Introduction
Recurrent ovarian cancer is incurable and,
accordingly, has poor prognosis. In a study analyzing survival data
from clinical trials of ovarian cancer, the median overall survival
(OS) after the first, second, third, fourth and fifth recurrence
was 17.6, 11.3, 8.9, 6.2 and 5.0 months, respectively (1). Therefore, novel treatment options are
urgently required for such patients. Radiofrequency hyperthermia
(RFH) therapy involves heating of the body using radiofrequency
energy. While it has been applied for the treatment of different
cancer types, its efficacy remains conflicting. For instance, in a
randomized trial of 73 patients with advanced ovarian cancer, those
who received chemotherapy with RFH achieved better tumor remission
rates than those who received chemotherapy alone (2). However, in a randomized trial of
patients with cervical cancer, there was no significant difference
in survival between those who received RFH with radiotherapy and
those who received radiotherapy alone. In addition, acute toxicity
was significantly worse in the RFH plus radiotherapy arm (3).
Modulated electro-hyperthermia (mEHT) is a type of
RFH that uses impedance coupling with amplitude-modulated 13.56 MHz
carrier radiofrequency (4). Similar
to conventional RFH, mEHT is usually administered for 60 min, 1-3
times per week (3,5-7).
However, unlike conventional RFH, the energy of radiofrequency is
selectively absorbed by the tumor cells in mEHT (8). In addition, an in vitro study
reported that the cellular response to mEHT is different from that
to conventional RFH. Specifically, in contrast to conventional RFH,
mEHT activates caspase-dependent pathways and induces apoptosis
(9). Therefore, it was hypothesized
that the oncologic effect of mEHT may be different from that of
conventional RFH.
To the best of our knowledge, only 3 trials
investigating the effects of mEHT therapy on cancer have been
published to date. Although the trials were on different cancers,
the results all suggested that the addition of mEHT was beneficial
for achieving a higher response rate (5) and better local control (6) than conventional treatments and was
highly feasible (7). However,
evidence on the usefulness and safety of mEHT combined with
chemotherapy in the treatment of ovarian cancer is currently
lacking (10). Thus, the present
study aimed to evaluate the safety of mEHT therapy with weekly
paclitaxel or cisplatin administration in females with recurrent or
persistent epithelial ovarian, fallopian tube or primary peritoneal
carcinoma.
Materials and methods
Trial design and randomization
The present trial (KGOG 3030) was a phase 1 trial
with 1 dose level performed at three tertiary hospitals (Seoul
National University Bundang Hospital, Seongnam, Gyeonggi; Gangnam
Severance Hospital, Seoul; Ewha Womans University Mokdong Hospital,
Seoul) in the Republic of Korea between February 2015 and November
2017. The study was conducted according to the tenets of the
Declaration of Helsinki and its later amendments, and the protocol
was approved by the Institutional Review Board (IRB) of each
hospital (Seoul National University Bundang Hospital IRB, approval
no. E-1407/258-001, approval date 17th Sep 2014; Yonsei
University Gangnam Severance Hospital IRB, approval no.
3-2014-0272, approval date 14th January 2015; Ewha
Womans University Medical Center IRB, approval no. EUMC
2014-09-009, approval date 1st December 2014) and
registered at www.clinicaltrials.gov (on January 22, 2015;
registration no. NCT02344095). Written informed consent was
obtained from all subjects. The present study was reported in line
with the Consolidated Standards of Reporting Trials guidelines
(11).
There is already a widely used protocol for mEHT
therapy and numerous cases in which mEHT therapy was combined with
various chemotherapy modalities were encountered in our clinical
practice. Therefore, the widely used protocol for mEHT therapy (1
h; 2 sessions per week; maximum energy, 140 W) (10) was adopted. In addition, it was
decided not to test several dose levels of chemotherapy and adopt a
3+3 design with only 1 dose level (70 mg/m2 for
paclitaxel, 40 mg/m2 for cisplatin). Specifically, 3
patients were enrolled and underwent therapy with a dose level of
chemotherapy plus mEHT. If dose-limiting toxicity (DLT) was
observed in <2 of 3 patients, 3 more patients were enrolled. If
DLT occurred in <2 of 6 patients, it was concluded that the dose
was safe enough for use in a further investigation. There was no
dose escalation or de-escalation. Therefore, the anticipated number
of patients was 12 (6 in each arm).
