Introduction
Liver cancer is one of the most common malignant
tumor types in the world. Its incidence is high in developing
countries. The associated mortality rate is second only to gastric
cancer and esophageal cancer (1).
The disease may occur in individuals of all ages but it most
commonly occurs at an age of onset of 40-49 years (2). The cancer is more common in male than
in female patients, with men accounting for approximately 6 out of
7 cases. China has a high incidence of liver cancer, with cases
accounting for 42% of liver cancer cases worldwide, and its
incidence exhibits annual increases. The number of newly diagnosed
patients in China is ~600,000 per year with an estimated 200,000
individuals succumb to liver cancer each year (3,4).
Surgical treatment has always been the major
treatment method for liver cancer, but the residual liver volume
after hepatectomy is insufficient to maintain normal liver function
due to the late detection of liver cancer in certain patients or
due to the presence of a large liver tumor. However, surgery is
likely to increase complications or risk of mortality, which limits
the use of hepatectomy (5,6). It is generally thought that if the
volume of the liver removed does not exceed 80% of the original
volume, it does not affect liver regeneration, thus preventing
liver failure (7). Associating
liver partition and portal vein ligation for staged hepatectomy
(ALPPS) is an effective method for the treatment of patients with
liver cancer who cannot undergo hepatectomy and may promote
short-term rapid proliferation of residual liver cells after
surgery (8,9). However, as ALPPS is complex and the
operation time is longer than that of common hepatectomy, the
anesthesia requirements for ALPPS are high, which limits the use of
numerous anesthetic methods and anesthetics. For patients with
ALPPS, propofol is one of the most widely used drugs with low
toxicity, low liver metabolism and no accumulation (10,11).
Sevoflurane is a novel type of inhaled anesthetic with no upper
respiratory tract irritation and low respiratory inhibition. It has
little effect on hemodynamics, as it blocks the action of
N-methyl-D aspartate receptors. After inhalation is terminated, it
may be quickly metabolized and eliminated through the respiratory
system (12). However, to the best
of our knowledge, studies have reported on the use of sevoflurane
in ALPPS have yet to be performed.
In the present study, the medical records of
patients with liver cancer who were anesthetized with propofol or
sevoflurane in ALPPS were retrospectively analyzed and the combined
application of sevoflurane in ALPPS was evaluated.
Materials and methods
Research subjects
A retrospective analysis of 40 medical cases of
liver cancer who underwent liver detachment and portal vein
ligation was performed at the Jilin Hepatobiliary Hospital
(Changchun, China) between November 2007 and December 2017. The
mean age of the patients was 45.62±5.36 years and the study
included 21 (control group) and 19 (observation group) patients who
were administered propofol anesthesia and who received propofol in
compliance with sevoflurane anesthesia, respectively. On the basis
of pathology, all patients were diagnosed with liver cancer, ASA
grade II/III, normal white blood cell (WBC) and no distant
metastasis based on imaging diagnosis, consistent with the surgical
indication of ALPPS (13). The
patients did not receive any anti-tumor treatment pre-operatively
and there was no previous history of other tumors, no pre-operative
abnormalities in the organs, including the heart and kidney, or
abnormal bleeding or coagulation abnormality at the pre-operative
stage. None of the patients had any allergy to propofol or
sevoflurane, and there was past evidence of alcohol abuse or use of
nitroglycerin. The following patients were excluded: Those who
failed to undergo the second surgery, those with a survival period
of <3 months, those who died during the study period, those with
contraindications for anesthesia, those with a pre-operative
mini-mental state examination (MMSE) score (14) of <24, those with incomplete
patient data, those with a history of hepatitis, those with mental
or learning dysfunction, and those with a tumor of large diameter
(>15 cm). The study was approved by the hospital ethics
committee of Jilin Hepatobiliary Hospital (Jilin, China) and the
patient or a family member signed an informed consent form.
