Introduction
Lipoblastomas (LB) are benign tumors rising from
embryonic white fatty cells that continue to proliferate and
develop during the postnatal period (1,2). They
are diagnosed almost exclusively in pediatric population and most
of the cases are encountered in infants and children under 3 years
of age; more frequently in male patients with a male:female ratio
ranging from 1.7 to 3:1 (3,4). Most lipoblastomas are
well-encapsulated tumors and malignant degeneration changes have
not been reported to date. However, local recurrence is noted in
several reports. Lipoblastomatosis (LBS), an uncommon variant in LB
presentation, is defined as a multicentric, infiltrative form of
presentation of the tumor, where the tumor has a diffuse, unclear
distinction from the nearby tissues (1-5).
LB vary widely in anatomical location. The most affected regions
reported are the subcutaneous tissue of the trunk and limbs
(3), but intrathoracic,
intraabdominal, head, neck, axillary, inguinal or genital
localizations are occasionally described in the literature
(1-11).
They usually present as a solitary soft palpable mass, usually
painless (3,5). On the other hand, radiological finding
of an unharmful well-delimited mass responsible for its enlarging
dysmorphic effect is rare, but well known (3). The size and the relatively growing
pattern of the LB guide its surgical indication. The cosmetic
aspects, the mass effect or the broad spectrum of the localization
of the LB (some of them requiring a cautious attitude) can
influence the surgeon's decision. Histopathologic examination along
with immunohistochemistry is the standard of definitive diagnosis,
while complete surgical excision is the current mainstay treatment
(2,9,11,12).
Patients and methods
We reviewed 8 LB cases, managed by a single team
from Emergency Clinical Hospital for Children ‘Marie S. Curie’,
Bucharest, between 2016 and 2019. Informed consent was obtained
from the patient's parents. All of the cases were diagnosed by
immunohistochemistry. We reviewed the patient age at surgery, the
site of the tumor, follow-up time and recurrence. However, our main
aim was to emphasize our results and the perioperative clinical
observations in the management of these rare tumors; diagnostic
pitfalls, considerations or surgical challenges that we met are
reviewed here.
Results
The age at surgery of the patients ranged from 7 to
36 months (mean age, 8 months; median age, 22 months). The
male/female ratio was 1.6 (5:3). The mean period of follow-up was
32 months (median, 29 months); the most recent patient being
operated 6 months prior to the study. We considered three cases
having the traits of LBS. No recurrence was noted to date. None of
the patients were referred for pain.
All the LB originating in the subcutaneous fat layer
(cases no. 1-4) were noted by parents 2 months to 2 years prior to
surgery (mean, 7 months; median, 13 months) and, after an initial
ultrasound evaluation, indication for surgery was realized by the
growing pattern of the tumor to subsequent clinical and
ultrasonographic evaluations. In all cases of this subgroup, except
for case no. 3, computed tomography (CT) or magnetic resonance
imaging (MRI) scanning was indicated for a more detailed
preoperative planning for vessel and nerve dissection and none
considered LB as a preoperative diagnosis. Langer's line incisions
in all case were conducted for cosmetic reasons. In all cases,
follow-up was conducted by clinical examination and ultrasound.
Further on, perioperative observations are emphasized.
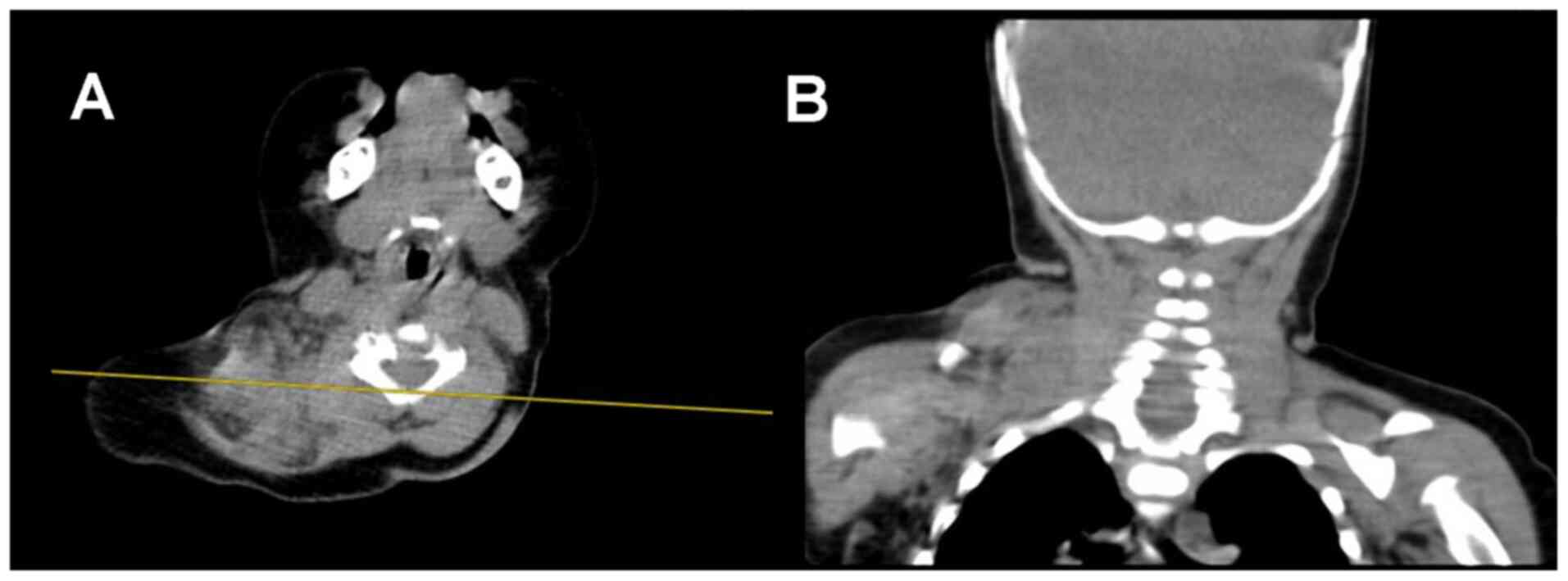
A subcutaneous palpable mass in the right axillary
region was diagnosed at 19 months of age in a female patient (case
no. 1). Surgery was performed shortly after the identified
extension of the tumor to the ipsilateral pectoral area and
supraclavicular fossa. CT scan prior to surgery was suggested for
the localization of the mass (Fig.