The optimal chemotherapy drug to be combined with
mEHT therapy in recurrent ovarian cancer has remained undetermined.
In vitro studies suggested that hyperthermia potentiates the
cytotoxic effects of cisplatin (12,13).
Furthermore, weekly paclitaxel administration is an effective
regimen in recurrent ovarian cancer (14). After a thorough review of the
literature and discussion, paclitaxel and cisplatin were selected
(12-14).
To determine which drug should be selected for further
investigation at the completion of the present trial, both the
paclitaxel and cisplatin arms were launched and compared using
randomization. Patients were randomized into the paclitaxel arm or
the cisplatin arm at a 1:1 ratio using block randomization with
‘hospital’ as a stratification factor. Randomization and
notification of results were performed by the independent data
center and the randomization result was not concealed.
Eligibility and intervention
The inclusion criteria were as follows: i) Recurrent
or persistent epithelial ovarian, fallopian tube or primary
peritoneal carcinoma; ii) tumor evaluable with radiologic study or
serum carbohydrate antigen (CA)125; and iii) Eastern Cooperative
Oncology Group performance status score (15) of 0-2. The exclusion criteria were as
follows: i) Tumor located in previously irradiated area; ii) brain
metastasis; iii) residual neurotoxicity or history of severe
neurotoxicity; iv) hypersensitivity to paclitaxel or cisplatin; and
v) pacemaker or metal implants. The number of previous chemotherapy
regimens was limited to <3 at initiation. However, due to slow
accrual, the limit was changed to <4 in August 2015 and was
removed in July 2016.
Patients in the paclitaxel arm received 4 cycles of
mEHT therapy with weekly paclitaxel chemotherapy, with each cycle
lasting 4 weeks. After steroids and anti-histamines were
administered to prevent infusion reactions, 70 mg/m2 of
paclitaxel was intravenously infused for 1 h on days 1, 8 and 15
every 4 weeks. Within 3 h of completion of paclitaxel infusion,
mEHT therapy was initiated. The mEHT therapy was performed 2 times
weekly (days 1, 4, 8, 11, 15, 18, 21 and 24 per cycle) using an EHY
2000 plus device (Oncotherm GmbH) and each mEHT therapy session
lasted 60 min. During the mEHT therapy, patients were placed in a
supine position and a 30-cm diameter circular mEHT electrode was
attached to the abdominal wall over the tumor. No precise targeting
of the tumor was performed. Starting from 60 W, energy was
gradually increased to 140 W. If the patient felt hot or had any
discomfort, the energy was decreased to the previous level and then
maintained at that level throughout the duration of the session.
When tumors were present in the abdomen and chest area, mEHT
therapy was performed sequentially (starting at the abdomen and
then the chest).
Patients in the cisplatin arm received 4 cycles of
mEHT therapy plus weekly cisplatin chemotherapy, with each cycle
lasting 4 weeks; 40 mg/m2 of cisplatin was intravenously
infused for 1 h on days 1, 8 and 15 every 4 weeks. The mEHT therapy
protocol was the same as that for the paclitaxel arm.
Endpoints
The primary endpoint was the occurrence of DLT from
enrollment to fourth cycle completion in evaluable patients of each
arm. DLT was defined as the occurrence of any of the following: i)
Neutropenic fever requiring inotropics or intensive care unit
admission; ii) hematologic toxicity not recovered to grade 1 or 2
within 3 weeks (except anemia); iii) non-hematologic toxicity not
recovered to grade 1 or 2 within 3 weeks (except alopecia); and iv)
death. Evaluable patients were defined as patients who completed
the second cycle.