Anesthetic method
All patients underwent two surgical anesthesia
treatments. All patients fasted 8 h pre-operatively and intake of
medications was prohibited. An intravenous injection of 0.3 mg
scopolamine (Chengdu No. 1 Pharmaceutical Co., Ltd.) was
administered 30 min pre-operatively. Arterial pressure, central
venous pressure, electrocardiogram, blood pressure, heart rate,
pulse and blood oxygen saturation were recorded. Anesthesia was
induced using 0.2 mg/kg midazolam (Jiangsu Enhua Pharmaceutical
Co., Ltd.), 10 µg/kg remifentanil (Jiangsu Enhua Pharmaceutical
Co., Ltd.) and 0.2 mg/kg atracurium (Zhejiang Xianju Pharmaceutical
Co., Ltd.). After induction, endotracheal intubation was performed
and an anesthesia machine (Yi'an anesthesia machine Aeon7200,
Shanghai Hanfei Medical Device Co., Ltd.) was used for mechanical
ventilation. The tidal volume was 8-10 ml/kg and the respiratory
rate was 12-14 times/min. For anesthesia maintenance, the control
group was treated with propofol (Guangdong Jiabo Pharmaceutical
Co., Ltd.) for target-controlled infusion (plasma concentration, 3
µg/ml) and the observation group was treated with propofol and
inhaled sevoflurane (0.5 MAC; Futian Gutian Pharmaceutical Co.,
Ltd.) for target-controlled infusion. The two groups were treated
with continuous infusion of remifentanil (0.05-0.25 µg/kg/min;
Jiangsu Enhua Pharmaceutical Co., Ltd.). In the course of the
surgery, 0.1 mg/kg of benzenesulfinic acid atracurium was added to
maintain muscle relaxation based on the condition and the
bispectral index (15), which is
one of several technologies used to monitor the depth of
anesthesia, was maintained between 40 and 60%.
Observational indexes
For liver cancer surgery, portal vein embolization
or liver disconnection and portal vein ligation was defined as the
first stage, while ALPPS was the second stage. The immediate
hemodynamic changes in the two groups of patients prior to and
after the first-stage and second-stage operation were recorded.
Changes in liver function indicators, in blood routine parameters
and in blood coagulation function, as well as cognitive function
(MMSE) 3 days prior to and after the first-stage operation/3 days
prior to and after the second-stage operation/after the
second-stage operation were recorded.
Statistical analysis
SPSS 19.0 (IBM Corp.) was used for statistical
analysis. The enumeration data were expressed as n (%), and the
ratio was compared using the χ2 test. Measurement data
were expressed as the mean ± standard deviation, and an
independent-samples t-test was used for comparison of between two
groups, while ANOVA with Bonferroni's post-hoc test was performed
for multiple-group comparisons. P<0.05 was considered to
indicate statistical significance.
Results
General patient characteristics
The control group comprised 21 patients (11 male and
10 female patients), with a mean age of 44.91±5.32 years. The
observation group was composed of 19 patients, including 10 male
and 9 female patients, with a mean age of 46.33±5.64 years. No
significant difference was observed in sex and age between the two
groups (P>0.05). The number of surgical interval days, liver
volume after the first-stage operation, liver volume prior to the
second-stage operation, the liver volume growth rate, operation
time of the first- and second-stage operation, the extent of first-
and second-stage bleeding during surgery, the degree of education
and area of residence were not significantly different between the
two groups (all P>0.05; Table
I).
 | Table IGeneral information of the cohort. |
Table I
General information of the cohort.
| Item | Control group
(n=21) | Observation group
(n=19) | t-value | P-value |
|---|
| Sex | | | <0.001 | 0.987 |
|
Male | 11 (52.38) | 10 (52.63) | | |
|
Female | 10 (47.62) | 9 (47.37) | | |
| Age (years) | 44.91±5.32 | 46.33±5.64 | 0.822 | 0.417 |
| Operative interval
(days) | 20.35±2.12 | 19.64±2.06 | 1.072 | 0.291 |
| Post-operative liver
volume (l) | | | | |
|
Primary
surgery | 0.39±0.12 | 0.40±0.11 | 0.274 | 0.786 |
|
Secondary
surgery | 0.56±0.13 | 0.57±0.14 | 0.234 | 0.816 |
| Liver volume growth
rate (%) | 43.59±3.72 | 42.50±3.69 | 0.929 | 0.358 |
| Operative time
(min) | | | | |
|
Primary
surgery | 231.42±11.33 | 224.59±12.36 | 1.824 | 0.076 |
|
Secondary
surgery | 281.17±20.12 | 286.75±18.49 | 0.910 | 0.369 |
| Bleeding (ml) | | | | |
|
Primary
surgery | 200.66±12.12 | 208.15±13.33 | 1.862 | 0.070 |
|
Secondary
surgery | 2512.86±142.44 | 2583.47±152.13 | 1.516 | 0.138 |
| Degree of
education | | | 0.007 | 0.935 |
|
Junior high
school and below | 8 (38.10) | 7 (36.84) | | |
|
Junior high
school above | 13 (61.90) | 12 (63.16) | | |
| R Area of
residence | | | 0.382 | 0.536 |
|
Rural | 9 (42.86) | 10 (52.63) | | |
|
Urban | 12 (57.14) | 9 (47.37) | | |
Hemodynamic changes in the two groups
of patients
The mean arterial pressure (MAP), heart rate and
oxygen saturation were not significantly different between the two
groups prior to and after the first-stage operation, as well as
prior to and after the second-stage operation (P>0.05). In both
groups of patients, although minor oscillations could be observed
in the MAP before and after the first and second surgeries, none of
the differences in this category were found to be statistically
significant (P>0.05; Table
II).