1). Intraoperative examinations revealed a soft mass, organized
in islands of adipose-like tissue, having a poor delineation by a
very thin connective tissue membrane from the adjacent structures.
No difficulties in the dissection were noted, except for the close
well-delimited contact to the axillary vein. Due to its
unsystematic growth, spread and poor delineation it was labeled as
LBS. No recurrence was noted after 22 months of follow-up.
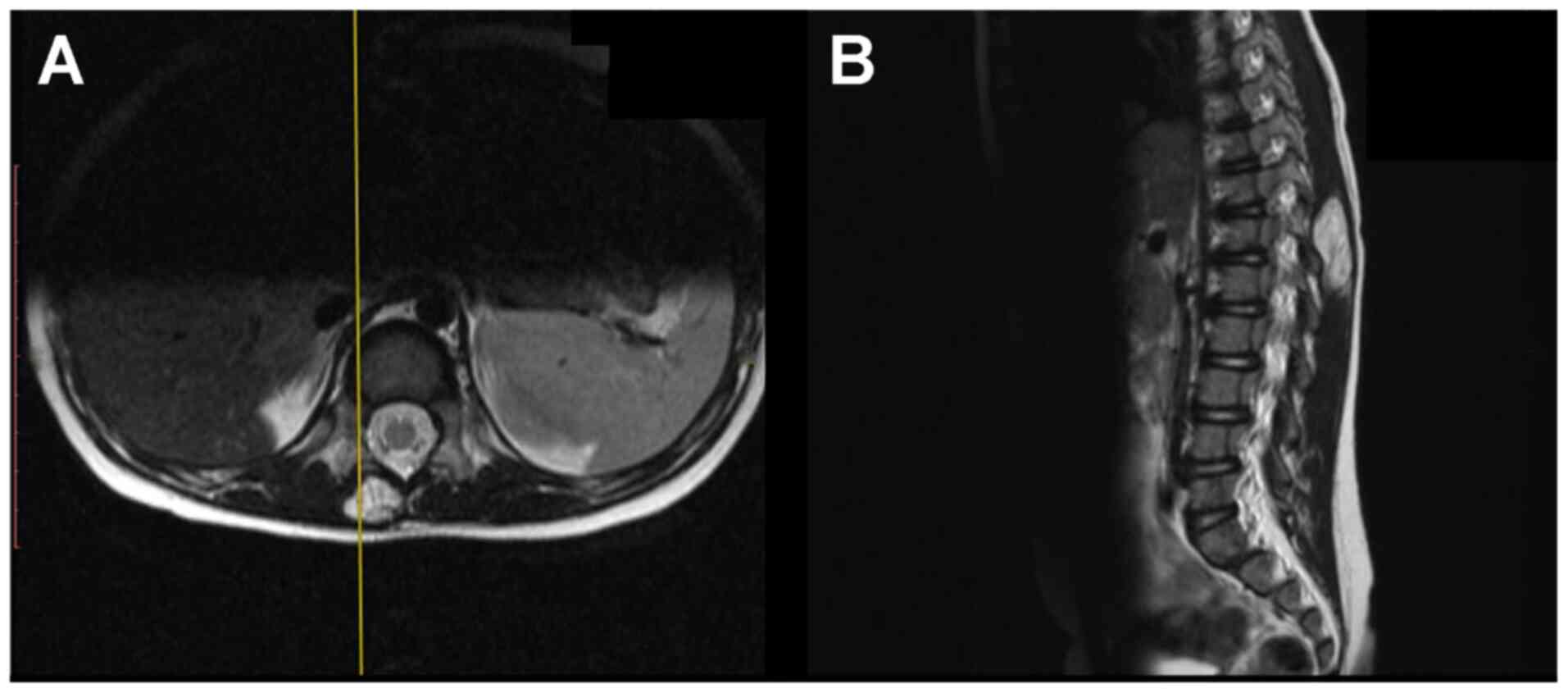
In case no. 2, a 36-month-old male underwent surgery
for a very well-delimited LB developed in the subcutaneous fatty
tissue adjacent to the lumbar spine. The CT scan showed that the
tumor was not infiltrating the posterior thoraco-lumbar fascia
(Fig. 2). Complete excision was
performed, and no recurrence was noted 2 years after surgery.
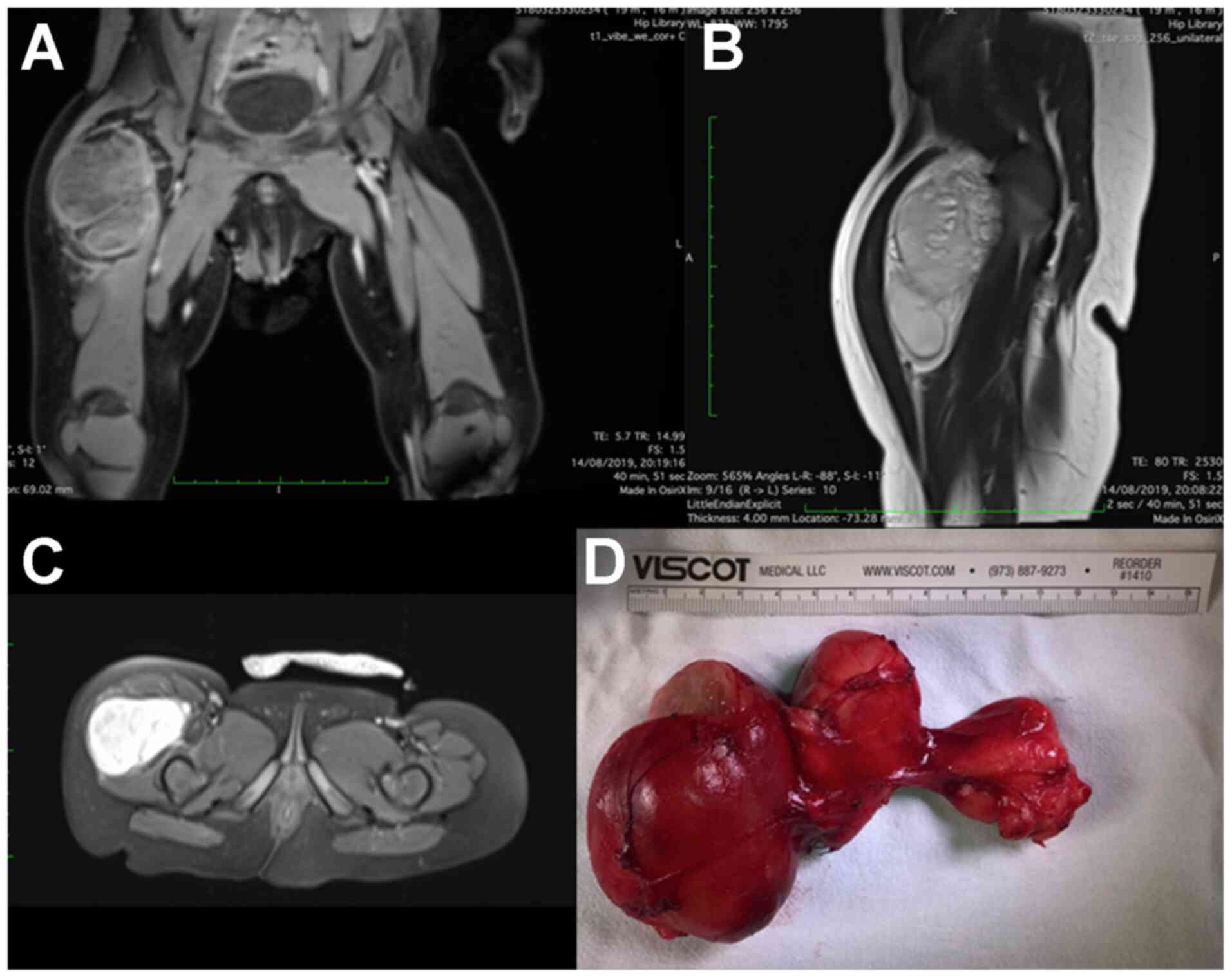
Case no. 3 was a 17-month old male, admitted for a
growing difference between the circumferences of the thighs, in
which the CT scan revealed a mass located in the anterolateral
aspect of the right thigh (Fig.