The secondary endpoints were safety and preliminary
efficacy. Safety was measured according to the type, grade and
incidence of treatment-emergent adverse events (TEAEs) evaluated
using the Common Terminology Criteria for Adverse Events version
4.0(16). The efficacy endpoints
were objective response rate in patients with measurable disease as
evaluated using the Response Evaluation Criteria in Solid Tumors
version 1.1(17), CA125 response
rate in patients with elevated baseline CA125, progression-free
survival (PFS) and OS. The CA125 response was defined as a decrease
of >50% from the baseline with confirming repeat test results.
During treatment, physical examination and CA125 test were
performed every cycle. After treatment was completed, patients were
followed up every 3 months until death. CA125 and imaging tests
were performed at the discretion of the physician
Statistical analysis
All statistical analyses were performed using SPSS
version 25 (IBM Corp.). Continuous variables were presented as the
median and range. Categorical variables were presented as counts
and percentages. PFS and OS were estimated using the Kaplan-Meier
method.
Results
Baseline characteristics
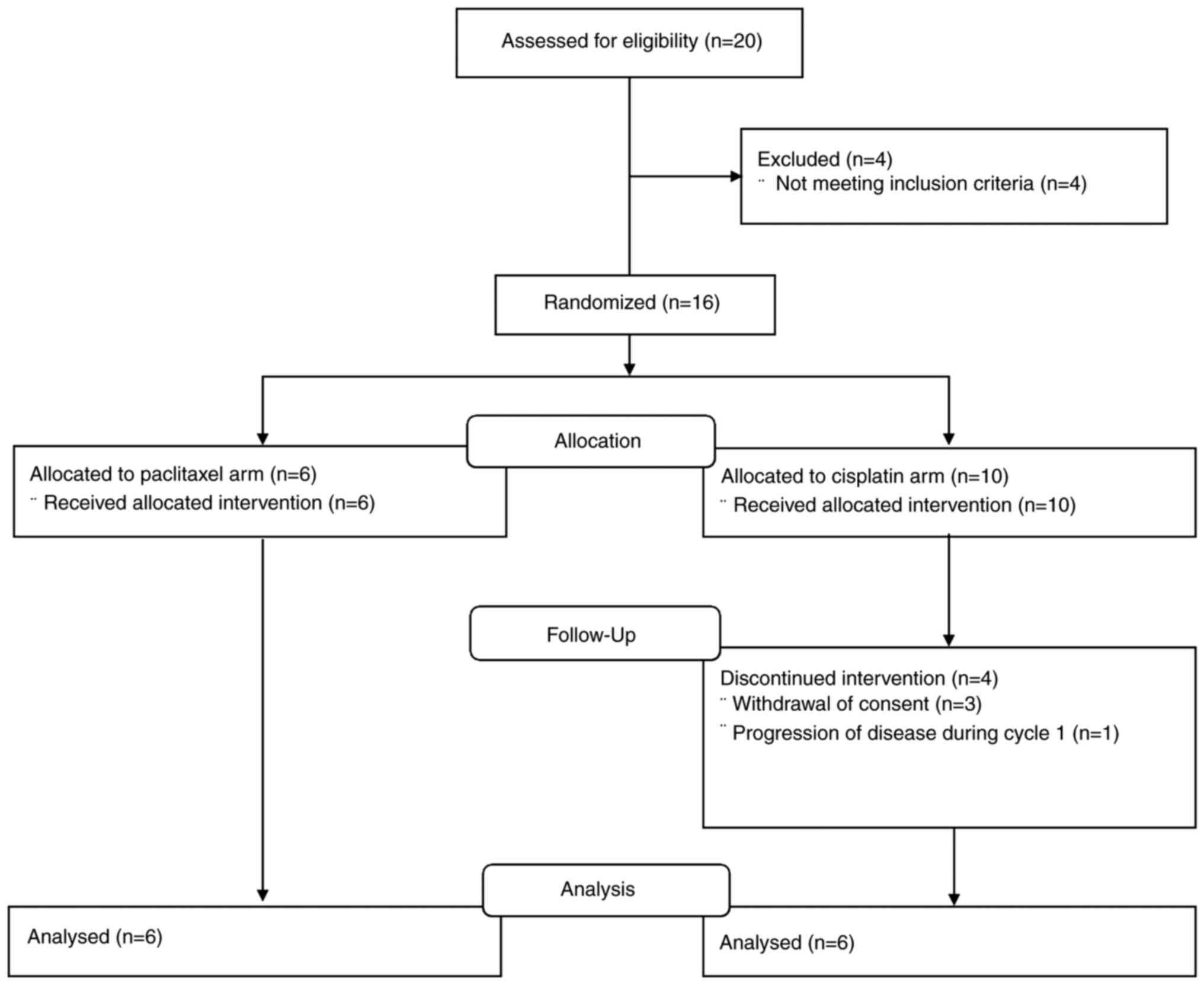
In total, 16 patients were recruited for the present
study. A flowchart depicting the movement of the patients
throughout the study is provided in Fig. 1. Of 16 patients, four patients in
the cisplatin arm did not complete the first cycle and were not
evaluable. The time-point and reasons for treatment discontinuation
of the 4 patients were as follows: Patient 1 (prior to cycle 1,
withdrawal of consent), patient 2 (cycle 1 day 1, withdrawal of
consent), patient 3 (cycle 1 day 15, clinical deterioration due to
presumed cancer progression) and patient 4 (cycle 1 day 8,
withdrawal of consent). No TEAEs of grade 3 or above were observed