| Table IIHemodynamic changes in the two groups
of patients. |
Table II
Hemodynamic changes in the two groups
of patients.
| Parameter | Control group
(n=21) | Observation group
(n=19) | t-value | P-value |
|---|
| MAP (mmHg) | | | | |
|
Prior to
first-stage operation | 104.38±9.64 | 102.49±9.42 | 0.626 | 0.535 |
|
Immediately
after first-stage operation | 108.94±10.13 | 107.42±10.09 | 0.475 | 0.637 |
|
Prior to
second-stage operation | 110.42±9.84 | 111.17±9.93 | 0.240 | 0.812 |
|
Immediately
after second-stage operation | 107.25±10.32 | 106.44±10.73 | 0.301 | 0.765 |
| Heart rate
(second/minute) | | | | |
|
Prior to
first-stage operation | 83.42±7.14 | 84.12±7.17 | 0.309 | 0.759 |
|
Immediately
after first-stage operation | 82.39±6.37 | 84.02±6.74 | 0.786 | 0.437 |
|
Prior to
second-stage operation | 83.65±6.96 | 82.41±6.14 | 0.595 | 0.556 |
|
Immediately
after second-stage operation | 83.47±6.48 | 83.17±6.69 | 0.144 | 0.886 |
| Blood oxygen
saturation (%) | | | | |
|
Prior to
first-stage operation | 96.34±4.33 | 96.72±4.25 | 0.215 | 0.831 |
|
Immediately
after first-stage operation | 97.58±3.26 | 98.22±3.37 | 0.610 | 0.545 |
|
Prior to
second-stage operation | 97.15±4.25 | 97.42±4.17 | 0.202 | 0.841 |
|
Immediately
after second-stage operation | 98.36±4.31 | 98.27±4.28 | 0.066 | 0.948 |
Changes in liver function indicators
in the two groups of patients
Total bilirubin (Tbil), direct bilirubin (Dbil),
alanine aminotransferase (ALT) and aspartate aminotransferase (AST)
levels were not significantly different between the two groups
prior to and after the first-stage operation, as well as prior to
and after the second-stage operation (P>0.05). The Tbil and Dbil
levels after the first- and second-stage operation were higher than
those prior to the first- and second-stage operation in each of the
two groups, respectively (P<0.05). The ALT level after the
first-stage operation in the two groups was also higher than that
prior to the first-stage operation (P<0.05), and the ALT level
after the second-stage operation in the two groups was
significantly lower than that prior to the second-stage operation
(P<0.05). The AST levels after the first- and second-stage
operation were lower than those prior to the first- and
second-stage operation, respectively (P<0.05; Table III).
| Table IIIChanges in liver function indicators
in the two groups of patients. |
Table III
Changes in liver function indicators
in the two groups of patients.