3A-C). Intraoperative exploration showed a solitary round mass,
that had developed between the muscles of the anterior compartment
(Fig. 3D). Complete excision was
performed and no recurrence was noted at the 8-month follow-up.
In regards to preoperative misleading diagnosis, we
identified three situations (cases no. 4-6) in which LB was
initially considered as lymphatic malformation, spermatic cord
cyst, and sacrococcygeal teratoma, respectively.
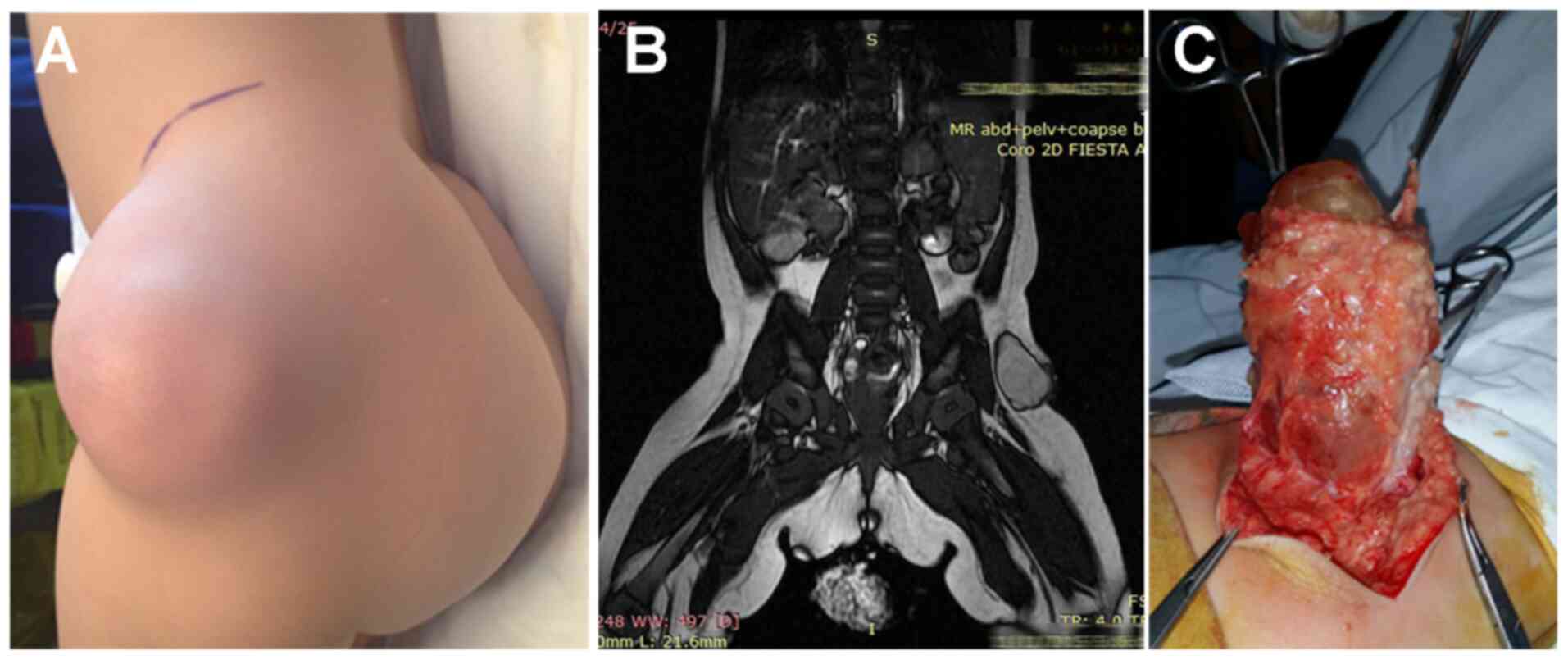
In case no. 4 (a 9-month-old patient), the
presumption of lymphatic malformation was made due to its similar
imagistic and clinical characteristics. The subcutaneous palpable
mass had developed in the left paragluteal region (Fig. 4A). An MRI was done demonstrating the
tumoral extension only in the subcutaneous tissue (Fig. 4B). The tumor was composed of locally
disseminated, relatively well-delimited cluster-like tumors,
alternating with clear fluid small cysts having a poor blood supply
(Fig. 4C). No recurrence was noted
at the 50-month follow-up after excision.