in the 4 patients. The 4 patients were excluded from the efficacy
and safety analysis according to the protocol.
The baseline characteristics of the 12 evaluable
patients are summarized in Table I.
The median age was 64 years and the high-grade serous type was the
most common histological type. The number of previous chemotherapy
regimens ranged from 1 to 5 and most of patients were
platinum-resistant or refractory.
 | Table IBaseline characteristics of the
patients. |
Table I
Baseline characteristics of the
patients.
| Variable | Paclitaxel + mEHT
(n=6) | Cisplatin + mEHT
(n=6) |
|---|
| Age, years | 67 (53-71) | 61 (56-72) |
| Body height, cm | 155 (143-163) | 153 (149-156) |
| Body weight, kg | 60 (50-64) | 55 (47-86) |
| Origin of cancer | | |
|
Ovary | 5(83) | 4(67) |
|
Peritoneal | 1(17) | 2(33) |
| FIGO stage | | |
|
3 | 4(67) | 5(83) |
|
4 | 2(33) | 1(17) |
| Histologic type | | |
|
High-grade
serous | 4(67) | 5(83) |
|
Clear
cell | 1(17) | 0 (0) |
|
Low-grade
serous | 0 (0) | 1(17) |
|
Carcinosarcoma | 1(17) | 0 (0) |
| Number of previous
regimens | 2 (1-4) | 2 (1-5) |
| Treatment-free
interval from previous treatment, months | 5 (1-16) | 6 (0-27) |
| Sensitivity to
platinum | | |
|
Sensitive | 2(33) | 1(17) |
|
Resistant | 2(33) | 4(67) |
|
Refractory | 2(33) | 1(17) |
Safety
None of the 12 evaluable patients experienced DLT.
No severe TEAE occurred in the paclitaxel arm. The common TEAEs
were constipation, dyspepsia, headache and neutropenia. A total of,
four grade-3 TEAEs occurred in the cisplatin arm. These were
grade-3 anemia (n=1), nausea (n=1), neutropenia (n=1) and
thrombocytopenia (n=1). The common TEAEs were neutropenia and
nausea. TEAEs according to type and grade in the paclitaxel and
cisplatin arms are summarized in Tables II and III, respectively.
| Table IITreatment-emergent adverse events in
the paclitaxel arm. |
Table II
Treatment-emergent adverse events in
the paclitaxel arm.