| Parameter | Control group
(n=21) | Observation group
(n=19) | F-value | P-value |
|---|
| Tbil (µmol/l) | | | | |
|
Prior to
first-stage operation | 18.21±1.12 | 18.43±1.09 | 0.766 | 0.312 |
|
After
first-stage operation |
21.25±1.22a |
21.67±1.18a | 1.953 | 0.225 |
|
Prior to
second-stage operation | 17.32±1.15 | 17.84±1.14 | 1.476 | 0.142 |
|
After
second-stage operation |
30.47±1.86a |
31.44±1.93a | 1.789 | 0.134 |
| Dbil (µmol/l) | | | | |
|
Prior to
first-stage operation | 14.74±0.75 | 14.36±0.76 | 1.625 | 0.141 |
|
After
first-stage operation |
19.58±1.21a |
19.02±1.18a | 1.512 | 0.126 |
|
Prior to
second-stage operation | 13.35±1.05 | 13.87±1.06 | 1.469 | 0.135 |
|
After
second-stage operation |
20.44±1.34a |
21.81±1.42a | 1.552 | 0.162 |
| ALT (U/l) | | | | |
|
Prior to
first-stage operation | 211.35±22.48 | 212.12±22.56 | 0.110 | 0.923 |
|
After
first-stage operation |
325.12±26.78a |
334.56±25.79a | 1.134 | 0.285 |
|
Prior to
second-stage operation | 105.42±11.25 | 109.34±11.26 | 1.108 | 0.292 |
|
After
second-stage operation |
42.73±7.31a |
46.29±6.99a | 1.523 | 0.152 |
| AST (U/l) | | | | |
|
Prior to
first-stage operation | 345.74±28.17 | 351.13±28.42 | 0.611 | 0.544 |
|
After
first-stage operation |
252.15±24.25a |
254.33±24.72a | 0.278 | 0.713 |
|
Prior to
second-stage operation | 259.87±23.14 | 262.48±23.56 | 0.360 | 0.744 |
|
After
second-stage operation |
42.58±7.59a |
44.32±8.01a | 0.802 | 0.474 |
Changes in blood routine indicators in
the two groups of patients
The neutrophil ratios, WBCs and hemoglobin (Hb)
concentrations were not significantly different between the two
groups in all four stages of operation (P>0.05). The WBC count
of the two groups was higher after the first-stage operation
compared with that prior to the first-stage operation, but the
difference was not statistically significant, which was increased
further following the second-stage operation (P>0.05); however,
the WBC and neutrophil counts were significantly lower after the
second-stage operation compared with that prior to the second-stage
operation (P<0.05; Table
IV).
| Table IVChanges in blood routine parameters
in the two groups of patients. |
Table IV
Changes in blood routine parameters
in the two groups of patients.
| Parameter | Control group
(n=21) | Observation group
(n=19) | F-value | P-value |
|---|
| Neutrophils
(%) | | | | |
|
Prior to
first-stage operation | 79.42±14.33 | 81.25±14.56 | 0.397 | 0.721 |
|
After
first-stage operation | 81.32±15.47 | 82.63±13.15 | 0.144 | 0.812 |
|
Prior to
second-stage operation | 80.48±13.24 | 80.91±12.33 | 0.111 | 0.943 |
|
After
second-stage operation |
73.45±13.46a |
74.58±12.72a | 0.236 | 0.740 |
| WBC
(x109/l) | | | | |
|
Prior to
first-stage operation | 10.12±1.45 | 10.48±1.39 | 0.901 | 0.479 |
|
After
first-stage operation | 11.27±1.62 | 11.73±1.48 | 0.924 | 0.376 |
|
Prior to
second-stage operation | 12.11±1.57 | 12.53±1.54 | 0.866 | 0.372 |
|
After
second-stage operation |
9.48±1.24a |
9.87±1.26a | 0.995 | 0.357 |
| Hb (g/l) | | | | |
|
Prior to
first-stage operation | 122.75±18.64 | 124.12±19.17 | 0.221 | 0.828 |
|
After
first-stage operation | 124.17±17.45 | 125.32±18.69 | 0.219 | 0.864 |
|
Prior to
second-stage operation | 125.58±17.68 | 123.86±18.84 | 0.307 | 0.743 |
|
After
second-stage operation | 123.96±18.03 | 124.49±19.33 | 0.024 | 0.992 |
Changes in coagulation function in the
two groups of patients
The prothrombin time (PT), plasma fibrinogen (FIB)
levels and international normalized ratio (INR) were not
significantly different between the two groups in all four stages
of operation examined (P>0.05). The PT and INR in the two groups
were not significantly different between the time-points prior to
and after the first- and second-stage operation (P>0.05), but
the FIB after the first-stage operation was higher than that prior
to the first-stage operation (P<0.05). The PT in the two groups
of patients was higher after the second-stage operation than that
prior to the second-stage operation (P<0.05), whereas the FIB
level was lower (P<0.05) and the INR was not significantly
changed (P>0.05; Table V).
| Table VChanges in coagulation function in
the two groups of patients. |
Table V
Changes in coagulation function in
the two groups of patients.