Case no. 5 was a 27-month-old male patient,
initially diagnosed as having a spermatic cord cyst. He was
surgically operated on via a lower inguinal crease incision
revealing a well-encapsulated lipomatous tumor adjacent to the
spermatic cord, protruding through the superficial inguinal ring
and bordering the epididymis. No recurrence was noted at the
43-month follow-up.
Parents of a 7-month-old female toddler noted a
gluteal lump 1 month prior to surgery. The patient also had
associated Dravet's syndrome (case no. 6). On digital rectal
examination, we did not note any changes in tissue consistency in
the presacral region. Following an MRI examination (Fig. 5) (presacral component identified) a
diagnosis of type 2 sacrococcygeal teratoma was made (serum β-human
chorionic gonadotropin and α-fetoprotein levels were within normal
values). The tumor was poorly delineated, infiltrating the gluteal
muscles and extending cranially in the presacral space. It was
resected together with the coccyx, through a Chevron incision. The
diagnosis of LBS was made considering its macroscopic traits, low
delineation and infiltrative behavior and the pathological aspect.
No local recurrence, fecal incontinence or soiling were noted at 51
months of follow-up.
In the following two cases (cases no. 7 and 8), the
diagnosis was delayed considering the low sensitivity of the
ultrasonography. Abdominal distension was the only clinical sign
noted in both cases and repeated ultrasonographic evaluation
performed prior to presentation in our clinic revealed only bowel
distension by gas or fluid; both children being under differential
diagnostic work-up for functional disorders.
A 19-month-old male patient (case no. 7) with
symptoms of progressive abdominal distension was evaluated with CT
scan in our clinic, after repeated false-negative ultrasonographic
examinations in the prior months. A lipomatous, homogenous tumor
was revealed in the retroperitoneal space in the left flank
(Fig. 6A and B). Open approach via a midline incision
was performed. The tumor was well-encapsulated and delineated in
the left retroperitoneal fat adjacent to the kidney, sigmoid and
transverse colon. Complete excision was able to be performed
(Fig. 6C), and no recurrence was
noted at 53 months of follow-up.
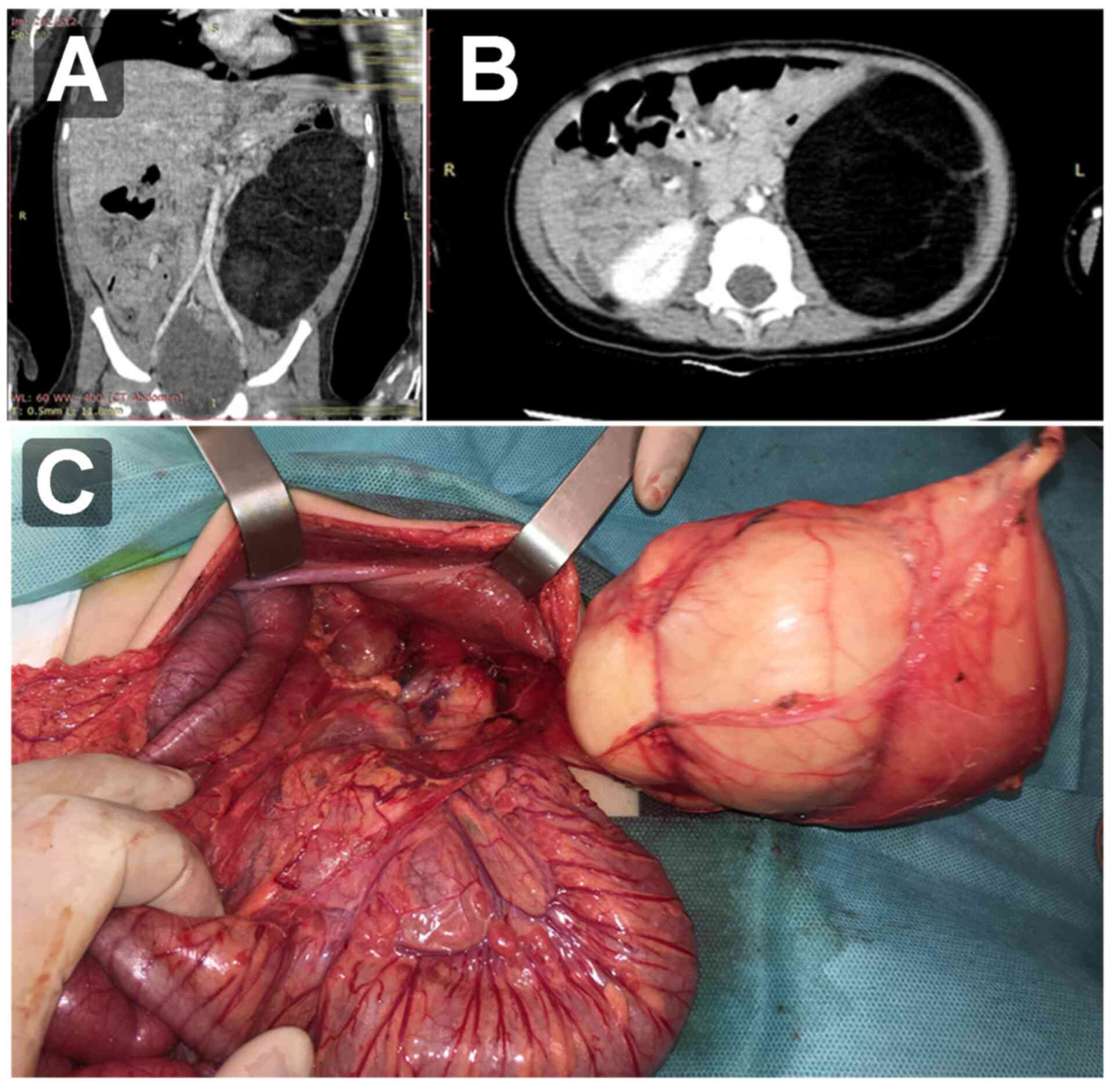
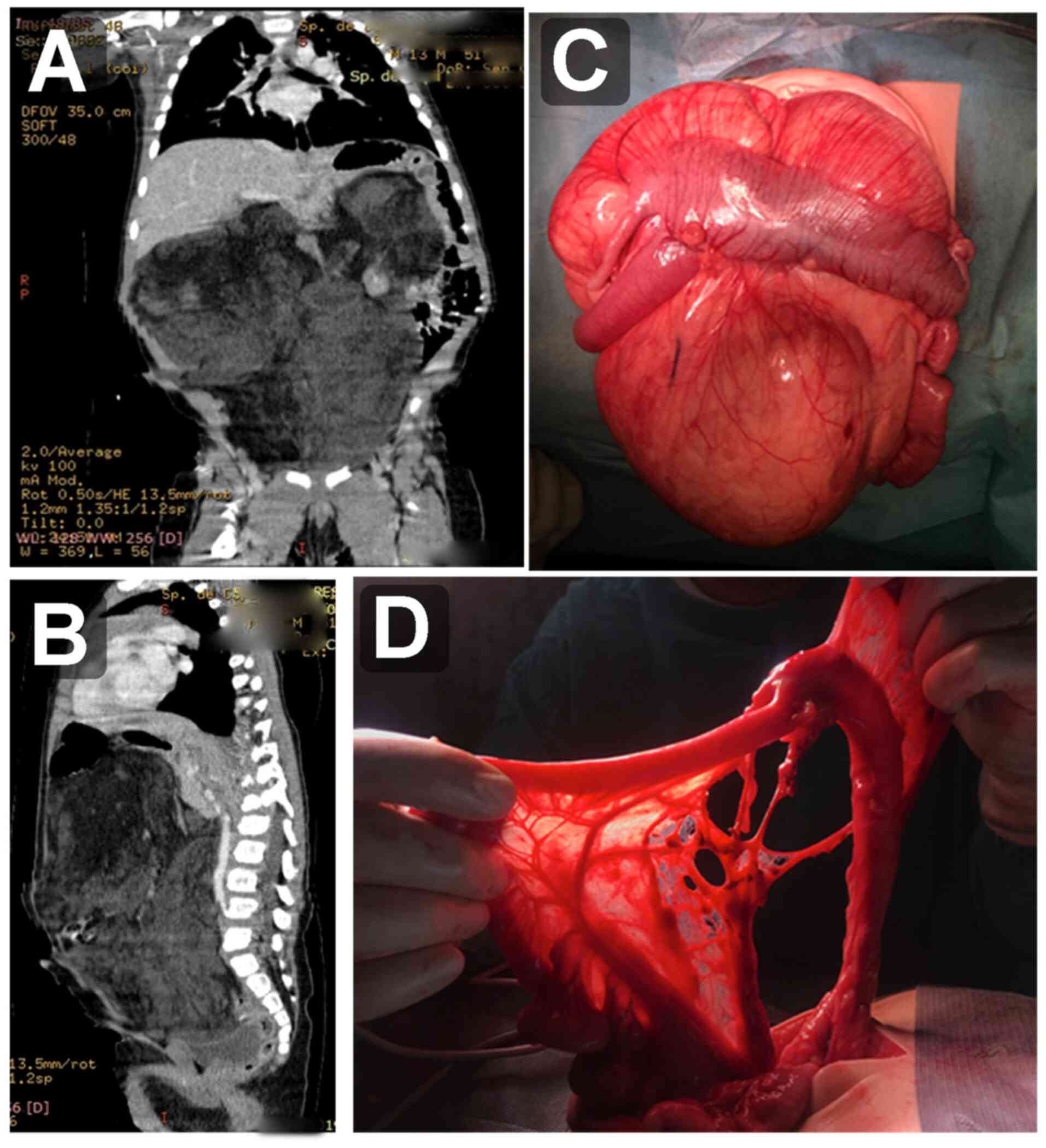
Moreover, in case no. 8 (a 14-month-old male