| Type | Grade 1 | Grade 2 | Sum |
|---|
| Abdominal
distension | 1 | 0 | 1 |
| Abdominal pain | 0 | 1 | 1 |
| Alopecia | 1 | 0 | 1 |
| Anorexia | 0 | 1 | 1 |
| Constipation | 1 | 1 | 2 |
| Creatinine
increased | 0 | 1 | 1 |
| Dysarthria | 0 | 1 | 1 |
| Dyspepsia | 2 | 0 | 2 |
| Dyspnea | 0 | 1 | 1 |
| Fatigue | 1 | 0 | 1 |
| Flank pain | 0 | 1 | 1 |
| Headache | 2 | 1 | 3 |
| Hyperkalemia | 1 | 0 | 1 |
| Hypocalcemia | 1 | 0 | 1 |
| Neutrophil count
decreased | 0 | 2 | 2 |
| Pain | 1 | 0 | 1 |
| Peripheral sensory
neuropathy | 0 | 1 | 1 |
| Productive
cough | 1 | 0 | 1 |
| Toothache | 0 | 1 | 1 |
| Tremor | 0 | 1 | 1 |
| Wound
complication | 1 | 0 | 1 |
| Sum | 13 | 13 | 26 |
| Table IIITreatment-emergent adverse events in
the cisplatin arm. |
Table III
Treatment-emergent adverse events in
the cisplatin arm.
| Type | Grade 1 | Grade 2 | Grade 3 | Sum |
|---|
| Abdominal pain | 1 | 1 | 0 | 2 |
| Anemia | 0 | 0 | 1 | 1 |
| Anorexia | 0 | 1 | 0 | 1 |
| Back pain | 1 | 1 | 0 | 2 |
| Dizziness | 0 | 1 | 0 | 1 |
| Dry mouth | 0 | 1 | 0 | 1 |
| Dyspepsia | 1 | 0 | 0 | 1 |
| Edema face | 1 | 0 | 0 | 1 |
| Fatigue | 1 | 0 | 0 | 1 |
| Gastrointestinal
pain | 1 | 0 | 0 | 1 |
| Headache | 2 | 0 | 0 | 2 |
| Mucositis oral | 1 | 0 | 0 | 1 |
| Nausea | 2 | 1 | 1 | 4 |
| Neutrophil count
decreased | 2 | 2 | 1 | 5 |
| Periodontal
disease | 1 | 0 | 0 | 1 |
| Peripheral sensory
neuropathy | 1 | 1 | 0 | 2 |
| Platelet count
decreased | 0 | 1 | 1 | 2 |
| Productive
cough | 1 | 0 | 0 | 1 |
| Skin and
subcutaneous tissue disorders-others | 1 | 0 | 0 | 1 |
| Skin
hyperpigmentation | 0 | 1 | 0 | 1 |
| Superficial
thrombophlebitis | 0 | 1 | 0 | 1 |
| Telangiectasia | 1 | 0 | 0 | 1 |
| Vomiting | 1 | 0 | 0 | 1 |
| Sum | 19 | 12 | 4 | 35 |
Efficacy
Of the 12 patients, 9 patients (5 in the paclitaxel
arm, 4 in the cisplatin arm) had measurable disease at baseline. Of
the 9 patients, 1 confirmed partial response was observed in the
cisplatin arm (platinum-resistant, high-grade serous). The duration
of response was 4 months. Furthermore, 9 of the 12 patients (4 in
the paclitaxel arm, 5 in the cisplatin arm) had elevated baseline
CA125 levels. Among them, 2 CA125 responses (2 in the cisplatin
arm, both were platinum-resistant, high-grade serous) were
observed. The duration of response was 4 and 10 months. Progression
was observed in all patients. The median PFS in the paclitaxel and
cisplatin arms was 3.0 months (range, 1.7-4.6 months) and 6.8
months (range, 3.9-11.8 months), respectively. At the cut-off of
September 12, 2018, 5 of the 12 patients had died (4 in the
paclitaxel arm, 1 in the cisplatin arm). The median OS in the
paclitaxel and cisplatin arms was 11.5 months (range, 8.4-28.8+
months) and not reached (range, 3.9-38.5+ months), respectively
(data not shown).