| Parameter | Control group
(n=21) | Observation group
(n=19) | F-value | P-value |
|---|
| PT (sec) | | | | |
|
Prior to
first-stage operation | 12.17±1.35 | 12.28±1.24 | 0.267 | 0.791 |
|
After
first-stage operation | 12.63±1.42 | 12.75±1.43 | 0.266 | 0.792 |
|
Prior to
second-stage operation | 14.18±1.51 | 14.29±1.53 | 0.229 | 0.820 |
|
After
second-stage operation |
17.52±1.64a |
17.68±1.71a | 0.302 | 0.764 |
| FIB (g/l) | | | | |
|
Prior to
first-stage operation | 2.63±0.12 | 2.71±0.14 | 1.946 | 0.059 |
|
After
first-stage operation |
4.35±0.83a |
4.28±0.79a | 0.273 | 0.787 |
|
Prior to
second-stage operation | 3.52±0.64 | 3.61±0.63 | 0.447 | 0.657 |
|
After
second-stage operation |
2.31±0.37a |
2.28±0.36a | 0.259 | 0.797 |
| INR | | | | |
|
Prior to
first-stage operation | 1.12±0.15 | 1.14±0.14 | 0.435 | 0.666 |
|
After
first-stage operation | 1.23±0.16 | 1.26±0.16 | 0.592 | 0.557 |
|
Prior to
second-stage operation | 1.42±0.18 | 1.41±0.19 | 0.171 | 0.865 |
|
After
second-stage operation | 1.41±0.18 | 1.42±0.18 | 0.175 | 0.862 |
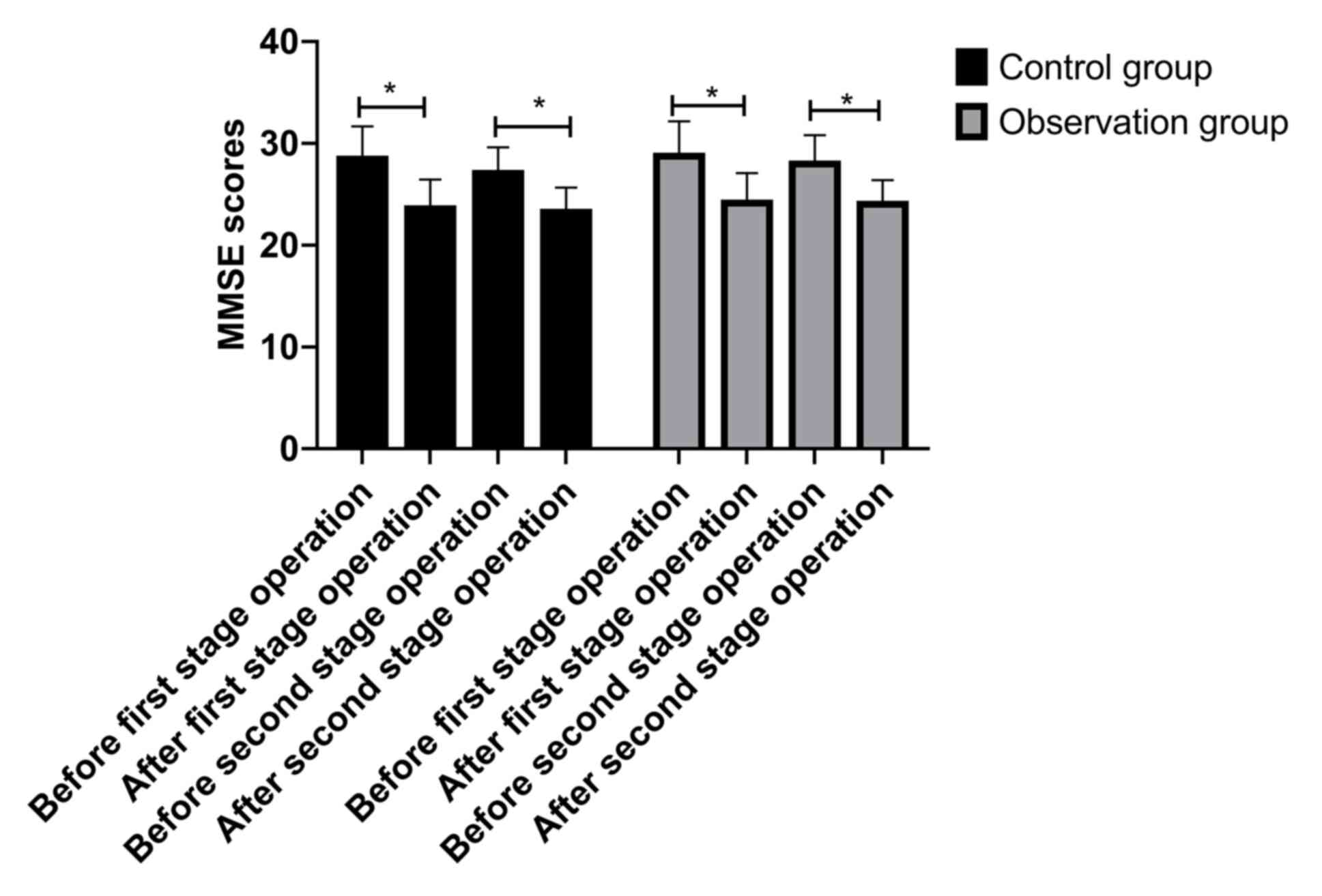
Changes in cognitive function in the
two groups of patients
Although significant declines were noted in
cognitive function after first stage and after second stage
operation within both control and observation groups (P<0.05),
no differences were observed between control and observation groups
at any of the four stages (Fig.