patient), a CT scan of the abdomen was performed after six months
of progressive abdominal distension in contrast with repeated
false-negative ultrasound exams. The work-up was delayed because of
poor family compliance. The CT scan revealed a poor delineated
impressive abdominal mass (Fig. 7A
and B). Excision via midline
incision was performed. Dissection was challenging as the
infiltrative, poor-delimitated, cluster-like tumors were spread
between the superior mesenteric vessels from the mesentery root to
marginal branches adjacent to the terminal ileum, cecum and
ascending colon (Fig. 7C and
D). No bowel ischemic complications
or prolonged ileus were noted postoperatively. No recurrence was
noted at 6-months of follow-up in this case of LBS.
Discussion
In our series there was a 5:3 (1.6) male:female
ratio and a median age at surgery of 22 months, comparable to a
large review of the literature of more than 263 case observations
by Shen et al (3). Ninety
percent of the lipoblastomas (LB) were identified in the first 3
years of life, while 10% were diagnosed in the first 12 months,
similar to the present study in which all cases were diagnosed at
an age younger than 36 months (13).
LB and LBS, along with angiolipoma, myolipoma,
lipomatosis or hibernoma are benign fat tissue tumors, while
liposarcomas are malignant, but exceptionally rare in children
(3,14). Other soft tissue tumors which may be
included in the differential diagnosis of LBs are embryonal
rhabdomyosarcoma or myxoid malignant fibrous histiocytoma, or other
rare tumors encountered in children (15,16).
Although adipose tumors of childhood are only 6% soft tissue
tumors, of which 95% are benign (17), other fat forming tumors such as
solitary fibrous tumors have been reported in the literature
(18). These predominantly develop
in the deep soft tissues of the retroperitoneum and thigh, but also
at the pleural level (19). LB is
focal, well-circumscribed, has a more superficial presentation and
a tendency to mimic lipoma, while LBS is diffuse, infiltrative of
deeper tissue layers, with a higher recurrence rate (2), similar to 3 of our reviewed cases. In
our series, two situations of preoperative misleading imaging and
clinical characteristic of the tumor were noted. In case no. 4,
multiple fluid cysts suggested a diagnosis of lymphangioma, while
in case no. 6 the clinical aspects of the tumor misled to a
postoperative presumption of sacrococcygeal teratoma.