Discussion
In a previous study, chemotherapy combined with
conventional RFH was reported to be more effective than
chemotherapy alone for the treatment of advanced ovarian cancer
(2). However, to the best of our
knowledge, no previous study has examined the efficacy and safety
of chemotherapy combined with mEHT for ovarian cancer. Therefore,
the present study is novel and it is the first to examine the
safety and efficacy of chemotherapy combined with mEHT for the
treatment of ovarian cancer.
The results of the present phase 1 trial indicated
that mEHT therapy combined with weekly chemotherapy is safe enough
to proceed to be investigated in further clinical trials.
Specifically, no DLT occurred in both the paclitaxel and cisplatin
arms, and only 4 grade 3 TEAEs were observed. Therefore, both
modalities appeared tolerable. The safety of RFH therapy combined
with chemotherapy has been reported in previous studies. In a trial
on RFH therapy combined with weekly docetaxel in patients with
locally advanced non-small cell lung cancer, grade 3 or 4
neutropenia occurred in only 24% of the patients (18). In a randomized trial comparing RFH
plus chemotherapy with chemotherapy alone in advanced ovarian
cancer, toxicity was similar between arms (2). Collectively, these findings and the
results of the current trial indicated that mEHT therapy may be
safely combined with chemotherapy.
To the best of our knowledge, no study has reported
superiority of RFH with chemotherapy over chemotherapy alone in the
treatment of platinum-resistant ovarian cancer. In the present
study, mEHT therapy combined with weekly chemotherapy showed
intermediate efficacy. Of the 9 patients, only 1 partial response
was confirmed (response rate, 11%). Response based on CA125 was
observed in 2 of 9 patients (22%). All responses were observed in
the cisplatin arm. Specifically, in the cisplatin arm, 1 of 4
patients with measurable disease responded (response rate, 25%),
and 2 of 5 patients with elevated baseline CA125 levels exhibited
CA125 response (40%). This suggests that when combined with mEHT,
while cisplatin appeared to be slightly more toxic, it was also
more efficacious than paclitaxel. Supporting the present results,
previous cell line studies suggested that hyperthermia enhanced the
cytotoxicity of cisplatin but inhibited that of paclitaxel
(12,13,19,20).
Thus, mEHT therapy combined with weekly cisplatin administration
should be considered a regimen for further investigation.
Of note, one radiologically confirmed partial
response and two CA125 responses were observed in the present study
in platinum-resistant patients in the cisplatin arm. A single-arm
trial testing the efficacy of oral etoposide plus weekly cisplatin
reported a 46% response rate in platinum-resistant patients and
high-dose intensity achieved by weekly dosing was suggested as a
mechanism for overcoming platinum resistance (21). Both weekly dosing and synergy
between cisplatin and mEHT may be the mechanisms accountable for
the responses observed in the present study.
The present study has certain limitations. First,
the safety of therapy was determined using data from only 6
patients per group. Therefore, the safety of therapy should be
considered preliminary and only be used to make decisions for
further investigations. As another limitation, the present trial
did not test multiple dose levels and did not investigate the
maximum tolerated dose of mEHT. This may have resulted in
undertreatment. However, a recent study indicated that the optimal
dose of mEHT in the treatment of recurrent ovarian cancer is 150 W
for 1 h (7), and that dose is
similar to the energy used in the present study (140 W).
Nevertheless, a strength of the present study was that it was a
multi-center study.
Our group is planning a subsequent phase 2 trial,
testing the efficacy and safety of weekly cisplatin plus mEHT for
recurrent ovarian cancer, and efficacy will be evaluated in
platinum-sensitive and -resistant subgroups separately.
In conclusion, mEHT therapy with weekly paclitaxel
or cisplatin appeared safe in female patients with recurrent or
persistent epithelial ovarian, fallopian tube, or primary
peritoneal carcinoma, thus warranting further investigation in
clinical trials.