1).
Discussion
The majority of patients are newly diagnosed with
liver cancer at the intermediate and advanced stages, and the use
of ALPPS in the surgical treatment of liver cancer is gradually
increasing (16). Effective and
reasonable anesthesia is an important step to ensure the success
rate and efficacy of surgery (17).
Although the use of ALPPS has been increasing in surgery, only a
few studies are available on the anesthesia for it. The present
study aimed to explore the application of sevoflurane in ALPPS by
retrospectively analyzing the medical records with regard to
propofol and sevoflurane in patients who underwent ALPPS to provide
a reference for clinical surgical anesthesia.
The present study included 40 patients with liver
cancer who underwent ALPPS. No statistically significant
differences between the two groups were identified regarding sex,
age, operation time, operation interval and liver volume growth
rate, suggesting that the data of the two groups included in the
present study were comparable. The results indicated that combined
sevoflurane anesthesia had no significant impact on hemodynamics
compared with propofol anesthesia. No statistically significant
difference in the hemodynamics indicators was identified between
the two groups at any time-point examined. This is similar to the
effect of propofol combined with sevoflurane anesthesia on
hemodynamics in general hepatectomy. Sevoflurane has little to
negligible effects on the respiratory system, does not stimulate
cardiomyocytes to respond to catecholamines and relieves the
decline in respiratory function due to extubation, improves the
blood oxygen supply capacity and stabilizes hemodynamics (18,19).
The study also indicated no significant changes in Hb levels in the
two groups. The anesthetic drugs used in patients undergoing ALPPS
should have low hepatotoxicity and low liver metabolism, should not
accumulate and not increase the liver burden. The liver function
analysis of the two groups of patients indicated a certain amount
of damage; bilirubin accumulation occurred in the peripheral blood,
and ALT and AST levels were increased after first-stage portal vein
ligation. The Tbil and Dbil levels in the peripheral blood of the
two groups were still elevated, but ALT and AST levels were
significantly decreased after the second-stage liver resection,
suggesting that the liver function of the two groups was recovering
to a certain degree. The underlying reason may be that the liver
was resected in the two operations and it was still unable to
completely metabolize bilirubin, so the level of bilirubin was
increased, while reductions in ALT and AST levels were mainly
caused by hepatocyte injury, and after the treatment, the tumor is
basically removed and the liver cells proliferate, so the levels of
ALT and AST are decreased. However, the liver function indicators
of the two groups were not significantly different between the two
groups at any of the time-points regarding the first and second
stage, suggesting that sevoflurane did not affect the liver
function of patients. In certain liver surgeries, propofol combined
with sevoflurane did not impair liver function (20,21).
The results of the present study indicated that the absence of any
changes in leukocyte levels after the first-stage operation may be
due to an increased inflammatory reaction in the body caused by the
separation of bile from the portal vein ligation (22). The proportion of neutrophils also
increased, which also suggested the occurrence of inflammation.
After the second-stage operation, the WBC count of the two groups
decreased, but the WBCs between the two groups were not
significantly different after the second-stage operation, and the
neutrophils also exhibited a downward trend. Anesthesia is well
known to cause a decline of immune function in patients (23). This may also be a reason for the
decline in WBCs after the second-stage operation. The coagulation
function of the two groups of patients was then tested. Spinal
anesthesia was not adopted for ALPPS, as it may affect the
patients' coagulation function. The present results also revealed
certain abnormalities in the coagulation function of the patients
after the first- and second-stage operation. The FIB level of the
two groups exhibited a significant increase after the first-stage
operation, whereas the PT of the two groups increased after the
second-stage operation, and statistically significant difference
was obtained between the groups in the respective indicators of
coagulation function. Certain studies reported that propofol and
sevoflurane affect the coagulation function of patients to a
certain extent, but the effect of sevoflurane on coagulation
function is less than that of propofol (24-26).
Therefore, propofol combined with sevoflurane anesthesia has better
safety in ALPPS, but monitoring of changes in coagulation function
of patients is still necessary to avoid post-operative major
bleeding. Another unavoidable side effect of anesthesia is the
impact on cognitive function (27,28).