Regarding the surgical decision, the well-documented
benign characteristics gives LB the advantage that radical surgery
may not be mandatory, considering its mutilating perspectives
depending on its localization and the predominant children
population in which the tumor is identified. Still, a recurrence
rate between 14 and 25% is reported, highly influenced by the LBS
subgroup. Moreover, a nonoperative attitude was proposed by Mognato
et al in a report mentioning a newborn with spontaneous
involution of the tumor within 8 months (13). Initially close dynamic observation
of the tumor's expansion through proper imaging tools and,
eventually, biological markers are mandatory. Subsequently,
according to its rapid growth attribute (20), we believe surgical excision should
be maintained as the standard treatment in order to relieve its
symptoms, to avoid developmental issues or for cosmetic reasons in
this order and keeping in mind that a disfiguring procedure should
be avoided in presumed LB, until histopathological examination may
backtrack this consideration. McVay et al suggest that
special attention be given regarding the invasion of deeper
structures of the neck, paraspinous region or abdomen by LB,
recommending MRI evaluation of any possible central nervous system
invasion (2). Neck LB were reviewed
by Pham et al in a series of 48 cases, considering this
localization as a clinical challenge as these tumors are often
invasive and extend through critical structures in a
‘tentacle-like’ manner, making them prone to high morbidity;
therefore, a careful follow-up is recommended in these cases
(21). However, age is essential to
differentiate LB from myxoid liposarcoma, the second one being
found in older age patients, after 15 years of life (13).
Even if most of the cases in the literature report
insidious mild symptoms, a relative mass effect or an aesthetic
effect, mediastinal localization may be life-threatening,
displaying acute respiratory distress, poor feeding or tachycardia,
requiring urgent challenging surgery and anesthesia due to
displacement of the trachea, heart, bronchi or close contact to the
pericardium (22,23).
LB is scarcely reported with associated conditions
in the current literature and these should not be ignored since, in
recent years, several studies have detailed the oncogenic
consequences of pleomorphic adenoma gene 1 (PLAG1)
alterations. Malformations such as cleft lip, cleft palate,
cephalic malformations and neurologic disorders have been reported
together with LB cases (24-26).
Therefore, a closer look at chromosome 8 (the PLAG1
location) is justified. In the presented case series, we
encountered one case of LBS associated with Dravet's syndrome. This
case strengthens Coffin et al observations of coexisting
neurological disorders, including seizures (24). Regarding the surgical aspects in the
case of presacral LB, some authors report sacral spinal canal
invasion (2,27). There is a reported coexistence
between lipoma and other tumors such as meningioma and also brain
tumors with lipomatous features such as meningioma or cystic
meningioma (28,29). Ahn et al mentioned coexisting
anorectal malformation (perineal groove type) with perineal LB, but
these were entirely intrapelvic tumors, either perineal
presentations (30). In our
situation, the aspect of the tumor was similar to an Altman II type
sacrococcygeal teratoma.
Preoperative diagnosis is not accurate in the case
of LB. Radiological diagnosis seems to be limited in LB, and CT and
MRI can underestimate the size of the lesion (2). Ultrasound may show a homogenous
hyperechoic mass or mixed echogenicity and fluid-filled spaces,
this aspect being very delicate when the radiologist examines the
abdomen whereas the tumor develops between the bowels. CT scan is
highly suggestive for identification of the fatty component where