Acknowledgements
The abstract of this study was previously
e-published for presentation at the 2019 Annual Meeting of the
American Society of Clinical Oncology (Chicago, USA). The authors
would like to thank Ms. EunSun Park (Clinical Research Nurse,
Gangnam Severance Hospital) and Ms. Moon Kyoung Bae (Clinical
Research Nurse, Ewha Womans University Medical Center) (both Seoul,
South Korea) for conducting this trial. Professor Soyeon Ahn
(Division of Statistics, Medical Research Collaborating Center,
Seoul National University Bundang Hospital, Seongnam, South Korea),
Professor Jae Yong Chung (Department of Clinical Pharmacology and
Therapeutics, Seoul National University College of Medicine and
Bundang Hospital, Seongnam, South Korea) and Professor Seok Ju
Seong (Department of Obstetrics and Gynecology, CHA Gangnam Medical
Center, CHA University, Seoul, South Korea) contributed to this
study as Data Safety Monitoring Board members.
Funding
Funding: This work was supported by a grant (grant no.
E-1407/258-001) from Hospicare Co. Ltd. (Seoul, Republic of Korea).
The funder was not involved in the study design, writing of the
manuscript and the decision to submit the manuscript for
publication.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
KK contributed to protocol/project development,
follow-up/examination/treatment of the patients, data collection or
management, data analysis and manuscript writing/editing. YBK and
BHN contributed to protocol/project development, data collection or
management and manuscript writing/editing. JHK, SCK, JHN, HC, WJ,
DHS and YHK contributed to follow-up/examination/treatment of the
patients, data collection or management and manuscript
writing/editing. KK and DHS checked and approved the authenticity
of the raw data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was performed according to the tenets of
the Declaration of Helsinki and its later amendments, and the
protocol was approved by the IRB of each hospital [Seoul National
University Bundang Hospital IRB (Seongnam, South Korea), approval
no. E-1407/258-001, approval date 17th Sep 2014; Yonsei
University Gangnam Severance Hospital IRB (Seoul, South Korea),
approval no. 3-2014-0272, approval date 14th January
2015; Ewha Womans University Medical Center IRB (Seoul, South
Korea), approval no. EUMC 2014-09-009, approval date 1st
December 2014]. Written informed consent was obtained from all
individual participants included in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hanker LC, Loibl S, Burchardi N, Pfisterer
J, Meier W, Pujade-Lauraine E, Ray-Coquard I, Sehouli J, Harter P
and du Bois A: AGO and GINECO study group. The impact of second to
sixth line therapy on survival of relapsed ovarian cancer after
primary taxane/platinum-based therapy. Ann Oncol. 23:2605–2612.
2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Li Z, Sun Q, Huang X, Zhang J, Hao J, Li Y
and Zhang S: The efficacy of radiofrequency hyperthermia combined
with chemotherapy in the treatment of advanced ovarian cancer. Open
Med (Wars). 13:83–89. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Vasanthan A, Mitsumori M, Park JH, Zhi-Fan
Z, Yu-Bin Z, Oliynychenko P, Tatsuzaki H, Tanaka Y and Hiraoka M:
Regional hyperthermia combined with radiotherapy for uterine
cervical cancers: A multi-institutional prospective randomized
trial of the international atomic energy agency. Int J Radiat Oncol
Biol Phys. 61:145–153. 2005.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Yang W, Han GH, Shin HY, Lee EJ, Cho H,
Chay DB and Kim JH: Combined treatment with modulated
electro-hyperthermia and an autophagy inhibitor effectively inhibit
ovarian and cervical cancer growth. Int J Hyperthermia. 36:9–20.
2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Lee SY, Lee NR, Cho DH and Kim JS:
Treatment outcome analysis of chemotherapy combined with modulated
electro-hyperthermia compared with chemotherapy alone for recurrent
cervical cancer, following irradiation. Oncol Lett. 14:73–78.