The present results indicated a reduction in cognitive function
after the first- and second-stage operation in the two groups, but
propofol combined with sevoflurane did not aggravate the decrease
of the cognitive function of patients, which may be due to the
faster metabolism of sevoflurane. In general, one hour after
stopping inhalation, the concentration of sevoflurane in the blood
may be reduced to 1/20 of the previous concentration, but
sevoflurane also causes inhibition of synaptic function, which is
one of the reasons for its effect on cognitive function (29). However, the effect of propofol
combined with sevoflurane on cognitive dysfunction is generally
acceptable. The present study also included a small number of
cases, so the results and conclusions require verification by
further studies with more clinical data. In addition, it is
required to investigate the mechanism with regard to the degree of
decline in cognitive function in future studies.
In conclusion, propofol combined with sevoflurane
has a good application value in ALPPS, as addition of sevoflurane
has little effect on the hemodynamic stability of patients and
improves the level of inflammatory response, but does not increase
the effects on liver function, coagulation and cognitive
function.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
FX and QHP conceived the study and designed the
experiments. HBJ and MSJ contributed to the data collection,
performed the data analysis and interpreted the results. FX wrote
the manuscript and QHP contributed to the critical revision of the
article. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the hospital ethics
committee of The Jilin Hepatobiliary Hospital (Jilin, China), and
the patients or a family member provided written informed
consent.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing
interests.
References
|
1
|
Kudo M, Matsui O, Izumi N, Iijima H,
Kadoya M, Imai Y, Okusaka T, Miyayama S, Tsuchiya K, Ueshima K, et
al: JSH consensus-based clinical practice guidelines for the
management of hepatocellular carcinoma: 2014 update by the Liver
Cancer Study Group of Japan. Liver Cancer. 3:458–468.
2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kudo M: Surveillance, diagnosis,
treatment, and outcome of liver cancer in Japan. Liver Cancer.
4:39–50. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Oishi N, Yamashita T and Kaneko S:
Molecular biology of liver cancer stem cells. Liver Cancer.
3:71–84. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Ryerson AB, Eheman CR, Altekruse SF, Ward
JW, Jemal A, Sherman RL, Henley SJ, Holtzman D, Lake A, Noone AM,
et al: Annual report to the nation on the status of cancer,
1975-2012, featuring the increasing incidence of liver cancer.
Cancer. 122:1312–1337. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Baltatzis M, Chan AK, Jegatheeswaran S,
Mason J and Siriwardena A: Colorectal cancer with synchronous
hepatic metastases: Systematic review of reports comparing
synchronous surgery with sequential bowel-first or liver-first
approaches. Eur J Surg Oncol. 42:159–165. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Silberhumer GR, Paty PB, Denton B, Guillem
J, Gonen M, Araujo RL, Nash GM, Temple LK, Allen PJ, DeMatteo RP,
et al: Long-term oncologic outcomes for simultaneous resection of
synchronous metastatic liver and primary colorectal cancer.
Surgery. 160:67–73. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Leung U, Gönen M, Allen PJ, Kingham TP,
DeMatteo RP, Jarnagin WR and D'Angelica MI: Colorectal cancer liver
metastases and concurrent extrahepatic disease treated with
resection. Ann Surg. 265:158–165. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Petrowsky H, Györi G, de Oliveira M,
Lesurtel M and Clavien PA: Is partial-ALPPS safer than ALPPS? A
single-center experience. Ann Surg. 261:e90–e92. 2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Lang H, de Santibanes E and Clavien PA:
Outcome of ALPPS for perihilar cholangiocarcinoma: Case-control
analysis including the first series from the international ALPPS
registry. HPB (Oxford). 19:379–380. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Olthof PB, van Gulik TM and Bennink RJ:
The Hiba index for Alpps, preliminary results to interpret with
caution. Ann Surg. 267:e97–e98. 2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Schadde E, Ardiles V, Robles-Campos R,
Malago M, Machado M, Hernandez-Alejandro R, Soubrane O,
Schnitzbauer AA, Raptis D, Tschuor C, et al: Early survival and
safety of ALPPS: First report of the International ALPPS registry.
Ann Surg. 260:829–838. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Pan X, Zhao B, Xiao Y, Hou J and Xia Z:
Effects of different duration of sevoflurane anesthesia in neonatal
period on long-term cognitive func-tion and hippocampal synaptic
plasticity in rats. Chin J Anesthesiol. 36:1085–1088. 2016.
|
|
13
|
Nadalin S, Capobianco I, Li J, Girotti P,
Königsrainer I and Königsrainer A: Indications and limits for
associating liver partition and portal vein ligation for staged
hepatectomy (ALPPS). Lessons learned from 15 cases at a single
centre. Z Gastroenterol. 52:35–42. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Trzepacz PT, Hochstetler H, Wang S, Walker
B and Saykin AJ: Alzheimer's disease neuroimaging initiative.