small areas of contrast enhancement may be seen (8). In addition to the tumor extension, the
goal of radiological evaluation is to evaluate the fat relative
proportion to the associated myxoid tissue; these aspects being
confirmed afterward in the pathological examination. Fat
suppression technique in MRI helps confirm the fatty tissue
component. In older children, fat tissue seem to be a dominant
constituent, while in infants myxoid tissue with scarce adipose
elements seem to be characteristic (21). All of this confusing preoperative
imaging aspects should guide the surgeon to a deeper clinical
analysis and should favor the operative approach in younger ages,
contrary to the belief of a ‘wait and see’ attitude to avoid
disfiguring procedures (2).
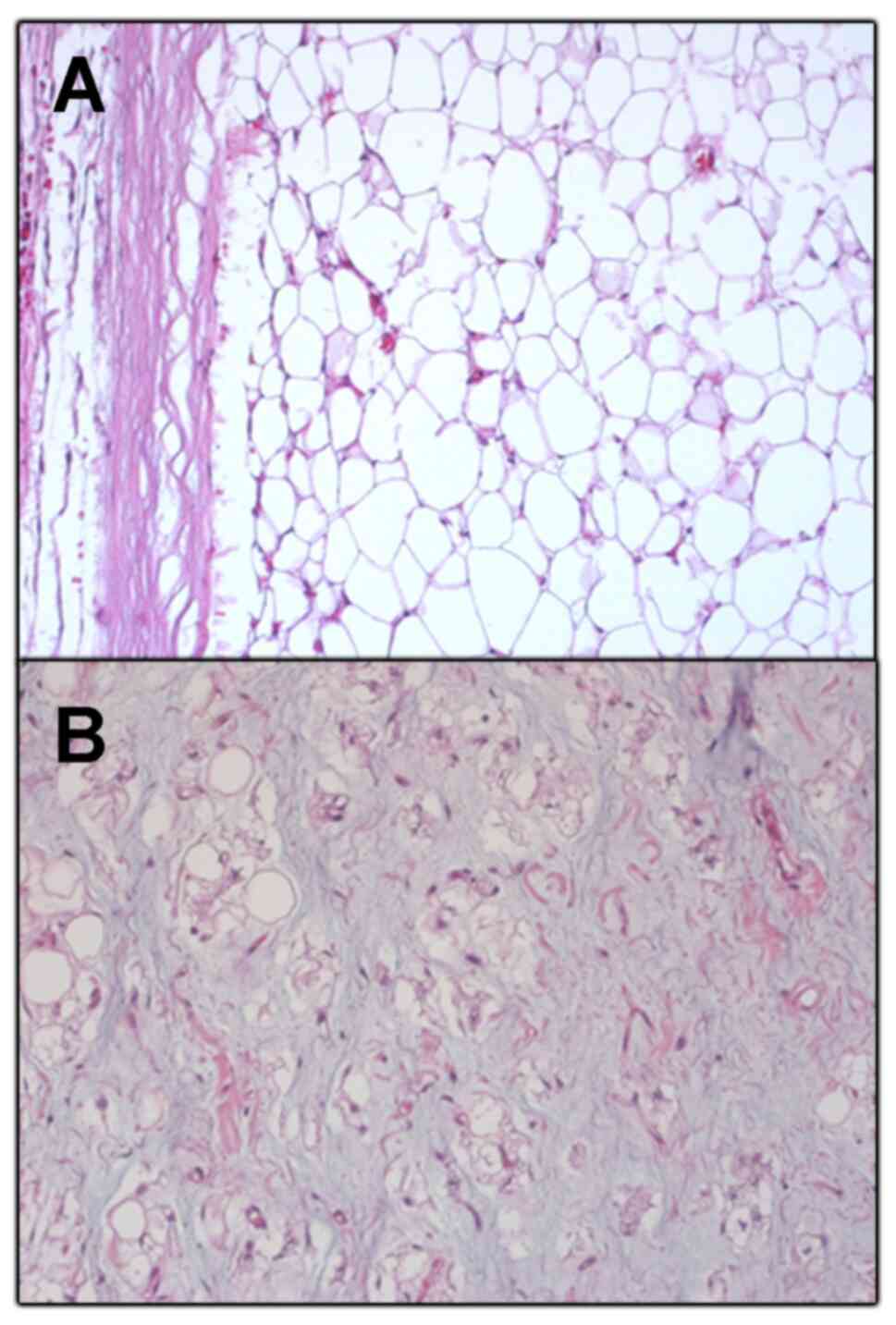
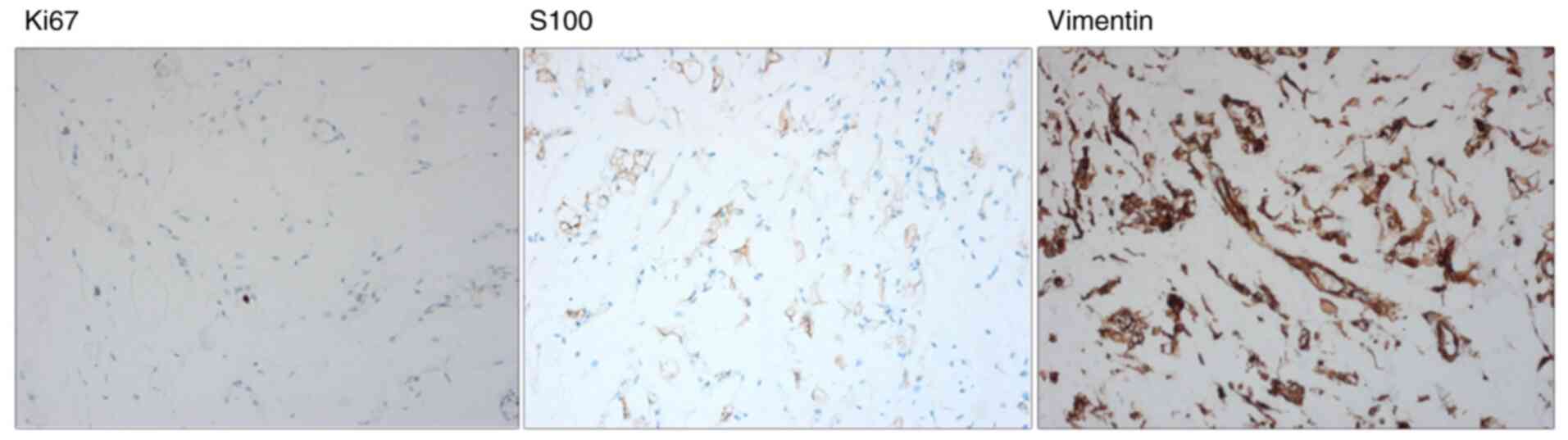
Pathologically (Figs.
8 and 9), LB is a benign tumor
covering the whole spectrum of adipose tissue differentiation
stages: From spindled and stellate cells in a myxoid background
having a plexiform vascular pattern to multivacuolated cells with a
central indented nucleus and monovacuolated cells with a marginal
flattened nucleus (mature adipocytes) (31). Immunohistochemistry staining is
recommended in all lipomatous tumors of children with ambiguous
morphology (1).
In conclusion, LB are uncommon tumors encountered in
childhood. They are benign, quick growing tumors which can have an
insidious presentation when they develop in internal, less visible
anatomical spaces. Radiological evaluation may be confusing,
missing the diagnosis or misleading to more common similar
imagistic aspects such as vascular tumors or lymphatic
malformations. However, despite its rarity, we should keep in mind
a diagnosis of LB in ambiguous imagistic cases and to point out
possible pitfalls between fluid, gas or fat tissue description.
Regarding the surgical aspects, LB is challenging based on two
aspects. The tumor boundaries of LBS are not so well defined and
the recurrence risk is high. Due to its ubiquity, originating from
embryonal fat tissue, with a local invasive growing pattern, LBS
can develop and be closely situated to essential anatomical
structures and this can turn a non-cancerous tumor excision into an
operative pitfall with potential unexpected unfavorable outcomes.
Surgery should be the mainstay of treatment. LB is a fast-growing
tumor with possible mass effect and its subsequent symptomatology,
developmental problems or cosmetic effects. Yet, the moment of
operation and its extent should be carefully evaluated according to
patient age, localization and dimensions of the tumor.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
available in this published article.
Authors' contributions
RIS and DAI contributed directly to the patient
diagnoses and surgical management. RIS, DAI and CC designed,
conceived and wrote the manuscript. DS, AE and LFT reviewed the
information and edited the article. All authors approved the final
manuscript for publication.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of ‘Maria S. Curie’ Emergency Clinic Hospital for
Children. Informed consent was obtained from all of the parents of
the patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Abdul-Ghafar J, Ahmad Z, Tariq MU, Kayani
N and Uddin N: Lipoblastoma: A clinicopathologic review of 23 cases
from a major tertiary care center plus detailed review of
literature. BMC Res Notes. 11(42)2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
McVay MR, Keller JE, Wagner CW, Jackson RJ
and Smith SD: Surgical management of lipoblastoma. J Pediatr Surg.
41:1067–1071. 2006.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Shen LY, Amin SM, Chamlin SL and Mancini
AJ: Varied presentations of pediatric lipoblastoma: Case series and
review of the literature. Pediatr Dermatol. 34:180–186.