2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Minnaar CA, Kotzen JA, Ayeni OA, Naidoo T,
Tunmer M, Sharma V, Vangu MDT and Baeyens A: The effect of
modulated electro-hyperthermia on local disease control in
HIV-positive and -negative cervical cancer women in South Africa:
Early results from a phase III randomised controlled trial. PLoS
One. 14(e0217894)2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Yoo HJ, Lim MC, Seo SS, Kang S, Joo J and
Park SY: Phase I/II clinical trial of modulated
electro-hyperthermia treatment in patients with relapsed,
refractory or progressive heavily treated ovarian cancer. Jpn J
Clin Oncol. 49:832–838. 2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Hegyi G, Szigeti GP and Szász A:
Hyperthermia versus oncothermia: Cellular effects in complementary
cancer therapy. Evid Based Complement Alternat Med.
2013(672873)2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Yang KL, Huang CC, Chi MS, Chiang HC, Wang
YS, Hsia CC, Andocs G, Wang HE and Chi KH: In vitro comparison of
conventional hyperthermia and modulated electro-hyperthermia.
Oncotarget. 7:84082–84092. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Szasz AM, Minnaar CA, Szentmártoni G,
Szigeti GP and Dank M: Review of the clinical evidences of
modulated electro-hyperthermia (mEHT) method: An update for the
practicing oncologist. Front Oncol. 9(1012)2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Schulz KF, Altman DG and Moher D: CONSORT
Group. CONSORT 2010 statement: Updated guidelines for reporting
parallel group randomized trials. Ann Intern Med. 152:726–732.
2010.PubMed/NCBI View
Article : Google Scholar
|
|
12
|
Haveman J, Bergs JWJ, Franken NAP, van
Bree C and Stalpers LJA: Effect of hyperthermia on uptake and
cytotoxicity of cisplatin in cultured murine mammary carcinoma
cells. Oncol Rep. 14:561–567. 2005.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Raaphorst GP and Yang DP: The evaluation
of thermal cisplatin sensitization in normal and XP human cells
using mild hyperthermia at 40 and 41 degrees C. Anticancer Res.
25:2649–2653. 2005.PubMed/NCBI
|
|
14
|
Gynecologic Oncology Group. Markman M,
Blessing J, Rubin SC, Connor J, Hanjani P and Waggoner S: Phase II
trial of weekly paclitaxel (80 mg/m2) in platinum and
paclitaxel-resistant ovarian and primary peritoneal cancers: A
gynecologic oncology group study. Gynecol Oncol. 101:436–440.
2006.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the eastern cooperative oncology group. Am J Clin
Oncol. 5:649–655. 1982.PubMed/NCBI
|
|
16
|
U.S.Department of Health and Human
Services: Common Terminology Criteriafor Adverse Events (CTCAE).
Version 4.0. https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf.
Accessed June 14, 2010.
|
|
17
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Jiang Z, Yan W and Ming J and Y: Docetaxel
weekly regimen in conjunction with RF hyperthermia for pretreated
locally advanced non-small cell lung cancer. A preliminary study.
7(189)2007.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Leal BZ, Meltz ML, Mohan N, Kuhn J,
Prihoda TJ and Herman TS: Interaction of hyperthermia with taxol in
human MCF-7 breast adenocarcinoma cells. Int J Hyperthermia.
15:225–236. 1999.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Rietbroek RC, Katschinski DM, Reijers MH,
Robins HI, Geerdink A, Tutsch K, d'Oleire F and Haveman J: Lack of
thermal enhancement for taxanes in vitro. Int J Hyperthermia.
13:525–533. 1997.PubMed/NCBI View Article : Google Scholar
|
|
21
|
van der Burg MEL, de Wit R, Van Putten WL,
Logmans A, Kruit WH, Stoter G and Verweij J: Weekly cisplatin and
daily oral etoposide is highly effective in platinum pretreated
ovarian cancer. Br J Cancer. 86:19–25. 2002.PubMed/NCBI View Article : Google Scholar
|