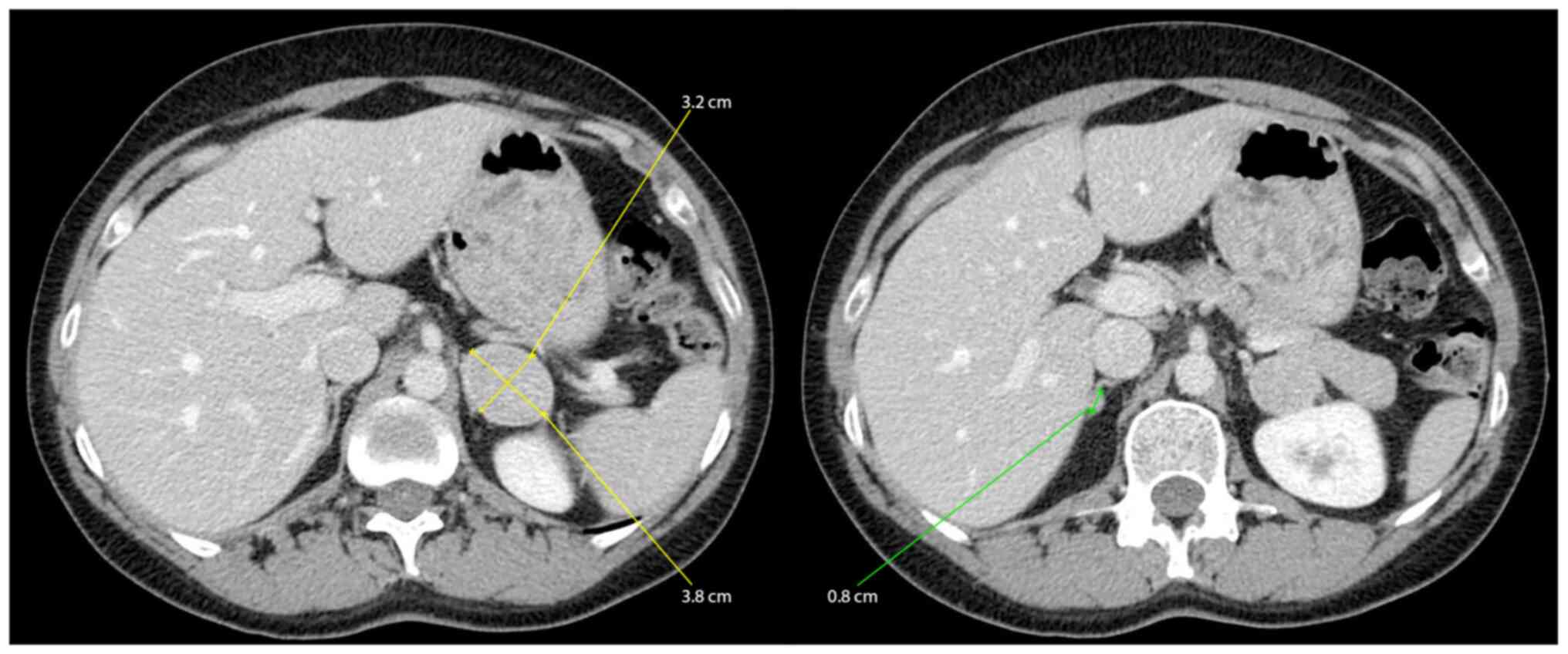
The abdominal contrast-enhanced computed tomography
scan showed nodular lesions in the adrenal glands-7 mm on the right
and 37 mm on the left which were probably adenoids with low lipid
substrate (32 HU-Hounsfield unit densities) (Fig. 1).
Subsequent head magnetic resonance imaging showed
the hypophysis with low 3-4 mm hypocaptant areas in the right and
left adenohypophysis with non-homogeneous loading with intravenous
contrast (possibly suggesting microadenomas).
The diagnosis of an ACTH-independent CS was
confirmed due to adrenal adenomas.