Relationship between the montreal cognitive assessment and
mini-mental state examination for assessment of mild cognitive
impairment in older adults. BMC Geriatr. 15(107)2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
De Valence T, Elia N, Czarnetzki C, Dumont
L, Tramèr MR and Lysakowski C: Effect of sufentanil on bispectral
index in the elderly. Anaesthesia. 73:216–222. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Xiao L, Li JW and Zheng SG: Totally
laparoscopic ALPPS in the treatment of cirrhotic hepatocellular
carcinoma. Surg Endosc. 29:2800–2801. 2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Jiang Y, Chen Y, Xin L and Shuchang X:
Factors influencing the detection rates of colonoscopic polyp and
adenoma in high-risk population in colorectal cancer screening.
Chin J Digestive Endoscopy. 32:649–652. 2015.
|
|
18
|
Mathur V, Garg D, Jain N, Singhal V, Khare
A and Sethi SK: A comparative study of propofol and N2O versus
sevoflurane and N2O with respect to haemodynamic response and ease
of laryngeal mask airway insertion: A prospective randomized double
blinded study. Int J Res Med Sci. 4:3421–3426. 2017.
|
|
19
|
Khare A, Mathur V, Jain K, Sethi SK, Garg
D and Vishnoi R: A prospective randomized study for comparison of
haemodynamic changes and recovery characteristics with propofol and
sevoflurane anaesthesia during laparoscopic cholecystectomies. Int
J Res Med Sci. 4:5241–5247. 2016.
|
|
20
|
Xu Z, Yu J, Wu J, Qi F, Wang H and Wang Z
and Wang Z: The effects of two anesthetics, propofol and
sevoflurane, on liver ischemia/reperfusion injury. Cell Physiol
Biochem. 38:1631–1642. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Yamada T, Nagata H, Kosugi S, Suzuki T,
Morisaki H and Kotake Y: Interaction between anesthetic
conditioning and ischemic preconditioning on metabolic function
after hepatic ischemia-reperfusion in rabbits. J Anesth.
32:599–607. 2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Neal C, Cairns V, Jones M, Garcea G and
Dennison AR: Comparison of the prognostic value of systemic
inflammatory indices in patients with resectable colorectal liver
metastases. HPB. 18:e722–e723. 2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Zhuo J, Liu C and Yin G: Effects of
dexmedetomidine on the perioperative stress response and
immunologic function in hepatectomy patients with hepatitis
cirrhosis. J Clin Anesthesiol. 32:645–649. 2016.
|
|
24
|
Shoreem H, Ayoub I, Lasheen H, Hegazy O,
Lotfy M, Saleh S, Yassein T, Sallam A, Aziz A, Ibrahim T and Abou
El-Ella K: Improved outcome of emergent management of incarcerated
Para-umbilical hernia in patients with decompensated cirrhosis
under local anesthesia and weak sedation: A prospective randomized
comparative study. HPB. 18:e79–e80. 2016.
|
|
25
|
Bu X, Wang B, Wang Y, Wang Z, Gong C, Qi F
and Zhang C: Pathway-related modules involved in the application of
sevoflurane or propofol in off-pump coronary artery bypass graft
surgery. Exp Ther Med. 14:97–106. 2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Zhang LJ, Lv JP and Wang XY: A comparison
of the effect of propofol versus sevoflurane on blood coagulation
functions of patients undergoing retroperitoneal laparoscopy. J
Clin Anesthesiol. 2(003)2015.
|
|
27
|
Cen S, Haiqing F and Liang L: Comparison
of sevoflurane and propofol on cerebral oxygen metabolism and
postoperative cognitive function during anesthesia maintenance.
Chin J Biochemical Pharmaceutics. 37:177–182. 2017.
|
|
28
|
Yang S, Gu C, Mandeville ET, Dong Y,
Esposito E, Zhang Y, Yang G, Shen Y, Fu X, Lo EH and Xie Z:
Anesthesia and surgery impair blood-brain barrier and cognitive
function in mice. Front Immunol. 8(902)2017.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Sorour K, Vyas P, Raval D, Donovan L and
Vyas A: Successful treatment of severe asthma exacerbation with
sevoflurane inhalation in the intensive care unit. J Anesth Crit
Care Open Access. 3(00092)2015.
|