2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Armenise T, Gentile O, Orofino A, Leggio
S, Lanzillotto MP, Zullino F and Paradies G: Lipoblastoma in
infant: Our experience. J Pediatr Surg Case Rep. 3:63–64. 2015.
|
|
5
|
Chun YS, Kim WK, Park KW, Lee SC and Jung
SE: Lipoblastoma. J Pediatr Surg. 36:905–907. 2001.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Abel RM, Bryan RT, Rafaat F, Haigh F,
Sethia B and Parikh D: Axillary lipoblastoma-tumor recurrence in
the right atrium. J Pediatr Surg. 38:1246–1247. 2003.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Eyssartier E, Villemagne T, Maurin L,
Machet MC and Lardy H: Intrascrotal lipoblastoma: A report of two
cases and a review of the literature. J Pediatr Urol. 9:E151–E154.
2013.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Moholkar S, Sebire NJ and Roebuck DJ:
Radiological-pathological correlation in lipoblastoma and
lipoblastomatosis. Pediatr Radiol. 36:851–856. 2006.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Mollaian M, Shahgholi E, Ghodsi M and
Oskuoei AK: Intrathoracic lipoblastoma in a 8 month old infant. J
Pediatr Surg Case Rep. 56(101429)2020.
|
|
10
|
Nagano Y, Uchida K, Inoue M, Ide S,
Shimura T, Hashimoto K, Koike Y and Kusunoki M: Mesenteric
lipoblastoma presenting as a small intestinal volvulus in an
infant: A case report and literature review. Asian J Surg.
40:70–73. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Mahmoud ME, Al-Onazi M, Al-Otaibi A and
Asiri S: Huge retro-peritoneal lipoblastoma in 3 year old child. J
Pediatr Surg Case Rep. 40:50–52. 2019.
|
|
12
|
Dilley AV, Patel DL, Hicks MJ and Brandt
ML: Lipoblastoma: Pathophysiology and surgical management. J
Pediatr Surg. 36:229–231. 2001.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Mognato G, Cecchetto G, Carli M, Talenti
E, d'Amore ES, Pederzini F and Guglielmi M: Is surgical treatment
of lipoblastoma always necessary? J Pediatr Surg. 35:1511–1513.
2000.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Susam-Sen H, Yalcin B, Kutluk T, Tanyel
FC, Haliloglu M, Orhan D, Aydin B, Kurucu N, Varan A and Akyuz C:
Lipoblastoma in children: Review of 12 cases. Pediatr Int.
59:545–550. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Spătaru RI, Enculescu A and Popoiu MC:
Gruber-Frantz tumor: A very rare pathological condition in
children. Rom J Morphol Embryo. l55:1497–1501. 2014.PubMed/NCBI
|
|
16
|
Suciu N, Serban A, Toader O, Oprescu D and
Spataru RI: Case report of fetal lingual tumor - perinatal care and
neonatal surgical intervention. J Matern Fetal Neonatal Med.
27:314–319. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kassem R, Faiz A, Kumar SY, John SA, Khan
YA and Khan AS: Lipoblastoma and lipomatosis in children - case
report. J Pediatr Surg Case Rep. 19:4–5. 2017.
|
|
18
|
Park CY, Rho JY, Yoo SM and Jung HK:
Fat-forming variant of solitary fibrous tumour of the pleura: CT
findings. Br J Radiol. 84:e203–e205. 2011.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Savu C, Melintea A, Posea R, Galie N,
Balescu I, Diaconu C, Cretoiu D, Dima S, Filipescu A, Balalau C and
Bacalbas N: Pleural solitary fibrous tumors - a retrospective study
of 45 patients. Medicina (Kaunas). 56(185)2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kerkeni Y, Sahnoun L, Ksia A, Hidouri S,
Chahed J, Krichen I, Mekki M, Belghith M and Nouri A: Lipoblastoma
in childhood: About 10 cases. Afr J Paediatr Surg. 11:32–34.
2014.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Pham NS, Poirier B, Fuller SC, Dublin AB
and Tollefson T: Pediatric lipoblastoma in the head and neck: A
systematic review of 48 reported cases. Int J Pediatr
Otorhinolaryngol. 74:723–728. 2010.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Geramizadeh B, Javadi F and Foroutan HR:
Intrathoracic lipoblastoma in a 15 month old infant. Rare Tumors.
3(e51)2011.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Benato C, Falezza G, Lonardoni A,
Magnanelli A, Ricci M, Gilioli E and Calabrò F: Acute respiratory
distress caused by a giant mediastinal lipoblastoma in a
16-month-old boy. Ann Thorac Surg. 92:e119–e120. 2011.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Coffin CM, Lowichik A and Putnam A:
Lipoblastoma (LPB): A clinicopathologic and immunohistochemical
analysis of 59 cases. Am J Surg Pathol. 33:1705–1712.
2009.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Gisselsson D, Hibard MK, Dal Cin P, Sciot
R, Hsi BL, Kozakewich HP and Fletcher JA: PLAG1 alterations in
lipoblastoma: Involvement in varied mesenchymal cell types and
evidence for alternative oncogenic mechanisms. Am J Pathol.
159:955–962. 2001.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Alperovich M, Diego A, Staffenberg DA and
Sharma S: Lipoblastoma of the hand and cleft palate: Is there a
genetic association? J Craniofac Surg. 25:e189–e191.
2014.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Choi SW and Song SH: Intrapelvic
lipoblastoma with massive spinal canal invasion. Childs Nerv Syst.
23:581–585. 2007.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Hayashi Y, Kimura M, Kinoshita A, Hasegawa
M and Yamashita J: Meningioma associated with intraosseous lipoma.
Clin neurol neurosurg. 105:221–224. 2003.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Yüksel MO, Gürbüz MS, Tanrıverdi O and
Özmen SA: Lipomatous meningioma: A rare subtype of benign
metaplastic meningiomas. J Neurosci Rural Pract. 8:140–142.
2017.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Ahn KH, Boo YJ, Seol HJ, Park HT, Hong SC,
Oh MJ, Kim T, Kim HJ, Kim YT, Kim SH and Lee KW: Prenatally
detected congenital perineal mass using 3D ultrasound which was
diagnosed as lipoblastoma combined with anorectal malformation:
Case report. J Korean Med Sci. 25:1093–1096. 2010.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Cappellesso R, D'Amore ESG, Dall'Igna P,
Guzzardo V, Vassarotto E, Rugge M and Alaggio R:
Immunohistochemical expression of p16 in lipoblastomas. Hum Pathol.
47:64–69. 2016.PubMed/NCBI View Article : Google Scholar
|