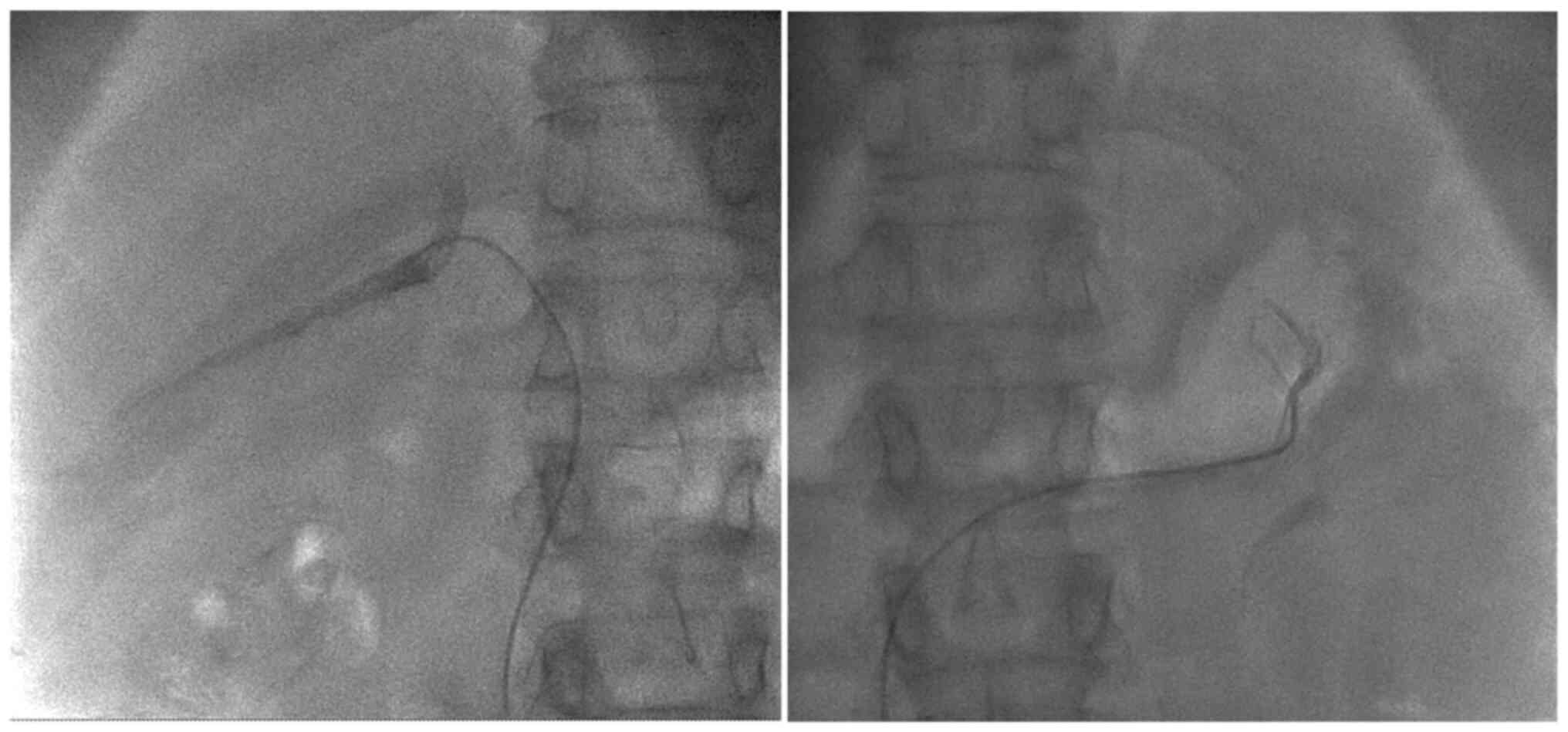
In order to accurately identify the hyperproductive
adenoma for surgical resection, supra-selective hormone dosage from
both of the suprarenal veins was obtained and the lateralization
index was calculated. Firstly, the right femoral vein was used as
an entry point, after that the right suprarenal vein was
catheterized followed by the left suprarenal vein and blood samples
for hormone dosage were obtained (Fig.
2).
The following cortisol values were confirmed: Right
adrenal vein, 5.91 µg/dl and left adrenal vein, >60 µg/dl. These
values confirmed the ACTH-independent CS due to a left adrenal
adenoma. Surgery was decided and a left laparoscopic adrenalectomy
was performed in January, 2018 (Table
I).
 | Table IPostoperative cortisol values. |
Table I
Postoperative cortisol values.
| Date | Cortisol (133-537
nmol/l) |
|---|
| 02.2018 | 8 nmol/l=0.28
µg/dl |
| 02.2018 | 106.3 nmol/l=3.85
µg/dl |
| 03.2018 | 141.7 nmol/l=5.13
µg/dl |
| 03.2018 | 148.4 nmol/l=5.37
µg/dl |
| 04. 2018 | 272.2 nmol/l=9.86
µg/dl |
| 05.2018 Stop
Prednisone | 360 nmol/l=13.04
µg/dl |
The 1-year follow-up was favorable. The patient was
started on supplements with vitamin D and the osteoporosis was
recovered completely.
Current diagnostic criteria and surgical
treatment options
The use of high-resolution imaging has led to an
increased rate of incidental detection of unilateral adrenal
masses, which most commonly are benign non-functioning adrenal
adenomas. Patients with bilateral adrenal masses are rarely
encountered. Patients with bilateral adrenal tumors can present
different clinical manifestations ranging from asymptomatic to
multi-organ dysfunctions (10).
In the patient with ACTH-independent Cushing's
syndrome, CT examination is the initial imaging procedure with
first intention. Abdominal MRI should be conducted when there is
ambiguity as it is not cost-effective. A retrospective study that
included 99 patients (48 women and 51 men) reported the imaging
characteristics of their 122 adrenal masses (10). Patients were either operated on to
obtain a tissue sample from the tumors or were enrolled in a
follow-up program with regular CT evaluations (10). CT scan images were recorded from all
the patients, both native (without intravenous contrast substance)
and after administration of 120 ml of intravenous contrast
substance (10). Subsequently, the
images were analyzed after mean attenuation, calculating relative
percentage washout (RPW) and absolute percentage washout (APW)
(10).
The specificity and sensitivity of identifying
malignant tumors with these criteria were 98 and 100%,
respectively. The attenuation of 43 HU was used as the threshold to
distinguish benign from malignant lesions. Thus, the surgical
approach must be guided by imaging suspicion (10).
Adrenal hyperplasia is a common cause of this
disease (11). This is followed by
infection, metastasis or lymphoma, while bilateral tumors usually
evolve as pheochromocytomas (12,13).
Tian et al highlighted the etiologies of bilateral adrenal
lesions in a study performed on 260 patients. Authors of that study
showed that bilateral adrenal hyperplasia was identified in 75
cases, followed in frequency by bilateral adrenal adenomas,
metastatic carcinoma, discordant bilateral adrenal lesions,
bilateral pheochromocytomas, among others. A mere 5 patients were
diagnosed with CS which consisted of only 2% of all cases (12). Zhou et al described in their
study 18 patients with bilateral adrenal masses from 565 patients
with adrenal tumors. Of the 18 patients, only 1 patient presented
CS (14).
The therapeutic management of patients with
bilateral adrenal masses and CS is challenging for the
endocrinologist, but also for the general surgeon. Surgical
excision of the adrenal glands must be avoided in the absence of a
certain diagnosis. Macronodular bilateral adrenal hyperplasia in a
patient with ACTH-independent Cushing syndrome is one of the rarest
causes of cortisol hyperproduction (5).
When a patient is diagnosed with bilateral adrenal
masses, it is crucial to determine whether both have hormonal
activity. High-resolution imaging does not bring important data
regarding the differentiation between a hyper-functional adenoma
and a non-functional one. Direct hormonal dosing from the adrenal
vein has been reported as an effective way to differentiate these
tumor masses in ACTH-independent Cushing syndrome (15).
Less than 2% of all cases of hypercorticism exist in
the form of two concomitant adrenal mass tumors, therefore the
possibility that only one of the tumors was responsible for the
Cushing syndrome was high in our patient (16).
However, improvements have been made and The Society
of Endocrinology recommends ultra-selective hormone dosage of blood
obtained directly from both the adrenal veins as a standard
diagnostic technique when such cases are encountered (5). However, few studies have described the
utility and effectiveness of this technique. The vast majority of
published articles on this subject are case studies, while major
prospective randomized trials are lacking.
However, Funder et al demonstrated the
effectiveness of this diagnostic technique, using a relatively
small batch of only 10 patients. Their study made a reference to
the threshold values for cortisol dosage. Thus the ratio between
cortisol values from the adrenal vein (AV) and peripheral vein (PV)
>6.5 is highly suggestive of a hyperproductive adenoma, whereas
a ratio value <3.3 is consistent with the presence of a
non-functional nodule. Regarding the percentage of lateralization,
those authors identified that the presence of a gradient >2.3
suggests the presence of a unilateral hyperfunctional tumor while
the presence of a gradient ≤2 raises the suspicion of
hyperproductive bilateral nodules (16).
The results of this groundbreaking study have
recently been questioned by Acharya et al (17) who, using criteria of Funder et
al (16), failed to confirm the
lateralization of adrenal adenomas, probably due to patient
selection criteria as mentioned in the study (17). Instead, the group focused on the
morphology identified at the computer tomography scan, and
surgically excised accordingly the larger suprarenal multinodular
gland, thus avoiding a life-altering bilateral suprarenalectomy.
The final results were satisfactory. Identical results were
obtained and discussed by Iacobone et al (18) and Debillon et al (19). From our point of view, long-term
confirmation of the effectiveness of this method is required;
however, the authors from the aforementioned studies did not report
a proper follow-up. Additionally, it is imperative to study the
improvement of the quality of life of the patients (20).
The contraindications of this procedure are
coagulation disorders (21), blood
hypertension, contrast substance allergy, pregnancy and kidney
failure (22). The association
between Cushing's syndrome and chronic kidney disease (CKD) is
known and accepted by researchers (23), and is presented in many studies. The
presence of blood hypertension leads to hypertensive nephrophathy
(24,25).
Unilateral adrenal venous sampling has been employed
by multiple endocrinology societies as the optimal diagnostic tool
when bilateral adenomas are encountered and associated with an
ACTH-independent CS (16,26).
Scintigraphy has a limited usage as frequently both
of the adenomas capture the tracer and the clinician cannot
distinguish which of them needs resecting (27).
In our case, the resection was performed by a
multidisciplinary team, which encompassed a general and vascular
surgeon. Postoperatively, the parietal wounds after laparoscopy
were treated with a gel with polyhexanidine, due to its antiseptic
properties (28).
Although the adrenal venous sampling technique is
reserved for diagnosis it is nonetheless an invasive procedure.
Thus, attention needs to be paid to the possible immediate
complications and the medical staff should be prepared if they
arise (29).
Complications may be severe, so it is highly
important to have a vascular surgery department in the center where
the investigation is performed. The complications encountered when
this procedure is performed include hemorrhage with retroperitoneal
hematoma, adrenal infarction and hematoma at the puncture site
(30,31).
The risk of rupturing the adrenal vein during this
procedure is <1% (32).
In conclusion, when bilateral adrenal tumors are
encountered a differential diagnosis is difficult to obtain. In the
case of an associated ACTH-independent Cushing syndrome,
scintigraphy has a limited utility. Hormone dosage from venous
blood of both adrenal veins is a key step in confirming the
presence of a lateral secretion of cortisol. Due to the rarity of
this pathology, it would be necessary to have an international
database in order to obtain data with the statistical value that
would allow optimization of the therapeutic management of these
patients. In our case, the intervention was performed by a
multidisciplinary team, general and vascular surgeons.
Postoperatively, the parietal wounds after laparoscopy were treated
with a gel with polyhexanidine, due to its antiseptic properties.
Although this technique is reserved for diagnosis it is nonetheless
an invasive procedure, and attention should be paid to the possible
immediate complications and the medical staff should be prepared if
they arise.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
RT, RIS, CRJ and AT made major contribution to the
conception and design of the study. RIS, AA, BS, LFT, AT, EM, CRJ
and OS, provided study material or patients, collected the data and
analyzed the datasets. RIS, RT, LFT, AA, BS, EM, AT and OS wrote
the manuscript. RT, AT, RIS and CRJ confirmed the authenticity of
all the raw data and RT, RIS and CRJ critically revised the
manuscript. All authors read and approved the final manuscript. The
contribution of all the authors on this article is greatly valued
and appreciated.
Ethics approval and consent to
participate
The study was conducted according to the World
Medical Association Declaration of Helsinki, using a protocol
approved by the local Bioethics Committee from ‘Prof. Dr. Agrippa
Ionescu’ Clinical Emergency Hospital (Bucharest, Romania).
Patient consent for publication
The patient previously signed informed written
consent about hospitalization, treatment and a future publication
of data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Pappachan JM, Hariman C, Edavalath M,
Waldron J and Hanna FW: Cushing's syndrome: A practical approach to
diagnosis and differential diagnoses. J Clin Pathol. 70:350–359.
2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Sharma ST, Nieman LK and Feelders RA:
Cushing's syndrome: Epidemiology and developments in disease
management. Clin Epidemiol. 7:281–293. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Stewart PM: The adrenal cortex. In:
Kronenberg HM, Melmed S, Polonsky KS, Larsen PR (eds): Williams
textbook of endocrinology. 11th edition. Saunders Elsevier,
Philadelphia, PH, pp445-503, 2008.
|
|
4
|
Dinneen SF, Carney JA, Carpenter PC, Grant
CS and Young WF Jr: Acth-independent Cushing's syndrome: Bilateral
cortisol-producing adrenal adenomas. Endocr Pract. 1:77–81.
1995.PubMed/NCBI View Article : Google Scholar
|
|
5
|
De Venanzi A, Alencar GA, Bourdeau I,
Fragoso MC and Lacroix A: Primary bilateral macronodular adrenal
hyperplasia. Curr Opin Endocrinol Diabetes Obes. 21:177–184.
2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Domino JP, Chionh SB, Lmanto D, Katara AN,
Rauff A and Cheah WK: Laparoscopic partial adrenalectomy for
bilateral cortisol-secreting adenomas. Asian J Surg. 30:154–157.
2007.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Yasuda A, Seki T, Ito K, Takagi A,
Watanabe D, Nakamura N, Hanai K, Terachi T, Maekawa T, Sasano H and
Fukagawa M: A rare case of Cushing's syndrome due to bilateral
adrenocortical adenomas. Tokai J Exp Clin Med. 39:158–165.
2014.PubMed/NCBI
|
|
8
|
Stewart PM and Allolio B: Adrenal vein
sampling for primary aldosteronism: Time for a reality check. Clin
Endocrinol (Oxf). 72:146–148. 2010.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Stanescu AMA, Grajdeanu IV, Iancu MA,
Pantea Stoian A, Bratu OG, Socea B, Socea LI and Diaconu CC:
Correlation of oral vitamin D administration with the severity of
psoriasis and the presence of metabolic syndrome. Rev Chim.
69:1668–1672. 2018.
|
|
10
|
Blake MA, Kalra MK, Sweeney AT, Lucey BC,
Maher MM, Sahani DV, Halpern EF, Mueller PR, Hahn PF and Boland GW:
Distinguishing benign from malignant adrenal masses: Multi-detector
row CT protocol with 10-minute delay. Radiology. 238:578–585.
2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lomte N, Bandgar T, Khare S, Jadhav S,
Lila A, Goroshi M, Kasaliwal R, Khadilkar K and Shah NS: Bilateral
adrenal masses: A single-centre experience. Endocr Connect.
5:92–100. 2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Tian Q, Zhang ST, Gao HW, Lu R, Yang J,
Wang HN and Hong TP: The etiological analysis of 260 hospitalized
cases with bilateral adrenal lesions. Zhonghua Yi Xue Za Zhi.
99:1246–1250. 2019.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
13
|
Bratu OG, Marcu RD, Socea B, Neagu TP,
Diaconu CC, Scarneciu I, Turcu FL, Radavoi GD, Bratila E, Berceanu
C and Spinu AD: Immunohistochemistry particularities of
retroperitoneal tumors. Rev Chim. 69:1813–1816. 2018.
|
|
14
|
Zhou J, Ye D, Wu M, Zheng F, Wu F, Wang Z
and Li H: Bilateral adrenal tumor: Causes and clinical features in
eighteen cases. Int Urol Nephrol. 41:547–551. 2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Young WF Jr, du Plessis H, Thompson GB,
Grant CS, Farley DR, Richards ML, Erickson D, Vella A, Stanson AW,
Carney JA, et al: The clinical conundrum of
corticotropin-independent autonomous cortisol secretion in patients
with bilateral adrenal masses. World J Surg. 32:856–862.
2008.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Funder JW, Carey RM, Fardella C,
Gomez-Sanchez CE, Mantero F, Stowasser M, Young WF Jr and Montori
VM: Endocrine Society. Case detection, diagnosis, and treatment of
patients with primary aldosteronism: An endocrine society clinical
practice guideline. J Clin Endocrinol Metab. 93:3266–3281.
2008.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Acharya R, Dhir M, Bandi R, Yip L and
Challinor S: Outcomes of adrenal venous sampling in patients with
bilateral adrenal masses and ACTH-independent Cushing's syndrome.
World J Surg. 43:527–533. 2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Iacobone M, Albiger N, Scaroni C, Mantero
F, Fassina A, Viel G, Frego M and Favia G: The role of unilateral
adrenalectomy in ACTH-independent macronodular adrenal hyperplasia
(AIMAH). World J Surg. 32:882–889. 2008.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Debillon E, Velayoudom-Cephise FL,
Salenave S, Caron P, Chaffanjon P, Wagner T, Massoutier M, Lambert
B, Benoit M, Young J, et al: Unilateral adrenalectomy as a
first-line treatment of Cushing's syndrome in patients with primary
bilateral macronodular adrenal hyperplasia. J Clin Endocrinol
Metab. 100:4417–4424. 2015.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Răducu L, Avino A, Purnichescu Purtan R,
Balcangiu-Stroescu AE, Bălan DG, Timofte D, Ionescu D and Jecan CR:
Quality of life in patients with surgically removed skin tumors.
Medicina (Kaunas). 56(66)2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Laslo CL, Pantea Stoian A, Socea B,
Paduraru DN, Bodean O, Socea LI, Neagu TP, Stanescu AMA, Marcu D
and Diaconu C: New oral anticoagulants and their reversal agents. J
Mind Med Sci. 5:195–201. 2018.
|
|
22
|
Gaman MA, Dobrica EC, Pascu EG, Cozma MA,
Epingeac ME, Gaman AM, Pantea Stoian AM, Bratu OG and Diaconu CC:
Cardio metabolic risk factors for atrial fibrillation in type 2
diabetes mellitus: Focus on hypertension, metabolic syndrome and
obesity. J Mind Med Sci. 6:157–161. 2019.
|
|
23
|
Li X, Xiang X, Hu J, Goswami R, Yang S,
Zhang A, Wang Y, Li Q and Bi X: Association between serum cortisol
and chronic kidney disease in patients with essential hypertension.
Kidney Blood Press Res. 41:384–391. 2016.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Mandita A, Timofte D, Balcangiu-Stroescu
AE, Balan D, Raducu L, Tanasescu MD, Diaconescu A, Dragos D,
Cosconel CI, Stoicescu SM and Ionescu D: Treatment of high blood
pressure in patients with chronic renal disease. Rev Chim Buchar.
70:993–995. 2019.
|
|
25
|
Balcangiu-Stroescu AE, Tanasescu MD,
Diaconescu A, Raducu L, Constantin AM, Balan DG, Tarmure V and
Ionescu D: Cardiovascular comorbidities, inflammation and serum
albumin levels in a group of hemodialysis patients. Rev Chim.
69:926–929. 2018.
|
|
26
|
Nishikawa T, Omura M, Satoh F, Shibata H,
Takahashi K, Tamura N and Tanabe A: Task Force Committee on Primary
Aldosteronism, The Japan Endocrine Society. Guidelines for the
diagnosis and treatment of primary aldosteronism-the Japan
endocrine society 2009. Endocr J. 58:711–721. 2011.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Oki K, Yamane K, Sakashita Y, Kamei N,
Watanabe H, Toyota N, Shigeta M, Sasano H and Kohno N: Primary
aldosteronism and hypercortisolism due to bilateral functioning
adrenocortical adenomas. Clin Exp Nephrol. 12:382–387.
2008.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Raducu L, Balcangiu-Stroescu AE, Stanescu
II, Tanasescu MD, Cozma CN, Jecan CR and Badita DG: Use of
polyhexanidine in treating chronic wounds. Rev Chim. 68:2112–2113.
2017.
|
|
29
|
Paduraru DN, Scanteie C, Bolocan A,
Andronic O, Morar A, Ghervan C, Ciunt R, Socea B, Bratu OG,
Dragomir LM, et al: Pasireotide after surgery for persistent
Cushing's disease. Mod Med. 26:227–231. 2019.
|
|
30
|
Marcu RD, Diaconu CC, Constantin T, Socea
B, Ionita-Radu F, Mischianu DLD and Bratu OG: Minimally invasive
biopsy in retroperitoneal tumors. Exp Ther Med. 18:5016–5020.
2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Marcu DR, Ionita-Radu F, Iorga LD, Manea
M, Socea B, Scarneciu I, Isvoranu G, Costache R, Diaconu CC and
Bratu OG: Vascular involvement in primary retroperitoneal tumors.
Rev Chim. 70:445–448. 2019.
|
|
32
|
Rossi GP, Barisa M, Allolio B, Auchus RJ,
Amar L, Cohen D, Degenhart C, Deinum J, Fischer E, Gordon R, et al:
The adrenal vein sampling international study (AVIS) for
identifying the major subtypes of primary aldosteronism. J Clin
Endocrinol Metab. 97:1606–1614. 2012.PubMed/NCBI View Article : Google Scholar
|